Back to Journals » Drug Design, Development and Therapy » Volume 20
Induction with Ciprofol Decreases Propofol Requirement During Propofol-Remifentanil Total Intravenous Anesthesia Maintenance in Elderly Patients Undergoing Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Trial
Authors Chen X ![]() , Lai Y, Shen Y, Gao S, Huang X, Yang L, Xiong W
, Lai Y, Shen Y, Gao S, Huang X, Yang L, Xiong W ![]()
Received 12 December 2025
Accepted for publication 13 March 2026
Published 27 March 2026 Volume 2026:20 584998
DOI https://doi.org/10.2147/DDDT.S584998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Tin Wui Wong
Xiaoxiang Chen,* Yu Lai,* Yuekun Shen, Shan Gao, Xiongqing Huang, Lu Yang, Wei Xiong
Department of Anesthesiology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Xiong, Department of Anesthesiology, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 510080, People’s Republic of China, Email [email protected] Lu Yang, Department of Anesthesiology, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 510080, People’s Republic of China, Email [email protected]
Purpose: Elderly patients are susceptible to dose-dependent perioperative hypotension caused by propofol. This study investigates whether general anesthesia induction with ciprofol reduces subsequent propofol maintenance requirements and improves hemodynamic stability compared to propofol induction in elderly patients undergoing total knee arthroplasty (TKA).
Participants and Methods: In this prospective, double-blind, randomized controlled trial, 52 elderly participants (≥ 65 years, ASA I-III) undergoing TKA were randomly allocated to receive propofol (2 mg/kg) or ciprofol (0.4 mg/kg) for anesthesia induction. All participants received standardized anesthesia protocol for maintenance. The primary outcome was the average propofol infusion rate. Secondary outcomes included intraoperative norepinephrine utilization, mean arterial pressure (MAP) fluctuations, time to extubation, and postoperative modified Aldrete scores. Data were analyzed using t-tests, Wilcoxon rank-sum, or Chi-square/Fisher’s exact tests as appropriate.
Results: The mean age was 70.62 ± 3.86 years in the ciprofol group and 69.08 ± 3.52 years in the propofol group with balanced sex distribution. During anesthesia maintenance, the ciprofol group required a significantly lower propofol infusion rate than the propofol group (2.70 ± 0.75 mg/kg/h vs. 4.18 ± 1.66 mg/kg/h; mean difference, − 1.48 mg/kg/h; [95% confidence interval, − 2.19 to − 0.77], P = 0.009). Additionally, the ciprofol group presented with a lower norepinephrine utilization rate (46.2% vs. 84.6%, P = 0.004) and a reduced median norepinephrine infusion rate (0 [interquartile range (IQR), 0– 0.05] μg/kg/min vs. 0.05 [IQR, 0.01– 0.08] μg/kg/min, P = 0.030). Norepinephrine initiation was significantly delayed in the ciprofol group (P = 0.047). No significant differences were observed in MAP variability or postoperative modified Aldrete scores.
Conclusion: In relatively healthy elderly patients undergoing total knee arthroplasty, anesthesia induction with ciprofol is associated with reduced propofol maintenance requirements and decreased intraoperative norepinephrine utilization. Ciprofol may represent a promising alternative for anesthesia induction in this population, although further multicenter validation is warranted.
Keywords: ciprofol, propofol, elderly patients, hypotension, total knee arthroplasty
Introduction
Knee osteoarthritis is a chronic degenerative joint disease and a major cause of disability, particularly among the elderly population.1,2 In elderly Chinese individuals, the prevalence of symptomatic knee osteoarthritis is reported to be 10.3% in women and 5.7% in men.3 Total knee arthroplasty (TKA) represents a standard procedure for patients with end-stage knee osteoarthritis.4 However, aging-related physiological changes render this population more susceptible to intraoperative hemodynamic instability.5
Propofol exerts its sedative effect by potentiation of the inhibitory neurotransmitter γ-aminobutyric acid (GABA) at the GABAA receptor.6 It is widely used for both induction and maintenance of general anesthesia due to its rapid onset, rapid distribution, and quick recovery profile.7 However, propofol-induced dose-dependent hypotension is common in geriatric patients.8 Perioperative hypotension has been associated with acute kidney injury, postoperative delirium, increased mortality and other adverse events in elderly patients.9–11 Therefore, optimal strategies for the prevention of perioperative hypotension, including appropriate choice of combination of general anesthetic drugs, should be carefully considered in this population.
Ciprofol, a novel sedative-hypnotic agent, exhibits a wider therapeutic window compared to propofol.12 Recent studies have demonstrated that ciprofol is noninferior to propofol for successful anesthesia induction13 and provides better hemodynamic stability during induction in elderly patients.14 However, propofol remains the established agent for anesthesia maintenance. It remains unclear whether ciprofol as an induction agent has impact on subsequent propofol-based general anesthesia.
We hypothesized that induction with ciprofol may reduce the propofol requirement during anesthesia maintenance in elderly patients undergoing TKA, thereby attenuating dose-dependent hypotension induced by propofol and improving intraoperative hemodynamic stability. To test this hypothesis, we conducted this prospective, double-blind, randomized controlled trial.
Participants and Methods
Ethics and Recruitment
This prospective, double-blind, randomized controlled trial was approved by the Clinical Research and Laboratory Animal Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University (No: [2025]102) and was registered at the Chinese Clinical Trial Registry (No: ChiCTR2500102267). This trial was conducted in accordance with ethical principles of the Declaration of Helsinki and followed the CONSORT reporting guidelines. Participants were recruited from the First Affiliated Hospital of Sun Yat-sen University between June 2025 and October 2025. Written informed consent was obtained from all participants or their legal authorized representatives.
The inclusion criteria included: (1) age over 65 years regardless of gender; (2) American Society of Anesthesiologists (ASA) physical status I-III; (3) scheduled for total knee arthroplasty. The exclusion criteria included: (1) history of cardiac or cerebrovascular disease; (2) untreated grade 2 or 3 hypertension; (3) hepatic impairment or renal insufficiency; (4) known allergy to eggs, soy products, propofol or ciprofol; (5) participation in another clinical trial within the past month.
Randomization and Blinding
Electronic medical record screening was conducted by an investigator to identify potential trial participants. Random sequence was generated using the website randomizer.org. Participants were randomly assigned to either the propofol or ciprofol groups in a 1:1 ratio. Group allocations were sealed in opaque envelopes and kept by one investigator not involved in recruitment, anesthesia care and outcome assessment. The calculated drug dose for each participant was diluted with normal saline to 25 mL in identical syringes by a research nurse. Syringes were then labelled “trial drug” and provided to the designated anesthesiologists who administrated the induction medication and provided the anesthesia care. Participants, anesthesiologists, surgeons and outcome assessors were blinded to the group assignments, with unblinding being permitted only in emergencies.
Perioperative Management and Intervention
All participants received our center’s standard anesthesia protocol for TKA procedure besides the trial intervention. A detailed timeline of the perioperative management and intervention procedures is presented in Figure 1. On the day of surgery, participants had an intravenous access established and standard monitoring was applied upon arrival in the anesthesia preparation unit. Ultrasound-guided ipsilateral femoral nerve block (FNB) (20 mL of 0.2% ropivacaine) combined with infiltration between the popliteal artery and posterior capsular of the knee (iPACK) (10 mL of 0.2% ropivacaine) was performed for analgesia.
 |
Figure 1 Timeline of the standardized perioperative anesthesia management and intervention protocol. Abbreviations: EtCO2, end-tidal carbon dioxide; FiO2, fraction of inspired oxygen; FNB, femoral nerve block; iPACK, infiltration between the popliteal artery and posterior capsule of the knee; IV, intravenous; LOC, loss of consciousness; MAP, mean arterial pressure; PACU, post-anesthesia care unit; PONV, postoperative nausea and vomiting; TCI, target-controlled infusion. |
Based on the randomized assignment, participants in the propofol group received an intravenous infusion of propofol at a dose of 2 mg/kg over 1 minute for induction, whereas those in the ciprofol group received ciprofol at a dose of 0.4 mg/kg over 1 minute.
This was followed by the administration of rocuronium (0.6 mg/kg) and sufentanil (0.3 μg/kg) after confirmation of loss of consciousness. Endotracheal intubation was performed using a video laryngoscope 5 minutes later. Following intubation, mechanical ventilation was initiated with an oxygen-air mixture (fraction of inspired oxygen, 50%), and ventilation parameters were adjusted to maintain an end-tidal carbon dioxide concentration between 32 and 35 mmHg with a tidal volume of 6–8 mL/kg predicted body weight and a positive end-expiratory pressure of 5 cmH2O. Dexmedetomidine was initiated as a continuous infusion at a rate of 0.5 μg/kg/h after intubation. Concurrently, propofol was administered via plasma-targeted controlled infusion (TCI) using the Marsh model15 with an initial target plasma concentration of 1 μg/mL and remifentanil was delivered through effect-site TCI based on the Minto model16 maintaining an effect-site concentration of at least 2 ng/mL. After induction, an ipsilateral thigh tourniquet was applied by the surgeon at a standardized pressure.
Intraoperatively, the target propofol concentration was adjusted (with a single increment or decrement of 0.1–0.2 μg/mL) to maintain the depth of anesthesia within the range of D2-E1, as monitored by Narcotrend®. The effect-site concentration of remifentanil was maintained at 2–4 ng/mL throughout the procedure. Oropharyngeal temperature was monitored and maintained between 36°C and 37°C using the Bairhugger® system. Lactated Ringer’s solution was infused in accordance with the “4-2-1 rule”17 supplemented with an additional of 4 mL/kg/h. Norepinephrine was initiated at 0.05 μg/kg/min when the intraoperative mean arterial pressure (MAP) was below 65 mmHg and adjusted accordingly to maintain MAP ≥ 65 mmHg. All participants received 5 mg of dexamethasone and 0.25 mg of palonosetron 30 minutes before the end of surgery for postoperative nausea and vomiting (PONV) prophylaxis. At the end of surgery, all anesthetics were discontinued and participants were transferred to the post-anesthesia care unit (PACU). Extubation was performed when the criteria for extubation were met. Participants were discharged from the PACU to the ward when the modified Aldrete score was ≥ 9.
Outcomes
The primary outcome was the average infusion rate of propofol (mg/kg/h) during the anesthesia maintenance phase, calculated as total propofol dose divided by body weight and infusion duration.
Secondary outcomes included: the intraoperative norepinephrine utilization (the utilization rate of norepinephrine, the median infusion rate of norepinephrine and the time to initiation of norepinephrine from anesthesia induction); average intraoperative MAP; range of MAP (maximum - minimum); duration of anesthesia; time to extubation; modified Aldrete score at 1 minute and 5 minutes after emergence from anesthesia.
Sample Size Calculation
Our pilot study revealed a mean difference of 1.097 mg/kg/h in the average propofol infusion rate between groups. Based on this, we aimed to detect a difference with 80% power at a 0.05 significance level, and sample size calculations revealed that a total of 46 participants were required using PASS (version 15.0, NCSS, Kaysville, Utah). Considering a 10% of dropout rate, the final sample size was determined at 52 (26 per group).
Statistical Analysis
Statistical analysis was performed using SPSS (version 27.0, IBM, Chicago, IL). Normally distributed data are expressed as mean ± standard deviation (SD) and were compared using Welch’s t-test. Non-normally distributed data are presented as median (interquartile range [IQR]) and were compared using the Wilcoxon rank-sum test. Categorical data are presented as number (percentage) and were analyzed using the chi-square test or Fisher’s exact test, as appropriate. All randomized patients completed the study without protocol violations. Therefore, the analysis was conducted on an intention-to-treat basis. A two-tailed P < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Participants
A total of 52 participants who met the inclusion and exclusion criteria were enrolled in this study and were randomly assigned to either the propofol group (n = 26) or the ciprofol group (n = 26). All participants completed the scheduled anesthesia and surgery, as shown in Figure 2.
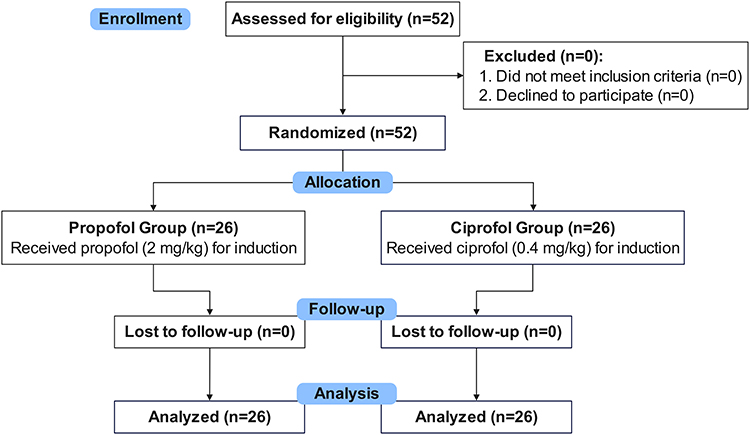 |
Figure 2 CONSORT Flow Diagram. |
Baseline characteristics were well balanced between the two groups (Table 1). The mean age was 69.08 ± 3.52 years in the propofol group and 70.62 ± 3.86 years in the ciprofol group. The proportion of male patients and the distribution of ASA physical status were similar between the two groups. No significant differences were observed in smoking history, alcohol use, and hypertension prevalence. Preoperative laboratory parameters, including hemoglobin level, blood urea nitrogen, and serum creatinine, were also comparable between the groups. Intraoperative parameters, such as duration of anesthesia, and baseline MAP, did not differ significantly.
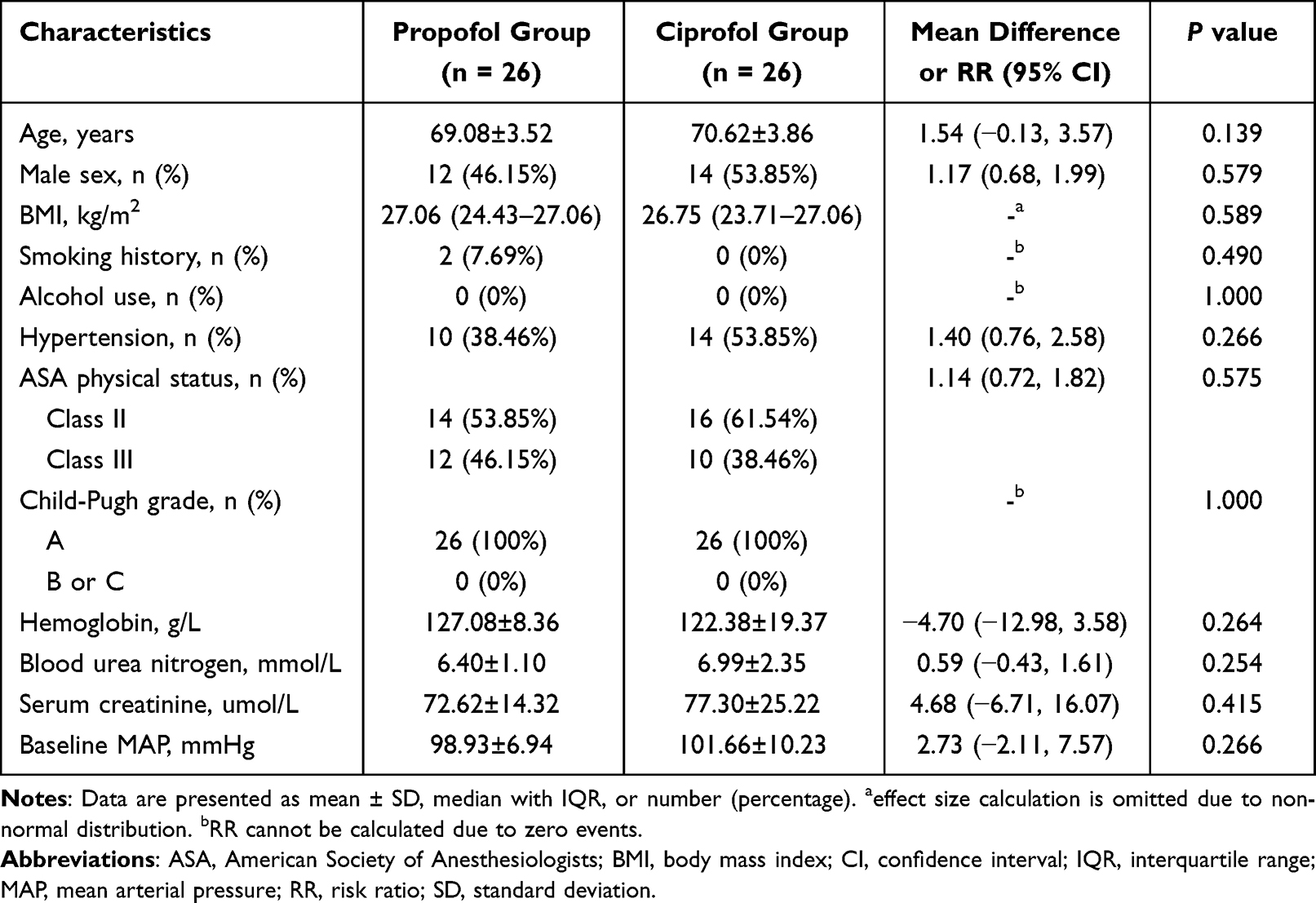 |
Table 1 Baseline Characteristics of Patients in the Propofol Group and Ciprofol Group |
Primary Outcome
The average propofol infusion rate during anesthesia maintenance was significantly lower in the ciprofol group than in the propofol group (4.18 ± 1.66 mg/kg/h in the propofol group vs. 2.70 ± 0.75 mg/kg/h in the ciprofol group; mean difference, −1.48; 95% confidence interval, −2.19 to −0.77; P = 0.009) (Table 2), indicating that participants receiving ciprofol for induction required significantly less propofol infusion rate for maintenance.
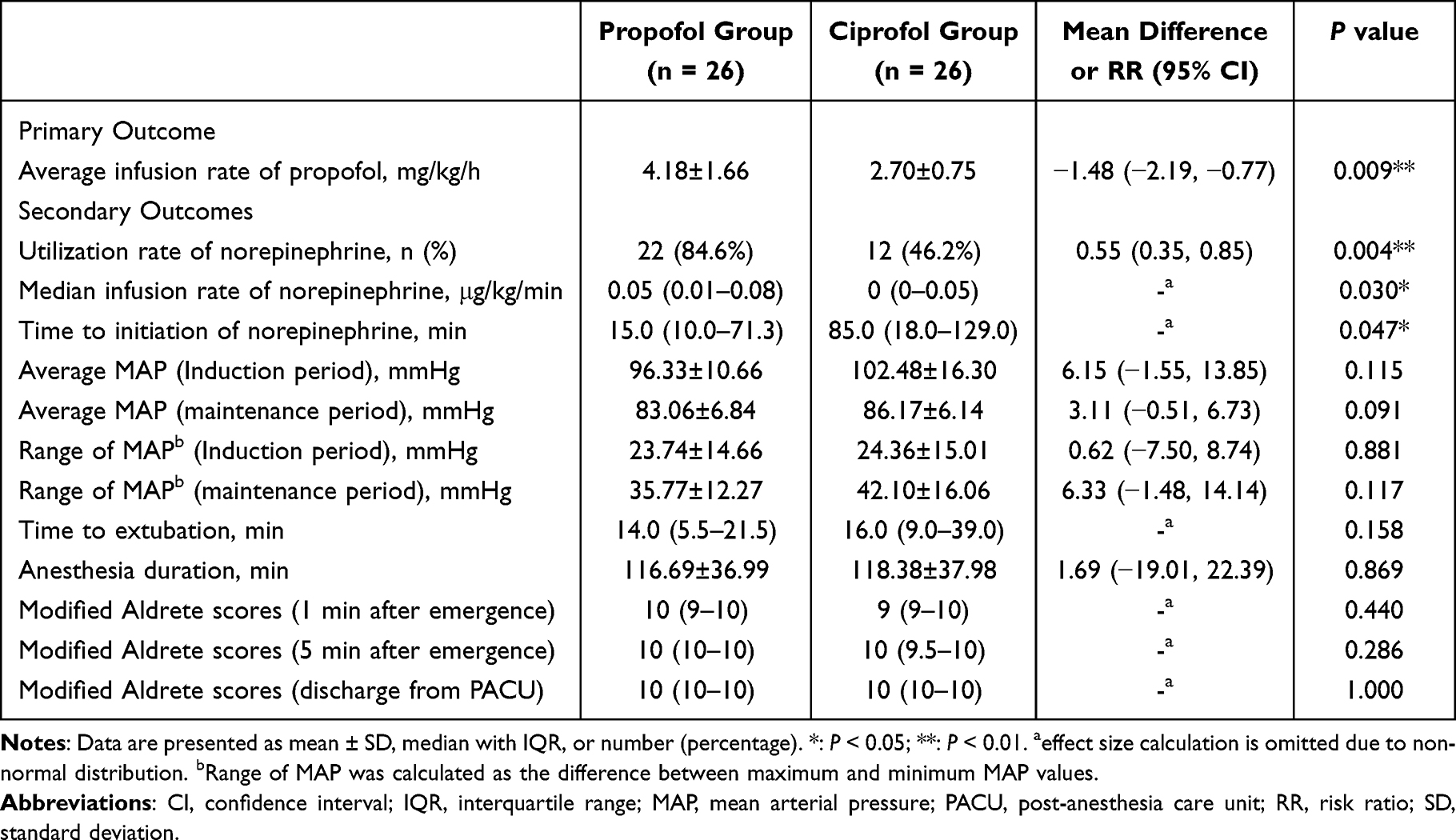 |
Table 2 Primary and Secondary Outcomes of the Two Groups |
Secondary Outcomes
During anesthesia maintenance period, norepinephrine was required in 84.6% of patients in the propofol group vs. 46.2% in the ciprofol group (P = 0.004) (Table 2). The median norepinephrine infusion rate was significantly lower in the ciprofol group (0 [IQR, 0–0.05] μg/kg/min) than in the propofol group (0.05 [IQR, 0.01–0.08] μg/kg/min; P = 0.030). The time interval from induction to the initiation of norepinephrine was also significantly longer in the ciprofol group (85.0 [IQR, 18.0–129.0] min) compared with the propofol group (15.0 [IQR, 10.0–71.3] min, P = 0.047), indicating that patients in the propofol group required earlier norepinephrine support to maintain MAP ≥ 65 mmHg.
The average MAP during both induction and maintenance phases did not show significant differences between two groups. Similarly, the range of MAP (maximum − minimum) was comparable between groups during both phases (Table 2). No significant differences were observed in time to extubation, anesthesia duration, or modified Aldrete scores at any time point (Table 2). The blood pressure trends within the first hour after the start of surgery are illustrated in Figure 3.
 |
Figure 3 Comparison of blood pressure trends between the two groups. Notes: Data were presented as mean ± standard deviation. No statistically significant differences in blood pressure were observed between the two groups at all time points. |
Adverse Events
No severe adverse events such as profound bradycardia requiring intervention, allergic reactions, or delayed emergence were observed in either group. PONV was prevented by routine prophylactic antiemetics. The primary adverse event was transient intraoperative hypotension, which was promptly corrected with norepinephrine infusion as per protocol. No participant experienced sustained hypotension refractory to vasopressor support.
Discussion
This randomized controlled trial demonstrates that, in elderly patients undergoing TKA, induction of general anesthesia with ciprofol significantly reduces the propofol requirement during maintenance and decreases the need for intraoperative norepinephrine support compared with propofol induction. Furthermore, the initiation of norepinephrine is substantially delayed following ciprofol induction. These findings suggest that ciprofol may offer hemodynamic advantages when used as an induction agent in this vulnerable population.
Dose-dependent cardiovascular depressant effects of propofol are a well-established independent predictor of post-induction hypotension.18,19 This effect is particularly pronounced in elderly patients,8 who often require vasopressor support to maintain blood pressure during surgery. Intraoperative hypotension has been shown to be significantly associated with increased 30-day postoperative mortality,20 and is a recognized risk factor for postoperative acute kidney injury.21 In elderly patients, episodes of intraoperative MAP falling below 55 mmHg may also increase the incidence of postoperative delirium.22 Thus, the prevention and prompt management of intraoperative hypotension is critical. Norepinephrine is a commonly used vasopressor to maintain blood pressure in older patients during anesthesia.23 However, overreliance on norepinephrine may introduce additional risks, including reflex reduction in cardiac output, elevations in lactate and glycogen production, and increased susceptibility to postoperative infections.24–28 Therefore, strategies that minimize propofol requirements and reduce norepinephrine use are clinically valuable.
Previous reports have demonstrated that the use of ciprofol instead of propofol for induction was associated with a reduced incidence of hypotension and severe hypotension.29,30 No studies have specifically examined the impact of ciprofol as an induction agent on subsequent propofol-based anesthesia maintenance. In the present study, using ciprofol for general anesthesia induction reduced the propofol maintenance infusion rate by 1.48 mg/kg/h. To put this into clinical perspective, for a standard 70 kg patient, this translates to a reduction of approximately 100 mg of propofol per hour. This reduction may attenuate the dose-dependent hypotension of propofol, thereby reducing the requirement for norepinephrine to maintain MAP during surgery. Regarding postoperative recovery, no statistically significant differences were observed in the time to extubation or recovery scores between the two groups, which is consistent with the previous studies.31,32
Our study also demonstrated that there were no statistically significant differences between the two groups in the average MAP or the intraoperative range of MAP, indicating that blood pressure was maintained at a comparable level throughout surgery. Additionally, the Narcotrend index was maintained within similar ranges in both groups during the procedure, indicating that the observed differences in propofol requirement and norepinephrine consumption were not attributable to variations in the depth of anesthesia. Notably, the norepinephrine was administered later intraoperatively in the ciprofol group than in the propofol induction group, further supporting that ciprofol as an induction agent contributed to more stable blood pressure during subsequent propofol maintenance.
Several mechanisms may explain this phenomenon. The addition of a cyclopropyl group to the side chain of the ciprofol structure disrupts the symmetry of the original molecule by increasing the spatial effect, resulting in stereoselective products.12 A recent study reported this modification enhances ciprofol’s GABAA receptor affinity compared to propofol.33 This enhanced binding is believed to contribute to ciprofol’s improved clinical profile, including more stable hemodynamics and reduced adverse effects during anesthesia induction.14,29 We speculate that a single bolus of ciprofol administered for induction may have a potential synergistic or additive interaction with propofol at the GABAA receptor level, thereby reducing the target blood concentration of propofol required to achieve adequate sedation depth during anesthesia maintenance. However, as ciprofol is characterized by rapid metabolic clearance and its hypnotic effect gradually diminishes over time following a single induction dose, this synergistic interaction wanes throughout the procedure. Consequently, the propofol infusion rate must be titrated upward accordingly to maintain the desired anesthetic depth.
In the standard TKA anesthesia and analgesia protocol of our center, nerve block and dexmedetomidine are two important components of multimodal and opioid sparing analgesia. Peripheral nerve block is strongly recommended by multiple high-quality guidelines for TKA to reduce postoperative pain and opioid requirements without increasing complications or adverse outcomes.34,35 The combination of FNB and iPACK is one of the recommended nerve block methods for TKA.36 And dexmedetomidine is also recommended for elderly patients to reduce postoperative delirium, pain and opioid use.37–39 A recent study revealed that the co-application of nerve block combined with intravenous dexmedetomidine accelerates rehabilitation for elderly patients undergoing TKA.40 These practices align with our study’s perspective which is optimizing perioperative care through anesthetic sparing and enhanced multimodal analgesia to improve the clinical outcomes for elderly patients.
This study has several limitations. First, it was a pragmatic clinical trial conducted under our center’s standardized anesthesia and analgesia protocol specifically for TKA procedure, which may limit generalizability. Second, as a single-center study with a relatively small sample size, we recruited only relatively healthy elderly patients (ASA I-III) without cardiac or cerebrovascular disease. Therefore, our findings may not apply to frail patients or those with significant comorbidities. Third, we did not assess postoperative cognitive outcomes such as delirium or long-term recovery quality. Fourth, the study was not designed to elucidate the molecular mechanisms underlying the observed interaction between ciprofol and propofol. Finally, while we monitored MAP and vasopressor use, we did not measure cardiac output or systemic vascular resistance, which could provide additional insights into hemodynamic changes. Future multicenter trials with larger, more diverse elderly populations are warranted to validate our findings and assess their generalizability.
Conclusion
In elderly patients undergoing total knee arthroplasty, general anesthesia induction with ciprofol significantly reduces the propofol requirement during maintenance and decreases the need for intraoperative norepinephrine support compared with propofol induction. Within the context of a multimodal analgesia protocol, ciprofol represents a promising alternative to propofol for anesthesia induction in relatively healthy geriatric patients. Further multicenter trials are needed to confirm these findings and evaluate their applicability to broader surgical populations.
Data Sharing Statement
Deidentified data supporting the findings of this study are available from the corresponding author on reasonable request. Data will be accessible beginning 6 months after publication and will remain available for 3 years.
Acknowledgments
The authors are grateful to the support from the Department of Anesthesiology and the Department of Joint Surgery of the First Affiliated Hospital of Sun Yat-sen University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mora JC, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: pathophysiology and current treatment modalities. J Pain Res. 2018;11:2189–10. doi:10.2147/JPR.S154002
2. Shao W, Hou H, Han Q, Cai K. Prevalence and risk factors of knee osteoarthritis: a cross-sectional survey in Nanjing, China. Front Public Health. 2024;12:1441408. doi:10.3389/fpubh.2024.1441408
3. Tang X, Wang S, Zhan S, et al. The prevalence of symptomatic knee osteoarthritis in China: results From the China Health and Retirement Longitudinal Study. Arthritis Rheumatol. 2016;68(3):648–653. doi:10.1002/art.39465
4. Price AJ, Alvand A, Troelsen A, et al. Knee replacement. Lancet. 2018;392(10158):1672–1682. doi:10.1016/S0140-6736(18)32344-4
5. Yang R, Wolfson M, Lewis MC. Unique aspects of the elderly surgical population: an anesthesiologist’s perspective. Geriatr Orthop Surg Rehabil. 2011;2(2):56–64. doi:10.1177/2151458510394606
6. Sahinovic MM, Struys MMRF, Absalom AR. Clinical pharmacokinetics and pharmacodynamics of propofol. Clin Pharmacokinet. 2018;57(12):1539–1558. doi:10.1007/s40262-018-0672-3
7. Walsh CT. Propofol: milk of Amnesia. Cell. 2018;175(1):10–13. doi:10.1016/j.cell.2018.08.031
8. Schonberger RB, Dai F, Michel G, et al. Association of propofol induction dose and severe pre-incision hypotension among surgical patients over age 65. J Clin Anesth. 2022;80:110846. doi:10.1016/j.jclinane.2022.110846
9. Maheshwari K, Turan A, Mao G, et al. The association of hypotension during non-cardiac surgery, before and after skin incision, with postoperative acute kidney injury: a retrospective cohort analysis. Anaesthesia. 2018;73(10):1223–1228. doi:10.1111/anae.14416
10. Duan W, Zhou CM, Yang JJ, et al. A long duration of intraoperative hypotension is associated with postoperative delirium occurrence following thoracic and orthopedic surgery in elderly. J Clin Anesth. 2023;88:111125. doi:10.1016/j.jclinane.2023.111125
11. Sessler DI, Bloomstone JA, Aronson S, et al. Perioperative quality initiative consensus statement on intraoperative blood pressure, risk and outcomes for elective surgery. Br J Anaesth. 2019;122(5):563–574. doi:10.1016/j.bja.2019.01.013
12. Qin L, Ren L, Wan S, et al. Design, Synthesis, and Evaluation of Novel 2,6-Disubstituted Phenol Derivatives as General Anesthetics. J Med Chem. 2017;60(9):3606–3617. doi:10.1021/acs.jmedchem.7b00254
13. Gan TJ, Bertoch T, Habib AS, et al. Comparison of the efficacy of HSK3486 and propofol for induction of general anesthesia in adults: a multicenter, randomized, double-blind, controlled, phase 3 noninferiority trial. Anesthesiology. 2024;140(4):690–700. doi:10.1097/ALN.0000000000004886
14. Akhtar SMM, Fareed A, Ali M, et al. Efficacy and safety of ciprofol compared with propofol during general anesthesia induction: a systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024;94:111425. doi:10.1016/j.jclinane.2024.111425
15. Marsh B, White M, Morton N, Kenny GN. Pharmacokinetic model driven infusion of propofol in children. Br J Anaesth. 1991;67(1):41–48. doi:10.1093/bja/67.1.41
16. Minto CF, Schnider TW, Egan TD, et al. Influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology. 1997;86(1):10–23.
17. Holliday MA, Segar WE. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957;19(5):823–832. doi:10.1542/peds.19.5.823
18. Reich DL, Hossain S, Krol M, et al. Predictors of hypotension after induction of general anesthesia. Anesth Analg. 2005;101(3):622–628. doi:10.1213/01.ANE.0000175214.38450.91
19. Kawasaki S, Kiyohara C, Tokunaga S, Hoka S. Prediction of hemodynamic fluctuations after induction of general anesthesia using propofol in non-cardiac surgery: a retrospective cohort study. BMC Anesthesiol. 2018;18(1):167. doi:10.1186/s12871-018-0633-2
20. Nakanishi T, Tsuji T, Sento Y, Hashimoto H, Fujiwara K, Sobue K. Association between postinduction hypotension and postoperative mortality: a single-centre retrospective cohort study. Can J Anaesth. 2024;71(3):343–352. doi:10.1007/s12630-023-02653-6
21. Saugel B, Sander M, Katzer C, et al. Association of intraoperative hypotension and cumulative norepinephrine dose with postoperative acute kidney injury in patients having noncardiac surgery: a retrospective cohort analysis. Br J Anaesth. 2025;134(1):54–62. doi:10.1016/j.bja.2024.11.005
22. Wachtendorf LJ, Azimaraghi O, Santer P, et al. Association between intraoperative arterial hypotension and postoperative delirium after noncardiac surgery: a retrospective multicenter cohort study. Anesth Analg. 2022;134(4):822–833. doi:10.1213/ANE.0000000000005739
23. Vokuhl C, Kouz K, Flick M, et al. Continuous versus bolus norepinephrine administration and arterial blood pressure stability during induction of general anaesthesia in high-risk noncardiac surgery patients: a randomised trial. Br J Anaesth. 2025;135(4):878–885. doi:10.1016/j.bja.2025.06.025
24. Hollenberg SM, Singer M. Pathophysiology of sepsis-induced cardiomyopathy. Nat Rev Cardiol. 2021;18(6):424–434. doi:10.1038/s41569-020-00492-2
25. Lyon AR, Rees PSC, Prasad S, Poole-Wilson PA, Harding SE. Stress (Takotsubo) cardiomyopathy--a novel pathophysiological hypothesis to explain catecholamine-induced acute myocardial stunning. Nat Clin Pract Cardiovasc Med. 2008;5(1):22–29.
26. Carrara M, Ferrario M, Bollen Pinto B, Herpain A. The autonomic nervous system in septic shock and its role as a future therapeutic target: a narrative review. Ann Intensive Care. 2021;11(1):80. doi:10.1186/s13613-021-00869-7
27. Vara E, Tamarit-Rodriguez J. Norepinephrine inhibits islet lipid metabolism, 45Ca2+ uptake, and insulin secretion. Am J Physiol. 1989;257(6 Pt 1):E923–929. doi:10.1152/ajpendo.1989.257.6.E923
28. Yu C, Fan W, Shao M. Norepinephrine dosage is associated with lactate clearance after resuscitation in patients with septic shock. Front Med. 2021;8:761656. doi:10.3389/fmed.2021.761656
29. Lu YF, Wu JM, Lan HY, Xu QM, Shi SQ, Duan GC. Efficacy and safety of general anesthesia induction with ciprofol in hip fracture surgery of elderly patients: a randomized controlled trial. Drug Des Devel Ther. 2024;18:3951–3958. doi:10.2147/DDDT.S475176
30. Chen BZ, Yin XY, Jiang LH, Liu JH, Shi YY, Yuan BY. The efficacy and safety of ciprofol use for the induction of general anesthesia in patients undergoing gynecological surgery: a prospective randomized controlled study. BMC Anesthesiol. 2022;22(1):245. doi:10.1186/s12871-022-01782-7
31. Shi S, Wu J, Wu Y, et al. Effects of ciprofol and propofol general anesthesia on postoperative recovery quality in patients undergoing ureteroscopy: a randomized, controlled, double-blind clinical trial. Drug Des Devel Ther. 2025;19:931–943. doi:10.2147/DDDT.S497554
32. Liang Z, Liu J, Chen S, et al. Postoperative quality of recovery comparison between ciprofol and propofol in total intravenous anesthesia for elderly patients undergoing laparoscopic major abdominal surgery: a randomized, controlled, double-blind, non-inferiority trial. J Clin Anesth. 2024;99:111660. doi:10.1016/j.jclinane.2024.111660
33. Li X, Yang X, Chen C, et al. A chronopharmacological comparison of ciprofol and propofol: focus on sedation and side effects. Front Mol Neurosci. 2025;18:1567453. doi:10.3389/fnmol.2025.1567453
34. Srivastava AK, Surgical Management of Osteoarthritis of the Knee Work Group, Staff of the American Academy of Orthopaedic Surgeons. American Academy of Orthopaedic Surgeons Clinical Practice Guideline Summary of Surgical Management of Osteoarthritis of the Knee. J Am Acad Orthop Surg. 2023;31(24):1211–1220.
35. Memtsoudis SG, Cozowicz C, Bekeris J, et al. Peripheral nerve block anesthesia/analgesia for patients undergoing primary hip and knee arthroplasty: recommendations from the International Consensus on Anesthesia-Related Outcomes after Surgery (ICAROS) group based on a systematic review and meta-analysis of current literature. Reg Anesth Pain Med. 2021;46(11):971–985. doi:10.1136/rapm-2021-102750
36. Xue X, Lv X, Ma X, Zhou Y, Yu N. Postoperative pain relief after total knee arthroplasty: a Bayesian network meta-analysis and systematic review of analgesic strategies based on nerve blocks. J Clin Anesth. 2024;96:111490. doi:10.1016/j.jclinane.2024.111490
37. Sieber F, McIsaac DI, Deiner S, et al. 2025 American Society of Anesthesiologists Practice Advisory for perioperative care of older adults scheduled for inpatient surgery. Anesthesiology. 2025;142(1):22–51. doi:10.1097/ALN.0000000000005172
38. Zhang X, Leng Y, Yuan X, Yang Y, Zhou C, Liu H. Efficacy of perioperative dexmedetomidine in postoperative pain and neurocognitive functions in orthopedic surgery: a systematic review and meta-analysis with trial sequential analysis of randomized controlled trials. Int J Surg. 2025;111(5):3525–3542. doi:10.1097/JS9.0000000000002315
39. Luney M, Holdsworth L, Hanaga A, et al. Effectiveness of drug interventions to prevent delirium after surgery for older adults: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2026;392:e085539. doi:10.1136/bmj-2025-085539
40. Gao C, Huang T, Wu K, et al. Multimodal analgesia for accelerated rehabilitation after total knee arthroplasty: a randomized, double-blind, controlled trial on the effect of the co-application of local infiltration analgesia and femoral nerve block combined with dexmedetomidine. Brain Sci. 2022;12(12):1652. doi:10.3390/brainsci12121652
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Ciprofol for Sedation/Anesthesia in Patients Undergoing Hysteroscopy: A Randomized, Parallel-Group, Controlled Trial
Lan H, Shan W, Wu Y, Xu Q, Dong X, Mei P, Duan G, You M, Jin L, Wu J
Drug Design, Development and Therapy 2023, 17:1707-1717
Published Date: 11 June 2023
Bispectral Index-Monitored Anesthesia Induction in Older Adults Undergoing Elective Surgery: Comparing Ciprofol and Propofol in a Prospective, Single-Center, Double-Blind, Randomized Controlled Study
Zou H, Xi F, Fu Y, Xu J, Zhang P, Li D, Luo H
Drug Design, Development and Therapy 2024, 18:4993-5003
Published Date: 5 November 2024
Effects of Ciprofol and Propofol General Anesthesia on Postoperative Recovery Quality in Patients Undergoing Ureteroscopy: A Randomized, Controlled, Double-Blind Clinical Trial
Shi S, Wu J, Wu Y, Han X, Dai H, Chen X, Sun Z, Wang F
Drug Design, Development and Therapy 2025, 19:931-943
Published Date: 11 February 2025
Effects of Ciprofol on Hemodynamics During Induction in Hypertensive Patients: A Prospective, Randomized, Double-Blind, Controlled Study
Xiao H, Ji M, Shi X, Sun Q, Chen Z, Dong G, Ji F
Drug Design, Development and Therapy 2025, 19:11259-11267
Published Date: 16 December 2025
Comparison of the Efficacy of Ciprofol and Propofol for Rapid Sequence Induction and Intubation in Elective Non-Cardiac Surgery: A Prospective, Randomized, Non-Inferiority Trial
Lin Y, Wu J, Wang C, Wu J, Liu J, Liu M, Miao C, Liang C
Drug Design, Development and Therapy 2026, 20:614980
Published Date: 8 July 2026