Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Ciprofol on Hemodynamics During Induction in Hypertensive Patients: A Prospective, Randomized, Double-Blind, Controlled Study
Authors Xiao H ![]() , Ji M, Shi X
, Ji M, Shi X ![]() , Sun Q, Chen Z, Dong G, Ji F
, Sun Q, Chen Z, Dong G, Ji F ![]()
Received 7 August 2025
Accepted for publication 11 December 2025
Published 16 December 2025 Volume 2025:19 Pages 11259—11267
DOI https://doi.org/10.2147/DDDT.S559096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Hongyi Xiao,1 Mingxin Ji,2 Xinyuan Shi,3 Qingqing Sun,1 Ziyuan Chen,1 Guimin Dong,1,* Fanceng Ji1,*
1Department of Anesthesiology, Weifang People’s Hospital, Weifang, 261041, People’s Republic of China; 2Qingdao Medical College of Qingdao University, Qingdao University, Qingdao, 266071, People’s Republic of China; 3School of Anaesthesiology, Shandong Second Medical University, Weifang, 261053, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanceng Ji, Department of Anesthesiology, Weifang People’s Hospital, Weifang, 261041, People’s Republic of China, Email [email protected] Guimin Dong, Department of Anesthesiology, Weifang People’s Hospital, Weifang, 261041, People’s Republic of China, Email [email protected]
Purpose: This study aims to compare the impact of ciprofol and propofol on post-induction hypotension in hypertensive patients undergoing gynecological surgery.
Patients and Methods: A total of 96 patients undergoing gynecological day surgery were enrolled and randomly assigned to either the propofol group or the ciprofol group. The ciprofol group received 0.5 mg/kg for anesthesia induction, while the propofol group received 2 mg/kg. The primary outcomes included the incidence of hypotension during anesthesia induction and the area under the curve (AUC) of hypotension during the induction phase. The secondary outcomes included the change in mean arterial pressure (MAP), the cumulative dose of vasopressors during induction, the time to loss of consciousness, BIS values, recovery time, the incidence of injection pain, and the incidence of postoperative nausea and vomiting (PONV) in the PACU.
Results: The ciprofol group exhibited significantly better hemodynamic stability compared to the propofol group, with a lower incidence of hypotension (66.7% vs 89.6%, RR= 0.415, 95% CI= 0.189– 0.915, P=0.007) and a smaller area under the curve during induction (− 274.81± 88.41mmHg·min vs − 323.40± 101.32mmHg·min, P=0.014). Secondary outcomes revealed that ciprofol administration resulted in less pronounced MAP fluctuations (37.27± 12.83mmHg vs 44.94± 13.06mmHg, P=0.005), reduced vasopressor requirements (6.0mg [0.0– 6.0] vs 6.0mg [6.0– 6.0], P=0.007), and lower incidence of injection pain (4.2% vs 72.9%, P=0.001). While no significant differences were observed in time to loss of consciousness and BIS values during induction (P> 0.05), the ciprofol group demonstrated a slightly prolonged recovery time (7.0min [5.0– 8.0] vs 5.0min [4.0– 6.0], P=0.004). In the PACU, there was no difference in the incidence of PONV between the two groups (4.2% vs 2.1%, P = 1.000).
Conclusion: Compared with propofol, ciprofol demonstrates superior hemodynamic stability during anesthesia induction in hypertensive patients.
Keywords: ciprofol, hemodynamics, hypertension, propofol, anesthesia, general
Introduction
General anesthesia induction represents a critical phase in the perioperative period,1 particularly for hypertensive patients who demonstrate a higher incidence of hemodynamic instability during this stage.2 Such instability may precipitate severe cerebrovascular complications and potentially compromise perioperative safety.3,4 Consequently, optimizing anesthesia induction protocols for hypertensive patients has emerged as a pivotal research focus in clinical anesthesiology.
Currently, propofol is widely used as a classic intravenous anesthetic induction agent due to its rapid onset and fast metabolism.5 However, its potent vasodilatory effects can induce hypotension,6,7 particularly in hypertensive patients. These patients often exhibit elevated baseline vascular tension and reduced cardiovascular compensatory capacity,8 making them more susceptible to drastic blood pressure fluctuations after propofol induction, which may further increase the risk of inadequate organ perfusion. Additionally, propofol has adverse effects such as injection pain and respiratory depression.9 In recent years, the introduction of novel intravenous anesthetics such as ciprofol and remimazolam has provided more potential alternatives for clinical practice.10–12 As a GABAA receptor agonist, ciprofol exhibits approximately five times stronger receptor binding affinity than propofol, while sharing similar mechanisms of action and pharmacokinetic profiles.11,13 Preliminary clinical studies indicate that compared with propofol, ciprofol demonstrates milder respiratory depression, more stable hemodynamics, and significantly reduced incidence of injection pain.14,15 Furthermore, its anesthetic success rate has been shown to be non-inferior to that of propofol.16
Although ciprofol demonstrates promising clinical potential, its efficacy in hypertensive patients remains unclear. To address this knowledge gap, this study aims to systematically evaluate the clinical effects of ciprofol for general anesthesia induction in hypertensive patients, thereby providing high-quality evidence to optimize anesthetic management for this population.
Materials and Methods
Study Design and Patient Enrollment
This study was approved by the Medical Research Ethics Committee of Weifang People’s Hospital and registered at the Chinese Clinical Trial Registry (www.chictr.org.cn; registration number: ChiCTR2500103391). The research was conducted at Weifang People’s Hospital with written informed consent obtained from all participating patients.
This study is a prospective, randomized, double-blind, controlled trial. Patients scheduled to undergo gynecological surgery under general anesthesia between May 2025 and July 2025 were selected. The inclusion criteria were as follows: aged 18–65 years, ASA class II–III, body mass index of 18–28 kg/m2, with a clinical diagnosis of hypertension and treated with a single antihypertensive medication in the past six months. Exclusion criteria included: preoperative blood pressure > 180/110 mmHg upon entering the operating room; patients with liver or kidney diseases, specifically those with abnormal liver or kidney function that impairs their ability to perform physiological processes such as metabolism, excretion, and detoxification; anticipated difficult airway; potential allergy to study-related medications; psychiatric or cognitive impairment; patients who received sedatives/anesthetics within 24 hours before anesthesia induction; and patients with cardiovascular comorbidities other than hypertension.
A researcher involved only in randomization allocated patients in a 1:1 ratio to either the ciprofol group or the propofol group using a random number table, with 48 patients in each group. The randomization results were sealed in sequentially numbered envelopes, and a staff member not involved in data collection prepared the study drugs according to the assigned group. Ciprofol and propofol are both presented as white emulsions with identical appearance. Moreover, since the induction dose was 0.2 mL/kg for both agents, the patients, anesthesiologists, and researchers responsible for postoperative follow-up and data analysis blinded to group assignment throughout the study.
Anesthesia Management
Patients were routinely fasted before surgery. Upon entering the operating room, standard monitoring was established, including electrocardiogram (ECG), non-invasive blood pressure, pulse oximetry (SpO2), and bispectral index (BIS). Before anesthesia induction, patients received oxygen via face mask at 6 L/min, followed by intravenous flurbiprofen axetil 50 mg and dexamethasone 5 mg. Anesthesia induction: In the ciprofol group, ciprofol 0.5 mg/kg was intravenously infused via syringe pump over 1 minute (total volume 0.2 mL/kg), while in the propofol group, propofol 2 mg/kg was administered using the same method and volume. Immediately after drug administration, the patient’s sedation level was assessed every 10 seconds using the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale until a MOAA/S score ≤1 was achieved. If the patient failed to achieve adequate sedation within 2 minutes, a supplemental dose of either ciprofol 0.25 mg/kg or propofol 1 mg/kg was administered accordingly. Upon successful induction (MOAA/S ≤1), patients received intravenous alfentanil 20 μg/kg followed by mivacurium 0.2 mg/kg. The laryngeal mask airway was inserted after 2 minutes, followed by initiation of mechanical ventilation to maintain adequate respiration. For anesthesia maintenance, patients in the ciprofol group received a continuous intravenous infusion of ciprofol at 1.25 mg/kg/h (0.5 mL/kg/h) combined with alfentanil at 40 μg/kg/h, while those in the propofol group received propofol at 5 mg/kg/h (0.5 mL/kg/h) with the same dose of alfentanil. The BIS was maintained within the target range of 40–60 for both groups during the entire maintenance phase. During the procedure, if the mean arterial pressure (MAP) dropped below 65 mmHg or decreased by more than 30% from baseline, the anesthesiologist administered ephedrine 6 mg or higher doses as needed. Atropine 0.5 mg was administered when a patient’s heart rate fell below 50 beats per minute. At the conclusion of surgery, all anesthetic maintenance medications were discontinued. Following recovery from anesthesia, the laryngeal mask airway was removed and the patient was transferred to the post-anesthesia care unit (PACU). Upon meeting PACU discharge criteria, patients were transferred to the general ward. Those who fulfilled the institutional discharge criteria were permitted to leave the hospital accompanied by family members.
Assessment of Primary and Secondary Outcomes
The primary outcome: The incidence of hypotension during anesthesia induction and the area under the curve (AUC) of hypotension during the induction period. Hypotension was defined as a mean arterial pressure (MAP) below 65 mmHg or a 30% decrease from baseline levels.17 The anesthesia induction period was defined as the interval from the start of anesthesia induction to the beginning of surgery. Hemodynamic changes were observed and recorded at the following time points: 5 minutes after entering the operating room (T0), before anesthesia induction (T1), immediately after anesthesia induction (T2), after laryngeal mask insertion (T3), and at the start of surgery (T4). Each time point after T1 was spaced 2 minutes apart. The detailed study procedure is shown in Figure 1. The average blood pressure at T0 and T1 was taken as the baseline blood pressure (Tbaseline). The calculation of AUC was derived based on formulas from previous relevant literature.18 The formula for calculating the AUC based on the patient’s baseline mean arterial pressure(MAP) is as follow:∑(((MAPi −MAPbaseline)+(MAPi-1 −MAPbaseline))/2 × ΔX). MAPi is the MAP at Ti (i = 2,3,4), with each time point spaced 2 minutes apart, and ΔX is the time interval between measurements.
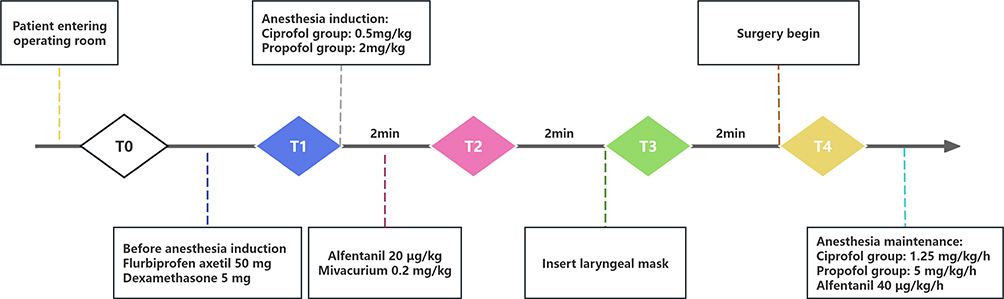 |
Figure 1 Study procedure. |
The secondary outcomes included the change in mean arterial pressure (ΔMAP, defined as the difference between the minimum MAP and baseline MAP), the cumulative dose of vasopressors during induction, the time to loss of consciousness (from study agent injection to disappearance of both consciousness and eyelash reflex), BIS values at each time point during induction, recovery time (from discontinuation of anesthetics to eye opening), the incidence of injection pain (patient-reported arm pain during drug infusion), and the incidence of postoperative nausea and vomiting (PONV) in the PACU.
Statistical Analysis
The sample size was calculated based on the results of a pilot study, in which the incidence rates of hypotension during the induction period of anesthesia were 57.9% for ciprofol and 83.2% for propofol. With the parameters set at α=0.05, 1-β=0.8, and a 1:1 ratio between the two groups, the sample size was computed using PASS software (2021 version). The calculation indicated that 48 patients were required for each group.
Normality was assessed using the Shapiro–Wilk test. Normally distributed continuous variables were expressed as mean ± standard deviation ( ) and compared between groups using the independent samples t-test, while non-normally distributed continuous variables were presented as median (M) with interquartile range (IQR) and analyzed using the Mann–Whitney U-test. Categorical data were described as percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. For continuously distributed variables with repeated measures, a two-way repeated measures ANOVA was employed to evaluate the effects of group, time, and their interaction. A P-value <0.05 was considered statistically significant. Multiple comparisons were adjusted using the Bonferroni correction for p-values. All analyses were generated using R (Version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria).
) and compared between groups using the independent samples t-test, while non-normally distributed continuous variables were presented as median (M) with interquartile range (IQR) and analyzed using the Mann–Whitney U-test. Categorical data were described as percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. For continuously distributed variables with repeated measures, a two-way repeated measures ANOVA was employed to evaluate the effects of group, time, and their interaction. A P-value <0.05 was considered statistically significant. Multiple comparisons were adjusted using the Bonferroni correction for p-values. All analyses were generated using R (Version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 103 patients were screened for this study. Among them, 6 patients did not meet the inclusion criteria and 1 patient refused to participate. Ultimately, 96 patients were enrolled and randomly assigned to either the ciprofol group or the propofol group (Figure 2).
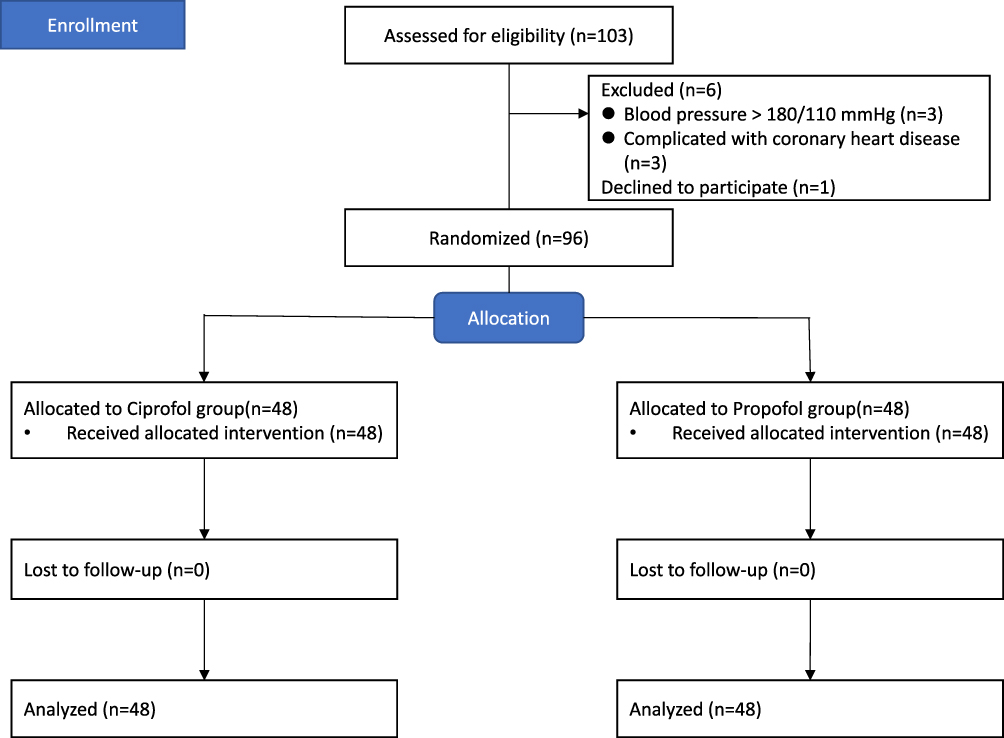 |
Figure 2 Study flowchart. |
Among the 96 enrolled patients, the mean age was 49.65±7.86 years. No statistically significant differences were observed in baseline characteristics or intraoperative features between the two groups (Table 1). Additionally, the success rate of anesthesia induction with a single dose was 100% in both groups, with no need for supplemental doses.
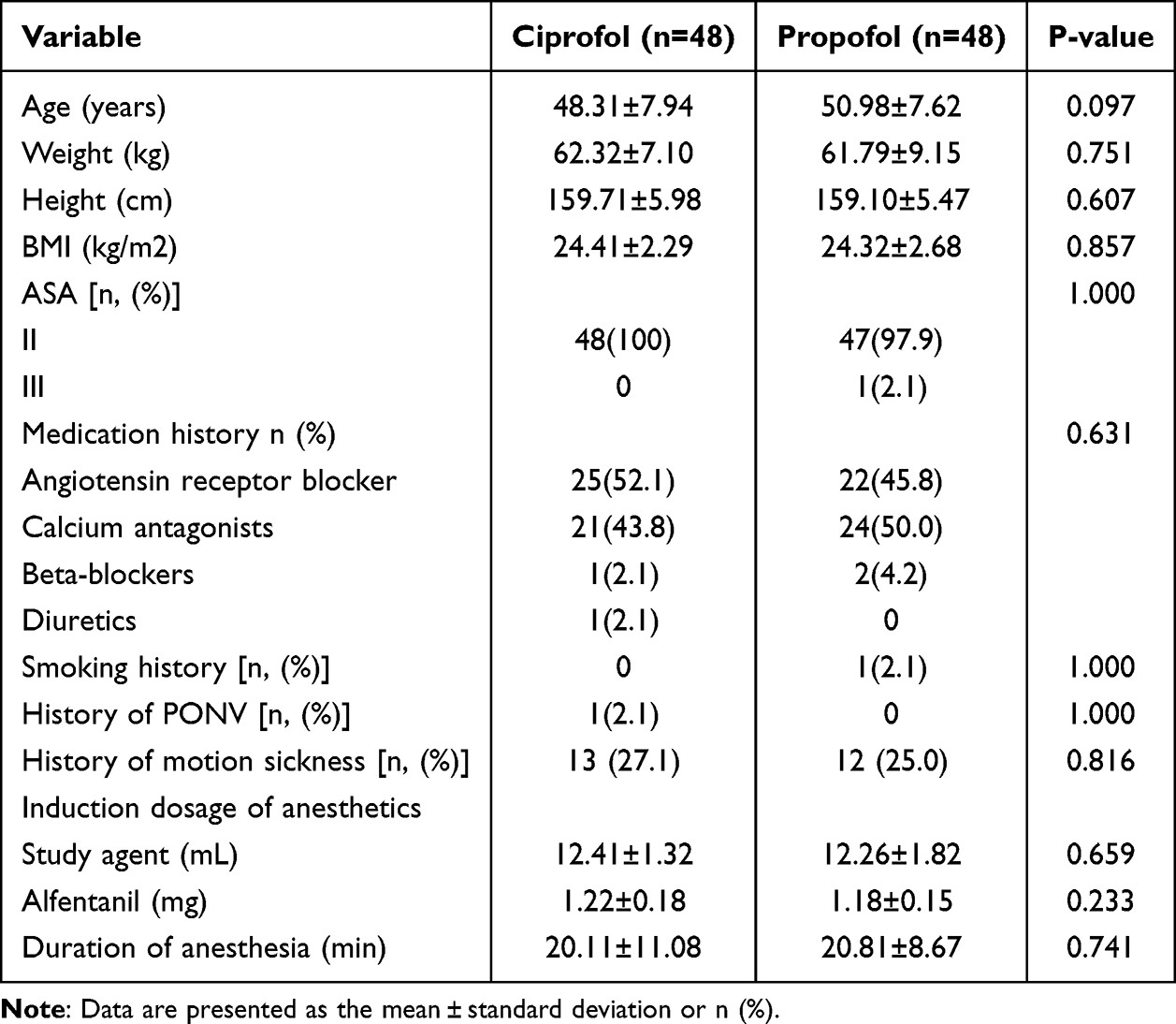 |
Table 1 Baseline Characteristics or Intraoperative Features of the Patients |
For the primary outcome, the incidence of hypotension was significantly lower in the ciprofol group compared to the propofol group (66.7% vs 89.6%, RR= 0.415, 95% confidence interval [95% CI] = 0.189–0.915, P=0.007). Additionally, the AUC during induction was significantly smaller in the ciprofol group (−274.81±88.41mmHg·min vs −323.40±101.32mmHg·min, P=0.014) (Table 2).
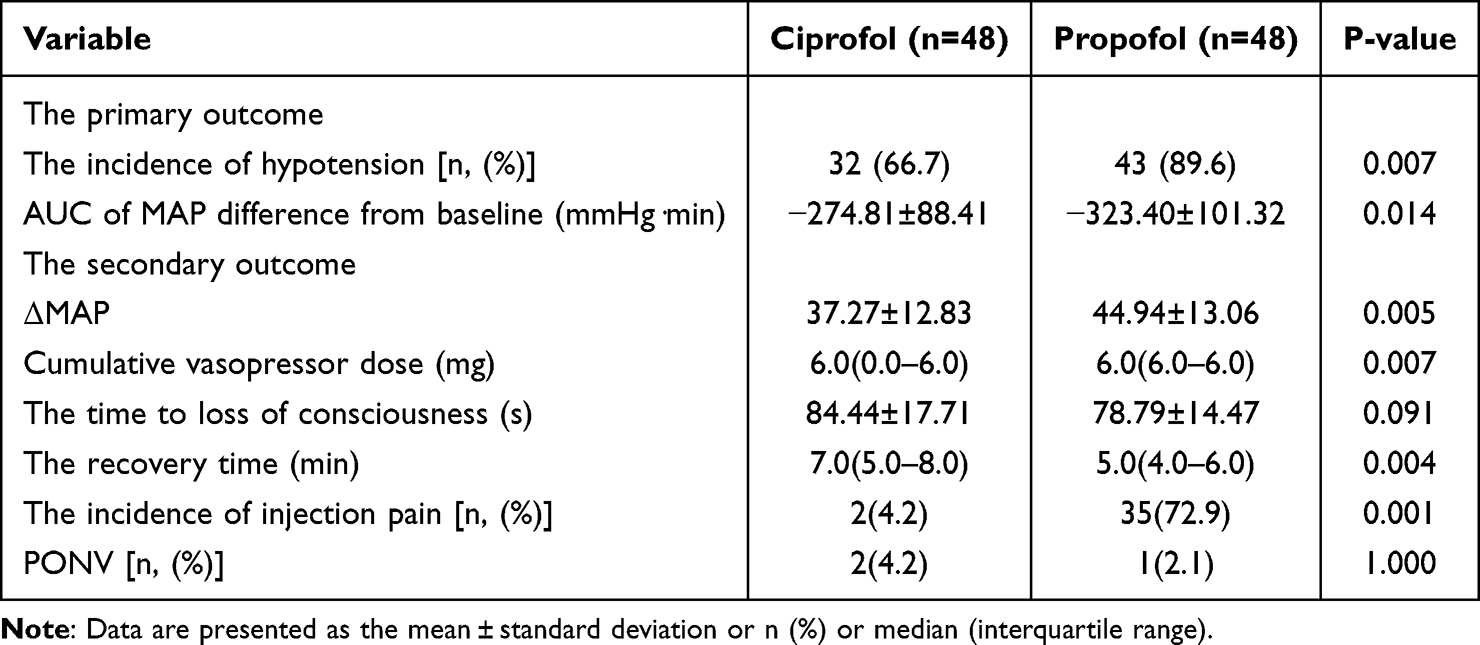 |
Table 2 Comparison of Hemodynamic Effects Between Ciprofol and Propofol in Patients Undergoing Induction of Anesthesia |
For repeatedly measured MAP, the study revealed statistically significant effects for time, group, and their interaction (Table 3). Although MAP in both groups gradually decreased over time, the interaction effect indicated that the trends of change differed between the two groups. At time points T3 and T4 during the induction period, MAP was higher in the ciprofol group than in the propofol group (P < 0.05), suggesting more stable hemodynamic changes.
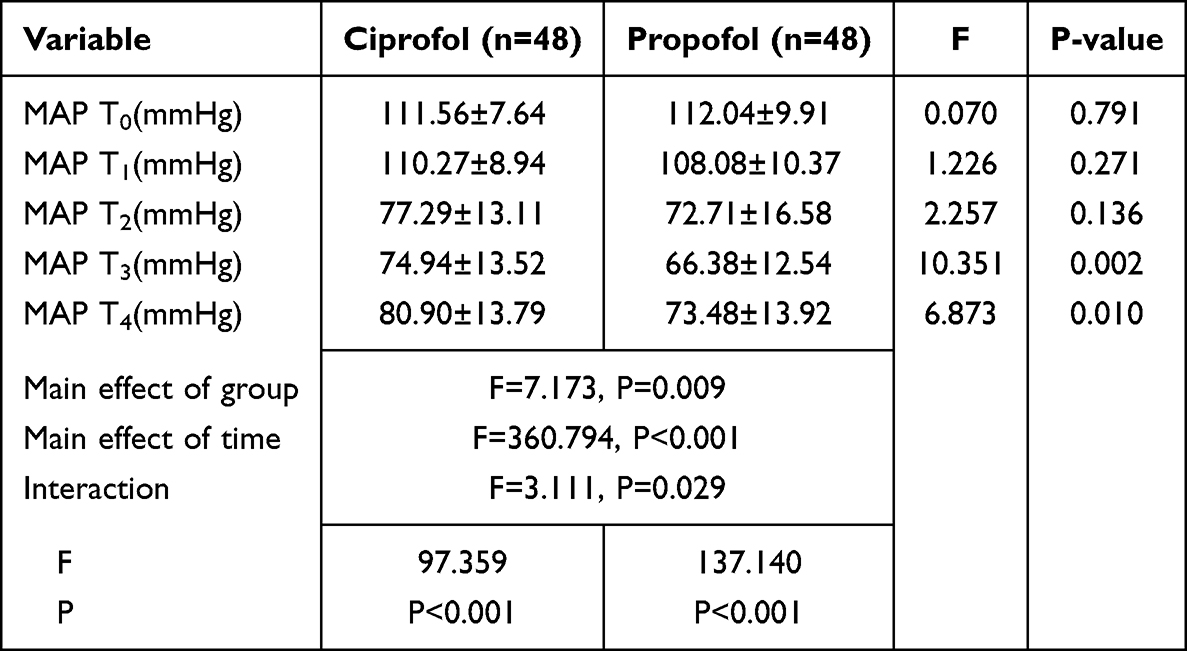 |
Table 3 Repeated-Measures ANOVA of MAP |
For the repeatedly measured BIS values, the study showed a statistically significant effect of time, but no statistically significant effects of group or group-time interaction (Table 4). This indicates that the BIS values in both groups gradually decreased over time, and the changing trends of BIS values were consistent between the two groups.
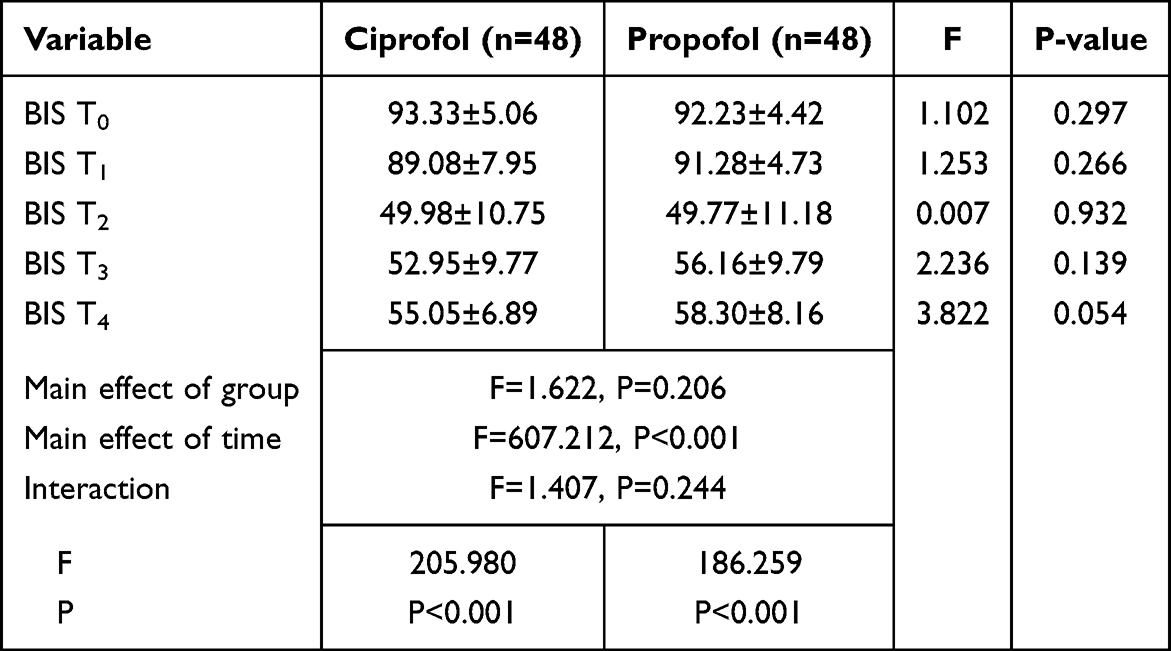 |
Table 4 Repeated-Measures ANOVA of BIS |
Among secondary outcomes, the ciprofol group demonstrated significantly less hemodynamic fluctuation (ΔMAP) compared to the propofol group (37.27±12.83 vs 44.94±13.06, P=0.005). Additionally, the ciprofol group required significantly lower doses of vasopressors (ephedrine) during the induction period (6.0 mg [0.0–6.0] vs 6.0 mg [6.0–6.0], P=0.007).
During the induction period, the incidence of injection pain was significantly lower in the ciprofol group compared to the propofol group (4.2% vs 72.9%, P=0.001). No statistically significant differences were observed between the two groups in terms of time to loss of consciousness or changes in BIS values during induction (P>0.05).
The recovery time was significantly longer in the ciprofol group compared to the propofol group (7.0min [5.0–8.0] vs 5.0min [4.0–6.0], P=0.004). In the PACU, there was no significant difference in the incidence of PONV between the two groups (4.2% vs 2.1%, P=1.000).
Hemodynamic changes during the induction period in the two groups of patients are shown in Figure 3
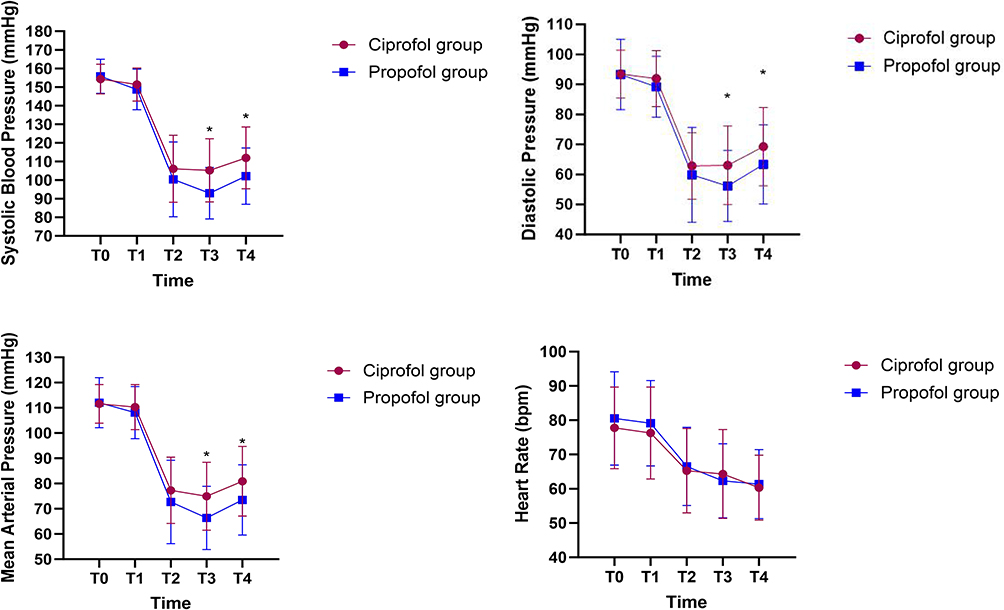 |
Figure 3 Hemodynamic Changes during Anesthesia Induction in Hypertensive Patients. *P<0.05 between-group. |
Discussion
This study found that for hypertensive patients during the induction period, ciprofol demonstrated superior hemodynamic stability compared to propofol at equivalent doses. Additionally, we continuously monitored the BIS values of patients in both groups during the procedure and observed no significant differences between the two groups. Therefore, it can also be concluded that, at equivalent sedation depths, ciprofol provides more stable hemodynamics for anesthetic induction in hypertensive patients.
Current evidence has confirmed the efficacy and safety of ciprofol for general anesthesia induction in healthy patients, but studies on special populations such as hypertensive patients remain limited. Hypertension is a systemic disorder characterized by pathological changes including intermittent spasmodic contraction and hyalinization of small arteries, as well as persistent elevated blood pressure leading to secondary target organ damage and multi-organ dysfunction.19,20 Existing studies indicate that hypertensive patients have a significantly higher incidence of hypotension during anesthesia induction compared to non-hypertensive individuals, thereby increasing their risk of intraoperative organ injury.21 As the first study to evaluate the anesthetic induction effects of ciprofol in hypertensive patients, this research provides critical evidence for its clinical application in this population.
In terms of hypotension during the induction period, ciprofol has demonstrated certain advantages. A Phase III clinical trial involving 120 gynecological surgery patients compared the hemodynamic changes between ciprofol and propofol during general anesthesia induction.22 The study found that ciprofol resulted in more stable blood pressure post-induction and had a lesser impact on circulation. Similarly, the study by Lu et al also reached comparable conclusions, confirming that ciprofol maintains more stable hemodynamics following anesthesia induction.23 However, the current body of research literature supporting this conclusion remains relatively limited, and most of the patients included in these studies had relatively normal preoperative blood pressure. This study specifically investigated hypertensive patients and systematically evaluated hemodynamic changes during anesthesia induction between the two anesthetic agents. It was found that compared with the propofol group, the incidence of hypotension in the ciprofol group during the induction period decreased by 22.9%, and the AUC decreased by 15%. Moreover, in patients induced with ciprofol, the fluctuation of mean arterial pressure during the induction period was smaller, and the cumulative dosage of vasoactive drugs (ephedrine) used was lower.
Regarding perioperative adverse effects, this study found that the incidence of injection pain during induction was significantly lower with ciprofol than with propofol. Injection pain is one of the most common adverse reactions associated with propofol. Previous studies have reported that approximately 70% of patients experience propofol-related injection pain,24 which is consistent with our current findings. As for PONV in the PACU, no significant difference was observed between the two groups. We believe that the mechanism by which ciprofol prevents PONV may be similar to that of propofol, as ciprofol is formed by introducing a cyclopropyl group into the molecular structure of propofol. Furthermore, we noted that the recovery time in the ciprofol group was slightly prolonged compared to the propofol group, though all recovery durations remained within clinically acceptable ranges. This is similar to the results of some previous studies,14,25 which may be related to the extremely short initial distribution half-life and high clearance rate of propofol.26
This study has several limitations. As a single-center prospective study, it found that ciprofol provides more stable hemodynamics during the induction period in hypertensive patients compared to propofol. However, these findings still require further validation through multicenter studies with larger sample sizes. The study did not stratify patients based on the severity of hypertension and only excluded those with severe preoperative hypertension. The enrolled hypertensive population was relatively healthy, with no coexisting cardiovascular diseases. Therefore, further research is needed to evaluate the effects in patients with severe cardiovascular comorbidities. Furthermore, despite rigorous blinding procedures in our study design, the high incidence of injection pain with propofol presents a potential risk of unblinding.
Conclusion
Compared with propofol, ciprofol demonstrates superior hemodynamic stability during anesthesia induction in hypertensive patients.
Data Sharing Statement
The datasets generated in this study are available from the first author (Hongyi Xiao, Email: [email protected]) upon reasonable request.
Ethics Approval
This study was approved by the Medical Ethics Committee of the Weifang People’s Hospital (approval number: KYLL20250508-4). Registered in the Chinese Clinical Trial Registry (www.chictr.org.cn; registration number: ChiCTR2500103391), the study was conducted at Weifang People’s Hospital and all enrolled patients provided signed informed consent. This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol followed the CONSORT guidelines.
Acknowledgments
We thank the patients who participated in this study.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Aslan NA, Ç V, Yılmaz AA, Alanoğlu Z. Propofol versus thiopental for rapid-sequence induction in isolated systolic hypertensive patients: a factorial randomized double-blind clinical trial. Turk J Anaesthesiol Reanim. 2018;46(5):367–372. doi:10.5152/TJAR.2018.44442
2. Huang Y, Yan T, Lu G, Luo H, Lai Z, Zhang L. Efficacy and safety of remimazolam compared with propofol in hypertensive patients undergoing breast cancer surgery: a single-center, randomized, controlled study. BMC Anesthesiol. 2023;23(1):409. doi:10.1186/s12871-023-02364-x
3. Jor O, Maca J, Koutna J, et al. Hypotension after induction of general anesthesia: occurrence, risk factors, and therapy. A prospective multicentre observational study. J Anesth. 2018;32(5):673–680. doi:10.1007/s00540-018-2532-6
4. Hanada S, Kawakami H, Goto T, Morita S. Hypertension and anesthesia. Curr Opin Anaesthesiol. 2006;19(3):315–319. doi:10.1097/01.aco.0000192811.56161.23
5. Sahinovic MM, Mmrf S, Absalom AR. Clinical pharmacokinetics and pharmacodynamics of propofol. Clin Pharmacokinet. 2018;57(12):1539–1558. doi:10.1007/s40262-018-0672-3
6. Chang KS, Davis RF. Propofol produces endothelium-independent vasodilation and may act as a Ca2+ channel blocker. Anesth Analg. 1993;76(1):24–32. doi:10.1213/00000539-199301000-00005
7. Bang JY, Kim S, Choi BM, Kim TY. Pharmacodynamic analysis of the influence of propofol on left ventricular long-axis systolic performance in cardiac surgical patients. J Korean Med Sci. 2019;34(16):e132. doi:10.3346/jkms.2019.34.e132
8. Yancey R. Anesthetic management of the hypertensive patient: part I. Anesth Prog. 2018;65(2):131–138. doi:10.2344/anpr-65-02-12
9. Marik PE. Propofol: therapeutic indications and side-effects. Curr Pharm Des. 2004;10(29):3639–3649. doi:10.2174/1381612043382846
10. J DU, Licheri M, Barucco G, et al. Remimazolam for anesthesia and sedation in cardiac surgery and for cardiac patients undergoing non-cardiac surgery: a systematic-narrative hybrid review. Minerva Anestesiol. 2024;90(7–8):682–693. doi:10.23736/S0375-9393.24.17943-6
11. Lu M, Liu J, Wu X, Zhang Z. Ciprofol: a novel alternative to propofol in clinical intravenous anesthesia? Biomed Res Int. 2023;2023:7443226. doi:10.1155/2023/7443226
12. Sneyd J. Remimazolam – current status, opportunities and challenges. APS. 2023;1(25). doi:10.1007/s44254-023-00021-7
13. Liao J, Li M, Huang C, et al. Pharmacodynamics and pharmacokinetics of HSK3486, a novel 2,6-disubstituted phenol derivative as a general anesthetic. Front Pharmacol. 2022;13:830791. doi:10.3389/fphar.2022.830791
14. Li J, Wang X, Liu J, et al. Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: a multi-centre, non-inferiority, randomized, controlled Phase 3 clinical trial. Basic Clin Pharmacol Toxicol. 2022;131(2):138–148. doi:10.1111/bcpt.13761
15. Hu C, Ou X, Teng Y, et al. Sedation effects produced by a ciprofol initial infusion or bolus dose followed by continuous maintenance infusion in healthy subjects: a phase 1 trial. Adv Ther. 2021;38(11):5484–5500. doi:10.1007/s12325-021-01914-4
16. Cheng S, Wu H, Liu Z, Liu D, Cao M, Fu G. Efficacy and safety of ciprofol for sedation/anesthesia in patients undergoing hysteroscopy: a prospective, randomized, non-inferiority trial. Ann Med. 2025;57(1):2517820. doi:10.1080/07853890.2025.2517820
17. Terwindt LE, Tol JTM, van der Ven WH, et al. The influence of anesthetic drug strategy on the incidence of post-induction hypotension in elective, non-cardiac surgery - A prospective observational cohort study. J Clin Anesth. 2024;99:111671. doi:10.1016/j.jclinane.2024.111671
18. Ni T, Zhou X, Wu S, et al. Hemodynamic impact of cipepofol vs propofol during anesthesia induction in patients with severe aortic stenosis: a randomized clinical trial. JAMA Surg. 2025;160(7):763–770. doi:10.1001/jamasurg.2025.1299
19. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi:10.1016/s0140-6736(02)11911-8
20. Lawes CM, Rodgers A, Bennett DA, et al. Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens. 2003;21(4):707–716. doi:10.1097/00004872-200304000-00013
21. Kalezic N, Stojanovic M, Ladjevic N, et al. Risk factors for intraoperative hypotension during thyroid surgery. Med Sci Monit. 2013;19:236–241. doi:10.12659/MSM.883869
22. Chen BZ, Yin XY, Jiang LH, Liu JH, Shi YY, Yuan BY. The efficacy and safety of ciprofol use for the induction of general anesthesia in patients undergoing gynecological surgery: a prospective randomized controlled study. BMC Anesthesiol. 2022;22(1):245. doi:10.1186/s12871-022-01782-7
23. Lu YF, Wu JM, Lan HY, Xu QM, Shi SQ, Duan GC. Efficacy and safety of general anesthesia induction with ciprofol in hip fracture surgery of elderly patients: a randomized controlled trial. Drug Des Devel Ther. 2024;18:3951–3958. doi:10.2147/DDDT.S475176
24. Bakhtiari E, Mousavi SH, Gharavi Fard M. Pharmacological control of pain during propofol injection: a systematic review and meta-analysis. Expert Rev Clin Pharmacol. 2021;14(7):889–899. doi:10.1080/17512433.2021.1919084
25. Teng Y, Ou M, Wang X, et al. Efficacy and safety of ciprofol for the sedation/anesthesia in patients undergoing colonoscopy: phase IIa and IIb multi-center clinical trials. Eur J Pharm Sci. 2021;164:105904. doi:10.1016/j.ejps.2021.105904
26. Luo Z, Tu H, Zhang X, et al. Efficacy and safety of HSK3486 for anesthesia/sedation in patients undergoing fiberoptic bronchoscopy: a multicenter, double-blind, propofol-controlled, randomized, phase 3 study. CNS Drugs. 2022;36(3):301–313. doi:10.1007/s40263-021-00890-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Ciprofol for Sedation/Anesthesia in Patients Undergoing Hysteroscopy: A Randomized, Parallel-Group, Controlled Trial
Lan H, Shan W, Wu Y, Xu Q, Dong X, Mei P, Duan G, You M, Jin L, Wu J
Drug Design, Development and Therapy 2023, 17:1707-1717
Published Date: 11 June 2023
Bispectral Index-Monitored Anesthesia Induction in Older Adults Undergoing Elective Surgery: Comparing Ciprofol and Propofol in a Prospective, Single-Center, Double-Blind, Randomized Controlled Study
Zou H, Xi F, Fu Y, Xu J, Zhang P, Li D, Luo H
Drug Design, Development and Therapy 2024, 18:4993-5003
Published Date: 5 November 2024
Determination of the Median Effective Dose (ED50) of Ciprofol for Successful Sedation in Pediatric Patients During General Anesthesia Induction
Nie P, Wu D, Du C, Wang X, Zhang H, Xiao H
Drug Design, Development and Therapy 2025, 19:6391-6397
Published Date: 28 July 2025
Induction with Ciprofol Decreases Propofol Requirement During Propofol-Remifentanil Total Intravenous Anesthesia Maintenance in Elderly Patients Undergoing Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Trial
Chen X, Lai Y, Shen Y, Gao S, Huang X, Yang L, Xiong W
Drug Design, Development and Therapy 2026, 20:584998
Published Date: 27 March 2026
Comparison of the Efficacy of Ciprofol and Propofol for Rapid Sequence Induction and Intubation in Elective Non-Cardiac Surgery: A Prospective, Randomized, Non-Inferiority Trial
Lin Y, Wu J, Wang C, Wu J, Liu J, Liu M, Miao C, Liang C
Drug Design, Development and Therapy 2026, 20:614980
Published Date: 8 July 2026