Back to Journals » Journal of Inflammation Research » Volume 17
Independent Association Between Malnutrition Inflammation Score and C Reactive Protein/Albumin Ratio in Hemodialysis Patients
Received 5 July 2024
Accepted for publication 17 November 2024
Published 22 November 2024 Volume 2024:17 Pages 9325—9333
DOI https://doi.org/10.2147/JIR.S477307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Kağan Tur,1 Aydın Güçlü2
1Ahi Evran University Faculty of Medicine, Internal Medicine Department, Kirsehir, Turkey; 2Ahi Evran University Faculty of Medicine, Nephrology Department, Kirsehir, Turkey
Correspondence: Kağan Tur, Ahi Evran University Faculty of Medicine, Internal Medicine Department, Kirsehir, Turkey, Tel +90 5057733927, Email [email protected]; [email protected]
Introduction: This study aimed to investigate the relationship between the Malnutrition Inflammation Score (MIS) and the C-reactive protein/albumin ratio (CAR) in patients undergoing hemodialysis (HD).
Materials and Methods: Sixty-six End-Stage Renal Disease (ESRD) patients on maintenance hemodialysis were recruited for the study. Malnutrition Inflammation Score, biochemical parameters, and C-reactive protein/albumin ratio were analyzed.
Results: The mean age of the participants was 56.47 ± 17.3 years. A statistically significant positive correlation was found between the CRP/albumin ratio and MIS ≥ 7 (r = 0.413, p = 0.026), CRP and MIS ≥ 7 (r = 0.388, p = 0.038) and a negative correlation between albumin and MIS (r = − 0.511, p = 0.005). Additionally, MIS was negatively correlated with hemoglobin (r = − 0.412, p = 0.026) and creatinine (r = − 0.568, p = 0.001), while a positive correlation was found between MIS and ferritin (r = 0.584, p = 0.001) for MIS ≥ 7. A multiple regression ANOVA model confirmed a significant association between CAR, CRP, albumin, and MIS (F = 6.432, p = 0.002), with significant contributions from CAR (p = 0.003), albumin (p = 0.008), and CRP (p = 0.003).
Conclusion: Our study is the first to show an independent association between CAR and MIS in hemodialysis patients. The CRP/albumin ratio can serve as a valuable indicator of malnutrition in this population, providing a reliable tool for assessing nutritional status.
Keywords: malnutrition inflammation score, malnutrition, CRP/albumin ratio, hemodialysis
Introduction
Patients with end-stage renal disease (ESRD) who receive hemodialysis (HD) therapy often have a chronic inflammatory condition.1 For patients undergoing HD, malnutrition is a prevalent issue with a prevalence that ranges from 28 to 54% worldwide.2 In this patient group, malnutrition and inflammation are coexisting, clinically serious illnesses. We looked at the relationship between Malnutrition Inflammation Score (MIS) and the inflammatory markers C-reactive protein/albumin ratio (CAR), albumin, and CRP in hemodialysis patients in this study.
The Malnutrition Inflammation Score is widely recognized as a comprehensive tool for assessing malnutrition and inflammation in hemodialysis patients. It combines multiple components, including biochemical markers, physical assessments, and subjective indicators, to predict adverse outcomes such as hospitalization and mortality. MIS has gained clinical importance because malnutrition and inflammation are common and interrelated issues in ESRD patients on hemodialysis, where both conditions contribute to poor patient prognosis.
Studies have consistently shown that higher MIS values are associated with increased mortality and hospitalization rates. For instance, Borges et al demonstrated that an MIS score greater than 7 predicted higher mortality in hemodialysis patients, making this threshold clinically significant.3 Furthermore, Bandeira et al found that patients with an MIS >9 had significantly lower survival rates compared to those with MIS ≤9, reinforcing its predictive value for negative clinical outcomes.4
Moreover, Jagadeswaran et al reported that patients with MIS ≥7 had elevated levels of inflammatory markers such as IL-6 and hsCRP, which further underscores the score’s utility in identifying patients at risk of malnutrition-inflammation complex syndrome and its associated complications.5 The prognostic significance of MIS was also confirmed in a large cohort study by Prelevic et al, where the score was a strong independent predictor of 4-year mortality in hemodialysis patients.6
Given these findings, the MIS is a valuable tool for assessing both malnutrition and inflammation in hemodialysis patients, enabling clinicians to better predict clinical outcomes and adjust treatment plans accordingly. Through cytokine-induced low appetite, endotoxin and reactive oxygen species (ROS) generation, and metabolic disturbances that result in malnutrition and protein energy wasting (PEW), systemic inflammation may deteriorate a patient’s nutritional condition.7 PEW and inflammation are both associated with disease severity and mortality at patients receiving HD.8 Seemingly intertwined relationship between malnutrition and inflammation at ESRD has led to the naming of malnutrition inflammatory complex syndrome at literature.9 However, further evidence needed in regard to association between inflammation and malnutrition in patients receiving HD.
Malnutrition Inflammation Score is an important nutritional assessment tool for chronic kidney disease (CKD). Anthropometric measurements, biochemical information, such as albumin and serum total iron-binding capacity (TIBC), and Subjective Global Assessment (SGA) components are all included in MIS.
C reactive protein (CRP) is an acute-phase protein with an impact on inflammatory processes, and albumin is an essential plasma protein with anti-inflammatory properties. A unique inflammatory measure known as the C reactive protein/albumin ratio has been linked to a number of diseases, including sepsis, nasopharyngeal carcinoma, and non-small cell lung cancer.10–12
Materials and Methods
The study was carried out at the Kirsehir Hemodialysis Unit of Ahi Evran University Faculty of Medicine in Turkey. The trial has enrolled 66 ESRD patients who have been receiving maintenance hemodialysis three times per week for at least three months. Hemodialysis patients were selected for this study due to their increased risk of malnutrition and inflammation, which are key contributors to adverse outcomes in End-Stage Renal Disease. Hemodialysis patients are known to frequently experience protein-energy wasting and chronic inflammation, making them an ideal population for studying the association between the C-reactive protein/albumin ratio and the Malnutrition Inflammation Score. CRP and albumin were chosen as primary inflammatory markers due to their widespread clinical availability and their established use in assessing inflammation and malnutrition in hemodialysis patients. While markers such as Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-α) are important indicators of inflammation, CRP and albumin are more practical for routine clinical use. Future studies may incorporate these additional markers to offer a more comprehensive evaluation. While normal controls were not included in this study, future research could benefit from comparing hemodialysis patients to non-dialysis controls. Such comparisons would provide valuable insights into the differential effects of dialysis on malnutrition and inflammation, particularly regarding the associations between CAR and MIS. All patients were undergoing regular bicarbonate dialysate-based 4-hour hemodialysis. All subjects provided their informed permission. The research did not include patients with active infections, connective tissue illnesses, sepsis, hepatic insufficiency, or other inflammatory conditions. The Ethics Committee has accepted the study (Decision Number 2020–19/145). The actions conducted adhered to the principles of the Helsinki Declaration. All participants completed an informed consent form that was approved by the Ahi Evran University Faculty of Medicine. Before the HD session began, all serum blood samples were collected, and standard protocols were used to analyze the samples. We took anthropometric measures before the HD session. Body weight (kg)/body height squared (m2) was used to compute the body mass index (BMI). In this study, all patients were treated using standard bicarbonate-based hemodialysis with high-flux dialyzers (HiF 16). Preservation of residual renal function (RRF) was not specifically measured, but patients with significant RRF were excluded from the study to ensure a more homogenous patient population. The choice of dialyzer and dialysis modality can influence patient outcomes, particularly with respect to inflammation and malnutrition, as these factors impact the clearance of toxins and inflammatory cytokines. Future studies should consider the role of RRF and specific dialysis modalities more explicitly.
Based on Kalantar Zadeh et al, the parameters for the malnutrition inflammation score were calculated.13 The MIS is based on ten components; change in end-dialysis dry weight in past 3–6 months; dietary intake; gastrointestinal symptoms including appetite; functional capacity and nutritionally related functional impairment evaluation; comorbid diseases including number of years on dialysis; physical examination according to SGA criteria including; assessment of patient’s loss of muscle mass (temple, clavicle, scapula, ribs, quadriceps, knee, interosseous) assessment of loss of fat stores or subcutaneous fat (below eyes, triceps, biceps, chest); BMI; laboratory parameters including measurement of serum albumin; and measurement of serum total iron-binding capacity. Each component is assessed using one of the four severity categories, ranging from 0 (normal) to 3 (very severe) and the sum of these ratings provides the overall MIS. Malnutrition is described by the MIS 7.3 The Malnutrition Inflammation Score (MIS) ranges from 0 to 30, with higher scores indicating more severe malnutrition and inflammation.
Statistical Analysis
The mean and standard deviation of numerical data with a normally distributed distribution are employed to describe the data. Appropriate statistical tests are then performed to determine the relationships between the variables; for nonparametric variables, the Spearman Correlation Test was used, and for continuous variables, Pearson’s Correlations Test. The chi-square test was used to assess categorical data. In order to determine a reasonable cutoff value for MIS, the area under the curve (AUC) was calculated using the receiver operating characteristic (ROC) curve. Prior to multivariate analysis, standardized skewness and Shapiro–Wilk tests are employed for normality checks. According to the created linear model, multivariate ANOVA regression analysis was utilized to examine the independent impacts of stated factors on MIS. Utilizing SPSS for Windows (version 25.0; SPSS Inc., USA) for all statistical analyses. Statistical significance was defined as a P-value 0.05.
Results
Mean age of the participants was 56.47 ± 17.3. About 42% of the patients were male. About 50% of the patients had malnutrition. About 34% of the study group had heart failure, 33% had hypertension, 17% had diabetes mellitus and 24% had coronary artery disease. Causes of hemodialysis were as follows; 33% hypertension, 17% diabetes mellitus, 15% obstructive nephropathy, 11% polycystic kidney disease, 2% glomerulonephritis, and 22% unknown causes. Descriptive characteristics of the patients have been shown at Table 1.
 |
Table 1 Descriptive Characteristics of the Study Group (N = 66) |
CAR and MIS showed a statistically significant positive connection (r = 0.413, p = 0.026), as did CRP and MIS (r = 0.388, p = 0.038), but albumin and MIS showed a statistically significant negative correlation (r = −0.511, p = 0.005). For MIS, there was a negative correlation between MIS and hemoglobin (r = −0.412, p = 0.026). For MIS, there was a positive connection with ferritin (r = 0.584, p = 0.001) and a negative correlation with creatinine (r = −0.568, p = 0.001). All of these relationships are shown in Table 2. The mean CAR value in our study was 4.21 ± 9, and it was found to be positively correlated with the Malnutrition Inflammation Score. Although there is no universally established threshold for CAR to definitively indicate malnutrition, higher CAR values have been associated with increased inflammation and poorer nutritional status in various studies. For instance, Sant’ana et al demonstrated that higher CAR values were significantly associated with higher mortality in hemodialysis patients during the first six months of treatment, highlighting its prognostic importance in this population.14 Similarly, Jeon et al found that CAR was a significant predictor of in-hospital mortality in patients, with acute kidney injury undergoing renal replacement therapy, further supporting its role as a marker of malnutrition and inflammation.15
 |
Table 2 Correlations Between Malnutrition Inflammation Score, CRP/Albumin Ratio and Biochemistry Parameters |
For testing the normality, standardized skewness and Shapiro–Wilk test indicated that data were statistically normal. For MIS, CAR, albumin and CRP, a multiple regression ANOVA model was conducted to examine that relation of CAR, CRP, and albumin on MIS (F = 6.432, p = 0.002). ANOVA revealed that there was a statistically significant relation between dependent and independent groups (for CRP p = 0.003, for albumin p = 0.008, for CAR p = 0.003). Model summary shown at Table 3, ANOVA results of the model and coefficients of the model are shown at Table 4 and Table 5, respectively.
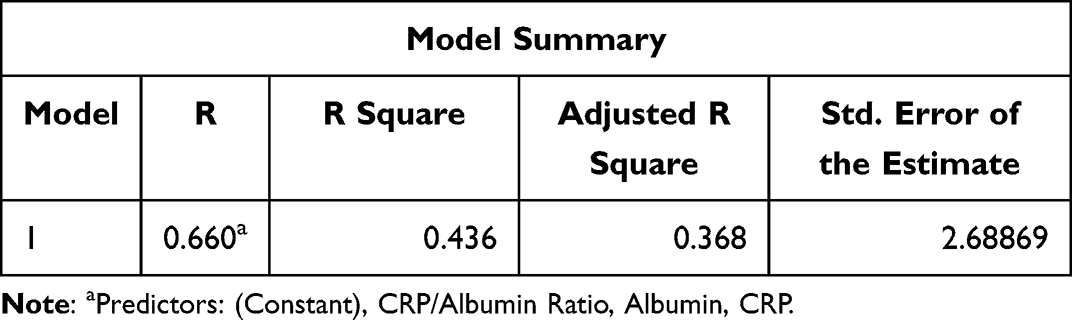 |
Table 3 Model Summary |
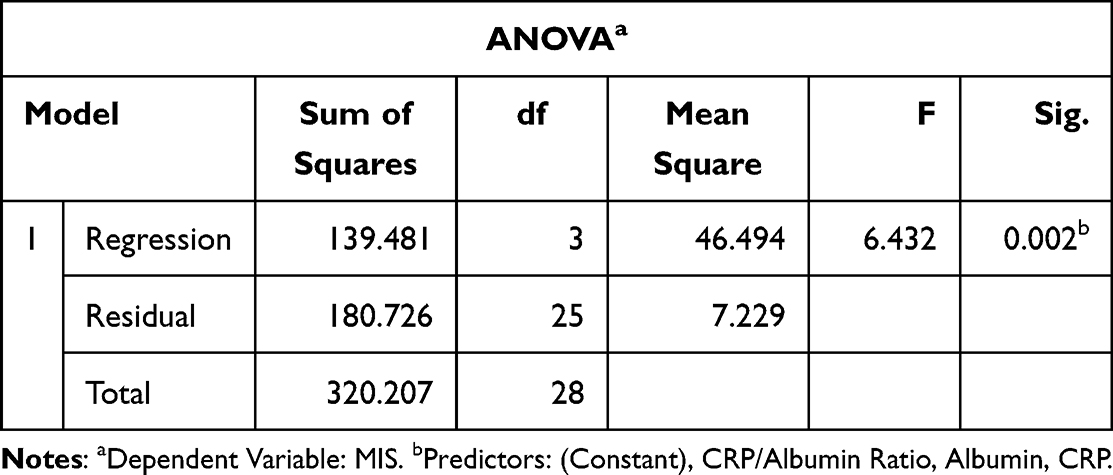 |
Table 4 ANOVA Results of the Model |
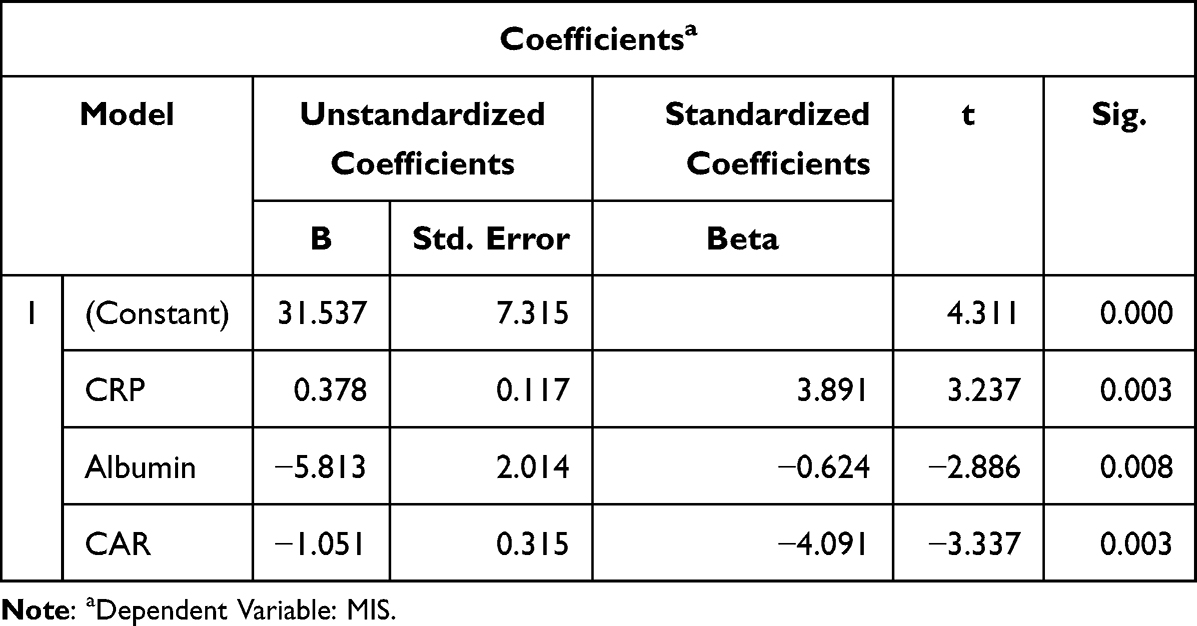 |
Table 5 Coefficients of the Model, CAR (CRP/Albumin Ratio) |
Discussion
While a cut-off point of 5 is commonly used in studies assessing malnutrition in various populations, we chose a cut-off point of 7 for the Malnutrition Inflammation Score based on prior research specifically in hemodialysis patients. Borges et al found that an MIS cut-off of greater than 7 predicted higher mortality rates in patients undergoing long-term hemodialysis, making it a clinically significant threshold for this population.3 Similarly, Jagadeswaran et al observed that patients with MIS ≥7 had elevated inflammatory markers such as IL-6 and hsCRP, further validating this cut-off in clinical settings.5 Given these findings, we believe that an MIS cut-off of 7 is more appropriate for identifying severe malnutrition and inflammation in patients undergoing hemodialysis. In the current investigation, we discovered a statistically significant association between CAR, CRP, albumin, and MIS (r = 0.413, p = 0.026, r = 0.388, p = 0.038, and r = −0.511, p = 0.005, respectively). According to an ANOVA, there is an independent connection between MIS, CRP, albumin, and CAR that is statistically significant (for CRP, p = 0.003, for albumin, p = 0.008, and for CAR, p = 0.003). In patients receiving HD, lower albumin values, higher CRP and CAR values were revealed to be strong indications of malnutrition.
Several methods are commonly used to assess nutritional status in clinical settings, including the Subjective Global Assessment, biochemical markers (eg, serum albumin, prealbumin), and body mass index. The SGA is widely used for its holistic approach, combining clinical judgment with anthropometric measurements, but it is subjective and may vary between assessors. Studies have demonstrated its effectiveness, showing significant correlations between SGA and markers such as BMI, serum albumin, and CRP in hemodialysis patients.16 Additionally, the modified SGA has been validated against anthropometric measures like mid-arm circumference and serum albumin, further confirming its clinical utility.17
Biochemical markers such as serum albumin and prealbumin are often used to indicate malnutrition, though these markers can be influenced by factors such as inflammation and fluid status, making them less reliable in isolation. For example, Dragović et al emphasized the limitations of relying solely on serum albumin due to its susceptibility to being affected by inflammation and hydration levels.18 Similarly, prealbumin has been shown to correlate with other nutritional markers, like BMI and serum albumin, but its reliability can be reduced in the presence of inflammation.19
In contrast, the C-reactive protein/albumin ratio offers a more integrative measure of both inflammation and nutritional status. Since inflammation plays a significant role in malnutrition among hemodialysis patients, CAR serves as a more dynamic marker by reflecting both inflammatory processes and protein-energy wasting. Studies such as those by Yang et al have demonstrated that CAR outperforms other markers, including albumin, in predicting systemic inflammation and associated complications.20 Furthermore, Rodrigues et al found that measures such as SGA and MIS were strong predictors of hospitalization and mortality, with SGA showing the strongest association with clinical outcomes.21 However, CAR provides a practical and reliable alternative or supplement to these traditional methods of nutritional assessment, particularly in early detection of malnutrition.
Our study highlights CAR’s potential as a practical and reliable tool to supplement or even improve traditional methods of nutritional assessment in this patient population. Future studies could further validate CAR’s role alongside existing methods such as SGA, particularly in the early detection of malnutrition and its associated risks. Malnutrition is an important phenomenon in patients receiving HD which is responsible for adverse outcomes. Quality of life impairment, infection risk, progressive loss of body muscle and fat mass and mortality are associated with malnutrition.2,7,22 The etiology of malnutrition in ESRD is multifactorial, comprised by declining appetite, impairment of glucose and amino acid transport and metabolism, low diet quality, uremia, cytokine production, comorbidities and the dialysis procedure itself.7
Low-grade chronic systemic inflammation in which patients with CKD are characterized by, is also a potential contributor to malnutrition development and progression. In patients receiving HD, the development of inflammation is caused by various factors, including oxidative stress, uremic milieu, increased cytokine production and decrease in clearance of cytokines, dialysis procedure and infection frequency.8,23 The coexistence of malnutrition and inflammation suggests the potential relationship between these two aspects of ESRD. However the precise role of inflammation in the physiopathology of malnutrition and PEW is not totally elucidated.24 There are several hypotheses regarding the role of inflammation at malnutrition development in ESRD. Cytokine production affects the regulation of appetite resulting anorexia.25 Inflammation may enhance insulin resistance and impair glucose and amino acid transport metabolism.7 Resting energy expenditure is reported to be raised because of inflammatory status, contributing to muscle mass loss.24 Anabolic hormone resistance caused by inflammation also prompts catabolism.26
There are studies27–29 on the interaction between SGA and inflammatory markers such CRP, adiponectin, and IL-6 in HD patients, but there are not many on the connection between MIS and CAR. The first research in the body of the literature to show an independent connection between CAR and MIS in HD patients is ours.
Association between CRP, albumin and MIS in CKD has been reported by number of studies. Aggarwal et al have found an association between MIS and inflammatory markers CRP and albumin, negative correlation for albumin (p < 0.01) and positive correlation for CRP (p < 0.01) in CKD stage 3 to 5.30 In a study conducted on patients with pre-dialysis CKD, it has been reported that patients with MIS ≥7 had significant increase in Hs-CRP levels (p < 0.001), albumin was negative correlated with MIS in the same research.5
Ashabi et al observed that albumin and MIS had a negative connection (p0.01) and a positive correlation (p0.01) when taking into account research on the HD group.31 Another study32 found that CRP level (=3.33, P 0.001) and albumin level (=1.95, P = 0.008) were independently associated with MIS in patients receiving HD. Martins et al33 discovered an independent relationship between higher CRP and a higher probability of MIS >5 (OR 1.01 p 0.001). Another study revealed similar findings, showing a relationship between CRP levels and MIS (B = −0.56; P = 0.0001).34 In our study, we found that CRP and CAR are positive correlated and albumin is negative correlated with MIS in patients receiving HD.
Literature also comprises conflicting results regarding relation of MIS, CRP and albumin in patients receiving HD. Pisetkul et al did not found a correlation between hs-CRP and MIS at patients receiving hemodialysis (r = 0.08, p 0.44).35 Different study has reported that albumin was not significantly correlated statistically with MIS in patients receiving HD (−0.189 p = 0.345).36 In the research of Ekremzadeh et al, albumin was not statistically significant between two MIS groups ≥10 and <10, in patients receiving HD.27 Another study conducted in patients receiving HD has found that while albumin level was lower when MIS ≥8 (p < 0.001), CRP levels did not differ between two MIS groups.37
CAR is a novel inflammation index that has been emerged in recent years and it has been reported recently that it can better reflect the inflammation status compared to other markers.38 In the current study, multiregression analysis showed that CRP, CAR, and albumin were independently associated with MIS. Our research demonstrates statistically significant independent positive correlation between CAR and MIS, CRP and MIS and negative correlation between MIS and albumin. Interesting feature of our study is that this is the first time in the literature that shows a strong relation between CAR and MIS in HD patients. Our findings indicate that CAR can be a reliable and practical measurement for assessing the nutritional status of patients receiving HD.
Precise nutritional status assessment and to be able to detect PEW before related complications emerge are two crucial aims for the management of malnutrition in patients receiving maintenance HD. CAR can be used as valuable tool for predicting and screening of PEW and malnutrition risk in patients receiving HD.
Conclusion
In conclusion, our study demonstrates a significant independent association between the C-reactive protein/albumin ratio and the Malnutrition Inflammation Score in patients undergoing hemodialysis. The findings highlight that a cut-off point of 7 for the MIS is clinically relevant in this population, aligning with previous research that has shown it to be a strong predictor of malnutrition and inflammation in hemodialysis patients. This cut-off point enables more precise identification of patients at higher risk of malnutrition-related complications.
Moreover, the role of the dialysis scheme and the specific dialyzer used may also impact these outcomes. Although this study did not directly measure the preservation of residual renal function or the effect of different dialyzers, future studies should explore how these factors influence nutritional and inflammatory markers, such as CAR and MIS. Understanding the interplay between dialysis modalities and nutritional status could lead to improved patient management strategies and better clinical outcomes. Precise nutritional status assessment and to be able to detect PEW before related complications emerge are two crucial aims for the management of malnutrition in patients receiving maintenance HD. CAR can be used as valuable tool for predicting and screening of PEW and malnutrition risk in patients receiving HD.
A key limitation of our study is the relatively small sample size (n = 66), which may limit the generalizability of our findings. Additionally, the mean age of the participants (56.47 ± 17.3 years) may reduce the ability to establish strong correlations with age-related variations in nutritional and inflammatory status. While the sample size was sufficient for initial exploratory analysis, future studies with larger and more diverse populations would help to validate and expand upon these findings. Moreover, the lack of stratification by age groups in this study may have masked any potential age-specific associations with MIS and inflammatory markers. Future research should aim to include a broader age range and larger sample size to further investigate these correlations. In the current study, we looked at how the inflammatory biomarkers CAR, CRP, albumin, and MIS related to patients undergoing HD. Interesting feature of our research is that our study showed first time in the literature that CAR is independently associated with MIS in patients receiving HD treatment. Although this study did not categorize the CAR into mild, moderate, or severe categories, future studies could explore such classifications to better understand how CAR correlates with different levels of malnutrition and inflammation. This could provide more granular insights into the severity of malnutrition and its clinical implications in hemodialysis patients.
In the current study, we looked at how the inflammatory biomarkers CAR, CRP, albumin, and MIS related to patients undergoing HD. Interesting feature of our research is that our study showed first time in the literature that CAR is independently associated with MIS in patients receiving HD treatment.
Data Sharing Statement
The datasets analyzed and used in this study are available via corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Study has been approved from Ahi Evran University Faculty of Medicine Research Ethics Committee (Decision Number 2020-19/145). The procedures followed were in accordance with the Declaration of Helsinki. All participants signed an informed consent form approved by the Ahi Evran University Faculty of Medicine.
Consent for Publication
Consent to publish was obtained from the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declared that they have no conflicts of interest in this work. We declare that we do not have any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
References
1. Cobo G, Lindholm B, Stenvinkel P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol Dial Transplant. 2018;Vol. 33(suppl_3):iii35–iii40. PMID: 30281126; PMCID: PMC6168801. doi:10.1093/ndt/gfy175
2. Carrero JJ, Thomas F, Nagy K, et al. Global prevalence of protein-energy wasting in kidney disease: a meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism. J Ren Nutr. 2018;28:380–392. doi:10.1053/j.jrn.2018.08.006
3. Borges MC, Vogt BP, Martin LC, Caramori JC. Malnutrition inflammation score cut-off predicting mortality in maintenance hemodialysis patients. Clin Nutr ESPEN. 2017;17:63–67. PMID: 28361749. doi:10.1016/j.clnesp.2016.10.006
4. Bandeira SB, Cansanção K, Paula TP, Peres W. Evaluation of the prognostic significance of the malnutrition inflammation score in hemodialysis patients. Clin Nutr ESPEN. 2020;35:109–115. doi:10.1016/j.clnesp.2019.10.019
5. Jagadeswaran D, Indhumathi E, Hemamalini AJ, Sivakumar V, Soundararajan P. Inflammation and nutritional status assessment by malnutrition inflammation score and its outcome in pre-dialysis chronic kidney disease patients. Clin Nutr. 2019;38(1):341–347. doi:10.1016/j.clnu.2018.01.001
6. Prelevic V, Antunovic T, Radunovic D, Gligorovic-Barhanovic N, Gledovic B, Ratkovic M. Malnutrition inflammation score is a predictor of mortality in hemodialysis patients. Int Urol Nephrol. 2021;1–6.
7. Sahathevan S, Khor B-H, Ng H-M, et al. Understanding development of malnutrition in hemodialysis patients: a narrative review. Nutrients. 2020;12(10):3147. doi:10.3390/nu12103147
8. Nowak KL, Chonchol M. Does inflammation affect outcomes in dialysis patients? Semin Dial. 2018;31(4):388–397. doi:10.1111/sdi.12686
9. Kalantar-Zadeh K, Ikizler TA, Block G, et al. Malnutrition-inflammation complex syndrome in dialysis patients: causes and consequences. Am J Kidney Dis. 2003;42(5):864–881. doi:10.1016/j.ajkd.2003.07.016
10. Gao N, Yang RN, Meng Z, Wang WH. The prognostic value of C-reactive protein/albumin ratio in nasopharyngeal carcinoma: a meta-analysis. Biosci Rep. 2018;38(6):BSR20180686. PMID: 30352836; PMCID: PMC6239271. doi:10.1042/BSR20180686
11. Ni XF, Wu J, Ji M, et al. Effect of C-reactive protein/albumin ratio on prognosis in advanced non-small-cell lung cancer. Asia Pac J Clin Oncol. 2018;14(6):402–409. PMID: 30178541. doi:10.1111/ajco.13055
12. Ranzani OT, Zampieri FG, Forte DN, et al. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One. 2013;8(3):e59321. doi:10.1371/journal.pone.0059321
13. Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2001;38(6):1251–1263. doi:10.1053/ajkd.2001.29222
14. Sant’Ana M, Gameiro J, Costa C, et al. C-reactive protein-to-albumin ratio and six-month mortality in incident hemodialysis patients. Renal Failure. 2023;45(1):2182615. doi:10.1080/0886022X.2023.2182615
15. Jeon YH, Lee SW, Jeon Y, et al. The impact of C-reactive protein-to-albumin ratio on mortality in patients with acute kidney injury requiring continuous renal replacement therapy: a multicenter retrospective study. Nephron. 2024;148(6):379–389. doi:10.1159/000534970
16. Kamal MO, Elbakary MM, Manal S, Gawaly AM. Subjective global assessment for nutritional assessment of patients on regular hemodialysis at dialysis unit at Tanta University Hospital. Med J Cairo Univ. 2019;87(September):3023–3029. doi:10.21608/mjcu.2019.59355
17. Peng H, Aoieong C, Tou T, Tsai T, Wu J. Clinical assessment of nutritional status using the modified quantified subjective global assessment and anthropometric and biochemical parameters in patients undergoing hemodialysis in Macao. J Int Med Res. 2021;49(9):03000605211045517. doi:10.1177/03000605211045517
18. Dragović T, Mijušković MM, Terzić B, Medić DR, Hajduković Z, Rađen S. Serum C-reactive protein and nutritional parameters in hemodialysis patients. Vojnosanit Pregl. 2019;76(7):723–727. doi:10.2298/VSP160912155D
19. Rahman MS, Sultana T, Sultana T, Alam SAU, Ershad SM, Hossain S. Association of serum prealbumin with nutritional status of end-stage renal disease patients under maintenance hemodialysis. J Prev Soc Med. 2021;40(2):9–15. doi:10.3329/jopsom.v40i2.61791
20. Yang WM, Zhang WH, Ying HQ, et al. Two new inflammatory markers associated with disease activity score-28 in patients with rheumatoid arthritis: albumin to fibrinogen ratio and C-reactive protein to albumin ratio. Int Immunopharmacol. 2018;62:293–298. doi:10.1016/j.intimp.2018.07.007
21. Rodrigues J, Santin F, Brito FDSB, Lindholm B, Stenvinkel P, Avesani CM. Nutritional status of older patients on hemodialysis: which nutritional markers can best predict clinical outcomes? Nutrition. 2019;65:113–119. doi:10.1016/j.nut.2019.03.002
22. Nagy E, Mahmoud M, El‐kannishy G, Sayed‐Ahmed N. Impact of malnutrition on health‐related quality of life in patients on maintenance hemodialysis. Therapeutic Apheresis Dialysis. 2021;25(4):467–474. doi:10.1111/1744-9987.13588
23. Mihai S, Codrici E, Popescu ID, et al. Inflammation-related mechanisms in chronic kidney disease prediction, progression, and outcome. J Immunol Res. 2018;2018:2180373. PMID: 30271792; PMCID: PMC6146775. doi:10.1155/2018/2180373
24. Jankowska M, Cobo G, Lindholm B, Stenvinkel P. Inflammation and protein-energy wasting in the uremic milieu. Contrib Nephrol. 2017;191:58–71. PMID: 28910791. doi:10.1159/000479256
25. Carrero JJ, Qureshi AR, Axelsson J, et al. Comparison of nutritional and inflammatory markers in dialysis patients with reduced appetite. Am J Clin Nutr. 2007;85(3):695–701. PMID: 17344489. doi:10.1093/ajcn/85.3.695
26. Stenvinkel P. Can treating persistent inflammation limit protein energy wasting? Semin Dial. 2013;26(1):16–19. PMID: 23043540. doi:10.1111/sdi.12020
27. Ekramzadeh M, Sohrabi Z, Salehi M, et al. Adiponectin as a novel indicator of malnutrition and inflammation in hemodialysis patients. Iran J Kidney Dis. 2013;7(4):304–308. PMID: 23880808.
28. Essadik R, Msaad R, Lebrazi H, et al. Assessing the prevalence of protein-energy wasting in haemodialysis patients: a cross-sectional monocentric study. Nephrol Ther. 2017;13(7):537–543. PMID: 29113907. doi:10.1016/j.nephro.2017.02.013
29. Carrero JJ, Chmielewski M, Axelsson J, et al. Muscle atrophy, inflammation and clinical outcome in incident and prevalent dialysis patients. Clin Nutr. 2008;27(4):557–564. PMID: 18538898. doi:10.1016/j.clnu.2008.04.007
30. Aggarwal HK, Jain D, Chauda R, Bhatia S, Sehgal R. Assessment of malnutrition inflammation score in different stages of chronic kidney disease. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2018;39(2–3):51–61. PMID: 30864357. doi:10.2478/prilozi-2018-0042
31. As’habi A, Tabibi H, Hedayati M, Mahdavi-Mazdeh M, Nozary-Heshmati B. Association of malnutrition-inflammation score, dialysis-malnutrition score and serum albumin with novel risk factors for cardiovascular diseases in hemodialysis patients. Ren Fail. 2015;37(1):113–116. PMID: 25296104. doi:10.3109/0886022X.2014.967615
32. Ko YT, Lin YL, Kuo CH, Lai YH, Wang CH, Hsu BG. Low serum leptin levels are associated with malnutrition status according to malnutrition-inflammation score in patients undergoing chronic hemodialysis. Hemodial Int. 2020;24(2):221–227. PMID: 31804777. doi:10.1111/hdi.12806
33. Martins VS, Aguiar L, Dias C, et al. Predictors of nutritional and inflammation risk in hemodialysis patients. Clin Nutr. 2020;39(6):1878–1884. doi:10.1016/j.clnu.2019.07.029
34. Chen J, Peng H, Xiao L, et al. Inflammation but not dietary macronutrients insufficiency associated with the malnutrition-inflammation score in hemodialysis population. PLoS One. 2013;8(12):e83233. doi:10.1371/journal.pone.0083233
35. Pisetkul C, Chanchairujira K, Chotipanvittayakul N, Ong-Ajyooth L, Chanchairujira T. Malnutrition-inflammation score associated with atherosclerosis, inflammation and short-term outcome in hemodialysis patients. J Med Assoc Thai. 2010;93(Suppl 1):S147–56. PMID: 20364569.
36. de Almeida HRM, Santos EMC, Dourado K, et al. Malnutrition associated with inflammation in the chronic renal patient on hemodialysis. Rev Assoc Med Bras. 2018;64:837–844. doi:10.1590/1806-9282.64.09.837
37. Katalinic L, Premuzic V, Basic-Jukic N, Barisic I, Jelakovic B. Hypoproteinemia as a factor in assessing malnutrition and predicting survival on hemodialysis. J Artif Organs. 2019;22(3):230–236. PMID: 30852693. doi:10.1007/s10047-019-01098-3
38. Park JE, Chung KS, Song JH, et al. The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients. J Clin Med. 2018;7(10):333. doi:10.3390/jcm7100333
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Does Control Nutritional Status (CONUT) Score Predict Early and Long-Term Mortality at the Initiation of Maintenance Hemodialysis?
Selen T, Ulusal Okyay G, Ayerden Ebinç F, Merhametsiz Ö, Şahin H, Aylı MD
International Journal of General Medicine 2025, 18:3775-3786
Published Date: 7 July 2025