Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Increased Stress Hyperglycemia Ratio Predicts Poor Clinical Outcome in Critically Ill COPD Patients: A Retrospective Study
Authors Qiao M ![]() , Yang H, Qin M, Li Y, Wang H
, Yang H, Qin M, Li Y, Wang H
Received 2 February 2025
Accepted for publication 9 April 2025
Published 24 April 2025 Volume 2025:20 Pages 1203—1215
DOI https://doi.org/10.2147/COPD.S520418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Mengyuan Qiao,1,* Hui Yang,2,* Mengzhen Qin,2 Yingyang Li,3 Haiyan Wang2
1School of Nursing, Henan University of Science and Technology, Luoyang, 471023, People’s Republic of China; 2People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, People’s Republic of China; 3The First Affiliated Hospital of Henan University of Science and Technology, Luoyang, 471003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyan Wang, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, People’s Republic of China, Email [email protected]
Objective: Stress hyperglycemia ratio (SHR) was introduced as an indicator of relative hyperglycaemia and is widely used for prognostic prediction in critically ill patients. The present study aimed to investigate the relationship between SHR and adverse clinical outcomes in critically ill COPD patients.
Methods: A total of 1,580 patients diagnosed with COPD were included in this retrospective cohort study. SHR = ABG (mmol/L) / [1.59 × HbA1c (%) - 2.59]. Primary endpoints included ICU mortality and in-hospital mortality. Secondary endpoints were acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and acute respiratory failure (ARF). Logistic regression, Restricted Cubic Sample (RCS) and Receiver Operating Characteristic (ROC) were used to explore the relationship between SHR and prognosis of COPD patients. In addition, subgroup analyses and interaction tests were performed to investigate potential heterogeneity.
Results: Multivariate logistic regression analysis showed that elevated SHR was not associated with ICU mortality and in-hospital mortality. In contrast, SHR quartiles were correlated with ICU mortality and in-hospital mortality. Restricted cubic spline regression models showed a nonlinear correlation between SHR and both ICU mortality and in-hospital mortality (all P< 0.001). In addition, a linear correlation was found between SHR and AECOPD and ARF, with elevated SHR associated with increased risk of AECOPD and ARF. ROC analyses showed that SHR was a more effective predictor of mortality and prognosis than admission blood glucose (ABG) and hemoglobin A1c (HbA1c) in patients with COPD, with the former being a better predictor of mortality and prognosis. In subgroup analyses, after adjusting for all covariates considered in the present study, the relationship between SHR and prognostic risk in patients with COPD remained stable across gender, age, BMI, smoking, drinking, history of hypertension, coronary heart disease, diabetes, and cerebrovascular disease.
Conclusion: SHR is independently associated with an increased risk of adverse clinical outcomes in critically ill COPD patients.
Keywords: stress hyperglycemia ratio, COPD, mortality, AECOPD, ARF
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and irreversible airflow limitation,1 and is a preventable, controllable and treatable chronic respiratory disease. Reports show that the prevalence of COPD in China is 8.6% for those over 20 years of age, 13.7% for those over 40 years of age, and more than 27% for those over 60 years of age, which is higher than the average of the global prevalence rate of the disease reported at 10.3%.2 It is predicted that the prevalence of COPD will continue to rise over the next 40 years and the number of patients will continue to increase.2 Currently, COPD is the third leading cause of death in the world, after ischaemic heart disease and stroke.3 According to the World Health Organization (WHO), about 3 million people currently die of COPD each year.4 It is projected that by 2060, more than 5.4 million people will die annually from COPD and its related diseases.5 COPD has become a respiratory disease that seriously endangers human health, poses a serious burden on economic development and social progress, and is a public health problem that requires urgent attention now and in the future.
Previous studies have found that patients with COPD experience an average of 0.5 to 3.5 acute exacerbation per year, with 22% to 40% of patients experiencing at least one moderate or severe exacerbation per year.6 Repeated and frequent acute exacerbation of COPD (AECOPD) increase morbidity, mortality and deterioration of lung function, especially in the intensive care unit (ICU).7 Under certain conditions, AECOPD can lead to the development of acute respiratory failure and rapid deterioration of the patient’s condition.8 Notably, type II respiratory failure is the complication that leads to high mortality and the highest adverse prognosis in AECOPD patients, and patients with COPD complicated by respiratory failure have an increased risk of readmission after discharge from the hospital.9 For these reasons, the clinical course of patients with COPD may be complicated by the complication of multi-organ dysfunction and high mortality rates.10 Ai-Ping and colleagues found that the mortality rates of patients with AECOPD at 6 months, 1 year and 5 years after admission were 39.0%, 42.7% and 75.9%, respectively.11 Therefore, identifying risk factors and predicting prognosis in patients with AECOPD is essential to guide early intervention.
Stress hyperglycaemia is a common complication in critically ill patients, and a hyperglycaemia environment in the organism exacerbates lung tissue damage and oedema, increases the area of inflammation and reduces the efficacy of pulmonary ventilation therapy, thus affecting the recovery of lung function.12 A retrospective study in the United States found that the prevalence of stress hyperglycaemia among AECOPD patients was 34.1%.13 From a pathophysiological point of view, the activation of the sympathetic nervous system and the hypothalamic - pituitary - adrenal axis results in the release of stress hormones, leading to this elevation.14 Considering that stress hyperglycaemia may be limited by factors such as poor diabetes control and diet, the stress hyperglycaemia ratio (SHR) has been proposed in recent years as a valuable biomarker by calculating blood glucose and haemoglobin A1c levels on admission, while taking into account the patient’s chronic glycaemic status in the previous two to three months adjusted to accurately identify and quantify the extent of stress hyperglycaemia, making more valuable predictions about overall health.15 The relationship between SHR and health outcomes is now a key area of interest in clinical research. Specifically, a large cohort study in China has established a positive correlation between SHR and the risk of in-hospital mortality from coronary artery disease, emphasizing the importance of this metric in predicting clinical outcomes.16 Furthermore, in the United States, higher SHR has been associated with significant predictors of increased all-cause and specific mortality in overweight and obese individuals, underscoring its potential role in assessing risk for a wide range of diseases.17 The relationship between SHR and the central nervous system has also been elucidated, with studies demonstrating a strong association with the risk of delirium,18,19 highlighting the neurological significance of increased glucose metabolism under stress. Given the substantial correlations between SHR and a myriad of disorders, providing valuable insights into the diagnosis and prognostic prediction of a wide range of diseases, its association with the prognosis of critically ill COPD patients has not yet been widely explored, and therefore a definitive review and further research is warranted.
The aim of the present study was to investigate the role of SHR ratio on the prognostic aspects of clinical outcomes in critically ill COPD patients and to analyse its predictive value to provide a theoretical basis for secondary prevention in COPD patients.
Methods
Study Population
A total of 1580 COPD patients who attended the intensive care unit of a tertiary hospital in Urumqi, Xinjiang Uygur Autonomous Region, from January 2018 to December 2023 were retrospectively collected. Diagnosis of COPD was confirmed by a spirometry using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, indicating a non-reversible ventilatory deficit (FEV 1/FVC < 0.70) following bronchodilation, with a reduction in the volume of forceful respiratory volume in one second (FEV 1) and forceful vital capacity (FVC).20 Patients with one of the following conditions were excluded: (a) less than 18 years older; (b) less than 24 hours of hospital stay; (c) patients with recent use of immunosuppressants or corticosteroids; (d) patients with severe psychiatric disorders or chronic alcohol abuse; (e) patients with advanced liver or kidney failure, or severe coagulation disorders; (f) and lack of baseline data for HbA1c or admission glucose levels, or measurements not taken within 24 hours of admission. The flowchart for data filtering can be found in Figure S1. The study was approved by the Ethics Committee of Xinjiang Uygur Autonomous Region People’s Hospital (KY2023071303).
Data Collection and Definitions
Baseline data of the patients were collected from the hospital information management system, including age, gender, body mass index (BMI), smoking, drinking, hypertension, coronary heart disease, diabetes, history of cerebrovascular disease, systolic blood pressure (SBP), diastolic blood pressure (DBP), and mechanical ventilation. The degree of disease severity was assessed by the APACHE II score on admission, which consists of three components: acute physiology score, age score, and chronic health status score, and the final score is the sum of the three, with a theoretical maximum score of 71, and the higher the score, the more severe the condition.21 All patients had fasting venous blood drawn in the early morning of the following day for laboratory tests, including: hemoglobin A1c (HbA1c), the admission blood glucose (ABG), haemoglobin (Hb), creatinine (Cr), albumin (Alb) and C-reactive protein (CRP). The detailed variables were shown in Table 1.
 |
Table 1 Comparison of Clinical Data of Four Groups |
SHR Calculation and Grouping
SHR were calculated based on ABG and HBA1c at the time of the patient’s admission to the ICU. ABG was defined as the first available plasma glucose measurement within one day of admission. Calculation of HbA1c-adjusted glycemic variables HbA1c-adjusted glycemic variables were calculated as follows:22 a. ADAG= 1.59×HbA1c-2.59; b. SHR= ABG (mmol/L) /ADAG. Based on the quartiles of SHR (Q1-Q4), the study participants were divided into four groups: group Q1 (SHR≤0.76), Q2 (0.76<SHR≤0.98), Q3 (0.98<SHR≤1.50), and Q4 (SHR>1.50), with 395 cases in each group.
Definition of AECOPD
AECOPD is defined as an event characterized by increased dyspnea and/or cough and sputum that worsens in ≤14 days, which may be accompanied by tachypnea and/or tachycardia and is often associated with increased local and systemic inflammation caused by infection, pollution, or other insult to the airways.20
Definition of ARF
Acute respiratory failure (ARF) is defined as a decrease in oxygen saturation (<92%) on room air with severe respiratory distress or hypoxaemia (partial pressure of oxygen <60 mm Hg) and/or the need for invasive/non-invasive mechanical ventilation.23
Endpoints
The primary endpoint includes in-hospital mortality and ICU mortality. The secondary endpoint was AECOPD and ARF. All of the endpoints occurred after admitting to the ICU.
Statistical Analysis
Continuous variables conforming to a normal distribution are denoted by, and one-way ANOVA was used for comparison between multiple groups; continuous variables not conforming to normal distribution was expressed as M (P25, P75), and the non-parametric Kruskal–Wallis H-test was used for comparison between multiple groups; and categorical variables was described using frequency and constitutive ratios (%), and chi-square test was used for comparison between groups.
We calculated variance inflation factors (VIF) for all covariates (Table S1). Logistic regression analyses were performed to assess the association between SHR and risk of endpoint events. Tests for trend were calculated using the quartile number as a continuous variable. Spearman correlation was employed to assess the relationship between mortality and prognosis and the level of SHR as a continuous variable. Restricted cubic spline (RCS) modelling to assess the dose-response relationship between SHR and endpoint events. In addition, receiver operating characteristic (ROC) curves were plotted to assess the predictive utility of SHR for priority events (AECOPD, ARF, ICU mortality, and in-hospital mortality). Stratified analyses were performed to assess potential interactions, and subgroup analyses were presented via forest plots. Detailed descriptions of the statistical methods used can be found in the Supplementary Material. All analyses were performed in R software (version 4.1.0). P < 0.05 was used to indicate a statistically significant difference between the two sides.
Results
Comparison of Groups
A total of 2,054 patients were extracted from the present study and 474 patients were excluded due to lack of ABG or HBA1c data, resulting in a total of 1,580 patients included. Baseline characteristics are shown in Table 1. Figure S2 provides comprehensive details of the SHR frequency distribution. The relationship between disease progression (AECOPD and ARF) and mortality (ICU mortality and in-hospital mortality) in patients with COPD and SHR is shown in Figures 1 and 2. To investigate the risk factors associated with the relationship between SHR levels and the duration of AECOPD, in-hospital all-cause mortality, and length of hospital stay, Pearson’s correlation analysis was performed (Table S2). In this analysis, AECOPD and ARF were found to be positively correlated with SHR levels, and ICU deaths and in-hospital deaths were not significantly correlated with SHR levels.
 |
Figure 1 AECOPD and ARF according to the quartiles of SHR. |
 |
Figure 2 Incidence of ICU mortality and in-hospital mortality according to the quartiles of SHR. |
SHR and Mortality
Table 2 shows the relationship between SHR and ICU mortality and in-hospital mortality. As a continuous variable, there was no statistically significant relationship between elevated SHR and ICU mortality and in-hospital mortality, with or without adjustment for confounders. However, the OR for in-hospital mortality for SHR greater than or equal to the median was 1.55 (95% CI, 1.11–2.18). In addition, the relationship between SHR quartiles and ICU mortality and in-hospital mortality was statistically significant only in terms of overall trends. We further found a significant dose-response relationship between SHR and ICU mortality and in-hospital mortality (P for nonlinear= 0.011 and P<0.001, Figure 3).
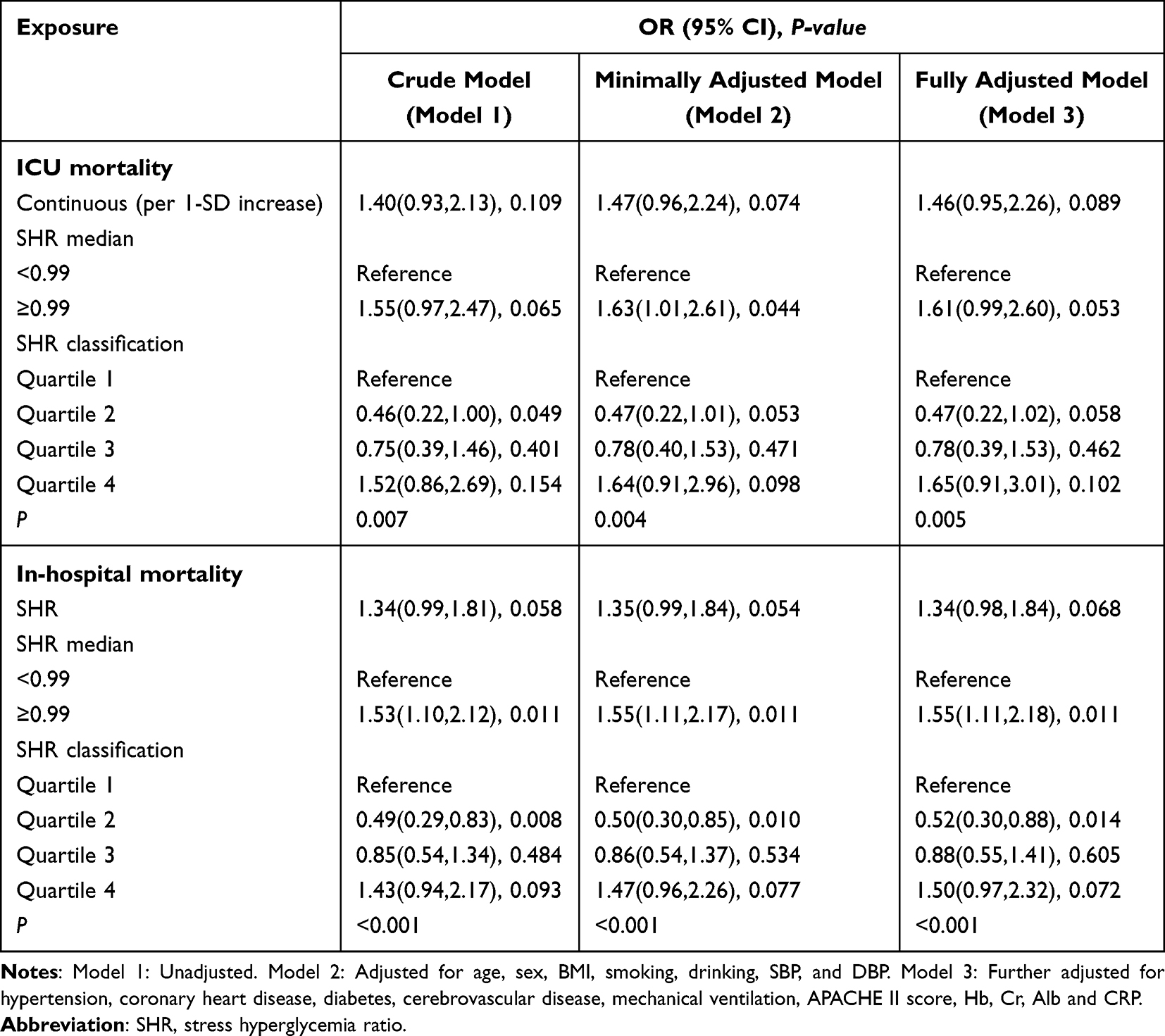 |
Table 2 The Relationship Between SHR and ICU Mortality and in-Hospital Mortality in Critically Ill COPD Patients |
 |
Figure 3 Dose-response association between SHR and mortality in ICU COPD patients. (A) ICU mortality, (B) In-hospital mortality. |
SHR and AECOPD/ARF
Table 3 shows the relationship between SHR and AECOPD and ARF. SHR is significantly and positively associated with the risk of AECOPD (per SD increase; OR, 2.28; 95% CI: 1.68–3.08) and ARF (per SD increase; OR, 2.18; 95% CI: 1.42–3.35). Additionally, in the bivariate model, the OR for AECOPD was 2.61 (95% CI, 1.92–3.55) in the SHR greater than or equal to the median. Further, in the multivariate model, the OR for AECOPD was 2.28 (95% CI, 1.50–3.47) in the third quartile (Q3) and 2.51 (95% CI, 1.63–3.88) in the fourth quartile (Q4) to the first quartile (Q1). Outcomes for ARF remained robustly significant in the fully adjusted model. We further found a significant dose-response relationship between SHR with AECOPD and ARF (P for nonlinear= 0.011 and P<0.001, Figure 4).
 |
Table 3 The Relationship Between SHR and AECOPD and ARF in Critically Ill COPD Patients |
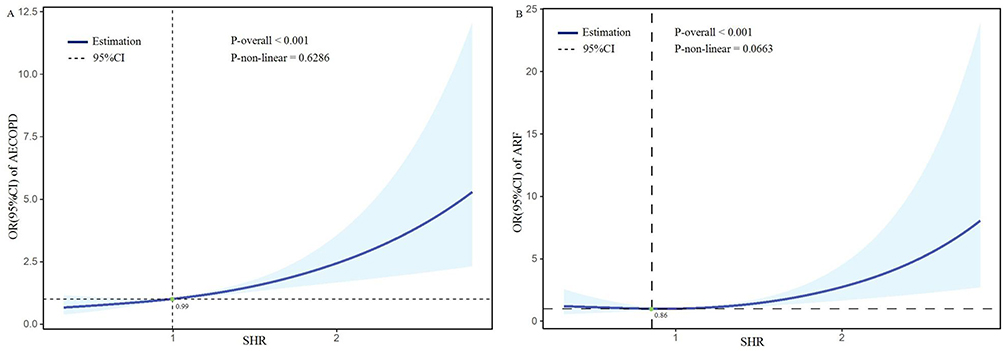 |
Figure 4 Dose-response association between SHR and prognosis in critically ill patients with COPD. (A) AECOPD, (B) ARF. |
ROC Analysis
To compare the superiority of the SHR with the traditional metrics ABG and HBA1c, we performed receiver operating characteristic curve (ROC) analyses. By calculating the area under the curve (AUC), we determined that the SHR predicted AECOPD with the largest AUC of 0.612. This predictive power was consistent for ARF, ICU mortality, and in-hospital mortality (Figure 5). These findings further emphasize the excellent predictive performance of the SHR.
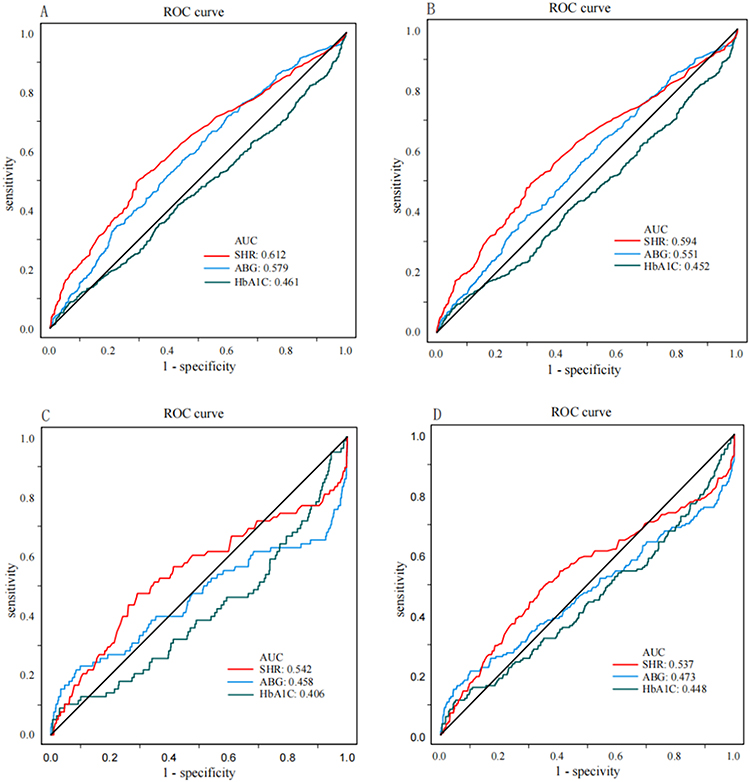 |
Figure 5 Receiver operating characteristic (ROC) analysis of SHR, GAP, ABG, and HbA1c for predicting the prognosis of critically ill COPD patients. (A) AECOPD, (B) ARF, (C) ICU death, (D) In hospital death. |
Subgroup Analysis
To investigate the potential interaction of SHR and related factors on disease progression (AECOPD and ARF) and mortality (ICU mortality and in-hospital mortality), we further performed stratified analyses. The variables of sex, age, BMI, smoking, drinking, history of hypertension, history of coronary heart disease, history of diabetes, and history of cerebrovascular disease did not significantly alter the SHR and ICU mortality and in-hospital mortality (P>0.05 for interaction, Figure 6). We further performed stratified analyses to assess the relationship between SHR and disease progression (AECOPD and ARF) in each subgroup (Figure 7). However, no statistically significant interaction was observed.
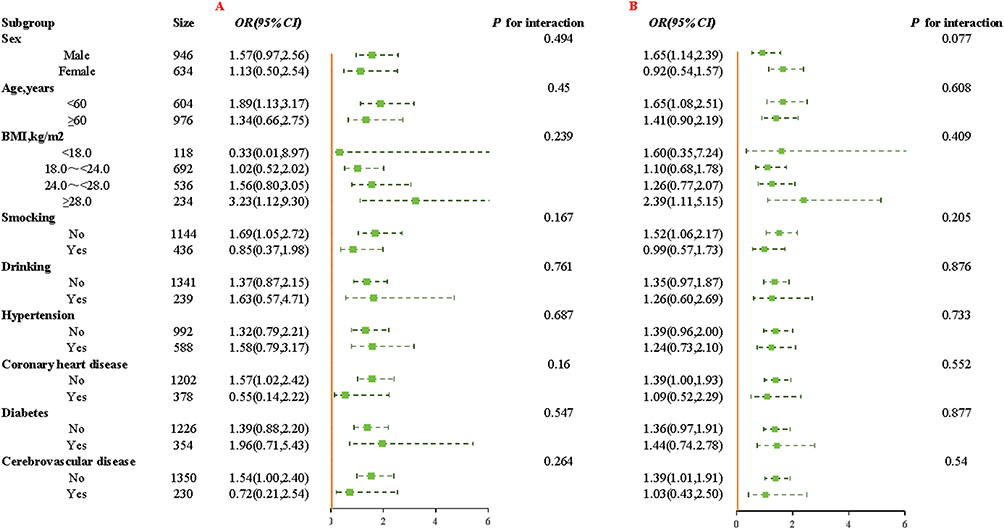 |
Figure 6 Stratified analyses of the association between SHR (per SD increment) and mortality in critically ill patients with COPD. (A) ICU mortality, (B) In-hospital mortality. |
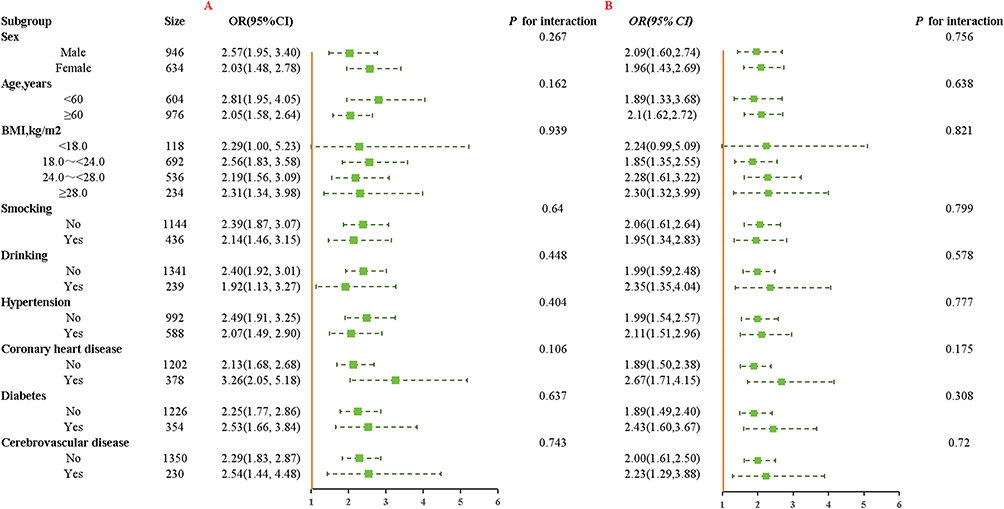 |
Figure 7 Stratified analyses of the association between SHR (per SD increment) and prognosis in critically ill patients with COPD. (A) AECOPD, (B) ARF. |
Discussion
To the best of our knowledge, this is the first study to explore the relationship between SHR and clinical outcomes in COPD patients admitted to the ICU. The current study has two major findings. First, SHR is non-linearly associated with ICU mortality and in-hospital mortality. Second, among patients with CODP, those with high SHR were at higher risk of disease progression, specifically, higher incidence of AECOPD and ARF. Even after multiple sensitivity analyses and adjustment for multiple variables, the correlation between SHR and mortality and prognosis in COPD patients remained strong.
Previous studies have confirmed that critically ill COPD patients have a high glycaemic burden.24 79.0% of AECOPD patients experienced hyperglycaemia during hospitalization, and the prevalence of hyperglycaemia was as high as 89.0% in AECOPD patients treated with mechanical ventilation.13,25 And hyperglycaemia is a significant predictor of disease progression in COPD patients independently of diabetes, age and gender.26 Because the local glucose concentration in human airway secretions is extremely low, when the blood glucose concentration rises above the threshold of 6.7 to 9.7 mmol/L, the glucose concentration in airway secretions rises by 1 to 11 mmol/L, and the high glucose state in the airway promotes the growth and reproduction of bacteria,27 which leads to respiratory tract infections, the innate immune function of the organism is disturbed, and the patient’s risk of adverse prognostic outcomes and death is Increased. According to Baker and colleagues, for every one mmol/L increase in blood glucose, there is a 15% increase in the risk of poor prognosis in patients with AECOPD.26 Therefore, the pre-existing state of stress hyperglycaemia needs to be taken into account when discussing the effect of hyperglycaemia on acute exacerbations in COPD patients.
SHR is a more effective quantitative indicator of stress hyperglycaemia than blood glucose levels in assessing the prognostic outcome of disease in critically ill patients.22 The SHR ratio, as a new biomarker, is able to accurately reflect changes in blood glucose levels in the presence of stress in the organism.28 Several previous studies have evaluated the relationship between SHR and clinical outcomes of different diseases. A meta-analysis involving 15,250 patients found that for every one unit increase in SHR, there was a 2.19-fold increase in the incidence of risk of death in patients with heart failure.29 In Japan, a multi-centre retrospective study suggest that SHR served as an independent predictor of in-hospital adverse cardiovascular events in patients with acute myocardial infarction.30 This indicates that SHR can be used as a valid biomarker for predicting adverse in-hospital clinical outcomes in critically ill populations. A large retrospective cohort study based on the MIMIC-IV database demonstrated that SHR was associated with increased 90-day mortality in patients with pulmonary hypertension in the ICU.31 A multi-centre cohort study similarly found that SHR was positively associated with clinical deterioration in idiopathic pulmonary arterial hypertension patients.32 The association seems to be partially mediated through the pathway of pulmonary vascular remodelling, suggesting that SHR may be a valuable indicator to provide information on the risk of respiratory disease progression.32 The present study explored the association between SHR and the risk of disease progression and mortality in COPD patients and concluded that SHR was an independent predictor of ICU mortality and in-hospital mortality in critically ill COPD patients.Elevated SHR was associated with an increased risk of AECOPD and ARF. Therefore, SHR is expected to be a new risk factor for early risk stratification of critically ill COPD patients.
Several potential mechanisms could explain the observed association between SHR and increased risk of disease progression and poor prognosis in critically ill COPD patients. First, oxidative stress and inflammation are key factors in COPD progression. In response to critically ill COPD patients, glucose levels increase rapidly in response to intracellular oxidative stress, which promotes the release of pro-inflammatory cytokines, such as tumour necrosis factor-alpha (TNF-alpha) and interleukin (IL-6), and exacerbates the body’s inflammatory response.33 Studies have shown that under stress, mediated by the hypothalamic-pituitary-adrenal axis and the sympathetic nervous system, the organism’s blood glucose level in critically ill COPD patients temporarily increases, leading to exacerbation of respiratory infections and a significant increase in the incidence of AECOPD.34 The incidence of stress hyperglycaemia in critically ill patients has been reported to be about 43% to 50%,35 with 89% of COPD patients experiencing hyperglycaemia during disease exacerbation.36 Secondly, hyperglycaemia leads to disturbances in glucose metabolism and lipid metabolism, and an increase in the production of ketone bodies with acidic metabolites may exacerbate hypoxia and pulmonary impairment, ultimately leading to the development of AECOPD.37 In acute exacerbation of COPD, there is often a sharp decrease in lung function, and severe dyspnoea may lead to hypoxaemia, which may affect the body’s energy metabolism, prompting the body to rely on the glycolytic pathway to produce energy, further exacerbating the disorders of glucose metabolism in the body.38 The two promote and influence each other. This also suggests that SHR is a therapeutic target to alleviate the poor prognosis of critically ill COPD patients.
The present study pioneered the investigation of the relationship between SHR and disease progression and poor prognosis in critically ill COPD patients. Our study has several strengths, including a large sample size, consistent data collection methods, and comprehensive information on potential confounders. While these results are compelling, it is imperative to recognize the limits of observational data in establishing causation. First, all baseline characteristics were obtained within 24 hours of ICU admission, and there is a lack of data on dynamic changes in SHR during hospitalization, requiring more in-depth investigation with larger sample sizes and longitudinal prospective studies to provide additional evidence for clinical diagnosis. Second, although we adjusted for a variety of known confounders, we were unable to exclude all potential confounders that may affect COPD, such as heritage factors. Third, the study failed to collect data from participants receiving glucose-lowering therapy and using medications that affect blood glucose concentrations, and therefore could not assess any other relationship between SHR and glucose-lowering therapy in patients with COPD. Finally, given that our study was limited to a Chinese population, caution is needed in generalizing these findings to other populations. Therefore, we hope to include a more diverse population and more comprehensive data in future studies to further consolidate and validate these findings.
Conclusion
The present study demonstrated that SHR was independently associated with an increased risk of AEOCOPD, ARF, ICU mortality and in-hospital mortality in critically ill COPD patients after adjusting for confounders. SHR can be used for prognostic prediction and risk stratification in critically ill patients with COPD. In the future, prospective cohort studies can be conducted to gain insights into the effects of changes in body glucose metabolism on disease progression and risk of death in critically ill patients with COPD under stress, so as to provide more effective guidance and strategies for the prevention and management of respiratory diseases.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
The present study involving human participants was carried out by the Helsinki Declaration and was approved by the hospital ethics committee (approval number: KY2023071303) and was exempted from the informed consent requirement because the medical records were de-identified and the study was retrospective in nature.
Acknowledgments
Mengyuan Qiao and Hui Yang are co-first authors for this study. The authors would like to thank all the patients who participated in the survey and the health care workers who assisted in the data collection process.
Funding
This study was funded by the Tianshan Talent Training Program-Science and Technology Innovation Team (No. TSYC202301A085).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Divo M, Celli BR. Multimorbidity in patients with chronic obstructive pulmonary disease. Clin Chest Med. 2020;41(3):405–419. doi:10.1016/j.ccm.2020.06.002
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study. Lancet. 2015;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
4. Chan KP KFW, Hui DS, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.127802
5. Ritchie AI, Definition WJA. Causes pathogenesis and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
6. Stone P, Sood N, Feary J, et al. Validation of acute exacerbation of chronic obstructive pulmonary disease (COPD) recording in electronic health records: a systematic review protocol. BMJ Open. 2020;10(2):e032467. doi:10.1136/bmjopen-2019-032467
7. van der Bie S, Haaksma ME, Vermin B, et al. A systematic review of the pulmonary microbiome in patients with acute exacerbation COPD requiring ICU admission. J Clin Med. 2024;13(2):472. doi:10.3390/jcm13020472
8. Prediletto I, Giancotti G, Nava S. COPD Exacerbation: why It Is Important to Avoid ICU Admission. J Clin Med. 2023;12(10):3369. doi:10.3390/jcm12103369
9. Dixit D, Bridgeman MB, Andrews LB, et al. Acute exacerbations of chronic obstructive pulmonary disease: diagnosis, management, and prevention in critically ill patients. Pharmacotherapy. 2015;35(6):631–648. doi:10.1002/phar.1599
10. Tabaza H, Farha RA, Gharaibeh L, et al. Length of hospital stay and its predictions among patients with exacerbations of chronic respiratory diseases. J Eval Clin Pract. 2025;31(1):e14308. doi:10.1111/jep.14308
11. Ai-Ping C, Lee KH, Lim TK. In-hospital and 5-year mortality of patients treated in the ICU for acute exacerbation of COPD: a retrospective study. Cheat. 2005;128(2):518–524. doi:10.1378/chest.128.2.518
12. Papathanassiou E, Papaioannou AI, Papanikolaou I, et al. Glycated hemoglobin (HbA1c) as a predictor of outcomes during acute exacerbations of chronic obstructive pulmonary disease. COPD. 2021;18(2):219–225. doi:10.1080/15412555.2021.1902491
13. Edriss H, Selvan K, Sigler M, et al. Glucose levels in patients with acute respiratory failure requiring mechanical ventilation. J Intensive Care Med. 2017;32(10):578–584. doi:10.1177/0885066616636013
14. Pan Y, Cai X, Jing J, et al. Stress hyperglycemia and prognosis of minor ischemic stroke and transient ischemic attack: the CHANCE Study (Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events). Stroke. 2017;48(11):3006–3011. doi:10.1161/STROKEAHA.117.019081
15. Roberts GW, Larwood C, Krinsley JS. Quantification of stress-induced hyperglycaemia associated with key diagnostic categories using the stress hyperglycaemia ratio[J]. Diabetic Med. 2022;39(10):e14930. doi:10.1111/dme.14930
16. Xu W, Song Q, Wang X, et al. Association of stress hyperglycemia ratio and in-hospital mortality in patients with coronary artery disease: insights from a large cohort study. Cardiovasc Diabetol. 2022;21(1):217. doi:10.1186/s12933-022-01645-y
17. Mohammed AQ, Liu L, Alifu J, et al. Association of novel inflammatory and metabolic markers with mortality in individuals with overweight and obesity. Nutr Metab Cardiovas. 2023;35(3):103859. doi:10.1016/j.numecd.2025.103859
18. Song Q, Dai M, Zhao Y, et al. Association between stress hyperglycemia ratio and delirium in older hospitalized patients: a cohort study. BMC Geriatr. 2022;22(1):277. doi:10.1186/s12877-022-02935-6
19. Kaeidi A, Hajializadeh Z, Jahandari F, et al. Leptin attenuates oxidative stress and neuronal apoptosis in hyperglycemic condition. Fund Clin Pharmacol. 2019;33(1):75–83. doi:10.1111/fcp.12411
20. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Arch Bronconeumol. 2023;59(4):232–248. doi:10.1016/j.arbres.2023.02.009
21. Lee H, Lim CW, Hong HP, et al. Efficacy of the APACHE II score at ICU discharge in predicting post-ICU mortality and ICU readmission in critically ill surgical patients. Anaesth Intens Care. 2015;43(2):175–186. doi:10.1177/0310057X1504300206
22. Roberts GW, Quinn SJ, Valentine N, et al. Relative hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio. J Clin Endocr Metab. 2015;100(12):4490–4497. doi:10.1210/jc.2015-2660
23. Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl. 2003;22(47 suppl):3s–14s. doi:10.1183/09031936.03.00038503
24. Cai BQ, Cai SX, Chen RC, et al. Expert consensus on acute exacerbation of chronic obstructive pulmonary disease in the People’s Republic of China. Int J Chron Obstruct Pulmon Dis. 2014;9:381–395. doi:10.2147/COPD.S58454
25. Koskela HO, Salonen PH, Niskanen L. Hyperglycaemia during exacerbations of asthma and chronic obstructive pulmonary disease. Clin Respir J. 2013;7(4):382–389. doi:10.1111/crj.12020
26. Baker EH, Janaway CH, Philips BJ, et al. Hyperglycaemia is associated with poor outcomes in patients admitted to hospital with acute exacerbations of chronic obstructive pulmonary disease. Thorax. 2006;61(4):284–289. doi:10.1136/thx.2005.051029
27. Wood DM, Brennan AL, Philips BJ, et al. Effect of hyperglycaemia on glucose concentration of human nasal secretions. Clin Sci. 2004;106(5):527–533. doi:10.1042/CS20030333
28. Li L, Zhao M, Zhang Z, et al. Prognostic significance of the stress hyperglycemia ratio in critically ill patients. Cardiovasc Diabetol. 2023;22(1):275. doi:10.1186/s12933-023-02005-0
29. Li L, Zhao Z, Wang S, et al. Stress hyperglycemia ratio and the clinical outcome of patients with heart failure: a meta-analysis. Front Endocrinol. 2023;15:1404028. doi:10.3389/fendo.2024.1404028
30. Okita S, Saito Y, Yaginuma H, et al. Impact of the stress hyperglycemia ratio on heart failure and atherosclerotic cardiovascular events after acute myocardial infarction. CIRC J. 2023;89(3):340–346. doi:10.1253/circj.CJ-24-0612
31. Long C, Fan W, Liu Y, et al. Stress hyperglycemia is associated with poor outcome in critically ill patients with pulmonary hypertension. Front Endocrinol. 2023;15:1302537. doi:10.3389/fendo.2024.1302537
32. Zhang S, Gao L, Li S, et al. Is pulmonary vascular remodeling an intermediate link between hyperglycemia and adverse outcomes in patients with idiopathic pulmonary arterial hypertension? Insights from a multi-center cohort study. Cardiovasc Diabetol. 2023;23(1):384. doi:10.1186/s12933-024-02476-9
33. Beitland S, Opdahl H, Aspelin T, et al. Blood leucocyte cytokine production after LPS stimulation at different concentrations of glucose and/or insulin. Acta Anaesth Scand. 2008;53(2):183–189. doi:10.1111/j.1399-6576.2008.01836.x
34. Chen G, Lin Q, Zhuo D, et al. Elevated blood Glucose is associated with severe exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2453–2459. doi:10.2147/COPD.S378259
35. Van den Berghe G, Wouters PJ, Bouillon R, et al. Outcome benefit of intensive insulin therapy in the critically ill: insulin dose versus glycemic control. Crit Care Med. 2003;31(2):359–366. doi:10.1097/01.CCM.0000045568.12881.10
36. Yang CJ, Liao WI, Tang ZC, et al. Glycated hemoglobin A1c-based adjusted glycemic variables in patients with diabetes presenting with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:1923–1932. doi:10.2147/COPD.S131232
37. Olver TD, Grunewald ZI, Jurrissen TJ, et al. Microvascular insulin resistance in skeletal muscle and brain occurs early in the development of juvenile obesity in pigs. Am J Physiol-Reg I. 2017;314(2):R252–R264. doi:10.1152/ajpregu.00213.2017
38. Oltmanns KM, Gehring H, Rudolf S, et al. Hypoxia causes glucose intolerance in humans. Am J Respir Crit Care Med. 2004;169(11):1231–1237. doi:10.1164/rccm.200308-1200OC
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Macrolide Antibiotics on In-Hospital Mortality Among Acute Exacerbation of COPD Patients: A Propensity Score-Matched Analysis
Morasert T, Kriengwattanakul O, Kulalert P
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2229-2239
Published Date: 13 September 2022
Six-Minute Walking Test and 30 Seconds Chair-Stand-Test as Predictors of Mortality in COPD – A Cohort Study
Höglund J, Boström C, Sundh J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2461-2469
Published Date: 4 October 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023
Respiratory Infection Triggering Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:555-565
Published Date: 27 February 2024