Back to Journals » Clinical Epidemiology » Volume 15
Increased Risk of Anemia in Patients with Asthma
Authors Rhew K ![]() , Choi J, Kim K
, Choi J, Kim K ![]() , Choi KH
, Choi KH ![]() , Lee SH, Park HW
, Lee SH, Park HW ![]()
Received 7 November 2022
Accepted for publication 23 December 2022
Published 5 January 2023 Volume 2023:15 Pages 31—38
DOI https://doi.org/10.2147/CLEP.S394717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Kiyon Rhew,1 Jisu Choi,1 Kyungim Kim,2,3 Kyung Hee Choi,4 So-Hee Lee,5 Heung-Woo Park6
1College of Pharmacy, Dongduk Women’s University, Seoul, Republic of Korea; 2Institute of Pharmaceutical Science, Korea University, Sejong, Republic of Korea; 3College of Pharmacy, Korea University, Sejong, Republic of Korea; 4College of Pharmacy, Gachon University, Incheon, Republic of Korea; 5Seoul National University Hospital Healthcare System Gangnam Center, Seoul, Republic of Korea; 6Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea
Correspondence: Kiyon Rhew; Heung-Woo Park, Tel +82 2 940 4519 ; +82 2 742 3291, Fax +82-2-940-4159 ; +82 2 2072 0699, Email [email protected]; [email protected]
Purpose: Asthma can cause a systemic inflammatory response, and anemia of chronic disease (ACD) is known to be caused by other disorders with a chronic inflammatory state. However, it is unclear whether the incidence of anemia is increased in patients with asthma. The objective of this study was to compare the incidence of anemia in patients with asthma and healthy adults.
Patients and Methods: This retrospective cohort study included patients newly diagnosed with asthma at Seoul National University Hospital from 2010 to 2017. Patients with comorbidities before the first visit (index date) that may increase anemia risk were excluded. Cox regression models adjusting for patient age, sex, and obesity were used to compare anemia hazard ratios (HRs) between asthma patients (n=1354) and healthy adults (n=1731).
Results: This study included 3085 patients. During 5-y follow-up, anemia occurred in 203 (15.0%) patients with asthma and 79 (4.6%) healthy adults. Compared with healthy adults, the HR for anemia after adjusting for age, sex, and obesity was 4.06 (95% CI: 2.70– 6.09) in patients with asthma. In patients aged 18– 64.9 y, the adjusted HR of anemia was 3.27 (95% CI: 2.12– 5.04) in patients with asthma, compared to healthy patients. In patients > 65 y, this adjusted HR was 5.56 (95% CI: 1.31– 23.67).
Conclusion: The risk of anemia was increased in patients with asthma after adjusting for sex, age, and obesity and excluding comorbidities that can cause anemia. These results suggest the need for regular monitoring for anemia in patients with asthma.
Keywords: anemia, asthma, inflammation, anemia of chronic disease
Introduction
Asthma is a well-known cause of systemic inflammatory response,1–3 and anemia of chronic disease (ACD) is caused by diseases inducing a chronic inflammatory state.4 ACD (also called anemia of inflammation) is the result of immune-mediated dysregulation of hepcidin and several cytokines that play an important role in iron homeostasis. ACD is associated with proliferating red blood cell (RBC) progenitors that can accelerate the turnover of RBCs and affect the activity of erythropoietin.5,6
ACD and iron deficiency anemia (IDA) have similar hematologic characteristics, including low hemoglobin and serum iron levels. However, the mechanism, treatment, and degree of treatment response differ between these two types of anemia.7 While the risk of ACD is higher in patients with chronic obstructive pulmonary disease (COPD), malignancy, or chronic heart failure,8–11 it is unclear whether the risk is increased in patients with asthma. It is essential to evaluate whether the risk of developing ACD is elevated in patients with asthma, similar to other chronic diseases.
Drury et al have shown a correlation between anemia and atopic diseases, including asthma, in children.12 Our prior studies suggested that the prevalence of anemia is high in patients with asthma13,14 and that the prevalence of anemia is higher in patients with poor asthma control than in patients with well-controlled asthma symptoms.15 However, all of these previous studies were cross-sectional. Although these findings suggested an association between anemia and asthma, their study design did not allow the determination of whether the relationship is causal.
We hypothesized that the systemic inflammatory state of asthma could increase the risk of developing ACD. Therefore, we conducted a cohort study to compare the incidence of anemia in patients with asthma and healthy adults.
Materials and Methods
Study Subjects
Adults 18 years or older were divided into two groups: asthma patients and healthy adults. The asthma patient group included patients who met all of the following criteria: 1) first diagnosed with asthma at the Department of Internal Medicine in Seoul National University Hospital from January 1, 2010 to December 31, 2017 (the date of diagnosis was considered the index date); 2) visited the Department of Internal Medicine for at least 3 years after the index date, with medical records available for four or more visits during this time; 3) medical records available from Seoul National University Hospital during the 2 years before the index date; 4) at least three available complete blood cell count (CBC) test results obtained after the index date.
The healthy adult control group included individuals who satisfied all of these criteria: 1) health checkups from January 1, 2010 to December 31, 2017 at the Seoul National University Hospital Healthcare System Gangnam Center, with no asthma diagnosis (the index date was considered the first examination date); 2) medical examination records available for the 2 years before the index date; 3) normal pulmonary function test results, with a forced expiratory volume in 1 s (FEV1)/forced vital capacity ≥ 70% and an FEV1 ≥ 80%); and 4) more than 3 years of available medical examination records and CBC test results after the index date.
We excluded patients diagnosed within 2 years before or at the index date with anemia or a disease that might increase the risk of ACD or IDA. These diseases included the following: 1) systemic infection (meningitis [International Classification of Diseases (ICD)-10 A87.X, A39.X], sepsis [A40.X, A41.X], tuberculosis [A15.X–A19.X], or human immunodeficiency virus disease [B20.X-B24.X]); 2) hepatitis (B15.X–19.X); 3) chronic kidney disease (CKD; N18.X); (4) heart failure (I50.X); (5) diabetes (E10.X–E14.X); (6) chronic inflammatory disease (COPD [J42.X, J43.X, J44.X], systemic lupus erythematosus [M32.X], or rheumatoid arthritis [M05.X, M06.X, M08.0]); and (7) malignant tumor (CXX.X). In addition, patients with an aspartate aminotransferase or alanine aminotransferase level 100 U/L or higher or an estimated glomerular filtration rate less than 60 mL/min/1.73 m2 on the index date were excluded. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (approval no. H-2110-164-1266). The Board waived the requirement for informed consent because of the study’s design (retrospective cohort study). This study complied with the Declaration of Helsinki and was performed according to ethics committee approval, including maintaining all the patients’ information confidentiality.
Definition of Disease and Study Outcome
Asthma was defined as the presence of one or more respiratory symptoms (eg, cough, shortness of breath, wheezing) and one or more of the following: 1) FEV1 of 12% or more and increased by more than 200 mL after bronchodilator; 2) positive bronchial provocation test (eg, methacholine, mannitol, exercise, aspirin); or 3) FEV1 increased by more than 12% and more than 200 mL after starting asthma treatment, compared to before treatment.
The study outcome was anemia. Anemia was defined as a hemoglobin level below the lower limit of the normal range (13.6 g/dL for men, 11.9 g/dL for women) and a low hematocrit level (< 40% for men, < 35% for women) or low RBC count (4.2×106/µL for men, 3.8×106/µL for women). Other diseases besides asthma and anemia were defined based on a physician’s diagnosis or the patient’s self-report of being diagnosed with the disease.
Follow-Up
Patients were censored when diagnosed with systemic infection, hepatitis, CKD, diabetes, chronic inflammatory disease, or malignancy, whichever occurred first. For patients who were not censored, we terminated the follow-up at a maximum of 60 months or December 31, 2021, whichever occurred earlier.
Sensitivity Analysis
A sensitivity analysis was conducted to evaluate the effect of potential outcome misclassification by restricting the analysis to individuals with persistent anemia, which was defined as two consecutive anemia diagnoses at least 3 months apart.
Statistical Analysis
In this study, we compared the distributions of demographic and clinical characteristics between the two groups (asthma patients and healthy adults) and calculated the incidence of anemia. A Cox regression model was used to estimate the hazard ratio (HR) for anemia by comparing asthma and healthy adults and their corresponding 95% confidence intervals (CIs) adjusted for covariates (age, sex, and obesity). All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Results were deemed statistically significant if the p-value was less than 0.05.
Results
Subject Characteristics
A total of 1802 adult patients were first diagnosed with asthma at the Seoul National University Hospital during the study period. Of these, 1354 patients were included in the asthma patient group after excluding 448 patients who were diagnosed with anemia before or at the index date or who had a potential confounding factor (abnormal renal function or liver enzymes or a disease diagnosis listed as exclusion criteria in the Methods). For the healthy adult group, 14,436 subjects underwent health checkups at Seoul National University Hospital Healthcare System Gangnam Center during the study period. After excluding 12,705 individuals with anemia or a potential confounding factor (as in the asthma group), 1731 adults were included in the final healthy adults group (Figure 1).
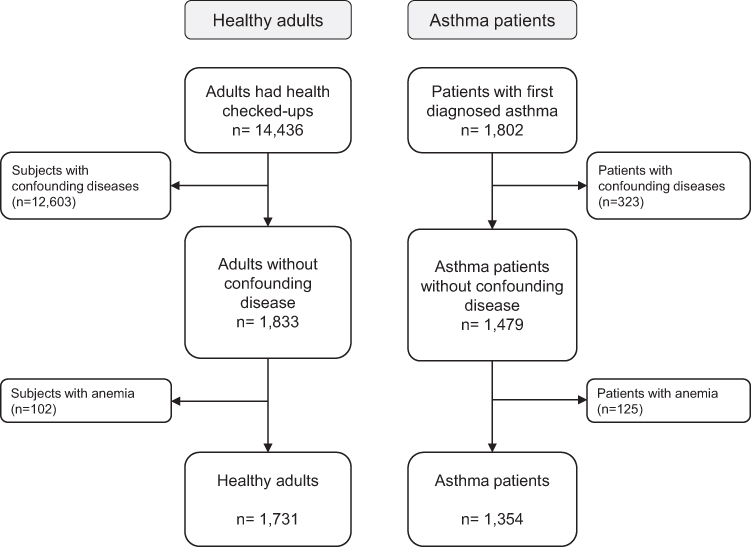 |
Figure 1 Flow diagram for study subject inclusion. |
Males accounted for 68.4% of patients with asthma, whereas females accounted for 63.4% of healthy adults. The number of adults younger than 65 years was 1657 (95.7%) in the healthy adults group and 1009 (74.5%) in the asthma patients group. The number of obese subjects was 499 (36.9%) in the asthma patients group and 485 (28.0%) in the healthy adults group (Table 1).
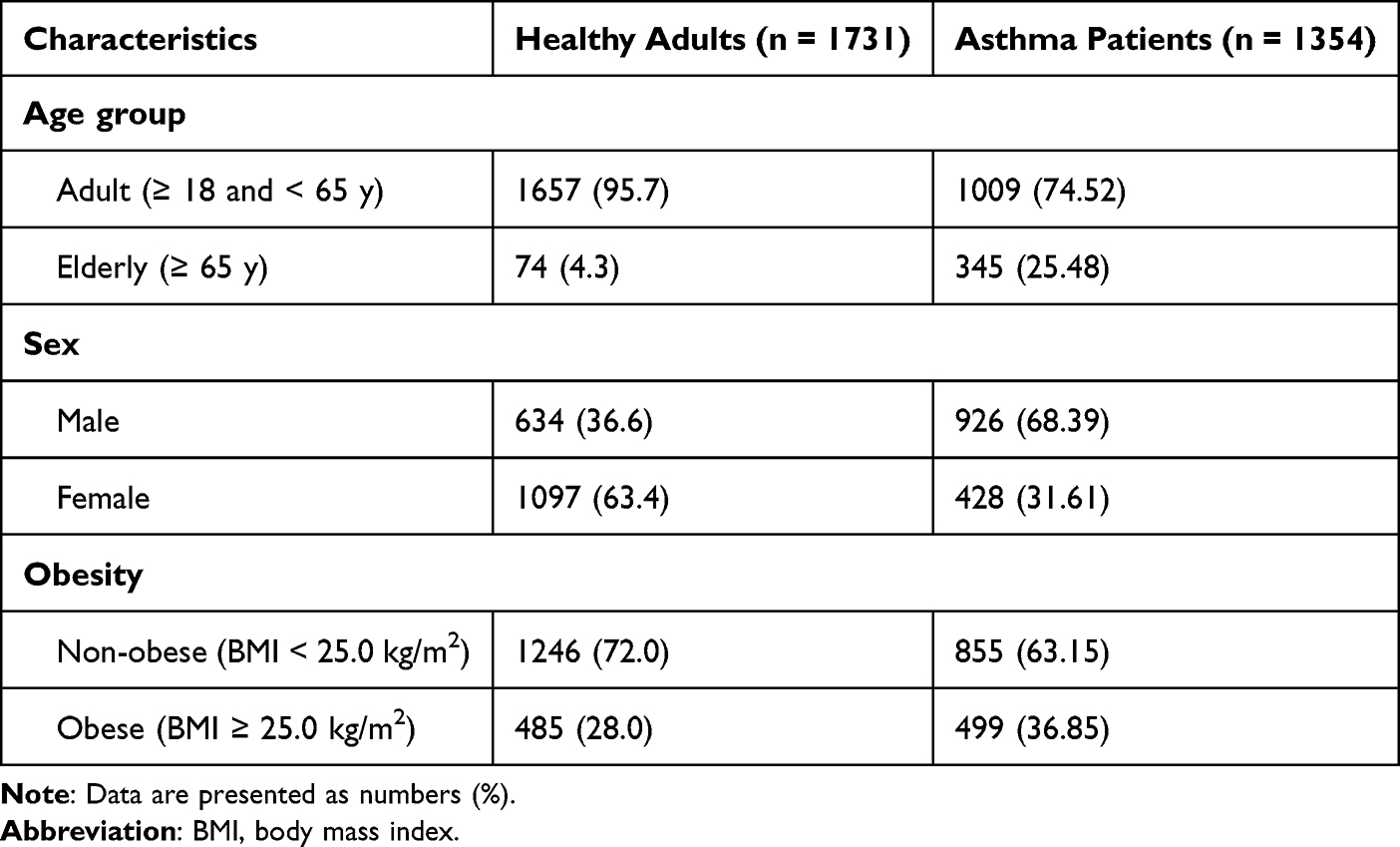 |
Table 1 Characteristics of Study Subjects |
Risk of Anemia in Asthma Patients Compared to Healthy Adults
When considering all patients, anemia occurred in 203 (15.0%) of the 1354 patients with asthma and 79 (4.6%) of the 1731 healthy adults. Compared with healthy adults, the HR for anemia in the asthma patients group was 4.06 (95% CI: 2.70–6.09), after adjusting for age, sex, and obesity as covariates. Age was also significantly associated with anemia (HR: 1.02 [95% CI: 1.01–1.03]), but sex and obesity were not statistically significant risk factors for anemia (Table 2).
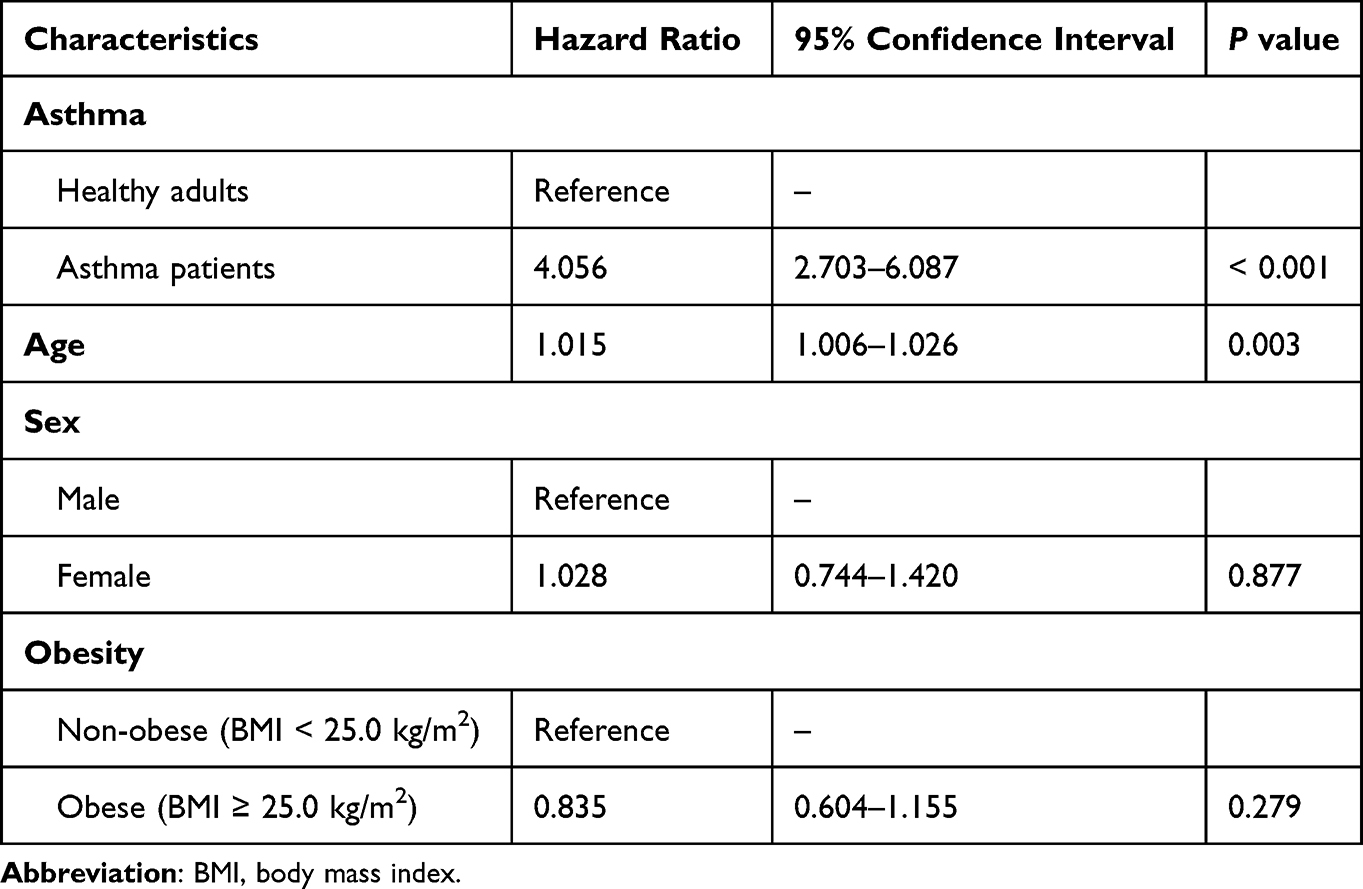 |
Table 2 The Risk of Anemia According to the Presence of Asthma and Other Potential Risk Factors |
When considering patients 18 to 65 years of age, anemia occurred in 122 (12.1%) of 1009 asthma patients and 76 (4.6%) of 1657 healthy adults. The rate ratio was 1.82 times in patients with asthma, compared to healthy patients. The adjusted HR for anemia was 3.27 (95% CI: 2.12–5.04) in the asthma patients group. In patients over 65 years of age, the rate ratio was 4.68 in patients with asthma, compared to healthy adults. The risk of anemia was higher in these older patients than in the younger adults, with an adjusted HR of 5.56 (95% CI: 1.31–23.67) in patients with asthma. In healthy adults, the risk of anemia did not vary with age, with similar incidence rates in the younger and older groups. By contrast, in the asthma patients group, the incidence of anemia in older patients was more than double the incidence in younger patients (Table 3).
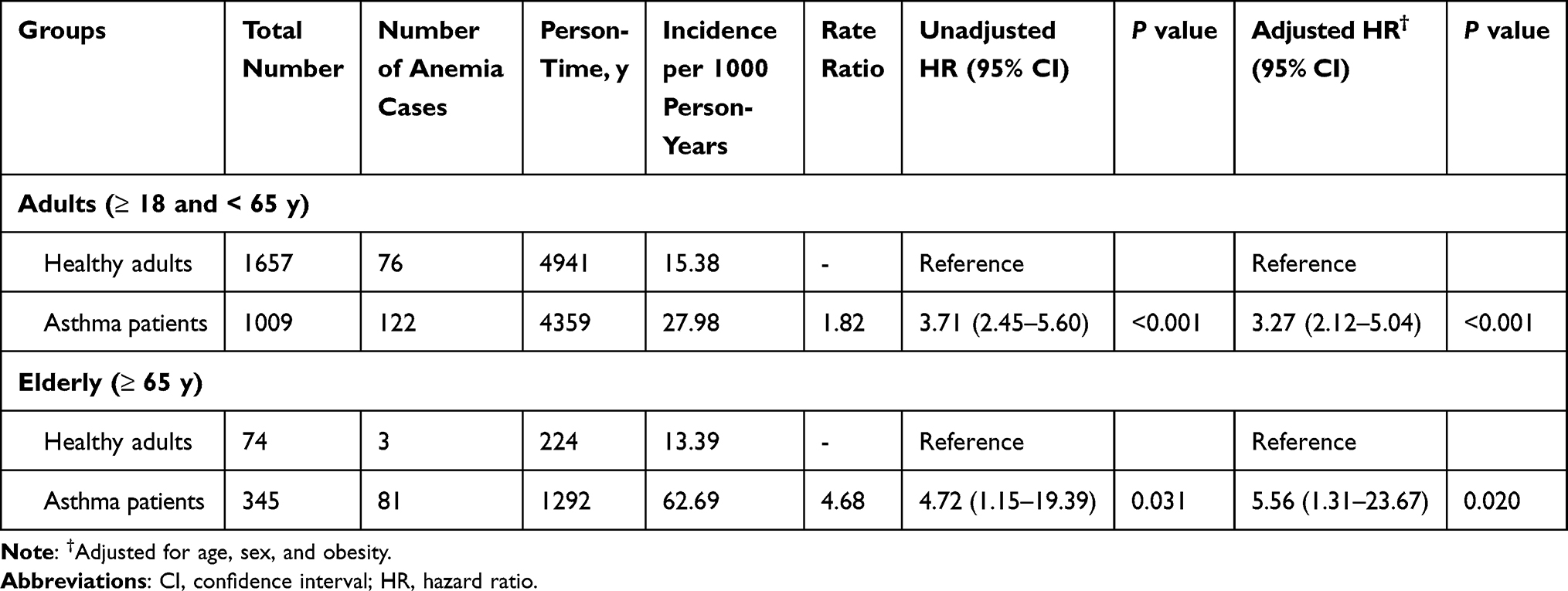 |
Table 3 Age-Stratified Risk of Anemia According to the Presence of Asthma |
Sensitivity Analysis
In the sensitivity analysis of only patients who met the criteria for diagnosis of anemia on two consecutive occasions, the risk of anemia was higher in patients with asthma than in healthy adults. The HR for anemia adjusted for age, gender, and obesity in the asthma patients group was 9.32 (95% CI: 4.16–20.89), which was statistically significant (Table 4).
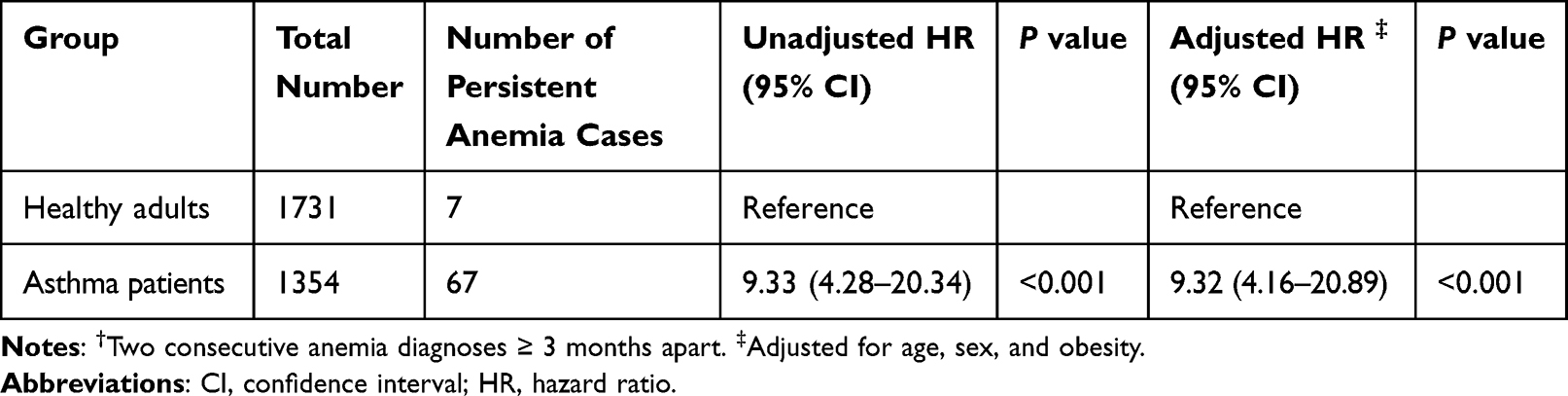 |
Table 4 Sensitivity Analysis for the Risk of Persistent Anemia† According to the Presence of Asthma |
Discussion
In this study, 203 (15.0%) of 1354 asthma patients developed anemia. The risk of developing anemia within 5 years (60 months) was 4.06 times higher in adults with asthma than in healthy adults. In a previous study, the prevalence of anemia in adults with asthma was 1.25 times higher than that in patients without asthma,14 similar to the results of the present study. Since this study excluded all patients with other diseases that may increase the risk of anemia, the results of this study may provide a more accurate estimate of the true risk of anemia in patients with asthma. It should also be noted that our results reflected the incidence of anemia, not the prevalence of anemia in patients with asthma. Our sensitivity analysis further confirmed that the risk of anemia was increased in patients with asthma.
The pathophysiologic mechanisms by which asthma can lead to anemia are unclear. The primary pathogenesis of asthma involves T helper 2 (Th2) or innate type 2 immune responses. Interleukin (IL)-4, IL-5, IL-13, and eosinophil infiltration may also play an important role. However, several mechanisms have been proposed for non-Th2–mediated asthma. First, the Th17 pathway promotes neutrophil infiltration of airways and increases IL-17 and IL-6 secretion.16,17 In addition, it has been demonstrated that interferon (IFN)-γ secretion is enhanced in Th1-mediated asthma.18 IL-1β and tumor necrosis factor (TNF)-α secretion and inflammation are also activated because of airway epithelial cell damage.19–23 The mechanism by which these inflammation inducible cytokines induce ACD has been well described by Guenter.4 TNF-α can reduce the half-life of RBCs and impair the responsiveness of progenitor cells to erythropoietin. IFN-γ can promote divalent metal transporter 1 (DMT1) synthesis and impair progenitor cells’ responsiveness to erythropoietin, leading to anemia.21 IL-6 can also increase hepcidin levels and cause ferritin transcription, suggesting a mechanism that may lead to ACD.8 Thus, anemia in asthma may be caused by an imbalance of several different cytokines.
It is known that C-reactive protein (CRP), IL-6, and IFNγ levels are increased in patients with COPD, which can lead to a systemic inflammatory state and cause ACD.24,25 In patients with CKD, increased serum CRP and IL-6 levels secondary to decreased renal function are also known to cause an inflammatory condition.26 Furthermore, elevated IL-1 and TNF-α levels have been reported in animals without renal function.27 In patients with rheumatoid arthritis, the severity of symptoms is positively correlated with hepcidin levels.28,29 Increased levels of hepcidin accompanying chronic diseases could induce anemia. If cytokine changes similar to those seen in these other chronic diseases also occur in asthma, they may contribute to the occurrence of ACD in patients with asthma.
Immune activation or inflammation in patients with asthma and iron deficiency are correlated. Macrophages are present in all tissues and function to support and restore tissue homeostasis balance.30 In addition, it serves as a sensor for iron demand in tissues and a supply of iron as an essential trace element.30 These iron-handling features determine anti-inflammatory and inflammatory status.31 Several studies have found an association between iron deficiency and atopic disease. Eventually, prolonged immune activation will lead to functional iron deficiency32 and, over time, will develop into ACD.33 The study by Shaheen reported that these direct links between asthma and iron deficiency are apparent.34
Anemia is an important risk factor for cardiovascular disease and mortality.35,36 Especially in older individuals, anemia has a major negative impact on the quality of life and survival rate.37 Asthma can also reduce quality of life and increase morbidity and mortality.38,39 If the risk of developing ACD increases in patients with asthma, it is important to incorporate the detection and management or treatment of anemia in the overall medical care of these patients.40 In ACD (unlike IDA), hemoglobin levels usually do not decrease below 7 g/dL, and RBCs are typically normocytic and normochromic.4,40 Therefore, the diagnosis of anemia in patients with asthma can be easily overlooked in clinical practice. However, our confirmed that the risk of developing anemia was increased when patients with asthma were followed for approximately 5 years. Thus, periodic blood tests for anemia are necessary for asthma patients. If anemia is detected, it is important to distinguish between ACD and IDA, as the therapeutic approaches differ between these two types.
This study has several limitations. First, Seoul National University Hospital is one of the largest hospitals in Korea. Therefore, patients with asthma in this study might have had more severe symptoms than the general population of patients with asthma. Also, even if patients seemed to be diagnosed with asthma for the first time at our hospital, we cannot be sure that they were not previously diagnosed with the disorder at another hospital. Second, it was not possible to evaluate confounding factors other than diseases excluded from this study because of the lack of available data on other factors. Third, the characteristics of the asthma patients group and healthy adults group were very different. As only patients without other underlying diseases were included in the control group, this group was relatively younger and contained more women than the asthma patients group.
Nevertheless, this study has several strengths. First, it is the first study to present the results of long-term follow-up on the risk of anemia in patients with asthma. Second, to the best of our knowledge, all previous studies examined the prevalence, not incidence, of anemia in patients with asthma. By focusing on incidence, our study provides information about a possible causal relationship between asthma and anemia. Finally, anemia was diagnosed solely on blood test results, not the patient’s self-report or a physician’s diagnosis.
Conclusion
The risk of anemia was increased in adults with asthma. This result was obtained after adjusting for patient sex, age, and obesity and excluding patients with other diseases that can increase the risk of anemia. The results of this study suggest that patients with asthma should undergo regular testing for the presence of anemia to allow early detection and initiation of treatment. Further studies on the mechanism of ACD development in patients with asthma are required. Such studies will help further our understanding of the chronic and systemic inflammatory responses of this patient population.
Abbreviations
ACD, anemia of chronic disease; CBC, complete blood cell count; Cis, confidence intervals; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; DMT1, divalent metal transporter 1; FEV1, forced expiratory volume in 1 s; ICD, International Classification of Diseases; IDA, iron deficiency anemia; IFN, interferon; IL, interleukin; RBC, red blood cell; Th2, T helper 2; TNF, tumor necrosis factor.
Acknowledgments
This work was supported by a grant (No. 2021R1F1A1059897) of the National Research Foundation (NRF) funded by the Ministry of Science and ICT (MSIT), Republic of Korea.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jousilahti P, Salomaa V, Hakala K, et al. The association of sensitive systemic inflammation markers with bronchial asthma. Ann Allergy Asthma Immunol. 2002;89(4):381–385. doi:10.1016/S1081-1206(10)62039-X
2. Girdhar A, Kumar V, Singh A, et al. Systemic inflammation and its response to treatment in patients with asthma. Respir Care. 2011;56(6):800–805. doi:10.4187/respcare.00601
3. Liang Z, Liu L, Zhao H, et al. A systemic inflammatory endotype of asthma with more severe disease identified by unbiased clustering of the serum cytokine profile. Medicine. 2016;95(25):e3774. doi:10.1097/MD.0000000000003774
4. Weiss G, Ganz T, Goodnough LT. Anemia of inflammation. Blood. 2019;133:40–50. doi:10.1182/blood-2018-06-856500
5. Armitage AE, Eddowes LA, Gileadi U, et al. Hepcidin regulation by innate immune and infectious stimuli. Blood. 2011;118:4129–4139. doi:10.1182/blood-2011-04-351957
6. Nemeth E, Valore EV, Territo M, et al. Hepcidin, a putative mediator of anemia of inflammation, is a type II acute-phase protein. Blood. 2003;101(7):2461–2463. doi:10.1182/blood-2002-10-3235
7. Theurl I, Mattle V, Seifert M, et al. Dysregulated monocyte iron homeostasis and erythropoietin formation in patients with anemia of chronic disease. Blood. 2006;107:4142–4148. doi:10.1182/blood-2005-08-3364
8. Boutou AK, Pitsiou GG, Stanopoulos I, et al. Levels of inflammatory mediators in chronic obstructive pulmonary disease patients with anemia of chronic disease: a case-control study. QJM. 2012;105(7):657–663. doi:10.1093/qjmed/hcs024
9. Hohaus S, Massini G, Giachelia M, et al. Anemia in hodgkin’s lymphoma: the role of interleukin-6 and hepcidin. J Clin Oncol. 2010;28(15):2538–2543. doi:10.1200/JCO.2009.27.6873
10. Falkensammer CE, Thurnher M, Leonhartsberger N, et al. C-reactive protein is a strong predictor for anaemia in renal cell carcinoma: role of IL-6 in overall survival. BJU Int. 2011;1072:1893–1898. doi:10.1111/j.1464-410X.2010.09817.x
11. Jankowska EA, Rozentryt P, Witkowska A, et al. Iron deficiency: an ominous sign in patients with systolic chronic heart failure. Eur Heart J. 2010;31:1872–1880. doi:10.1093/eurheartj/ehq158
12. Drury KE, Schaeffer M, Silverberg JI. Association between atopic disease and anemia in US children. JAMA Pediatr. 2016;170(1):29–34. doi:10.1001/jamapediatrics.2015.3065
13. Rhew K, Brown JD, Oh JM. Atopic disease and anemia in Korean patients: cross-sectional study with propensity score analysis. Int J Environ Res Public Health. 2020;17(6):1978. doi:10.3390/ijerph17061978
14. Rhew K, Oh JM. Association between atopic disease and anemia in pediatrics: a cross-sectional study. BMC Pediatr. 2019;19(1):455. doi:10.1186/s12887-019-1836-5
15. Chang J-E, Lee H-M, Kim J, et al. Prevalence of anemia in pediatric patients according to asthma control: propensity score analysis. J Asthma Allergy. 2021;14:743–751. doi:10.2147/JAA.S318641
16. Ricciardolo FLM, Sorbello V, Folino A, et al. Identification of IL-17F/frequent exacerbator endotype in asthma. J Allergy Clin Immunol. 2017;140:395–406. doi:10.1016/j.jaci.2016.10.034
17. Turan N, Edwards MJ, Bates S, et al. IL-6 pathway upregulation in subgroup of severe asthma is associated with neutrophilia and poor lung function. Clin Exp Allergy. 2018;48:475–478. doi:10.1111/cea.13085
18. Raundhal M, Morse C, Khare A, et al. High IFN-γ and low SLPI mark severe asthma in mice and humans. J Clin Invest. 2015;125(8):3037–3050. doi:10.1172/JCI80911
19. Kim RY, Pinkerton JW, Essilfie AT, et al. Role for NLRP3 inflammasome-mediated, IL-1β-dependent responses in severe, steroid-resistant asthma. Am J Respir Crit Care Med. 2017;196:283–297. doi:10.1164/rccm.201609-1830OC
20. Vroman H, Bergen IM, van Hulst JAC, et al. TNF-α-induced protein 3 levels in lung dendritic cells instruct TH2 or TH17 cell differentiation in eosinophilic or neutrophilic asthma. J Allergy Clin Immunol. 2018;141:1620–1633. doi:10.1016/j.jaci.2017.08.012
21. Lachowicz-Scroggins ME, Dunican EM, Charbit AR, et al. Extracellular DNA, neutrophil extracellular traps, and inflammasome activation in severe asthma. Am J Respir Crit Care Med. 2019;199:1076–1085. doi:10.1164/rccm.201810-1869OC
22. Cooper AC, Mikhail A, Lethbridge MW, et al. Increased expression of erythropoiesis inhibiting cytokines (IFN-γ, TNF-α, IL-10, and IL-13) by T cells in patients exhibiting a poor response to erythropoietin therapy. J Am Soc Nephrol. 2003;14(7):1776–1784. doi:10.1097/01.ASN.0000071514.36428.61
23. Cavallaro F, Duca L, Pisani LF, et al. Anti-TNF-mediated modulation of prohepcidin improves iron availability in inflammatory bowel disease, in an IL-6-mediated fashion. Can J Gastroenterol Hepatol. 2017;2017:6843976. doi:10.1155/2017/6843976
24. Nemeth E, Rivera S, Gabayan V, et al. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest. 2004;113:1271–1276. doi:10.1172/JCI200420945
25. Markoulaki D, Kostikas K, Papatheodorou G, et al. Hemoglobin, erythropoietin and systemic inflammation in exacerbations of chronic obstructive pulmonary disease. Eur J Intern Med. 2011;22:103–107. doi:10.1016/j.ejim.2010.07.010
26. Panichi V, Migliori M, De Pietro S, et al. C reactive protein in patients with chronic renal diseases. Ren Fail. 2001;23:551–562. doi:10.1081/JDI-100104737
27. Bemelmans MH, Gouma DJ, Buurman WA. Influence of nephrectomy on tumor necrosis factor clearance in a murine model. J Immunol. 1993;150:2007–2017.
28. Abdel-Khalek MA, El-Barbary AM, Essa SA, et al. Serum hepcidin: a direct link between anemia of inflammation and coronary artery atherosclerosis in patients with rheumatoid arthritis. J Rheumatol. 2011;38:2153–2159. doi:10.3899/jrheum.110339
29. Chen Y, Xu W, Yang H, et al. Serum levels of hepcidin in rheumatoid arthritis and its correlation with disease activity and anemia: a meta-analysis. Immunol Invest. 2021;50(2–3):243–258. doi:10.1080/08820139.2020.1742731
30. Winn NC, Volk KM, Hasty AH. Regulation of tissue iron homeostasis: the macrophage “ferrostat”. JCI Insight. 2020;5(2):e132964. doi:10.1172/jci.insight.132964
31. Roth-Walter F. Iron-deficiency in atopic diseases: innate immune priming by allergens and siderophores. Front Allergy. 2022;3:859922. doi:10.3389/falgy.2022.859922
32. Petje LM, Jensen SA, Szikora S, et al. Functional iron-deficiency in women with allergic rhinitis is associated with symptoms after nasal provocation and lack of iron-sequestering microbes. Allergy. 2021;76(9):2882–2886. doi:10.1111/all.14960
33. Nairz M, Weiss G. Iron in infection and immunity. Mol Aspects Med. 2020;75:100864. doi:10.1016/j.mam.2020.100864
34. Shaheen SO, Gissler M, Devereux G, et al. Maternal iron supplementation in pregnancy and asthma in the offspring: follow-up of a randomised trial in Finland. Eur Respir J. 2020;55(6):1902335. doi:10.1183/13993003.02335-2019
35. Collins AJ, Li S, Gilbertson DT, et al. Chronic kidney disease and cardiovascular disease in the medicare population. Kidney Int Suppl. 2003;87:S24–S31. doi:10.1046/j.1523-1755.64.s87.5.x
36. Sarnak MJ, Tighiouart H, Manjunath G, et al. Anemia as a risk factor for cardiovascular disease in The Atherosclerosis Risk in Communities (ARIC) study. J Am Coll Cardiol. 2002;40:27–33. doi:10.1016/S0735-1097(02)01938-1
37. Wouters HJCM, van der Klauw MM, de Witte T, et al. Association of anemia with health-related quality of life and survival: a large population-based cohort study. Haematologica. 2019;104:468–476. doi:10.3324/haematol.2018.195552
38. Engelkes M, de Ridder MA, Svensson E, et al. Multinational cohort study of mortality in patients with asthma and severe asthma. Respir Med. 2020;165:105919. doi:10.1016/j.rmed.2020.105919
39. To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey [published correction appears in BMC Public Health. 2021 Oct 8;21(1):1809]. BMC Public Health. 2012;12:204. doi:10.1186/1471-2458-12-204
40. Ganz T. Anemia of Inflammation. N Engl J Med. 2019;381:1148–1157. doi:10.1056/NEJMra1804281
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Potential of the Advanced Lung Cancer Inflammation Index as a Risk Marker for Asthma-Chronic Obstructive Pulmonary Disease Overlap Syndrome and COPD: Evidence from NHANES 2007-2018
Chen N, Liu Y, Wang Q, Wang M, Wang J, Chen W
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:905-917
Published Date: 31 March 2025
The Associations of Anaemia Status and Body Mass Index with Asthma Severity in Saudi Arabia: A Comparative Study
Bugis AA, Bugis B, Alzahrani A, Alamri AH, Almalki HH, Alshehri JH, Alqarni AA, Turkestani FA
Journal of Asthma and Allergy 2025, 18:927-940
Published Date: 5 June 2025
IL-17A as a Key Mediator of Pulmonary-Intestinal Immune Interactions in a Mouse Model of Asthma and Colitis
Wu C, Hu X, Mo Z, Meng Y, Du Y, Duan Y, Zeng Z, Shan J, Li J, Zhang N, Ma Y, Wang H, Liu C, Zhang G, Foster PS, Xu H, Li F, Yang M
Journal of Inflammation Research 2025, 18:8199-8216
Published Date: 21 June 2025
TIM-4 Regulates Allergic Airway Inflammation and Mast Cell Activation by Binding to CD300b
Tanabe Y, Kamachi F, Ito J, Harada N, Harada S, Makino F, Abe Y, Nakano N, Izawa K, Niyonsaba F, Nishiyama C, Kitaura J, Okumura K, Takahashi K, Akiba H, Miyake S
Journal of Asthma and Allergy 2025, 18:1477-1492
Published Date: 1 November 2025
Long-Acting Muscarinic Antagonists for the Treatment of Difficult-to-Treat and Severe Asthma: A Narrative Review Focusing on Inflammation from Bench to Bedside
Calzetta L, Manzetti GM, Pistocchini E, Lauro RF, Gholamalishahi S, Cazzola M, Rogliani P
Journal of Inflammation Research 2026, 19:552261
Published Date: 14 March 2026