")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
In-Hospital Mortality Prediction Model for Critically Ill Older Adult Patients Transferred from the Emergency Department to the Intensive Care Unit
Received 26 October 2023
Accepted for publication 15 November 2023
Published 22 November 2023 Volume 2023:16 Pages 2555—2563
DOI https://doi.org/10.2147/RMHP.S442138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Yan Lu, Chaoxiang Ren, Chaolong Wu
Clinical Laboratory, Affiliated Dongyang Hospital of Wenzhou Medical University, Dongyang, Zhejiang, 322100, People’s Republic of China
Correspondence: Yan Lu, Clinical Laboratory, Affiliated Dongyang Hospital of Wenzhou Medical University, 60 West Wuning Road, Dongyang, Zhejiang, 322100, People’s Republic of China, Tel +86 18367815795, Email [email protected]
Purpose: Studies on the prognosis of critically ill older adult patients admitted to the emergency department (ED) but requiring immediate admission to the intensive care unit (ICU) remain limited. This study aimed to develop an in-hospital mortality prediction model for critically ill older adult patients transferred from the ED to the ICU.
Patients and Methods: The training cohort was taken from the Medical Information Mart for Intensive Care IV (version 2.2) database, and the external validation cohort was taken from the Affiliated Dongyang Hospital of Wenzhou Medical University. In the training cohort, class balance was addressed using Random Over Sampling Examples (ROSE). Univariate and multivariate Cox regression analyses were performed to identify independent risk factors. These were then integrated into the predictive nomogram. In the validation cohort, the predictive performance of the nomogram was evaluated using the area under the curve (AUC) of the receiver operating characteristic curve, calibration curve, clinical utility decision curve analysis (DCA), and clinical impact curve (CIC).
Results: In the ROSE-balanced training cohort, univariate and multivariate Cox regression analysis identified that age, sex, Glasgow coma scale score, malignant cancer, sepsis, use of mechanical ventilation, use of vasoactive agents, white blood cells, potassium, and creatinine were independent predictors of in-hospital mortality in critically ill older adult patients, and were included in the nomogram. The nomogram showed good predictive performance in the ROSE-balanced training cohort (AUC [95% confidence interval]: 0.792 [0.783– 0.801]) and validation cohort (AUC [95% confidence interval]: 0.780 [0.727– 0.834]). The calibration curves were well-fitted. DCA and CIC demonstrated that the nomogram has good clinical application value.
Conclusion: This study developed a predictive model for early prediction of in-hospital mortality in critically ill older adult patients transferred from the ED to the ICU, which was validated by external data and has good predictive performance.
Keywords: nomogram, Medical Information Mart for Intensive Care IV database, random over sampling examples, external validation, prognosis
Introduction
Patients presenting to the emergency department (ED) are heterogeneous, and the severity of their clinical symptoms determines whether they need to receive further care.1,2 If patients require a transfer from the ED to the intensive care unit (ICU), this indicates that they have life-threatening organ dysfunction or have a risk of death.3 Critically ill older adult patients who are admitted to the ED usually require emergency treatment and monitoring due to emergencies such as acute diseases, trauma, and cardiovascular and cerebrovascular events. Therefore, significant instability and severe physiological dysfunction may have already occurred at the time of admission.4,5 As the population ages, the number of critically ill older adult patients seeking treatment in the ED is rapidly increasing.6,7 Because older adult patients often have chronic diseases and organ dysfunction, they tend to have a poor prognosis.8 Therefore, the care of critically ill older adult patients is challenging. Establishing early prognosis prediction to identify high-risk critically ill older adult patients is conducive to maximum rational allocation of medical resources and early discussion of end-of-life issues with the patient’s family, if necessary.9 However, the ED is a high-need but resource-limited department,10 and comprehensive disease assessment and diagnosis have not yet been conducted. Therefore, early prognosis prediction after entering the ICU is crucial.
In past studies, many prognostic prediction models have been established for critically ill older adult patients. For example, mortality prediction models have been proposed for older adult patients with severe community acquired pneumonia,11 older adult patients with ischemic stroke,12 and older adult patients with hip fractures.13 However, there is still limited research on critically ill older adult patients transferred from the ED to the ICU.
In this study, we used data from the Medical Information Mart for Intensive Care IV (MIMIC-IV version 2.2) to build an in-hospital mortality prediction model for critically ill older adult patients transferred from the ED to the ICU, and validated this model with an external dataset from the Affiliated Dongyang Hospital of Wenzhou Medical University.
Materials and Methods
Training Cohort
The patient data for the training cohort was sourced from the MIMIC-IV version 2.2 database.14 The MIMIC-IV database contains de-identified clinical information related to patients admitted to the ICU or ED between 2008 and 2019. This database was reviewed and approved by the Institutional Review Committee of the Beth Israel Deaconess Medical Center. Since this was a retrospective collection of medical data, all patient data were de-identified, and the study did not guide patient diagnosis and treatment; the need for informed consent was waived. One author (Lu) carefully studied the relevant training courses and obtained permission for their use according to the database use agreement (license number: 35953547).
In this study, we included patients admitted from the ED and screened them based on the following exclusion criteria: (1) patients with > 30% missing data, (2) duplicate transfer data except for detailed information on the patient’s first transfer from the ED to the ICU, (3) patients aged ≤ 65 years old, and (4) patients transferred to the ICU more than 24 hours after admission.
External Validation Cohort
The external validation cohort included patients from the Affiliated Dongyang Hospital of Wenzhou Medical University from 2016 to 2023. The exclusion criteria were the same as those for the training cohort. This study was reviewed and approved by the Ethics Committee of the Affiliated Dongyang Hospital of Wenzhou Medical University. As this was a retrospective clinical data analysis, the necessity of informed consent was waived by the ethics committee.
Data Extraction
We used Postgre SQL software to obtain raw data from the MIMIC-IV database using a structured query language. The extracted data included patient demographics, comorbidities (malignant cancer and sepsis), medical treatment and laboratory parameters within the first 24 hours, Glasgow coma scale (GCS) score, patient survival status, and survival time. Medical treatment included mechanical ventilation and vasoactive agents. The laboratory parameters extracted were the first detection values within the first 24 hours, including white blood cells (WBC), hemoglobin, platelets, sodium, chloride, potassium, creatinine, and international normalized ratio. Variables with ≥ 25% missing values were excluded (ratio of missing data for excluded variables: albumin 74.1%, bilirubin 61.4%, lactate 58.7%, prothrombin time 25.2%, partial thromboplastin time 27.5%).
The extracted outcome variable was the all-cause in-hospital mortality of critically ill older adult patients.
Statistical Analysis
The Stata software (version 14.0; Stata Corp., College Station, TX, USA) and R software version 4.2.0 (http://www.r-project.org/) was used for statistical analysis and data visualization.
Continuous variables are expressed as mean ± standard deviation or median [interquartile range (IQR)] according to the normality of their distribution. Categorical variables are expressed as numbers (percentages). Differences in the distribution of continuous variables between the two cohorts were compared using the Student’s t-test or Wilcoxon test. Categorical variables were compared between the groups using the χ2 test. When variables had missing values and the percentage of missing values was < 25%, the missing values were processed by multiple interpolation using the “mice” package in R software.15
The training cohort was used to build a prediction model. The outcome variable is binary, and the incidence of negative events is higher than that of positive events. When the incidence of negative events is five times higher than that of positive events, it is considered to have a significant class imbalance. Class imbalance leads to overfitting issues in the obtained classification model, and accuracy and robustness is also affected.16 Therefore, class imbalance was addressed using Random Over-Sampling Examples (ROSE). ROSE produces a sample of synthetic data by enlarging the features space of minority and majority class examples. The “ROSE” package in R language can generate synthetic data based on sampling and smooth bootstrap methods.17 Univariate and multivariate Cox regression analyses were used to screen candidate variables. The final statistically significant variables (P < 0.05) were considered independent predictors and were used to build the prediction models. A visualized nomogram model was built using the “rms” package in R software.
The external validation cohort was used to evaluate the performance of the predictive model. Calibration plots with resampling of 1000 bootstraps were plotted to assess the accuracy of the nomogram model. In addition, the receiver operating characteristic (ROC) curve, clinical utility decision curve analysis (DCA), and clinical impact curve (CIC) were plotted to demonstrate the clinical utility of the nomogram model.
Results
As shown in Figure 1, according to the screening criteria, a total of 10,233 critically ill older adult patients transferred from the ED to the ICU were selected from the MIMIC-IV database as the training cohort, and a total of 277 critically ill older adult patients admitted to Affiliated Dongyang Hospital of Wenzhou Medical University were selected as the external validation cohort.
 |
Figure 1 Screening process of the study population. Abbreviation: ROSE, Random Over-Sampling Examples. |
Construction of the Prediction Model
As shown in Supplemental Table 1, the in-hospital mortality rate of the patients in the original training cohort was 17.7%, with a significant class imbalance. Table 1 shows the characteristics of the ROSE-balanced training cohort, where class imbalance was eliminated and the numbers of survivors and non-survivors were 5160 and 5073, respectively. In the ROSE-balanced training cohort, univariate and multivariate Cox regression analyses were performed to identify independent risk factors. The results showed that age, sex, GCS score, malignant cancer, use of mechanical ventilation, use of vasoactive agents, WBC, potassium, and creatinine were independent predictors of in-hospital mortality in critically ill older adult patients (Table 2). According to the results of multivariate Cox regression analysis, we constructed a nomogram to predict the in-hospital mortality of critically-ill older adult patients who needed to be transferred from ED to ICU (Figure 2).
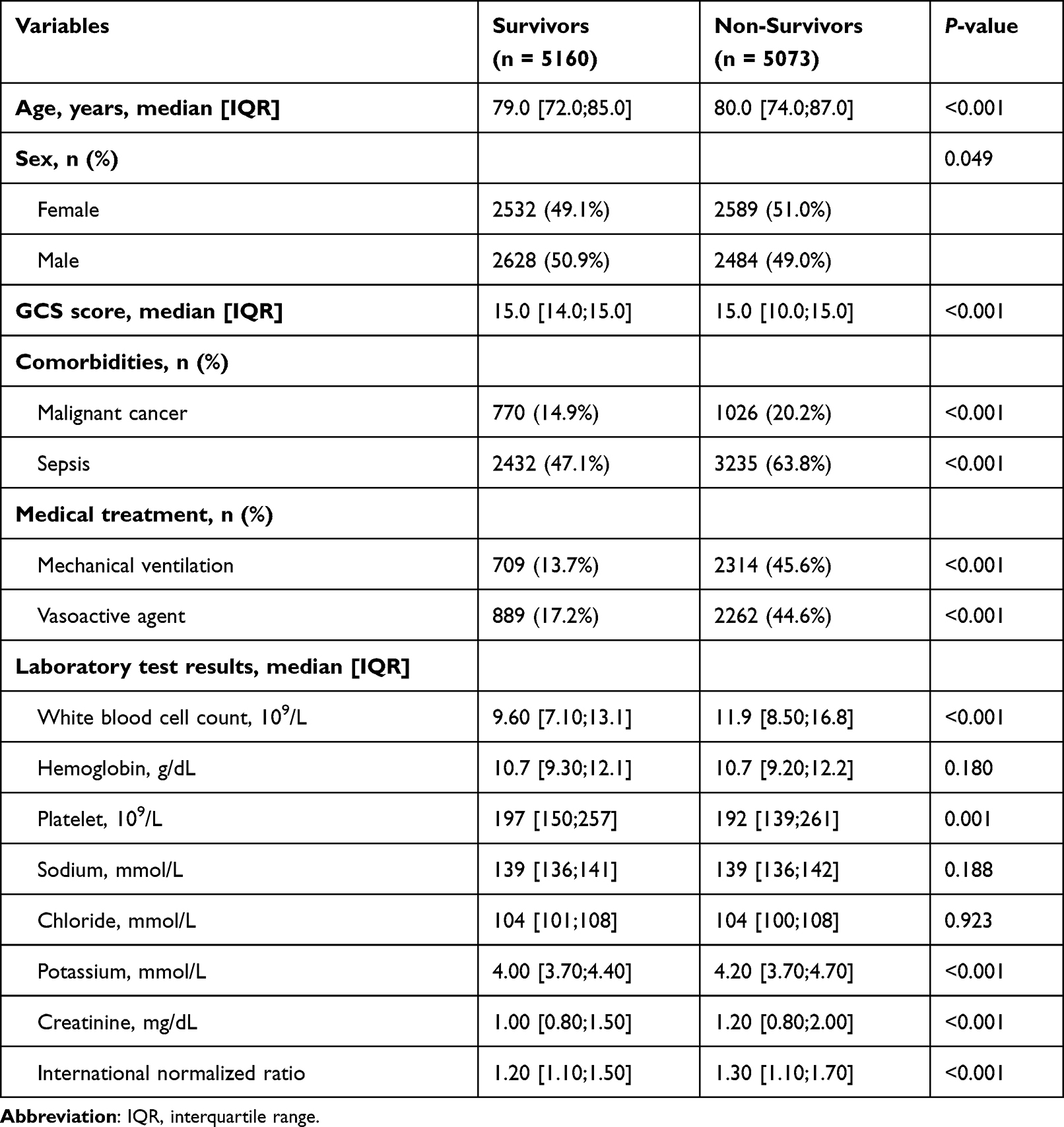 |
Table 1 Characteristics of the ROSE-Balanced Training Cohort Used for Constructing Prediction Models |
 |
Table 2 Univariate and Multivariate Analysis of in-Hospital Mortality of Critically Ill Older Adult Patients in ROSE-Balanced Training Cohort |
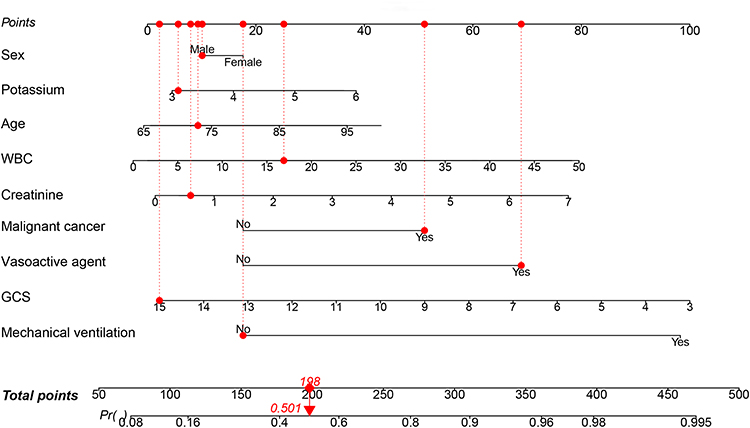 |
Figure 2 A nomograph for predicting the in-hospital mortality of critically ill older adult patients who transferred from ED to ICU. When using, draw a vertical line up from each variable to the “point” axis, and then record the corresponding point. Then the total score is obtained by adding each variable corresponding to the in-hospital mortality predicted by the nomogram. Abbreviations: WBC, white blood cells; GCS, Glasgow coma scale. |
Validation of the Prediction Model
In the ROSE-balanced training cohort, the nomogram showed good predictive performance (Figure 3). The AUC [95% confidence interval (95% CI)], sensitivity, specificity, positive predictive value, and negative predictive value of the training cohort were 0.792 [0.783–0.801], 0.803, 0.670, 0.705, and 0.775, respectively. The calibration curve shows the accuracy of the nomogram in predicting prognosis, and the good consistency of results demonstrate that there is no significant deviation between the model’s predicted value and the actual value. The DCA and CIC demonstrate that this model improves patient outcomes and has clinical application value.
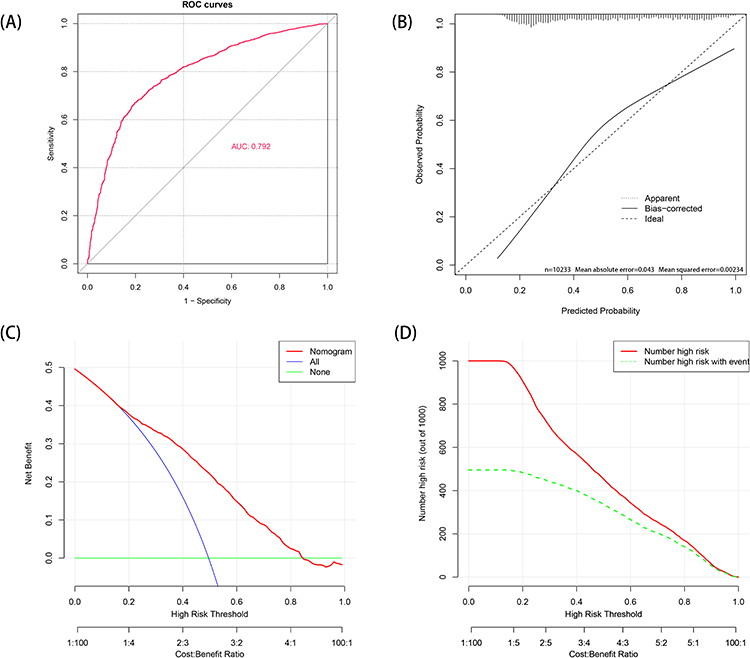 |
Figure 3 Performance evaluation of the model in the ROSE-balanced training cohort. (A) Receiver operating characteristic curve to assess the ability of the nomogram to predict in-hospital mortality. (B) Calibration curves of the nomogram model. (C) Decision curve analysis of the nomogram model. The x-axis represents the threshold probability, which is the minimum predicted probability for clinical intervention. The y-axis represents net benefit. When the net benefit of nomogram is higher than that of treat-none and treat-all under the same threshold probability, it indicates that nomogram improves patient outcomes. (D) Clinical impact curve of the nomogram model. Using the nomogram model to predict risk stratification for 1000 individuals. The red curve (number of high risk) represents the number of people classified as positive (high risk) by the nomogram model at each threshold probability. The green curve (number of high risk with event) represents the number of people who are truly positive at each threshold probability. |
In addition, the prediction model was validated using the external validation cohort. The predictive variables of patients in the external validation cohort are shown in Supplementary Table 2. The AUC [95% CI], sensitivity, specificity, positive predictive value, and negative predictive value of the external validation cohort were 0.780 [0.727–0.834]), 0.805, 0.639, 0.673, and 0.780, respectively (Figure 4A). In addition, the calibration curve (Figure 4B) shows that the model fits well. The DCA and CIC demonstrate that the predictive model has good clinical application value (Figure 4C and D).
 |
Figure 4 Performance evaluation of the model in the validation cohort. (A) Receiver operating characteristic to assess the ability of nomogram to predict in-hospital mortality. (B) Calibration curves of the nomogram model. (C) Decision curve analysis of the nomogram model. (D) Clinical impact curve of the nomogram model. |
Discussion
In this retrospective study, we developed a predictive model for in-hospital mortality of critically ill older adult patients who need to transfer from ED to ICU using a large publicly available MIMIC-IV database, and conducted external validation using patient data from the Affiliated Dongyang Hospital of Wenzhou Medical University. This study identified age, sex, GCS score, malignant cancer, use of mechanical ventilation, use of vasoactive agents, WBC, potassium, and creatinine as independent predictors of in-hospital mortality in critically ill older adult patients, which were then used to construct a nomogram model. Based on the performance evaluation, we found that the nomogram model has good predictive performance and clinical application value.
The ED is one of the main sources of critically ill patients in the ICU. The transfer of older adult patients from the ED to the ICU results in a marked dramatic decline in health status.18 Studies have found that the challenge of caring for most critically ill older adult patients is not just to prolong survival time, but to reduce unanticipated mortality.19–21 In addition, with limited resources in the ICU, age may become an important discriminatory factor, and older adult patients are more likely to give up active treatment.6,22 Therefore, different prognostic tools should be used for critically ill older adult and young patients. Moreover, early prognostic assessment of critically ill patients can help reduce the impact on subsequent medical decisions.23
Most previous studies on the prognosis of patients admitted to the ED have included hospital mortality and the occurrence of critical illness as joint outcomes. Goodacre et al included age, diagnostic code, malignant tumor, vital signs, and laboratory test results in a prediction model for 7-day mortality in patients admitted to the ED.24 Busch et al predicted the short- and long-term mortality of patients based on age, vital signs, mobility, and physician assessment.25 However, these studies were conducted on unselected emergency patients, therefore the in-hospital mortality rate was < 10%, which may have affected the reliability of the results. Severe sample imbalance issues can lead to a decrease in the accuracy of the model, thereby affecting the reliability of the prediction model.26,27 In addition, due to the limited resources and time of the ED, there may be execution pressure to select predictive factors obtained during the ED period (eg, detailed physical examination and adequate laboratory testing). The strength of this study is the development of a predictive model for in-hospital mortality in critically ill older adult patients requiring transfer to the ICU, based on a large sample from publicly available databases and an external validation dataset. In addition, prediction variables within the prediction model are easily available within the first 24 hours of entering the ICU. Furthermore, the apparent class imbalance in the data was handled using ROSE, which has been shown in many previous studies to improve the model.28,29
Nevertheless, our study has some limitations. First, all patient data for the study were obtained from the medical center and the electronic health record system in a retrospective manner. Some variables that could not be included due to an excessive number of missing values, such as lactate and albumin, may be significant. Therefore, further validation is needed through prospective research. Secondly, older adult patients admitted to the emergency department are often delirious, which poses certain difficulties in obtaining baseline medical conditions before admission. Finally, the study considered only critically-ill older adult patients who died in the hospital after admission to the ICU, and did not consider those who were less critically ill and did not require ICU admission, or who died without ICU admission or immediately after discharge.
Conclusion
In this retrospective analysis of critically-ill older adult patients who needed to be transferred from the ED to the ICU, factors of age, sex, GCS score, malignant cancer, use of mechanical ventilation, use of vasoactive agents, WBC, potassium, and creatinine were considered independent risk factors for in-hospital mortality of critically-ill older adult patients and were used to construct a nomogram model. The nomogram model was shown to have good predictive performance using the external validation cohort.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Yang C, Yang TT, Tsou YJ, et al. Initiating palliative care consultation for acute critically ill patients in the emergency department intensive care unit. J Chin Med Assoc. 2020;83(5):500–506. doi:10.1097/JCMA.0000000000000297
2. Chang JC, Yang C, Lai LL, Huang HH, Tsai SH. Differences in characteristics, hospital care, and outcomes between acute critically Ill emergency department patients Receiving palliative care and usual care. Int J Environ Res Public Health. 2021;18(23):12546. doi:10.3390/ijerph182312546
3. García-Gigorro R, Dominguez Aguado H, Barea Mendoza JA, Viejo Moreno R, Sánchez Izquierdo JA, Montejo-González JC. Short- and long-term prognosis of critically-ill patients referred to the ICU from the emergency department of a tertiary hospital. Med Clin (Barc). 2017;148(5):197–203. doi:10.1016/j.medcli.2016.10.037
4. Kao CC, Chen YC, Huang HH, Hsu TF, Yen DH, Fan JS. Prognostic significance of emergency department modified early warning score trend in critical ill elderly patients. Am J Emerg Med. 2021;44:14–19. doi:10.1016/j.ajem.2021.01.047
5. McDowald K, Direktor S, Hynes EA, Sahadeo A, Rogers ME. Effectiveness of collaboration between emergency department and intensive care unit teams on mortality rates of patients presenting with critical illness: a systematic review. JBI Database Syst Rev Implement Rep. 2017;15(9):2365–2389. doi:10.11124/JBISRIR-2017-003365
6. Akinosoglou K, Schinas G, Almyroudi MP, Gogos C, Dimopoulos G. The impact of age on intensive care. Ageing Res Rev. 2023;84:101832. doi:10.1016/j.arr.2022.101832
7. Fan L, Xue H, Wang Q, Yan Y, Du W. Development and validation of a nomogram for predicting risk of emergency department revisits in Chinese older patients. Risk Manag Healthc Policy. 2022;15:2283–2295. doi:10.2147/RMHP.S391731
8. Brunker LB, Boncyk CS, Rengel KF, Hughes CG. Elderly patients and management in Intensive Care Units (ICU): clinical challenges. Clin Interv Aging. 2023;18:93–112. doi:10.2147/CIA.S365968
9. Ashana DC, Anesi GL, Liu VX, et al. Equitably allocating resources during crises: racial differences in mortality prediction models. Am J Respir Crit Care Med. 2021;204(2):178–186. doi:10.1164/rccm.202012-4383OC
10. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316
11. Song Y, Wang X, Lang K, et al. Development and validation of a nomogram for predicting 28-day mortality on admission in elderly patients with severe community-acquired pneumonia. J Inflamm Res. 2022;15:4149–4158. doi:10.2147/JIR.S369319
12. Jin G, Hu W, Zeng L, et al. Development and verification of a nomogram for predicting short-term mortality in elderly ischemic stroke populations. Sci Rep. 2023;13(1):12580. doi:10.1038/s41598-023-39781-4
13. Chen Q, Hao P, Wong C, Zhong X, He Q, Chen Y. Development and validation of a novel nomogram of 1-year mortality in the elderly with hip fracture: a study of the MIMIC-III database. BMJ open. 2023;13(5):e068465. doi:10.1136/bmjopen-2022-068465
14. Johnson A, Bulgarelli L, Pollard T, Horng S, Celi LA, Mark R. MIMIC-IV (version 2.2). PhysioNet. 2023.
15. Zhang Z. Multiple imputation with multivariate imputation by chained equation (MICE) package. Ann Transl Med. 2016;4(2):30. doi:10.3978/j.issn.2305-5839.2015.12.63
16. Blagus R, Lusa L. Class prediction for high-dimensional class-imbalanced data. BMC Bioinform. 2010;11(1):523. doi:10.1186/1471-2105-11-523
17. Hashimoto-Roth E, Surendra A, Lavallée-Adam M, Bennett SAL, Čuperlović-culf M. METAbolomics data Balancing with Over-sampling Algorithms (META-BOA): an online resource for addressing class imbalance. Bioinformatics. 2022;38(23):5326–5327. doi:10.1093/bioinformatics/btac649
18. Ouchi K, George N, Schuur JD, et al. Goals-of-care conversations for older adults with serious illness in the emergency department: challenges and opportunities. Ann Emerg Med. 2019;74(2):276–284. doi:10.1016/j.annemergmed.2019.01.003
19. O’Connor AE, Winch S, Lukin W, Parker M. Emergency medicine and futile care: taking the road less travelled. Emerg Med Australas. 2011;23(5):640–643. doi:10.1111/j.1742-6723.2011.01435.x
20. Ouchi K, Strout T, Haydar S, et al. Association of emergency clinicians’ assessment of mortality risk with actual 1-month mortality among Older adults admitted to the hospital. JAMA Netw Open. 2019;2(9):e1911139. doi:10.1001/jamanetworkopen.2019.11139
21. Gao Z, Qi X, Zhang X, et al. Developing and validating an emergency triage model using machine learning algorithms with medical big data. Risk Manag Healthc Policy. 2022;15:1545–1551. doi:10.2147/RMHP.S355176
22. Mukhopadhyay A, Tai BC, See KC, et al. Risk factors for hospital and long-term mortality of critically ill elderly patients admitted to an intensive care unit. Biomed Res Int. 2014;2014:960575. doi:10.1155/2014/960575
23. Jesus JE, Marshall KD, Kraus CK, Derse AR, Baker EF, McGreevy J. Should emergency department patients with end-of-life directives be admitted to the ICU? J Emerg Med. 2018;55(3):435–440. doi:10.1016/j.jemermed.2018.06.009
24. Goodacre S, Wilson R, Shephard N, Nicholl J. Derivation and validation of a risk adjustment model for predicting seven day mortality in emergency medical admissions: mixed prospective and retrospective cohort study. BMJ. 2012;344:e2904. doi:10.1136/bmj.e2904
25. Busch JM, Arnold I, Kellett J, Brabrand M, Bingisser R, Nickel CH. Validation of a simple score for mortality prediction in a cohort of unselected emergency patients. Int J Clin Pract. 2022;2022:7281693. doi:10.1155/2022/7281693
26. Liu ZT, Wu BH, Li DY, Xiao P, Mao JW. Speech emotion recognition based on selective interpolation synthetic minority over-sampling technique in small sample environment. Sensors. 2020;20(8). doi:10.3390/s20082297
27. Yang K, Li J, Gao H. The impact of sample imbalance on identifying differentially expressed genes. BMC Bioinform. 2006;7(Suppl 4):S8. doi:10.1186/1471-2105-7-S4-S8
28. Zhang J, Chen L. Clustering-based undersampling with random over sampling examples and support vector machine for imbalanced classification of breast cancer diagnosis. Comput Assist Surg. 2019;24(sup2):62–72.
29. Alshakhs F, Alharthi H, Aslam N, Khan IU, Elasheri M. Predicting postoperative length of stay for isolated coronary artery bypass graft patients using machine learning. Int J Gen Med. 2020;13:751–762. doi:10.2147/IJGM.S250334
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.