Back to Journals » Journal of Pain Research » Volume 16
Improving Access to Care for Patients Taking Opioids for Chronic Pain: Recommendations from a Modified Delphi Panel in Michigan
Authors Kehne A, Bernstein SJ ![]() , Thomas J, Bicket MC
, Thomas J, Bicket MC ![]() , Bohnert ASB, Madden EF, Powell VD, Lagisetty P
, Bohnert ASB, Madden EF, Powell VD, Lagisetty P
Received 14 March 2023
Accepted for publication 20 June 2023
Published 10 July 2023 Volume 2023:16 Pages 2321—2330
DOI https://doi.org/10.2147/JPR.S406034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Supplementary video 1 of "Access to care for patients taking opioids for chronic pain" [ID 406034].
Views: 276
Adrianne Kehne,1,2 Steven J Bernstein,1– 3 Jennifer Thomas,1 Mark C Bicket,3,4,* Amy SB Bohnert,2– 4,* Erin Fanning Madden,5,* Victoria D Powell,6,7,* Pooja Lagisetty1– 3
1Division of General Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, MI, USA; 2Center for Clinical Management Research, VA Ann Arbor Healthcare System, Ann Arbor, MI, USA; 3Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor, MI, USA; 4Department of Anesthesiology, University of Michigan, Ann Arbor, MI, USA; 5Department of Family Medicine and Public Health Sciences, Wayne State University School of Medicine, Detroit, MI, USA; 6Palliative Care Program, Division of Geriatric and Palliative Medicine, Department of Internal Medicine, University of Michigan, Ann Arbor, MI, USA; 7Geriatrics Research, Education, and Clinical Center, LTC Charles S. Kettles VA Medical Center, Ann Arbor, MI, USA
*These authors contributed equally to this work
Correspondence: Adrianne Kehne, Division of General Internal Medicine, University of Michigan, 2800 Plymouth Road, Building 16, Floor 4, Ann Arbor, MI, 48109, USA, Tel +1 301 503 3936, Email [email protected]
Purpose: About 5– 8 million US patients take long-term opioid therapy for chronic pain. In the context of policies and guidelines instituted to reduce inappropriate opioid prescribing, abrupt discontinuations in opioid prescriptions have increased and many primary care clinics will not prescribe opioids for new patients, reducing access to care. This may result in uncontrolled pain and other negative outcomes, such as transition to illicit opioids. The objective of this study was to generate policy, intervention, and research recommendations to improve access to care for these patients.
Participants and Methods: We conducted a RAND/UCLA Modified Delphi, consisting of workshops, background videos and reading materials, and moderated web-based panel discussions held September 2020–January 2021. The panel consisted of 24 individuals from across Michigan, identified via expert nomination and snowball recruitment, including clinical providers, health science researchers, state-level policymakers and regulators, care coordination experts, patient advocates, payor representatives, and community and public health experts. The panel proposed intervention, policy, and research recommendations, scored the feasibility, impact, and importance of each on a 9-point scale, and ranked all recommendations by implementation priority.
Results: The panel produced 11 final recommendations across three themes: reimbursement reform, provider education, and reducing racial inequities in care. The 3 reimbursement-focused recommendations were highest ranked (theme average = 4.2/11), including the two top-ranked recommendations: increasing reimbursement for time needed to treat complex chronic pain (ranked #1/11) and bundling payment for multimodal pain care (#2/11). Four provider education recommendations ranked slightly lower (theme average = 6.2/11) and included clarifying the spectrum of opioid dependence and training providers on multimodal treatments. Four recommendations addressed racial inequities (theme average = 7.2/11), such as standardizing pain management protocols to reduce treatment disparities.
Conclusion: Panelists indicated reimbursement should incentivize traditionally lower-paying evidence-based pain care, but multiple strategies may be needed to meaningfully expand access.
Keywords: long-term opioid therapy, pain care access, reimbursement models, expert panel
Introduction
With drug-related overdose deaths steadily increasing over the past two decades, to a record 100,000 annual deaths in April 2021,1 there has been a concerted nationwide effort to limit opioid-related harms. To this end, guidelines, such as the 2016 Centers for Disease Control (CDC) prescribing guideline,2 have been disseminated, and subsequent state policies limiting dosages and durations3 have been instituted to reduce inappropriate opioid prescribing. While these policies have been associated with decreased prescribing,4 there is concern that they have also resulted in negative consequences for the estimated 5–8 million patients receiving opioid therapy for chronic pain,5 including limited access to primary care and specialty pain care.6–10 Recent secret shopper studies have found that approximately 40% of primary care clinics were unwilling to schedule a new primary care appointment for simulated patients seeking a provider to manage an existing opioid prescription,11,12 and that nearly a quarter of specialty pain clinics in the state of Michigan (23%) did not offer patients medication management.13 Moreover, 48% of these pain clinics did not accept Medicaid and 55% required a referral from a primary care provider, further limiting access to pain care for a patient population that struggles to access primary care.13 Inadequate access to both primary and specialty pain care could lead to abrupt discontinuation of opioid therapy and poorly controlled pain and opioid withdrawal,14 which could result in the use of non-prescribed opioids,15 unintentional overdoses,16,17 or even suicides.18,19
Providers have also expressed dissatisfaction with the current approach to caring for patients with chronic pain on prescribed opioids. Physicians note that primary care appointment times are insufficient to adequately counsel a patient taking opioids for complex pain, particularly given the associated administrative burdens, such as checking prescription drug monitoring programs and completing additional paperwork, such as opioid contracts.20 Providers also cite fear of liability as a disincentive against taking on patients who receive opioids for chronic pain.20 Limited knowledge regarding guideline-concordant care, particularly combined with poor care coordination, may further hinder the provision of high-quality care.21,22 Given the prevalence of chronic pain and opioid therapy, and the distress that limited treatment access can cause to both patients23 and providers,24 there is a need for policies, interventions, and additional research to improve access to care for this patient population and mitigate future harms.
To address this multifaceted issue, it is important to incorporate multiple perspectives in the generation of potential solutions. We therefore sought input from an expert panel of stakeholders with a wide range of backgrounds, including payors, primary and specialty pain care providers, patient advocates, researchers, and policymakers from across Michigan. Using the RAND/UCLA modified Delphi method,25 we tasked this panel with recommending policies, interventions, and areas where more research is needed to help improve access to care for individuals receiving opioid therapy for chronic pain.
Materials and Methods
Study Design
The study design followed a modified Delphi process, incorporating elements of the RAND/UCLA Appropriateness Method.25 The traditional Delphi process is used to compile a group response to questions that cannot be answered via experimental methods and consists of multiple rounds of anonymous surveys issued to a panel of experts, with summaries of the group’s responses provided to participants between rounds.25,26 This methodology is ideal for complex issues where there may be multiple stakeholders with potentially divergent or opposing interests and goals, and where responses could be influenced by participant response bias. Consistent with the RAND/UCLA Appropriateness method, we included a virtual face-to-face discussion of panelists’ viewpoints (hosted virtually due to the COVID-19 pandemic) between surveys. This modification removes some of the anonymity of the classic Delphi method but allows for a live discussion among panelists. This expert panel protocol was reviewed by the University of Michigan Institutional Review Board and deemed not regulated as human subject research.
Participant Recruitment
To assemble the expert panel, panelist nominations were solicited from collaborators, past state task forces, other researchers in Michigan, and candidate panelists themselves. Using this snowball recruitment approach, we emailed informational materials and invitations to a diverse group of stakeholders and experts from across the state, including patients, payors, state officials such as from the Department of Health and Human Services and the Department of Licensing and Regulatory Affairs, providers, and researchers. To ensure sufficient representation from all stakeholder groups, invitees who were unable to attend were asked to provide alternate recommendations. For the completion of all rounds, panelists were offered a $500 honorarium.
Process and Outcomes
Before convening the panel, we conducted an evidence synthesis on access to chronic pain care and long-term opioid therapy, excluding end-of-life and oncologic care. This review identified barriers to chronic pain treatment and existing efforts and strategies to address these barriers, drawing from national and state policies, insurer programs, reports from federal and state agencies, and the peer-reviewed literature around chronic pain, long-term opioid therapy, and other states of chronic opioid use, such as opioid use disorders. The evidence synthesis was presented to panelists in the form of two videos that reviewed both barriers to care (Supplementary Video 1, 45 minutes) and potential solutions (Supplementary Video 2, 30 minutes). The video format was chosen to limit reader fatigue and present information in a manner more accessible to stakeholders with varying levels of familiarity with health research methods.
The panel consisted of a preliminary pilot round, followed by two rounds of 60–90-minute virtual meetings and follow-up online surveys (see Supplementary Figure 1).
Pilot Round
Following review of the background videos, participants completed a pilot survey. The pilot survey solicited feedback on the comprehensiveness and validity of the background materials with both quantitative and open-ended questions, such as “what additional access barriers should we consider?”
Round 1
During the first virtual meeting, panelists participated in breakout groups of 4–5 panelists, moderated by experts in the field, to brainstorm preliminary recommendations. The panel was tasked with proposing intervention, policy, and research recommendations. Because the panel was comprised of patients, payors, state officials, providers, and researchers, they were not asked to produce clinical guidelines. These recommendations were then presented for consideration by the full panel. Panelists scored the feasibility, impact on patients’ access to care, and importance of each recommendation in the Round 1 Survey on a 9-point Likert scale (see Supplementary Table 1 for definitions). Scores of 1–3 defined as a low score, 4–6 a moderate score, and 7–9 a high score for each metric.25 Recommendations that received median importance scores <6 on the Round 1 Survey were eliminated from further consideration.
Round 2
Panelists reconvened in plenary for the second virtual meeting one month later, which was moderated by an expert on the Delphi process (SB) and a content expert (PL). Based on the Round 2 meeting, the research team reviewed the remaining recommendations for substantial overlap in their objectives and methods and consolidated redundant recommendations. These revised recommendations were then re-scored by the panel for their feasibility, impact, and importance, and panelists then generated a final ranking of recommendations in order of implementation priority.
Data Analysis
Panelists scored the recommendations on 9-item Likert scales for feasibility, impact, and importance twice, following both the Round 1 and Round 2 meetings. The final priority ranking of all recommendations was obtained using a two-part process following the Round 2 meeting: first, panelists were asked to group the recommendations into high-, moderate-, and low-priority tiers. Next, they were asked to provide more granular priority rankings of the recommendations within each tier (high, moderate, and low). This two-part process was utilized to reduce participant burden, as ranking all recommendations at once was deemed a more challenging task. In each panelist’s individual rankings, the highest-ranked recommendation was #1, the second ranked #2, and so on. The panelists’ individual priority rankings were then averaged to generate an overall final priority ranking of the recommendations, with lower numerical rankings corresponding to higher average priority.
Upon receipt of the final scores and rankings, the research team noted similarities in the objectives and mechanisms of the final recommendations and grouped them into thematic domains. To describe the relative prioritization of these thematic domains, the research team pooled all panelist rankings of all recommendations within each theme and averaged these rankings to produce a “theme average”. Lower ranking indicated higher priority.
Results
Participation and Demographics
Of 44 experts contacted, 24 agreed to participate in the panel, which consisted of 6 healthcare providers including physicians, a physician assistant, a pharmacist, and a social worker (25%), 4 researchers (17%), 4 policymakers and regulators (17%), 3 care coordination experts (13%), 3 patient advocates (13%), 2 payor representatives (8%), and 2 experts on community and public health (8%). Twenty panelists (80%) completed all rounds; one provider and three policymakers did not participate in the second-round survey. Panel demographics can be found in Table 1.
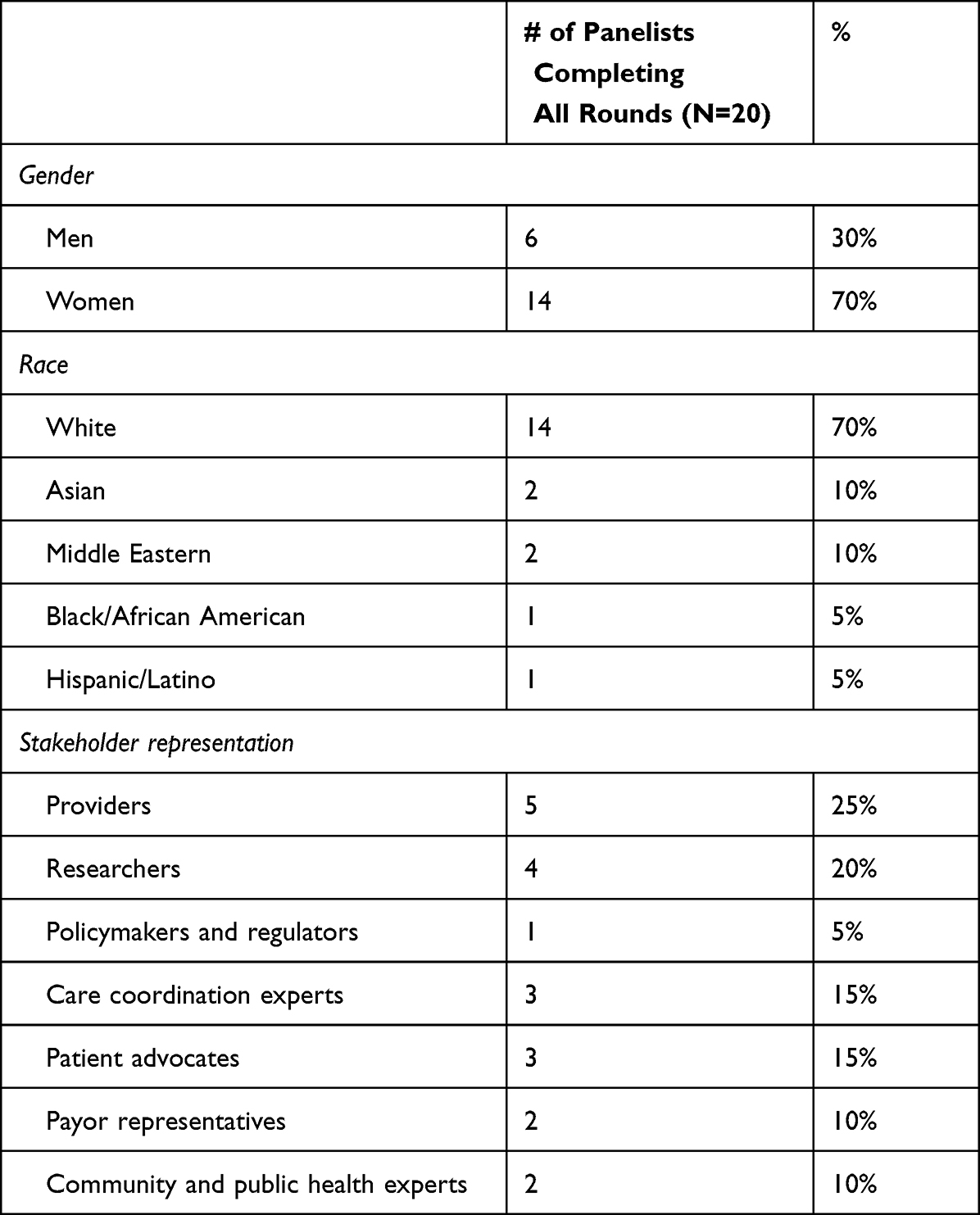 |
Table 1 Demographics of the Expert Panel |
Recommendations
The panel identified 11 final recommendations (Table 2; see Supplementary Table 2 for additional details and summaries of panelist discussion), with median scores on feasibility ranging from 5.5 to 7, impact from 5 to 8, and importance from 5.5 to 9. For these final recommendations, all median scores fell at or above the midpoint of the 9-point scoring scale (5), meaning that the panel considered them to be moderate to very feasible, impactful, and important.
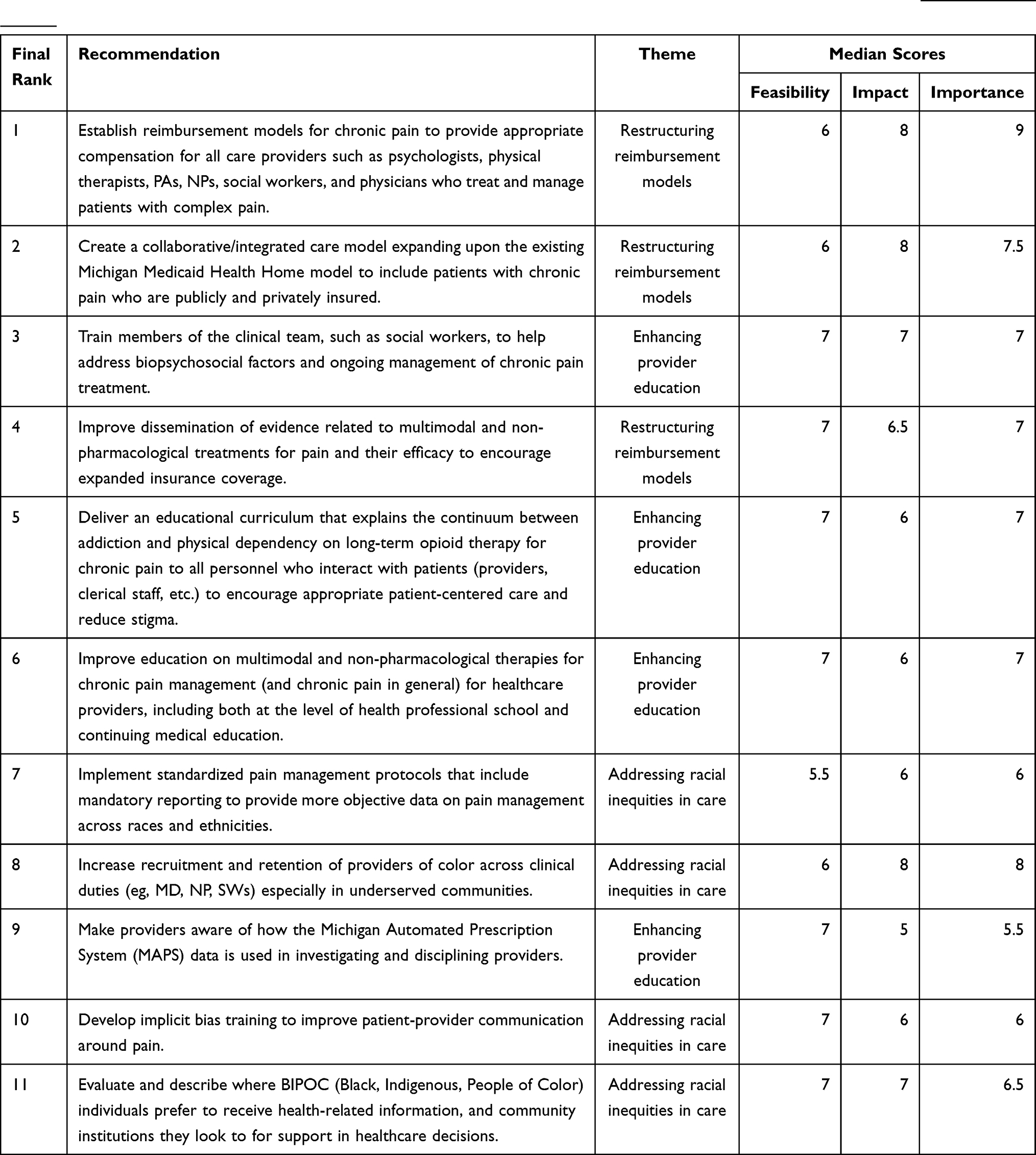 |
Table 2 Final Recommendation Priority Rankings and Median Scores of Feasibility, Impact, and Importance. (See Supplementary Table 2 for Additional Details) |
Three thematic domains emerged from the recommendations: restructuring reimbursement models, enhancing provider education, and addressing racial inequities in care. The first theme, restructuring reimbursement models, included three recommendations (#1, #2, #4). On average, recommendations in this theme received the highest priority rankings (theme average = 4.2/11). Four recommendations focused on enhancing provider education (#3, #5, #6, #9). These recommendations received slightly lower priority rankings (theme average = 6.2/11). The remaining four recommendations sought to address racial inequities in care (#7, #8, #10, #11; theme average = 7.2/11).
Discussion
The expert panel consistently emphasized that the lack of access to care for patients taking opioids is an important problem, echoing concerns from researchers, clinicians, and regulators.11,12,22,27,28 This panel was intentionally focused on improving access to care specifically for these patients, not pain care generally, and the panel’s recommendations reflected this narrow emphasis. In response to the various barriers to care they discussed, the panel generated a set of 11 distinct recommendations regarding policies, interventions, and research. All final recommendations received moderate to high median scores on feasibility, impact, and importance, suggesting panelists perceived there to be numerous viable options for stakeholder action. The final set of recommendations revealed 3 key themes: restructuring reimbursement models, enhancing provider education, and addressing racial inequities in care.
The highest priority recommendations involved restructuring care models through changes to payment structures. Payment-related recommendations, such as increased reimbursement for pain care providers, increased coverage of non-pharmacologic treatment, and integrative care models, received very high median importance and impact scores. As stakeholders consider these recommendations, it is also worth noting that policies and interventions similar to those the panel recommended have been implemented at the state and federal level. For example, five states—Iowa, Missouri, New York, South Dakota, and Washington—currently list at least one type of chronic pain as a qualifying condition for their Medicaid Health Homes, which grants Medicaid enrollees with chronic pain access to a coordinated care model.29,30 In addition, several state governments have utilized a slightly different strategy to restructure pain care: increasing Medicaid reimbursement rates for pain care. For example, Colorado increased Medicaid coverage of non-opioid pain management, including reimbursement rates for physical therapy, and Oregon added coverage for acupuncture, chiropractic services, osteopathic manipulation, cognitive behavioral therapy, and physical therapy for Medicaid beneficiaries with back and neck pain.31,32 At the federal level, the Centers for Medicare & Medicaid Services recently considered a change to the physician fee schedule that would increase provider reimbursement specifically for treating chronic pain.33 Though this change was not implemented in 2022, implementation is still under consideration for future rulemaking,34 and further research should examine its potential impact on patient access to pain care. Finally, the Veterans Health Administration is implementing the Whole Health program, which strives to increase veterans’ access to complementary and integrative pain treatments, and may provide a valuable alternative to patients on long-term opioid therapy who are losing access to treatment.35 Despite the high scores for importance and impact, and numerous examples of existing state and federal policy changes, these recommendations received relatively lower feasibility scores from the panel, suggesting panelists foresee implementation challenges with these types of systemic changes. However, during discussion, panelists representing insurer perspectives indicated that the suggested changes were feasible, and their implementation would likely be effective in driving behavioral change among providers. These discrepant perspectives were not reconciled during the panel discussions. It is possible that the optimism of panelists representing payor perspectives could have been due in part to desirability bias; conversely, perhaps the payors have a more realistic understanding of what reimbursement changes are possible, and other panelists were unduly critical about implementation.
Following reimbursement, recommendations on enhancing provider education, such as providing training on biopsychosocial factors of chronic pain management and on the spectrum of physical dependency and opioid use disorder (OUD), were the next highest thematic priority. Many states36 already mandate continuing medical education credits in pain management for maintaining licensure.37 Current qualifying training, however, is often limited in scope and duration and emphasizes the risk of opioid addiction rather than focusing on improving multimodal pain care.38,39 A growing number of health professional schools have started to offer training around OUD,40,41 including via the recent federal funding from SAMSHA’s Provider Clinical Decision Support System (PCSS) – University program.42,43 Yet, pain-related curricula that emphasize multimodal pain care, and not just opioid safety, remain limited. Analogous grant opportunities focused on patient-centered pain care may spur on growth across multiple institutions. The panel scored education recommendations as having lower impact than reimbursement-focused recommendations, suggesting that education on its own was unlikely to address access issues. However, existing medical education may be readily revised to include training on opioid-related care, chronic pain treatment, and associated stigma based on the panel’s recommended updates.
Recommendations to address racial bias and inequities ranked below education on the panelists’ final priority list. However, their median scores on feasibility, impact, and importance ranged from moderate to high, and were comparable to those of other recommendations. Outside of the panel’s findings, ongoing efforts to address racial inequities in pain care emphasize the perceived importance of these types of recommendations. In Michigan, the Department of Licensing and Regulatory Affairs recently instituted a new rule mandating 1 hour of implicit bias training per year for healthcare professional licensure.44 This new training requirement is not specific to pain- or addiction-related care, and its impact on pain-related care and racial inequities more broadly is not yet clear. More generally, the effectiveness of implicit bias training in addressing inequities remains unclear.45,46 At the federal level, the Office of National Drug Control Policy recently announced its intention to address racial inequities in substance use disorder treatment, including by identifying data gaps to target unmet treatment needs and identifying culturally competent and evidence-based practices.47 While specific to substance use disorder, these priorities provide a possible blueprint for future efforts to address racial inequities in pain care. It is worth noting, however, that these are still in the stage of identifying gaps and effective practices to remedy them; there is little consensus as to evidence-based, turnkey solutions for implementation. Throughout the panel’s discussion of racial inequities, there was general agreement that addressing racial inequities was important, but some concern that existing intervention strategies (ie, implicit bias training) might not be sufficient, and panelists expressed a desire for more efficacious avenues for intervention.
Limitations
This study had several limitations. By design, this panel focused on the state of Michigan. While the expertise and recommendations were therefore grounded in Michigan’s healthcare system, the content of discussions pertain to other states, and panelists (eg, payors, providers, patients, etc.) represented perspectives common to other regions of the country. Consequently, we believe these recommendations may be generalizable, and there is both opportunity and reason to believe that these recommendations for the State of Michigan could also potentially be implemented in other states. Their applicability to international health systems may be limited, as healthcare policies and landscapes differ substantially and were beyond the scope of this study. However, the panel’s findings do overlap significantly with those of a recent Canadian Pain Task Force Report, which also recommended expanding provincial healthcare coverage to incentivize multimodal pain treatment, considering alternative clinician reimbursement models, increasing provider education around pain, and working to address the unequal treatment access and implicit biases that disproportionately affect marginalized groups.48 Finally, this panel was conducted virtually due to the COVID-19 pandemic, which precluded in-person meetings. It is possible that in-person discussion meetings might have facilitated more panelist engagement and allowed for nonverbal communication that was limited by the virtual setting. Conversely, however, the virtual setting may have enabled participation that would not otherwise have been possible due to the time and resources needed to attend in-person events.
Conclusion
Patients who take opioids for chronic pain face unique challenges in the present opioid policy landscape, including reduced access to care. While there have been substantial efforts to improve access to care for OUD, the needs of this patient population have gone largely unrecognized and unaddressed. Limited access to high-quality care has caused significant distress among both patients and providers, and increasing access is an urgent priority. There have been some attempts to reverse the access barriers that have arisen in the current opioid prescribing climate, such as the letter issued in 2020 by the authors of the 2016 CDC opioid prescribing guideline warning clinicians against misapplication49 and, more recently, the release of an updated 2022 guideline, which emphasizes the importance of patient-centered care, multimodal pain treatments, and a more individualized, flexible approach to opioid prescribing.50 However, it remains to be seen how providers and policymakers respond to these new recommendations. The non-binding guideline may not be sufficient to reverse prescribing rules at the state and health system level or significantly change provider behaviors. Therefore, solutions such as those recommended by this Delphi panel may be required to meaningfully improve access to care. The results of this study emphasize the importance of a multifaceted approach, prioritizing reimbursement reform while also addressing limitations in clinical provider training and reducing racial inequities to improve access to care.
External Contributions
We are deeply grateful to our panelists for their thoughtful, sustained engagement and to our facilitators for leading such rich discussions. We would also like to thank the following organizations, which provided invaluable guidance: the Institute for Healthcare Policy and Innovation at the University of Michigan, the Michigan Primary Care Association, and the Michigan Department of Health and Human Services. Finally, we would like to thank Lizbeth Guerrero, Colin Macleod, Shivam Patel, and Avani Yaganti for their assistance in data collection and preparation of meeting materials.
Funding
This work was funded by the Michigan Health Endowment Fund [#R-1808-143371] (AK, JT, PL – all stages of study), the National Institute on Drug Abuse [#K23 DA047475] (PL, JT, AK – securing funding, conceptualization of theory), and the National Institute on Aging [#AG062043] (VP – facilitation and revision).
Disclosure
Dr Bicket reported receiving personal fees from Axial Healthcare and Alosa Health outside the submitted work. Authors note that a non peer-reviewed preprint white paper, entitled “Improving Access to Primary and Pain Care for Patients Taking Opioids for Chronic Pain in Michigan: Recommendations from an Expert Panel”, was written on this study, and shared with policymakers in advance of the publication of this peer-reviewed manuscript to expedite the dissemination of relevant policy implications. This white paper is available in perpetuity at https://dx.doi.org/10.7302/1699. No other disclosures were reported.
References
1. Ahmad F, Rossen L, Sutton P. Provisional Drug Overdose Death Counts. National Center for Health Statistics; 2021.
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain--United States, 2016. JAMA. 2016;315(15):1624–1645. doi:10.1001/jama.2016.1464
3. National Conference of State Legislatures. Prescribing policies: states confront opioid overdose epidemic. Available from: https://www.ncsl.org/research/health/prescribing-policies-states-confront-opioid-overdose-epidemic.aspx.
4. Bohnert ASB, Guy GP, Losby JL. Opioid prescribing in the United States before and after the Centers for Disease Control and Prevention’s 2016 opioid guideline. Ann Intern Med. 2018;169(6):367–375. doi:10.7326/M18-1243
5. Reuben DB, Alvanzo AAH, Ashikaga T, et al. National institutes of health pathways to prevention workshop: the role of opioids in the treatment of chronic pain. Ann Intern Med. 2015;162(4):295–300. doi:10.7326/M14-2775
6. Kertesz SG, Satel SL, DeMicco J, Dart RC, Alford DP. Opioid discontinuation as an institutional mandate: questions and answers on why we wrote to the Centers for Disease Control and Prevention. Subst Abuse. 2019;40(4):466–468. doi:10.1080/08897077.2019.1635973
7. Hamilton K. How the crackdown on painkillers is killing people; 2017. Available from: https://www.vice.com/en_us/article/ywn54b/how-the-crackdown-on-painkillers-is-killing-people.
8. Kertesz SG, Manhapra A, Gordon AJ. Nonconsensual dose reduction mandates are not justified clinically or ethically: an analysis. J Law Med Ethics J Am Soc Law Med Ethics. 2020;48(2):259–267. doi:10.1177/1073110520935337
9. Darnall BD, Juurlink D, Kerns RD, et al. International stakeholder community of pain experts and leaders call for an urgent action on forced opioid tapering. Pain Med. 2019;20(3):429–433. doi:10.1093/pm/pny228
10. Mark TL, Parish W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J Subst Abuse Treat. 2019;103:58–63. doi:10.1016/j.jsat.2019.05.001
11. Lagisetty PA, Healy N, Garpestad C, Jannausch M, Tipirneni R, Bohnert ASB. Access to primary care clinics for patients with chronic pain receiving opioids. JAMA Netw Open. 2019;2(7):e196928–e196928. doi:10.1001/jamanetworkopen.2019.6928
12. Lagisetty P, Macleod C, Thomas J, et al. Assessing reasons for decreased primary care access for individuals on prescribed opioids: an audit study. Pain. 2021;162(5):1379–1386. doi:10.1097/j.pain.0000000000002145
13. Lagisetty P, Slat S, Thomas J, Macleod C, Golmirzaie G, Bohnert AS. Access to multimodal pain management for patients with chronic pain: an audit study. J Gen Intern Med. 2020;36:818–820. doi:10.1007/s11606-020-05866-3
14. Fenton JJ, Agnoli AL, Xing G, et al. Trends and rapidity of dose tapering among patients prescribed long-term opioid therapy, 2008–2017. JAMA Netw Open. 2019;2(11):e1916271. doi:10.1001/jamanetworkopen.2019.16271
15. Behar E, Bagnulo R, Knight K, Santos GM, Coffin PO. “Chasing the pain relief, not the high”: experiences managing pain after opioid reductions among patients with HIV and a history of substance use. PLoS One. 2020;15(3):e0230408. doi:10.1371/journal.pone.0230408
16. Agnoli A, Xing G, Tancredi DJ, Magnan E, Jerant A, Fenton JJ. Association of dose tapering with overdose or mental health crisis among patients prescribed long-term opioids. JAMA. 2021;326(5):411–419. doi:10.1001/jama.2021.11013
17. James JR, Scott JM, Klein JW, et al. Mortality after discontinuation of primary care–based chronic opioid therapy for pain: a retrospective cohort study. J Gen Intern Med. 2019;34(12):2749–2755. doi:10.1007/s11606-019-05301-2
18. US Food and Drug Administration. FDA identifies harm reported from sudden discontinuation of opioid pain medicines and requires label changes to guide prescribers on gradual, individualized tapering. FDA; 2019. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-identifies-harm-reported-sudden-discontinuation-opioid-pain-medicines-and-requires-label-changes.
19. Oliva EM, Bowe T, Manhapra A, et al. Associations between stopping prescriptions for opioids, length of opioid treatment, and overdose or suicide deaths in US veterans: observational evaluation. BMJ. 2020;368:m283. doi:10.1136/bmj.m283
20. Slat S, Yaganti A, Thomas J, et al. Opioid policy and chronic pain treatment access experiences: a multi-stakeholder qualitative analysis and conceptual model. J Pain Res. 2020;2020:1161–1169.
21. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. National Academies Press (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK92522/.
22. U.S. Department of Health and Human Services. Pain management best practices inter-agency task force report: updates, gaps, inconsistencies, and recommendations; 2019. Available from: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html.
23. Gruß I, Firemark A, Mayhew M, McMullen CK, DeBar LL. Taking opioids in times of crisis: institutional oversight, chronic pain and suffering in an integrated healthcare delivery system in the U.S. Int J Drug Policy. 2019;74:62–68. doi:10.1016/j.drugpo.2019.08.009
24. Matthias MS, Parpart AL, Nyland KA, et al. The patient-provider relationship in chronic pain care: providers’ perspectives. Pain Med Malden Mass. 2010;11(11):1688–1697. doi:10.1111/j.1526-4637.2010.00980.x
25. Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR. The RAND/UCLA Appropriateness Method User’s Manual. Santa Monica CA: Rand Corp; 2001.
26. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6(6):e20476. doi:10.1371/journal.pone.0020476
27. Pitt AL, Humphreys K, Brandeau ML. Modeling health benefits and harms of public policy responses to the US opioid epidemic. Am J Public Health. 2018;108(10):1394–1400. doi:10.2105/AJPH.2018.304590
28. Kroenke K, Alford DP, Argoff C, et al. Challenges with implementing the Centers for Disease Control and Prevention opioid guideline: a consensus panel report. Pain Med. 2019;20(4):724–735. doi:10.1093/pm/pny307
29. Centers for Medicare & Medicaid Services. Conditions targeted by Medicaid health homes; 2021. Available from: https://www.medicaid.gov/state-resource-center/medicaid-state-technical-assistance/health-home-information-resource-center/downloads/targeted-conditions-matrix.pdf.
30. New York State Department of Health. Eligibility requirements: identifying potential members for health home services. 2020. Available from: https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/health_home_chronic_conditions.pdf.
31. American Medical Association, Manatt Health. National roadmap on state-level efforts to end the opioid epidemic: leading-edge practices and next steps; 2019. Available from: https://www.end-opioid-epidemic.org/wp-content/uploads/2019/09/AMA-Manatt-National-Roadmap-September-2019-FINAL.pdf.
32. Centers for Medicare & Medicaid Services. Medicaid innovation accelerator program targeted learning opportunity: CDC guideline for prescribing opioids for chronic pain; 2016. Available from: https://www.medicaid.gov/state-resource-center/innovation-accelerator-program/iap-downloads/06102016-iap-sud-tlo14.pdf.
33. Centers for Medicare & Medicaid Services. Federal register:: medicare program; CY 2022 payment policies under the physician fee schedule and other changes to part B payment policies; medicare shared savings program requirements; provider enrollment regulation updates; provider and supplier prepayment and post-payment medical review requirements. Available from: https://www.federalregister.gov/documents/2021/07/23/2021-14973/medicare-program-cy-2022-payment-policies-under-the-physician-fee-schedule-and-other-changes-to-part.
34. Centers for Medicare & Medicaid Services. Medicare program; CY 2022 payment policies under the physician fee schedule and other changes to part B payment policies; medicare shared savings program requirements; provider enrollment regulation updates; and provider and supplier prepayment and post-payment medical review requirements. Federal Register; 2021. Available from: https://www.federalregister.gov/documents/2021/11/19/2021-23972/medicare-program-cy-2022-payment-policies-under-the-physician-fee-schedule-and-other-changes-to-part.
35. Zeliadt SB, Douglas JH, Gelman H, et al. Effectiveness of a whole health model of care emphasizing complementary and integrative health on reducing opioid use among patients with chronic pain. BMC Health Serv Res. 2022;22(1):1053. doi:10.1186/s12913-022-08388-2
36. Michigan Department of Licensing and Regulatory Affairs. Continuing education requirements for Michigan medical doctors; 2019. Available from: https://www.michigan.gov/documents/lara/LARA_Medicine_CE_Brochure_5-11_376428_7.pdf.
37. Federation of State Medical Boards. Continuing medical education board-by-board overview. 2021.
38. NEJM Knowledge+. State requirements for pain management CME; 2020. Available from: https://knowledgeplus.nejm.org/cme-moc/pain-management-and-opioids-cme/state-requirements-for-pain-management-cme/.
39. Mezei L, Murinson BB. Pain education in North American medical schools. J Pain. 2011;12(12):1199–1208. doi:10.1016/j.jpain.2011.06.006
40. Murinson BB, Nenortas E, Mayer RS, et al. A new program in pain medicine for medical students: integrating core curriculum knowledge with emotional and reflective development. Pain Med. 2011;12(2):186–195. doi:10.1111/j.1526-4637.2010.01050.x
41. Tauben DJ, Loeser JD. Pain education at the University of Washington School of Medicine. J Pain. 2013;14(5):431–437. doi:10.1016/j.jpain.2013.01.005
42. Riser E, Holterman LA, Maruti S, et al. Integrating DATA 2000 waiver training into undergraduate medical education: the time is now. Subst Abuse. 2021;42(2):236–243. doi:10.1080/08897077.2021.1903653
43. Substance Abuse and Mental Health Services Administration. Provider’s clinical support system - universities notice of funding opportunity. 2022. Available from: https://www.samhsa.gov/grants/grant-announcements/ti-22-011.
44. Michigan Office of Administrative Hearings and Rules Administrative Rules Division. Request for rulemaking; 2021. Available from: https://ars.apps.lara.state.mi.us/Transaction/RFRTransaction?TransactionID=1235.
45. FitzGerald C, Martin A, Berner D, Hurst S. Interventions designed to reduce implicit prejudices and implicit stereotypes in real world contexts: a systematic review. BMC Psychol. 2019;7(1):29. doi:10.1186/s40359-019-0299-7
46. Gopal DP, Chetty U, O’Donnell P, Gajria C, Blackadder-Weinstein J. Implicit bias in healthcare: clinical practice, research and decision making. Future Healthc J. 2021;8(1):40–48. doi:10.7861/fhj.2020-0233
47. Executive Office of the President Office of National Drug Control Policy. The Biden-Harris administration’s statement of drug policy priorities for year one; 2021. Available from: https://www.whitehouse.gov/wp-content/uploads/2021/03/BidenHarris-Statement-of-Drug-Policy-Priorities-April-1.pdf?fbclid=IwAR2TBk34U_XRqlqK_pAYnUd_9f7zY3IbCQI9KxI6S5eYeRJdFzl9B09hZ84.
48. Canada.ca. Canadian pain task force report: march 2021. Available from: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021.html.
49. Dowell D, Haegerich T, Chou R. No shortcuts to safer opioid prescribing. N Engl J Med. 2019;380(24):2285–2287. doi:10.1056/NEJMp1904190
50. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71:1–95. doi:10.15585/mmwr.rr7103a1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.