Back to Journals » Journal of Pain Research » Volume 16
Implementing Telemedicine During the COVID-19 Pandemic: Disparities in Utilization in an Urban Pain Medicine Practice
Authors Rockholt MM ![]() , Addae G, Chee A, Chin W, Cuff G, Wang J, Umeh UO, Doan LV
, Addae G, Chee A, Chin W, Cuff G, Wang J, Umeh UO, Doan LV ![]()
Received 2 April 2023
Accepted for publication 19 July 2023
Published 8 August 2023 Volume 2023:16 Pages 2763—2775
DOI https://doi.org/10.2147/JPR.S415415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Mika M Rockholt,1 Gifty Addae,1 Alexander Chee,1 Wanda Chin,1 Germaine Cuff,1 Jing Wang,1,2 Uchenna O Umeh,1,3 Lisa V Doan1
1Department of Anesthesiology, Perioperative Care and Pain Management, New York University Grossman School of Medicine, New York, NY, 10016, USA; 2Department of Neuroscience & Physiology, Neuroscience Institute, New York University Grossman School of Medicine, New York, NY, 10016, USA; 3Department of Orthopedic Surgery, New York University Grossman School of Medicine, New York, NY, 10016, USA
Correspondence: Mika M Rockholt, Department of Anesthesiology, Perioperative Care and Pain Medicine, New York University Grossman School of Medicine, New York, NY, 10016, USA, Tel +1 646-209-7590, Email [email protected]
Purpose: The COVID-19 pandemic led to a drastic expansion in utilizing telemedicine, circumventing some of the geographical barriers to accessing pain care. However, uncertainties around the impact of telemedicine across various sociodemographic groups still exist, prompting further exploration. Therefore, this study aimed to evaluate the impact of sociodemographic factors in telemedicine utilization during and after the COVID-19 pandemic.
Patients and methods: All outpatient non-procedural visits at the pain medicine division of a large academic institution in the epicenter of the pandemic (New York, USA), between March 2019 and October 2021, were retrospectively included. Sociodemographic data including gender, age, ethnicity/race, postal code, and type of health insurance, across three time periods associated with the COVID-19 pandemic - pre-lockdown (in-office visits only), lockdown (telemedicine visits only) and post-lockdown (offering both in-office and telemedicine visits) – were analyzed and compared.
Results: In total, 12,615 unique patients - The majority being women (58%) - were seen during the whole study period. In the post-lockdown period, telemedicine was utilized by 42% of all patients. Follow-up visits, younger patients, white patients, patients residing further away from the hospital, and privately insured patients were more likely to utilize telemedicine post-lockdown (p < 0.05). Older patients, minorities, Manhattan residents, and Medicare/Medicaid recipients, were more likely to use in-office visits post-lockdown (p < 0.05).
Conclusion: We identified disparities in the utilization of telemedicine in Pain Medicine, which may be due to socioeconomic factors such as lack of access to reliable internet access, cost of devices, and technological know-how. This emphasizes the need for further studies to better understand the reasons for and barriers to telemedicine use. This could help inform policymaking to safeguard equitable access to telemedicine use for pain care.
Keywords: telemedicine, pain medicine, health care access, covid-19, disparities
Introduction
Billions of people around the world are affected by pain on a daily basis. It is estimated that approximately 20% of all adults suffer from pain worldwide, making it one of the largest global health problems.1 Chronic pain has become a growing public health concern in the United States, where it is said to affect over 35% of the US population, resulting in over 100 million patients requiring specialty treatment and costing an estimated $560 billion each year for medical care, lost productivity, or disability services.2,3 Moreover, chronic pain is associated with a high incidence of opioid use – contributing to the current opioid epidemic, as well as anxiety, depression, and a poor quality of life.4,5
Despite its prevalence, chronic pain is undertreated in the United States.4,6 A variety of contributing factors have been identified – including treatment-related stigma, geographic distance from specialty treatment providers, functional disability that limits mobility, lack of knowledge about specialty care, as well as differences in socioeconomic status with disparities seen among different racial and ethnic groups.3,6–8 Another major contributor to undertreated pain is the timely access to pain specialty care, where wait times often exceed six months – even when the services are geographically available.9 As undertreated pain exacerbates pain chronicity, there is widespread agreement that pain management must evolve to address these barriers.3,6
One potential solution to increase access to care is the utilization of telemedicine.10 Telemedicine has been defined as the real-time transmission of medical information using technologies such as video imaging and telecommunication devices to aid the provision of health care services at a distance.11 It involves audio and/or video interactions between patient and provider in two distinct locations and includes remote consultation, diagnosis, monitoring, and counseling of patients.12,13 The service has previously been shown to not only improve patient access to healthcare, but it has also shown other important advantages such as cost-effectiveness and increased resource efficiency.13–16 The use of telemedicine was accelerated by the COVID-19 pandemic.
Following a worldwide outbreak of SARS-CoV-2, the virus that causes COVID-19, the World Health Organization (WHO) declared the novel coronavirus (COVID-19) outbreak as a pandemic on March 11th 2020.17 Shortly after the declaration of the pandemic and in response to surging infection rates, the Centers for Disease Control (CDC) encouraged all outpatient clinics, hospitals, and ambulatory surgical centers to limit all non-essential activity to prevent the spread and reduce strain on healthcare systems with mitigating shortage of personal protective equipment (PPE).18 With patients being asked to follow stay-at-home orders and clinics closed to in-person visits, telemedicine quickly became a necessary component of non-emergency healthcare.18,19 Telemedicine also became an important healthcare access tool for chronic pain patients, a cohort that often requires frequent office visits for treatment and management, with an increased risk of being neglected in the occurred scenario.20
With time, the expansion of telemedicine use was further supported by federal and state policy changes, including the Medicare telemedicine expansion, which lifted restrictions to telemedicine use and established parity in reimbursement rates for virtual vs in-office care.21–23 With its crux focused on connecting patients with healthcare providers via video-enabled virtual visits, telemedicine eliminated travel-related costs and reduced the burden of travel time, thereby ameliorating some traditional access-level barriers to treatment while maintaining patient satisfaction.18,22,24
In the aftermath, increased use of telemedicine to meet clinical needs has now been well documented and there is evidence that it may continue to play an important role in healthcare delivery in the foreseeable future.11 However, telemedicine also presents many limitations, and studies have suggested it might be tailored for selected patient categories.16,25 One concern is the impact of Telemedicine on different populations with differences in healthcare access – one of the already known barriers to undertreated pain. Access to telemedicine generally relies on the patient’s ability to obtain and use technology - factors that are usually dictated by age, education, and socioeconomic status.16,26 While many studies have focused on the direct benefits and limitations of the utilization of telemedicine, few studies have focused on potential socio-demographic factors, including health insurance coverage, which could impact a wider adoption of this service in the context of pain medicine.27,28
To further assess the demographics of patients utilizing telemedicine services for pain medicine during and after the first wave of the COVID-19 pandemic, we conducted this retrospective, cohort study, hypothesizing that minority patients with non-commercial insurance would utilize telemedicine less. Secondarily, we aim to identify independent socio-demographic factors associated with the utilization of telemedicine.
Methods
This study was approved by the Institutional Review Board (IRB; S21-00643) at the NYU Grossman School of Medicine. Informed consent was waived due to the retrospective nature of the study with protections for patient confidentiality. It was conducted in accordance with the Declaration of Helsinki. The manuscript was prepared according to the STROBE guidelines for observational studies.
All documented non-procedural visits to Manhattan locations of the NYU Langone Health Pain Medicine Division, between March 1, 2019 and October 21, 2021, were eligible for inclusion. There were no exclusion criteria.
Data were obtained from the institutional electronic medical record (Epic, Verona, Wisconsin, USA). Visit-related and sociodemographic data obtained included: the date of visit, type of visit (new patient or follow-up visit), gender, age, ethnicity/race, postal code, and health insurance type.
The main outcome of interest was visit type (in office vs telemedicine) according to the various periods associated with the COVID-19 pandemic (see Supplemental File 1). Before the COVID-pandemic, telemedicine was not an option – a period defined as pre-lockdown (from March 1, 2019 until March 19, 2020). In-office visits at NYU Langone Health were paused in early March 2020, and the health system transitioned to telemedicine. The “lockdown period” is defined as the period when primarily telemedicine was used, between March 20, 2020 and June 1, 2020. Post-lockdown started on June 2, 2020, when in-office visits resumed but where telemedicine remained an option for patients.
Variables of interest were the type of visit (new patient or follow-up visit), gender, age, ethnicity/race, postal code, and health insurance type, across the three time periods (main outcomes) were analyzed. Categorical data encoding was applied and IBM SPSS Statistical software (Version 28, IBM, New York, USA) was used to perform all statistical analyses. Results were expressed as mean (± standard deviation) or range (min-max) for continuous variables and a number (percentage) for categorical variables.
To compare baseline variables across the three time periods (pre-lockdown, lockdown, and post-lockdown periods), non-parametric Mann–Whitney and chi-square tests were used for continuous and/or categorical variables, respectively. The Kruskal–Wallis test was applied for baseline variables to compare main outcome groups, using the Bonferroni test for adjusted significance. Differences amongst post-lockdown patients utilizing telemedicine were tested against non-telemedicine users using regression analyses, where all baseline variables were considered potential independent variables for utilizing telemedicine. Given a presumed complex interdependence of these variables, multivariable regression analyses were performed. The selection of variables in the multivariable regression analyses was based on results from previous studies and the univariate analyses.27,28 The Hosmer-Lemeshow test was used to test the goodness of fit for multivariable testing. P<0.05 was considered significant and all tests were two-tailed.
Results
Baseline characteristics of the study cohorts, including comparisons, across the three time periods are presented in Tables 1–3. In summary, a total of 12,615 unique patients were seen at the Manhattan offices of the NYU Langone Health Pain Medicine division between March 1, 2019 and October 21, 2021. In total, 25,926 patient visits were registered during the complete study period, yielding an average of two visits per patient (range 1–23). Before the COVID-19 pandemic, telemedicine was not an option for visits (pre-lockdown period). Telemedicine was instituted during the lockdown period, and it continued to be an option in the post-lockdown period.
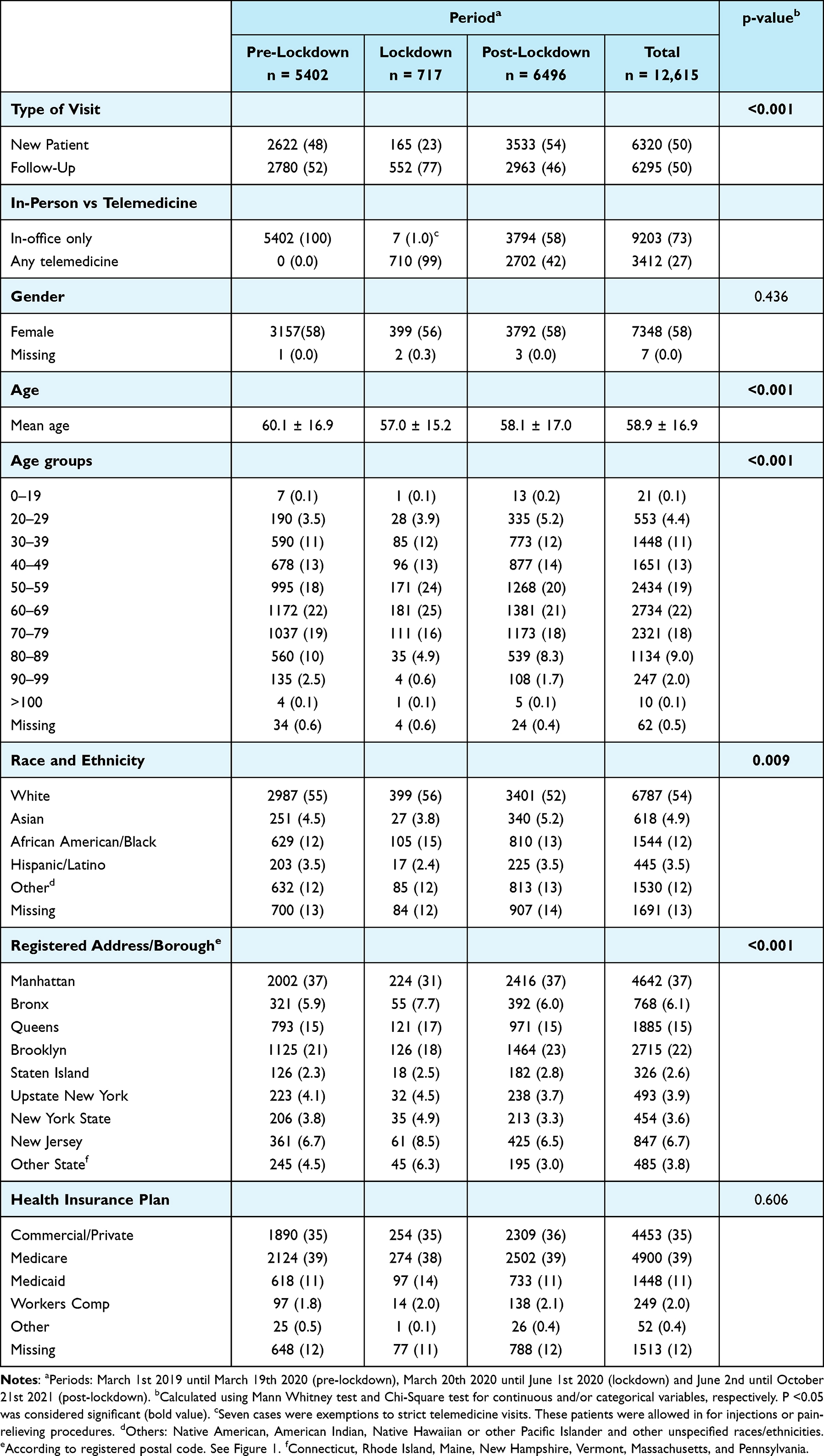 |
Table 1 Baseline Data Including Patient Characteristics and Visit Details. Data are Presented as Mean ± Standard Deviation or Number (Percentage) |
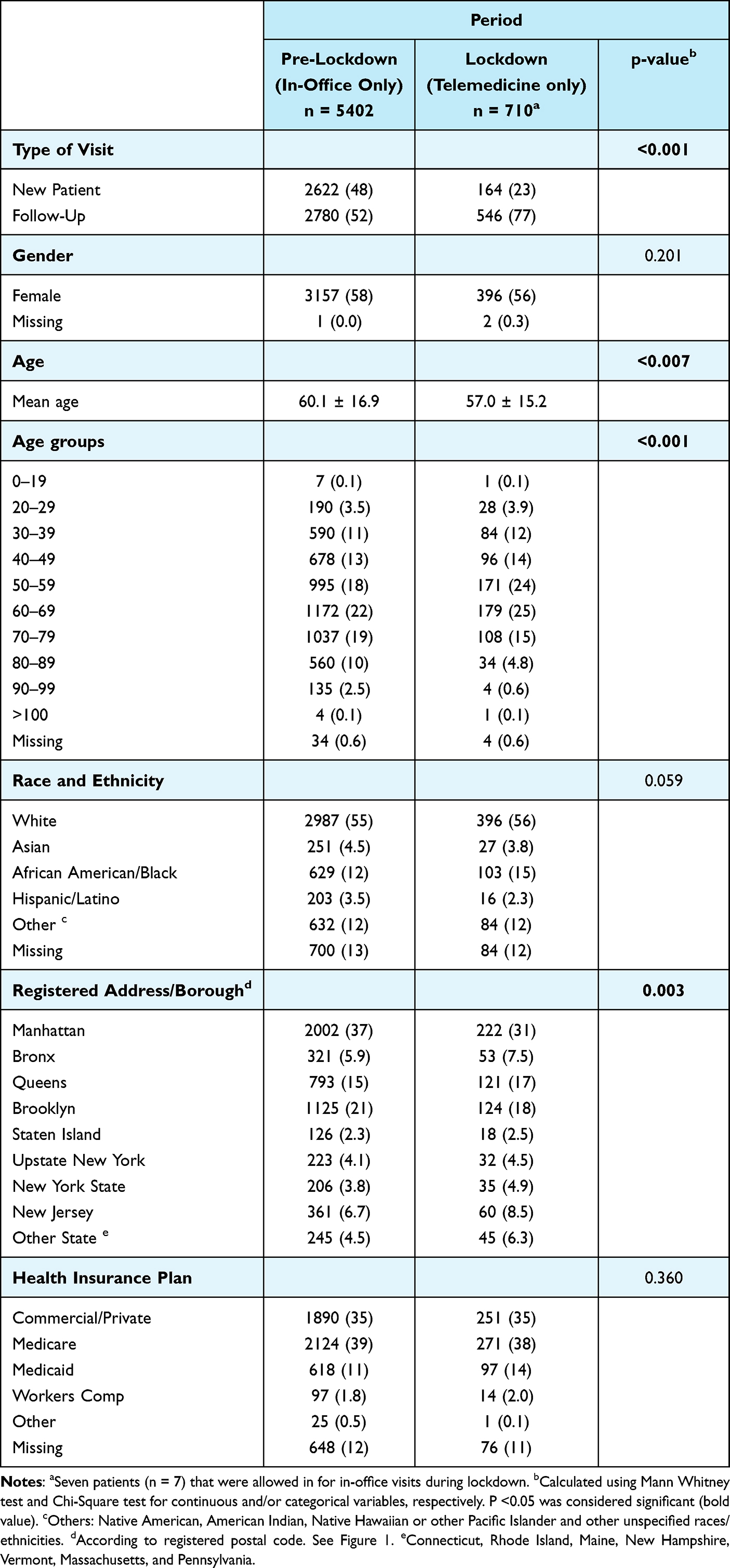 |
Table 2 Demographic Comparisons Pre-Lockdown and During Lockdown. Data are Presented as Mean ± Standard Deviation or Number (Percentage) |
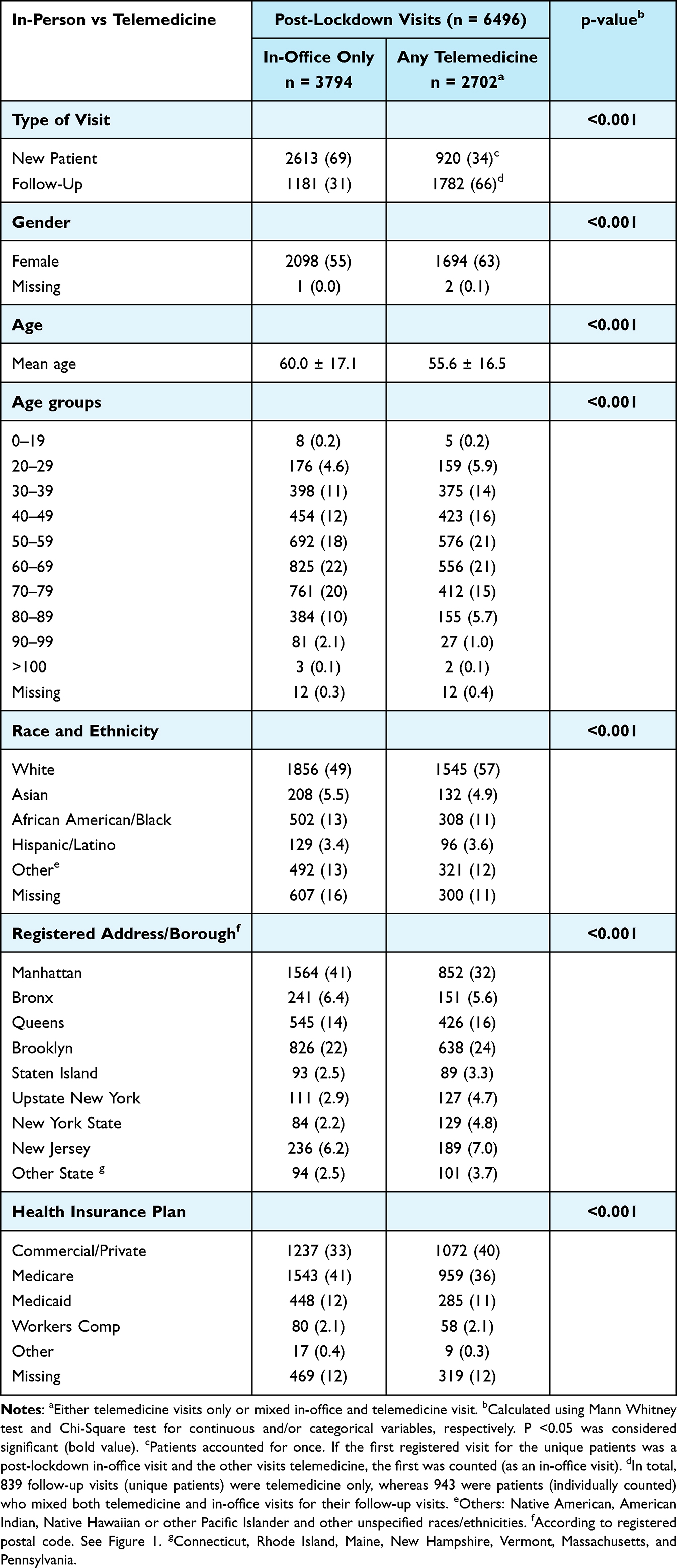 |
Table 3 Characteristics of Post-Lockdown Patients and Visits (In-Office Only vs Any Telemedicine Visit). Data are Presented as Mean ± Standard Deviation or Number (Percentage) |
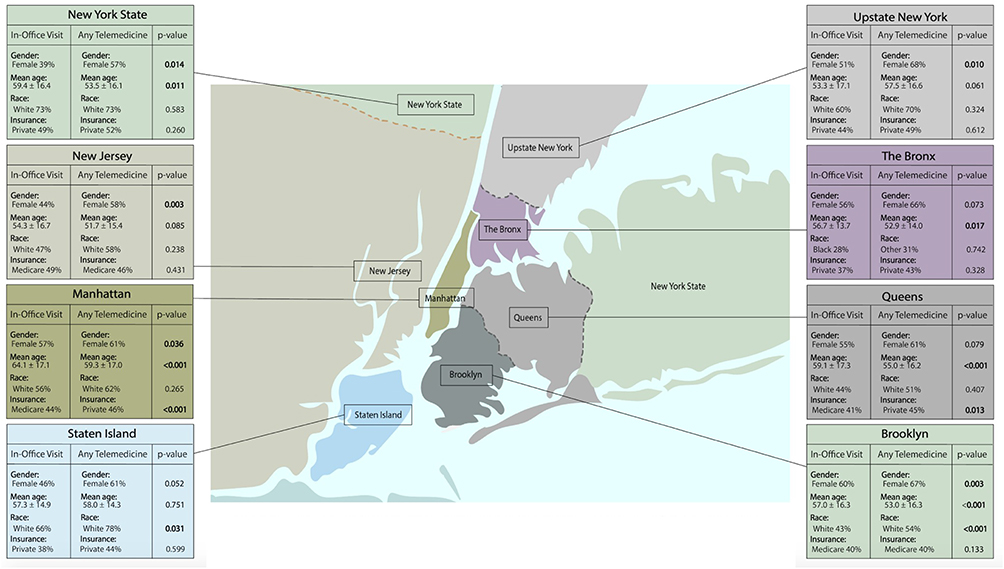 |
Figure 1 The most prevalent patient characteristics within each category according to borough/state are presented. For further details, see Supplemental Files 2 and 3. Data are presented as mean ± standard deviation for continuous variables or number (percentage) for categorical variables. The Kruskal–Wallis test was applied for independent parameters to compare groups, using the Bonferroni test for adjusted significance (p-value). P <0.05 was considered significant (bold value). Illustration by Mika M. Rockholt. |
Pre-lockdown (March 1, 2019 until March 19, 2020), a total of 10,768 office-based visits were registered in a total of 5402 unique patients, yielding two average visits per patient (range 1–15). During lockdown (March 20, 2020 until June 1, 2020) only telemedicine was offered – with the exception of seven patients seen in person, who were evaluated for pain interventions. A total of 919 telemedicine visits were registered in a total of 717 unique patients, yielding an average of 1.3 visits per patient (range 1–4). Once in-office visit restrictions were removed, patients were offered in-office visits and/or telemedicine (post-lockdown period). During this period of the study, spanning between June 2, 2020 and October 21, 2021, a total of 14,239 visits were registered in 6496 unique patients, yielding an average of 2.2 visits per patient (range 1–23). Of these patients with post-lockdown visits (n = 6496), 42% used telemedicine (n = 2702). The type of visit across the three time periods varied significantly (p <0.001). Prior to lockdown when only in-person visits were available, there was a roughly equal distribution between new patient visits and follow-up visits (48% vs 52%). The majority of lockdown visits and post-lockdown telemedicine visits were follow-up visits (77% and 66%, respectively). Post-lockdown in-person visits were mainly dedicated toward new patients (69%) (p < 0.001).
The majority of patients across all three time periods were female (58%), and a significantly higher proportion of women utilized telemedicine over in-person visits post-lockdown (63% vs 45%, p < 0.001). Demographically, significantly more women vs men residing in Manhattan, Brooklyn, Upstate New York, New York State, and New Jersey preferred telemedicine post-lockdown (p <0.05, please see Figure 1). Moreover, there was also a significant difference (p <0.001) in age across telemedicine vs in-person visitors, with telemedicine users during lockdown and post-lockdown being younger (mean age 57.0 ± 15.2 and 55.6 ± 16.5, respectively) as compared to in-person pre-lockdown and post-lockdown patients (60.1 ± 16.9 and 60.0 ± 17.1, respectively). As presented in Figure 1, residents of Manhattan, the Bronx, Queens Brooklyn, and New York State who more often utilized telemedicine instead of in-office visits were significantly younger than patients residing in Staten Island, Upstate New York, and New Jersey (p < 0.05). Overall, the majority of patients in the study population were white (54%), and a significantly higher proportion of white patients utilized telemedicine post-lockdown (p < 0.001), particularly amongst residents of Brooklyn and Staten Island (Figure 1 and Supplemental File 2).
The majority of patients visiting the pain medicine division in the studied time period resided in Manhattan (37%), followed by Brooklyn (22%) and Queens (15%). During lockdown, a significantly higher proportion of patients residing outside of New York City (Upstate New York, New York State, New Jersey, and other states) utilized telemedicine, as compared with the pre-lockdown and post-lockdown in-office visits. Post-lockdown, there was a statistically significant shift in patients visiting from different boroughs/states (p <0.05), with Manhattan residents (41% vs 32% utilizing telemedicine) using in-office visits more frequently. In contrast, patients residing in Queens, Brooklyn, Staten Island, and outside of New York City were more prone to use telemedicine during lockdown and/or post-lockdown (p < 0.05).
The majority of patients across all time periods were insured through Medicare (39%), followed by commercial/private health insurance (35%) and Medicaid (11%). There was no statistically significant difference when comparing the type of health insurance used across the three groups nor between patients visiting pre-lockdown and during lockdown. Post-lockdown however, there was a statistically significant difference across in-person visitors vs telemedicine users (p < 0.001), where the majority of in-office patients were insured through Medicare (41%) whereas telemedicine users mainly had commercial/private health insurance (40%). As presented in Figure 1 and Supplemental File 3, there was a statistically significant difference in patients utilizing telemedicine vs in-office visits amongst patients residing in Manhattan and Queens, where the majority of telemedicine utilizers were insured through private health insurance (p < 0.005) vs in-office patients which were insured through Medicare.
All independent variables were selected for investigation of post-lockdown utilization of telemedicine (n = 2702) vs in-office visits only (n = 5402). The detailed results of the multivariable regression analysis are shown in Table 4. Follow-up visits, female gender, white race, patients residing outside of Manhattan and Staten Island, and patients insured through commercial/private health insurance were all positively associated with the utilization of telemedicine post-lockdown (OR >1; p < 0.05). In contrast, older patients, racial and ethnic minorities such as Asians, African Americans/Black and Hispanic/Latino, patients living in Manhattan, and those insured through Medicare or Medicaid, were all negatively associated with the utilization of telemedicine and thus, more likely to use in-office visits (OR < 1; p <0.05).
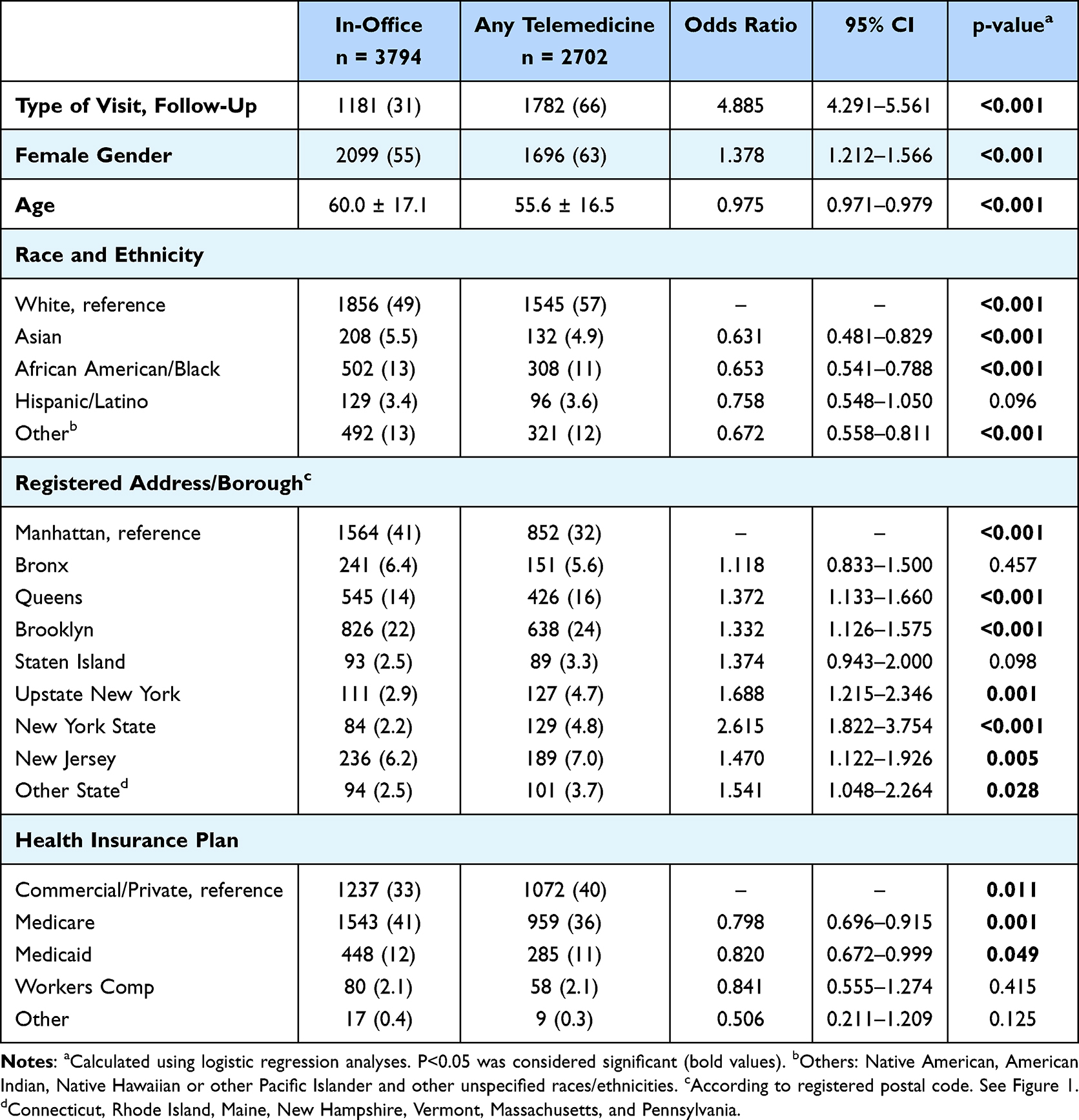 |
Table 4 Multivariate Logistic Regression Analysis of Patients Visits Post-Lockdown (Comparing in-Office Visits vs Any Telemedicine Visits). Data are Presented as Mean ± Standard Deviation or Number (Percentage) |
Discussion
Telemedicine has become an important resource for healthcare delivery in the United States and around the world, with its use drastically increasing during the COVID-19 pandemic.13,16,19,24,29,30 In the context of pain care, the utilization of telemedicine could eliminate some of the major geographical barriers, as well as the resources to attend in-person visits such as taking time off work and transportation to the office, which may all be contributing to the current undertreatment of chronic pain.12,13 However, the service has several limitations and questions remain on the equitable distribution of this resource and its impact on various communities, especially on those from disadvantaged backgrounds. In this study, we compared demographic information of patients that utilized in-person pain medicine visits in the year before the pandemic, to that of patients who utilized telemedicine visits during lockdown at the peak of the COVID-19 pandemic, and those who continued utilizing telemedicine in the post-lockdown era. Our results indicate important disparities in the utilization of telemedicine services, where sociodemographic factors such as age, race, ethnicity, area of residence and type of insurance, seem to play a key role.
Our study analyzed a total of12615visiting our pain medicine division over a transitional 32-month period, where the possibility to choose a virtual physician-patient encounter was established. As seen in Table 1 and Table 2, our results show that 42% of all post-lockdown patients utilized telemedicine for their visits, despite now having the option for an in-office visit as well. This could be attributed to multiple factors, which have been mentioned in previous publications, including the convenience of receiving care from the comfort of one’s home and the elimination of travel and wait time.16,21,22 This is further supported when looking at the results from the regression analysis (Table 4), demonstrating a significant association between residing outside of Manhattan and the utilization of telemedicine. In contrast, patients residing in Manhattan – in proximity to the locations examined in the study, but also an area well served by public transportation - preferred in-office visits post-lockdown. Furthermore, as follow-up visits are usually less acute, patients may have been more comfortable using telemedicine for this purpose.
The pandemic had a tremendous impact on the implementation and utilization of telemedicine. Studies have demonstrated the clear cost-economic benefits of this service – including increased annual patient volumes, reduced travel distances, fuel costs, and climate impact, but also lower amortization and discount rates.13,20–22 Moreover, telemedicine is a good choice when it comes to visits such as follow-up visits, since it opens up another opportunity for patients to improve their treatment compliance and adherence.16 These unique aspects of delivering care via telemedicine in the context of pain management can circumvent some of the major contributors to undertreated chronic pain, and thus improve the quality of care in this population.
The majority of patients utilizing pain medicine services and telemedicine in our cohort were females, which is unsurprising given that chronic pain affects a higher proportion of females than males around the world.28,31–33 Another possibility is that male individuals may be underutilizing pain management services.28,34
Furthermore, we observed that younger patients were more likely to utilize telemedicine. This finding is in line with the findings from the National Survey Trends in Telehealth Use in 2021, concluding that younger adults (defined as age < 65) were more likely to utilize telemedicine software as compared to their senior counterparts.35 This may be due to younger adults being more technologically savvy and more willing to embrace new technology. In addition, seniors may encounter barriers related to costs as well as barriers to technological literacy and know-how, thereby making it difficult to access telemedicine services.16,21
As presented in Table 1, we observed a statistically significant difference in the distribution of patients of certain race/ethnicity across the three time periods, with the majority of patients being white. During lockdown, with telemedicine being the only option, a larger proportion of white and African American/Black patients visited our service. Post-lockdown, we observed that minorities more often used in-office visits than telemedicine visits (Table 4).
In a recent study from a different New York health system, 3314 patients in the NYC area were evaluated for disparities in the utilization of telemedicine during lockdown and post-lockdown. The study demonstrated that African American/Black patients had an increased likelihood of accessing medical care within both periods, but also suggested that the usage of telemedicine during lockdown was a strong predictor for continued telemedicine utilization post-lockdown.28 We did not observe the same predictor in our analyses. Instead, our results are more consistent with those of studies conducted in other parts of the country, demonstrating a negative association between being a minority and the utilization of telemedicine.27,36 These findings highlight an important disparity in the utilization of telemedicine and as in other publications, we are in agreement that healthcare systems should work towards minimizing such barriers to telemedicine – especially in minorities suffering from chronic pain, as it has been demonstrated that this population is undertreated.6,8,36
Lastly, private health insurance was positively associated with the utilization of telemedicine, whereas the opposite was seen with patients insured through Medicare or Medicaid. This could also be due to socioeconomic differences where people with private insurance have higher incomes but also may have better access to newer technology and thus, be more tech-savvy. However, the significance of these results was not unexpected, as the policies on health insurance coverage changed during the pandemic to establish parity in reimbursement rates in both in-office and virtual patient visits.
At the beginning of the pandemic, Centers for Medicare & Medicaid Services (CMS) enhanced parity in reimbursement for Medicare with fee-for-service costs comparable to private insurance. Additionally, CMS waived traditional Medicare geographical restrictions, so that providers in various settings could expand telehealth services and continue providing care. State Medicare and Medicaid programs also made several policy changes21–23 to encourage greater telemedicine use for healthcare services, and they significantly expanded access to telemedicine services to ensure that Medicare/Medicaid enrollees could receive healthcare services outside of their regular healthcare delivery sites.37,38 Despite these efforts, some barriers to accessing telemedicine services have still been encountered. In a recent nationwide study, it was demonstrated that about 26% of Medicare beneficiaries lack access to a desktop, laptop, or smartphone at home.39 This issue is further compounded by the fact that senior patients (65 years and older) are more likely to encounter barriers related to technological literacy and more likely to experience physical disability and cognitive decline.37,39 These challenges could be contributing to the disparity in the usage of telemedicine services by Medicare recipients. However, our findings did not show that Medicare and Medicaid enrollees were more or less likely to utilize telemedicine visits at our center. Nevertheless, further analyses are needed to determine the significance of these results.
As demonstrated, our study findings show consistency – but also some inconsistencies – when compared with previous studies looking into disparities in the use of telehealth modalities by race/ethnicity, age, education, income, and health insurance coverage. This raises questions about barriers to equitable access to telemedicine.22,28,36,40 Telemedicine use requires a complex setup, video-enabled devices, and broadband internet access, which may be barriers for older adults, lower-income households, and those with limited English proficiency.16,28,35,36 These barriers likely have disproportionate impacts across different populations and patient categories as reflected in our findings.
The main limitation of the present study is its retrospective design. The majority of data presented is descriptive and information on confounders, such as patient and physician preferences and socioeconomic factors, which might have influenced the results is lacking. Moreover, the patients seen in our offices do not reflect the overall demographic distribution of the city (nyc.gov). These limitations are in part mitigated by our use of a large cohort of patients in one of the most diverse cities in the US. Our results are also compatible with previously published results from the same geographical area.28 At the same time, the differences in racial/ethnic distribution among telemedicine utilizers in our results when compared with previously published results indicate the complexity of this clinical problem, especially in the context of pain care, necessitating future studies. Our study also informs on potential barriers to telemedicine access. The results of this study suggest disparities in access to telemedicine use and raise questions about barriers to equitable access and its future impact on healthcare delivery. Future studies should be aimed at elucidating these barriers and should inform on the design and implementation of future policies that could mitigate these disparities and increase equitable access to telemedicine use. This is especially important in chronic pain sufferers, as socioeconomic disparities within this population are known contributors to undertreated pain.
Conclusions
Telemedicine has become an integral part of healthcare delivery and will remain so in the foreseeable future. This study examined the demographics of patients that utilize telemedicine in pain management clinics. We found disparities in the utilization of telemedicine services. Our results show that most telemedicine visits were used for follow-up visits. Telemedicine users were more likely to be younger, white, residing further away from the hospital, and privately insured. In contrast, older patients, racial and ethnic minorities, patients residing in Manhattan, and patients insured through Medicare and Medicaid were less likely to utilize telemedicine.
The results of this study suggest disparities in access to telemedicine use, possibly due to socioeconomic factors such as lack of access to reliable internet access, technological cost of devices, and technological know-how. Our findings emphasize the need for further studies to better understand the value of telehealth on health outcomes across various patient populations. This will inform policymaking to safeguard equitable access to telemedicine use and delivery of high-quality care via telemedicine visits.
Funding
This study was funded by the Department of Anesthesiology, Perioperative Care, and Pain Medicine at NYU Grossman School of Medicine.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11(1):770. doi:10.1186/1471-2458-11-770
2. Institute of Medicine Committee on Advancing Pain Research C, Education. The National Academies Collection: reports funded by National Institutes of Health. In: Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US) Copyright © 2011; 2011.
3. Kuehn B. Chronic pain prevalence. JAMA. 2018;320(16):
4. Goldberg DS. Job and the stigmatization of chronic pain. Perspect Biol Med. 2010;53(3):425–438. doi:10.1353/pbm.0.0166
5. Marshall B, Bland MK, Hulla R, Gatchel RJ. Considerations in addressing the opioid epidemic and chronic pain within the USA. Pain Manag. 2019;9(2):131–138. doi:10.2217/pmt-2018-0070
6. McGeary DD, McGeary CA, Gatchel RJ. A comprehensive review of telehealth for pain management: where we are and the way ahead. Pain Pract. 2012;12(7):570–577. doi:10.1111/j.1533-2500.2012.00534.x
7. Keogh E, Rosser BA, Eccleston C. e-health and chronic pain management: current status and developments. Pain. 2010;151(1):18–21. doi:10.1016/j.pain.2010.07.014
8. Goree JH, Jackson J. Do racial and ethnic disparities lead to the undertreatment of pain? Are there solutions? Curr Opin Anaesthesiol. 2022;35(3):273–277. doi:10.1097/ACO.0000000000001139
9. Lynch ME, Campbell F, Clark AJ, et al. A systematic review of the effect of waiting for treatment for chronic pain. Pain. 2008;136(1–2):97–116. doi:10.1016/j.pain.2007.06.018
10. Byrne MD. Telehealth and the COVID-19 pandemic. J Perianesth Nurs. 2020;35(5):548–551. doi:10.1016/j.jopan.2020.06.023
11. Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. 2020;27(7):1132–1135. doi:10.1093/jamia/ocaa072
12. Emerick T, Alter B, Jarquin S, et al. Telemedicine for chronic pain in the COVID-19 era and beyond. Pain Med. 2020;21(9):1743–1748. doi:10.1093/pm/pnaa220
13. Cascella M, Marinangeli F, Vittori A, et al. Open issues and practical suggestions for telemedicine in chronic pain. Int J Environ Res Public Health. 2021;18(23):12416. doi:10.3390/ijerph182312416
14. Pronovost A, Peng P, Kern R. Telemedicine in the management of chronic pain: a cost analysis study. Can J Anaesth. 2009;56(8):590–596. doi:10.1007/s12630-009-9123-9
15. Baldwin L, Clarke M, Hands L, Knott M, Jones R. The effect of telemedicine on consultation time. J Telemed Telecare. 2003;9(Suppl 1):S71–S73. doi:10.1258/135763303322196420
16. Perez J, Niburski K, Stoopler M, Ingelmo P. Telehealth and chronic pain management from rapid adaptation to long-term implementation in pain medicine: a narrative review. Pain Rep. 2021;6(1):e912. doi:10.1097/PR9.0000000000000912
17. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
18. Colbert GB, Venegas-Vera AV, Lerma EV. Utility of telemedicine in the COVID-19 era. Rev Cardiovasc Med. 2020;21(4):583–587. doi:10.31083/j.rcm.2020.04.188
19. Eccleston C, Blyth FM, Dear BF, et al. Managing patients with chronic pain during the COVID-19 outbreak: considerations for the rapid introduction of remotely supported (eHealth) pain management services. Pain. 2020;161(5):889–893. doi:10.1097/j.pain.0000000000001885
20. Singh P, Gautam S, Agarwal A. Telemedicine pain clinic facilities in the era of COVID-19. Indian J Pain. 2020;34(2):141. doi:10.4103/ijpn.ijpn_71_20
21. Wahezi SE, Kohan LR, Spektor B, et al. Telemedicine and current clinical practice trends in the COVID-19 pandemic. Best Pract Res Clin Anaesthesiol. 2021;35(3):307–319. doi:10.1016/j.bpa.2020.11.005
22. Jalilian L, Wu I, Ing J, et al. Evaluation of telemedicine use for anesthesiology pain division: Retrospective, Observational Case Series Study. JMIR Perioper Med. 2022;5(1):e33926. doi:10.2196/33926
23. Richardson PA, Parker DM, Chavez K, et al. Evaluating telehealth implementation in the context of pediatric chronic pain treatment during COVID-19. Children. 2021;8(9):764. doi:10.3390/children8090764
24. Harnik MA, Blättler L, Limacher A, Reisig F, Grosse Holtforth M, Streitberger K. Telemedicine for chronic pain treatment during the COVID-19 pandemic: do pain intensity and anxiousness correlate with patient acceptance? Pain Pract. 2021;21(8):934–942. doi:10.1111/papr.13071
25. Hasoon J, Urits I, Viswanath O, Kaye AD. Pain management and telemedicine: a look at the COVID experience and beyond. Health Psychol Res. 2022;10(3):38012. doi:10.52965/001c.38012
26. Ramirez AV, Ojeaga M, Espinoza V, Hensler B, Honrubia V. Telemedicine in minority and socioeconomically disadvantaged communities amidst COVID-19 pandemic. Otolaryngol Head Neck Surg. 2021;164(1):91–92. doi:10.1177/0194599820947667
27. Lattimore CM, Kane WJ, Fleming MA II, et al. Disparities in telemedicine utilization among surgical patients during COVID-19. PLoS One. 2021;16(10):e0258452. doi:10.1371/journal.pone.0258452
28. Mueller BR, Lawrence S, Benn E, et al. Disparities in telehealth utilization in patients with pain during COVID-19. Pain Rep. 2022;7(3):e1001. doi:10.1097/PR9.0000000000001001
29. Novara G, Checcucci E, Crestani A, et al. Telehealth in urology: a systematic review of the literature. How much can telemedicine be useful during and after the COVID-19 pandemic? Eur Urol. 2020;78(6):786–811. doi:10.1016/j.eururo.2020.06.025
30. Shanthanna H, Strand NH, Provenzano DA, et al. Caring for patients with pain during the COVID-19 pandemic: consensus recommendations from an international expert panel. Anaesthesia. 2020;75(7):935–944. doi:10.1111/anae.15076
31. Häggman-Henrikson B, Liv P, Ilgunas A, et al. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain. 2020;161(8):1768–1775. doi:10.1097/j.pain.0000000000001872
32. van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13–18. doi:10.1093/bja/aet123
33. Lott A, Campbell KA, Hutzler L, et al. Telemedicine utilization at an academic medical center during COVID-19 pandemic: are some patients being left behind? Telemed J E Health. 2022;28(1):44–50. doi:10.1089/tmj.2020.0561
34. Marcell AV, Klein JD, Fischer I, Allan MJ, Kokotailo PK. Male adolescent use of health care services: where are the boys? J Adolesc Health. 2002;30(1):35–43. doi:10.1016/S1054-139X(01)00319-6
35. Karimi M, Lee EC, Couture SJ, et al. National Survey Trends in Telehealth Use in 2021: Disparities in Utilization and Audio Vs. Video Services. Department of Health and Human Services, Office of the Assistant Secretary; 2022.
36. Hsiao V, Chandereng T, Lankton RL, et al. Disparities in telemedicine access: a Cross-Sectional Study of a newly established infrastructure during the COVID-19 pandemic. Appl Clin Inform. 2021;12(03):445–458. doi:10.1055/s-0041-1730026
37. Samson LW, Tarazi W, Turrini G, Sheingold S. Medicare Beneficiaries’ Use of Telehealth in 2020: Trends by Beneficiary Characteristics and Location. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation; 2021.
38. Chu RC, Peters C, De Lew N, Sommers BD. State Medicaid Telehealth Policies Before and During the COVID-19 Public Health Emergency. Department of Health and Human Services, Office Of the Assistant Secretary; 2021.
39. Roberts ET, Mehrotra A. Assessment of disparities in digital access among medicare beneficiaries and implications for telemedicine. JAMA Intern Med. 2020;180(10):1386–1389. doi:10.1001/jamainternmed.2020.2666
40. Koonin LM, Hoots B, Tsang CA, et al. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(43):1595. doi:10.15585/mmwr.mm6943a3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experience of Telemedicine in Gastroenterology Out-Patient Practice During the COVID-19 Pandemic: Experiences from a Tertiary-Care Hospital in a Developing Country
Shaikh A, Khan M, Ismail FW
Clinical and Experimental Gastroenterology 2022, 15:91-99
Published Date: 17 June 2022
Geriatric Health Care During the COVID-19 Pandemic: Managing the Health Crisis
Zhu Y, Liu Y, Jiang H
Clinical Interventions in Aging 2022, 17:1365-1378
Published Date: 17 September 2022
The Role of Teledermatology During the COVID-19 Pandemic: A Narrative Review
Ruggiero A, Martora F, Fabbrocini G, Villani A, Marasca C, Megna M, Fornaro L, Comune R, Potestio L
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2785-2793
Published Date: 19 December 2022
Rural, Regional, Racial Disparities in Telemedicine Use During the COVID-19 Pandemic Among US Adults: 2021 National Health Interview Survey (NHIS)
Park JH, Lee MJ, Tsai MH, Shih HJ, Chang J
Patient Preference and Adherence 2023, 17:3477-3487
Published Date: 20 December 2023