Back to Journals » Clinical Ophthalmology » Volume 20
Implementation and Clinical Application of 24-Hour Intraocular Pressure Monitoring in China: A Nationwide Survey
Authors Hu M, Liu T, Yao K ![]() , Wang Z, Chen M, Wang K
, Wang Z, Chen M, Wang K
Received 22 October 2025
Accepted for publication 24 January 2026
Published 17 February 2026 Volume 2026:20 572357
DOI https://doi.org/10.2147/OPTH.S572357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mengyuan Hu,1– 4 Tong Liu,1– 4 Ke Yao,1– 4 Zongrong Wang,5,6 Min Chen,1– 4 Kaijun Wang1– 4
1Eye Center of Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Provincial Key Laboratory of Ophthalmology, Hangzhou, Zhejiang, People’s Republic of China; 3Zhejiang Provincial Clinical Research Center for Eye Diseases, Hangzhou, Zhejiang, People’s Republic of China; 4Zhejiang Provincial Engineering Institute on Eye Diseases, Hangzhou, People’s Republic of China; 5Huanjiang Laboratory, State Key Laboratory of Silicon and Advanced Semiconductor Materials, Zhejiang University School of Aeronautics and Astronautics, Hangzhou, People’s Republic of China; 6Key Laboratory of Soft Machines and Smart Devices of Zhejiang Province, Hangzhou, People’s Republic of China
Correspondence: Kaijun Wang, Eye Center of Second Affiliated Hospital, School of Medicine, Zhejiang University, No. 1 Xihu Avenue, Shangcheng District, Hangzhou, Zhejiang, People’s Republic of China, Tel +86-571-87783907, Email [email protected] Min Chen, Eye Center of Second Affiliated Hospital, School of Medicine, Zhejiang University, No. 1 Xihu Avenue, Shangcheng District, Hangzhou, Zhejiang, People’s Republic of China, Tel +86-571-87783907, Email [email protected]
Purpose: To evaluate the nationwide implementation and clinical application of 24-hour intraocular pressure (IOP) monitoring in China.
Methods: A nationwide descriptive cross-sectional study was conducted from September 2024 to March 2025. Two structured questionnaires were distributed to 467 hospitals across China (400 valid responses) and 170 patients recruited from our institution who were undergoing 24-hour IOP monitoring for the first time. Collected data included implementation rates, tonometer types, measurement protocols, examiner consistency, and patient-reported perceptions.
Results: Among the 400 responding hospitals, 261 (65.3%) had implemented 24-hour IOP monitoring; however, 85.1% managed fewer than 20 patients per month. The most common measurement frequencies within a 24-hour period were 12 (37.2%), 6 (32.6%), and 7 times (27.2%), respectively. Non-contact tonometer (NCT) was the predominant device for both daytime (67.8%) and nighttime (64.6%) measurements. Among the 175 hospitals performing nocturnal measurements, only 7.4% employed supine positioning. In 65.5% of institutions, 24-hour IOP measurements for individual patients were performed by multiple nurses. Regarding patient perceptions, 95.8% considered 24-hour IOP monitoring important, yet 52.9% expressed reluctance to undergo the repeated procedure, citing hospitalization inconvenience (80%), sleep disruption (28.9%), concerns about measurement accuracy (4.4%), and cost (4.4%).
Conclusion: Although over half of the surveyed hospitals had implemented 24-hour IOP monitoring, overall clinical utilization remained suboptimal, with highly heterogeneous local protocols and considerable patient reluctance toward the current inpatient-based, nurse-dependent monitoring paradigm. Standardized implementation of national guidelines, enhanced patient education, and development of patient-centric, wearable IOP monitoring technologies are essential to optimize accessibility and support glaucoma management.
Keywords: glaucoma management, 24-hour intraocular pressure monitoring, nocturnal measurement, clinical implementation, nationwide survey, China
Introduction
Glaucoma is a chronic, progressive optic neuropathy characterized by the retinal ganglion cells degeneration and irreversible visual field loss.1 As a leading global cause of irreversible blindness, it is projected to affect approximately 111.8 million individuals aged 40–80 years by 2040.2 Elevated intraocular pressure (IOP) is the most well-established modifiable risk factor for disease progression, with substantial evidence highlighting that both absolute IOP levels and their fluctuations contribute to optic nerve damage.3,4
Given the pivotal role of IOP in disease pathogenesis, accurate and comprehensive IOP assessment is essential for diagnosis, treatment individualization, and prognosis evaluation. In routine clinical practice, IOP is predominantly measured as a single-point value during office hours using tonometers such as Goldmann applanation tonometry (GAT) or non-contact tonometers (NCTs).5 This conventional approach carries inherent limitations: IOP follows a circadian rhythm and exhibits short-term fluctuations influenced by posture, blood pressure, intracranial pressure, and diurnal activities.5–7 Notably, over 50% of glaucoma patients—particularly those with normal-tension glaucoma (NTG)—experience peak IOP outside regular clinic hours, a critical period missed by single-timepoint measurements.8–11 Moreover, growing evidence suggests that diurnal IOP variability, independent of mean IOP, is a strong predictor of glaucoma progression, further underscoring the inadequacy of relying solely on conventional, single-point office measurements.6,12
In response to these limitations, 24-hour IOP monitoring has emerged as a clinically valuable tool to capture the full circadian IOP profiles, including nocturnal peaks, daytime troughs, and fluctuation amplitudes, all of which are critical for informed clinical decision-making. Studies have demonstrated that 24-hour IOP monitoring not only facilitates diagnosis and effective IOP control but also contributes to the formulation of personalized therapeutic strategies.13 A comprehensive review by Konstas et al emphasized that diurnal and 24-hour IOP monitoring strategies significantly enhance prognosis assessment and treatment optimization in glaucoma management.12 Despite its recognized value, implementation practices vary widely.
In China, 24-hour IOP monitoring is primarily conducted through intermittent manual measurements during hospitalization.14 However, its real-world adoption, standardization of protocols—including measurement frequency, patient positioning, and tonometer type—and integration into routine glaucoma care remain poorly documented. Internationally, systematic evaluations of institution-based 24-hour IOP monitoring are also limited. Most existing surveys have focused on newer technologies such as contact lens sensors or home rebound tonometry, rather than on characterizing conventional inpatient monitoring practices.15,16 This global variability highlights the need for region-specific assessments to guide local clinical protocol optimization.
To date, no nationwide study in China has comprehensively examined current 24-hour IOP monitoring practices, including rates of institutional implementation, procedural heterogeneity, or patient perspectives. Therefore, we conducted the first nationwide descriptive cross-sectional survey to (1) evaluate the implementation status and clinical application patterns of 24-hour IOP monitoring in China, and (2) investigate patient perceptions, acceptance, and barriers to its adoption. Our findings aim to inform efforts toward protocol standardization, improve patient adherence, and guide the development of next-generation IOP monitoring technologies aligned with real-world clinical needs.
Materials and Methods
Study Design and Participants
This nationwide, cross-sectional study was conducted between September 2024 and March 2025 and comprised two parallel components: an institutional survey and a patient-based survey.
Institutional recruitment targeted public tertiary hospitals and private ophthalmic specialty hospitals across China. Primary and secondary public hospitals were excluded due to anticipated limitations in infrastructure and specialized personnel for 24-hour intraocular pressure (IOP) monitoring. To enhance broad geographic coverage, a convenience sampling strategy was applied across the eastern, central, and western regions of China.
Potential institutions were initially identified through a combination of the official national hospital registry and referrals from regional ophthalmological society networks. Invitations and the institutional questionnaire were then distributed electronically via the professional online survey platform Wenjuanxing (https://www.wjx.cn),17 using a peer-to-peer dissemination strategy within these established professional networks. Regional coordinators, who were senior ophthalmologists in each region, supervised questionnaire distribution and data quality control. Each participating institution was permitted to submit a response only once, completed by the head of the glaucoma service or a designated senior clinician.
Sample Size Calculation and Response
The minimum required sample size was calculated to be 96 institutions, based on an assumed 24-hour IOP monitoring implementation rate of 50%, a margin of error of 10%, and a 95% confidence level. To compensate for potential non-response, the recruitment target was set at 110 hospitals. In total, 467 hospitals meeting the eligibility criteria were identified and approached. Ultimately, 400 valid institutional responses were received and included in the analysis, yielding a response rate of 85.6%.
Patient Recruitment and Survey
In parallel, a patient survey was conducted at a single, large-volume tertiary eye center in our institution, selected for its established, high-volume protocol for inpatient 24-hour IOP monitoring. This center was chosen to ensure access to a sufficient and representative cohort of patients undergoing the procedure as part of their standard clinical care. A convenience sample of 170 patients was recruited from the center’s glaucoma service.
Eligible participants were adults (aged ≥ 18 years) with suspected glaucoma, ocular hypertension, or established glaucoma requiring treatment reassessment, who were consecutively admitted for their first 24-hour IOP monitoring. Participants voluntarily completed the paper-based questionnaire immediately following the final IOP measurement of their 24-hour monitoring cycle, ensuring that their perceptions and feedback were captured while the experience was fresh and relevant.
Questionnaire Design and Data Collection
Two separate questionnaires were developed for the institutional and patient survey components (Supplementary Figures S1 and S2). Item generation and refinement followed a multi-stage process: an initial draft was created by a multidisciplinary panel of glaucoma specialists, a clinical epidemiologist, and an ophthalmic nurse, all experienced in 24-hour IOP monitoring. This draft was refined through a two-round Delphi process involving seven experts from tertiary centers across China. Both questionnaires were then pilot-tested (15 institutional staff; 20 patients) to optimize clarity and relevance.
The institutional questionnaire covered: implementation status; operational protocols (tonometer type, measurement frequency, posture, staffing); service volume and fees; and perceived barriers. To facilitate recall and completion, quantitative items used predefined ordinal categories (eg, 1–10, 11–20 patients/month). It was completed by the glaucoma service head or a designated senior clinician at each site.
The patient questionnaire assessed: prior awareness and information sources; acceptance and willingness; perceived barriers (discomfort, cost, time); and overall satisfaction. For barrier-related items (eg, Question 6), multiple selections were permitted. Patients completed the paper questionnaire with the coordinator’s assistance immediately after their final 24-hour IOP measurement.
The study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of the Second Affiliated Hospital, Zhejiang University School of Medicine (Approval No.: 2022-Research-1051). Written informed consent was obtained from all participants before data collection.
Statistical Analysis
All statistical analyses were performed using SPSS version 23.0 and GraphPad Prism version 9.0. As all questionnaire responses were collected using predefined ordinal categories or nominal options (eg, “1–10” or “11–20” patients per month; “≤ 5 years” or “6–10 years” since implementation), all variables were analyzed as categorical or ordinal. Descriptive statistics are presented as frequencies and percentages.
Comparisons between public tertiary hospitals and private ophthalmic hospitals were conducted using Pearson’s chi-square test or Fisher’s exact test, as appropriate. These comparisons included key categorical variables such as implementation rate, monthly patient volume, service fees, device types, measurement schedules, patient positioning, and examiner staffing arrangements. For ordered categories variables (eg, duration since implementation), the Cochran–Armitage chi-square test for trend was applied after excluding responses with an open-ended option (eg, “≥ 10 years”) and “unknown”. For questions allowing multiple selections (eg, Question 6: reasons for reluctance), each response option was treated as a separate binary variable, and its selection frequency is reported as a proportion of respondents.
Questionnaires missing key grouping variables (eg, institution type/implementation status for institutional surveys; patient age/awareness for patient surveys) were excluded from the respective comparative analysis. An available-case approach was used for handling item-level non-response. A two-tailed p-value < 0.05 was considered statistically significant.
According to the Glaucoma Group of the Chinese Ophthalmological Society, the standard six-point IOP monitoring schedule includes measurement at 05:00, 07:00, 10:00, 14:00, 18:00, and 22:00.14 For analyses involving nocturnal IOP, this schedule was excluded, as the 22:00 and 05:00 time points fall outside the physiological sleep window (00:00–04:00) and were therefore not considered representative of true nocturnal IOP.
Results
General Characteristics and Implementation Rates
A total of 467 hospitals were invited to participate, of which 400 returned valid questionnaires, yielding a response rate of 85.6%. Respondents comprised 250 (62.5%) public tertiary hospitals and 150 (37.5%) private ophthalmic specialty hospitals. Geographically, responses were distributed across mainland China (Figure 1), with 205 (51.2%) institutions in the eastern region, 121 (30.3%) in the central region, and 87 (18.5%) in the western region.
 |
Figure 1 Geographic distribution of surveyed hospitals. Distribution of participating hospitals across China’s eastern, central, and western regions (N = 400). |
Overall, 261 of the 400 responding hospitals (65.3%) reported currently offering 24-hour IOP monitoring services. A significant difference in adoption rate was observed between hospital types (p < 0.01). Private ophthalmic hospitals demonstrated a higher implementation rate (74.7%,112/150) compared to public tertiary hospitals (59.6%, 149/250) (Figure 2A).
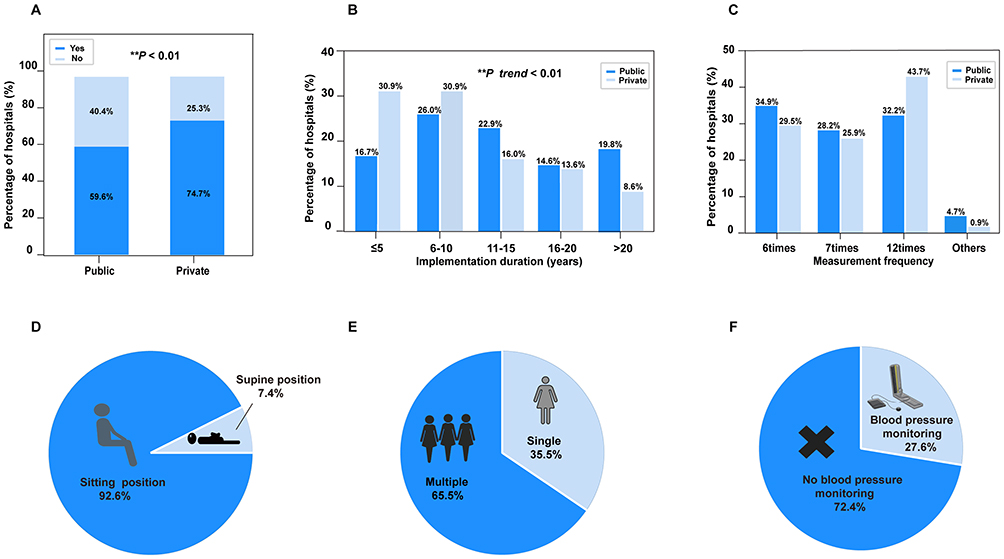 |
Figure 2 Practice patterns of 24-hour intraocular pressure (IOP) monitoring in Chinese hospitals. (A) Implementation rate by hospital type (public tertiary vs private). (B) Implementation duration by hospital type. (**p < 0.01). (C) Measurement frequencies of 24-hour IOP monitoring. (D) Body position during nocturnal IOP assessment (sitting vs supine). (E) Examiner pattern for a single patient (single vs multiple examiners). (F) Blood pressure monitoring during 24-hour IOP monitoring. |
A significant difference in the implementation duration of 24-hour IOP monitoring was observed between hospital types (n=177; p trend = 0.006). Public tertiary hospitals were more likely to be classified into longer-duration categories (eg, “≥10 years”), while private hospitals were predominantly in the shorter-duration categories (eg, “<10 years”, Figure 2B).
Patient Volume and Service Fees
Among the 261 hospitals that offered 24-hour IOP monitoring, the majority (85.1%) reported a monthly service volume of fewer than 20 patients. A detailed breakdown showed that 57.1% managed between 1–10 patients per month, while only 6.1% served more than 30 patients monthly (Table 1).
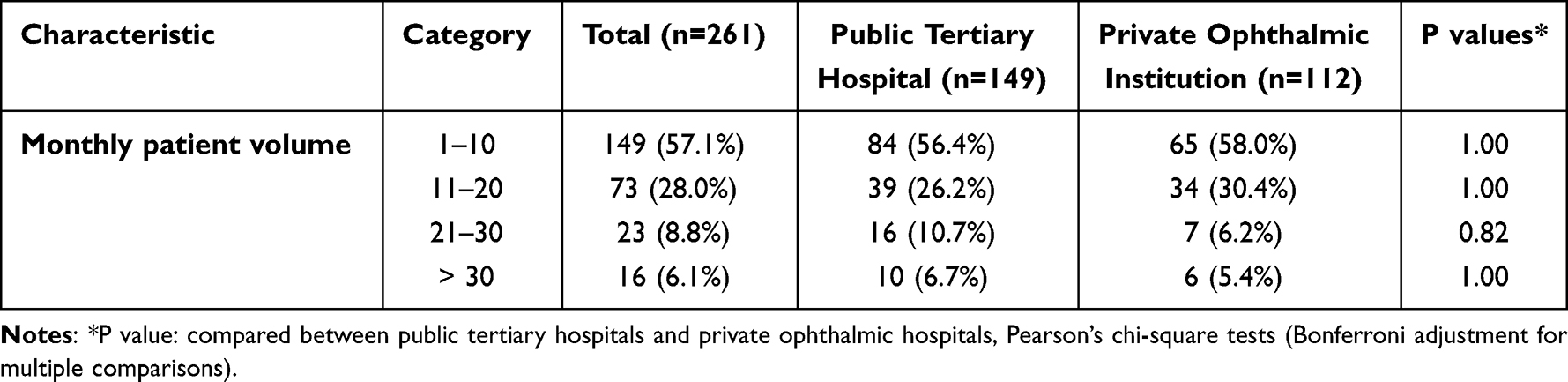 |
Table 1 Patient Volume for 24-Hour Intraocular Pressure Monitoring |
Regarding service fees, most institutions (51.7%) charged less than 28 USD (200 RMB) for the procedure, with 39.9% setting fees between 28–70 USD (200–500 RMB). Fewer than 10% of hospitals charged more than approximately 70 USD (500 RMB, Table 2). No statistically significant differences in patient volume distribution or service pricing were observed between public tertiary hospitals and private institutions.
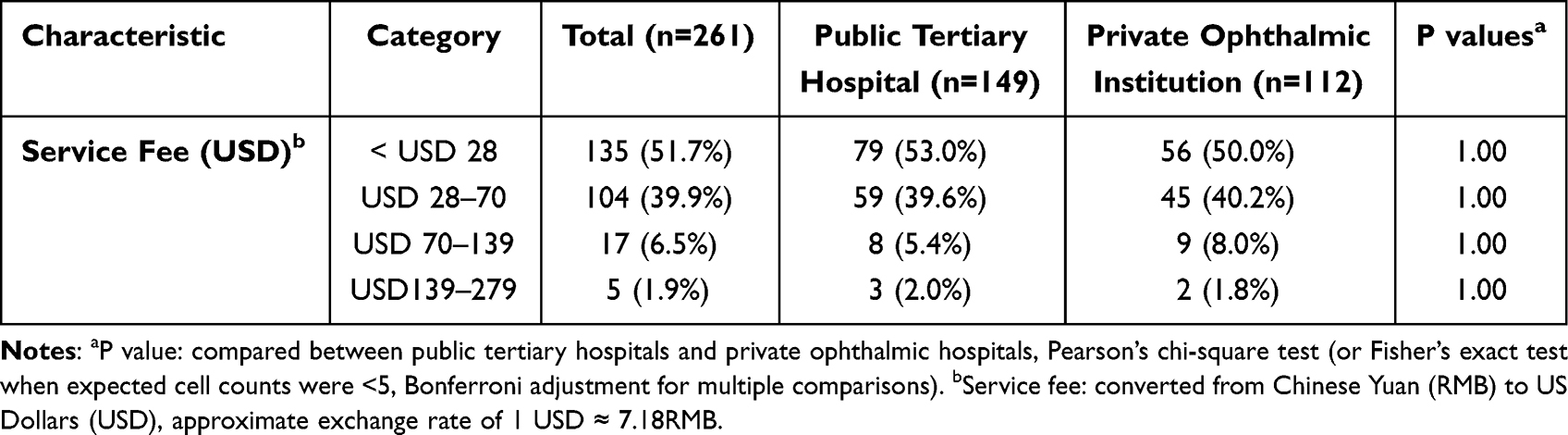 |
Table 2 Service Fees for 24-Hour Intraocular Pressure Monitoring |
Measurement Protocols
Measurement Frequency
Among hospitals performing 24-hour IOP monitoring, the most common measurement frequency was 12 times (37.2%), followed by 6 times (32.6%) and 7 times (27.2%). The use of other frequencies (eg, 8, 10, or 11 times) was uncommon. While private ophthalmology institutions most frequently reported using a 12-time protocol (43.7%), public hospitals more commonly employed a 6-time protocol (34.9%). This difference in preference did not reach statistical significance (Figure 2C).
Devices and Patient Positioning
The choice of tonometer for 24-hour IOP monitoring varied significantly between daytime and nocturnal periods, and between public and private institutions. During daytime measurements, the overall profile of tonometer use differed significantly between settings (p < 0.01). Public hospitals predominantly used the NCT (74.5%), while private institutions used it less frequently (58.9%) in favor of a higher rate of iCare Rebound Tonometer use (24.1% vs 10.7% in public hospitals, Table 3).
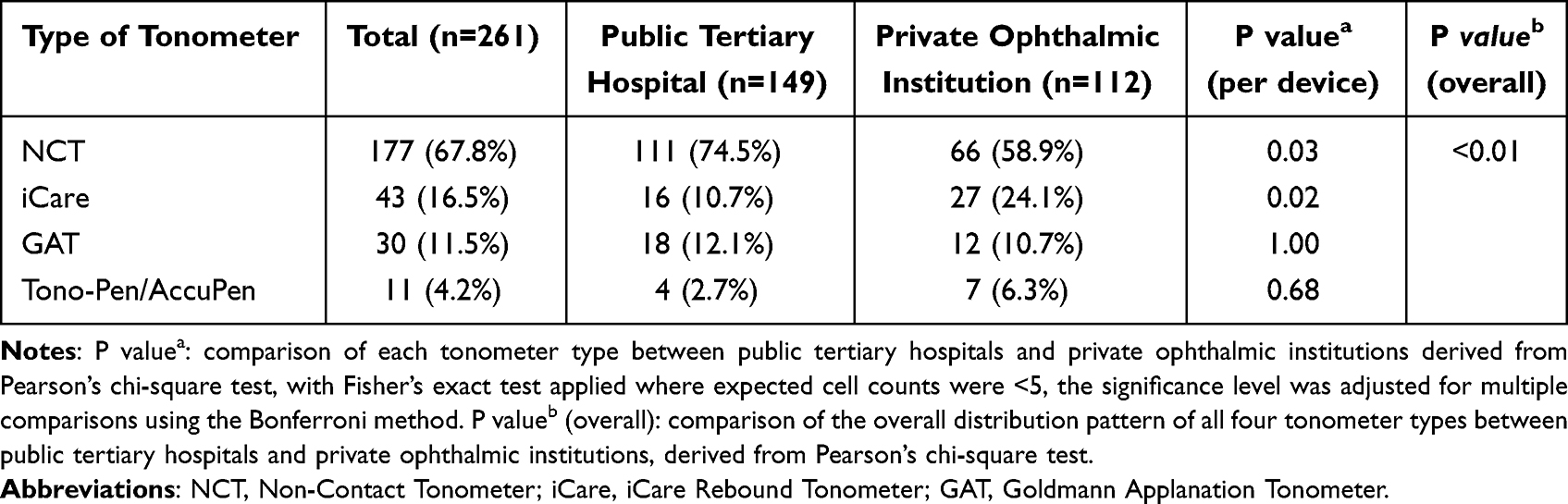 |
Table 3 Tonometers Used for Daytime Measurement in 24-Hour Intraocular Pressure Monitoring |
In contrast, nocturnal measurements revealed a consistent and non-significant pattern across both institution types (overall p=0.57), with the NCT being the dominant device (public: 66.7%; private: 62.0%) and no significant differences found for any specific tonometer (Table 4).
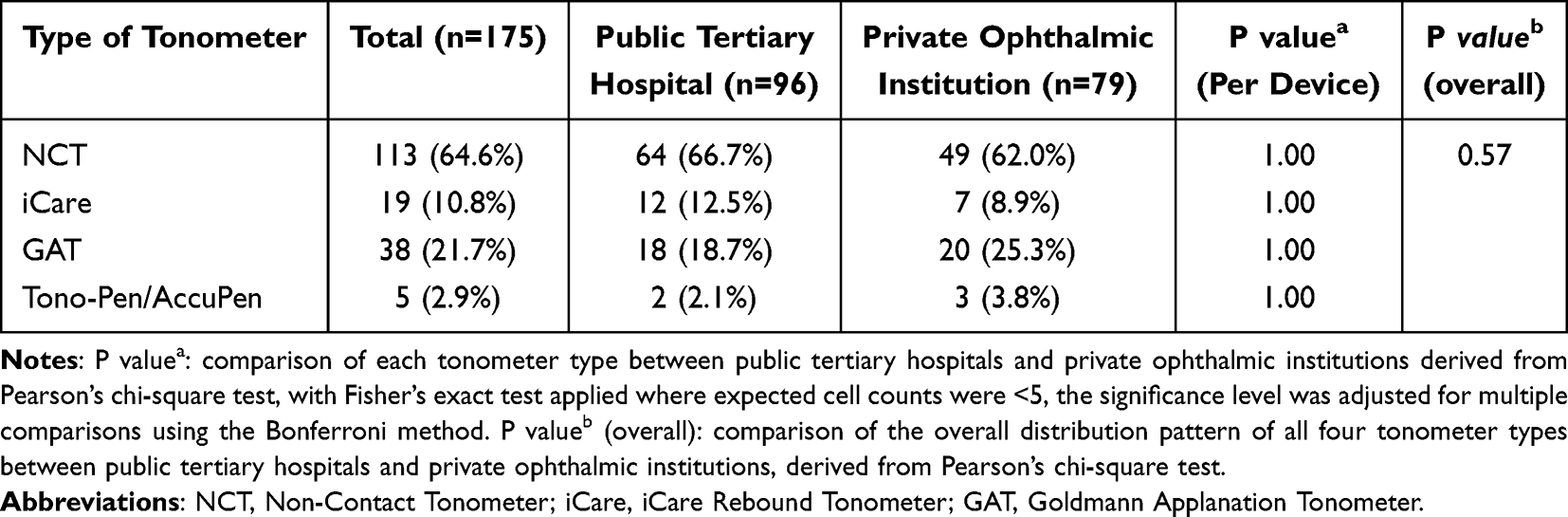 |
Table 4 Tonometers Used for Nocturnal Measurement in 24-Hour Intraocular Pressure Monitoring |
Regarding patient positioning during nocturnal measurements, despite established evidence that IOP increases in the supine position,18 only 7.4% (13/175) of institutions performed measurements with patients lying down. The vast majority (92.6%) assessed nocturnal IOP with patients in the seated position, a practice that may underestimate true nocturnal IOP (Figure 2D).
Staffing Patterns and Ancillary Monitoring
The staffing model for 24-hour IOP monitoring predominantly involved multiple nursing staff performing measurements at different time points for an individual patient (65.5% of institutions). In contrast, a single on-call physician conducting all measurements was reported by only 35.5% of hospitals (Figure 2E).
Regarding ancillary monitoring, 27.6% of institutions performed simultaneous blood pressure (BP) monitoring during the IOP assessment (Figure 2F). This practice reflects a clinical recognition of the role of hemodynamic fluctuations in glaucoma pathophysiology.19,20
Perceived Patient Demand and Clinical Value
Institutions generally reported a moderate perceived demand for 24-hour IOP monitoring among their glaucoma patients. Over half of public hospitals (56.4%) and nearly half of private hospitals (45.5%) rated the demand as “moderate”. An additional 13.4% of public hospitals and 18.8% of private hospitals categorized it as “high”, while 26.2% and 29.5%, respectively, described demand as “low”. The extreme response categories (“very high” or “no demand”) were rarely chosen (Figure 3A).
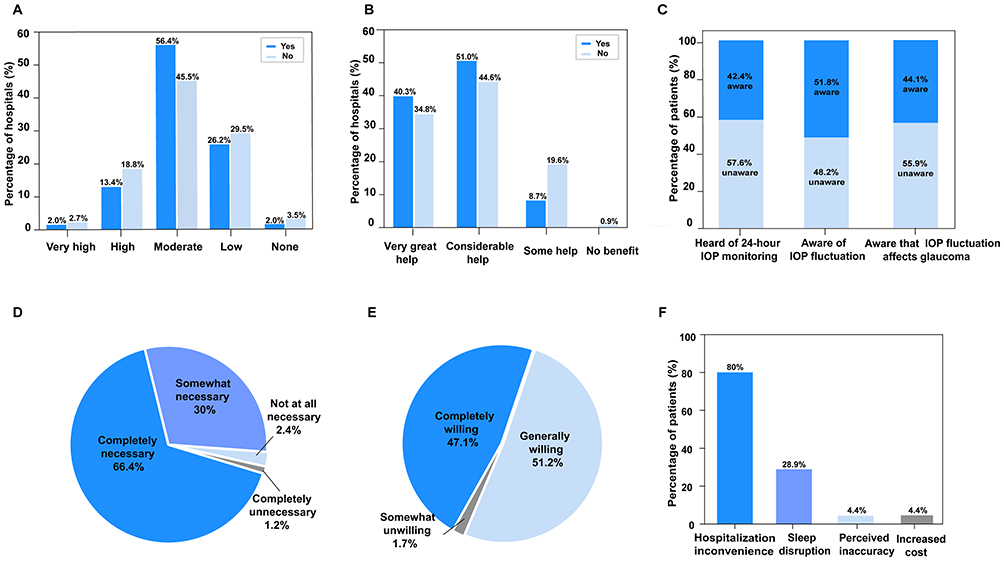 |
Figure 3 Institutional and patient perspectives on 24-hour intraocular pressure (IOP) monitoring. (A) Perceived patient demand for 24-hour IOP monitoring by hospital type. (B) Perceived necessity for inclusion of 24-hour IOP monitoring. (C) Patient awareness of diurnal IOP fluctuation,the impact of IOP variability on glaucoma progression,and 24-hour IOP monitoring, (N = 170). (D) Patients’ perceived clinical necessity of 24-hour IOP monitoring. (E) Patient acceptance and willingness to undergo the current protocol. (F) Primary reasons for patient reluctance to undergo the current protocol (N=90, multiple responses allowed). |
In contrast, institutions held highly positive views regarding the clinical value of the procedure. An overwhelming majority considered it beneficial for glaucoma management: 79.4% of private hospitals and 91.3% of public hospitals rated the benefit as “very great” or “considerable”. Almost all remaining respondents indicated “some” benefit. Only one private hospital (0.9%) reported no perceived benefit (Figure 3B).
Patients’ Awareness and Acceptance
A total of 170 patients participated in the survey, of whom 48.2% were unaware that IOP fluctuates over the day, 55.9% lacked knowledge regarding the impact of IOP variability on glaucoma progression, and 57.6% had never heard of 24-hour IOP monitoring prior to their current admission (Figure 3C). After receiving a brief explanation of the procedure, the majority (66.4%) perceived it as highly necessary, and 30% considered it moderately necessary (Figure 3D).
Despite this perceived necessity, a substantial proportion of patients (52.9%, 90/170) were unable to fully accept the current inpatient protocol, reporting only “generally willing” or “somewhat unwilling” (Figure 3E). Among those reluctant, the most frequently cited concerns were the inconvenience of hospitalization (80%), sleep disruption (28.9%), perceived inaccuracy (4.4%), and increased cost (4.4%) (Figure 3F).
Discussion
To our knowledge, this is the first nationwide survey to comprehensively evaluate the implementation patterns and clinical integration of 24-hour IOP monitoring in China. While the diagnostic and therapeutic value of 24-hour IOP monitoring is well documented, its real-world adoption and standardization remain poorly characterized.9,21 Our findings reveal a critical paradox: although institutional availability is relatively high, routine clinical utilization is limited, and protocols are highly heterogeneous, significantly constraining its potential clinical impact.
In our survey, approximately two-thirds (65.3%, 261/400) of surveyed hospitals reported offering 24-hour IOP monitoring. Private ophthalmic institutions demonstrated a significantly higher adoption rate than public tertiary hospitals (74.7% vs 59.6%, p < 0.01), whereas public hospitals tended to have longer-established services. This discrepancy likely reflects differing institutional drivers: private hospitals, operating in a competitive market, may prioritize innovative, patient-attracting services, whereas public tertiary centers often face constraints from rigid reimbursement systems, such as Diagnosis-Related Group (DRG) payments, which may not explicitly compensate for the additional resources required for 24-hour monitoring.22
Despite this availability, clinical uptake was strikingly low, with over 85% of implementing hospitals managing fewer than 20 patients per month. This is likely due to multifaceted barriers. On the supply side, the procedure is resource-intensive, requiring inpatient admission and dedicated staffing. On the demand side, patient awareness was a major issue. Over half (57.6%) of the 170 surveyed patients were unaware of the procedure prior to the current admission. This finding, though seemingly contradictory given that all respondents had just undergone monitoring, underscores a critical communication gap: patients may be admitted for “glaucoma assessment” without receiving a clear, prior explanation of the specific 24-hour monitoring protocol, its rationale, and its distinct value compared to a single clinic measurement. This highlights a need for improved patient education prior to admission.
A further disconnect emerged between perceived clinical value and patient demand. While the vast majority of institutions (91.3% of public hospitals) rated 24-hour IOP monitoring as providing “very great” or “considerable” benefit, most described patient demand as only “moderate”. This mismatch likely stems from patient-reported barriers identified in our parallel survey—over half of patients were reluctant to repeat the procedure, chiefly due to hospitalization inconvenience (80%) and sleep disruption (28.9%). Thus, the current inpatient monitoring model, despite its clinical value, appears to suppress patient acceptance and dampen perceived demand. Moving forward, optimizing the real-world utility of 24-hour IOP monitoring will require transitioning toward less-disruptive, outpatient-based, or wearable solutions that align better with patient tolerability and lifestyle.
A major barrier to reliability is the profound lack of protocol standardization. All institutions relied on manual intermittent measurements, with schedules varying from 6 to 12 times per 24 hours. Such intervals may miss transient IOP peaks or subtle fluctuations. Furthermore, despite physiological evidence recommending supine positioning for nocturnal measurements,23 only 7.4% of institutions followed this practice, with the majority (92.6%) measuring seated. This represents a significant implementation gap that can lead to underestimation of true nocturnal IOP. Operator inconsistency also introduces error, as 65.5% of hospitals used multiple nurses for measurements on the same patient. Technical variations in applanation or rebound tonometry can significantly affect readings.24 These issues underscore an urgent need for national guidelines and standardized training.
Given the resource intensity of inpatient monitoring, practical alternatives are often employed in clinical practice. Shorter office-hour diurnal tension curves provide a snapshot of daytime fluctuations. The water-drinking test (WDT), a one-hour provocative test, has been shown to induce IOP peaks that correlate strongly with those observed during longer diurnal curves in patients with open-angle glaucoma, offering a time-efficient surrogate for assessing IOP peak propensity.25,26 However, these methods cannot replace the comprehensive circadian profiling and detection of off-hour (e.g., nocturnal) peaks that are uniquely provided by full 24-hour monitoring when such data are critical for glaucoma diagnosis and management.
Technological innovations aim to bridge these gaps. Home rebound tonometers (eg, iCare HOME) enable outpatient self-monitoring but are limited by intermittent sampling, and, notably, most models do not permit reliable supine measurements, restricting nocturnal assessment.27 Contact lens sensors (e.g., Triggerfish®) represent a leap toward continuous monitoring but face challenges including patient discomfort, sleep disturbance, relative (not absolute) IOP reporting, and limited regulatory approval and access in many regions, including China.15,28 The ideal solution—a comfortable, calibrated, continuous IOP monitor suitable for long-term ambulatory use—remains an unmet need.
Taken together with our findings, these observations have several implications for clinical practice and future directions. National efforts should focus on standardizing protocols (specifying frequency, nocturnal supine positioning, and single-examiner consistency) through evidence-based guidelines and training. To increase patient acceptance, improved pre-procedure education and less burdensome models (e.g., structured day-curves) should be implemented. Reimbursement pathways within current payment systems should be established to incentivize adoption. Finally, the gap between high perceived clinical value and low patient uptake highlights the urgent need for investment in next-generation, patient-friendly technologies capable of accurate, continuous, or frequent IOP profiling in ambulatory settings.
This study has several limitations. First, the patient survey was conducted at a single high-volume tertiary center in a developed region, which may limit the generalizability of the findings to rural or resource-limited settings. Second, hospital sampling relied on a convenience sampling and focused on tertiary public and private specialty hospitals, thereby excluding primary and secondary care centers due to their anticipated low prevalence of 24-hour IOP monitoring services. While this sampling strategy enhances clinical relevance of the data for advanced ophthalmic practice, it may overestimate national implementation rates and introduce selection bias. Finally, our analysis was based on the reported use of tonometer categories but did not capture the specific device models or their technical capabilities for supine measurement. This limitation prevents a definitive assessment of whether the observed low rate of supine nocturnal monitoring was attributable to equipment constraints or to clinical protocol adherence. Consequently, these findings should be interpreted as representative of settings where such service is most feasible. Future studies involving a broader range of healthcare tiers, geographic regions, and more granular device specifications are warranted to provide a more comprehensive understanding.
Conclusion
This nationwide survey reveals that while 24-hour IOP monitoring is widely available in China, its effective implementation is constrained by multifaceted factors. Hospitals acknowledge its clinical value yet face operational and reimbursement challenges, whereas patients report low awareness and high reluctance due to hospitalization inconvenience and sleep disruption. The primary barrier is thus not insufficient clinical utility, but the lack of a feasible and patient-centered implementation framework. Future efforts should focus on developing practical clinical guidelines, optimizing monitoring models, and advancing patient-friendly technologies to integrate circadian IOP assessment into routine glaucoma care.
Abbreviations
IOP, intraocular pressure; NCT, non-contact tonometer; iCare, iCare Rebound Tonometer; GAT, Goldmann Applanation Tonometer; RMB, Renminbi; USD, United States Dollar; BP, blood pressure.
Acknowledgments
The authors sincerely thank all participating hospitals and patients for their invaluable contributions to this study. We are also grateful to Xiaoning Yu and Xin Liu for their dedicated assistance with the statistical analysis. Furthermore, we also acknowledge the insightful comments and constructive feedback provided by peer reviewers.
Funding
Supported by the Key Research and Development Program of Zhejiang Province (2025C02154).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jonas JB, Aung T, Bourne RR, et al. Glaucoma. Lancet. 2017;390:2183–11.
2. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–2090.
3. Jayaram H, Kolko M, Friedman DS, et al. Glaucoma: now and beyond. Lancet. 2023;402:1788–1801.
4. Rezapour A, Mansouri G, Chauhan DP, et al. Relationship between intraocular pressure fluctuation and visual field progression rates in the United Kingdom glaucoma treatment study. Ophthalmology. 2024;131:893–901.
5. Mansouri K, Tanna AP, De Moraes CG, et al. Review of the measurement and management of 24-hour intraocular pressure in patients with glaucoma. Surv Ophthalmol. 2020;65:171–186.
6. Kim JH, Cho J. Intraocular pressure fluctuation: is it important? J Ophthalmic Vis Res. 2018;13:170–174. doi:10.4103/jovr.jovr_35_18
7. Lin JN, Ebinger P, Hofer A, et al. Posture-related fluctuations of intraocular pressure in healthy children with suspicion of glaucoma. Graefes Arch Clin Exp Ophthalmol. 2024;262:45–54.
8. Liu T, Chen Y, Huang M, et al. The impact of intraocular pressure fluctuations on the progression of glaucoma and associated factors. Adv Ophthalmol Pract Res. 2025;5:100062.
9. Chen CH, Wong JKW. Role of 24-hour intraocular pressure monitoring in glaucoma management. J Ophthalmol. 2019;2019:3632197. doi:10.1155/2019/3632197
10. Tan S, Bhandari N, Ho L, et al. Comparison of self-measured diurnal intraocular pressure profiles using rebound tonometry between primary angle closure glaucoma and primary open angle glaucoma patients. PLoS One. 2017;12:e0173905.
11. Wu X, Konieczka K, Liu X, et al. Role of ocular blood flow in normal tension glaucoma. Adv Ophthalmol Pract Res. 2022;2:100036.
12. Konstas AG, Kahook MY, Araie M, et al. Diurnal and 24-h intraocular pressures in glaucoma: monitoring strategies and impact on prognosis and treatment. Adv Ther. 2018;35:1775–1804.
13. Tsironi S, Almaliotis D, Ntonti P, et al. Clinical outcomes of the implementation of IOP monitoring, in and out of office time, to 1500 patients—a cohort study. Vision. 2022;6:69.
14. Beijing Medical Association Ophthalmology Branch. Discussion on the standardization of 24-hour intraocular pressure monitoring [in Chinese]. Zhonghua Yan Ke Za Zhi. 2014;50:384–385.
15. Otsuka M, Hayashi A, Tojo N, et al. Questionnaire survey on complications during 24-h measurement of intraocular pressure-related patterns with a contact lens sensor. Int Ophthalmol. 2020;40:1963–1968. doi:10.1007/s10792-020-01370-z
16. Alagappan U, Stewart C, Azuara-Blanco A, et al. Which glaucoma patients should be monitored at home and exploration of clinician perceptions on home monitoring? A survey of glaucoma specialists in the UK. BMJ Open. 2024;14:e080873.
17. Su L, Lin Z, Li Y, et al. Autism spectrum disorder knowledge scale: chinese revision of the general population version. BMC Psychiatry. 2023;23(1):66. doi:10.1186/s12888-023-04538-w
18. Erb P, Schmid C, Schulze S, et al. Dependency of intraocular pressure on body posture in glaucoma patients: new approaches to pathogenesis and treatment. Ophthalmologe. 2020;117:702–708.
19. De Moraes R, Jonas AA, Greenfield DS, et al. Relationship between blood pressure and rates of glaucomatous visual field progression: the vascular imaging in glaucoma study. Ophthalmology. 2025;132:34–42.
20. Hartmann A, Scholz I, Hoffmann EM, et al. Change of intraocular pressure over 5 years and its relationship to cardiovascular parameters: results from the Gutenberg Health Study. Invest Ophthalmol Vis Sci. 2024;65:12.
21. Bhartiya S, Gangwani M, Kalra RB, et al. 24-hour intraocular pressure monitoring: the way ahead. Rom J Ophthalmol. 2019;63(4):315–320. doi:10.22336/rjo.2019.50
22. Du L, Fang S, Zhang Q. Trend analysis of medical expenses under DRG payment reform in China. Sci Rep. 2025;15(1):36961. doi:10.1038/s41598-025-20902-0
23. Sang Q, Xin C, Yang D, et al. Effect of different postures on intraocular pressure in open-angle glaucoma. Ophthalmol Ther. 2024;13:149–160. doi:10.1007/s40123-023-00845-3
24. Bormann P, Schultz ML, Ziemssen M, et al. How to measure intraocular pressure: an updated review of various tonometers. J Clin Med. 2021;10:3860. doi:10.3390/jcm10173860
25. Mohammed SW, Adio AO, Ejimadu CSS, et al. Comparative evaluation of modified diurnal tension curve with water drinking test among glaucoma suspects. J Clin Ophthalmol Res. 2024;12(3):267–272. doi:10.4103/jcor.jcor_80_24
26. Yap TE, Gao Y, Ahmad H, et al. Comparison of intraocular pressure profiles during the water drinking test and the modified diurnal tension curve. Eye. 2024;38(8):1567–1574. doi:10.1038/s41433-024-02954-0
27. Cvenkel B, Atanasovska Velkovska M. Self-monitoring of intraocular pressure using Icare HOME tonometry in clinical practice. Clin Ophthalmol. 2019;13:841–847. doi:10.2147/OPTH.S198846
28. Dunbar GE, Shen BY, Aref AA. The Sensimed Triggerfish contact lens sensor: efficacy, safety, and patient perspectives. Clin Ophthalmol. 2017;11:875–882. doi:10.2147/OPTH.S109708
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023