Back to Journals » International Journal of General Medicine » Volume 16
Impact of Transcutaneous Electrical Acupoint Stimulation on BDNF Expression and IVF Outcomes in Patients with Infertility
Authors Zhou X, Li Y, Chen J, Fang Z, Kong W, Wen J, Zhang Q
Received 16 August 2023
Accepted for publication 23 November 2023
Published 7 December 2023 Volume 2023:16 Pages 5751—5762
DOI https://doi.org/10.2147/IJGM.S435701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xueyuan Zhou, Yan Li, Jun Chen, Zhou Fang, Wei Kong, Ji Wen, Qiyao Zhang
Reproductive Medical Center, The Second Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250000, People’s Republic of China
Correspondence: Ji Wen; Qiyao Zhang, Reproductive Medical Center, The Second Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250000, People’s Republic of China, Tel +86 531-82436297, Email [email protected]; [email protected]
Purpose: Transcutaneous electrical acupoint stimulation (TEAS) can be used in patients with infertility. This study explored the impact of TEAS on brain-derived neurotrophic factor (BDNF) levels and in-vitro fertilization (IVF) outcomes in patients with infertility.
Patients and Methods: This quasi-experimental study included infertile women undergoing IVF and embryo transfer (IVF-ET) at one hospital between January 2018 and December 2021. The TEAS group received TEAS before IVF, while the placebo group received mock stimulation. The primary outcomes were serum and follicular fluid (FF) BDNF expression levels. Finally, 510 and 518 participants were included in TEAS and placebo groups.
Results: The serum (P< 0.001) and FF (P< 0.001) BDNF expression levels were higher in the TEAS group than in the placebo group. The TEAS group had a lower total dose of gonadotropins (P=0.007), higher fertilization rates (P=0.006), higher high-quality embryo rates (P=0.013), and higher pregnancy rates per ET (P=0.031). The subgroup analysis showed that the Val/Val genotype was associated with the differences in serum and FF BDNF between the TEAS and placebo groups (all P< 0.05).
Conclusion: In conclusion, TEAS might increase serum and FF BDNF expression levels and improve IVF embryological and clinical outcomes. Patients with the Val/Val genotype might be more likely to benefit from TEAS.
Keywords: transcutaneous electrical acupoint stimulation, brain-derived neurotrophic factor, infertility, in-vitro fertilization, embryo transfer, quasi-experimental study
Introduction
The prevalence of infertility is 15–20% in women of reproductive age worldwide and is the third most common condition that seriously affects family harmony and social cohesion.1 Infertility is difficult to manage because the etiology of human infertility is complex and involves intrinsic and extrinsic factors. Infertility outcomes have been greatly improved by in vitro fertilization and embryo transfer (IVF-ET), but the pregnancy rate of IVF-ET still hovers around 50%. Therefore, safe, effective, and economical methods to improve the success rate of assisted reproductive technology (ART) are important.2 Acupuncture is now increasingly accepted as a complementary therapy for infertility because of its multi-level, multi-targeted, and comprehensive treatment characteristics. Acupuncture in adjuvant interventions can significantly improve IVF-ET outcomes.3–5 Han’s Acupoint Nerve Stimulator (HANS) is a portable device for administering transcutaneous electrical acupoint stimulation (TEAS) treatment, avoiding needles, and can be used in patients with infertility.6
Still, the available literature on acupuncture for infertility is limited to describing the phenomenological aspects. Acupuncture might first activate the peripheral nerves to generate action potentials, transmit them to the central nerves at all levels,7 and then trigger the neuro-endocrine system.8 The brain-derived neurotrophic factor (BDNF) is known for its widespread expression in the nervous systems and for maintaining and regulating neuronal survival, differentiation, and growth.9,10 BDNF and the tyrosine kinase type B (TrkB) receptor, which exhibits a high affinity to BDNF, are expressed in gonadotropin-releasing hormone (GnRH) expressing neurons, ductless glands, and ovaries of adult mammals.11–13 BDNF participates in female fertility14,15 as a component of the local ovarian microenvironment and physiological processes such as follicle development and ovulation.16 Plasma and follicular fluid (FF) BDNF levels change dynamically during the menstrual cycle in fertile women or during controlled ovarian stimulation in IVF.17–19 BDNF is indispensable in promoting oocyte maturation and early human embryo development.12,20–25 Reduced FF BDNF levels might be a reason for low IVF-ET pregnancy rates.26
A single nucleotide polymorphism (SNP) in BDNF (Val66Met) leads to impaired BDNF intracellular transportation and reduced activity-dependent secretion, effectively affecting the ability to increase BDNF levels in response to external stimuli.27 Patients homozygote for Val66Met require significantly higher doses of gonadotrophin during IVF treatment. Still, these patients show low mature oocyte numbers, fertilization rates, and high-quality embryo numbers, and poor pregnancy outcomes.26
At present, there were no previous studies on the influence of the BDNF Val66Met SNP on the therapeutic effect of TEAS in infertility. Therefore, this study explored the impact of TEAS on BDNF levels and IVF outcomes in infertility patients with different BDNF Val66Met genotypes. The findings of this study could provide clinical evidence and theoretical guidance for the individualized application of TEAS in the treatment of female infertility and in the IVF-ET process from the perspective of modern medicine.
Materials and Methods
Study Design and Participants
This quasi-experimental study included infertile women at the Reproductive Medical Center of one hospital between January 2018 and December 2021. The inclusion criteria were 1) diagnosed with infertility for the lack of success in conceiving after >12 consecutive months of unprotected sex,28 2) 22–38 years of age, 3) Han ethnicity, and 4) scheduled for IVF-ET. The exclusion criteria were 1) history of abdominal or pelvic surgery, ovarian tuberculosis, or other conditions that could lead to severe ovarian dysfunction, 2) received ICSI therapy because of male fertility factors, or 3) chromosome abnormalities in either spouse.
This study was conducted according to the guidelines of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of the hospital (***). The participants provided written informed consent after being informed of the purpose, content, potential benefits, risks, trial group settings, possible interventions they will receive, and responsibilities associated with the study. The participants had the right to drop out of this study at any time, for any reason, without losing any rights or care to which they were entitled.
Recruitment Strategies and Enrollment
At present, a large number of infertile patients are seeking treatments at Chinese hospitals. Subjects were recruited in the following methods: 1)Spending time in a waiting room area hoping to run into patients that might be eligible for our study. 2) Asking colleagues to give us names of potential Subjects for our study. 3) Looking through our department’s clinical database for potential study subjects, then contacting them. 4) Recruiting through advertisements placed via local media (television and newspaper) and recruitment posters in the reproductive center of our hospital.
Interested patients will be screened by trained recruiters who have detailed understanding of the trial aims, who are very familiar with the study inclusion and exclusion criteria, and who appeal to altruism. Patients who are willing to participate and meet the eligibility criteria will be referred to the acupuncturist at the hospitals.
Randomization and Allocation Concealment
The randomization sequence will be generated by a computerized random number generator using the simple randomization method (Excel, Microsoft Office 2016). A “patients” database will be generated, listing basic information such as patient names and contact details, as well as a “randomization” database containing data on patients enrolled in the trial and their allocations. Any researcher can access the “patients” database, while the “randomization” database is password-protected; therefore, it will be accessible only by the principal investigator and a nominated computer technician. Prior to the intervention, the acupuncturist will immediately access the “patients” database, type in the patient’s name and details, and click on the icon to randomize the patient. This act will lead to a dialog box asking the researcher to confirm that the patient is eligible. After pressing the “OK” button, patient information is automatically sent to the randomization database, where randomization takes place. Grouping information will subsequently be sent to the acupuncturists for TEAS or placebo TEAS treatments.
As far as possible, the procedure will be carried out by blinded staff; All tests were administered by examiners blind to the grouping of the participants. All data were analyzed by third-party statisticians who were not part of the study staff. The participants will be blinded because the placebo group obtained placebo TEAS. However, the acupuncturists will not be blinded.
Intervention
The participants were allocated to the TEAS and placebo groups according to their orders of admission. The participants in the TEAS group received electrical stimulation (2 Hz, 20–25 mA) for 30 min/day for three menstrual cycles before the IVF cycle (artificial induction of menstrual cycle by Western medicine as a complementary therapy). Each menstrual cycle of treatment was administered from the 3rd day of a menstrual period to the beginning of the next one. The HANS −200A TEAS instrument (Nanjing Jisheng Medical Technology Co., Ltd., China) was used to stimulate the following acupoints: Guanyuan (RN4), Zhongji (RN3), bilateral Sanyinjiao (SP6), bilateral Zigong (EX-CA1), bilateral Tianshu (ST25), bilateral Shenshu (BL23), Yaoyangguan (DU3), and Mingmen (DU4) (Supplementary Figure S1).
In the placebo group, the placebo HANS, which is identical in appearance to the HANS device, was used. Irrespective of the information displayed on the device, its current strength is always maintained at 5 mA (the minimum stimulation that can barely cause a numbing sensation under the acupoints), and it remains on for 3 s and off for 7 s so that the patient feels some electrical current. This strategy helps achieve the placebo effect of the treatment without really delivering therapy. The acupoint selection and course of treatment were the same for the placebo and TEAS groups.
Follicle Stimulation and Oocyte Harvest
The participants in the two groups underwent a standard GnRH-antagonist (GnRH-ant) protocol. Recombinant human follicle-stimulating hormone (FSH) (75 IU, Recombinant Human Follitropin Injection, GONAL-f®, Merck Serono S.p.A., Italy, specification) was administered on menstrual cycle day 3 (MCD3) based on antral follicle count, serum basic sexual hormone levels and BMI. Adjustments of the gonadotropin dose were made based on follicular growth, characterized by transvaginal ultrasound and serum concentration of E2. On day 5 or 6 of gonadotropin stimulation, subcutaneous injections of GnRH-ant (0.25 mg, cetrorelix acetate powder for injection, Cetrotide®, Merck Serono S.p.A., Idron, France) were administered daily up to and including the day of human chorionic gonadotropin (hCG) administration. hCG (Lizhu Ltd., Guangdong, China) at a dose of 5000–10,000 IU was administered when ≥2 follicles possessed a mean diameter of 18 mm or ≥3 follicles exhibited a mean diameter of 17 mm. Oocyte retrieval was performed 36 h later via transvaginal follicular aspiration. Conventional IVF was performed for all participants.
Routine embryo quality examination assessed the number of blastomeres, degree of fragmentation, and blastomere uniformity. Depending on the patient’s situation and the availability of embryos, ≤2 embryos would be transferred, or all embryos would be frozen on the 3rd or 5th day after oocyte retrieval. Progesterone (Xianju Ltd., Zhejiang, China) was supplemented to support the luteal phase.
Outcomes and Measurement
The primary outcome was the serum and FF BDNF levels. The secondary outcomes were the total dose of gonadotropins, days of stimulation, number of mature oocytes, fertilization rate, high-quality embryo rate, pregnancy rate per ET, and implantation rate.
Mature oocytes were defined as oocytes in which the polar body emerged within 4–6 h post-insemination. The fertilization rate was calculated by dividing the number of oocytes having two pronuclei by the total number of oocytes/cycle. High-quality embryo was defined as embryos generated from normal inseminated oocytes with no or ≤1/3 fragmentation, no multinucleation, 3–5 or more blastomeres 48 h after the oocyte was harvested, and ≥7 blastomeres 72 h after oocyte retrieval were regarded as high-quality embryos. The high-quality embryo rate was calculated by dividing the number of high-quality embryos by the total number of embryos retrieved. The pregnancy rate was obtained by dividing the total number of clinical pregnancy cycles by the number of IVF cycles in which fresh embryo transfer was performed. The implantation rate was determined by dividing the total number of gestation sacs by the number of embryos transferred/group. Clinical pregnancy was determined by ultrasound visualization of fetal heartbeat in a gestation sac. Patients were followed up based on a telephone contact at 6 weeks after ET to determine pregnancy and the number of gestation sacs. Clinical and laboratory data will be collected from the IVF center databases. Data on acupuncture safety and any adverse events will be collected from practitioner treatment records.
Genotype Analysis
Peripheral blood samples were collected and centrifuged to separate the leukocytes. Genomic DNA was isolated by the saturated potassium iodide method. All genotyping assays were conducted using the fluorescence resonance energy transfer (FRET) method using a Light Cycler 2.0 (Roche Diagnostics, Germany). According to the results of the melting curve analysis, peaks for the Met-allele and Val-allele were acquired at 588°C and 658°C, respectively. In order to observe the impact of the BDNF Val66Met SNP on the therapeutic outcomes of TEAS, all participants were subgrouped based on the BDNF genotypes: BDNF Val/Val subgroup, BDNF Val/Met subgroup, and BDNF Met/Met subgroup.
Plasma and Follicular Fluid BDNF Levels
Blood was sampled between 08:00 and 08:30 on MCD3 before and after treatment with TEAS/placebo. The samples were centrifuged to isolate the plasma stored at −80°C. FF was obtained during the routine oocyte retrieval and centrifuged. The supernatant was stored at −80°C. The BDNF levels were measured using the BDNF Emax Immunoassay System (BDNF Emax® ImmunoAssay System, Promega, USA) following the provider’s instructions. Briefly, 96-well plates were coated with anti-BDNF monoclonal antibody overnight at 4°C. Then, the wells were blocked with blocking buffer and incubated with follicular fluid or plasma samples and standards at room temperature for 2h. Anti-human BDNF polyclonal antibody was used as reporter antibody, and the amount of specifically bound polyclonal antibody was detected using the anti-IgY-horseradish peroxidase conjugate. After incubation with the chromogenic substrate and stopping of the reaction with 1 N hydrochloric acid, the absorbency was measured at 450 nm by using a microplate reader (Model 680 microplate reader, Bio-Rad Laboratories Ltd, CA, USA). All samples were assayed in duplicates. Serum BDNF levels collected on MCD3 and FF BDNF levels are defined as MCD3-BDNF and FF-BDNF levels, respectively.
Statistical Analysis
On the basis of pretesting, we calculated that group sample sizes of 928 patients (464 in TEAS group; 464 in placebo group) would provide 90% power to reject the null hypothesis of equal means when the mean difference is 49 with standard deviations of 240 for TEAS group and 220 for placebo group at a two-sided alpha of 0.05. Given an anticipated dropout rate of 15%, total minimum sample size required is 1092 (546 in TEAS group; 546 in placebo group).
All statistical analyses were performed using SPSS 26.0 (IBM, Armonk, NY, USA). The continuous variables were tested using the Kolmogorov–Smirnov test. Those with a normal distribution were shown as means ± standard deviation (SD). Differences among three or more groups were examined using one-way analysis of variance (ANOVA), followed by multiple comparisons using the least significant difference (LSD)-t-test to identify the groups showing significant differences. Differences between two groups were tested using the independent-sample Student’s t-test. The continuous variables with a abnormal distribution were shown as medians (ranges) and tested using Wilcoxon’s rank-sum test. Categorical variables were displayed as n (percentages) and analyzed using the chi-square test. Repeated ANOVA was used to analyze serum BDNF at different time points between groups. Subgroup analysis was done in patients with different BDNF Val66Met genotypes. A two-sided P <0.05 was considered statistically significant. All of the analyses will be based on a treated-per-protocol analysis (TPP).
Results
Baseline Characteristics and BDNF Genotypes
Between January 2018 and December 2021, 1608 patients were screened for eligibility. Of them, 168, 188, and 21 patients were excluded for severe ovarian dysfunction, intracytoplasmic sperm injection (ICSI) therapy because of male fertility factors, and chromosome abnormalities in either spouse. A total of 1100 participants met the inclusion criteria and were divided into the TEAS group (n=550) or the placebo group (n=550). Forty participants in the TEAS group and 32 participants in the placebo group were not included in the statistical analysis due to spontaneous pregnancy (n=3 and n=2), choosing another protocol of controlled ovarian hyperstimulation (COH) (n=5 and n=7), failure to adhere to the doctor-prescribed treatment (n=19 and n=14), failure to obtain test data (n=10 and n=7), and loss to follow-up (n=3 and n=2). Finally, 510 (240, 165, and 105 with the Val/Val, Val/Met, and Met/Met genotypes) and 518 (243, 174, and 101 with the Val/Val, Val/Met, and Met/Met genotypes) participants were included in the TEAS and placebo groups, respectively (Figure 1). There were no significant differences in age, duration of infertility, body mass index (BMI), and basal follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), progesterone (P), and testosterone (T) levels between the TEAS and placebo groups and among the subgroups (all P>0.05) (Table 1).
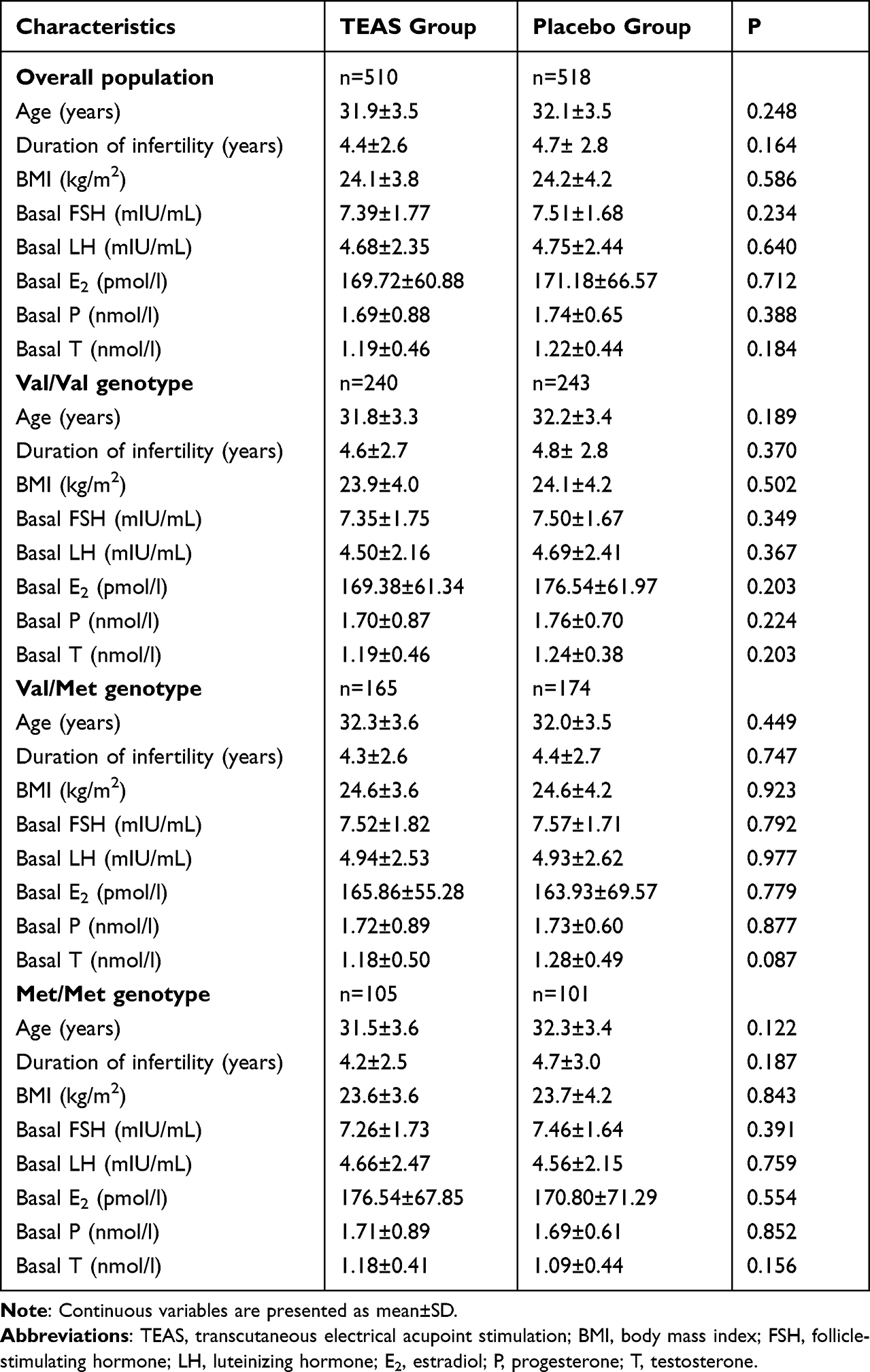 |
Table 1 Characteristics of the Participants |
 |
Figure 1 Study flowchart. |
BDNF Levels in the TEAS and Placebo Groups
The serum BDNF expression levels were different between the TEAS and placebo groups (P<0.001) and varied over time (P<0.001). Besides, the FF BDNF levels during ovum pick-up (OPU) were higher in the TEAS group compared with the placebo group (768.36±246.68 vs 714.50±221.67, P<0.001) (Table 2).
 |
Table 2 Primary Outcomes |
In the Val/Val genotype subgroup, the serum BDNF levels were also different between the TEAS and placebo groups (P<0.001) and varied over time (P<0.001). The FF-BDNF levels during OPU were also higher in the TEAS group compared with the placebo group (847.99±252.33 vs 784.79±214.27, P=0.003).
In the Val/Met and Met/Met subgroups, the serum BDNF levels varied over time (both P<0.001), while there were no significant differences between the TEAS and placebo groups. In the Val/Met genotype subgroup, the FF-BDNF levels during OPU were higher in the TEAS group compared with the placebo group (759.04±217.20 vs 697.02±212.78, P=0.008).
Embryological and Pregnancy Outcomes
A total of 145 and 157 participants in the TEAS and placebo groups canceled embryo transfer because of a high risk of ovarian hyperstimulation syndrome (OHSS) (n=96 and n=91), fever (n=2 and n=3), high P levels or poor endometrium quality (n=14 and n=20), no available embryos (n=27 and n=38), and other personal factors (n=6 and n=5) (Figure 1). Finally, transfer was completed in 365 and 361 participants in the TEAS and placebo groups, respectively: 178 and 168 in the Val/Val subgroup, respectively, 117 and 123 in the Val/Met subgroup, respectively, and 70 and 70 in the Met/Met subgroup, respectively.
In the overall population, the participants in the TEAS group had a lower total dose of gonadotropins (2146.35±693.00 vs 2267.18±730.10 UI, P=0.007), higher fertilization rates (71.5±20.1 vs 67.9 ±22.5, P=0.006), higher high-quality embryo rates (55.3±25.0 vs 51.3±26.4, P=0.013), and higher pregnancy rates per ET (54.5% vs 46.3%, P=0.031).
In the Val/Val genotype subgroup, the participants in the TEAS group had lower total doses of gonadotropins (2019.74±644.43 vs 2149.95±696.45 UI, P=0.034), higher numbers of mature oocytes (12.6±6.4 vs 11.5±6.2, P=0.048), higher fertilization rates (74.8±18.0 vs 70.1±22.4, P=0.012), higher high-quality embryo rates (59.0±25.7 vs 54.1±26.3, P=0.039), and higher implantation rates (43.6% vs 35.4, P=0.038).
In the Val/Met and Met/Met subgroups, the embryological and pregnancy outcomes were not significantly different between the TEAS and placebo groups (all P>0.05) (Table 3).
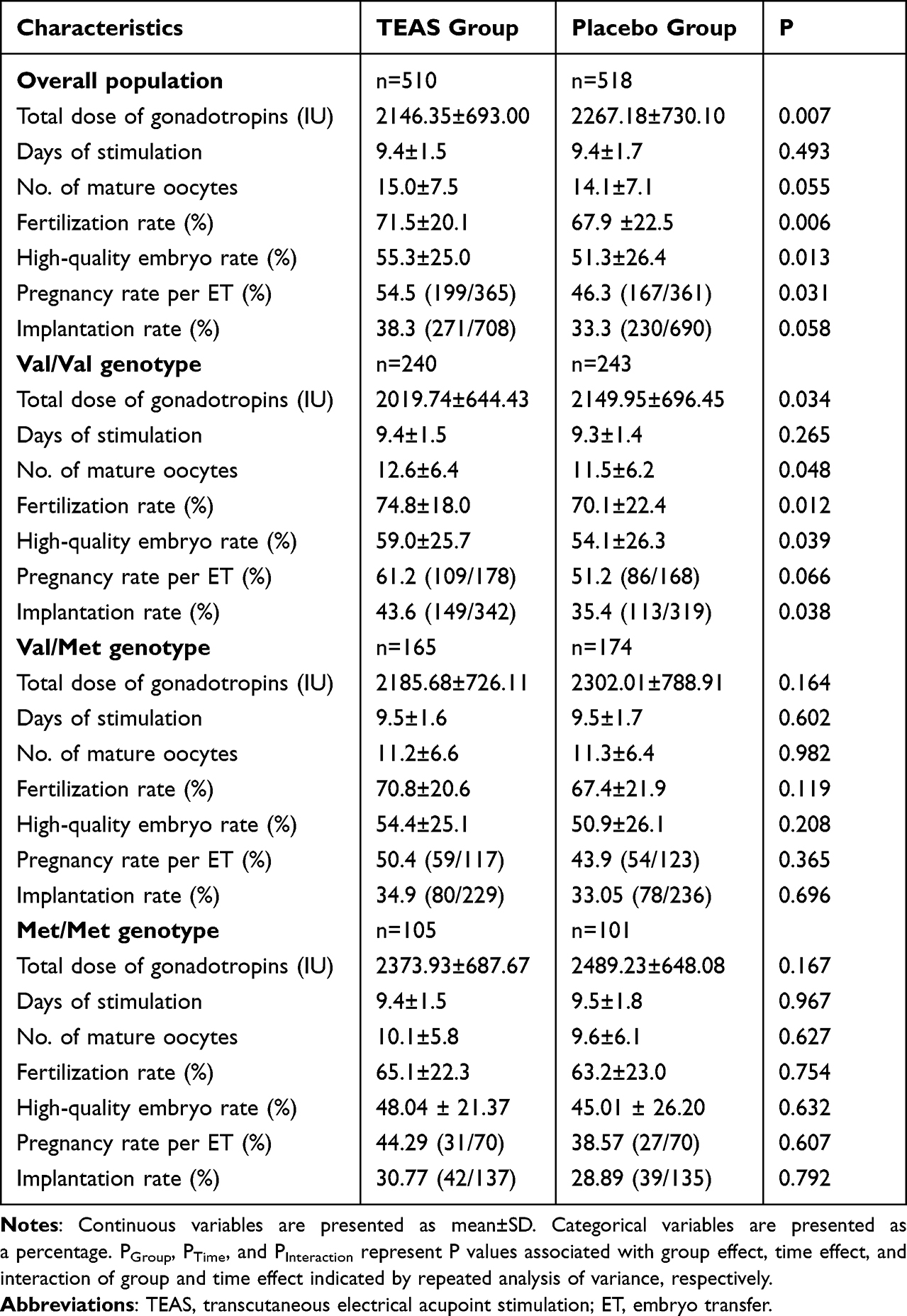 |
Table 3 IVF Outcomes Patients Between TEAS and Placebo Group |
Discussion
This study suggests that TEAS can increase serum and FF BDNF levels and improve IVF embryological and clinical outcomes. The presence of the BDNF Val66Met allele appears to inhibit the effect of TEAS, and the participants with Val/Val genotype were more likely to benefit from TEAS. The findings might provide clinical evidence and theoretical guidance for the popularization of TEAS in treating female infertility and during the IVF-ET process.
The theory of Traditional Chinese Medicine (TCM) purports that the sperm-ovum-embryo axis in assisted reproductive technology is closely related to the essence of the kidney. “kidney sperm storage and reproduction”. Because of IVF-ET patients have poor status of reproductive function, resulting in a deficiency of kidney essence. TCM mainly focuses on tonifying the kidney and improving its essence. According to a systematic review, the selected acupoints were mainly for tonifying the kidney before IVF, the highly frequently used acupuncture points are Guanyuan (RN4), Zhongji (RN3), Sanyinjiao (SP6), Zigong (EX-CA1), Tianshu (ST25), Shenshu (BL23), Yaoyangguan (DU3), and Mingmen (DU4).29 The RN4 and RN3 acupoints belong to the Ren Meridian, both located on the abdomen and have the effect of invigorating the kidney for regulating menstruation. DU3 and DU4 belong to the Du Meridian; both are located on the back and have the effects of warming and recuperating kidney yang. Both pairs of acupoints are useful for treating diseases of the reproductive system. SP6 belongs to the spleen Meridian of Foot-Taiyin and has the effect of replenishing kidney essence, cooperating with ST25, which belongs to the stomach Meridian of Foot-Yangming and has the effects of regulating spleen and stomach to replenish congenital foundation, to treat gynecological and obstetric diseases such as irregular menstruation, dysmenorrhea, and infertility. BL23 is the acupoint of the Bladder Meridian of Foot-Taiyang, cooperating with EX-CA1 to improve the patient’s uterine environment and help embryo implantation.30 With the clinical experience of our principal investigator and co-investigators, the above acupoints are effective for the treatment of infertility. TEAS take acupoints as a starting point and exerts curative effects by means of electrical nerve stimulation, which is the organic combination of syndrome differentiation and the treatment of TCM and modern science and technology. In this study, among all participants, those in the TEAS group had a lower total dose of gonadotropins, higher fertilization rates, higher high-quality embryo rates, and higher pregnancy rates per ET compared with the placebo group. These findings are supported by previous findings. Indeed, a study showed that acupuncture could enhance the expression of BDNF,27 and TEAS could improve the number of oocytes retrieved and the rates of pregnancy, implantation, and live birth.31–37
A good pregnancy outcome is dependent on good-quality follicles. The FF is the environment in which the oocytes are in direct contact with the cytokines, which have a strong influence on the development and maturation of the oocytes. The FF BDNF levels in women treated with IVF positively correlated with the mature oocyte number.25 It serves as a marker for the quality of oocytes and infertility.38 BDNF can increase the glutathione content in oocytes23,39 and the antioxidant capacity of the cells, promoting oocyte survival and reducing apoptosis.40 Moreover, it can promote the first polar body extrusion,23 affect the meiotic process, spindle morphology, and positioning and rearrangement of cortical granules in mature oocytes in vitro,41 and enhance nuclear and cytoplasmic maturation of the oocytes.23,42,43 TEAS can effectively increase the level of BDNF in the ovary and serum and regulate the local microenvironment of the ovary; it can, consequently, reduce gonadotropin requirement in the process of COH, enhance the maturation rate and quality of oocytes in vitro, improve fertilization rate, promote early embryo development and the formation of blastocysts,26,44 and increase the rates of high-quality embryos and pregnancy, as observed in the present study.
The BDNF Val66Met polymorphism has been correlated with BDNF levels and IVF pregnancy outcomes in women,26,45 and the variant occurs in approximately 40–60% of Asians.27 In this study, 53% of the enrolled participants carried the BDNF Val66Met variant, which agrees with the frequency in Asians. The TEAS Val/Val subgroup showed higher serum BDNF and FF BDNF, lower gonadotropin dosage in the process of COH, higher mature oocyte number, and higher rates of fertilization rate, high-quality embryo, and implantation. These differences were partly lost in the Val66Met carriers. There were no previous studies on the influence of the BDNF Val66Met SNP on the therapeutic effect of TEAS in infertility. These results suggest that the BDNF Val66Met gene variants inhibit TEAS treatment from regulating BDNF concentrations and improving embryological and clinical outcomes of IVF. Still, the mechanisms are unknown, and the present study was not designed to explore them.
Adverse reactions of patients undergoing acupuncture mainly include cross infection, tissue and organ damage, physiological and psychological responses (such as weakness and allergic reactions), and other unforeseen conditions caused by clinical errors.46 TEAS could avoid adverse reactions caused by traditional acupuncture, such as infection, skin damage, and fainting.47 In this study, only 9 patients had mild allergic reactions at the electrode site during the follow-up of all patients performed.
This study has some limitations. First, due to time constraints, this study only observed the intermediate outcome indicators of IVF-ET and not the long-term outcomes. The next stage of the study will be to follow up on the relevant endpoint indicators, such as the live birth rate. Another key limiting factor was that this study mainly explored the effects of TEAS on BDNF levels and IVF pregnancy outcomes in infertility patients showing different BDNF Val66Met genotypes through clinical observation. The specific mechanisms of action still need to be investigated.
Despite the above limitations, this study has strengths. One strength is that the study used a HANS device to deliver TEAS. Unlike manual acupuncture, which achieves the therapeutic effect through manual needling, TEAS generates electrical pulses that stimulate the tissues at acupoints via self-adhesive electrodes attached to the skin surface. Compared with traditional manual acupuncture, TEAS has better reproducibility and easy operation. Another strength of the study was using placebo TEAS instead of sham acupuncture. Sham acupuncture has long been questioned as a control in acupuncture therapies because, in sham acupuncture, needles are inserted into tissues not corresponding to acupoints, which will inevitably generate physiological effects and thereby affect the interpretation of the acupuncture outcomes. Placebo TEAS, in contrast, can represent a better control because it generates no or negligible stimulation on acupoints with no therapeutic effects. Therefore, in the present study, placebo TEAS was adopted as a sham intervention to control for the possible impacts of psychological and physiological factors on BDNF levels and IVF outcomes in female infertility.
Conclusion
In conclusion, TEAS can increase serum and FF BDNF levels and improve IVF embryological and clinical outcomes. The presence of the BDNF Val66Met allele appears to inhibit the effect of TEAS, and patients with Val/Val genotype were more likely to benefit from TEAS.
Abbreviations
TEAS, transcutaneous electrical acupoint stimulation; BDNF, brain-derived neurotrophic factor; IVF, in-vitro fertilization; IVF-ET, in vitro fertilization and embryo transfer; FF, follicular fluid; ART, assisted reproductive technology; HANS, Han’s Acupoint Nerve Stimulator; TEAS, transcutaneous electrical acupoint stimulation; BDNF, brain-derived neurotrophic factor; TrkB, tyrosine kinase type B; GnRH, gonadotropin-releasing hormone; SNP, single nucleotide polymorphism; ICSI, intracytoplasmic sperm injection; GnRH-ant, GnRH-antagonist; FSH, follicle-stimulating hormone; MCD3, menstrual cycle day 3; Hcg, human chorionic gonadotropin; FRET, fluorescence resonance energy transfer; SD, standard deviation; ANOVA, analysis of variance; LSD, least significant difference.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and Supplementary Information.
Ethics Approval and Consent to Participate
This study was conducted according to the guidelines of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of Shandong University of Traditional Chinese Medicine Second Affiliated Hospital (approval #2017SDZYDEY-003). The participants provided written informed consent after being informed of the purpose, content, potential benefits, risks, alternatives, and responsibilities associated with the study. Participants had the right to drop out of this study at any time, for any reason, without losing any rights or care to which they were entitled.
Acknowledgments
We wish to convey our special thanks to John Xingqi Zhang, Ph.D., for his guidance in conceptualizing and designing the whole project. We also thank all the participants in this study. We also thank TopEdit (www.topeditsci.com) for their language polishing service on this manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (#81771557).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Qiao J, Li R. Fertility preservation: challenges and opportunities. Lancet. 2014;384(9950):1246–1247. doi:10.1016/s0140-6736(14)61749-9
2. Kyrou D, Kolibianakis EM, Venetis CA, Papanikolaou EG, Bontis J, Tarlatzis BC. How to improve the probability of pregnancy in poor responders undergoing in vitro fertilization: a systematic review and meta-analysis. Fertil Sterility. 2009;91(3):749–766. doi:10.1016/j.fertnstert.2007.12.077
3. Ng EH, So WS, Gao J, Wong YY, Ho PC. The role of acupuncture in the management of subfertility. Fertil Sterility. 2008;90(1):1–13. doi:10.1016/j.fertnstert.2008.02.094
4. Zheng CH, Zhang MM, Huang GY, Wang W. The role of acupuncture in assisted reproductive technology. Evid Based Complement Altern Med. 2012;2012:543924. doi:10.1155/2012/543924
5. Stener-Victorin E, Waldenström U, Nilsson L, Wikland M, Janson PO. A prospective randomized study of electro-acupuncture versus alfentanil as anaesthesia during oocyte aspiration in in-vitro fertilization. Hum Reprod. 1999;14(10):2480–2484. doi:10.1093/humrep/14.10.2480
6. Qu F, Li R, Sun W, et al. Use of electroacupuncture and transcutaneous electrical acupoint stimulation in reproductive medicine: a group consensus. J Zhejiang Univ Sci B. 2017;18(3):186–193. doi:10.1631/jzus.B1600437
7. Maeda Y, Kettner N, Lee J, et al. Acupuncture-evoked response in somatosensory and prefrontal cortices predicts immediate pain reduction in carpal tunnel syndrome. Evid Based Complement Alternat Med. 2013;2013:795906. doi:10.1155/2013/795906
8. Liu HR, Fang XY, Wu HG, et al. Effects of electroacupuncture on corticotropin-releasing hormone in rats with chronic visceral hypersensitivity. World J Gastroenterol. 2015;21(23):7181–7190. doi:10.3748/wjg.v21.i23.7181
9. Park H, Poo MM. Neurotrophin regulation of neural circuit development and function. Nat Rev Neurosci. 2013;14(1):7–23. doi:10.1038/nrn3379
10. Autry AE, Monteggia LM. Brain-derived neurotrophic factor and neuropsychiatric disorders. Pharmacol Rev. 2012;64(2):238–258. doi:10.1124/pr.111.005108
11. Russo N, Russo M, Daino D, et al. Evaluation of brain-derived neurotrophic factor in menstrual blood and its identification in human endometrium. Gynecol Endocrinol. 2012;28(6):492–495. doi:10.3109/09513590.2011.633667
12. Seifer DB, Feng B, Shelden RM, Chen S, Dreyfus CF. Brain-derived neurotrophic factor: a novel human ovarian follicular protein. J Clin Endocrinol Metab. 2002;87(2):655–659. doi:10.1210/jcem.87.2.8213
13. Smith MA, Makino S, Kim SY, Kvetnansky R. Stress increases brain-derived neurotropic factor messenger ribonucleic acid in the hypothalamus and pituitary. Endocrinology. 1995;136(9):3743–3750. doi:10.1210/endo.136.9.7649080
14. Bódis J, Sulyok E, Kőszegi T, Prémusz V, Várnagy Á, Koppán M. Serum and follicular fluid levels of serotonin, kisspeptin, and brain-derived neurotrophic factor in patients undergoing in vitro fertilization: an observational study: neurohormones in patients receiving IVF. Int J Med Res. 2020;48(4):300060519879330. doi:10.1177/0300060519879330
15. Dong F, Zhang Q, Kong W, et al. Regulation of endometrial cell proliferation by estrogen-induced BDNF signaling pathway. Gynecol Endocrinol. 2017;33(6):485–489. doi:10.1080/09513590.2017.1295439
16. Bernabé BP, Woodruff T, Broadbelt LJ, Shea LD. Ligands, receptors, and transcription factors that mediate inter-cellular and intra-cellular communication during ovarian follicle development. Reprod Sci. 2020;27(2):690–703. doi:10.1007/s43032-019-00075-8
17. Seifer DB, Lambert-Messerlian G, Schneyer AL. Ovarian brain-derived neurotrophic factor is present in follicular fluid from normally cycling women. Fertil Sterility. 2003;79(2):451–452. doi:10.1016/s0015-0282(02)04669-1
18. Monteleone P, Artini PG, Simi G, et al. Brain derived neurotrophic factor circulating levels in patients undergoing IVF. J Assist Reprod Genet. 2007;24(10):477–480. doi:10.1007/s10815-007-9169-y
19. Begliuomini S, Casarosa E, Pluchino N, et al. Influence of endogenous and exogenous sex hormones on plasma brain-derived neurotrophic factor. Hum Reprod. 2007;22(4):995–1002. doi:10.1093/humrep/del479
20. Streiter S, Fisch B, Sabbah B, Ao A, Abir R. The importance of neuronal growth factors in the ovary. Mol Hum Reprod. 2016;22(1):3–17. doi:10.1093/molehr/gav057
21. Kawamura K, Kawamura N, Fukuda J, Kumagai J, Hsueh AJ, Tanaka T. Regulation of preimplantation embryo development by brain-derived neurotrophic factor. Dev Biol. 2007;311(1):147–158. doi:10.1016/j.ydbio.2007.08.026
22. Kawamura K, Kawamura N, Mulders SM, Sollewijn Gelpke MD, Hsueh AJ. Ovarian brain-derived neurotrophic factor (BDNF) promotes the development of oocytes into preimplantation embryos. Proc Natl Acad Sci U S A. 2005;102(26):9206–9211. doi:10.1073/pnas.0502442102
23. Lee E, Jeong YI, Park SM, et al. Beneficial effects of brain-derived neurotropic factor on in vitro maturation of porcine oocytes. Reproduction. 2007;134(3):405–414. doi:10.1530/rep-06-0288
24. Linher-Melville K, Li J. The roles of glial cell line-derived neurotrophic factor, brain-derived neurotrophic factor and nerve growth factor during the final stage of folliculogenesis: a focus on oocyte maturation. Reproduction. 2013;145(2):R43–R54. doi:10.1530/rep-12-0219
25. Wang X, Sun Z, Zhen J, Yu Q. Brain-derived neurotrophic factor from follicular fluid is positively associated with rate of mature ooocytes collected and cleavage rate in intracytoplasmic sperm injection patients. J Assist Reprod Genet. 2011;28(11):1053–1058. doi:10.1007/s10815-011-9635-4
26. Zhang QY, Guan Q, Wang Y, et al. BDNF val66met polymorphism is associated with Stage III-IV endometriosis and poor in vitro fertilization outcome. Hum Reprod. 2012;27(6):1668–1675. doi:10.1093/humrep/des094
27. Lin D, De La Pena I, Lin L, Zhou SF, Borlongan CV, Cao C. The neuroprotective role of acupuncture and activation of the BDNF signaling pathway. Int J Mol Sci. 2014;15(2):3234–3252. doi:10.3390/ijms15023234
28. Carson SA, Kallen AN. Diagnosis and management of infertility: a review. JAMA. 2021;326(1):65–76. doi:10.1001/jama.2021.4788
29. Yang H, Hu WH, Xu GX, et al. Transcutaneous electrical acupoint stimulation for pregnancy outcomes in women undergoing in vitro fertilization-embryo transfer: a systematic review and meta-analysis. Front Public Health. 2022;10:892973. doi:10.3389/fpubh.2022.892973
30. Zhang LX, Zhao B, Wu J, et al. Effect of transcutaneous electrical acupoint stimulation on the clinical pregnancy rate and the live birth rate in in vitro fertilization-embryo transfer. Chin J Reprod Contracept. 2018;38:284–287.
31. Zhan XX, Cai HC, Wang Y, et al. Transcutaneous electrical acupoint stimulation improves pregnancy outcomes of in vitro fertilization- embryo transfer: a meta-analysis of randomized controlled trials. Zhonghua Nan Ke Xue. 2021;27(9):825–832.
32. Shuai Z, Li X, Tang X, Lian F, Sun Z. Transcutaneous electrical acupuncture point stimulation improves pregnancy outcomes in patients with recurrent implantation failure undergoing in vitro fertilisation and embryo transfer: a prospective, randomised trial. Acupunct Med. 2019;37(1):33–39. doi:10.1136/acupmed-2017-011483
33. Zhong J, Zhang L. [Transcutaneous electrical acupoint stimulation for pregnancy of in vitro fertilization-embryo transfer]. Zhongguo Zhen Jiu. 2017;37(3):253–255. Chinese. doi:10.13703/j.0255-2930.2017.03.008
34. Qu F, Wang FF, Wu Y, et al. Transcutaneous electrical acupoint stimulation improves the outcomes of in vitro fertilization: a Prospective, Randomized and Controlled Study. Explore. 2017;13(5):306–312. doi:10.1016/j.explore.2017.06.004
35. Hsu YC, Liang IT, Huang SY, Wang HS, Soong YK, Chang CL. Transcutaneous electrical acupoint stimulation (TEAS) treatment improves pregnancy rate and implantation rate in patients with implantation failure. Taiwan J Obstet Gynecol. 2017;56(5):672–676. doi:10.1016/j.tjog.2017.08.017
36. Zheng CH, Zhang J, Wu J, Zhang MM. The effect of transcutaneous electrical acupoint stimulation on pregnancy rates in women undergoing in vitro fertilization: a study protocol for a randomized controlled trial. Trials. 2014;15:162. doi:10.1186/1745-6215-15-162
37. Shuai Z, Lian F, Li P, Yang W. Effect of transcutaneous electrical acupuncture point stimulation on endometrial receptivity in women undergoing frozen-thawed embryo transfer: a single-blind prospective randomised controlled trial. Acupunct Med. 2015;33(1):9–15. doi:10.1136/acupmed-2014-010572
38. Giannini A, Bucci F, Luisi S, Cela V, Genazzani AR. Brain-derived neurotrophic factor in plasma of women with endometriosis. J Endometr. 2010;2(3):144–150.
39. Abazari-Kia AH, Dehghani-Mohammadabadi M, Mohammadi-Sangcheshmeh A, Zhandi M, Salehi M. Regulation of embryonic development and apoptotic-related gene expression by brain-derived neurotrophic factor in two different culture conditions in ovine. Theriogenology. 2015;84(1):62–69. doi:10.1016/j.theriogenology.2015.02.012
40. Anderson RA. Brainwork in the ovary: kisspeptin and BDNF signaling converge to ensure oocyte survival. Endocrinology. 2014;155(8):2751–2753. doi:10.1210/en.2014-1447
41. Zhang L, Li J, Su P, Xiong C. The role of brain-derived neurotrophic factor in mouse oocyte maturation in vitro. J Huazhong Univ Sci Technol Med Sci J. 2010;30(6):781–785. doi:10.1007/s11596-010-0658-3
42. Zhao X, Du F, Liu X, et al. Brain-derived neurotrophic factor (BDNF) is expressed in buffalo (Bubalus bubalis) ovarian follicles and promotes oocyte maturation and early embryonic development. Theriogenology. 2019;130:79–88. doi:10.1016/j.theriogenology.2019.02.020
43. Zhao P, Qiao J, Huang S, et al. Gonadotrophin-induced paracrine regulation of human oocyte maturation by BDNF and GDNF secreted by granulosa cells. Hum Reprod. 2011;26(3):695–702. doi:10.1093/humrep/deq390
44. Li C, Zhou X. The potential roles of neurotrophins in male reproduction. Reproduction. 2013;145(4):R89–R95. doi:10.1530/rep-12-0466
45. Frielingsdorf H, Bath KG, Soliman F, Difede J, Casey BJ, Lee FS. Variant brain-derived neurotrophic factor val66met endophenotypes: implications for posttraumatic stress disorder. Ann N Y Acad Sci. 2010;1208:150–157. doi:10.1111/j.1749-6632.2010.05722.x
46. Ernst E, White AR. Prospective studies of the safety of acupuncture: a systematic review. Am J Med. 2001;110(6):481–485. doi:10.1016/s0002-9343(01)00651-9
47. Zheng Y, Feng X, Mi H, et al. Effects of transcutaneous electrical acupoint stimulation on ovarian reserve of patients with diminished ovarian reserve in in vitro fertilization and embryo transfer cycles. J Obstet Gynaecol R. 2015;41(12):1905–1911. doi:10.1111/jog.12810
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.