Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Impact of the Charlson Comorbidity Index on the Short-Term and Long-Term Prognoses of Patients with Coronary Artery Disease Undergoing Percutaneous Coronary Intervention
Authors Ma Y, Luo H, Zhao H, Zhao O, Ma L ![]() , Yang W, Yi M, Sun L, Li J
, Yang W, Yi M, Sun L, Li J
Received 1 September 2025
Accepted for publication 28 December 2025
Published 14 January 2026 Volume 2026:22 559412
DOI https://doi.org/10.2147/TCRM.S559412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Yixin Ma, Hongyu Luo, Huan Zhao, Ou Zhao, Lina Ma, Wei Yang, Ming Yi, Lijie Sun, Jing Li
Department of Geriatrics, Xuanwu Hospital Capital Medical University, National Clinical Research Center for Geriatric Diseases, Beijing, 100053, People’s Republic of China
Correspondence: Jing Li, Department of Geriatrics, Xuanwu Hospital Capital Medical University, National Clinical Research Center for Geriatric Diseases, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Email [email protected]
Background: The Charlson Comorbidity Index (CCI) is widely used to assess comorbidity burden, its prognostic role in patients undergoing percutaneous coronary intervention (PCI) remains underexplored. This study aimed to investigate the impact of CCI on in-hospital adverse events and long-term major adverse cardiovascular and cerebrovascular events (MACCEs) in patients with coronary artery disease (CAD) treated with PCI.
Methods: A total of 572 consecutive CAD patients who underwent PCI between October 2016 and October 2020 were included. Patients were divided into low (CCI ≤ 4, n = 453) and high (CCI > 4, n = 119) comorbidity burden groups. Clinical characteristics, in-hospital adverse events, and long-term MACCEs were compared. Multivariate logistic regression and Cox proportional hazards models were used to identify independent predictors of outcomes.
Results: Compared to the low-CCI group, patients in the high-CCI group were older, more frequently male, and had higher rates of diabetes, left main CAD, and multivessel disease (all p < 0.05). In-hospital adverse events were significantly more common in the high-CCI group (13.4% vs 2.0%, p < 0.01). CCI was an independent predictor of in-hospital events (OR = 3.13; 95% CI: 1.40– 7.02). During a median follow-up of five years, the high-CCI group had a significantly higher incidence of MACCEs (51.3% vs 6.2%; HR = 2.72; 95% CI: 2.25– 3.30, p < 0.01).
Conclusion: CCI is a significant and independent predictor of both in-hospital and long-term adverse outcomes in CAD patients undergoing PCI.
Keywords: Charlson comorbidity index, coronary artery disease, percutaneous coronary intervention, in-hospital adverse events, major adverse cardiovascular and cerebrovascular events, prognostic evaluation
Introduction
Coronary artery disease (CAD) is a leading public health issue globally. According to a recent worldwide study, CAD accounted for 37.7% of all disability-adjusted life years attributable to cardiovascular diseases in 2021.1 Percutaneous coronary intervention (PCI) is currently the most commonly used revascularization strategy for CAD, and this method has significantly improved the clinical outcomes and quality of life of affected patients. However, despite the implementation of guideline-directed medical therapy, patients undergoing PCI remain at considerable risk for subsequent cardiovascular adverse events.2 Therefore, enhancing postoperative individualized risk stratification and optimizing secondary prevention strategies are essential for reducing the incidence of mid- to long-term adverse events. Various risk assessment tools have been widely applied in PCI patients, including the Global Registry of Acute Coronary Events (GRACE) score, the Synergy between PCI with TAXUS and Cardiac Surgery (SYNTAX) score, the residual SYNTAX score, the left ventricular ejection fraction (LVEF), and biomarkers such as the N-terminal prohormone of brain natriuretic peptide and high-sensitivity C-reactive protein. Each of these indicators offers specific advantages and is suited for distinct patient populations, aiding the development of personalized treatment plans. For example, the GRACE score is often used to predict short-term mortality and reinfarction risk in patients with acute coronary syndrome; the SYNTAX score evaluates coronary anatomical complexity to guide interventional strategies; and both the LVEF and biomarkers play important roles in assessing cardiac function and systemic inflammation. Nevertheless, for certain subgroups—such as older adults, patients with multiple comorbidities, or those with a history of repeated PCI—these scoring systems present notable limitations in real-world clinical practice. Hence, there is an urgent need for a simple, practical, and broadly applicable tool to achieve precise and individualized risk assessment and stratification in these populations.
The Charlson Comorbidity Index (CCI) is a widely used scoring system for assessing the burden of comorbidities. Originally developed in 1987 to predict 10-year mortality, the CCI has since demonstrated prognostic value for patients affected by a variety of chronic diseases, including chronic respiratory disease, chronic kidney disease, metabolic disorders, and malignancies. Patients with a high comorbidity burden often present with multiple systemic conditions, such as diabetes, chronic kidney disease, and hypertension—metabolic and inflammatory disorders that are frequently interrelated.3,4 In the context of cardiovascular disease, the impact of comorbidity burden is equally significant. Previous studies have shown that high-risk comorbidities are highly prevalent among patients with common cardiovascular conditions such as heart failure and atrial fibrillation—for instance, diabetes has a prevalence of up to 48%, and chronic kidney disease affects approximately 22% of these patients.5,6 These comorbid states are closely associated with systemic atherosclerosis and have been shown to markedly increase the risk of major adverse cardiovascular events.
Data from the US National Inpatient Sample indicate that more than 10% of patients undergoing PCI present with a substantial comorbidity burden. This elevated burden increases perioperative risk and may influence key therapeutic decisions, including the choice of antithrombotic regimens and strategies for contrast agent use.7 As a result, comorbidities may exert both direct and indirect effects on post-PCI outcomes.
Although previous studies have demonstrated the prognostic utility of the CCI in certain disease populations, its role in risk stratification and outcome prediction among patients undergoing PCI remains insufficiently explored, and supporting clinical data are limited. In particular, the mechanisms by which multiple comorbidities jointly influence cardiovascular outcomes have yet to be fully elucidated. Therefore, evaluating the applicability of the CCI in the post-PCI population may offer a more comprehensive assessment of patients’ overall health status and inform clinical decision-making regarding revascularization strategies. The early identification of high-risk individuals through the CCI might facilitate more targeted secondary prevention interventions, providing critical support for personalized care. This approach is especially relevant for younger patients and those with complex comorbidity profiles, in whom traditional risk models may be less effective for stratifying long-term cardiovascular risk.
This study aimed to investigate the association between the CCI and clinical outcomes following PCI. Although a recent study by Balun et al identified CCI > 2 as an independent predictor of the 1-year mortality in elderly patients undergoing PCI, their analysis using a CCI threshold of 2 did not concurrently evaluate short-term in-hospital outcomes or long-term composite cardiovascular events.8 Therefore, the goal of the current study was to evaluate the utility of the CCI as a tool for risk stratification and prognostic assessment in patients undergoing PCI.
Materials and Methods
Study Population and Data Collection
This was a single-center, prospective cohort study, which was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University (approval number: [2024]233–002 and AEEI-2024-359). The study population consisted of patients who underwent PCI at Xuanwu Hospital, Capital Medical University, between October 2016 and October 2020. The baseline demographic and clinical data were obtained through structured questionnaires and the hospital’s electronic medical record system. Written informed consent was obtained from all participants. Collected variables included the patients’ age, sex, medication use, comorbidities, laboratory test results, and details regarding their procedural and pharmacological treatment. The CCI was calculated for each patient, and the median CCI score in this cohort was 4. Therefore, the patients were categorized into two groups based on their CCI: the low comorbidity burden group (CCI ≤ 4) and the high comorbidity burden group (CCI > 4). The exclusion criteria were as follows (Figure 1): (1) patients with ST-elevation myocardial infarction, which was defined as persistent chest pain accompanied by newly developed ST-segment elevation, with or without pathological Q waves, and a marked elevation of cardiac biomarkers such as troponin or creatine kinase-MB;9 (2) patients with non-ST-elevation myocardial infarction, which was defined as acute ischemic symptoms accompanied by ST-segment depression or T-wave inversion on an electrocardiogram and dynamic elevation of troponin levels consistent with a diagnosis of myocardial infarction;9 (3) patients with incomplete clinical records or substantial loss of follow-up data that precluded reliable evaluation; and (4) patients who declined to participate in the study or were unable to complete follow-up assessments. The flow chart of this study is presented in Figure 1.
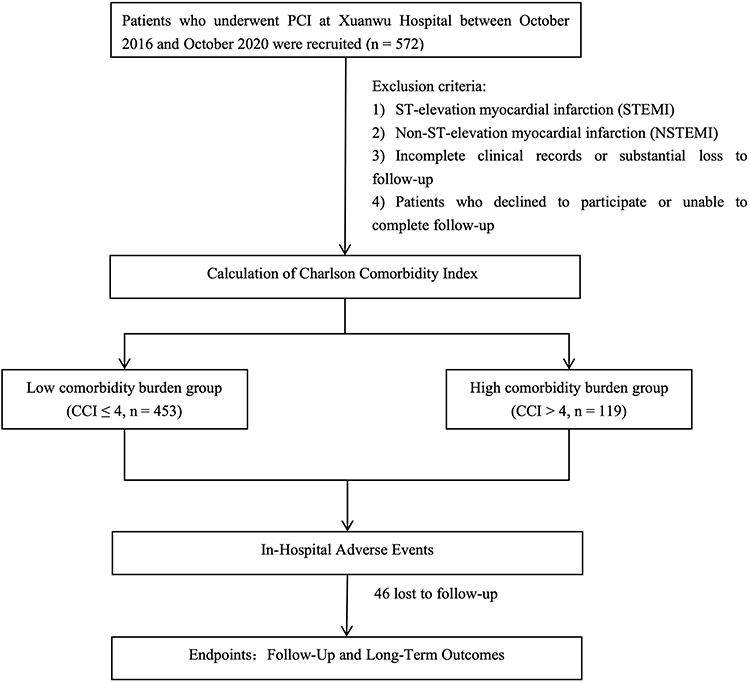 |
Figure 1 The flowchart of this study. |
Calculation of the CCI
Upon hospital admission, the CCI was calculated by trained healthcare professionals based on each patient’s medical history, physical examination findings, and relevant laboratory and imaging results. The CCI assigns weighted scores to a range of chronic conditions—such as myocardial infarction, heart failure, peripheral vascular disease, stroke, diabetes, chronic pulmonary disease, renal disease, liver disease, and malignancies—according to their severity. This index reflects the overall comorbidity burden of the patient.
In this study, the scoring of comorbidities followed the original system proposed by Charlson et al and was further adapted based on the modified version by Deyo et al, which maps comorbidities to the International Classification of Diseases coding system for clinical application.10
In-Hospital Adverse Events
In-hospital adverse events were defined as any unexpected clinical events occurring from the time of PCI admission to hospital discharge. These included complications that necessitated changes in treatment strategy, prolonged hospitalization, or resulted in significant clinical consequences. The major adverse cardiovascular events and systemic complications as well as other serious adverse events were recorded. Specific definitions were as follows: (1) periprocedural myocardial infarction, an elevation in cardiac troponin levels to at least five times the upper reference limit within 48 h after PCI, accompanied by new pathological Q waves or new-onset left bundle branch block;9 (2) access site complications, puncture site hematoma or other vascular access-related events that interfered with vascular use or caused secondary infection;11 (3) acute left heart failure, new-onset pulmonary congestion or pulmonary edema after PCI, presenting with dyspnea and radiographic evidence (eg, chest X-ray or ultrasound) requiring clinical intervention;12 (4) malignant arrhythmias, life-threatening arrhythmias such as ventricular fibrillation or sustained ventricular tachycardia that required immediate intervention;13 (5) acute kidney injury, an increase in serum creatinine levels of ≥0.3 mg/dL or a relative increase of ≥50% from baseline within 48–72 h post-procedure;14 (6) periprocedural stroke, ischemic or hemorrhagic stroke occurring intra- or postoperatively, characterized by new-onset neurological deficits lasting more than 24 h;15 (7) hospital-acquired infections, clinically diagnosed infections such as pneumonia or urinary tract infections that required antimicrobial therapy; (8) clinically significant bleeding events, bleeding episodes that required blood transfusion, altered treatment strategy, or led to hemodynamic instability.16
Follow-up and Long-Term Outcomes
Adverse events during follow-up were independently assessed and verified by two cardiologists. All discharged patients were contacted for clinical follow-up at 6 and 12 months after hospitalization through outpatient visits and telephone interviews. Follow-ups continued annually thereafter until the occurrence of a study endpoint or the end of the follow-up period.
The primary long-term outcome of this study was the occurrence of major adverse cardiovascular and cerebrovascular events (MACCEs) during the follow-up period, defined as the composite of the three following events:17 (1) all-cause mortality, including both cardiac deaths (eg, sudden cardiac death, fatal arrhythmia, heart failure) and noncardiac deaths (eg, death due to infection, malignancy, or other noncardiac causes); (2) nonfatal myocardial infarction, new myocardial infarction events during follow-up that fulfilled the diagnostic criteria outlined in the Fourth Universal Definition of Myocardial Infarction (2018) and did not result in death;13 (3) repeat revascularization, including PCI and coronary artery bypass grafting as well as rehospitalization due to heart failure or unstable angina (defined as unplanned hospital admissions resulting from acute decompensation of heart failure or worsening of unstable angina requiring inpatient care; (4) nonfatal stroke, ischemic or hemorrhagic stroke confirmed by clinical assessment and imaging, without resulting in death.
Statistical Analysis
Continuous variables were expressed as the mean ± standard deviation (SD) or median with interquartile range, as appropriate. Categorical variables were presented as counts (n) and percentages (%). For between-group comparisons, continuous variables were analyzed using the independent samples t-test or the Mann–Whitney U-test, while categorical variables were compared using the Chi-squared test or Fisher’s exact test. A logistic regression model was used to identify independent predictors of in-hospital adverse events. Kaplan–Meier survival curves were generated to estimate event-free survival, and the Log rank test was used to compare survival distributions between groups. A Cox proportional hazards regression model was applied to assess the association between the CCI and long-term MACCEs after adjusting for potential confounders. The proportional hazards assumption was evaluated using Schoenfeld residuals. The p-value for trend analysis was determined to evaluate the linear relationship between increasing CCI scores and the risk of MACCEs.
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). A two-sided p-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 572 patients with CAD who underwent PCI between October 2016 and October 2020 were included in this study. The mean age of the patients was 61.0 ± 10.36 years, and 402 patients (70.3%) were male. The CCI ranged from 0 to 7. Figure 2 shows the distribution of comorbidities comprising the CCI in this cohort. Based on the median CCI score of 4, the patients were divided into two groups: low comorbidity burden (CCI ≤ 4, n = 453) and high comorbidity burden (CCI > 4, n = 119). Compared with the low-CCI group, the patients in the high-CCI group were more likely to be male (81.5% vs 67.3%, p = 0.003) and older (median age: 65.0 vs 62.0 years, p = 0.001). They also were more likely to have longer hospital stays (8.9 vs 5.7 days, p < 0.001), a higher prevalence of diabetes (44.5% vs 29.1%, p = 0.001), and higher serum creatinine levels (75.74 μmol/L vs 68.39 μmol/L, p = 0.002) as well as present with left main CAD (15.13% vs 7.95%, p = 0.017) or multivessel disease (62.18% vs 45.92%, p = 0.019) (Table 1).
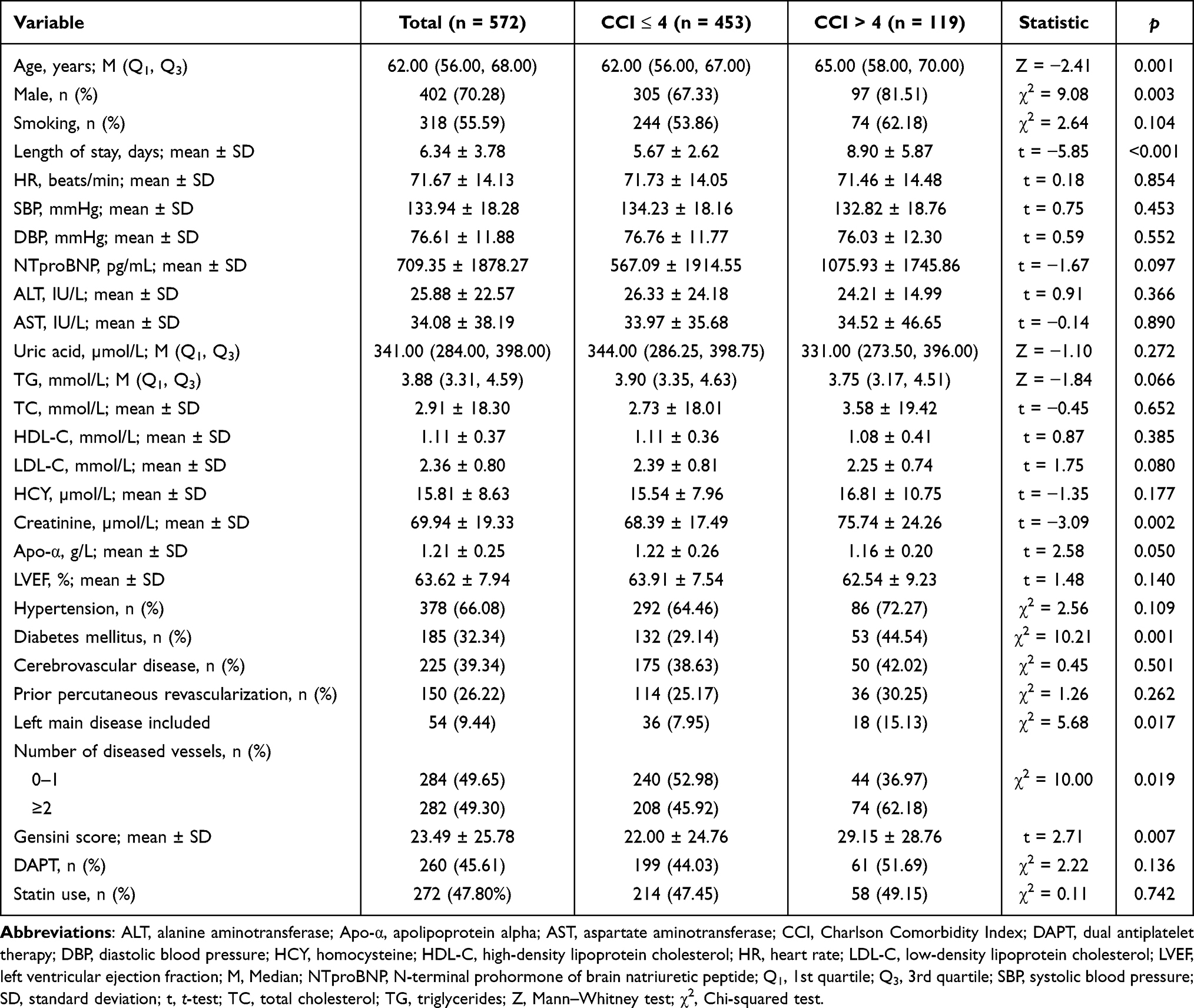 |
Table 1 Baseline Demographic and Clinical Characteristics According to the Charlson Comorbidity Index |
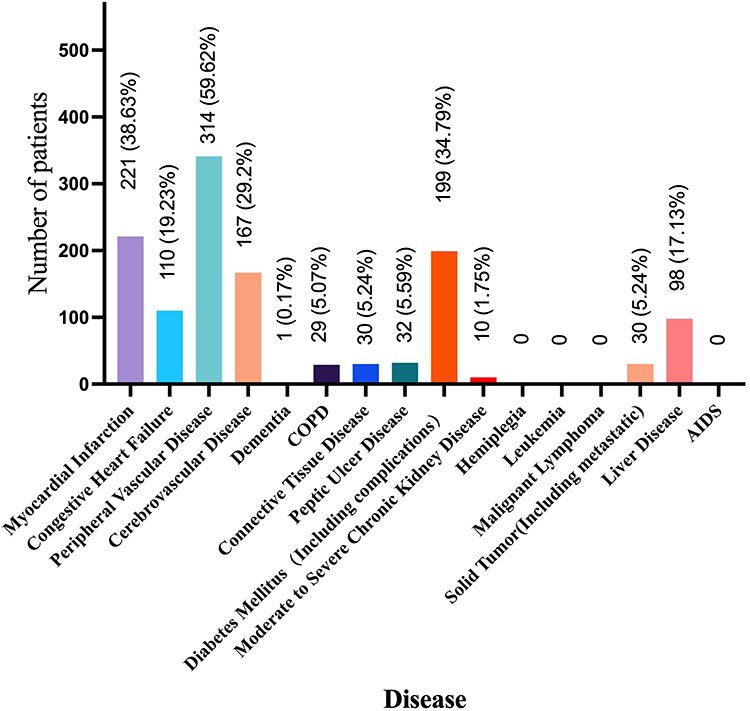 |
Figure 2 Distribution of the diseases assessed by the Charlson Comorbidity Index in this study. |
In-Hospital Outcomes
The overall incidence of in-hospital adverse events was 4.4% (25 cases). The patients in the high comorbidity burden group had a significantly higher rate of in-hospital events compared to those in the low-CCI group (13.4% vs 2.0%, p < 0.01). After adjusting for baseline clinical variables—including age, sex, history of hypertension, diabetes, cerebrovascular disease, admission heart rate and blood pressure, lipid profile, LVEF, characteristics of coronary lesions, and major medications—the analysis revealed that a higher CCI was independently associated with an increased risk of in-hospital adverse events [odds ratio (OR) = 3.13; 95% confidence interval (CI): 1.40–7.02, p < 0.01]. In addition, a history of prior PCI (OR = 0.27; 95% CI: 0.08–0.89, p = 0.032) and an elevated heart rate (OR = 0.93; 95% CI: 0.88–0.97, p = 0.002) were also identified as independent predictors of in-hospital outcomes (Table 2).
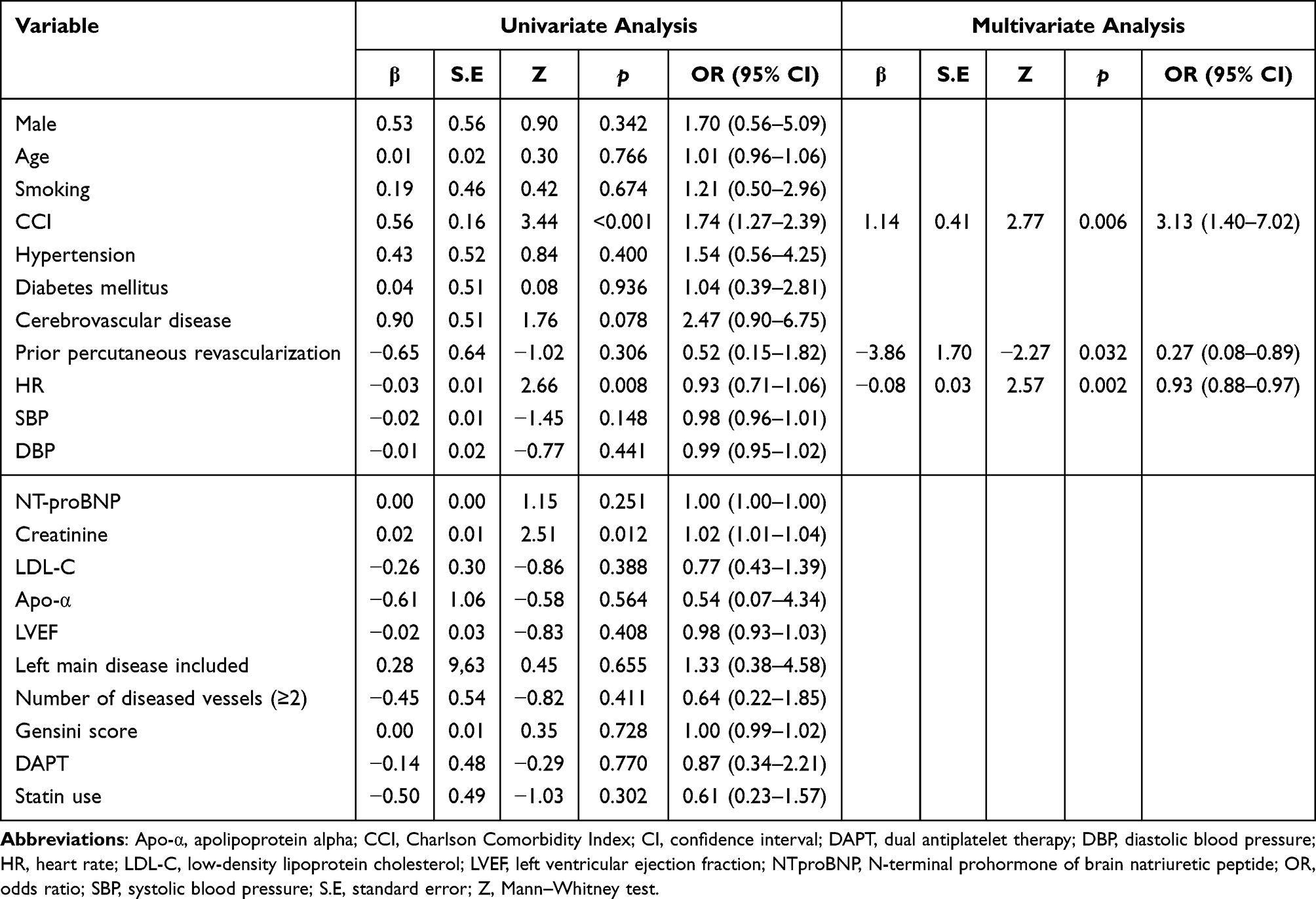 |
Table 2 Univariate and Multivariate Regression Analysis of Factors Associated with Adverse Events During Hospitalization |
Long-Term Outcomes
Among the enrolled patients, 526 completed follow-ups, while 46 were lost to follow-up, resulting in a follow-up loss rate of 8.0%. There was no significant difference in loss to follow-up between the high and low comorbidity burden groups (8.2% vs 7.6%, p = 0.502). During a median follow-up period of five years, Kaplan–Meier survival analysis showed that the cumulative incidence of MACCEs was significantly higher in the high-CCI group compared to the low-CCI group (51.3% vs 6.2%, log-rank p < 0.001) (Figure 3).
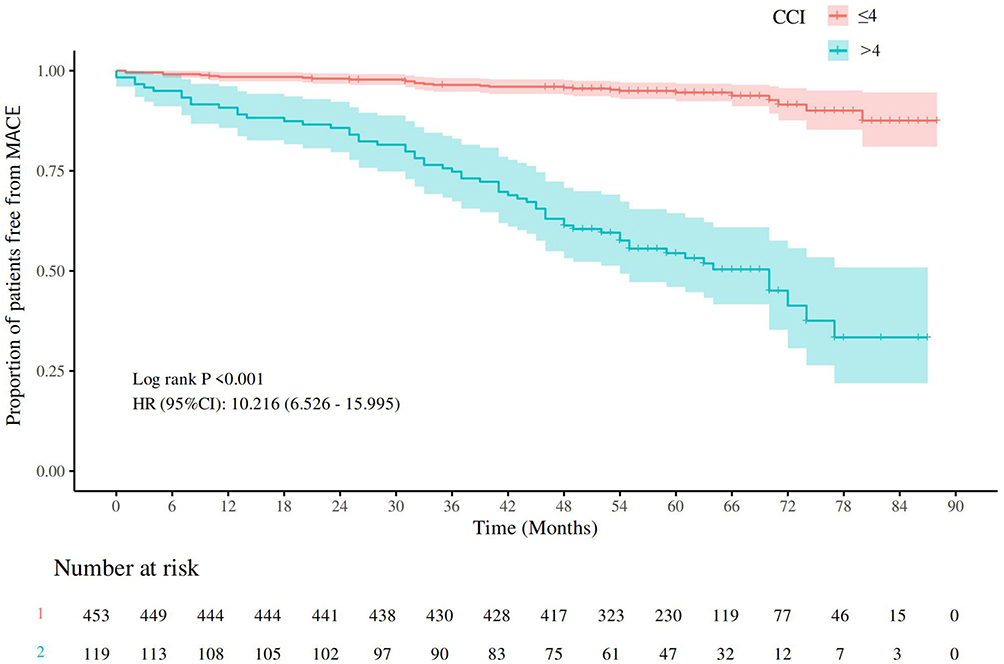 |
Figure 3 Kaplan–Meier survival curves illustrating freedom from major adverse cardiovascular and cerebrovascular events (MACCEs), stratified by the Charlson Comorbidity Index. |
Cox Multivariate Models for Long-Term Outcomes
After adjusting for age, sex, comorbidity history, admission heart rate, blood pressure, lipid profile, LVEF, characteristics of coronary lesions, and major medications, multivariate Cox regression analysis revealed that the CCI was independently associated with the occurrence of MACCEs (HR = 2.72; 95% CI: 2.25–3.30, p < 0.001). Moreover, a history of prior PCI (HR = 0.27; 95% CI: 0.08–0.89, p = 0.032), LVEF (HR = 0.93; 95% CI: 0.88–0.97, p = 0.002), and multivessel disease (HR = 1.93; 95% CI: 1.03–3.59, p = 0.04) were also identified as independent predictors of long-term MACCEs (Table 3). Furthermore, after adjusting for covariates in the Cox regression model (Table 4), a significant linear trend was observed, indicating that the risk of MACCEs increased with higher CCI scores (p for trend < 0.05).
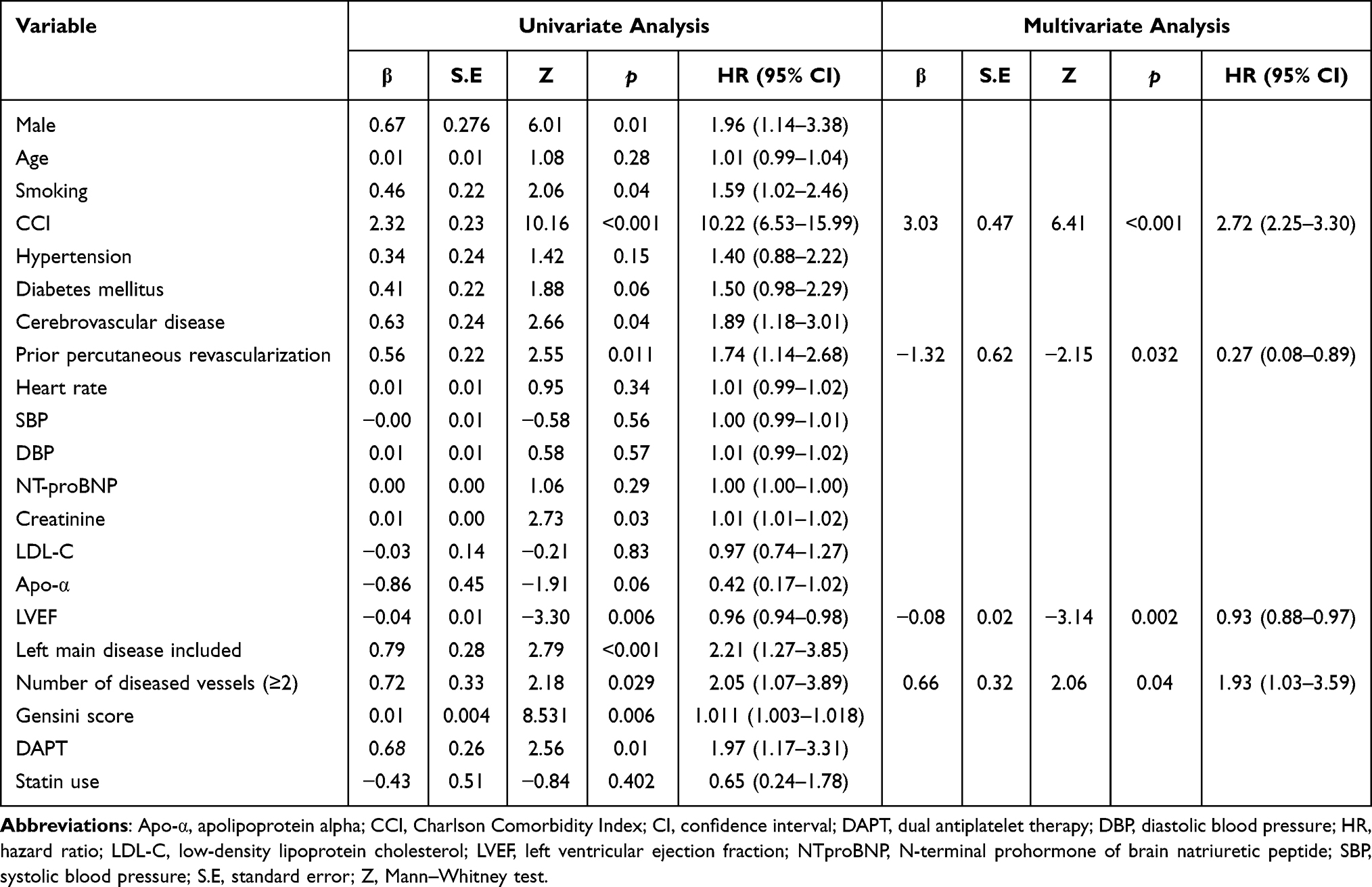 |
Table 3 Cox Regression Analysis on Major Adverse Cardiovascular Events in the Long Term |
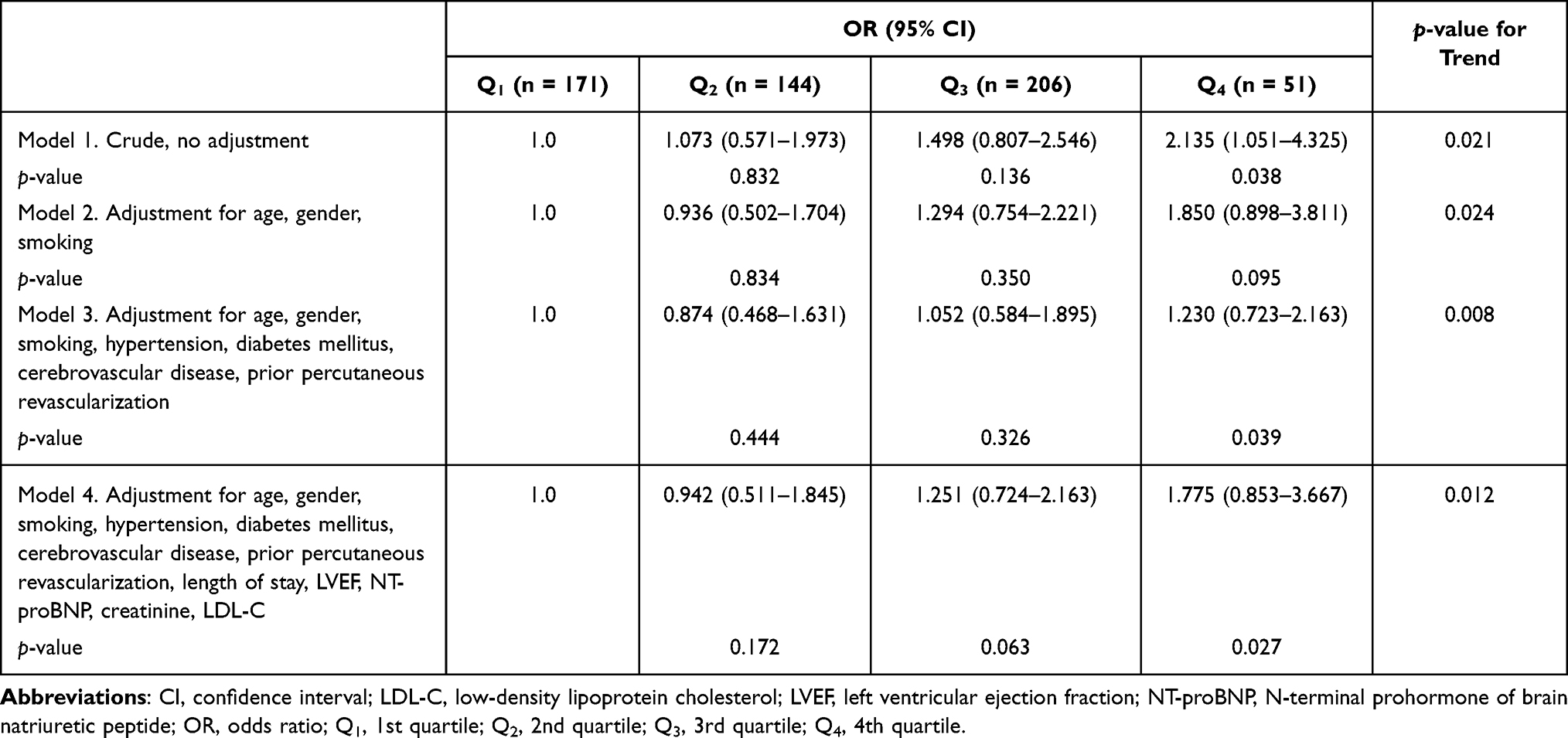 |
Table 4 Risk Factor Analysis of the Charlson Comorbidity Index Using the Cox Proportional Hazards Regression Model |
Discussion
This prospective cohort study characterized the clinical features and prognostic impact of a high comorbidity burden in patients undergoing PCI. We found that 20.8% of the enrolled patients had a high CCI, and this subgroup exhibited more complex clinical profiles, including an older age, a higher proportion of males, prolonged hospital stays, elevated serum creatinine levels, a higher prevalence of diabetes, and more frequent involvement of left main and multivessel CAD. The CCI was identified as an independent predictor of in-hospital adverse events, with significantly higher event rates observed in the high comorbidity group compared to the low comorbidity group. More importantly, during a median follow-up period of five years, the high-CCI group demonstrated approximately twice the risk of MACCEs compared with the low-CCI group. These findings suggest that the CCI, as a tool for quantifying the burden of multiple chronic conditions, can effectively identify high-risk patients in the PCI population.
Comorbidity refers to the coexistence of two or more chronic diseases or pathological conditions in a single patient that are clinically independent yet collectively exert a significant impact on their health status. As an important parameter in clinical prognostic assessment, the comorbidity burden is commonly quantified using the CCI. This index assigns weighted scores of 1–6 to nearly 20 underlying diseases based on severity, with the total score reflecting the overall disease burden of the patient. Previous studies have confirmed the prognostic value of the CCI in various surgical and oncology-related conditions. For example, in patients undergoing an esophagectomy for esophageal cancer, those with a CCI score ≥ 2 had a significantly lower three-year overall survival rate (59.7%) compared to those with a CCI ≤ 1 (77.9%).18,19 Additionally, patients in the high-CCI group had a poorer nutritional status one month postoperatively, as indicated by a lower Prognostic Nutritional Index, suggesting a greater nutritional risk during postoperative recovery.20 Similarly, in non-small cell lung cancer patients, those with CCI ≥ 1 had a five-year overall survival rate of 84%, compared to 88% for those with CCI = 0, and their median postoperative hospital stay was longer (15 vs 11 days).21 In the cardiovascular field, the CCI has been used to assess risk and predict outcomes in patients with conditions such as heart failure and atrial fibrillation. In elderly patients with atrial fibrillation, the comorbidity burden also has been identified as a key determinant of adverse clinical outcomes. One study reported a 41.6% incidence of all-cause mortality or rehospitalization during a one-year follow-up period; patients in the event group had significantly higher CCI scores than those without events (2.5 ± 1.9 vs 1.7 ± 1.3), and the incidence of heart failure was also higher (32.9% vs 17.4%).22,23 These findings support the prognostic relevance of the CCI in both noncardiac and selected cardiovascular populations. Nevertheless, systematic investigations of the prognostic utility of the CCI specifically in PCI populations—particularly regarding long-term risk stratification—remain limited. Most existing studies have focused on short-term outcomes such as rehospitalization, in-hospital complications, and healthcare costs. A study based on a US national database reported that from 2004 to 2014, the proportion of PCI patients with a high comorbidity burden (CCI ≥ 3) increased from 5.3% to 14.2%. During hospitalization, patients without comorbidities had a mortality rate of 1.0%, whereas that of patients with high CCI scores was three times higher (3.2%). Moreover, the total hospitalization costs increased significantly with higher CCI scores.24 Despite these findings, whether the CCI can reliably predict long-term MACCEs after PCI remains insufficiently explored and warrants further investigation.
In the risk assessment of CAD patients, traditional tools such as the Thrombolysis in Myocardial Infarction (TIMI) score and the GRACE score have been widely used for prognostic evaluation in patients with acute coronary syndrome. The TIMI score is favored for its simplicity and ease of use, enabling rapid estimation of the risk of ischemic events within 30 days following an acute episode.25,26 However, it does not account for comorbid conditions, offers limited insight into the patients’ chronic disease status and overall systemic health, and has relatively little utility for predicting long-term outcomes such as MACCEs beyond one year. The GRACE score incorporates more comprehensive physiological and clinical parameters, including heart rate, systolic blood pressure, serum creatinine, and Killip class, to provide a broader risk assessment. Nonetheless, it still omits a wide range of chronic comorbidities—such as diabetic neuropathy and chronic pulmonary disease—that may contribute to cumulative organ damage over time. Additionally, the complexity of its calculation limits its practicality in routine clinical settings.
The SYNTAX score is another established tool designed to quantify the anatomical complexity of coronary lesions.27 It is based on coronary angiographic findings, scoring lesion characteristics such as number, location, branch involvement, occlusions, and calcification. While the SYNTAX score provides valuable guidance for selecting PCI strategies and predicting procedural outcomes, it primarily focuses on anatomical and procedural factors, without accounting for the patient’s systemic health or comorbidity profile, thus limiting its utility for long-term, holistic prognostic evaluation. Similarly, the Gensini score, another angiography-based tool, offers advantages in quantifying the severity of coronary artery stenosis and ischemic burden.28 However, like the SYNTAX score, it remains confined to anatomical parameters and lacks integration of comorbidity burden or chronic disease status. In summary, although these scoring systems play important roles in assessing coronary lesion complexity and short-term procedural risk, they fall short in evaluating chronic comorbid conditions and overall systemic health. This limitation is particularly relevant for PCI patients with a substantial comorbidity burden, where long-term risk prediction requires a more comprehensive and patient-centered approach.
Against this background, the present study introduced comorbidity as a key indicator to reflect patients’ overall health status. Although recent research has explored alternative tools such as the age-adjusted CCI (aCCI) and the Elixhauser Comorbidity Measure, each with its own advantages, limitations remain.7 The aCCI extends the original CCI by incorporating age into the scoring system, thereby broadening its applicability. Meanwhile, the Elixhauser index includes 31 comorbid conditions and has demonstrated strong adaptability in large administrative database studies. However, the aCCI merges age with the chronic disease burden into a single score, which may compromise the ability to discern the independent impact of chronic diseases.29 The Elixhauser score, while comprehensive, is complex, involving a large number of variables and requiring intricate calculations, which limit its practicality in routine clinical settings. Furthermore, validation of the Elixhauser model specifically in PCI populations is still lacking.
It is important to note that there is currently no universally accepted classification threshold for the CCI. Some studies, based on clinical experience or prior literature, commonly use a CCI score of 2–3 as a cutoff to define high-risk patients.23,30 This criterion has been applied in research involving populations with ischemic stroke, heart failure, and other chronic diseases. However, studies specifically focusing on PCI patients remain relatively limited, and this population differs significantly in terms of disease spectrum and clinical complexity. In practice, CCI classification often varies depending on the study objective, characteristics of the study population, and specific clinical requirements, resulting in inconsistencies in cutoff values. Given the relatively high comorbidity burden typically observed in PCI patients, we adopted the median CCI score as the threshold for stratification in this study. This approach allowed for a more accurate reflection of the clinical characteristics of our cohort and improved the precision of risk stratification. Our findings also underscore the need for future research to refine and individualize CCI classification standards according to specific disease profiles and population settings. Such optimization may enhance the clinical utility of the CCI in prognostic evaluation and decision-making across diverse patient populations.
In recent years, the CCI has increasingly been used in combination with other key clinical indicators to improve the accuracy of disease risk prediction. Previous studies have demonstrated that biomarkers such as cystatin C and pentraxin-3, along with nutritional status indicators like the neutrophil-to-lymphocyte ratio and the prognostic nutritional index, have significant prognostic value across a range of conditions, including heart failure and various malignancies.31–33 Such integrated assessment approaches allow for a more comprehensive evaluation of a patient’s systemic condition, functional reserve, and chronic disease burden, highlighting the potential of multidimensional risk stratification in personalized medicine. In our study, LVEF, history of prior PCI, and multivessel disease were also identified as independent predictors of the long-term outcomes of PCI patients. These findings suggest that an increased comorbidity burden may be closely associated with a diminished organ functional reserve and reduced compensatory capacity, particularly in elderly patients. Furthermore, we observed that as the comorbidity burden increases, the complexity of clinical management and follow-up also rises. This includes challenges such as drug–disease and drug–drug interactions in those with chronic conditions as well as reduced patient adaptability to standard treatment regimens.
Therefore, our findings suggest that clinicians should consider incorporating the CCI into early risk stratification strategies. For patients with a high comorbidity burden, more proactive interventions—such as optimized pharmacotherapy, enhanced rehabilitation management, and regular follow-up—may be warranted to improve the long-term outcomes. Ultimately, integrating comorbidity assessment into clinical practice may help to refine personalized care for patients with cardiovascular disease.
Limitations
This study was conducted at a single center with a relatively limited sample size, which may limit the generalizability of the findings. Future studies should aim to validate these results through large-scale, multicenter, prospective investigations. Second, the lack of standardized cutoff values for the CCI poses a challenge for consistent risk classification. There is currently no universally accepted threshold to define a high CCI, and heterogeneity in cutoff selection across different studies may lead to variability in reported outcomes. Third, the CCI is inherently a static scoring tool and does not account for temporal changes in a patient’s comorbidity status. As comorbid conditions can evolve over time, incorporating dynamic measures—such as biomarker or imaging-based assessments—may improve the predictive performance of future risk models.
Conclusion
This study systematically evaluated the prognostic utility of the CCI in patients undergoing PCI for CAD. The findings demonstrate that patients with a higher comorbidity burden had significantly increased rates of MACCEs, underscoring the clinical value of the CCI as a comorbidity assessment tool in the risk stratification and outcome prediction of PCI patients.
Data Sharing Statement
The datasets generated and analyzed in the study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University (approval number: [2024]233-002 and AEEI-2024-359) and adhered to the principles outlined in the Declaration of Helsinki. All procedures were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was funded by the National Natural Science Foundation of China (No. 82170347), Beijing Municipal Public Welfare Development and Reform Pilot Project for Medical Research Institutes (No. JYY2023-13), and the National Clinical Key Specialty Construction Project supported by the Central Government of China (2025).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhu XY, Shi MQ, Jiang ZM, Xiao L, Tian JW, Su FF. Global, regional, and national burden of cardiovascular diseases attributable to metabolic risks across all age groups from 1990 to 2021: an analysis of the 2021 global burden of disease study data. BMC Public Health. 2025;25:1704. doi:10.1186/s12889-025-22702-7
2. Catapano AL, Graham I, De Backer G; Authors/Task Force M, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;253:281–13. doi:10.1016/j.atherosclerosis.2016.08.018
3. Nakaya A, Ochi K, Tokitsu K, et al. Retrospective analysis of Charlson comorbidity index (CCI). Gan To Kagaku Ryoho. 2014;41:673–675.
4. Pladys A, Vigneau C, Raffray M, et al. Contribution of medico-administrative data to the development of a comorbidity score to predict mortality in End-Stage Renal Disease patients. Sci Rep. 2020;10:8582. doi:10.1038/s41598-020-65612-x
5. Formiga F, Ferrer A, Sanz H, et al. Patterns of comorbidity and multimorbidity in the oldest old: the Octabaix study. Eur J Intern Med. 2013;24:40–44. doi:10.1016/j.ejim.2012.11.003
6. Abellana R, Gonzalez-Loyola F, Verdu-Rotellar JM, et al. Predictive model for atrial fibrillation in hypertensive diabetic patients. Eur J Clin Invest. 2021;51:e13633. doi:10.1111/eci.13633.
7. Potts J, Nagaraja V, Al Suwaidi J, et al. The influence of Elixhauser comorbidity index on percutaneous coronary intervention outcomes. Catheter Cardiovasc Interv. 2019;94:195–203. doi:10.1002/ccd.28072
8. Balun A, Akgümüs A. Charlson comorbidity index and 1-year poor outcomes in elderly patients undergoing successful percutaneous coronary intervention: a retrospective study. Medicine. 2023;102. doi:10.1097/Md.0000000000033792.
9. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618–e651. doi:10.1161/CIR.0000000000000617
10. Ghali WA, Hall RE, Rosen AK, Ash AS, Moskowitz MA. Searching for an improved clinical comorbidity index for use with ICD-9-CM administrative data. J Clin Epidemiol. 1996;49:273–278. doi:10.1016/0895-4356(95)00564-1
11. Naidu SS, Baran DA, Jentzer JC, et al. SCAI SHOCK stage classification expert consensus update: a review and incorporation of validation studies: this statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J Am Coll Cardiol. 2022;79:933–946. doi:10.1016/j.jacc.2022.01.018
12. McDonagh TA, Metra M, Adamo M, et al. [2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC]. G Ital Cardiol. 2022;23:e1–e127. doi:10.1714/3777.37630
13. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2018;15:e190–e252. doi:10.1016/j.hrthm.2017.10.035
14. Disease K. Improving Global outcomes blood pressure work G. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99:S1–S87. doi:10.1016/j.kint.2020.11.003
15. Demaerschalk BM, Berg J, Chong BW, et al. American Telemedicine Association: telestroke Guidelines. Telemed J E Health. 2017;23:376–389. doi:10.1089/tmj.2017.0006
16. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the bleeding academic research consortium. Circulation. 2011;123:2736–2747. doi:10.1161/CIRCULATIONAHA.110.009449
17. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115:2344–2351. doi:10.1161/CIRCULATIONAHA.106.685313
18. Backemar L, Lagergren P, Djarv T, Johar A, Wikman A, Lagergren J. Comorbidities and risk of complications after surgery for esophageal cancer: a nationwide cohort study in Sweden. World J Surg. 2015;39:2282–2288. doi:10.1007/s00268-015-3093-6
19. Baranov N, Claassen L, van Workum F, Rosman C. Age and Charlson Comorbidity Index score are not independent risk factors for severe complications after curative esophagectomy for esophageal cancer: a Dutch population-based cohort study. Surg Oncol. 2022;43:101789. doi:10.1016/j.suronc.2022.101789
20. Kubo Y, Tanaka K, Yamasaki M, et al. Influences of the Charlson Comorbidity Index and nutrition status on prognosis after esophageal cancer surgery. Ann Surg Oncol. 2021;28:7173–7182. doi:10.1245/s10434-021-09779-1
21. Simon TG, Beland MD, Machan JT, Dipetrillo T, Dupuy DE. Charlson Comorbidity Index predicts patient outcome, in cases of inoperable non-small cell lung cancer treated with radiofrequency ablation. Eur J Radiol. 2012;81:4167–4172. doi:10.1016/j.ejrad.2012.06.007
22. van Deutekom C, Velt MJH, van Gelder IC, Rienstra M, Mulder BA, Investigators RI. Multimorbidity increases risk of cardiovascular outcomes in permanent atrial fibrillation: data from the RACE II study. Int J Cardiol Heart Vasc. 2025;59:101686. doi:10.1016/j.ijcha.2025.101686
23. Rashid M, Kwok CS, Gale CP, et al. Impact of co-morbid burden on mortality in patients with coronary heart disease, heart failure, and cerebrovascular accident: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2017;3:20–36. doi:10.1093/ehjqcco/qcw025
24. Potts J, Kwok CS, Ensor J, et al. Temporal changes in co-morbidity burden in patients having percutaneous coronary intervention and impact on prognosis. Am J Cardiol. 2018;122:712–722. doi:10.1016/j.amjcard.2018.05.003
25. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842. doi:10.1001/jama.284.7.835
26. Amador P, Santos JF, Goncalves S, Seixo F, Soares L. Comparison of ischemic and bleeding risk scores in non-ST elevation acute coronary syndromes. Acute Card Care. 2011;13:68–75. doi:10.3109/17482941.2011.567287
27. Thuijs D, Kappetein AP, Serruys PW, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394:1325–1334. doi:10.1016/S0140-6736(19)31997-X
28. Yokokawa T, Yoshihisa A, Kiko T, et al. Residual gensini score is associated with long-term cardiac mortality in patients with heart failure after percutaneous coronary intervention. Circ Rep. 2020;2:89–94. doi:10.1253/circrep.CR-19-0121
29. de Oliveira Bezerra MR, de Sousa IM, Miranda AL, et al. Age-adjusted Charlson comorbidity index and its association with body composition and overall survival in patients with colorectal cancer. Support Care Cancer. 2024;32:517. doi:10.1007/s00520-024-08730-w
30. Karisik A, Bader V, Moelgg K, et al. Comorbidities associated with dysphagia after acute ischemic stroke. BMC Neurol. 2024;24:358. doi:10.1186/s12883-024-03863-1
31. Risch M, Risch L, Purde MT, et al. Association of the cystatin C/creatinine ratio with the renally cleared hormones parathyroid hormone (PTH) and brain natriuretic peptide (BNP) in primary care patients: a cross-sectional study. Scand J Clin Lab Invest. 2016;76:379–385. doi:10.1080/00365513.2016.1183262
32. Larsen MK, Skov V, Kjaer L, et al. Neutrophil-to-lymphocyte ratio and all-cause mortality with and without myeloproliferative neoplasms-a Danish longitudinal study. Blood Cancer J. 2024;14:28. doi:10.1038/s41408-024-00994-z
33. Huang Y, Zhang Q, Li P, et al. The prognostic nutritional index predicts all-cause mortality in critically ill patients with acute myocardial infarction. BMC Cardiovasc Disord. 2023;23:339. doi:10.1186/s12872-023-03350-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated HsCRP in Chronic Obstructive Pulmonary Disease: A Prospective Study of Long-Term Outcomes After Percutaneous Coronary Intervention
Zheng Y, Qi Y, Seery S, Yang J, Li C, Wang W, Gao J, Meng X, Shao C, Tang YD
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2517-2528
Published Date: 7 October 2022
Exploring the Complementary Role of Traditional Chinese Medicine in Enhancing Percutaneous Coronary Intervention Outcomes: Mechanisms, Benefits, and Future Research Directions
Zheng S, Guo J, Wang Q
Therapeutics and Clinical Risk Management 2025, 21:1069-1083
Published Date: 10 July 2025
Comparison of Percutaneous Coronary Intervention Outcomes for in-Stent vs de Novo Chronic Total Occlusions: A Meta-Analysis
Mao Q, Xie L, Wu J
Therapeutics and Clinical Risk Management 2026, 22:576328
Published Date: 15 April 2026
Apolipoprotein B/A1 Ratio for Predicting Major Adverse Cardiovascular Events in Coronary Artery Disease: Development and Validation of a Nomogram
Zhu H, Jin Q
International Journal of General Medicine 2026, 19:605828
Published Date: 7 May 2026