Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Impact of Multidisciplinary Team Decision-Making on Clinical Outcomes and Healthcare Resource Utilization in Tertiary Hospital Settings: A Retrospective Cohort Study
Received 28 November 2025
Accepted for publication 7 February 2026
Published 9 March 2026 Volume 2026:19 585133
DOI https://doi.org/10.2147/JMDH.S585133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Brian Nyatanga
Qiuqi Ou,1 Xi Yang2
1Department of Medical Affairs, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 2Department of Breast Surgery, Affiliated Tumor Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China
Correspondence: Xi Yang, Email [email protected]
Objective: Multidisciplinary team (MDT) decision-making is widely adopted in tertiary hospitals, yet evidence regarding its impact on clinical outcomes and resource utilization remains inconsistent. This study evaluated the association between MDT participation and clinical outcomes as well as healthcare resource utilization among hospitalized patients in tertiary hospital settings.
Methods: This retrospective cohort study analyzed 158,358 adult hospital admissions from January 2020 to December 2024. Patients were categorized into MDT (n=16,202) and non-MDT groups (n=142,156) based on documented multidisciplinary discussions within 7 days before or after admission. Propensity score weighting with inverse probability of treatment weighting was applied to balance baseline characteristics. Primary outcomes included in-hospital mortality, 30-day mortality, and length of stay. Secondary outcomes encompassed readmission rates, complications, and resource utilization metrics.
Results: After propensity score adjustment, MDT participation was associated with significantly reduced in-hospital mortality (adjusted OR=0.78, 95% CI: 0.70– 0.87, P< 0.001), 30-day mortality (adjusted HR=0.82, 95% CI: 0.75– 0.90, P< 0.001), 30-day readmission (adjusted OR=0.88, 95% CI: 0.82– 0.94, P< 0.001), and complications (adjusted OR=0.91, 95% CI: 0.86– 0.97, P=0.003). However, MDT involvement was associated with increased resource utilization, including 24% more imaging studies (P< 0.001), 31% more laboratory tests (P< 0.001), longer hospital stays (P< 0.001), and 18% higher total costs (P< 0.001).
Conclusion: In this retrospective cohort study, MDT decision-making was associated with improved clinical outcomes but increased healthcare resource consumption. These findings inform hospital policies regarding MDT implementation and resource allocation strategies.
Keywords: multidisciplinary team, clinical outcomes, healthcare resource utilization, propensity score analysis, tertiary hospital, mortality
Introduction
Multidisciplinary team (MDT) decision-making has been widely adopted in managing complex hospitalized patients, particularly in oncology, cardiovascular disease, and other specialties requiring collaborative expertise.1 As a key form of interprofessional collaboration, MDT brings together professionals from different disciplines to work toward shared patient care goals.2 The approach is recognized as the gold standard of cancer care, with the expectation that bringing together professionals from different disciplines will enhance diagnostic accuracy, optimize treatment planning, and improve care coordination.1,3 Studies have documented potential benefits including improved patient assessment, management and outcomes in oncology settings, and a step towards personalized medicine in cardiovascular care.4,5 However, the actual impact on clinical outcomes and healthcare resource utilization remains uncertain.
Evidence regarding MDT effects on clinical outcomes and health service utilization is inconsistent. While some research suggests improvements in patient-reported outcomes, the effects on clinical outcomes, health utilization, and costs are not evident.6,7 The quality of MDT decision-making depends on information quality and team processes, yet few studies have examined these factors using standardized approaches.8 Furthermore, evidence quality has been rated as low, with well-designed prospective studies still needed. Most existing studies focus on specific disease populations such as cancer or surgical cohorts with relatively small sample sizes, limiting generalizability to broader inpatient populations.9
The gap between theoretical benefits and demonstrated real-world impact underscores the need for large-scale observational research across diverse patient populations in tertiary hospital settings. MDT implementation in Chinese tertiary hospitals aligns with international practice, with MDT collaboration expanding from oncology to various departments as a core component of medical quality management.10 Understanding whether MDT participation influences mortality, length of stay, readmission rates, and resource consumption requires analysis of routine clinical data involving substantial patient cohorts. Such evidence would inform hospital policies regarding MDT implementation, resource allocation, and care pathway optimization. This retrospective cohort study aimed to evaluate the association between MDT decision-making and clinical outcomes as well as healthcare resource utilization among adult hospitalized patients at tertiary hospitals, using data from over 150,000 admissions between 2020 and 2024.
Methods
Study Design and Data Source
This retrospective cohort study analyzed hospital admission data spanning from January 1, 2020, to December 31, 2024. Data were extracted from hospital information systems, including the electronic medical record database, hospital discharge registry, clinical order management system, laboratory and imaging information systems, billing and cost settlement records, and the institutional MDT documentation platform. The MDT documentation system captures all formalized multidisciplinary discussions with recorded conclusions and recommendations for individual patients. All data sources were linked using unique patient identifiers to construct complete longitudinal records for each hospitalization episode.
Study Population
Adult patients who were admitted to inpatient departments during the study period were eligible for inclusion. The study population included patients from internal medicine, surgery, obstetrics and gynecology, and pediatric services. Patients were excluded if they had missing data on essential variables including sex, age, admission or discharge dates, or primary diagnosis codes, which precluded valid outcome ascertainment. Additional exclusions included hospitalizations with extreme length of stay values exceeding the 99th percentile to minimize outlier bias. Day-case admissions and observation unit stays lasting less than 24 hours were also excluded as these represent ambulatory care pathways with limited opportunity for MDT involvement.
MDT and Group Assignment
MDT was defined as a documented consultation involving two or more distinct clinical specialties addressing the care of an individual hospitalized patient, with formal conclusions or management recommendations recorded in the institutional system. These discussions occurred through in-person meetings or virtual platforms.
The primary exposure divided patients into MDT and non-MDT groups based on whether they had at least one MDT discussion within 7 days before or after the admission date. Patients meeting this criterion were classified as the MDT group, while those without any MDT discussion during this 14-day window formed the non-MDT comparison group.
Secondary analyses explored three additional dimensions of MDT exposure. The dose-response analysis categorized patients by the total number of MDT discussions during hospitalization: zero discussions as reference, one discussion, and two or more discussions. The specialty breadth analysis distinguished between MDT discussions involving one to two specialties versus those involving three or more specialties. The temporal analysis classified patients based on timing of the initial MDT discussion, comparing those receiving MDT within 72 hours of admission versus those receiving MDT after 72 hours.
Outcome Measures
The primary clinical outcomes are in-hospital mortality defined as death occurring during the index hospitalization, 30-day all-cause mortality calculated from the discharge date when linkage to mortality registries was available, and length of hospital stay measured in days from admission to discharge. Secondary clinical outcomes included 30-day all-cause readmission defined as any unplanned hospital admission within 30 days following discharge, composite complication rates derived from diagnostic codes and adverse event documentation, intensive care unit admission status and cumulative ICU days, occurrence and frequency of major surgical or interventional procedures, and time intervals from admission to initiation of critical therapeutic interventions such as antimicrobial therapy or thrombolytic procedures measured in hours or days.
Resource utilization and cost outcomes encompassed the total number of imaging studies including computed tomography, magnetic resonance imaging, and ultrasonography examinations performed during hospitalization, aggregate laboratory test orders, antimicrobial drug utilization measured in days of therapy, and total direct medical costs representing the complete hospitalization expenditure with logarithmic transformation applied when currency-specific sensitivity warranted adjustment for skewed distributions.
Covariates and Confounding Control
Demographic characteristics included patient age, sex, and health insurance type or self-payment status at admission. Baseline disease burden and clinical severity were quantified using the Charlson Comorbidity Index or Elixhauser Comorbidity Score derived from diagnostic codes, supplemented by vital signs and key laboratory parameters documented at admission when available. Disease classification variables captured the primary diagnosis coded according to ICD-10 specifications, diagnosis-related group assignments, and surgical procedure categories. Care delivery characteristics incorporated admission source, admitting clinical department, attending physician credentials and experience level, and weekend versus weekday admission timing. Temporal and policy-related factors were represented through calendar year indicators as fixed effects and phase-specific variables denoting periods of public health emergency when applicable. Institutional clustering was addressed through hospital department or facility-level random effects in multilevel modeling frameworks to account for within-cluster correlation.
Statistical Analysis
Missing data were handled through multiple imputation using chained equations, with complete case analysis conducted as a sensitivity check. Propensity scores for MDT exposure were estimated using logistic regression incorporating all baseline covariates. Inverse probability of treatment weights with stabilization were constructed to achieve covariate balance between groups. One-to-one nearest neighbor matching with caliper restrictions served as an alternative balancing approach. The sample size provided >99% power to detect an odds ratio of 0.78 for in-hospital mortality at α=0.05, given baseline mortality of 2.2% and a 1:9 group ratio.
Outcome analyses employed weighted regression models appropriate to each outcome’s distribution. Binary outcomes were analyzed using weighted logistic regression reporting odds ratios with 95% confidence intervals. Time-to-event outcomes utilized weighted Cox regression reporting hazard ratios. Count outcomes were modeled using negative binomial or zero-inflated models reporting incidence rate ratios. Length of stay and costs were analyzed using generalized linear models with log link and gamma or log-normal distributions. Multilevel models or robust standard errors addressed clustering within departments and facilities.
Subgroup analyses examined effect heterogeneity across age (below versus 65 years and older), sex, clinical service type, oncology status, baseline severity, ICU admission, and time periods (2020–2022 versus 2023–2024). Sensitivity analyses tested alternative MDT exposure windows (±3 and ±10 days), calculated E-values for unmeasured confounding, evaluated negative control outcomes, and excluded extreme values for length of stay and costs. Two-sided P values less than 0.05 indicated statistical significance, with false discovery rate correction applied when appropriate. Analyses were performed using R version 4.3.0, Stata version 17, and Python version 3.10.
Results
Study Population and Baseline Characteristics
The study population selection process is illustrated in Figure 1. Among 186,542 total hospital admissions during the study period from January 2020 to December 2024, 15,284 were excluded for not meeting age or temporal criteria. After excluding 9468 patients with missing essential data, extreme length of stay values, or day-case admissions, 161,790 patients remained. Following propensity score assessment and trimming of extreme propensity scores, the final analytical cohort comprised 158,358 patients. Of these, 142,156 patients (89.8%) constituted the non-MDT group with no documented multidisciplinary team discussion within 7 days before or after admission, while 16,202 patients (10.2%) comprised the MDT group with at least one MDT discussion during this time window.
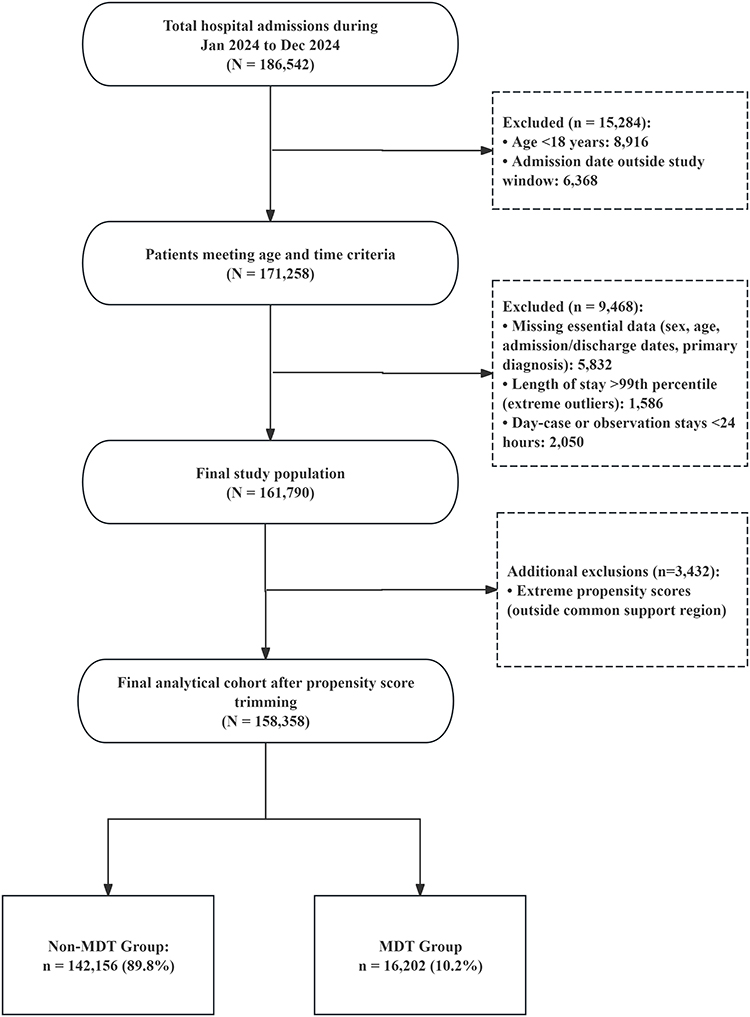 |
Figure 1 Study Population Selection Flowchart. |
The study included a total of 158,358 adult hospitalized patients, with the majority not receiving MDT discussion during their index admission. As shown in Table 1, Before propensity score weighting, substantial differences existed between the MDT and non-MDT groups across multiple baseline characteristics. Patients who received MDT consultation were older, had higher comorbidity burden as indicated by elevated Charlson Comorbidity Index scores, and were more likely to carry oncological diagnoses. The MDT group also demonstrated higher proportions of emergency department admissions and were predominantly managed in internal medicine departments. These findings suggested that MDT discussions were preferentially applied to patients with greater disease complexity and clinical severity, reflecting selection patterns in real-world clinical practice. Following inverse probability of treatment weighting, balance was achieved across all measured covariates between the two groups. The standardized mean differences for all variables were reduced to values indicating negligible differences, confirming successful mitigation of baseline confounding. The weighted populations showed comparable distributions in demographic characteristics, insurance status, comorbidity profiles, primary diagnostic categories, care delivery patterns, and temporal trends. This balance enabled valid comparisons of clinical outcomes and resource utilization between patients who did and did not receive MDT discussion, with reduced bias from measured confounders.
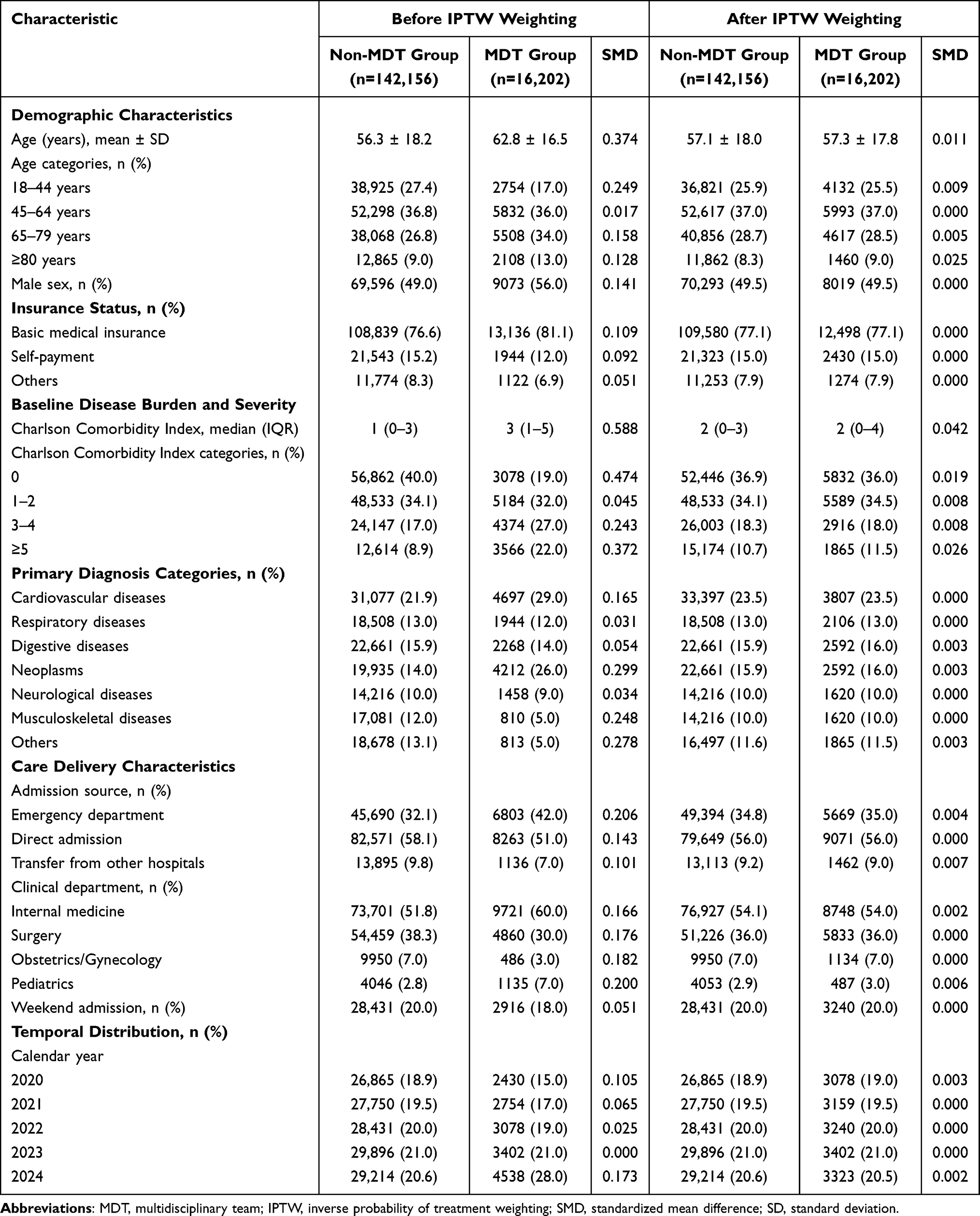 |
Table 1 Baseline Characteristics of Study Population Before and After Propensity Score Weighting |
Clinical Outcomes and Resource Utilization
After propensity score weighting, adjust model was adjusted for age, sex, insurance status, Charlson Comorbidity Index, primary diagnosis, admission source, clinical department, weekend admission, calendar year, and hospital clustering using multilevel modeling or robust standard errors. As shown in Table 2, MDT involvement was associated with significant reductions in adverse clinical outcomes. In-hospital mortality was lower in the MDT group compared to the non-MDT group (adjusted OR = 0.78, P<0.001). Similarly, 30-day all-cause mortality showed a significant decrease (adjusted HR = 0.82, P<0.001). The MDT group also demonstrated lower rates of 30-day readmission (adjusted OR = 0.88, P<0.001) and complications (adjusted OR = 0.91, P=0.003). No statistically significant differences were observed in ICU admission rates or ICU length of stay between the two groups after adjustment.
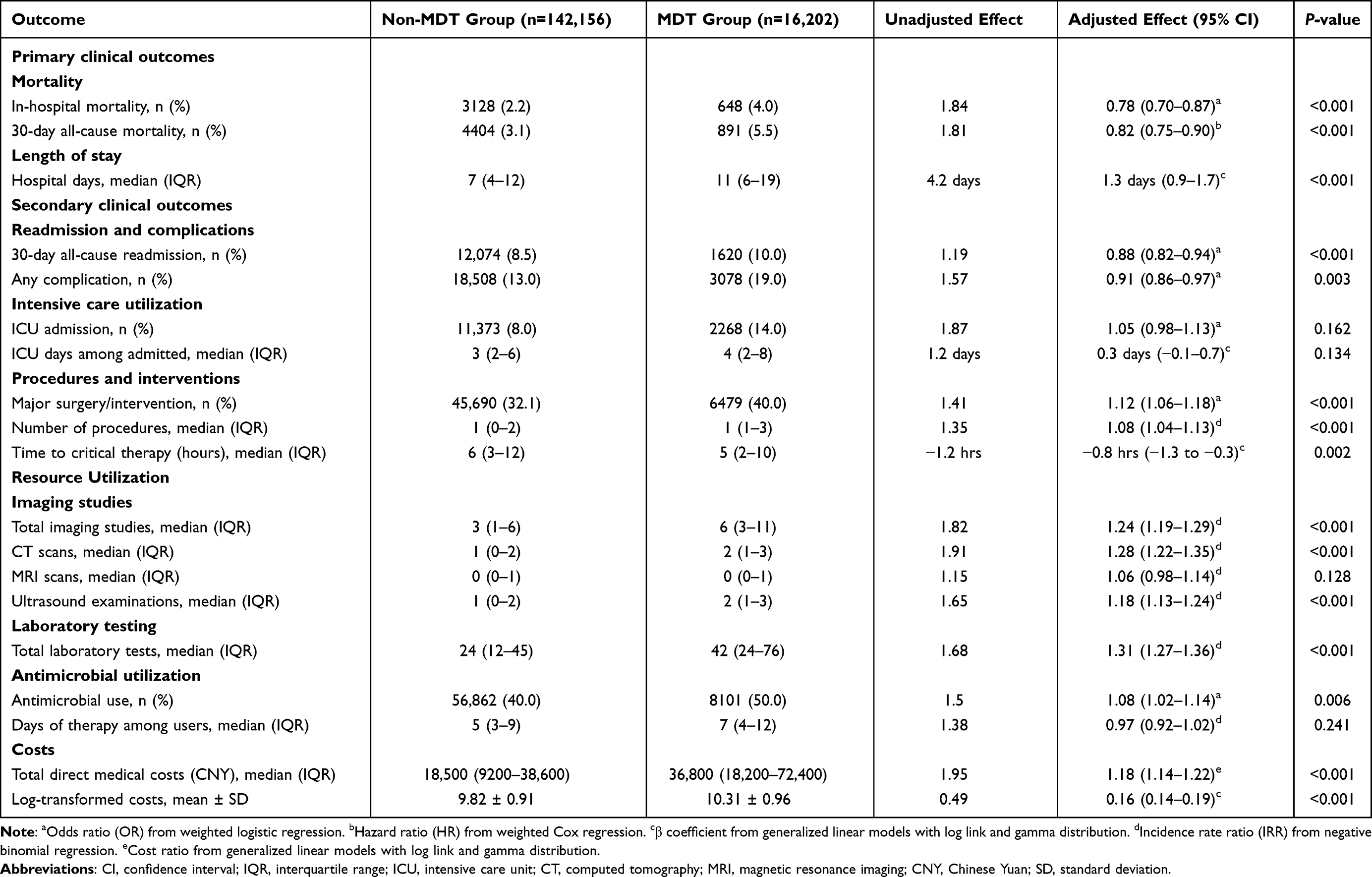 |
Table 2 Adjusted Effect Estimates for Primary and Secondary Outcomes |
Regarding procedural interventions, patients in the MDT group had higher rates of major surgery or interventional procedures (adjusted OR = 1.12, P<0.001) and shorter time to critical therapy initiation. However, MDT participation was associated with increased healthcare resource utilization across multiple domains. The adjusted median length of stay was longer in the MDT group (P<0.001). Imaging studies showed substantial increases, with total imaging examinations elevated by 24% (adjusted IRR = 1.24, P<0.001) and CT scans by 28% (adjusted IRR = 1.28, P<0.001). Laboratory testing frequency increased by 31% (adjusted IRR = 1.31, P<0.001). Total direct medical costs were 18% higher in the MDT group after adjustment (cost ratio = 1.18, P<0.001), reflecting the increased resource consumption associated with multidisciplinary care coordination.
Subgroup and Sensitivity Analyses
The protective association between MDT participation and in-hospital mortality remained consistent across many prespecified subgroups (Figure 2A). The effect was evident across all age categories, with adjusted ORs ranging from 0.71 to 0.84, though statistical significance was marginal among patients aged 80 years or older (P=0.046). No sex-related differences were observed. Significant heterogeneity emerged across clinical service types (P for interaction=0.037), with internal medicine patients demonstrating substantial mortality reduction (adjusted OR 0.73) while surgical, obstetric/gynecological, and pediatric patients showed no significant benefit. The protective effect was present across major diagnostic categories including cardiovascular, respiratory, and neoplastic diseases. Both oncology patients (adjusted OR 0.81) and non-oncology patients (adjusted OR 0.77) demonstrated similar mortality reductions with no significant interaction (P=0.684). Baseline disease severity significantly modified the MDT effect (P for interaction=0.012). Patients with lower comorbidity burden experienced greater mortality reductions, with adjusted OR of 0.59 among those with Charlson Index of zero compared to 0.89 among those with index of 5 or higher. Similarly, the protective effect was more pronounced in patients not requiring ICU admission (adjusted OR 0.68) versus those admitted to ICU (adjusted OR 0.91, P for interaction=0.006). Temporal analysis revealed consistent effects between 2020–2022 and 2023–2024 periods.
 |
Figure 2 Subgroup and Sensitivity Analyses for the Association Between MDT Participation and In-Hospital Mortality. (A) Forest plot of adjusted OR for in-hospital mortality across prespecified subgroups defined by demographic, clinical, and care delivery characteristics. (B) Forest plot of sensitivity analyses examining robustness under alternative analytic approaches including varying exposure windows, exclusion of extreme values, complete case analysis, propensity score matching, and different adjustment strategies. |
Multiple sensitivity analyses confirmed robustness of the primary findings (Figure 2B). Alternative MDT exposure windows (±3 and ±10 days) yielded comparable estimates (adjusted OR 0.75 and 0.80, respectively). Exclusion of extreme values, complete case analysis, and propensity score matching (adjusted OR 0.76) all produced consistent results. Both minimal and maximal covariate adjustment strategies supported the primary analysis. E-value analysis indicated that unmeasured confounders would require associations of magnitude 2.04 with both exposure and outcome to nullify the observed effect for in-hospital mortality (E-value for CI lower bound=1.73), and 1.86 for 30-day mortality (E-value for CI lower bound=1.60), suggesting reasonable robustness to unmeasured confounding.
Discussion
This retrospective cohort study involving hospitalized patients across tertiary hospital settings demonstrated that MDT decision-making was associated with significant reductions in mortality and adverse clinical outcomes, alongside substantial increases in healthcare resource utilization. After propensity score adjustment to address baseline differences between groups, MDT participation showed protective associations with in-hospital mortality, 30-day mortality, readmission rates, and complication occurrence. These clinical improvements, however, came at the cost of increased consumption of diagnostic resources, extended hospital stays, and elevated direct medical expenditures.
The magnitude of mortality reduction observed in this study aligned with findings from intensive care settings. Kim et al11 in a population-based cohort of 107,324 medical ICU patients across 169 Pennsylvania hospitals, found that MDT rounds were associated with reduced 30-day mortality (OR=0.84), with benefits particularly evident in ICUs with low-intensity physician staffing. The present study observed a similar effect size (adjusted HR=0.82) but validated this finding in a broader hospitalized patient population, suggesting that MDT benefits may extend beyond critically ill patients. Notably, Srinivas et al recently reported that MDT rounds reduced all-cause mortality from 2.8% to 1.6%, a greater reduction than observed in the current study, potentially reflecting differences in MDT implementation models and patient populations.12 Within specific disease contexts, Roy et al13 demonstrated that infective endocarditis patients managed by MDTs experienced a 39% reduction in short-term mortality risk (RR=0.61, 95% CI: 0.47–0.78), suggesting that MDT clinical benefits may be more pronounced in conditions with high complexity requiring multi-specialty collaboration.
Regarding increased resource utilization, the present findings show both consistencies and contradictions with existing literature. Weinstein et al studying a community-based heart failure unit, found that MDT intervention paradoxically reduced hospitalizations by 50% and total healthcare costs by 34%.14 This contradictory results may stem from several differences: their study focused on outpatient heart failure management where the primary MDT role was optimizing medication therapy and preventing decompensation, whereas the inpatient MDT in the current study more frequently involved diagnostic workups and treatment strategy modifications. Jokelin et al15 in a scoping review of primary care MDTs, noted that while MDT interventions generally demonstrated positive clinical outcomes, cost-effectiveness evidence remained insufficient and highly heterogeneous. An economic review that reported costs and resource use required to support MDTs varied considerably, with MDTs representing substantial expenses despite presumed clinical benefits.16 A recent review demonstrated that interdisciplinary team-based care improved self-management and patient-reported outcomes in chronically ill patients, though effects on clinical outcomes remained heterogeneous, suggesting the notion that patient characteristics substantially influence MDT impact.17 The resource increases observed in this study may reflect more aggressive diagnostic strategies following MDT discussions, including more frequent imaging assessments and laboratory monitoring, which ensure comprehensive treatment decision-making while increasing healthcare system burden.
Subgroup analyses in this study revealed the critical importance of patient selection for MDT effectiveness. Patients with lower baseline comorbidity burden (Charlson index of 0) exhibited greater mortality reduction (OR=0.59), while benefits diminished among those with high comorbidity burden (index ≥5, OR=0.89). This finding is similar to observations by Stairmand et al in cancer MDTs, where insufficient comorbidity information often rendered MDT treatment recommendations difficult to implement in complex patients.18 Another prospective study of neuromodulation candidates, confirmed that patients screened and optimized through MDT conferences achieved trial success rates of 80.5% compared to 45.7% without MDT involvement (OR=4.9) emphasizing the pivotal role of precise patient selection in enhancing MDT efficacy.19 The present study suggested that for patients with relatively straightforward conditions and lighter comorbidity burden, MDT may deliver greater benefits through more precise diagnosis and treatment planning; conversely, for multimorbid patients, disease complexity and treatment limitations may attenuate the relative advantages of MDT. This effect modification should guide healthcare institutions to prioritize complex but non-terminal patients for MDT discussions when resources are constrained. The findings from this study have important implications for optimizing MDT implementation in clinical practice. Recent evidence from cancer care settings has proposed streamlining strategies whereby complex cases are prioritized for full MDT discussion while straightforward cases follow standardized pathways.20 Such risk-stratified approaches could enhance efficiency without compromising quality, particularly given the resource intensification observed in this study. Integration of clinical decision support systems represents another promising direction. A prospective multicenter study demonstrated 83% concordance between MDT recommendations and guideline-based clinical decision trees in oncology settings, suggesting that technology-assisted decision-making could standardize MDT processes while reducing unnecessary variation.21 The 2024 European Society of Cardiology guidelines for atrial fibrillation explicitly advocate for MDT approaches, emphasizing integrated care models that include nurses and allied professionals alongside physicians.22 This guideline-driven endorsement reflects growing recognition of MDT value in managing complex conditions. Implementation research has highlighted that successful adoption requires addressing organizational barriers, establishing clear role definitions, and fostering supportive team climates.23 These strategies could mitigate the resource burden identified in this study while maintaining clinical benefits, particularly through selective application to patients most likely to benefit and integration of technology to streamline workflows.
Several methodological strengths support the validity of these findings. The large sample size (>150,000 admissions) provided robust statistical power and enabled extensive subgroup evaluations. Propensity score methods with multiple sensitivity analyses, including E-value calculations, demonstrated reasonable robustness to unmeasured confounding. The simultaneous assessment of clinical outcomes and resource utilization offers practical insights for healthcare policy.
Several limitations should be acknowledged. As an observational study, unmeasured confounding and selection bias cannot be entirely excluded, as patients with more complex conditions were more likely selected for MDT discussion. The study lacked direct measurements of MDT discussion quality, including participating specialties, discussion duration, decision implementation rates, and adherence to MDT recommendations—an inherent limitation of registry-based analyses. The inclusion of data exclusively from Chinese tertiary hospitals limits generalizability, although MDT protocols at participating institutions align with international standards. Future research should focus on prospective trials to establish causal effects and identify optimal patient selection criteria for MDT implementation.
Conclusion
In this retrospective observational study, MDT decision-making in tertiary hospital settings was associated with improved clinical outcomes including reduced mortality, readmission rates, and complications, particularly among internal medicine patients with lower baseline comorbidity burden. These benefits occurred alongside increased healthcare resource utilization and costs. These hypothesis-generating findings require confirmation through prospective studies, and highlight the need for careful patient selection and implementation strategies to optimize the balance between clinical effectiveness and resource efficiency.
Data Sharing Statement
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by the Ethics Committee of The First Affiliated Hospital of Guangxi Medical University (Approval Number: ZS2022022). Due to the retrospective nature of the study, the requirement for informed consent was waived by the Ethics Committee of The First Affiliated Hospital of Guangxi Medical University. Patient confidentiality was ensured by anonymizing the data prior to analysis.
Funding
This study was supported by 2024 Self-funded Research Project of Health Commission of Guangxi Zhuang Autonomous Region (No.: Z-A20240516); The Hospital Management Research and Cultivation Project of the First Affiliated Hospital of Guangxi Medical University in 2022 (No.: YYZS2022022).
Disclosure
The authors declare that there are no conflicts of interest related to this study.
References
1. Taberna M, Gil Moncayo F, Jané-Salas E, et al. The Multidisciplinary Team (MDT) approach and quality of care. Front Oncol. 2020;10:85. doi:10.3389/fonc.2020.00085
2. Kobrai-Abkenar F, Salimi S, Pourghane P. “Interprofessional collaboration” among pharmacists, physicians, and nurses: a hybrid concept analysis. Iran J Nurs Midwifery Res. 2024;29(2):238–12. doi:10.4103/ijnmr.ijnmr_336_22
3. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: a systematic review of the literature. Cancer Treat Rev. 2016;42:56–72. doi:10.1016/j.ctrv.2015.11.007
4. Hendriks MP, Jager A, Ebben KCWJ, van Til JA, Siesling S. Clinical decision support systems for multidisciplinary team decision-making in patients with solid cancer: composition of an implementation model based on a scoping review. Crit Rev Oncol Hematol. 2024;195:104267. doi:10.1016/j.critrevonc.2024.104267
5. Rizky D, Yunarvika V, Putra YR, et al. Impact of independent multidisciplinary work on the survival rate of stage 3 and 4 nasopharyngeal cancer in Indonesia: a retrospective cohort study. Ann Med Surg. 2023;85(9):4248–4255. doi:10.1097/MS9.0000000000001074
6. Shi Y, Li H, Yuan B, Wang X. Effects of multidisciplinary teamwork in non-hospital settings on healthcare and patients with chronic conditions: a systematic review and meta-analysis. BMC Primary Care. 2025;26(1):110. doi:10.1186/s12875-025-02814-0
7. Williams GJ, Thompson JF. Management changes and survival outcomes for cancer patients after multidisciplinary team discussion; a systematic review and meta-analysis. Cancer Treat Rev. 2025;139:102997. doi:10.1016/j.ctrv.2025.102997
8. Hahlweg P, Didi S, Kriston L, Härter M, Nestoriuc Y, Scholl I. Process quality of decision-making in multidisciplinary cancer team meetings: a structured observational study. BMC Cancer. 2017;17(1):772. doi:10.1186/s12885-017-3768-5
9. Shaw M, Pelecanos AM, Mudge AM. Evaluation of internal medicine physician or multidisciplinary team comanagement of surgical patients and clinical outcomes: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(5):e204088. doi:10.1001/jamanetworkopen.2020.4088
10. Jia J, Sun T, Tang J, et al. Participation in multidisciplinary teams among healthcare professionals: a discrete choice experiment in tertiary public hospitals in China. J Multidiscip Healthc. 2024;17:4397–4409. doi:10.2147/JMDH.S473675
11. Kim MM, Barnato AE, Angus DC, Fleisher LF, Kahn JM. The effect of multidisciplinary care teams on intensive care unit mortality. Arch Intern Med. 2010;170(4):369–376.
12. Srinivas V, Choubey U, Motwani J, et al. Synergistic strategies: optimizing outcomes through a multidisciplinary approach to clinical rounds. Bayl Univ Med Cent Proc. 2024;37(1):144–150.
13. Roy A-S, Hagh-Doust H, Abdul Azim A, et al. Multidisciplinary teams for the management of infective endocarditis: a systematic review and meta-analysis. Open Forum Infect Dis. 2023;10(9):ofad444. doi:10.1093/ofid/ofad444
14. Weinstein JM, Greenberg D, Sharf A, Simon-Tuval T. The impact of a community-based heart failure multidisciplinary team clinic on healthcare utilization and costs. ESC Heart Fail. 2022;9(1):676–684. doi:10.1002/ehf2.13689
15. Jokelin E, Karreinen S, Mustonen E, Torkki P. Clinical and economic outcomes of multidisciplinary team members in primary care: a scoping review. BMC Health Serv Res. 2025;25(1):1025. doi:10.1186/s12913-025-13243-1
16. Ke KM, Blazeby JM, Strong S, Carroll FE, Ness AR, Hollingworth W. Are multidisciplinary teams in secondary care cost-effective? A systematic review of the literature. Cost Eff Resour Alloc. 2013;11(1):7. doi:10.1186/1478-7547-11-7
17. Kongkar R, Ruksakulpiwat S, Phianhasin L, et al. The impact of interdisciplinary team-based care on the care and outcomes of chronically Ill patients: a systematic review. J Multidiscip Healthc. 2025;18:445–457. doi:10.2147/JMDH.S497846
18. Stairmand J, Signal L, Sarfati D, et al. Consideration of comorbidity in treatment decision making in multidisciplinary cancer team meetings: a systematic review. Ann Oncol. 2015;26(7):1325–1332. doi:10.1093/annonc/mdv025
19. Salmasi V, Rasouli MR, Kao MC, et al. Application of multidisciplinary team conference for neuromodulation candidates facilitates patient selection and optimization. Front Pain Res. 2023;4:1331883. doi:10.3389/fpain.2023.1331883
20. Al-Hammouri T, Almeida-Magana R, Soukup T, Lamb B. Implementation of streamlining measures in selecting and prioritising complex cases for the cancer multidisciplinary team meeting: a mini review of the recent developments. Front Health Serv. 2024;4:1340320. doi:10.3389/frhs.2024.1340320
21. Ebben KCWJ, Hendriks MP, Markus L, et al. Using guideline-based clinical decision support in oncological multidisciplinary team meetings: a prospective, multicenter concordance study. Int J Qual Health Care. 2022;34(1):mzac007. doi:10.1093/intqhc/mzac007
22. Desteghe L, Lee G, Antoniou S, et al. A multidisciplinary team approach in the 2024 ESC guidelines for the management of patients with Atrial Fibrillation—what is the role of nurses and allied professionals? A clinical consensus statement of the association of cardiovascular nursing and allied professions (ACNAP) and the European Heart Rhythm Association (EHRA) of the ESC. Eur J Cardiovasc Nurs. 2025;24(6):828–840. doi:10.1093/eurjcn/zvaf083
23. McGuier EA, Kolko DJ, Aarons GA, et al. Teamwork and implementation of innovations in healthcare and human service settings: a systematic review. Implement Sci. 2024;19(1):49. doi:10.1186/s13012-024-01381-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Healthcare Resource Utilization, Cost and Clinical Outcomes in Patients Diagnosed with COPD Initiating Tiotropium Bromide/Olodaterol versus Fluticasone Furoate/Umeclidinium/Vilanterol Based on Exacerbation History
Sethi S, Clark B, Bengtson LG, Buysman EK, Palli S, Sargent A, Shaikh A, Ferguson GT
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:625-641
Published Date: 19 April 2023
Risk Factors for 30-Days Mortality After Proximal Femoral Fracture Surgery, a Cohort Study
de Haan E, Roukema GR, van Rijckevorsel VA, Kuijper TM, de Jong L
Clinical Interventions in Aging 2024, 19:539-549
Published Date: 21 March 2024
Characteristics and Outcomes of People With COPD Who Experience Exacerbations While on Inhaled Triple Therapy: Results of the SIRIUS I Cohort Study in the US (2015–2019)
Nordon C, Carstens D, Fagerås M, Müllerová H, Veeranki PS, Alves JA, Germack HD, Barnes TL, McCormack MC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1851-1864
Published Date: 11 June 2025