Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Healthcare Resource Utilization, Cost and Clinical Outcomes in Patients Diagnosed with COPD Initiating Tiotropium Bromide/Olodaterol versus Fluticasone Furoate/Umeclidinium/Vilanterol Based on Exacerbation History
Authors Sethi S ![]() , Clark B
, Clark B ![]() , Bengtson LG, Buysman EK, Palli S, Sargent A, Shaikh A
, Bengtson LG, Buysman EK, Palli S, Sargent A, Shaikh A ![]() , Ferguson GT
, Ferguson GT ![]()
Received 30 August 2022
Accepted for publication 18 March 2023
Published 19 April 2023 Volume 2023:18 Pages 625—641
DOI https://doi.org/10.2147/COPD.S386962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Sanjay Sethi,1 Brendan Clark,2 Lindsay GS Bengtson,3 Erin K Buysman,3 Swetha Palli,2 Andrew Sargent,3 Asif Shaikh,2 Gary T Ferguson4
1Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, Buffalo, NY, USA; 2Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA; 3Optum Life Sciences, Eden Prairie, MN, USA; 4Department of Medicine, Pulmonary Research Institute of Southeast Michigan, Farmington Hills, MI, USA
Correspondence: Brendan Clark, Boehringer Ingelheim Pharmaceuticals, Inc, 900 Ridgebury Road, Ridgefield, CT, 06877, USA, Email [email protected]
Background: ATS and GOLD guidelines recommend treating low-exacerbation risk COPD patients with dual (LAMA/LABA) agents and reserving triple therapy (TT; LAMA/LABA and inhaled corticosteroids [ICS]) for severe cases with higher-exacerbation risk. However, TT often is prescribed across the COPD spectrum. This study compared COPD exacerbations, pneumonia diagnosis, healthcare resource utilization, and costs for patients initiating tiotropium bromide/olodaterol (TIO/OLO) and a TT, fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI), stratified by exacerbation history.
Methods: COPD patients who initiated TIO/OLO or FF/UMEC/VI between 06/01/2015— 11/30/2019 (index date=first pharmacy fill-date with ≥ 30 consecutive treatment days) were identified from the Optum Research Database. Patients were ≥ 40 years old and continuously enrolled for 12 months during the baseline period and ≥ 30 days during follow-up. Patients were stratified into GOLD A/B (0– 1 baseline non-hospitalized exacerbation), No exacerbation (subset of GOLD A/B), and GOLD C/D (≥ 2 non-hospitalized and/or ≥ 1 hospitalized baseline exacerbation). Baseline characteristics were balanced with propensity score matching (1:1). Adjusted risks of exacerbation, pneumonia diagnosis, and COPD and/or pneumonia-related utilization and costs were evaluated.
Results: Adjusted exacerbation risk was similar in GOLD A/B and No exacerbation subgroups, and lower in GOLD C/D for FF/UMEC/VI versus TIO/OLO initiators (hazard ratio: 0.87; 95% CI: 0.78, 0.98, p=0.020). Adjusted pneumonia risk was similar between cohorts across the GOLD subgroups. Adjusted COPD and/or pneumonia-related population annualized pharmacy costs were significantly higher for FF/UMEC/VI versus TIO/OLO initiators across subgroups, p< 0.001. Adjusted COPD and/or pneumonia-related population annualized total healthcare costs were significantly higher for FF/UMEC/VI versus TIO/OLO initiators in the GOLD A/B and No exacerbation, subgroups, p< 0.001 (cost ratio [95% CI]: 1.25 [1.13, 1.38] and 1.21 [1.09, 1.36], respectively), but similar in the GOLD C/D subgroup.
Conclusion: These real-world results support ATS and GOLD recommendations for treating low-exacerbation risk COPD patients with dual bronchodilators and TT for more severe, higher-exacerbation risk COPD patients.
Keywords: COPD, tiotropium bromide/olodaterol, fluticasone furoate/umeclidinium/vilanterol, exacerbation history, healthcare resource utilization, cost, clinical outcomes
Plain Language Summary
The American Thoracic Society (ATS) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommend prescribing dual therapy (LAMA/LABA) for COPD patients with low-exacerbation risk and reserving triple therapy (TT) for patients with severe/higher-exacerbation risk COPD. Patients often receive treatment that overlooks this guidance, and lower-risk patients are treated with TT rather than dual or monotherapy. We assessed COPD exacerbations, pneumonia risk, resource use and costs in insured patients with COPD who started COPD treatment with either a dual therapy TIO/OLO or the TT, FF/UMEC/VI. First, we categorized the patients into subgroups by their exacerbation history: GOLD A/B (0–1 baseline non-hospitalized exacerbation), No exacerbation (a subset of GOLD A/B), and GOLD C/D (≥2 non-hospitalized and/or ≥1 hospitalized baseline exacerbation). After adjusting for baseline differences between the TIO/OLO and FF/UMEC/VI cohorts, there was no difference in exacerbation risk between the TIO/OLO and the FF/UMEC/VI cohorts in the GOLD A/B and No exacerbation subgroups. In the GOLD C/D subgroup, however, patients in the FF/UMEC/VI cohort had a lower adjusted exacerbation risk than patients in the TIO/OLO cohort. In the GOLD A/B and No exacerbation subgroups, healthcare costs were significantly higher for the FF/UMEC/VI cohort compared to the TIO/OLO cohort but similar between cohorts in the GOLD C/D subgroup. These results support the ATS and GOLD recommendations for treating mild-to-moderate COPD patients with dual therapy, and suggest considerable cost savings could be realized in following them in everyday practice.
Introduction
The American Thoracic Society (ATS) 2020 Clinical Practice Guidelines recommend long-acting muscarinic antagonist/beta2-agonist (LAMA/LABA) combination therapy versus monotherapy for patients with COPD who experience dyspnea/exercise intolerance. Escalation to triple therapy (TT), with LAMA, LABA and inhaled corticosteroids (ICS), is recommended for patients continuing to experience dyspnea/exercise intolerance, and who had ≥1 exacerbation requiring hospitalization and/or treatment with antibiotics/oral steroids in the prior year.1
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has similar recommendations, and identifies COPD patient exacerbation risk subgroupings based on their prior year history: A/B (low) and C/D (high).2 GOLD guidance recommends LAMA/LABA as next-in-line therapy for symptomatic COPD patients on mono-maintenance therapy.2 GOLD 2022 recommends consideration of ICS and/or escalating to TT for patients experiencing further exacerbation(s) on dual therapy, after a risk/benefit assessment related to the potential for pneumonia and other side-effects.2
The rationale for our study is that results from randomized clinical trials (RCTs) of fixed dose combination (FDC) TTs, which included a mostly severe COPD subpopulation at higher risk for exacerbations, may not be generalizable to real-world practice. Real-world studies suggest that TT is overprescribed across all COPD severities,3–6 especially to patients in low exacerbation risk Groups A and B who comprise the majority of the COPD population.7 Other real-world US studies in maintenance-treated COPD patients report that 60–80% of patients were prescribed TT treatment in discordance with GOLD recommendations.6,8
A German DACCORD registry study found that at 1-year follow-up, significantly fewer patients on LABA+LAMA experienced an exacerbation, and at a significantly lower rate versus patients on triple therapy.9 Furthermore, an observational study suggested that tiotropium bromide/olodaterol (TIO/OLO) may be associated with improved economic and COPD-related health outcomes, with less pneumonia risk versus TT,8 and an economic analysis of a managed care Medicare population reported that COPD-related and all-cause costs were lower for TIO/OLO versus TT.6 These studies, however, focused on free-dose TT, reflecting a need for real-world evidence on FDC TT.
The purpose of this study was to compare COPD exacerbations, pneumonia, COPD and/or pneumonia-related and all-cause healthcare resource utilization (HCRU) and costs among patients newly treated with TIO/OLO or fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI), stratified by GOLD exacerbation risk.5
Methods
Study Design and Data Source
This retrospective observational cohort study included administrative claims data from the Optum Research Database (ORD), a repository of deidentified information for more than 73 million enrollees with commercial or Medicare Advantage with Part D (MAPD) insurance coverage. Institutional review board and informed consent procedures were not sought nor required for this study, which accessed no identifiable protected health information in accordance with the United States Department of Health and Human Services Privacy Rule requirements for de-identification codified at 45 C.F.R. § 164.514 (b). Patient privacy was preserved, and Health Insurance Portability and Accountability Act (HIPAA) rules were complied with throughout.
Study Population
Inclusion Criteria
Included patients had ≥30 consecutive days of TIO/OLO or FF/UMEC/VI treatment initiated during the identification period. The US Food and Drug Administration (FDA) approved Stiolto® Respimat® (TIO/OLO) on 05/21/2015,10 and Trelegy® Ellipta® (FF/UMEC/VI) on 09/18/2017,11 for COPD. TIO/OLO initiators before and after the launch of FF/UMEC/VI were compared to ensure similar population characteristics before and after FDA’s FF/UMEC/VI approval. TIO/OLO initiators were well-balanced on a priori characteristics. The index date was set to the first qualifying pharmacy fill-date between 06/01/2015-11/30/2019. Patients with ≥1 facility claim with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and/or International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) primary diagnosis for COPD or ≥2 professional claims with a COPD diagnosis, on separate service dates during the study period (06/01/2014-12/31/2019), who were ≥40 years of age as of the index year and had continuous enrollment with medical and pharmacy coverage for 12 months prior to and including the index date (baseline period) and for ≥30 days following the index date were included.
Exclusion Criteria
Patients were excluded if they had ≥2 baseline medical claims on separate dates of service with asthma, cystic fibrosis, lung cancer, or interstitial lung disease diagnosis; index date pharmacy claims for both TIO/OLO and FF/UMEC/VI; pharmacy claims for any non-index COPD maintenance medication on the index date (LAMA, LABA, or ICS monotherapy; LABA/ICS or non-TIO/OLO LAMA/LABA FDC); free or FDC LAMA/LABA or TT (defined as ≥7 consecutive days of overlapping days’ supply with a LAMA and LABA or an ICS, LABA, and LAMA, respectively) during the 6-months prior to and excluding the index date; ≥1 medical claim with a procedure code for lung volume reduction during the study period; and unknown age/gender/insurance coverage, or unknown or other geographic region.
GOLD Groups
The GOLD A/B population consisted of patients with 0–1 baseline exacerbation not leading to hospitalization. The No Exacerbation population, a subset of the GOLD A/B, consisted of patients with no baseline exacerbation. The GOLD C/D population included patients with ≥2 baseline exacerbations not leading to hospitalization and/or ≥1 baseline exacerbation leading to hospitalization.
Baseline Variables
Baseline demographics, clinical characteristics including comorbidity burden, COPD severity score, and baseline medication use were assessed from both pharmacy and medical claims.
Follow-Up and Outcomes
Follow-up continued until the earliest of switch to non-index maintenance COPD medication, discontinuation of index medication, disenrollment from health plan, 12 months post-index date, or end of the study period. All outcomes were assessed during this variable period starting on the day after the index date, with a minimum of 30-days duration up to a maximum of 12 months. Clinical outcomes included COPD exacerbations and pneumonia-related events.
Exacerbations occurring within 14 days of each other were considered a single exacerbation episode and were classified according to the highest severity contributing event. A severe exacerbation was defined as hospitalization/emergency room (ER) visit with a primary COPD diagnosis; or hospitalization/ER visit with a primary acute respiratory failure diagnosis and a COPD diagnosis; or hospitalization/ER visit with a primary acute respiratory failure diagnosis plus hospitalization/ER visit within ±7 days with a COPD diagnosis. A moderate exacerbation was defined as an office/outpatient visit with a COPD diagnosis plus a pharmacy claim for oral corticosteroids (OCS) and/or antibiotics within ±7 days.
All-cause HCRU included hospitalizations, ER visits, physician office visits, hospital outpatient visits, other services (including but not limited to independent laboratories, assisted living facilities, and home health providers) and pharmacy claims. All-cause healthcare costs were assessed using plan paid plus patient paid amounts. Total healthcare costs combined pharmacy, and medical costs categorized as hospitalization, ER services, physician office, hospital outpatient, and other costs. COPD and/or pneumonia-related HCRU and costs were analogous to their respective all-cause outcomes but restricted to utilization with a diagnosis for COPD, pneumonia, or acute bronchitis/bronchiolitis in any position or for a COPD-related treatment including rescue and controller therapies and COPD-guideline recommended antibiotics. Costs were adjusted to 2020 US dollars based on the medical care component of the Consumer Price Index (CPI).12
Statistical Analysis
A stratified propensity score match (PSM) was used to 1:1 hard match TIO/OLO and FF/UMEC/VI patients on baseline exacerbation (yes/no), baseline GOLD A/B and C/D status, and baseline maintenance therapy naive status (yes/no). The propensity score model included demographics, baseline comorbidity burden, COPD disease characteristics, use of respiratory medications, and all-cause, COPD-related, and pneumonia-related HCRU and costs. A standardized mean difference (SMD) of ≤10% for each measure was deemed acceptable to indicate balance between the cohorts.
Follow-up variables were presented as population annualized averages with Wald 95% confidence intervals using Taylor expansion to estimate the standard error, and were calculated as:

Kaplan-Meier analysis was used to estimate time to first COPD exacerbation and pneumonia diagnosis. To adjust for baseline characteristics that remained imbalanced post-match, multivariable analyses (MVA) were conducted for COPD and/or pneumonia-related total (pharmacy and medical) costs, and hospitalization, any exacerbation, and pneumonia diagnosis. Cost outcomes were modeled with generalized linear models (GLM) using a gamma distribution and log link; except for the GOLD C/D population, where total costs were modeled with inverse Gaussian distribution. Cost ratios were estimated via exponentiated coefficients from a GLM. The average adjusted cost for each cohort was estimated using recycled predictions. Counts of hospitalizations were modeled with negative binomial models, and time to first exacerbation and pneumonia diagnosis with Cox proportional hazard models. All models accounted for clustering within the matched pairs with an a-priori α=0.05 for statistical significance. Statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC).
Results
Patient Disposition
The analysis included 16,338 patients: approximately 40% initiated TIO/OLO (n=6681) and 60% initiated FF/UMEC/VI (n=9657). SMDs between TIO/OLO initiators before (n=3085; 46.2%) and after FF/UMEC/VI approval (n=3596; 53.8%) were balanced on all a-priori specified characteristics, except insurance type for which imbalances were not meaningful (data not shown). TIO/OLO and FF/UMEC/VI post-match treatment cohorts included 3884, 2552, and 1774 matched pairs for the GOLD A/B, No exacerbation, and GOLD C/D subgroups, respectively (Supplemental Figure 1).
Baseline Patient Characteristics
Pre-Match
Pre-match patient characteristics provided in Supplemental Table 1.
Baseline Patient Characteristics
Post-Match
Post-match, the TIO/OLO and FF/UMEC/VI cohorts were similar in age, gender, and insurance type; however, some imbalances persisted (Table 1). Imbalance was frequently observed for other/unknown race/ethnicity, any LAMA, LABA, ICS, and LABA/ICS FDC, and pneumonia-related hospitalization days.
 |
Table 1 Post-Match Clinical and Demographic Characteristics at Baseline |
Exacerbation and Pneumonia Diagnosis
GOLD A/B
Time to follow-up for any exacerbation, severe exacerbation, or pneumonia diagnosis was similar for patients in the TIO/OLO and FF/UMEC/VI cohorts. The population annualized count of any COPD exacerbations was also similar. In Kaplan-Meier analysis, 41.4% and 41.6% of patients treated with TIO/OLO and FF/UMEC/VI, respectively, had any COPD exacerbation at one year, sandwich p=0.916, while 12.9% and 13.1%, respectively, had a severe exacerbation at one year, sandwich p-value=0.731. Similarly, in Kaplan-Meier analysis, 12.5% and 14.5% of TIO/OLO and FF/UMEC/VI initiators, respectively, had a pneumonia diagnosis at one year, sandwich p-value=0.077. There was no difference in adjusted risks for any exacerbation or pneumonia diagnosis between the FF/UMEC/VI and TIO/OLO initiators. (Figure 1a)
Figure 1 Continued. Figure 1 (a) Follow-up exacerbation and pneumonia diagnosis in the GOLD A/B subgroup. (b): Follow-up exacerbation and pneumonia diagnosis in the No Exacerbation subgroup. (c): Follow-up exacerbation and pneumonia diagnosis in the GOLD C/D subgroup. Notes: (a): aA severe exacerbation was defined as a hospitalization or an ER visit with: a COPD diagnosis code in the primary position; a diagnosis code for acute respiratory failure in the primary position and a COPD diagnosis code in any position; or a diagnosis code for acute respiratory failure in the primary position + a hospitalization or an ER visit within ±7 days with a COPD diagnosis code in any position. A moderate exacerbation was defined as: an ambulatory (office or outpatient) visit with a COPD diagnosis code in any position + a pharmacy claim for an oral corticosteroid (OCS) prescription within ±7 days of the office/outpatient visit; an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for COPD-guideline recommended antibiotic prescription within ±7 days of the office/outpatient visit; or an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for an OCS + a pharmacy claim for COPD-guideline recommended antibiotic prescription within ±7 days of the office/outpatient visit. bAdjusted for race/ethnicity, baseline LAMA monotherapy pharmacy claims, baseline LABA/ICS pharmacy claims, and baseline length of pneumonia-related hospitalization; p-values account for clustering within matched pairs. (b) aA severe exacerbation was defined as a hospitalization or an ER visit with: a COPD diagnosis code in the primary position; a diagnosis code for acute respiratory failure in the primary position and a COPD diagnosis code in any position; or a diagnosis code for acute respiratory failure in the primary position + a hospitalization or an ER visit within ±7 days with a COPD diagnosis code in any position. A moderate exacerbation was defined as: an ambulatory (office or outpatient) visit with a COPD diagnosis code in any position + a pharmacy claim for an oral corticosteroid (OCS) prescription within ±7 days of the office/outpatient visit; an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for COPD-guideline recommended antibiotic prescription within ±7 days of the office/outpatient visit; or an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for an OCS + a pharmacy claim for COPD-guideline recommended antibiotic prescription within =/-7 days of the office/outpatient visit; bAdjusted for race/ethnicity, baseline LAMA monotherapy pharmacy claims, baseline LABA/ICS pharmacy claims, baseline of COPD-related hospitalization, and and baseline length of pneumonia-related hospitalization; p-values account for clustering within matched pairs. (c): aA severe exacerbation was defined as a hospitalization or an ER visit with: a COPD diagnosis code in the primary position; a diagnosis code for acute respiratory failure in the primary position and a COPD diagnosis code in any position; or a diagnosis code for acute respiratory failure in the primary position + a hospitalization or an ER visit within ±7 days with a COPD diagnosis code in any position. A moderate exacerbation was defined as: an ambulatory (office or outpatient) visit with a COPD diagnosis code in any position + a pharmacy claim for an oral corticosteroid (OCS) prescription within ±7 days of the office/outpatient visit; an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for COPD-guideline recommended antibiotic prescription within ±7 days of the office/outpatient visit; or an office or outpatient visit with a COPD diagnosis code in any position + a pharmacy claim for an OCS + a pharmacy claim for COPD-guideline recommended antibiotic prescription within =/-7 days of the office/outpatient visit; bAdjusted for race/ethnicity, baseline count of SAMA fills, baseline count of medical claims for controller medications, baseline LAMA monotherapy pharmacy fills, baseline LABA/ICS pharmacy fills, baseline OCS pharmacy fills, baseline pharmacy claim count, and baseline pneumonia-related other medical visits; p-values account for clustering within matched pairs.
No Exacerbation
No difference was seen between cohorts in time to exacerbation and population annualized count of exacerbations in the No exacerbation subgroup. The time to pneumonia diagnosis, however, was significantly longer among TIO/OLO versus FF/UMEC/VI initiators. In Kaplan-Meier analysis, 36.8% and 38.4% of the TIO/OLO and FF/UMEC/VI cohorts, respectively, had an exacerbation at one year, sandwich p=0.608. In addition, 12.1% and 11.2% of the TIO/OLO and FF/UMEC/VI cohorts, respectively, had a severe exacerbation at one year, sandwich p-value=0.559. However, in Kaplan-Meier analysis, 10.0% TIO/OLO and 13.8% FF/UMEC/VI initiators had a pneumonia diagnosis at one year, sandwich p=0.037. There was no difference in adjusted risk of any exacerbation or risk of pneumonia diagnosis between the FF/UMEC/VI and TIO/OLO initiators. (Figure 1b)
GOLD C/D
The population annualized count of any COPD exacerbation was higher among TIO/OLO initiators (1.82; 95% CI: 1.69, 1.95) compared to FF/UMEC/VI (1.59; 95% CI: 1.48, 1.71), p=0.013. In Kaplan-Meier analysis, 71.0% and 70.6% of the TIO/OLO and FF/UMEC/VI cohorts, respectively, had an exacerbation at one year, sandwich p=0.024, and 33.8% and 29.6%, respectively, had a severe exacerbation at one year, sandwich p=0.255. Also, in Kaplan-Meier analysis, 26.6% TIO/OLO and 30.7% FF/UMEC/VI initiators had a pneumonia diagnosis at one year, sandwich p=0.745. In adjusted analyses, FF/UMEC/VI initiators had a lower risk of any exacerbation and a similar risk of pneumonia diagnosis versus TIO/OLO initiators. (Figure 1c)
COPD and/or Pneumonia-Related and All-Cause HCRU (Table 2)
GOLD A/B
Follow-up COPD and/or pneumonia-related HCRU was lower among TIO/OLO initiators compared with FF/UMEC/VI initiators; significant differences were observed for hospitalizations (0.27 vs 0.33; p=0.022), ambulatory visits (7.02 vs 7.72; p=0.036) and other medical visits (3.10 vs 3.62; p=0.004). The adjusted rate of COPD and/or pneumonia-related hospitalizations among FF/UMEC/VI initiators was higher than among TIO/OLO initiators (1.18; 95% CI: 1.00, 1.38; p=0.048). All-cause HCRU in the TIO/OLO and FF/UMEC/VI cohorts was similar, except for fewer ER visits among TIO/OLO versus FF/UMEC/VI initiators (0.95 vs 1.10; p=0.019), respectively.
 |
Table 2 All-Cause and COPD and/or Pneumonia-Related Healthcare Utilization |
No Exacerbation
COPD and/or pneumonia-related HCRU measures were similar between the cohorts with the exception of other medical visits that was lower for the TIO/OLO (2.71; 95% CI: 2.43, 2.99) versus FF/UMEC/VI cohort (3.39; 95% CI: 3.07, 3.71), p=0.001. All-cause HCRU measures were similar between the TIO/OLO and FF/UMEC/VI cohorts.
GOLD C/D
COPD and/or pneumonia-related HCRU generally was similar for the TIO/OLO and FF/UMEC/VI cohorts, except for higher outpatient pharmacy fills for TIO/OLO (19.74 vs 18.18; p<0.001), respectively. Follow-up all-cause HCRU was similar, except for higher pharmacy fills among TIO/OLO versus FF/UMEC/VI initiators (72.01 vs 65.37; p<0.001), respectively.
COPD and/or Pneumonia-Related and All-Cause Healthcare Costs (Figure 2)
GOLD A/B
The population annualized COPD and/or pneumonia-related total costs were significantly lower among TIO/OLO initiators versus FF/UMEC/VI initiators ($11,521 vs $14,464; p<0.001). Pharmacy costs were significantly lower for TIO/OLO versus FF/UMEC/VI initiators ($4612 vs $6484; p<0.001). For medical costs, COPD and/or pneumonia-related ER costs were significantly lower among TIO/OLO versus FF/UMEC/VI initiators ($303 vs $390; p=0.031). Population annualized all-cause total costs ($23,309 vs $26,244; p=0.002) and pharmacy costs ($9676 vs $11,484; p<0.001) were significantly lower among TIO/OLO versus FF/UMEC/VI initiators. Adjusted COPD and/or pneumonia-related pharmacy ($4632 vs $6455; p<0.001) and total healthcare costs ($11,557 vs $14,422; p<0.001) were significantly lower for TIO/OLO initiators compared to FF/UMEC/VI (Table 3). COPD and/or pneumonia-related medical costs were not significantly different between cohorts.
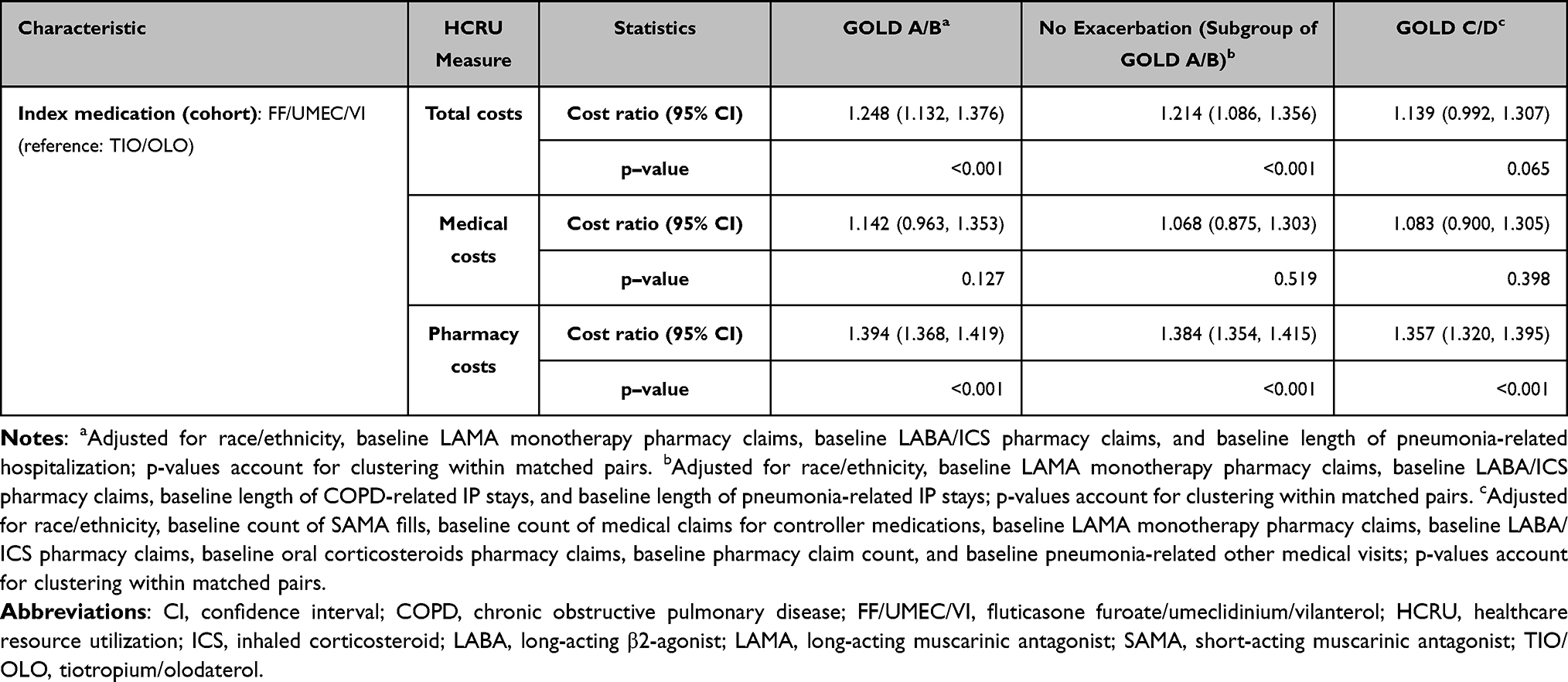 |
Table 3 Multivariable Analysis of COPD and/or Pneumonia-Related Costs |
 |
Figure 2 All-cause and COPD and/or pneumonia-related costs by GOLD subgroups. Notes: aOther costs include service in independent laboratory, home health, durable medical equipment, etc. *p-value <0.05 for comparison of cost for TIO/OLO and FF/UMEC/VI; **p-value <0.001 for comparison of cost for TIO/OLO and FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; TIO/OLO, tiotropium/olodaterol. Annualized population averages are calculated as the ([sum of all costs for all individuals during the follow-up period]/[sum of follow-up on-treatment time in in years (365 days) for all individuals]). Wald 95% confidence limits for this ratio used the Taylor expansion to estimate standard error. Patient and insurer paid amounts are combined. Identified during the follow-up period. The index date is included in the baseline period except for the index pharmacy claims, which are included in the follow-up period. Costs are adjusted using the most recent year of the medical care component of the Consumer Price Index (CPI) to reflect inflation to 2020. Retrieved from US Department of Labor, Bureau of Labor Statistics. Consumer Price Index. Medical Care. Series ID: CUUR0000SAM. Washington, DC; U.S> Dept. of Labor, Bureau of Labor Statistics, 2012. http://data.bls.gov/cgi-bin/surveymost?su. Open Access.12 |
No Exacerbation
Population annualized COPD and/or pneumonia-related total costs were significantly lower among TIO/OLO initiators ($11,116) compared with FF/UMEC/VI initiators ($13,640), p<0.001, including significantly lower pharmacy costs ($4605 vs $6451; p<0.001). All-cause healthcare cost measures were similar between the TIO/OLO and FF/UMEC/VI cohorts, but the population annualized pharmacy costs were significantly lower for TIO/OLO ($9582 vs $11,409; p=0.002). Adjusted COPD and/or pneumonia-related total ($11,179 vs $13,567; p<0.001) and pharmacy ($4631 vs $6411; p<0.001) healthcare costs were significantly lower among TIO/OLO initiators versus FF/UMEC/VI (Table 3); adjusted COPD and/or pneumonia-related medical costs did not statistically differ between cohorts.
GOLD C/D
The only statistically significant difference in COPD and/or pneumonia-related costs was the population annualized pharmacy spending (TIO/OLO: $5027, vs FF/UMEC/VI: $6754; p<0.001). Adjusted COPD and/or pneumonia-related total or medical healthcare costs were similar for TIO/OLO and FF/UMEC/VI initiators (Table 3). Adjusted COPD and/or pneumonia-related pharmacy costs were significantly lower for TIO/OLO ($5001) versus FF/UMEC/VI ($6788) initiators, p<0.001. There was no difference in all-cause healthcare costs between cohorts.
Discussion
In this study, a sizeable proportion of patients initiated treatment on TT contrary to guideline recommendations. While TT provided no clinical benefit such as reduced exacerbations in the GOLD A/B and No exacerbation subgroups, its use resulted in greater HCRU and costs. Results in the GOLD C/D subgroup were consistent with the IMPACT and ETHOS RCTs, which indicated that TT may reduce the risk of exacerbation relative to dual (LAMA/LABA or LABA/ICS) therapy in patients at high exacerbation risk (GOLD C/D).13–15 As in the RCTs, the more severe, GOLD C/D, patients in our study who initiated on TT had better exacerbation outcomes.
While the current study cannot accurately classify the patients in the GOLD subgroups, as claims data lack spirometric severity and other clinical characteristics, it is plausible that our GOLD C/D patients were similar to RCT patients, given their exacerbation history, higher COPD severity scores, and comorbidity burden. This is a possible explanation for the similar exacerbation risks observed between cohorts in our GOLD C/D subgroup and in the RCTs, further validating our findings.
Adjusted COPD and/or pneumonia-related total healthcare costs also were significantly lower for TIO/OLO initiators (vs FF/UMEC/VI) in the GOLD A/B and No exacerbation subgroups, driven by significantly lower pharmacy spending in this study. There was no statistically significant difference between the treatment cohorts in medical spending in the GOLD A/B and No exacerbation subgroups. The pattern in the GOLD C/D subgroup, however, was different. The adjusted COPD and/or pneumonia-related total and medical healthcare costs were similar for TIO/OLO and FF/UMEC/VI initiators, despite the significantly lower adjusted pharmacy costs for TIO/OLO. Our study’s focus on FDC TT expands upon the findings of Palli et al, which reported average annualized health-plan savings of $8586 for COPD and/or pneumonia-related costs, when enrollees were treated with TIO/OLO versus mostly free-dose TT.6 Consistent with the Palli et al study, our results suggest that adherence to treatment guidelines could result in considerable cost savings.
This study’s detailed HCRU and cost findings based on a contemporary COPD population treated with a LAMA/LABA and FDC TT, and stratified by exacerbation risk spectrum, could help to guide future treatment decisions.
Limitations
These results are subject to inherent susceptibilities of administrative claims data repurposed for research, including miscoding and omissions, among others. A claim for a filled prescription does not necessarily mean the medication was used as prescribed or at all, and medicines acquired over the counter or as physicians’ samples are not captured in claims data. Moreover, it is not possible to identify the reasons for treatment initiation of the index therapy. Also, largely absent is information on lifestyle behaviors and relevant clinical characteristics such as lung function, smoking status, and symptom burden, among others, that could affect disease progression and study outcomes. Inherent biases from non-randomized patient and treatment selections that are present in observational studies were mitigated with PSM that adequately balanced many baseline characteristics between cohorts and further, post-match residual imbalances between cohorts were addressed with MVA techniques. The on-treatment study design precluded the capture of outcomes occurring right after censoring, including any potentially associated with the index medication. In addition, exacerbations were identified via a claims algorithm. These results may not be generalizable to patients with noncommercial or non-MAPD health insurance.
Conclusions
Initiating maintenance treatment with TIO/OLO rather than FF/UMEC/VI may represent a more cost-effective treatment decision, especially in GOLD A/B and No exacerbation subgroups. Exacerbation risk did not differ between the treatment cohorts in these two subgroups, and the incidence of pneumonia was lower in the No exacerbation subgroup for TIO/OLO versus FF/UMEC/VI. These clinical and economic findings support ATS and GOLD recommendations for treating COPD patients with low exacerbation risk with a LAMA/LABA and those at higher risk with TT.
Ethics Statement
Institutional review board approval or waiver was not sought nor required for this study because no identifiable protected health information was accessed in the conduct of this study in accordance with the United States Department of Health and Human Services Privacy Rule requirements for de-identification codified at 45 C.F.R. § 164.514 (b). Patient privacy was preserved, and Health Insurance Portability and Accountability Act (HIPAA) data handling rules and were complied with throughout. Hence, no relevant institutional name or other detail is applicable.
Acknowledgments
The authors wish to thank Bernard Tulsi, Sarah Hague and Noah Webb, all of Optum, for writing and editorial support, project management, and preparation of graphic elements, respectively, and Felix Cao, Yiyu Fang, Michael Johnson, and Havisha Taneja, all of Optum, for dataset programming support. Relevant reviewers from Boehringer Ingelheim Pharmaceuticals, Inc. assessed the contents of the manuscript for medical and scientific accuracy, and for intellectual property considerations. A selection of the study’s results have been presented as a poster at the American Thoracic Society International Conference, May 13–18, 2022 with interim findings. The poster’s abstract was published in “Poster Abstracts” in ATS Journal: Hyperlink: https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2022.205.1_MeetingAbstracts.A5018
Funding
Funding for this study was provided by Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA.
Disclosure
Clark and Shaikh are employees of Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). Palli was employed by BIPI at the time of study. Buysman and Sargent are employees of Optum, which was contracted by BIPI to conduct this study. Bengtson was employed by Optum at the time of study. Sethi of Jacobs School of Medicine and Biomedical Sciences at University at Buffalo and Ferguson of the Department of Medicine, Pulmonary Research Institute of Southeast Michigan are subject matter clinical experts contracted by BIPI for this study. Sethi declares that he has received honoraria/fees for consulting/speaking from AstraZeneca, BIPI, Chiesi, GlaxoSmithKline, Merck and Uptodate. He has received consulting fees for serving on Data safety monitoring boards from Nuvaira, Inc. and Pulmotect, Inc. He has received consulting fees from Apellis Pharmaceuticals and Aerogen Pharma. His institution has received research funds for his participation in Clinical Trials from Regeneron Pharma, Sanofi, Theravance and AstraZeneca. Ferguson reports consulting fees from BIPI, AstraZeneca, DevPro, Syneos Health, GlaxoSmithKline, Teva, Orpheris and Verona Pharma, speaker fees from GlaxoSmithKline and Theravance and is in receipt of research grants from AstraZeneca, Chiesi Novartis International AG, Teva, Galderma, Syneos, PPD, Orpheris, Verona Pharma and GlaxoSmithKline. The authors report no other conflicts of interest in this work.
References
1. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201:e56–e69.
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2022. Available from: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf.
3. Safka KA, Wald J, Wang H, McIvor L, McIvor A. GOLD stage and treatment in COPD: a 500 patient point prevalence study. Chronic Obstr Pulm Dis. 2016;4:45–55. doi:10.15326/jcopdf.4.1.2016.0126
4. Simeone JC, Luthra R, Kaila S, et al. Initiation of triple therapy maintenance treatment among patients with COPD in the US. Int J Chron Obstruct Pulmon Dis. 2017;12:73–83. doi:10.2147/COPD.S122013
5. Li Y, Lim J, Stemkowski S, Kaila S, Renda A, Shaikh A. Initiation of triple therapy maintenance treatment among patients with COPD. Am J Manag Care. 2020;26:e106–e112.
6. Palli SR, Frazer M, DuCharme M, Buikema AR, Anderson AJ, Franchino-Elder J. Differences in Real-world health and economic outcomes among patients with COPD treated with combination tiotropium/olodaterol versus triple therapy. J Manag Care Spec Pharm. 2020;26:1363–1374. doi:10.18553/jmcp.2020.20159
7. Palli SR, Zhou S, Shaikh A, Willey VJ. Effect of compliance with GOLD treatment recommendations on COPD health care resource utilization, cost, and exacerbations among patients with COPD on maintenance therapy. J Manag Care Spec Pharm. 2021;27:625–637. doi:10.18553/jmcp.2021.20390
8. Palli SR, Buikema AR, DuCharme M, Frazer M, Kaila S, Juday T. Costs, exacerbations and pneumonia after initiating combination tiotropium olodaterol versus triple therapy for chronic obstructive pulmonary disease. J Comp Eff Res. 2019;8:1299–1316. doi:10.2217/cer-2019-0101
9. Buhl R, Criee CP, Kardos P, et al. Dual bronchodilation vs triple therapy in the “real-life” COPD DACCORD study. Int J Chron Obstruct Pulmon Dis. 2018;13:2557–2568. doi:10.2147/COPD.S169958
10. Boehringer Ingelheim Pharmaceuticals, Inc. STIOLTO RESPIMAT (tiotropium bromide and olodaterol) inhalation spray for oral inhalation use [prescribing information]. CT, USA: Boehringer Ingelheim Pharmaceuticals, Inc.; 2018. Available from: https://docs.boehringer-ingelheim.com/Prescribing%20Information/PIs/Stiolto%20Respimat/stiolto.pdf.
11. TRELEGY ELLIPTA (fluticasone furoate, umeclidinium, and vilanterol inhalation powder) GlaxoSmithKline, NC 27709. Research Triangle Park; 2022. Available from: https://gskpro.com/content/dam/global/hcpportal/en_US/Prescribing_Information/Trelegy_Ellipta/pdf/TRELEGY-ELLIPTA-PI-PIL-IFU.PDF.
12. U.S. Department of Labor, Bureau of Labor Statistics. Consumer price index. medical care. Series ID: CUUR0000SAM. Washington, DC: U.S. Dept. of Labor, Bureau of Labor Statistics; 2022. Available from: http://data.bls.gov/cgi-bin/surveymost?cu.
13. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378:1671–1680. doi:10.1056/NEJMoa1713901
14. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201:1508–1516. doi:10.1164/rccm.201911-2207OC
15. Martinez FJ, Rabe KF, Ferguson GT, et al. Benefits of budesonide/glycopyrrolate/formoterol fumarate (BGF) on symptoms and quality of life in patients with COPD in the ETHOS trial. Respir Med. 2021;185:106509. doi:10.1016/j.rmed.2021.106509
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Healthcare Utilization and Clinical Outcomes of Patients with Chronic Obstructive Pulmonary Disease Initiating Single-Inhaler Long-Acting β2-Agonist/Long-Acting Muscarinic Antagonist Dual Therapy in Primary Care in England
Requena G, Banks V, Czira A, Wood R, Tritton T, Wild R, Compton C, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:231-245
Published Date: 5 March 2023
Benzodiazepine Usage, Healthcare Resource Utilization, and Costs Among Older Adults Treated with Common Insomnia Medications: A Retrospective Cohort Study
Wickwire EM, Juday TR, Gor D, Amari DT, Frech FH
ClinicoEconomics and Outcomes Research 2023, 15:413-424
Published Date: 2 June 2023
Clinical and Economic Burden of Managing Patients with Sickle Cell Disease Receiving Frequent Red Blood Cell Transfusions in the United States
Udeze C, Jerry M, Evans KA, Li N, Jain S, Andemariam B
ClinicoEconomics and Outcomes Research 2025, 17:303-313
Published Date: 11 April 2025
Characteristics and Outcomes of People With COPD Who Experience Exacerbations While on Inhaled Triple Therapy: Results of the SIRIUS I Cohort Study in the US (2015–2019)
Nordon C, Carstens D, Fagerås M, Müllerová H, Veeranki PS, Alves JA, Germack HD, Barnes TL, McCormack MC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1851-1864
Published Date: 11 June 2025
A Systematic Literature Review of the Humanistic, Economic, Sociodemographic, and Environmental Burden Associated with Severe COPD
Vlachaki I, Donhauser S, Wise RA, Chen Y, Madoni A, Scaffidi Argentina U, Mir JN, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2493-2523
Published Date: 17 July 2025