Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Impact of Multidisciplinary Continuity of Care on Postoperative Outcomes in Liver Cancer Surgical Patients
Authors Yuan Y ![]()
Received 10 March 2025
Accepted for publication 24 July 2025
Published 6 August 2025 Volume 2025:18 Pages 4749—4759
DOI https://doi.org/10.2147/JMDH.S527399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Yuxun Yuan
Outpatient Department of Multidisciplinary Consultation, Xingtai People’s Hospital, Xingtai, Hebei Province, 054001, People’s Republic of China
Correspondence: Yuxun Yuan, Email [email protected]
Objective: To evaluate the impact of Multidisciplinary Continuity of Care (MCC) on postoperative outcomes for liver cancer surgical patients compared to routine continuity care.
Methods: A retrospective cohort study was conducted involving 103 liver cancer patients who underwent surgical treatment between January 2021 and January 2023. Patients were assigned to groups based on the standard care protocol in effect at the time of their admission: the control group (n=50), admitted before July 2022, received conventional continuity care, while the observation group (n=53), admitted from July 2022 onward, received multidisciplinary continuity care. This temporal allocation strategy reduced selection bias by linking group assignment to hospital-wide protocol updates rather than patient-specific factors. Key outcomes assessed included physiological recovery (measured by the Chang-Hai Pain Scale and ECOG performance status), psychological status (SDS and SAS), self-management ability (ESCA), quality of life (QOL-LC), and postoperative complication rates.
Results: Post-intervention outcomes significantly favored the observation group. Patients demonstrated lower Chang-Hai Pain scores (P< 0.05), improved ECOG performance status (P< 0.05), reduced SDS and SAS scores (P< 0.05), and higher ESCA self-management scores across all dimensions (P< 0.05) compared to controls. The observation group also showed superior QOL-LC scores in all domains (psychological, physical, social, and symptom management; P< 0.05) and significantly lower complication rates (9.43% vs 26.00%, P< 0.05). No significant between-group differences existed pre-intervention for any measure (P> 0.05).
Conclusion: Implementing MCC in postoperative care for liver cancer patients significantly enhances self-management ability, reduces anxiety/depression, lowers complication risk, and improves physical function and quality of life compared to routine care. MCC demonstrates high clinical value and warrants promotion.
Keywords: multidisciplinary continuity care, liver cancer, surgery, effectiveness study
Introduction
Liver cancer is a frequently occurring malignant tumor worldwide, with both its incidence and mortality consistently on the rise.1 According to the World Health Organization (WHO), hundreds of thousands of people die from liver cancer annually, posing a significant threat to global health.2 Currently, clinical treatments for liver cancer encompass various approaches such as surgical resection, interventional therapy, radiotherapy, and chemotherapy, among which surgical treatment is considered a feasible and effective therapeutic modality.3 Although surgical treatment for liver cancer effectively removes tumor tissues, postoperative recovery and care for patients are equally crucial.4 Following surgery, patients with hepatocellular carcinoma (HCC) face unique challenges including complex physiological alterations due to hepatic resection, high metabolic demands for regeneration, vulnerability to complications such as liver failure or infection, and significant psychological distress related to the underlying chronic liver disease and cancer diagnosis.5 These HCC-specific factors create a complex recovery trajectory demanding integrated care beyond physical wound management. Traditionally, postoperative care for patients heavily relies on conventional continuity care models, focusing predominantly on the physical aspects of disease treatment, often neglecting these holistic and HCC-specific needs.
In recent years, multidisciplinary continuity care (MCC) models have garnered considerable attention within the medical community. This model transcends the limitations of traditional single medical specialty approaches by integrating healthcare professionals from diverse backgrounds, collectively providing patients with more comprehensive and personalized care services.6 Its essence lies in consolidating medical resources to offer systematic and all-encompassing care plans, including but not limited to medical, rehabilitative, nutritional, and psychological aspects, aimed at promoting both physical and psychological recovery of patients.7 To date, the multidisciplinary continuity care model has been applied in the treatment of various clinical conditions, yielding certain achievements.8,9 However, robust research specifically evaluating the impact of MCC on postoperative outcomes for HCC patients remains scarce.10 Given the intricate interplay of surgical stress, underlying liver dysfunction, nutritional vulnerability, and psychological burden characteristic of HCC recovery, MCC holds particular promise for optimizing outcomes in this population.
Therefore, this study aims to retrospectively analyze clinical data from liver cancer patients admitted to our hospital, comparing the effects of conventional continuity care models versus multidisciplinary continuity care models specifically for postoperative HCC management. Through this investigation, we hope to provide more effective and comprehensive intervention strategies for postoperative care in HCC patients, aiding in enhancing patients’ self-recovery abilities, improving their quality of life, and reducing the occurrence of complications. Additionally, we aspire to offer theoretical support for practical applications in the field of medical care, promoting the application and development of multidisciplinary continuity care models in postoperative care for HCC.
Objects and Methods
Study Design and Subjects
A retrospective cohort study was conducted on 103 liver cancer patients undergoing surgical treatment at our hospital (January 2021–January 2023). Patients were assigned to groups based on the standard care protocol active during their admission: Those admitted before July 2022 received conventional continuity care (Control Group, n=50), while those admitted from July 2022 onward received multidisciplinary continuity care (Observation Group, n=53). This temporal assignment minimized selection bias as group allocation was determined by hospital-wide protocol changes rather than individual patient characteristics.
Inclusion criteria: ① Patients diagnosed with liver cancer through clinical examinations and received curative surgical treatment in our hospital; ② Patients aged between 18 and 75 years, regardless of gender; ③ Patients and their families willing to cooperate with the required follow-up investigations for the study; ④ Patients with stable postoperative conditions, clear self-awareness, and the ability for self-directed action; ⑤ Patients with complete and authentic clinical data available for analysis.
Exclusion criteria: ① Excluding those with metastatic liver cancer or extensive intra-abdominal tumor metastasis; ② Excluding individuals with severe dysfunction in vital organs; ② Excluding cases with abnormalities in the immune system, coagulation function, or other major systems; ③ Excluding patients with concurrent other tumors; ④ Excluding individuals with cognitive impairment, consciousness disorders, etc.; ⑤ Excluding individuals with allergic reactions or relevant contraindications to the surgical, anesthesia, or nursing interventions applied in this study.
Interventions
Control Group
During the study period (January 2021–June 2022), all patients received standard postoperative care according to the hospital protocol. This care included pre-discharge instructions, which consisted of brief verbal and written guidance on medications, diet, and activity restrictions, typically lasting 5 to 10 minutes. Following discharge, patients were followed up with one structured telephone call (lasting approximately 15 minutes) within 1 to 4 weeks. Additionally, patients had monthly outpatient visits for clinical assessments during the first 6 months post-surgery. In the months 2 through 6, patients received bi-monthly phone calls (lasting less than 10 minutes) for symptom checks.
Observation Group
Patients in the observation group received interventions based on multidisciplinary continuity care mode. The specific measures were as follows:
- Establishment of a Multidisciplinary Continuity Care Team: To improve the post-discharge quality of life for liver cancer patients and meet their disease guidance needs, our hospital established a multidisciplinary continuity care team for liver cancer. The team consisted of 14 members, led by the department head (chief physician) as the team leader and the head nurse as the deputy team leader (chief nurse). The team included 3 doctors (1 associate chief physician, 2 attending physicians), 1 nutritionist, 1 psychologist, 1 nursing graduate student (part of the research team), and 6 nurses (classified according to the hospital’s nursing hierarchy: 1 N4 level nurse, 1 N3 level nurse, 2 N2 level nurses, and 2 N1 level nurses). The team leader and deputy leader assigned roles and specific job responsibilities based on the professional technical capabilities and expertise of the team members. Before implementation, all team members underwent training in relevant continuity care knowledge. The researcher and N3 level nurse were primarily responsible for evaluating research indicators of liver cancer patients one day before discharge (pre-care) and three months after discharge (post-care). Two N2 level nurses were primarily responsible for collecting, organizing, and archiving the discharged patients’ data to ensure its integrity and continuity. The team members collaborated on their designated tasks, earnestly fulfilling their responsibilities. The team leader, deputy leader, and one N4 level nurse were primarily responsible for quality control, ensuring the smooth implementation of the multidisciplinary continuity care model for liver cancer.
- Formulation of the Multidisciplinary Collaboration Model Continuity Care Plan: The care plan was mainly divided into two phases. ① Phase 1: Implemented by the researcher and dedicated nurse one day before patient discharge. Firstly, a comprehensive assessment of the patient’s social environment, psychological state, physiological status, and health behavior was conducted, along with the collection of basic patient information and the completion of various evaluation scales in the observation indicators. Subsequently, patient needs were clarified through face-to-face discussions with the patient and their family. Tailored health education and guidance were provided, and an individualized outpatient continuity care plan was developed, focusing on various aspects such as dietary health, medication guidance, pain control management, psychological health, rehabilitation exercises, follow-up schedules, and observation and handling of potential postoperative complications. Two copies of this plan were generated, one held by the continuity care team and the other by the patient, and consolidated into an electronic document to establish a comprehensive personal patient file. ② Phase 2: Post-discharge patient follow-ups were conducted by members of the multidisciplinary continuity care team. Telephone follow-ups were done once at 3 days post-discharge, weekly for the first month, and biweekly for the second and third months. A home visit was scheduled at 1 month post-discharge to assess the patient’s recovery and develop appropriate solutions for any existing issues. Another home visit was conducted at 3 months post-discharge, focusing on reassessing previously identified problems and conducting evaluations using various assessment scales from the observation indicators.
- Implementation of Outpatient Multidisciplinary Continuity Care: ① Establishment of a WeChat communication group for post-discharge continuity care services composed of multidisciplinary members, with the head nurse as the administrator. Patients or their families were guided to join the group by scanning the QR code one day before discharge. Multidisciplinary members shared links related to liver cancer recovery and self-care in this group to provide patients with relevant health knowledge. They also responded to inquiries related to daily treatment, care, diet, and psychological concerns between 6:00 PM to 8:00 PM daily, offering professional guidance. Patients were encouraged to enhance interaction within the group, share self-care experiences, cultivate a positive and optimistic mindset, and mutually encourage each other to increase confidence in anti-tumor treatment. ② Telephone Follow-ups: Follow-up calls were conducted according to the time and content outlined in the multidisciplinary collaboration model continuity care plan, and patient discharge follow-up records were completed. ③ Home Visits: Two home visits were conducted according to the care plan, and liver cancer patient follow-up records were completed. Initially, a comprehensive assessment of the patient’s physical condition was performed, including self-care ability, daily tolerable activity levels, pain severity and duration, anxiety levels, and dietary structure. Subsequently, assessments were made regarding the presence of complications, the patient’s health behaviors (compliance with medication, adopting healthy lifestyle habits, alcohol consumption, etc), and finally, evaluations of the patient’s psychological and social factors, including family relationships, attitudes towards treatment, adaptation to the social environment, and active engagement in social activities. Careful analysis was conducted to provide scientific, reasonable guidance, and education for any potential health issues. ④ Regular Health Education Symposiums: Each month, the department organized a health education seminar held within the hospital, inviting renowned experts to host lectures and interactive sessions. Liver cancer patients and their families were encouraged to participate, allowing patients to express their inner feelings and experience society’s attention and support. This interaction played a positive role in the patients’ disease recovery.
Observation Indicators
Level of Physical Recovery Indicators
Longhai Pain Scale11 was used to assess patients’ pain conditions one day before discharge (pre-care) and three months after discharge (post-care). This scale combines the Numeric Rating Scale (NRS) and the Verbal Rating Scale (VRS), incorporating the advantages of both scales. Scores range from 0 to 10, with higher scores indicating more severe pain. The Eastern Cooperative Oncology Group performance status (ECOG)12 was used to evaluate patients’ daily activity levels. This scale scores from 0 to 5, where 0 indicates normal and 5 indicates death. Higher scores indicate lower physical functional levels.
Psychological and Emotional State Indicators13
The Self-Rating Depression Scale (SDS) was used to evaluate patients’ depression levels, with a total score of 100 and a cutoff value of 53. The Self-Rating Anxiety Scale (SAS) was used to assess patients’ anxiety levels, with a total score of 100 and a cutoff value of 50. Lower scores indicate lower levels of depression or anxiety.
Level of Self-Management Ability
The Self-Care Ability Scale (ESCA)14 was employed to assess patients’ self-care abilities, encompassing four dimensions: self-care skills, self-care responsibility, self-concept, and health knowledge, with a total of 43 items. Each item is scored on a 1–4 scale, where higher scores indicate stronger self-care abilities.
Level of Quality of Life
The Quality of Life in Patients with Liver Cancer Scale (QOL-LC)15 was used to evaluate patients’ quality of life, consisting of four dimensions: psychological function (maximum score of 60), physical function (maximum score of 60), social function (maximum score of 50), and symptoms/adverse effects (maximum score of 50). Higher scores indicate a better quality of life.
Occurrence of Complications During Follow-Up
Complications observed in this study included abdominal distension or pain, jaundice, anemia, nausea, vomiting, and liver function biochemical changes. The occurrence of these complications was uniformly recorded by relevant medical staff at our hospital.
Statistical Analysis
Data were analyzed using SPSS 22.0 and GraphPad Prism 8. Normality was confirmed via Shapiro–Wilk tests (P>0.05 for all continuous variables); homogeneity of variance was verified using Levene’s test. Continuous data were expressed as mean ± SD and compared using independent samples t-tests (between groups) and paired t-tests (within groups). Categorical data were presented as frequencies (%) and analyzed by χ2 test or Fisher’s exact test for sparse cells (expected count <5). A priori sample size calculation using G*Power 3.1 (Faul et al, 2007) indicated that 52 patients (26 per group) would provide 80% power (α=0.05, two-tailed t-test) to detect large effect sizes (d=0.8) in primary outcomes (eg, pain, QOL). Our final sample size (N=103) exceeded this requirement, ensuring adequate statistical power. Significance was set at P<0.05.
Results
Comparison of Baseline Data
The baseline characteristics of both groups were comparable, with no significant differences (P > 0.05), confirming homogeneity prior to intervention (Table 1).
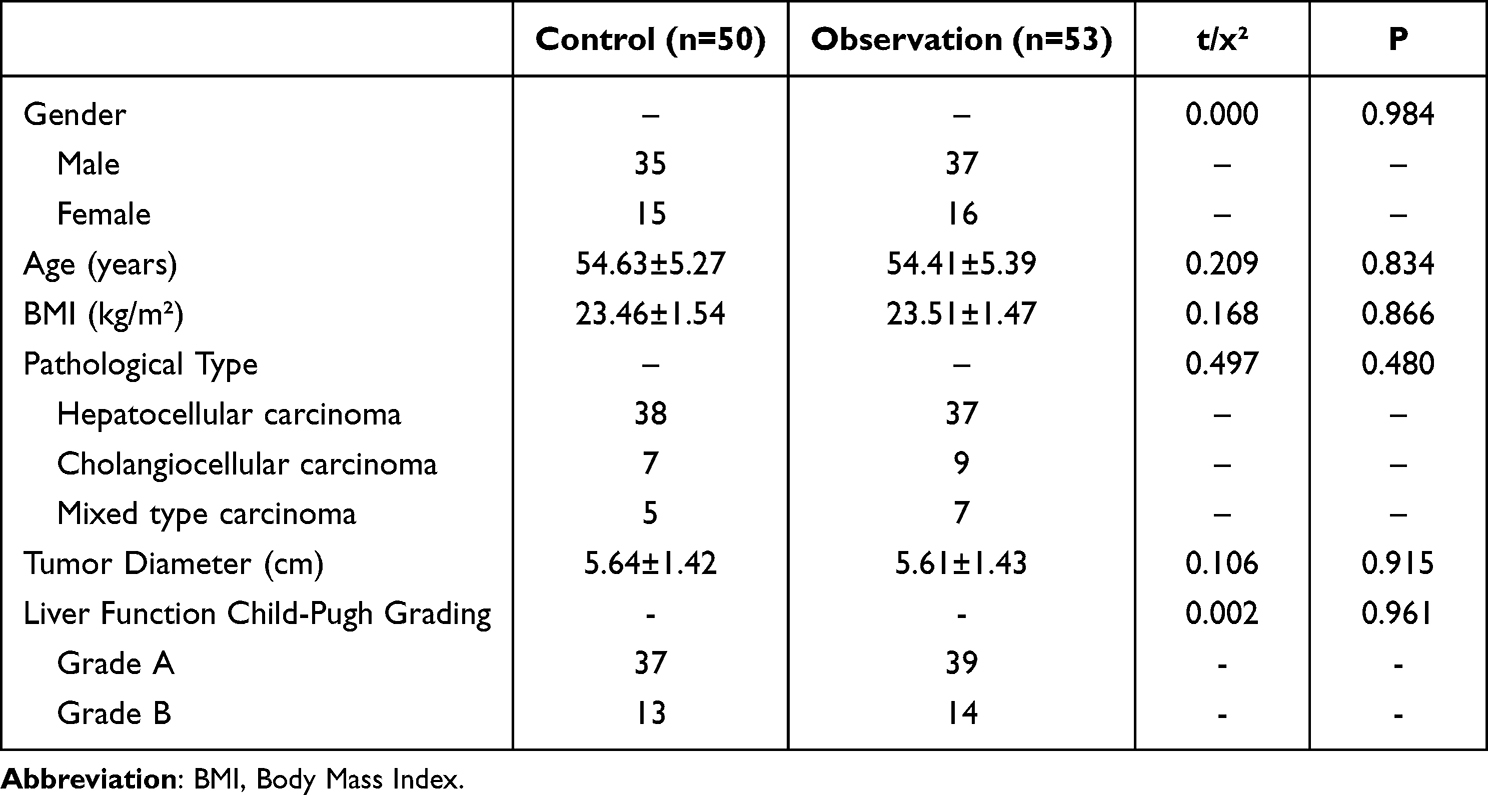 |
Table 1 Comparison of Baseline Data |
Comparison of Physiological Recovery Indicators
As shown in Figure 1, the observation group demonstrated significantly greater improvements in pain and functional status compared to the control group. Pain scores (PRS) were lower in the observation group (3.45 ± 1.76) than in the control group (4.81 ± 1.63), with a mean difference of −1.36 (95% CI: −1.96 ~ −0.76, p < 0.001, Cohen’s d = 0.81). Functional status (ECOG) also improved more markedly in the observation group (1.41 ± 0.31) compared to the control (1.75 ± 0.26), with a mean difference of −0.34 (95% CI: −0.44 ~ −0.24, p < 0.001, d = 1.19). No significant differences were observed between groups at baseline (p > 0.05).
 |
Figure 1 Comparison of Physiological Recovery Indicator Levels. Abbreviation: ECOG, Eastern Cooperative Oncology Group. Note: Data are presented as mean ± SD. *P < 0.05 vs control group. |
Comparison of Psychological State Indicators
As shown in Figure 2, MCC significantly reduced anxiety and depression levels compared to the control group. Depression scores (SDS) were lower in the observation group (35.56 ± 5.71) than in the control group (44.82 ± 5.39), with a mean difference of −9.26 (95% CI: −11.42 ~ −7.10, p < 0.001, d = 1.67). Similarly, anxiety scores (SAS) were lower in the observation group (32.39 ± 4.34) than in the control group (41.23 ± 3.37), with a mean difference of −8.84 (95% CI: −10.23 ~ −7.45, p < 0.001, d = 2.27). Pre-intervention scores were comparable between groups (p > 0.05).
 |
Figure 2 Comparison of Psychological State Indicator Levels. Abbreviations: SDS, Self-Rating Depression Scale; SAS, Self-Rating Anxiety Scale. Note: Data are presented as mean ± SD. *P < 0.05 vs control group. |
Comparison of Self-Management Capability Levels
As shown in Figure 3, the observation group demonstrated significantly higher self-management capability across all dimensions compared to the control group after the intervention. Self-care skills were higher in the observation group (38.84 ± 4.27) than in the control group (29.49 ± 4.96), with a mean difference of 9.35 (95% CI: 7.35 ~ 11.35, p < 0.001, d = 2.02). Self-care responsibility was higher in the observation group (20.47 ± 2.38) than in the control group (17.63 ± 2.04), with a mean difference of 2.84 (95% CI: 1.97 ~ 3.71, p < 0.001, d = 1.28). Self-concept was higher in the observation group (25.56 ± 1.78) than in the control group (21.63 ± 2.97), with a mean difference of 3.93 (95% CI: 2.97 ~ 4.89, p < 0.001, d = 1.78). Health knowledge was higher in the observation group (70.13 ± 1.94) than in the control group (55.56 ± 3.91), with a mean difference of 14.57 (95% CI: 13.27 ~ 15.87, p < 0.001, d = 4.18). Pre-intervention scores showed no significant differences for any dimension (all p > 0.05).
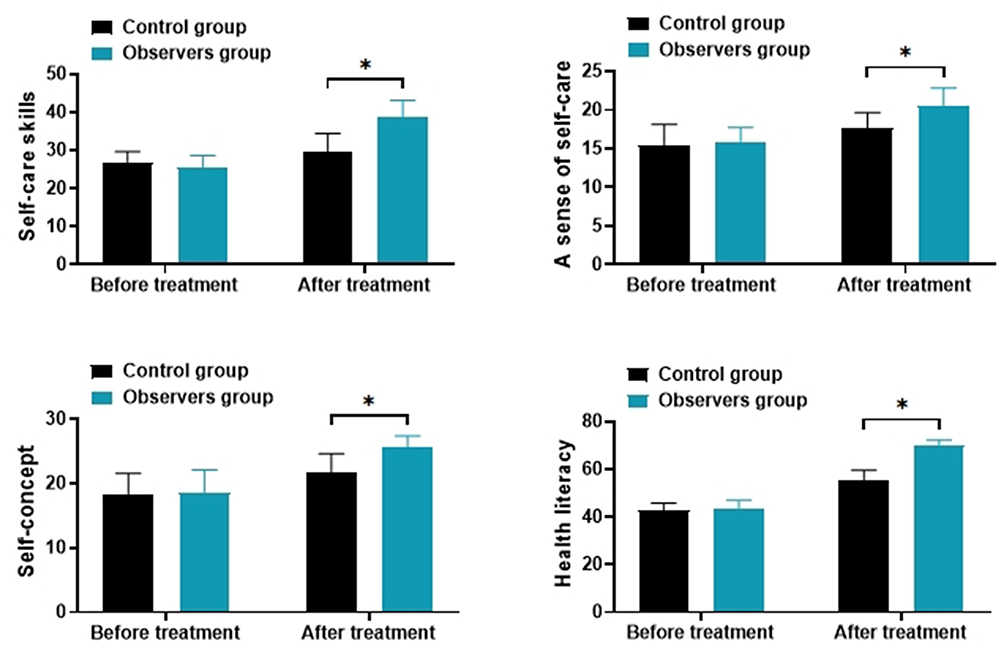 |
Figure 3 Comparison of Self-Management Capability Levels. Note: Data are presented as mean ± SD. *P < 0.05 vs control group. |
Comparison of Quality of Life Levels
As illustrated in Figure 4, the observation group showed significantly improved quality of life across all domains compared to the control group after the intervention. Psychological function was higher in the observation group (42.21 ± 5.83) than in the control group (36.54 ± 4.47), with a mean difference of 5.67 (95% CI: 3.48 ~ 7.86, p < 0.001, d = 1.09). Physical function was higher in the observation group (49.41 ± 5.39) than in the control group (45.86 ± 4.67), with a mean difference of 3.55 (95% CI: 1.49 ~ 5.61, p = 0.001, d = 0.70). Social function was higher in the observation group (31.49 ± 3.34) than in the control group (27.83 ± 4.09), with a mean difference of 3.66 (95% CI: 2.13 ~ 5.19, p < 0.001, d = 0.98). Symptoms/adverse effects management was higher in the observation group (43.77 ± 4.12) than in the control group (40.61 ± 3.95), with a mean difference of 3.16 (95% CI: 1.56 ~ 4.76, p < 0.001, d = 0.78). Pre-intervention scores showed no significant differences for any domain (all p > 0.05).
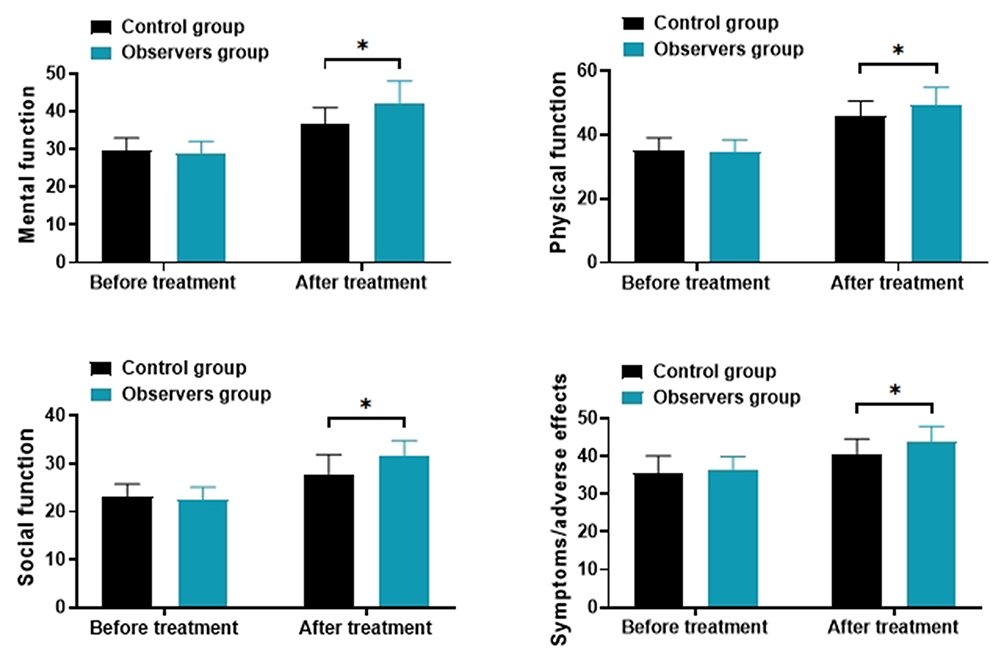 |
Figure 4 Comparison of Quality of Life Levels. Note: Data are presented as mean ± SD. *P < 0.05 vs control group. |
Comparison of Complications During Follow-up Period
As detailed in Table 2, the total incidence of complications was significantly lower in the observation group (9.43%, 5/53) compared to the control group (26.00%, 13/50), with p = 0.026 by χ²-test.
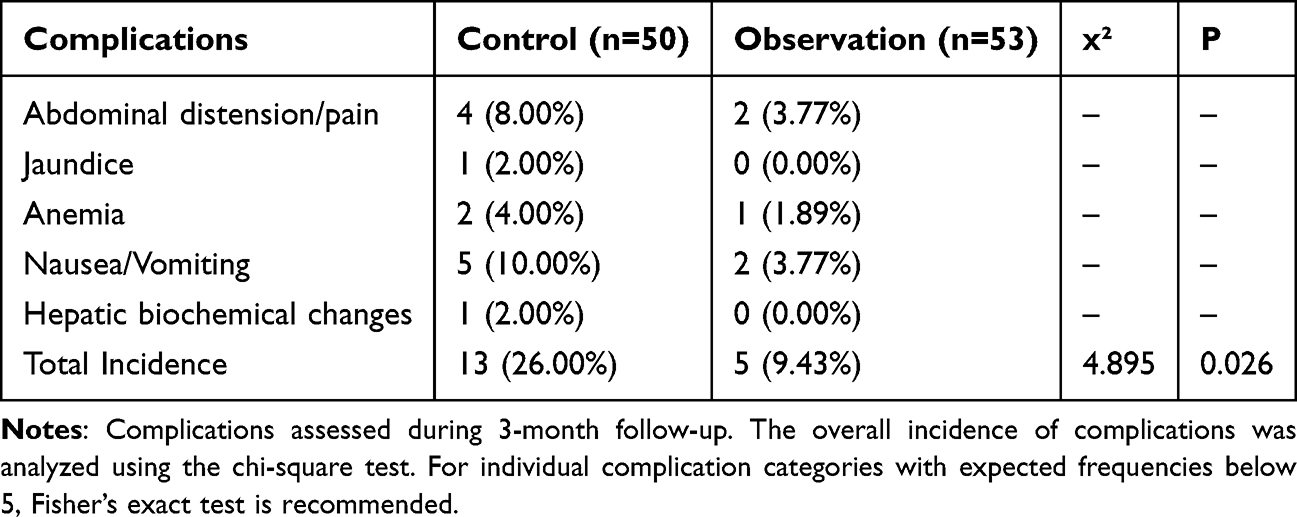 |
Table 2 Comparison of Complications During Follow-up Period |
Discussion
Liver cancer is a commonly occurring malignant tumor in clinical practice, with a relatively high risk of mortality. Research16 has demonstrated that actively pursuing effective treatment during the early stages of liver cancer significantly prolongs patient survival. Surgery is a common treatment choice for liver cancer patients. However, improper postoperative care can lead to various issues, subsequently affecting patient recovery and overall health. Hence, the selection of a scientific, rational, and effective nursing model is crucial for the recovery of the patient’s body.17 Continuity of care is an extension of inpatient nursing services, extending nursing services to various treatments, care, and rehabilitation exercises after the patient’s discharge. This approach assists patients in improving their self-care abilities, harnessing their subjective initiative, and actively participating in the process, thereby enhancing their quality of life. Previously, cancer patients typically received routine continued care after discharge. However, research18 found that routine continued care usually involved discharge guidance from nursing staff and follow-up calls after discharge, which was relatively monotonous. Moreover, due to limitations in the patient and family’s ability to grasp health education content, most patients and their families could not fully understand the related health education, leading to poor compliance. In recent years, with the increasing specialization of medical services and the interdisciplinary nature of healthcare, interdisciplinary continued care service teams composed of professional physicians, nurses, nutritionists, and psychologists have fully utilized the professional advantages of interdisciplinary teams, significantly enhancing patient trust and treatment compliance.19
Impact of Multidisciplinary Collaborative Continued Care on Liver Cancer Patients’ Quality of Life
The aggressive nature and recurrence risk of liver cancer profoundly impact quality of life.20 Our MCC intervention—featuring personalized plans, continuous home support, and professional guidance—significantly improved QOL-LC scores across all domains (psychological, physical, social, symptom management; P<0.05). This aligns with Yang et al’s21 HCC study, where MCC reduced symptom burden through behavioral modification. Importantly, our model specifically addresses unmet needs identified in liver cancer qualitative studies:22 fragmented post-discharge support, inadequate pain management, and psychosocial neglect. By integrating WeChat consults, home visits, and tailored rehabilitation, we provide a replicable blueprint for bridging these gaps.
Impact of Multidisciplinary Collaborative Continued Care on Self-Care Abilities of Liver Cancer Patients
Our results demonstrate MCC’s superiority in enhancing self-management (ESCA scores: d=1.28–4.18, P<0.05), corroborating Wang et al’s findings.23 The 24/7 accessibility via multidisciplinary WeChat groups was pivotal, enabling real-time adjustments to care plans—a feature absent in conventional models. This directly responds to liver cancer patients’ expressed needs for ongoing expert support during recovery transitions.24 The collaborative synergy among team members amplified intervention efficacy, transforming passive recipients into active participants in their care.
Multidisciplinary Collaborative Continued Care Reduces Patient-Related Complications and Promotes Physical and Mental Recovery of Patients
Pain and functional impairment critically undermine postoperative adaptation in liver cancer patients.25 In this study, the multidisciplinary collaborative continued care (MCC) model significantly outperformed routine care in alleviating pain (Cohen’s d = 0.81), improving physical performance as measured by ECOG scores (d = 1.19), and reducing psychological distress, with large effects observed for both depression (d = 1.67) and anxiety (d = 2.27). Furthermore, the complication rate in the observation group was markedly lower than in the control group (9.43% vs 26.00%). These improvements were achieved through standardized home-based pain management protocols, psychologist-led interventions for anxiety relief, and tailored rehabilitation programs designed to support physical recovery and social reintegration. In contrast to earlier MCC models in liver cancer that primarily emphasized clinical or medical endpoints,26 our approach takes a comprehensive biopsychosocial perspective, addressing both physiological and psychosocial barriers to recovery.
Limitations and Future Directions
Despite the encouraging findings, several limitations should be acknowledged. First, although the sample size (N = 103) provided adequate power for detecting differences in primary outcomes such as pain and quality of life (post-hoc power >80%), it limited the ability to conduct subgroup analyses or assess infrequent complications like postoperative jaundice. Second, the retrospective design with temporal group assignment, while balanced at baseline, may still harbor residual confounding; unmeasured variables such as socioeconomic status or caregiver support could have influenced the outcomes. Third, the single-center setting at a tertiary hospital may limit generalizability, particularly to resource-constrained environments where replicating a multidisciplinary collaborative care (MCC) model may be challenging due to institutional or staffing limitations. Fourth, the three-month follow-up period was appropriate for capturing nursing-sensitive outcomes but insufficient to assess long-term endpoints such as survival or tumor recurrence. To address these limitations, future research should include prospective multicenter randomized controlled trials with larger samples (eg, >200 participants) to confirm the efficacy of MCC. Additionally, cost-effectiveness analyses are warranted to evaluate the model’s scalability, and longitudinal studies extending beyond 12 months are needed to track survival and recurrence. Finally, implementation science approaches should be employed to adapt and optimize the MCC model across diverse healthcare contexts.
Conclusion
In conclusion, this study provides preliminary evidence that MCC improves postoperative recovery in liver cancer patients by addressing domain-specific needs (self-care, QOL, complications) more effectively than routine care. While methodological constraints necessitate cautious interpretation, our feasibility-tested framework offers a practical implementation pathway. Future research should prioritize prospective validation and long-term outcome assessment.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics and consent statements
This study was approved by the ethics committee of Xingtai People’s Hospital. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The author declares no competing interests in this work.
References
1. Brown ZJ, Tsilimigras DI, Ruff SM, et al. Management of hepatocellular carcinoma: a review. JAMA Surg. 2023;158(4):410–420. doi:10.1001/jamasurg.2022.7989
2. Vogel A, Meyer T, Sapisochin G, et al. Hepatocellular carcinoma. Lancet. 2022;400(10360):1345–1362. doi:10.1016/S0140-6736(22)01200-4
3. Gilles H, Garbutt T, Landrum J. Hepatocellular carcinoma. Crit Care Nurs Clin North Am. 2022;34(3):289–301. doi:10.1016/j.cnc.2022.04.004
4. Ganesan P, Kulik LM. Hepatocellular carcinoma: new developments. Clin Liver Dis. 2023;27(1):85–102. doi:10.1016/j.cld.2022.08.004
5. Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv238–iv255. doi:10.1093/annonc/mdy308
6. Tarrant C, Lewis R, Armstrong N. Polypharmacy and continuity of care: medicines optimisation in the era of multidisciplinary teams. BMJ Qual Saf. 2023;32(3):121–124. doi:10.1136/bmjqs-2022-015082
7. Luis-Martínez R, Monje MHG, Antonini A, et al. Technology-enabled care: integrating multidisciplinary care in parkinson’s disease through digital technology. Front Neurol. 2020;11:575975. doi:10.3389/fneur.2020.575975
8. Barros-Leite B, Andrade LBD. Post-COVID-19 syndrome: a call for continuity of multidisciplinary care. Med Intensiva. 2022;46(8):482–483. doi:10.1016/j.medin.2021.12.001
9. Karasic DH, Fraser L. Multidisciplinary care and the standards of care for transgender and gender nonconforming individuals. Clin Plast Surg. 2018;45(3):295–299. doi:10.1016/j.cps.2018.03.016
10. Tseng YC, Kung P-T, Peng C-Y, et al. Effect of multidisciplinary team care on patient survival in chronic hepatitis B or C hepatocellular carcinoma. Front Oncol. 2023;13:1251571. doi:10.3389/fonc.2023.1251571
11. Zhang CH, Hsu L, Zou B-R, et al. Effects of a pain education program on nurses’ pain knowledge, attitudes and pain assessment practices in China. J Pain Symptom Manage. 2008;36(6):616–627. doi:10.1016/j.jpainsymman.2007.12.020
12. Hernández-Quiles C, Bernabeu-Wittel M, Pérez-Belmonte LM, et al. Concordance of Barthel Index, ECOG-PS, and Palliative Performance Scale in the assessment of functional status in patients with advanced medical diseases. BMJ Support Palliat Care. 2017;7(3):300–307. doi:10.1136/bmjspcare-2015-001073
13. Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry. 2017;17(1):329. doi:10.1186/s12888-017-1489-6
14. Zhang L, Zhang W, Jiang Y, et al. Effects and satisfaction of comfort nursing plus psychological nursing in the clinical nursing of neurology patients: a comparative study. Evid Based Complement Alternat Med. 2022;2022:8013787. doi:10.1155/2022/8013787
15. Zou Y, Yang Q, Guan B, et al. Survey on mental health status and quality of life and correlation among patients with permanent stoma of colorectal tumor. Comput Math Methods Med. 2022;2022:5792312. doi:10.1155/2022/5792312
16. Renne SL, Sarcognato S, Sacchi D, et al. Hepatocellular carcinoma: a clinical and pathological overview. Pathologica. 2021;113(3):203–217. doi:10.32074/1591-951X-295
17. Calderaro J, Seraphin TP, Luedde T, et al. Artificial intelligence for the prevention and clinical management of hepatocellular carcinoma. J Hepatol. 2022;76(6):1348–1361. doi:10.1016/j.jhep.2022.01.014
18. Shun SC, Chou Y-J, Chen C-H, et al. Change of uncertainty in illness and unmet care needs in patients with recurrent hepatocellular carcinoma during active treatment. Cancer Nurs. 2018;41(4):279–289. doi:10.1097/NCC.0000000000000487
19. Chen YC, Weng S-F, Hsu Y-J, et al. Continuity of care: evaluating a multidisciplinary care model for people with early CKD via a nationwide population-based longitudinal study. BMJ Open. 2020;10(12):e041149. doi:10.1136/bmjopen-2020-041149
20. Piñero F, Dirchwolf M, Pessôa MG. Biomarkers in hepatocellular carcinoma: diagnosis, prognosis and treatment response assessment. Cells. 2020;9(6):1370. doi:10.3390/cells9061370
21. Yang L, Yan C, Wang J. Effect of multi-disciplinary team care program on quality of life, anxiety, and depression in hepatocellular carcinoma patients after surgery: a randomized, controlled study. Front Surg. 2022;9:1045003. doi:10.3389/fsurg.2022.1045003
22. National Guideline, C. NICE Evidence Reviews Collection, in Multidisciplinary care: myalgic encephalomyelitis (or encephalopathy) / chronic fatigue syndrome: diagnosis and management: evidence review I. In: National Institute for Health and Care Excellence (NICE) Copyright © NICE 2021. London; 2021.
23. Wang Z, Deng S, Lv H, et al. Effect of WeChat -based continuous care intervention on the somatic function, depression, anxiety, social function and cognitive function for cancer patients: Meta-analysis of 18 RCTs. Nurs Open. 2023;10(9):6045–6057. doi:10.1002/nop2.1916
24. Brand S, Pollock K. How is continuity of care experienced by people living with chronic kidney disease? J Clin Nurs. 2018;27(1–2):153–161. doi:10.1111/jocn.13860
25. Wen N, Cai Y, Li F, et al. The clinical management of hepatocellular carcinoma worldwide: a concise review and comparison of current guidelines: 2022 update. Biosci Trends. 2022;16(1):20–30. doi:10.5582/bst.2022.01061
26. Payno E, Juez LD, Nuñez J, et al. Surgical treatment of hepatocarcinoma after Fontan surgery. Cir Esp. 2023;101(10):724–727. doi:10.1016/j.ciresp.2022.08.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Mediating Effect of Resilience on the Relationship Between Symptom Burden and Anxiety/Depression Among Chinese Patients with Primary Liver Cancer After Liver Resection
Zhang X, Zhang H, Zhang Z, Fan H, Li S
Patient Preference and Adherence 2023, 17:3033-3043
Published Date: 20 November 2023
Length of Hospital Stay in Patients with Primary Liver Cancer Undergoing Surgery: Risk Factors and Predictive Model Development
Sun B, Li X, He X, Zhang N
Journal of Hepatocellular Carcinoma 2026, 13:584645
Published Date: 17 February 2026