Back to Journals » International Journal of Women's Health » Volume 17
Impact of Maternal Weight and Gestational Weight Gain on Postpartum Hemorrhage and Adverse Outcomes: A Case–Control Study
Authors Chawanpaiboon S ![]() , Lucksanapanij M
, Lucksanapanij M
Received 10 July 2025
Accepted for publication 3 October 2025
Published 8 October 2025 Volume 2025:17 Pages 3567—3575
DOI https://doi.org/10.2147/IJWH.S552037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Saifon Chawanpaiboon,* Mananya Lucksanapanij*
Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand
*These authors contributed equally to this work
Correspondence: Saifon Chawanpaiboon, Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand, Email [email protected]
Objective: To assess the impact of maternal weight on postpartum hemorrhage (PPH) and other adverse outcomes at Siriraj Hospital.
Materials and Methods: We conducted a retrospective chart review of 835 women who underwent spontaneous vaginal deliveries between January 2019 and August 2020. The study group comprised pregnant women experiencing PPH (167 out of 835), whereas the control group included pregnant women without PPH (668 out of 835). We documented demographic information, maternal medical complications, estimated blood loss, causes of PPH, neonatal outcomes, and other maternal adverse outcomes.
Results: Baseline characteristics such as maternal age, pre-existing medical conditions, pre-pregnancy body mass index, total pregnancy weight gain, estimated blood loss, anemia, gestational age at delivery, and neonatal outcomes were not significantly different between the two groups. Mothers with excessive weight gain had a significantly greater incidence of PPH compared with those without PPH (41.9%, 70/167 vs 27.1%, 181/668; P = 0.0001). Similarly, maternal anemia (hematocrit < 33%) was more common in the PPH group (28.7%, 48/167) than in the non-PPH group (20.4%, 136/668; P = 0.019). Fetal macrosomia (neonatal weight > 4000 g) was also observed more frequently among women with PPH (3.0%, 5/167) compared with those without PPH (0.9%, 6/668; P = 0.049). These differences were statistically significant. Multiple logistic regression analysis revealed that both excessive gestational weight gain and maternal anemia were independently associated with PPH. Maternal anemia remained the strongest predictor, with an adjusted odds ratio (aOR) of 1.86 (95% CI 1.24– 2.79; P = 0.003), while excessive gestational weight gain also showed a significant association (aOR) = 1.64, 95% CI 1.08– 2.51; P = 0.021).
Conclusion: PPH was not associated with overweight or obesity. However, it was correlated with excessive gestational weight gain during pregnancy and maternal anemia.
Clinical Trial Registration: Thai Clinical Trials Registry (TCTR) 20220919004.
Plain Language Summary: We studied 835 women who gave birth at Siriraj Hospital to see whether a mother’s weight affects the risk of heavy bleeding after childbirth (postpartum hemorrhage, PPH). About one in five women had PPH. Being overweight or obese before pregnancy did not increase the risk. However, gaining too much weight during pregnancy was linked to a higher chance of PPH. Women with anemia and those who delivered very large babies were also more likely to have PPH. After accounting for other factors, anemia was the strongest predictor. These findings show that monitoring gestational weight gain and preventing or treating anemia during pregnancy are practical steps that may lower the risk of serious bleeding after birth.
Keywords: adverse outcomes, anemia, excessive weight gain, macrosomia, maternal weight, obesity, overweight, postpartum hemorrhage
Introduction
The increasing global prevalence of maternal overweight and obesity has led to a surge in pregnancy-related complications, notably, gestational hypertension, gestational diabetes, fetal macrosomia, and postpartum hemorrhage (PPH).1 Over the past 2 decades, the incidence of PPH has risen substantially, posing a critical threat to maternal health worldwide.2 The key risk factors for PPH include multiple gestations, polyhydramnios, placenta previa, placental abruption, myoma uteri, and maternal overweight and obesity.1,3 The World Health Organization defines PPH as blood loss of 500 mL or more in spontaneous vaginal delivery and 1000 mL or more in cesarean section within 24 hours after delivery.4 In Thailand, the incidence of PPH ranges from approximately 1.4% to 10.6%, with common causes including uterine atony, genital tract laceration, retained placental tissue, maternal bleeding disorders, and maternal obesity.5
Body mass index (BMI), a key indicator of maternal weight status, is calculated by dividing an individual’s weight in kilograms by the square of their height in meters (BMI = kg/m²). The World Health Organization classifies BMI into six categories:6 underweight (BMI <18.5 kg/m²), normal weight (18.5–24.9 kg/m²), overweight (25–29.9 kg/m²), obese class I (30–34.9 kg/m²), obese class II (35–39.9 kg/m²), and obese class III (≥40 kg/m²).
Previous research has consistently shown that overweight and obesity are associated with nearly twice the risk of PPH compared with normal weight.7–9 Wastnedge reported PPH rates as high as 44.6% in women with obesity.10 Obesity is also linked to lower uterine pressure during labor, which can lead to uterine atony and subsequent PPH.1,11 Furthermore, nulliparous women are found to have a greater risk of PPH.11 Overweight mothers are also more likely to require cesarean delivery because of soft tissue dystocia.12 The current study was designed to assess whether maternal overweight, obesity, and excessive gestational weight gain are associated with the occurrence of PPH. In addition, we aimed to identify other contributing factors that could inform prevention and management strategies for this potentially life-threatening condition.
Materials and Methods
Study Design
This retrospective chart review was conducted within the Statistical Unit of the Department of Obstetrics and Gynecology at the Faculty of Medicine, Siriraj Hospital. The study protocol received approval from the Siriraj Ethics Committee (Si-026/2020) and was registered in the Thai Clinical Trials Registry under the identifier 20220919004.
Sample Size Calculation
Based on findings from our pilot study, PPH occurred in 25% of women with overweight or obesity and in 10% of women with normal weight. We calculated the sample size using a significance level of 0.01 (type I error of 1%; two-sided) and a test power of 80% (type II error of 20%). Using the nQuery Advisor program, we determined that at least 162 cases were needed in each group. We set the control-to-case ratio at 4:1, resulting in 668 controls and 167 cases, totaling 835 participants.
Inclusion and Exclusion Criteria
The study included pregnant women who underwent spontaneous singleton vaginal delivery at Siriraj Hospital and had attended at least one antenatal care session. Exclusion criteria were a history of bleeding disorders (including use of anticoagulants or antiplatelets), underlying conditions causing platelet dysfunction, placenta previa, placental accreta spectrum, cancer, or incomplete data. Of 876 initially identified women, 41 were excluded due to incomplete records. Their baseline characteristics were similar to those of women included in the analysis, with no significant differences in maternal age, parity, or gestational age at delivery (data not shown). The final study population comprised 835 women.
Data Collection
Pre-pregnancy BMI was determined using height and weight measured before 12 weeks of gestation, or when unavailable by self-reported pre-pregnancy weight documented in the medical records at the first antenatal visit. As this information relied on maternal recall, there is potential for recall bias; however, the risk was minimized because data were recorded early in pregnancy by healthcare staff.
Maternal weight gain was classified relative to pre-pregnancy BMI according to the Institute of Medicine (IOM) guidelines:6 12.5–18 kg for normal BMI, 11.5–16 kg for underweight, 7–11.5 kg for overweight, and 5–9 kg for obesity.
Blood loss during delivery was measured using calibrated blood collection bags placed immediately after birth. This allowed direct quantification of postpartum blood loss and minimized potential errors from visual estimation. Postpartum hemorrhage (PPH) was defined as an estimated blood loss of ≥500 mL during vaginal delivery.
From 2019 to 2020, 835 women who met the inclusion and exclusion criteria were identified from hospital databases, of whom 167 experienced PPH (study group) and 668 did not (control group). (Figure 1).
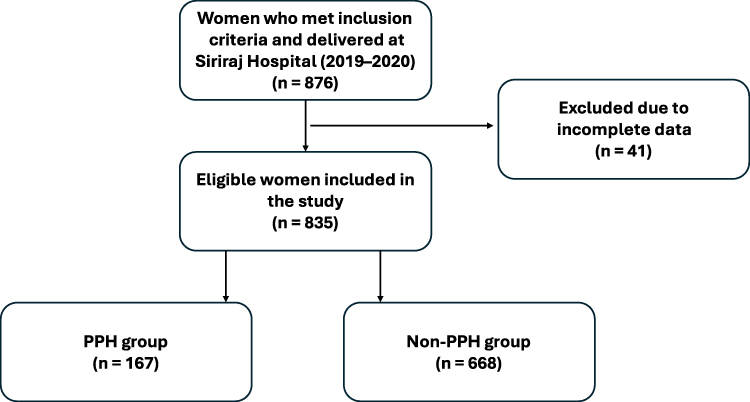 |
Figure 1 Flow diagram of participant selection. |
Baseline Characteristics
We recorded baseline characteristics, including maternal hematocrit, the number of antenatal visits, maternal complications during pregnancy (such as pregnancy-induced hypertension and gestational diabetes mellitus), maternal height, and pre-pregnancy weight. Additional data collected included gestational age at delivery, maternal underlying diseases, neonatal weight, Apgar scores, and neonatal intensive care unit admission. Postpartum hemorrhage was defined as an estimated blood loss of 500 mL or more during vaginal delivery.
Outcome Measures
The primary aim was to examine the associations between maternal overweight or obesity and the incidence of PPH. The secondary objectives were to determine the relationships between maternal anemia, the number of antenatal care visits, and the blood group with the rate of PPH. We also examined neonatal complications and admission to the neonatal intensive care unit.
Statistical Analysis
Analyses were conducted using SPSS Statistics version XX (IBM Corp., Armonk, NY, USA). Continuous variables were compared using Student’s t-test or Mann–Whitney U-test, depending on data distribution. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. Multiple logistic regression was used to identify independent risk factors for postpartum hemorrhage. A two-sided P value < 0.05 was considered statistically significant.
Results
Baseline Characteristics Comparison
The baseline characteristics were not significantly different between the two groups (Table 1). The mean maternal age was 30.8 ± 5.6 years in the PPH group and 30.4 ± 6.4 years in the non-PPH group. Multiparity was observed in 54.5% of women with PPH and 52.8% of women without PPH. Neither group had underlying diseases, hypertensive disorders, or gestational diabetes mellitus.
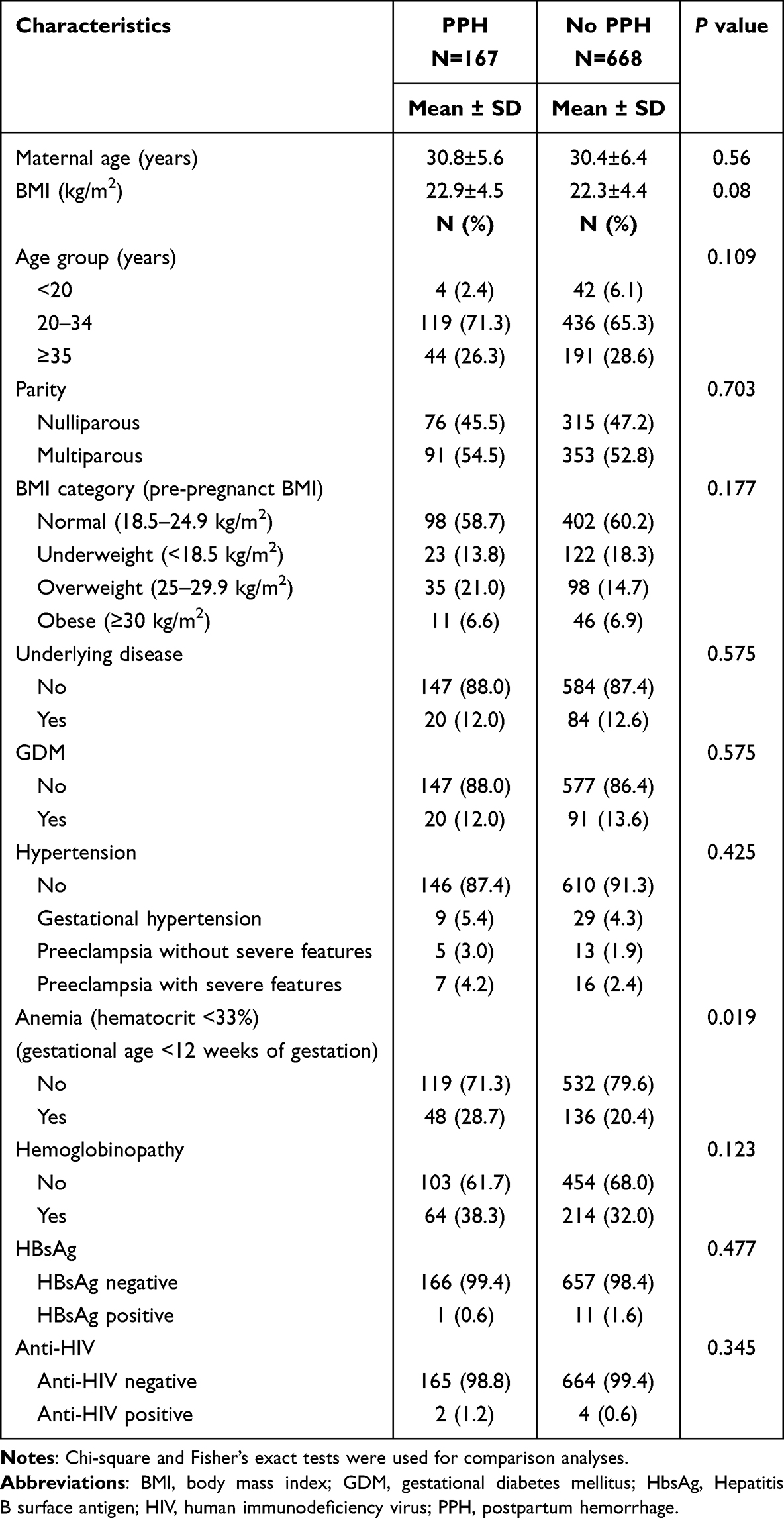 |
Table 1 Baseline Characteristics Comparison Between Pregnant Women with and Without Postpartum Hemorrhage |
Gestational Age and Weight Gain
The mean gestational age at delivery was similar between the groups: 38.4 ± 2.0 weeks in the PPH group and 38.2 ± 2.0 weeks in the non-PPH group. Most women (751 out of 835) delivered at term. Excessive weight gain was observed in 41.9% (70/167) of women with PPH, whereas it was detected in 27.1% (181/668) of women without PPH. This difference was statistically significant (P = 0.001; Table 2). The incidence of PPH was significantly greater among women with excessive weight gain than among those without excessive weight gain.
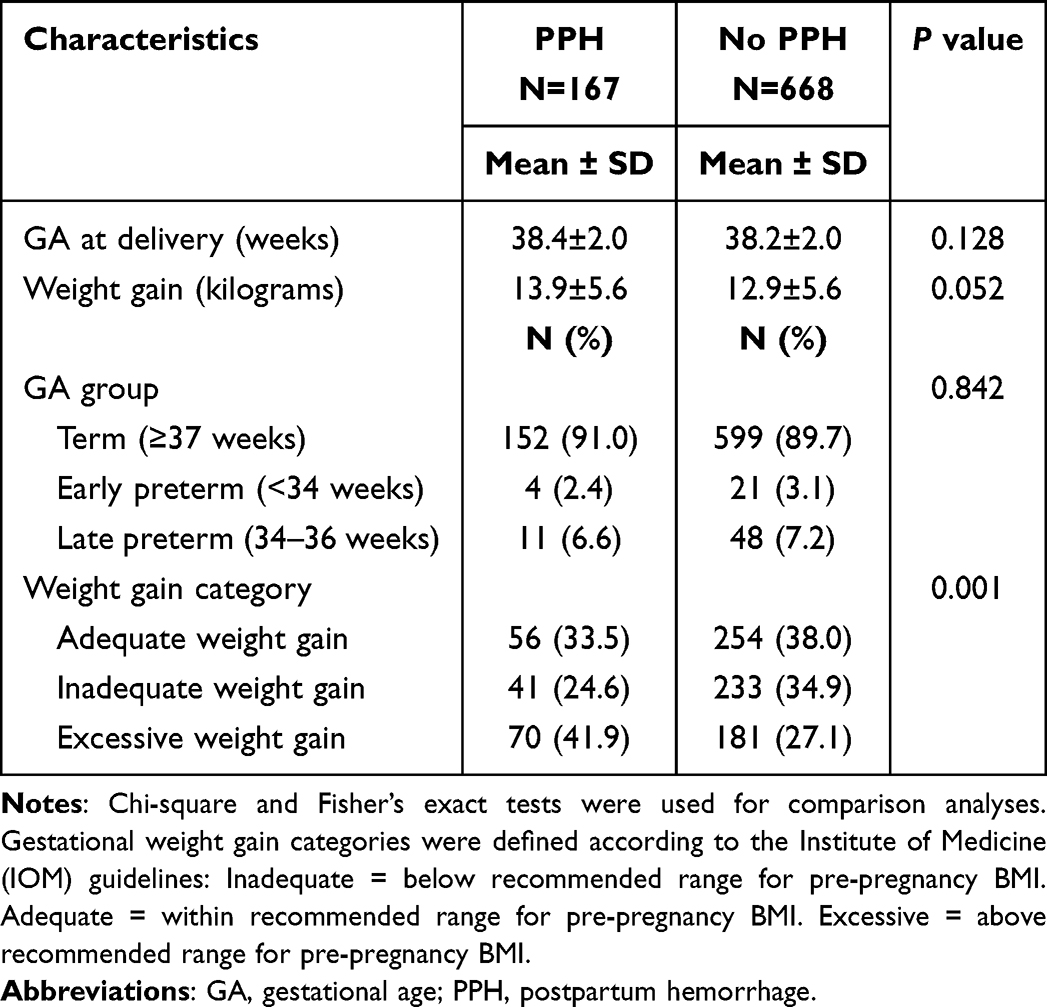 |
Table 2 Delivery Characteristics Comparison Between Women with and Without Postpartum Hemorrhage |
Estimated Blood Loss and Causes of PPH
The mean estimated blood loss was significantly greater in the PPH group (723.6 ± 264.2 mL) than in the non-PPH group (211.5 ± 112.6 mL; P < 0.01). The leading causes of PPH were uterine atony (76%), wound laceration (46.7%), retained placenta (16.8%), and cervical tear (14.4%). Blood transfusions were required in 12.6% of women with PPH, whereas they were needed in 0.7% of those without PPH. Surgical interventions were performed in 21.6% of the patients in the PPH group and in 1.5% of those in the non-PPH group (P < 0.01; Table 3).
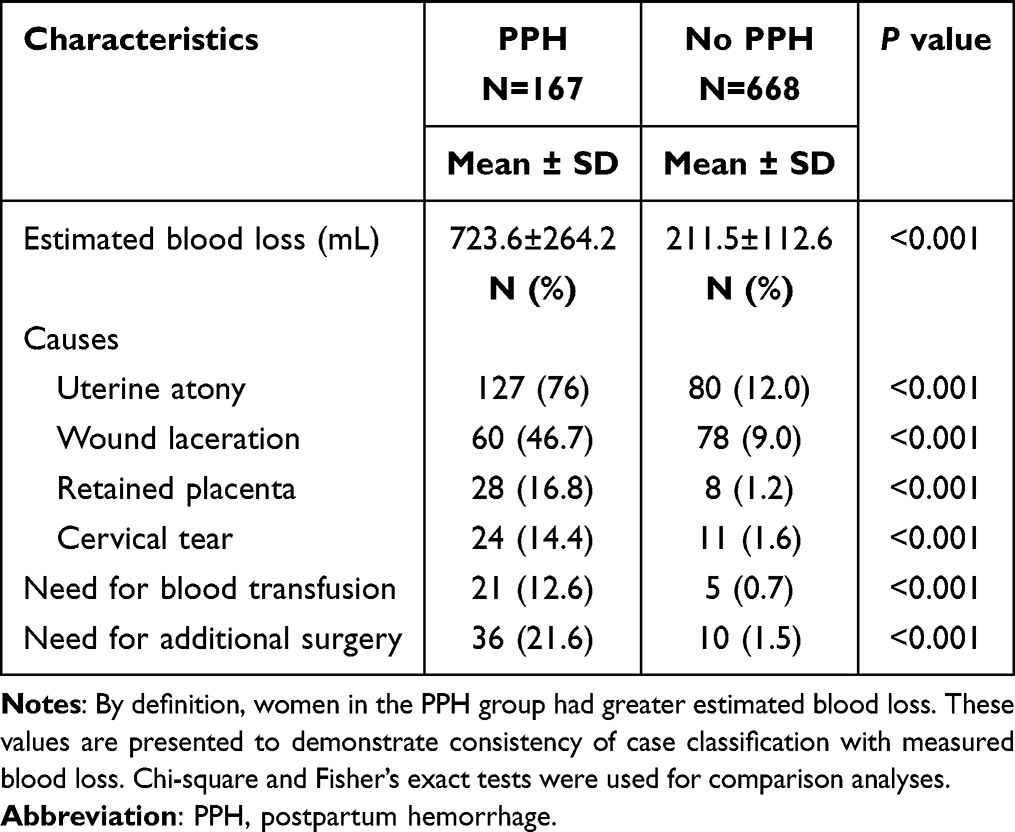 |
Table 3 Postpartum Hemorrhage Characteristics Comparison Between the Two Groups |
Neonatal Outcomes
Neonates born to mothers with PPH had a significantly greater mean birth weight (3124 ± 509 g) than those in the non-PPH group (2991 ± 470 g; P = 0.001). Approximately 75% of the newborns had a birth weight appropriate for gestational age (Table 4). The incidence of neonatal macrosomia (birth weight ≥ 4000 g) was significantly higher in the PPH group (3.0%, 5/167) than in the non-PPH group (0.9%, 6/668; P = 0.049). However, neonatal intensive care unit admission rates did not differ significantly between the two groups (Table 4).
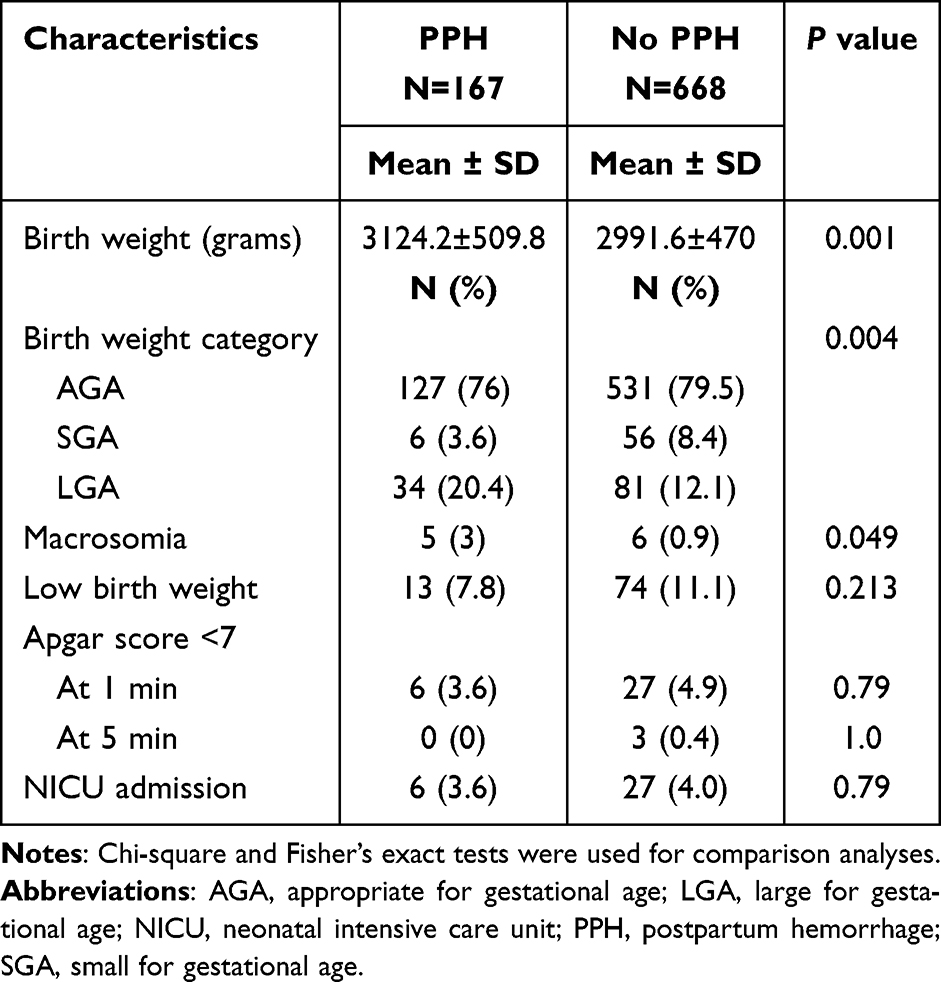 |
Table 4 Neonatal Outcomes Comparison Between Women with and Without Postpartum Hemorrhage |
Logistic Regression Analysis
Multivariate logistic regression analysis revealed that maternal anemia and excessive gestational weight gain were independently associated with an increased risk of PPH. Maternal anemia had an adjusted odds ratio of 1.86 (95% confidence interval 1.24–2.79; P = 0.03). Excessive gestational weight gain had an adjusted odds ratio of 1.64 (95% confidence interval 1.08–2.51; P = 0.021; Table 5). Maternal obesity was not independently associated with PPH.
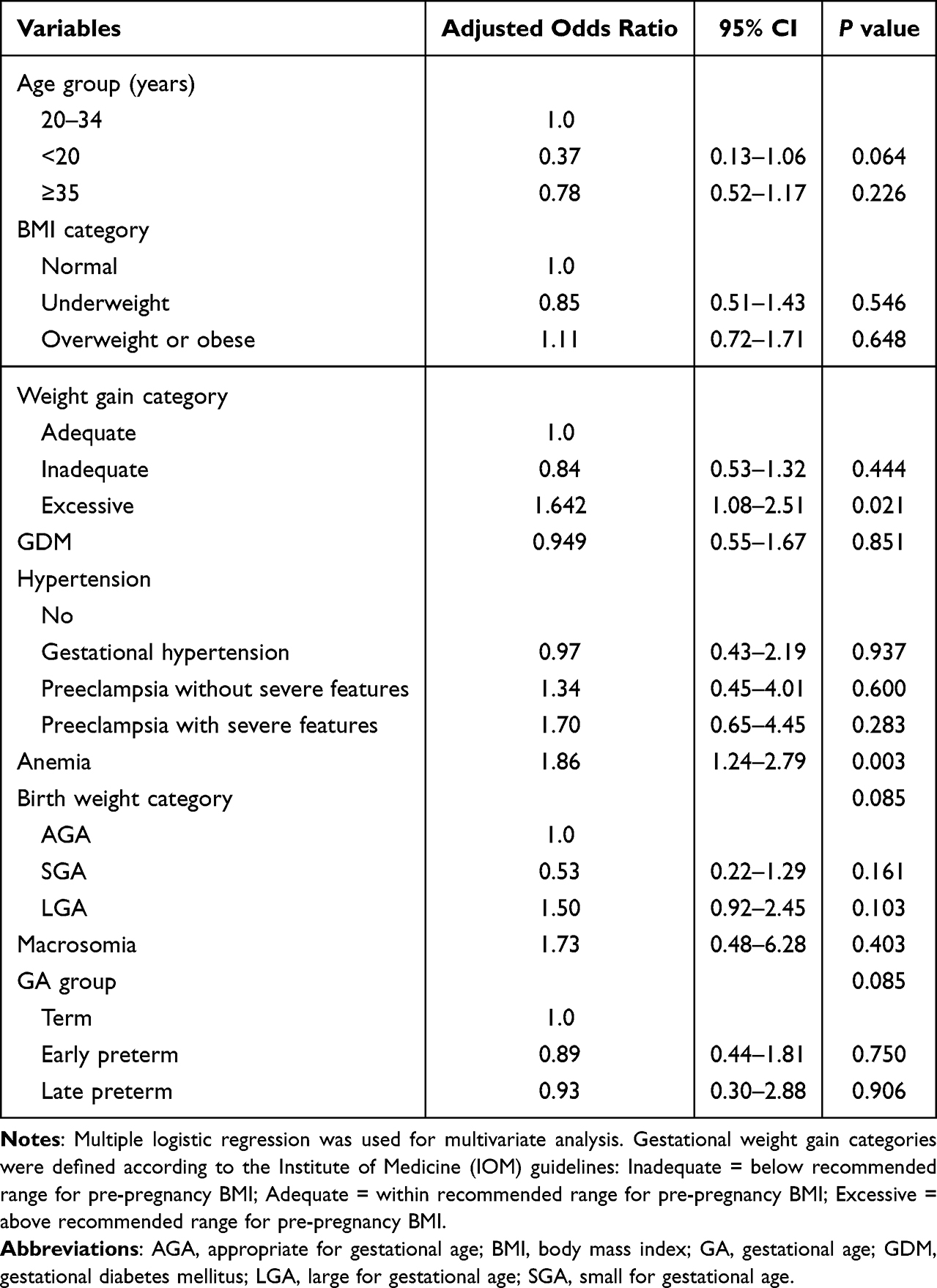 |
Table 5 Logistic Regression Analysis of Independent Factors Associated with Postpartum Hemorrhage |
Discussion
In this case–control study of 835 women with spontaneous vaginal delivery, pre-pregnancy overweight and obesity were not associated with postpartum hemorrhage (PPH). By contrast, excessive gestational weight gain and maternal anemia were independently associated with PPH, with anemia the stronger predictor. Women with macrosomia and excessive weight gain were also more likely to experience PPH. Although higher blood loss in the PPH group is expected by definition, reporting these values confirms internal validity of case classification and supports the robustness of our findings.
Maternal obesity has been linked to adverse outcomes including PPH, gestational hypertension, gestational diabetes, and preterm birth, and excessive gestational weight gain is an additional risk factor for adverse outcomes.13 Prior Western studies often report an association between obesity and PPH, potentially mediated by uterine atony, macrosomia, prolonged labor, or cesarean delivery.14 However, several Asian cohorts report less consistent associations, suggesting effects of BMI distribution, obstetric practices, and baseline nutritional status.15,16 Our finding that obesity itself was not associated with PPH is consistent with reports from Japan and China, where obesity may be a less dominant determinant of hemorrhage risk.3,16 In contrast, excessive gestational weight gain has repeatedly been linked to macrosomia, prolonged and greater blood loss13,17 patterns mirrored in our cohort.
Recent studies also highlight that gestational diabetes mellitus (GDM); influenced by obesity and weight gain, is associated with adverse outcomes, while treatment reduces large-for-gestational-age infants and macrosomia.18 Mechanistically, excessive weight gain can contribute to uterine over-distension and atony; obesity is associated with prolonged labor and higher rates of induction failure and cesarean delivery1,14,17 with uterine atony a key pathway to PPH11 Insulin resistance in obesity may promote inflammation and endothelial activation, potentially exacerbating bleeding after perineal/cervical trauma.13
Maternal anemia has been consistently associated with adverse maternal outcomes, including PPH.19,20 In Southeast Asia, where anemia prevalence can reach 30–40%, its effect may exceed that of obesity.21 Physiologically, anemia reduces oxygen-carrying capacity and may impair myometrial contractility, increasing susceptibility to atony and clinically significant blood loss.19,20 Taken together, these findings highlight the need to distinguish pre-pregnancy BMI, which reflects a static maternal characteristic, from gestational weight gain, which is dynamic and modifiable, when evaluating the risk of PPH.
Clinical Implications
Our results support antenatal interventions targeting modifiable risks: (i) individualized counseling to keep gestational weight gain within guideline ranges; and (ii) systematic screening and treatment of anemia, particularly relevant in Southeast Asian settings. Region-specific policy should integrate nutrition counseling, iron/folate supplementation, and culturally tailored weight-management strategies. Intrapartum care may be refined by flagging women with excessive weight gain or anemia for enhanced surveillance and proactive PPH prevention (eg, prophylactic uterotonics, active management of the third stage, readiness of blood products).
Strengths and Limitations
Strengths include a relatively large cohort, calibrated blood-collection bags for objective blood-loss measurement, and detailed documentation of PPH causes and management. Limitations include the retrospective design and possible misclassification of pre-pregnancy weight where self-report was used. Despite these limitations, the findings are consistent and clinically actionable: excessive gestational weight gain and maternal anemia rather than obesity per se are key, modifiable targets for PPH prevention in this context.
Conclusions
Postpartum hemorrhage is correlated with excessive gestational weight gain and maternal anemia rather than with maternal obesity or overweight. High-risk mothers should receive education on proper nutrition during pregnancy, and their weight gain should be carefully monitored. Appropriate weight gain during pregnancy can reduce both maternal and neonatal adverse outcomes.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The Ethics Committee of the Faculty of Medicine Siriraj Hospital approved its protocol. All procedures were conducted in accordance with the ethical standards of the institutional research committee (Si 026/2020) and the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study is retrospective; therefore, informed consent was not required.
Acknowledgments
We express our sincere gratitude to the Faculty of Medicine at Siriraj Hospital, Mahidol University, for support in promoting our publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We thank the Faculty of Medicine Siriraj Hospital, Mahidol University, for its funding support.
Disclosure
All authors have no conflicts of interest in this work.
References
1. Butwick AJ, Abreo A, Bateman BT, et al. Effect of maternal body mass index on postpartum hemorrhage. Anesthesiology. 2018;128(4):774–783. doi:10.1097/ALN.0000000000002082
2. Chauke L, Bhoora S, Ngene NC. Postpartum haemorrhage - an insurmountable problem? Case Rep Womens Health. 2023;37:e00482. doi:10.1016/j.crwh.2023.e00482
3. Fukami T, Koga H, Goto M, et al. Incidence and risk factors for postpartum hemorrhage among transvaginal deliveries at a tertiary perinatal medical facility in Japan. PLoS One. 2019;14(1):e0208873. doi:10.1371/journal.pone.0208873
4. Committee on Practice Bulletins-Obstetrics. Practice Bulletin No. 183: postpartum hemorrhage. Obstet Gynecol. 2017;130(4):e168–e186. PMID: 28937571. doi:10.1097/AOG.0000000000002351
5. Prapawichar P, Ratinthorn A, Utriyaprasit K, Viwatwongkasem C. Maternal and health service predictors of postpartum hemorrhage across 14 district, general and regional hospitals in Thailand. BMC Pregnancy Childbirth. 2020;20(1):172. doi:10.1186/s12884-020-2846-x
6. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
7. Fuchs F, Bouyer J, Rozenberg P, Senat MV. Adverse maternal outcomes associated with fetal macrosomia: what are the risk factors beyond birthweight? BMC Pregnancy Childbirth. 2013;13:90. doi:10.1186/1471-2393-13-90
8. Lawand G, Minisha F, Yaqoub SA, Al Dewik N, Al Rifai H, Farrell T. The impact of abnormal maternal body mass index during pregnancy on perinatal outcomes: a registry-based study from Qatar. J Perinat Med. 2023;51(9):1197–1205. doi:10.1515/jpm-2023-0198
9. Naik R, Karmali D, Nagarsenkar A, Mainath S, Pednekar G. Effect of pre-pregnancy maternal body mass index on obstetric outcomes in a Tertiary Care Hospital in Goa, India. J Obstet Gynaecol India. 2022;72(2):141–146. doi:10.1007/s13224-021-01565-z
10. Wastnedge EAN, Fretwell J, Johns EC, Denison FC, Reynolds RM. First and second pregnancy outcomes in women with class III obesity: an observational cohort study. Obes Res Clin Pract. 2021;15(4):357–361. doi:10.1016/j.orcp.2021.05.004
11. Driessen M, Bouvier-Colle MH, Dupont C, Khoshnood B, Rudigoz RC, Deneux-Tharaux C. Postpartum hemorrhage resulting from uterine atony after vaginal delivery: factors associated with severity. Obstet Gynecol. 2011;117(1):21–31. doi:10.1097/AOG.0b013e318202c845
12. Fyfe EM, Anderson NH, North RA, et al. Risk of first-stage and second-stage cesarean delivery by maternal body mass index among nulliparous women in labor at term. Obstet Gynecol. 2011;117(6):1315–1322. doi:10.1097/AOG.0b013e318217922a
13. Leung TY, Leung TN, Sahota DS, et al. Trends in maternal obesity and associated risks of adverse pregnancy outcomes in a population of Chinese women. Br J Obstet Gynaecol. 2008;115(12):1529–1537. doi:10.1111/j.1471-0528.2008.01931.x
14. Blomberg M. Maternal obesity and risk of postpartum hemorrhage. Obstet Gynecol. 2011;118(3):561–568. doi:10.1097/AOG.0b013e31822a6c59
15. Lautredou M, Pan-Petesch B, Dupré PF, et al. Excessive gestational weight gain is an independent risk factor for gestational diabetes mellitus in singleton pregnancies: results from a French cohort study. Eur J Obstet Gynecol Reprod Biol. 2022;275:31–36. doi:10.1016/j.ejogrb.2022.06.009
16. Li S, Gao J, Liu J, et al. Incidence and risk factors of postpartum hemorrhage in China: a multicenter retrospective study. Front Med Lausanne. 2021;8:673500. doi:10.3389/fmed.2021.673500
17. Carpenter JR. Intrapartum management of the Obese Gravida. Clin Obstet Gynecol. 2016;59(1):172–179. doi:10.1097/GRF.0000000000000174
18. Ugwudike B, Kwok M. Update on gestational diabetes and adverse pregnancy outcomes. Curr Opin Obstet Gynecol. 2023;35(5):453–459. doi:10.1097/GCO.0000000000000901
19. Omotayo MO, Abioye AI, Kuyebi M, Eke AC. Prenatal anemia and postpartum hemorrhage risk: a systematic review and meta-analysis. J Obstet Gynaecol Res. 2021;47(8):2565–2576. doi:10.1111/jog.14834
20. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33. doi:10.1016/S2214-109X(14)70227-X
21. Hasna Afifa Huwaida. Relationship between anemia in pregnancy and postpartum hemorrhage. World J Adv Res Rev. 2024;24(03):753–758. doi:10.30574/wjarr.2024.24.3.3728
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Intermittent Fasting Better Than Continuous Energy Restriction for Adults with Overweight and Obesity?
Ye YF, Zhang MX, Lin Z, Tang L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2813-2826
Published Date: 15 September 2022
Correlation of Obesity and Overweight with Cervical Vascular Function Among Healthy Populations
Pan X, Chen X, Ren L, Li Z, Chen S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2927-2938
Published Date: 25 September 2022
Association Between Nutritional Knowledge, Dietary Regimen, and Excess Body Weight in Primary School Teachers
Saintila J, Calizaya-Milla YE, Calizaya-Milla SE, Elejabo-Pacheco AA, Sandoval-Valentin GA, Rodriguez-Panta SG
Journal of Multidisciplinary Healthcare 2022, 15:2331-2339
Published Date: 14 October 2022
Patient and Healthcare Professional Preferences for Prescription Weight Loss Medications in Australia: Two Discrete Choice Experiments
Fifer S, Keen B, Porter A
Patient Preference and Adherence 2024, 18:435-454
Published Date: 19 February 2024
The Economic Impact of Obesity in Turkey: A Micro-Costing Analysis
Gogas Yavuz D, Akhtar O, Low K, Gras A, Gurser B, Yilmaz ES, Basse A
ClinicoEconomics and Outcomes Research 2024, 16:123-132
Published Date: 5 March 2024