Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Impact of Chronic Obstructive Pulmonary Disease on Mortality Rates After Hip Pertrochanteric Fracture: A Nationwide Population-Based Cohort Study
Authors Wu PK, Ho CH ![]() , Wu YC
, Wu YC ![]() , Liao KM
, Liao KM ![]() , Chien CS
, Chien CS
Received 12 August 2025
Accepted for publication 19 November 2025
Published 12 December 2025 Volume 2025:20 Pages 4019—4029
DOI https://doi.org/10.2147/COPD.S559900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Po-Kuan Wu,1 Chung-Han Ho,2,3 Yu-Cih Wu,2 Kuang-Ming Liao,4,5 Chi-Sheng Chien1
1Department of Orthopedic Surgery, Chi Mei Medical Center, Tainan, Taiwan; 2Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan; 3Department of Information Management, Southern Taiwan University of Science and Technology, Tainan, Taiwan; 4Department of Internal Medicine, Chi Mei Medical Center, Chiali, Tainan, Taiwan; 5Department of Nursing, Min-Hwei Junior College of Health Care Management, Tainan, Taiwan
Correspondence: Kuang-Ming Liao, Department of Internal Medicine, Chi Mei Medical Center, No. 606, Jialixing Jiali Dist, Chiali, Tainan, 72263, Taiwan, Email [email protected] Chi-Sheng Chien, Department of Orthopedic Surgery, Chi Mei Medical Center, No. 901 Zhonghua Road YongkangDist, Tainan, 71004, Taiwan, Email [email protected]
Purpose: Hip fractures are a major public health concern, especially among older adults. Chronic obstructive pulmonary disease (COPD) is a famous comorbidity that can increase post-fracture outcomes. This retrospective population-based cohort study evaluated the impact of COPD on mortality and contralateral hip fracture risk following pertrochanteric fracture.
Patients and Methods: We included patients diagnosed with pertrochanteric fracture (ICD-10-CM S72.1) between January 1, 2016, and December 31, 2022, from Taiwan’s National Health Insurance Research Database. Mortality risk was assessed using Cox proportional hazards models, adjusted for sex, age, and Charlson Comorbidity Index (CCI) score. Contralateral hip fracture risk was estimated using competing risk analysis with death as a competing event. Subgroup analyses were stratified by sex, age, and CCI group.
Results: After adjustment, COPD was significantly associated with higher 1-year mortality (AHR: 1.12, 95% CI: 1.06– 1.19, p< 0.0001). Conversely, COPD patients had a lower 1-year incidence of contralateral hip fracture compared with non-COPD patients (3.12% vs 4.40%; adjusted subdistribution HR: 0.70, 95% CI: 0.61– 0.81, p< 0.0001). Similar patterns were observed across all subgroups.
Conclusion: COPD is an independent predictor of increased 1-year mortality after pertrochanteric fracture. The observed reduction in contralateral fracture risk likely reflects the competing risk of early mortality. These findings suggest that elderly patients with COPD should pay more attention in post-hip fracture management with personalized rehabilitation strategies.
Keywords: pertrochanteric fracture, hip fracture, chronic obstructive pulmonary disease, real-world database, mortality, contralateral fracture
Introduction
Hip fractures are a major public health issue, particularly among the elderly, due to the association with increased morbidity, mortality, and considerable healthcare costs.1,2 Globally, patients with hip fractures will rise annually to 2.6 million by 2025 and 4.5 million by 2050,3 and Asia’s proportion will increase from 26% in 1990 to 45% by 2050.4 Hip fractures currently rank among the top ten causes of global disability and impose enormous direct and indirect costs.5 In Taiwan, the incidence rates of hip fractures among individuals aged over 50 years in 2015 were 209.1 per 100,000 person-years for males and 293.9 per 100,000 person-years for females.6 Previous studies have indicated that pertrochanteric fractures represented more than half of all hip fracture cases,7,8 which are typically caused by low-energy falls in individuals with underlying osteoporosis or other conditions compromising bone integrity.
Multiple risk factors contribute to both the incidence and poor outcomes of hip fractures. These include advanced age,9 frailty,10 and chronic medical conditions such as chronic obstructive pulmonary disease (COPD),11 cardiovascular disease,12 and diabetes.13 Understanding these risk factors is important for developing effective preventive strategies. It also plays a key role in optimizing outcomes through early intervention, timely surgical management, and coordinated post-fracture rehabilitation.
Among comorbidities, COPD is a particularly concerning factor that significantly worsens post-hip fracture prognosis.14,15 In Taiwan, estimates derived from national survey data suggest the true prevalence of COPD falls within the 5% to 6% range.16 Patients with COPD face increased post-operative mortality, driven by a complex interplay of physiological and clinical challenges. Pulmonary complications, including pneumonia and respiratory failure, are common due to postoperative immobilization and pre-existing respiratory compromise.17 Additionally, many COPD patients are affected by frailty and malnutrition, which contribute to sarcopenia and impede functional recovery.18,19 This impaired mobility frequently culminates in long-term disability or death. Several studies in Taiwan also have investigated the relationship between COPD and hip fractures.20 National hip-fracture incidence was 649 per 100,000 person-years in the COPD cohort and 369 per 100,000 person-years among controls.21
Despite existing research on the relationship between COPD and hip fractures, data specifically addressing post-fracture mortality in COPD patients remain limited. Moreover, few large-scale, population-based studies have focused on a common and clinically significant subtype of hip fractures, pertrochanteric fractures. Therefore, the aim of this retrospective population-based cohort study was to investigate the impact of COPD on mortality rates following pertrochanteric fracture.
Materials and Methods
Data Source
This retrospective, population-based cohort study used a claims data from the National Health Insurance Research Database (NHIRD), which covers over 99% of the population in Taiwan from a single-payer population insurance program. The NHIRD included the diagnosis and procedure codes of outpatient and inpatient, medication prescriptions, and associated medical expenditures. The diagnosis codes were based on the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). The procedure codes are identified using the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS). For research purposes, NHIRD is managed by the Health and Welfare Data Science Center (HWDC) to integrate health-related databases. All databases in HWDC were under a deidentified and anonymized format. Due to the secondary data study and de-identified information in the dataset, the IRB waived the requirement for individual informed consent. The study protocol was followed to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for this observational research study. This study was conducted in compliance with the ethical standards and guidelines of the 2013 revision of the Declaration of Helsinki and the International Ethical Guidelines for Health-related Research Involving Humans developed by the Council for International Organizations of Medical Sciences (CIOMS) in collaboration with the World Health Organization. The study protocol was approved by the Institutional Review Board of Chi Mei Medical Centre (IRB: 11407–013). Informed consent was also waived by the Institutional Review Board of Chi Mei Medical Centre owing to the use of secondary data and the absence of personal information in the study.
Study Design and Population
Due to NHIRD included detailed longitudinal health records, a retrospective cohort study design was used in this study. Patients who aged 65 years or older diagnosed with pertrochanteric fracture, identified using the ICD-10-CM code S72.1, between January 1, 2016, and December 31, 2022, were included in the initial cohort. A total of 84,415 patients were identified. The exclusion criteria were patients with prior hip fractures, indeterminate laterality, or incomplete information. Therefore, 7269 patients were excluded due to insufficient data to determine the laterality of the fracture, and an additional 18,711 patients were excluded due to a history of other types of fractures prior to the pertrochanteric fracture. After applying exclusion criteria, 58,135 patients remained eligible for analysis. The final study cohort consisted of 6664 patients with a diagnosis of COPD (ICD-10-CM: J40-J44) and 51,471 patients without COPD, who served as the control group. All patients were followed for one year from the index date of the pertrochanteric fracture diagnosis to assess outcomes, mortality and contralateral hip fracture (Figure 1).
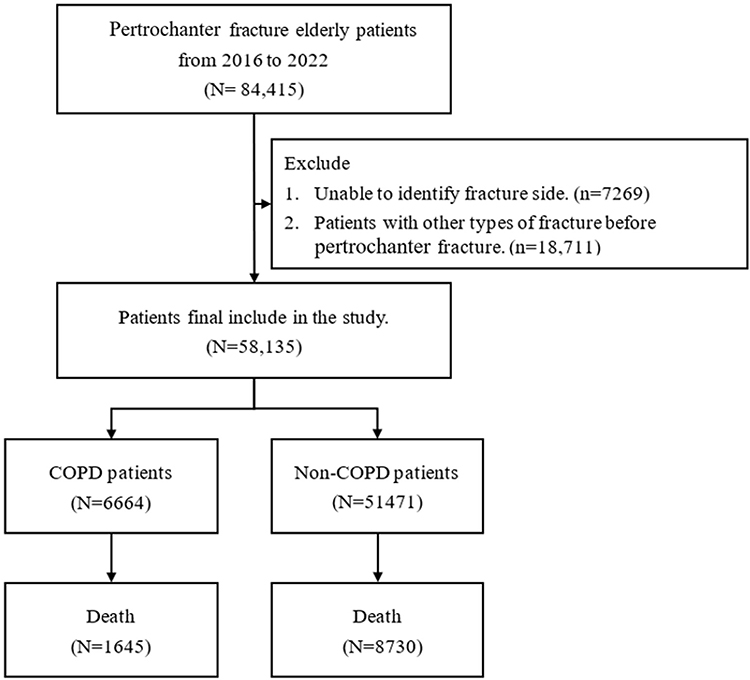 |
Figure 1 Flowchart of study subjects’ selection. |
Measurements and Outcome
Baseline information among pertrochanteric fracture patients included sex, age, and Charlson Comorbidity Index (CCI). The CCI score was calculated based on diagnoses recorded within one year before the date of the new-onset pertrochanteric fracture. The CCI was identified using ICD-10-CM codes to quantify the burden of comorbidities, and CCI was also used for risk adjustment in the analysis.22,23 Patients were categorized into three levels of disease severity according to their CCI scores: none (CCI=0), mild (CCI=1–2), and severe (CCI≥3).
The primary outcome of the study was all-cause mortality within one-year, and the secondary outcome was contralateral hip fracture. Contralateral hip fracture was identified by laterality information in the third decimal place of the ICD-10-CM diagnosis code, where “1” and “4” denote the right side and “2” and “5” denote the left side. Patients were classified as having a contralateral fracture if a hip fracture occurred on the opposite side compared with the index pertrochanteric fracture during the follow-up period. The ICD-10-CM codes used to identify contralateral hip fractures were S72.0X1, S72.0X4, S72.1X1, S72.1X4, S72.2X1, and S72.2X4 for the right side, and S72.0X2, S72.0X5, S72.1X2, S72.1X5, S72.2X2, and S72.2X5 for the left side. Cases with unspecified laterality were excluded to avoid misclassification. The mortality was based on the death-of-cause records within the HWDC.
Statistical Analysis
The distribution between pertrochanteric fracture patients with COPD and those without was estimated using Pearson’s chi-squared test for categorical variables and Student’s t-test for continuous variables. The trends in incidence of mortality and contralateral hip fracture between pertrochanteric fracture patients with COPD and those without were plotted with the Kaplan–Meier method, and differences were compared using the Log rank test. The risk of mortality was expressed as hazard ratios (HRs) with 95% confidence intervals (CIs), calculated using the Cox proportional hazards model after adjusting for potential confounding variables. The Schoenfeld residuals test was used to assess whether the proportional hazards assumption of the Cox proportional hazards model was satisfied. Additionally, the model’s goodness-of-fit was evaluated using the Akaike Information Criterion (AIC). Similarly, for the competing risk analysis of contralateral hip fracture, the Fine-Gray subdistribution hazards model, with death from any cause defined as a competing event, was used to estimate subdistribution HR (HRSD) with 95% Cis. Additionally, a subgroup analysis stratifying pertrochanteric fracture patients based on sex, age groups, and CCI groups was conducted. All statistical analyses were performed in SAS 9.4 for Windows (SAS Institute, Inc., Cary, NC, USA). Kaplan–Meier curves were plotted in STATA version 12 (Stata Corp., College Station, TX, USA). Statistical significance was set at 0.05 (two-tailed).
Results
Table 1 presented the baseline characteristics of patients aged over 65 years with pertrochanteric fractures, stratified by the presence or absence of chronic obstructive pulmonary disease (COPD). A total of 58,135 patients were included in the analysis, of 6664 (11.5%) patients with COPD and 51,471 (88.5%) without. Patients with COPD were older, more likely to be male, and had higher comorbidity scores compared to non-COPD patients. Interestingly, despite these risk factors, they had a lower incidence and longer time to development of contralateral hip fractures within one year.
 |
Table 1 Baseline Information Between Pertrochanteric Fracture Patients Who Aged Over 65 Years with COPD and Those Without |
The Kaplan–Meier survival curve illustrated the 1-year survival probability of pertrochanteric fracture patients aged over 65 years between patients with COPD and those without (Figure 2). This trend demonstrated that patients with COPD have a significantly higher mortality rate than non-COPD patients following pertrochanteric fractures (Log rank test: p<0.0001). After adjusting for sex, age, and CCI score, COPD was significantly associated with increased 1-year mortality following pertrochanteric fracture (AHR: 1.12, 95% CI: 1.06–1.19, p<0.0001). Subgroup analyses also indicated that this association presented similar results across multiple strata. Patients with COPD had higher one-year mortality compared with those without, including males (AHR: 1.13, 95% CI: 1.06–1.21, p=0.0003), females (AHR: 1.12, 95% CI: 1.01–1.23, p=0.0261), patients aged 65–74 years (AHR: 1.26, 95% CI: 1.11–1.42, p=0.0003), patients aged more than 75 years (AHR: 1.10, 95% CI: 1.03–1.17, p=0.0026), and patients with moderate comorbidity (CCI=1-2, AHR: 1.22, 95% CI: 1.12–1.33, p<0.0001) The proportional assumption was not violated due to the assessment of Schoenfeld residuals test (p>0.05) (Table 2).
 |
Table 2 Overall and Subgroup Analysis of Mortality Risk Between COPD and Non-COPD Patients Stratified by Sex, Age Groups, and CCI Categories |
 |
Figure 2 The trend of mortality risk between COPD and non-COPD among patients aged over 65 years with pertrochanteric fractures. |
Figure 3 show the cumulative incidence curves of contralateral hip fracture, and it indicated that a lower contralateral hip fracture in COPD patients compared with non-COPD patients (Log rank test, p<0.0001). Additionally, patients with COPD had a significantly lower 1-year incidence of contralateral hip fracture than non-COPD patients (3.12% vs 4.40%; AHRSD: 0.70, 95% CI: 0.61–0.81, p<0.0001) after considering of death from any cause as competing event and adjusting for sex, age, and CCI score. In the subgroup analysis, sex, age groups, and the classification of CCI score also presented a protective effect of COPD compared with those without, with subdistribution hazard ratios ranging from 0.61 (95% CI: 0.48–0.78) to 0.77 (95% CI: 0.62–0.96) (Table 3).
 |
Table 3 Overall and Subgroup Analysis of Contralateral Fractures Risk Between COPD and Non-COPD Patients Using Competing Risk Model, Stratified by Sex, Age Groups, and CCI Categories |
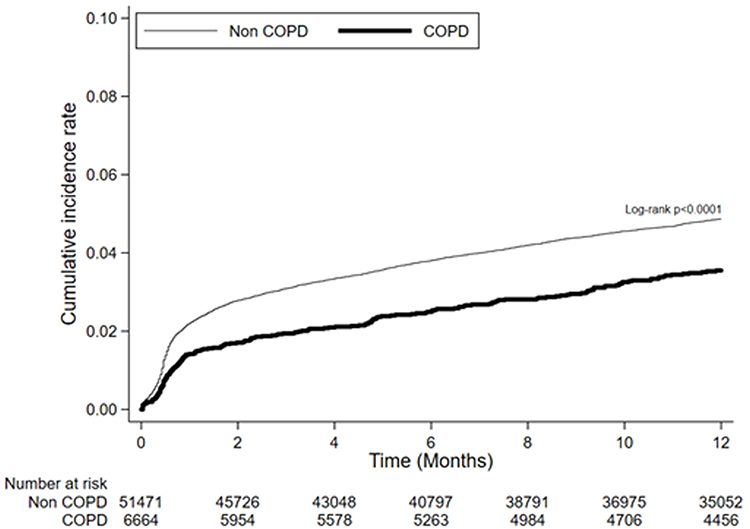 |
Figure 3 The trend of contralateral fracture risk between COPD and non-COPD among patients aged over 65 years with pertrochanteric fractures. |
Discussion
Recovery following hip fracture is often protracted in patients with COPD.24 The presence of respiratory symptoms, particularly exertional dyspnea, can significantly impede early mobilization and limit engagement in postoperative rehabilitation protocols.25 A study by Chen et al identified obstructive pulmonary disease as an independent risk factor for postoperative respiratory failure in elderly patients undergoing hip fracture surgery, highlighting the vulnerability of this patient population to respiratory complications.26 Additionally, research by Tian et al demonstrated that respiratory disease significantly increases the risk of perioperative acute heart failure in older hip fracture patients, underscoring the impact of pulmonary comorbidities on cardiac outcomes.27 Furthermore, a study by Li et al reported that COPD is an independent risk factor for perioperative paroxysmal atrial fibrillation in elderly patients with hip fractures, indicating the complex interplay between pulmonary and cardiac complications in this demographic.28
Our study found that patients with COPD exhibited a higher mortality rate following pertrochanteric fractures compared to those without COPD. The increased mortality observed in COPD patients following pertrochanteric fractures results from a complex interplay of respiratory compromise, systemic inflammation, and multimorbidity that creates substantial perioperative risk. Diminished respiratory reserve predisposes these patients to pulmonary complications including pneumonia and respiratory failure,26,29 while the systemic inflammatory nature of COPD impairs wound healing and increases susceptibility to multiorgan dysfunction.30,31 The high prevalence of malnutrition in COPD patients further compounds surgical risk, with studies demonstrating up to approximately a 3.7-fold higher one-year post-fracture mortality.32 A population-based cohort study in Denmark found that patients with COPD had a 60–70% increased risk of death after hip fracture compared to those without COPD, with a one-year mortality rate approximately 3–5 times greater than in controls without hip fracture.33 Similarly, a Japanese nationwide inpatient database study reported that COPD patients with hip fractures had an in-hospital mortality rate of 7.4%, higher than that of COPD patients with other types of fractures.14 Surgical treatment was associated with lower mortality compared to conservative treatment.14 In addition to COPD, several factors such as advanced age, higher comorbidity burden, and male sex have been associated with increased post-hip fracture mortality.34,35 Consistently, our subgroup analyses demonstrated higher mortality association among these groups in this study.
Interestingly, the analysis revealed a significantly lower rate of contralateral hip fractures among patients with COPD. Several factors may contribute to this finding. First, increased post-fracture mortality in COPD patients may reduce the time window during which a subsequent fracture could occur. Second, in light of the established association between COPD and osteoporosis,36 patients with COPD may be more likely to receive targeted secondary prevention measures, including pharmacologic interventions and structured fall prevention strategies. Third, COPD-related functional limitations, including reduced mobility due to dyspnea, may lead to early adoption of assistive devices and greater avoidance of high-risk activities, thereby decreasing fall risk.37,38
This study presented the evidence of the association between COPD and hip fracture outcomes using population-based data from Taiwan. Furthermore, our findings demonstrate that COPD was independently associated with increased post-fracture mortality and a lower risk of contralateral hip fracture in elderly patients with COPD. The paradoxical finding of reduced contralateral hip fracture rates among COPD patients likely reflects the competing risk of mortality, where patients succumb to complications before experiencing subsequent fractures. These findings highlight the critical importance of identifying COPD as a high-risk comorbidity in hip fracture management protocols. Mitigating the fall risk in COPD patients necessitates a multi-factorial strategy that focuses on three key areas: first, implementing pulmonary rehabilitation centered on targeted balance and strength training;39 second, conducting systematic medication reviews to reduce the burden of fall-risk Increasing drugs;40 third, optimizing co-morbidities alongside environmental modifications to prevent injurious falls. Clinicians should prioritize comprehensive risk stratification for COPD patients presenting with hip fractures. Evidence emphasizes the importance of early surgery,41 careful optimization of COPD and comorbidities, multimodal pulmonary care and analgesia, early mobilization, and the adoption of orthogeriatric multidisciplinary care models.42 Strategies aimed at improving bone health and preventing future fractures are equally important for long-term outcomes in this vulnerable population.
Several limitations should be considered in this study. First, this retrospective cohort study used claims data from the NHIRD, so the accuracy of diagnoses depended on ICD-10-CM coding may have potential misclassification or overdiagnosis bias. However, the spirometry test may be generally used by healthcare facilities, especially for elderly hospitalized patients. Therefore, the study likely captured the majority of COPD cases diagnosed within the healthcare system, although some underdiagnosis in outpatient cannot be excluded. Second, the database lacked detailed clinical information, including of smoking history, body mass index, pulmonary function test results, the use of home oxygen therapy, history of hip replacement, the presence of physical disability, and laboratory parameters. The absence of these variables may have limited the adjustment for all potential confounders in the statistical analysis. Third, the severity of COPD, such as GOLD stage, which is typically categorized based on post-bronchodilator FEV1, could not be directly assessed in this study. Additionally, the frequency and severity of acute exacerbations of COPD (AECOPD) could not be assessed due to this information was unavailable in the claims database. Since AECOPD episodes may affect postoperative outcomes and mortality risk,43,44 future studies should include the related clinical data to further evaluate this association. Finally, since only hospitalized patients with COPD were included in this study, the possibility of selection bias cannot be excluded. Despite these limitations, the large sample population and standardized data collection in the NHIRD still could show the generalizability of our results.
Conclusions
Elderly patients with COPD and hip fractures show higher peri operative and one-year mortality. Considering of pre operative evaluation, including spirometry, symptom assessment, and pulmonary rehabilitation, coupled with timely surgical intervention and multidisciplinary orthogeriatric care, can reduce complications and improve survival. Future research should focus on developing targeted interventions to improve survival outcomes in this vulnerable population. These findings provide essential evidence for evidence-based guidelines in managing hip fractures among patients with chronic obstructive pulmonary disease. Ultimately, this research emphasizes the imperative for personalized medicine approaches that consider the complex interaction between COPD and orthopedic outcomes.
Data Management and Sharing
The data have been sourced from the Taiwan Nation Health Insurance Database and Taiwan Cancer Registry. The data are available with permission from the Taiwan Health and Welfare Data Science Centre: https://dep.mohw.gov.tw/DOS/cp-5119-59201-113.html (accessed 10 August 2025). Restrictions apply to the availability of these data, which were used under license for this study.
Ethics Approval and Consent to Participate
This study was conducted in compliance with the ethical standards and guidelines of the 2013 revision of the Declaration of Helsinki and the International Ethical Guidelines for Health-related Research Involving Humans developed by the Council for International Organizations of Medical Sciences (CIOMS) in collaboration with the World Health Organization. The study protocol was approved by the Institutional Review Board of Chi Mei Medical Centre (IRB: 11407-013). Informed consent was also waived by the Institutional Review Board of Chi Mei Medical Centre owing to the use of secondary data and the absence of personal information in the study.
Acknowledgments
The authors are grateful to the Health Data Science Centre of the National Cheng Kung University Hospital for providing administrative and technical support.
Funding
This study was supported by grants from the Chi Mei Medical Center (grant number: CMFHR114102). The funding agency was not involved in any aspect of the study design, including data collection, data interpretation, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leal J, Gray AM, Prieto-Alhambra D, et al. Impact of hip fracture on hospital care costs: a population-based study. Osteoporos Int. 2016;27(2):549–558. doi:10.1007/s00198-015-3277-9
2. Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018;49(8):1458–1460. doi:10.1016/j.injury.2018.04.015
3. Babagoli M, Ghaseminejad Raeini A, Sheykhvatan M, Baghdadi S, Shafiei SH. Influencing factors on morbidity and mortality in intertrochanteric fractures. Sci Rep. 2023;13(1):12090. doi:10.1038/s41598-023-38667-9
4. Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7(5):407–413. doi:10.1007/pl00004148
5. Daskalakis II, Bastian JD, Tosounidis TH. Time is bone: missed opportunities for secondary prevention after a hip fracture. J Clin Med. 2025;14(16):5816. doi:10.3390/jcm14165816
6. Lee MT, Fu SH, Hsu CC, et al. Epidemiology and clinical impact of osteoporosis in Taiwan: a 12-year trend of a nationwide population-based study. J Formos Med Assoc. 2023;122 Suppl 1:S21–S35. doi:10.1016/j.jfma.2023.05.001
7. Chie WC, Yang RS, Liu JP, Tsai KS. High incidence rate of hip fracture in Taiwan: estimated from a nationwide health insurance database. Osteoporos Int. 2004;15(12):998–1002. doi:10.1007/s00198-004-1651-0
8. Tsai KS, Tai TY. Epidemiology of osteoporosis in Taiwan. Osteoporos Int. 1997;7(Suppl 3):S96–8. doi:10.1007/BF03194352
9. Buzkova P, Cauley JA, Fink HA, Robbins JA, Mukamal KJ, Barzilay JI. Age-related factors associated with the risk of hip fracture. Endocr Pract. 2023;29(6):478–483. doi:10.1016/j.eprac.2023.03.001
10. Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5):513–521. doi:10.1001/jama.2009.50
11. Herland T, Apalset EM, Eide GE, Tell GS, Lehmann S. Airflow limitation as a risk factor for low bone mineral density and Hip fracture. Eur Clin Respir J. 2016;3:32214. doi:10.3402/ecrj.v3.32214
12. Xu B, Han L, Liu H, et al. Cardiovascular disease and hip fracture among older inpatients in Beijing, China. Biomed Res Int. 2013;2013:493696. doi:10.1155/2013/493696
13. Rolland Y, Abellan van Kan G, Benetos A, et al. Frailty, osteoporosis and hip fracture: causes, consequences and therapeutic perspectives. J Nutr Health Aging. 2008;12(5):335–346. doi:10.1007/BF02982665
14. Yamauchi Y, Yasunaga H, Sakamoto Y, et al. Mortality associated with bone fractures in COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:2335–2340. doi:10.2147/COPD.S112142
15. Buss L, McKeever TM, Nightingale J, et al. Hip fracture outcomes in patients with chronic obstructive pulmonary disease. Br J Anaesth. 2018;121(6):1377–1379. doi:10.1016/j.bja.2018.09.008
16. Cheng SL, Chan MC, Wang CC, et al. COPD in Taiwan: a national epidemiology survey. Int J Chron Obstruct Pulmon Dis. 2015;10:2459–2467. doi:10.2147/COPD.S89672
17. Carpintero P, Caeiro JR, Carpintero R, Morales A, Silva S, Mesa M. Complications of Hip fractures: a review. World J Orthop. 2014;5(4):402–411. doi:10.5312/wjo.v5.i4.402
18. Yogesh M, Patel J, Makwana N, Mody M. The triad of physiological challenges: investigating the intersection of sarcopenia, malnutrition, and malnutrition-sarcopenia syndrome in patients with COPD - a cross-sectional study. BMC Pulm Med. 2024;24(1):71. doi:10.1186/s12890-024-02884-3
19. Kaluzniak-Szymanowska A, Krzyminska-Siemaszko R, Deskur-Smielecka E, Lewandowicz M, Kaczmarek B, Wieczorowska-Tobis K. Malnutrition, sarcopenia, and malnutrition-sarcopenia syndrome in older adults with COPD. Nutrients. 2021;14(1):44. doi:10.3390/nu14010044
20. Liao KM, Shen CW, Chiu KL, Lu CH, Fang CW, Chen CY. Epidemiology of osteoporosis in patients with chronic obstructive pulmonary disease in Taiwan. J Epidemiol Glob Health. 2024;14(1):213–222. doi:10.1007/s44197-023-00183-4
21. Huang SW, Wang WT, Chou LC, Chen HC, Liou TH, Lin HW. Chronic obstructive pulmonary disease increases the risk of hip fracture: a nationwide population-based cohort study. Sci Rep. 2016;6:23360. doi:10.1038/srep23360
22. Glasheen WP, Cordier T, Gumpina R, Haugh G, Davis J, Renda A. Charlson comorbidity index: ICD-9 update and ICD-10 translation. Am Health Drug Benef. 2019;12(4):188.
23. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
24. Cha YH, Ha YC, Park HJ, et al. Relationship of chronic obstructive pulmonary disease severity with early and late mortality in elderly patients with hip fracture. Injury. 2019;50(9):1529–1533. doi:10.1016/j.injury.2019.05.021
25. Teng H, Tian J, Shu Q. Comprehensive pulmonary rehabilitation for a 90-year-old patient with intertrochanteric fracture complicated by chronic obstructive pulmonary disease: a case report. Physiother Theory Pract. 2024;40(11):2712–2718. doi:10.1080/09593985.2023.2268170
26. Chen J, Tian Z, Zhang H, et al. Risks of postoperative respiratory failure in elderly patients after Hip surgery: a retrospective study. J Orthop Surg Res. 2022;17(1):140. doi:10.1186/s13018-022-02909-9
27. Tian M, Li W, Wang Y, et al. Risk factors for perioperative acute heart failure in older Hip fracture patients and establishment of a nomogram predictive model. J Orthop Surg Res. 2023;18(1):347. doi:10.1186/s13018-023-03825-2
28. Li W, Min A, Zhao W, et al. Predictors and prognosis of elderly hip fracture patients with perioperative atrial fibrillation: a nested case-control study. BMC Geriatr. 2025;25(1):4. doi:10.1186/s12877-024-05647-1
29. Liao KM, Lu HY. A national analysis of complications following total hip replacement in patients with chronic obstructive pulmonary disease. Medicine. 2016;95(12):e3182. doi:10.1097/MD.0000000000003182
30. Tkacova R. Systemic inflammation in chronic obstructive pulmonary disease: may adipose tissue play a role? Review of the literature and future perspectives. Mediators Inflamm. 2010;2010:585989. doi:10.1155/2010/585989
31. Agusti A. Systemic effects of chronic obstructive pulmonary disease: what we know and what we don’t know (but should). Proc Am Thorac Soc. 2007;4(7):522–525. doi:10.1513/pats.200701-004FM
32. Chiavarini M, Ricciotti GM, Genga A, et al. Malnutrition-related health outcomes in older adults with hip fractures: a systematic review and meta-analysis. Nutrients. 2024;16(7):1069. doi:10.3390/nu16071069
33. de Luise C, Brimacombe M, Pedersen L, Sorensen HT. Chronic obstructive pulmonary disease and mortality following hip fracture: a population-based cohort study. Eur J Epidemiol. 2008;23(2):115–122. doi:10.1007/s10654-007-9211-5
34. Sing CW, Lin TC, Bartholomew S, et al. Global epidemiology of hip fractures: secular trends in incidence rate, post‐fracture treatment, and all‐cause mortality. J Bone Miner Res. 2023;38(8):1064–1075. doi:10.1002/jbmr.4821
35. Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016;16(1):158. doi:10.1186/s12877-016-0332-0
36. Chen SJ, Liao WC, Huang KH, et al. Chronic obstructive pulmonary disease and allied conditions is a strong independent risk factor for osteoporosis and pathologic fractures: a population-based cohort study. QJM. 2015;108(8):633–640. doi:10.1093/qjmed/hcv012
37. Roig M, Eng JJ, MacIntyre DL, et al. Falls in people with chronic obstructive pulmonary disease: an observational cohort study. Respir Med. 2011;105(3):461–469. doi:10.1016/j.rmed.2010.08.015
38. Lahousse L, Ziere G, Verlinden VJ, et al. Risk of frailty in elderly with COPD: a Population-Based Study. J Gerontol a Biol Sci Med Sci. 2016;71(5):689–695. doi:10.1093/gerona/glv154
39. Delbressine JM, Vaes AW, Goertz YM, et al. Effects of exercise-based interventions on fall risk and balance in patients with chronic obstructive pulmonary disease: a systematic review. J Cardiopulm Rehabil Prev. 2020;40(3):152–163. doi:10.1097/HCR.0000000000000513
40. McDermott CL, Feemster LC, Engelberg RA, Spece LJ, Donovan LM, Curtis JR. Fall risk and medication use near end of life among adults with chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis. 2024;11(6):604–610. doi:10.15326/jcopdf.2024.0551
41. Lo IL, Siu CW, Tse HF, Lau TW, Leung F, Wong M. Pre-operative pulmonary assessment for patients with Hip fracture. Osteoporos Int. 2010;21(Suppl 4):S579–86. doi:10.1007/s00198-010-1427-7
42. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in Hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma. 2014;28(3):e49–55. doi:10.1097/BOT.0b013e3182a5a045
43. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
44. Prediletto I, Giancotti G, Nava S. COPD exacerbation: why it is important to avoid ICU admission. J Clin Med. 2023;12(10):3369. doi:10.3390/jcm12103369
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intertrochanteric Fracture Surgery Patients with Diabetes Mellitus are Prone to Suffer Perioperative Neurological and Endocrine/Metabolic Complications: A Propensity-Score Matched Analysis
Tang Y, Kang L, Guo M, Fan L
Therapeutics and Clinical Risk Management 2022, 18:775-783
Published Date: 6 August 2022
Characteristics of Elderly Hip Fracture Patients in Jordan: A Multicenter Epidemiological Study
Dawod MS, Alisi MS, Saber YO, Abdel-Hay QA, Al-Aktam BM, Alfaouri Y, Alfraihat LB, Albadaineh AA, Abuqudiri AZ, Odeh RM, Altamimi AAR, Alrawashdeh MA, Alebbini MM, Abu-Dhaim OA, Al-Omari AA, Alaqrabawi I, Alswerki MN, Abuawad A, Al Nawaiseh MR, Hammad Y, Al-Ajlouni J
International Journal of General Medicine 2022, 15:6591-6598
Published Date: 13 August 2022
Six-Minute Walking Test and 30 Seconds Chair-Stand-Test as Predictors of Mortality in COPD – A Cohort Study
Höglund J, Boström C, Sundh J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2461-2469
Published Date: 4 October 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023