Back to Journals » Clinical Ophthalmology » Volume 20
Impact of a Patient Navigator Program on Access to Outpatient Ophthalmic Surgery
Authors Tallapaneni PS, Zaheer HA, Cassidy J, Liang HW, McGinnis-Thomas DM, Williams AM ![]()
Received 12 March 2026
Accepted for publication 9 June 2026
Published 16 June 2026 Volume 2026:20 608653
DOI https://doi.org/10.2147/OPTH.S608653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Pooja Sree Tallapaneni, Haniah A Zaheer, Julie Cassidy, Hai-Wei Liang, Dana Marie McGinnis-Thomas, Andrew M Williams
Department of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
Correspondence: Andrew M Williams, Email [email protected]
Purpose: To evaluate the impact of a patient navigator program on surgical completion rates and visual outcomes among ophthalmology patients.
Setting: Tertiary academic eye institute.
Design: Retrospective cohort study.
Methods: Patients recommended ophthalmic surgery who were referred to a patient navigator program to address barriers to surgical care in 2023 were included. The patient navigator program provided individualized logistical, financial, and social support to facilitate surgical completion, including transportation coordination and access to financial assistance. The primary outcome was surgical completion rate. A secondary outcome was change in visual acuity and time from program referral to surgery.
Results: In total, 82 eyes of 64 patients were referred to our patient navigator program for surgical coordination. In all, 64 of 82 eyes (78%) referred for surgery successfully underwent the recommended operation. Resolution rates were highest for patient referred for transportation needs (28 of 31, 90%) or a surgical companion (25 of 30, 83%), with more modest success for cases involving lack of insurance (8 of 15, 53%) (p< 0.001). Cataract extraction was the most commonly recommended procedure (53, 65%), followed by retinal detachment repair (15, 18%). The median time from referral to surgery was 39 days (interquartile range: 12, 78), with no significant difference across surgery types (p=0.60). Among those who successfully received surgery, mean best-corrected visual acuity (BCVA) improved significantly with a mean change of − 0.37 logarithm of the minimum angle of resolution (logMAR) (95% CI: − 0.59 to − 0.15; p< 0.001) overall, with the greatest improvement observed in cataract surgery (mean change − 0.44 logMAR, 95% CI: − 0.67 to − 0.21).
Conclusion: A patient navigator program demonstrates potential to facilitate access to outpatient ophthalmic surgery for patients who face barriers to care. These preliminary findings support further investigation of patient navigation in ophthalmology as a strategy to enhance equitable access to outpatient surgical treatment.
Plain Language Summary: Many patients who need eye surgery face challenges such as lack of transportation, difficulty finding someone to accompany them to surgery, or problems with insurance coverage. These barriers can prevent patients from receiving vision-restoring procedures.
In this study, we examined whether a patient navigator program could help address these challenges. Patient navigators worked directly with patients to identify barriers to care and connect them with appropriate community and health-system resources, including transportation services, surgical companions, and assistance with insurance or financial issues.
We reviewed records from patients referred to the patient navigator program at a large academic eye center in 2023. Most patients referred to the program were able to successfully undergo their recommended eye surgery, and vision outcomes improved after surgery.
These findings suggest that patient navigator programs can play an important role in improving access to outpatient eye surgery, particularly for patients facing social or logistical barriers.
Keywords: patient navigation, ophthalmic surgery, access to care, social determinants of health, health equity
Introduction
Many patients face barriers to regular eye care, including lack of health insurance, limited access to transportation, and financial strain.1 These barriers can be particularly salient for ophthalmic patients in need of surgery. Most eye surgery occurs in outpatient, ambulatory surgery settings that require advanced scheduling, coordinating of preoperative clearances, adequate health insurance, arranged transportation, and an accompanying companion or support person.2 These logistical requirements can be difficult to meet for socially disadvantaged patients. Accessibility to ambulatory surgery centers (ASCs), where most outpatient ophthalmic surgery occurs, is a particular challenge for patients with limited resources, due in part to geographic disparity with disproportionate location of ASCs in neighborhoods with high socioeconomic status.3–5 It is therefore no surprise that socially disadvantaged patients have less access to common ophthalmic procedures, such as cataract surgery, and thus face a higher burden of untreated eye disease and visual impairment.6,7
Transportation, insurance coverage, and need for a companion are among the most common preventable barriers to outpatient ophthalmic surgery. For instance, one retrospective analysis of glaucoma surgery cancellations at a tertiary academic center found that 28% were preventable, with lack of transportation accounting for 34% of preventable cases and insurance-related issues accounting for 14%.8 Adults with glaucoma face more than twice the adjusted odds of delaying medical care due to transportation barriers compared to those without the condition, with those experiencing glaucoma-related vision loss at even greater risk.9 At our own institution, nearly three-quarters of glaucoma patients who missed a scheduled appointment reported at least one barrier to care — most commonly transportation and cost concerns — and one-third expressed interest in a patient navigator program.10 Despite recognition of these barriers, transportation-only interventions have shown inconsistent effects on care completion in randomized trials,11 suggesting that more comprehensive, multi-domain support may be needed for disadvantaged patients in need of outpatient surgery.
Barriers to ophthalmic surgical care may be addressable through a patient navigator program, which provides individualized assistance to patients with health-related social needs. These consultations connect patients to community resources to address specific barriers to care, such as need for medical transportation or financial assistance. Patient navigator programs serve as intermediaries between patients, healthcare providers, and community resources, and these programs facilitate access to a range of health services, including screening, cancer care, and chronic disease management.12–14 Recently, implementation of a patient navigator program in our academic ophthalmology department has demonstrated high case resolution and positive patient feedback.15 However, the ability of a patient navigator program to address barriers to outpatient eye surgery has not been examined.
The purpose of this study is to examine the outcomes of our patient navigator program on providing access to outpatient ophthalmic surgery among patients with self-reported barriers to ambulatory surgical care.
Methods
This retrospective study was approved by the University of Pittsburgh Institutional Review Board (IRB), adhered to the tenets of the Declaration of Helsinki, and complied with the Health Insurance Portability and Accountability Act of 1996. Patient informed consent was waived by the IRB.
Patient Navigator Program
Our patient navigator program was established in 2021 after growing recognition of the need to address social barriers to eye care. Supported by departmental and foundation funding, the program connects patients with local resources including the Pennsylvania Medical Assistance Transportation Program, senior support centers, vision rehabilitation organizations, and home care agencies. Department physicians or staff make referrals to the program when they recognize an unmet need and receive permission from a patient to place a consultation request. Social needs may be expressed during the office visit, the surgery scheduling process, or through a screening tool embedded in the electronic health record (EHR).16 Referrals occur in person, through the EHR, or by secure email, and follow-up is conducted through phone calls or at the time of in-person clinic visits. Patients generally engage with the patient navigator program on the day of referral, and all interactions come at no cost to the patient. The patient navigator team provides relevant resources to address the expressed needs and assists in completing related forms. The program follows up after consultation to ensure needs have been addressed.15
Data Collection
A retrospective chart review of all adult patients referred to the patient navigator program in 2023 was conducted to identify those referred to access outpatient ophthalmic surgery. Demographic and clinical information was extracted via EHR, including age, gender, race, insurance status, and visual acuity as well as data on referral source, reason for referral, and case resolution. The best-corrected visual acuity (BCVA) was documented on the day of referral and, for those who underwent surgery, again on the first postoperative month. BCVA was converted to logarithm of the minimum angle of resolution (logMAR) for analysis.
Outcome Measures
The primary outcome was successful receipt of recommended surgery, as defined by documentation in the EHR with a supporting operative report. Secondary outcomes included time from program referral to surgery completion and improvement in BCVA at one month postoperatively.
Statistical Analysis
Descriptive statistics included mean ± standard deviation (SD) for continuous variables. Statistical analyses were performed using the chi-squared test or Fisher’s exact test for categorical variables and the Mann–Whitney test for continuous variables.
To account for the non-independence of observations arising from patients contributing multiple referral needs or more than one eye, generalized estimating equations (GEE) with a Poisson log link, exchangeable correlation structure, and robust sandwich variance estimation were used throughout the analysis. For referral need analyses, resolution rates across need types were compared using a Wald test, with pairwise comparisons made against transportation as the reference group. Results are reported as relative risk (RR) with 95% confidence intervals (CI). For visual acuity analyses, GEE with a Gaussian family was used to estimate mean change in logMAR from referral date to one month after surgery. Time from referral to surgery was described by surgery type using median and interquartile range (IQR). Kaplan-Meier curves were generated, and groups were compared using the Log rank test. Eyes were treated as the unit of analysis; as some patients contributed both eyes, observations were not fully independent, and results should be interpreted accordingly. Analyses were performed using R (version 4.4.1). All tests were two-sided, and a p<0.05 was considered statistically significant.
Results
In total, 64 unique patients utilized the patient navigator program to address barriers to surgery. Analyses were conducted at three levels: patient-level characteristics (n=64 patients), referral need-level analysis (n=79 identified needs), and eye-level surgical outcomes (n=82 eyes). The mean ± SD age was 67 ± 11 years, and most patients were female sex (40, 63%) or white race (46, 72%). Most spoke English as a primary language (55, 86%) and had health insurance (49, 77%), with Medicare (30%) and dual Medicare/Medicaid plans (19%) being the most common coverage types (Table 1).
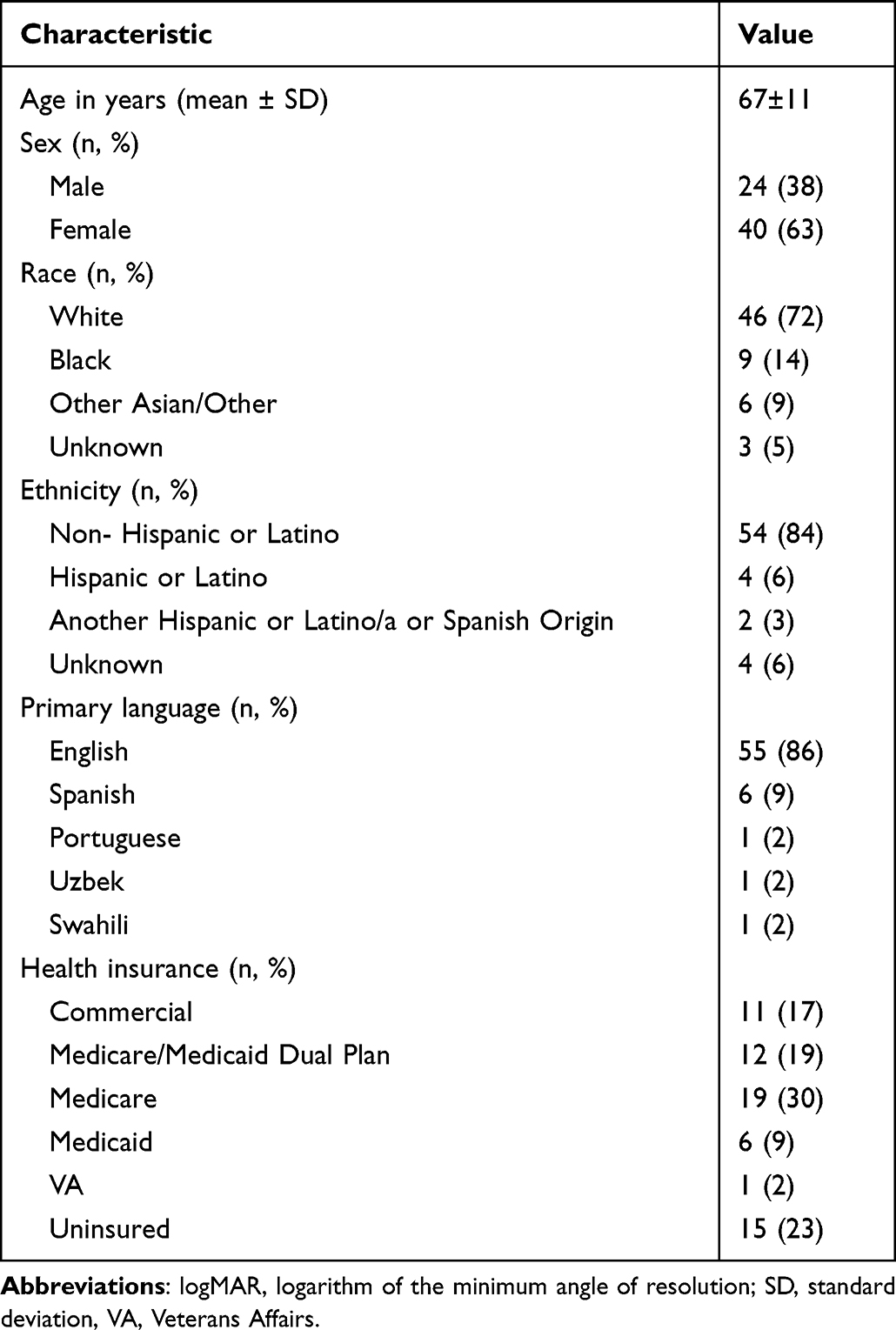 |
Table 1 Demographic and Clinical Characteristics of 64 Patients Referred to the Patient Navigator Program for Access to Ophthalmic Surgery in 2023 |
Patients were referred to the patient navigator program for a total of 79 identified needs. Overall, 61 (77%) were successfully resolved. The most common referral needs were for transportation assistance (31, 39%), need for a surgical companion (30, 38%), and lack of insurance (15, 19%). Resolution rates differed across referral need types: transportation (90%) and companion for surgery (83%) had the highest resolution rates, while insurance (53%) and financial assistance (0%) were substantially lower (Wald test, p<0.01). After accounting for within-patient correlation using GEE, lack of insurance had a significantly lower resolution rate compared to need for transportation (RR=0.77, 95% CI: 0.63, 0.93). Financial assistance could not be reliably estimated due to complete separation, as no referrals in this group were resolved (0 out of 3) (Table 2).
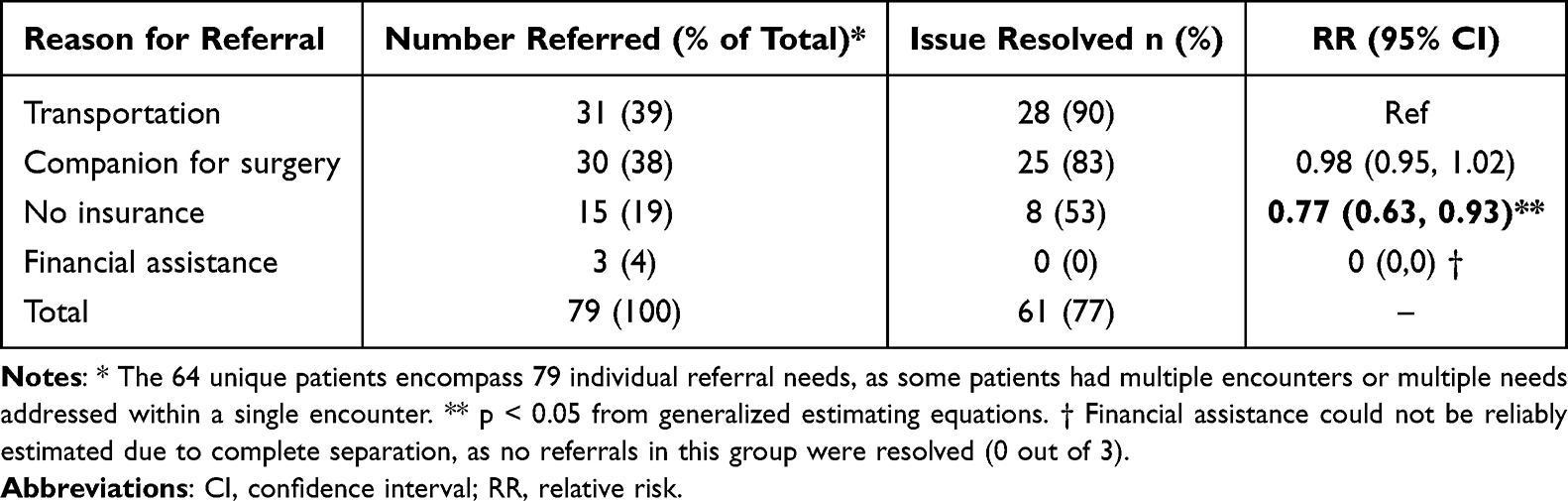 |
Table 2 Reason for Referral to the Patient Navigator Program and Case Outcomes for 79 Individual Referral Needs Among 64 Unique Patients |
Surgical intervention was recommended for 82 eyes among the 64 patients referred to the patient navigator program, with procedures completed across multiple ophthalmic subspecialties (Table 3). The most common indication was cataract (n=53, 65%), for which 39 eyes (74%) underwent cataract extraction. Retinal detachment was the next most frequent diagnosis (n=15, 18%), with 14 eyes (93%) receiving pars plana vitrectomy, including two combined with cataract extraction. Other completed procedures included one each for conjunctival excision biopsy, pterygium excision, ERM peel with PPV, blepharoplasty, ptosis repair, orbitotomy, enucleation, choroidal drainage (tube revision), tube shunt, cataract extraction with goniotomy, anterior chamber washout, and transscleral diode. In all, 64 of 82 eyes (78.0%) referred for surgery successfully underwent the recommended operation.
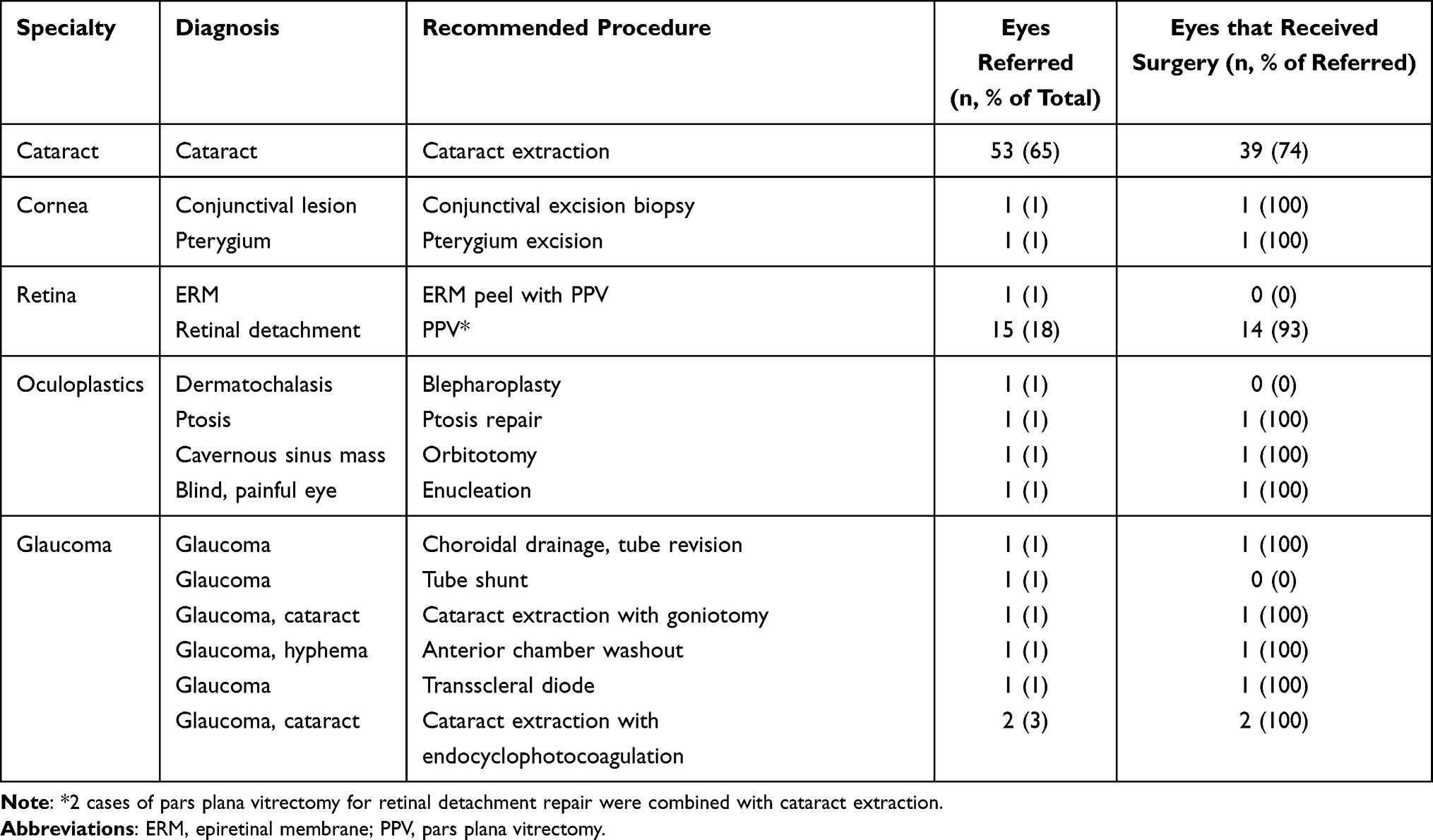 |
Table 3 Recommended and Completed Surgeries for 82 Eyes |
Time from referral to surgery was available for 63 eyes, with one eye excluded due to a missing date. Overall, the median time from referral to surgery was 39 days (IQR: 12, 78), ranging from 1 to 406 days. Cataract surgery had a median time of 41 days between referral and surgical completion (IQR: 23, 84), whereas retina and glaucoma surgery had median times of 27 days (IQR: 2, 39) and 30 days (IQR: 14, 58), respectively. Kaplan-Meier curves demonstrated that most eyes across all surgery types received surgery within the first 90 days following referral, with cataract showing the longest tail extending to 406 days. No statistically significant difference in time to surgery was observed across surgery types (log-rank p=0.60) (Supplemental Table 1 and Supplemental Figure 1).
Postoperative visual outcomes demonstrated clinically meaningful improvements. Among patients who underwent surgery with complete BCVA data (n=47 unique patients; n=62 eyes), mean BCVA improved from referral date to one month postoperatively, with a mean change of −0.37 logMAR (95% CI: −0.59, −0.15; p<0.001). In subgroup analysis by surgery type, cataract surgery (n=39) demonstrated the greatest improvement, with a mean change of −0.44 logMAR (95% CI: −0.67, −0.21; p<0.001) (Table 4).
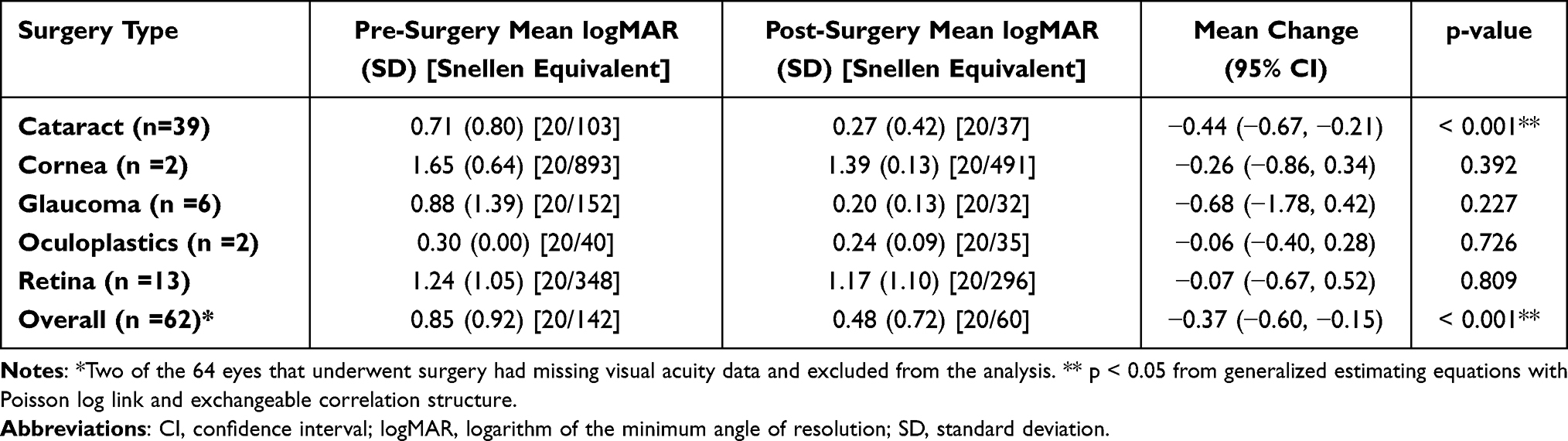 |
Table 4 Change in Visual Acuity by Surgery Type |
Discussion
Our patient navigator program assisted 64 patients with 79 referral needs, among whom 82 eyes were recommended surgery. In all, 64 of 82 eyes (78%) underwent the recommended outpatient ophthalmic surgical procedure among a patient population with documented barriers to surgical care. The most common barriers addressed were transportation, a companion for surgery, and lack of insurance. Several patients faced multiple simultaneous barriers rather than a single isolated barrier. By engaging patients directly, identifying individual needs, and leveraging a broad network of community resources, the patient navigator program may facilitate access to surgical care.
Patient navigator programs have gained increasing recognition as an effective strategy for reducing barriers to healthcare access. Patient navigation interventions have been shown to improve access to health services among vulnerable populations, particularly older adults, by addressing barriers such as limited awareness of available resources, challenges with enrollment processes, and fragmented care coordination. Programs like the 2-1-1 San Diego Healthcare Navigation Service have demonstrated success in enrolling eligible individuals into Medicaid and other assistance programs, with high satisfaction reported among older participants.17 In primary care settings, the integration of patient navigators has been especially beneficial for elderly patients with complex medical and social needs, facilitating access to social services, health coverage, and continuity of care.18
The referral process to our patient navigator program was streamlined through multiple pathways, including referrals via the EHR, secure email, and direct phone calls from office staff. In the majority of cases, referrals were addressed on the same day they were received. The navigator initiated outreach either by telephone or in person during scheduled clinic visits. This direct, personalized interaction also enabled real-time support with navigating complex administrative processes, such as completing applications for financial aid or public insurance programs, which are often burdensome and inaccessible for patients navigating these issues alone.
In addition to assisting with paperwork, the navigator maintained close communication with ophthalmologists to secure letters of medical necessity, procedural authorizations, and other supporting documentation required to advance care. Importantly, referrals often revealed previously unrecognized or undocumented barriers to care. These included housing insecurity, utility shut-off risks, employment limitations, disability benefit applications, and concerns regarding post-operative support. The navigator’s comprehensive and patient-centered approach allowed for simultaneous management of both immediate surgical barriers and broader unmet social needs.
A prior evaluation of our navigator program found a 90% overall case resolution rate across referral types, with high patient satisfaction (mean 4.87 of 5) and 72% of patients reporting that navigator involvement directly contributed to their ability to manage their eye health.15 These findings underscore the effectiveness of patient navigation in enhancing patient experience, particularly when navigators offer hands-on support with transportation, insurance, and financial barriers and in improving access to essential community resources.
Our patient navigator addressed barriers to surgical care through coordination with a range of community and government programs. Transportation needs were met primarily through state-funded services, including the Pennsylvania Medical Assistance Transportation Program, ACCESS, and Freedom Transit.19 Companion needs were addressed through structured volunteer and home care organizations, which also offered ancillary support such as post-operative assistance and health insurance counseling.20
Through our program, the patient navigator also provided hands-on assistance with insurance and financial aid applications, including form completion and communication with clinical staff to obtain supporting documentation. While many of these resources are publicly available, patient awareness and navigation of enrollment processes remain major barriers, especially for elderly individuals. One finding that warrants direct interpretation is the inability to resolve financial assistance referrals (0 of 3 cases). Unlike transportation and companion barriers, which could be addressed through established programs with active referral pathways, financial assistance required identifying emergency surgical funding for patients who did not meet standard eligibility criteria. These challenges are consistent with findings from Moneme et al21 that found that among surgical patient navigators, financial and insurance securement was identified as the most structurally complex navigation domain, characterized by administrative inefficiencies and processing timelines poorly matched to surgical urgency.21 Future programs should consider dedicated financial counseling resources to address this gap. The need for direct assistance with insurance and financial aid processes among older adults is well-documented in the medical literature. A review by Abdi et al22 utilizing the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) framework, identified environmental barriers, such as limited access to information and professional guidance, as key impediments to care for older individuals with chronic conditions. The review specifically highlights that poor coordination between service providers and a lack of awareness about available programs significantly hinder older adults’ ability to navigate complex enrollment procedures. These challenges are further compounded by the administrative burden of acquiring supporting documentation and completing lengthy application forms, which often necessitate hands-on support from navigators or clinical staff.22,23
Results from our patient navigator program are consistent with reports about patient navigation in other surgical settings. For instance, a patient navigator program for trauma patients at one level I hospital improved outpatient trauma clinic appointment attendance.24 In a qualitative interview study of volunteer patient navigators for surgery, bureaucracy was a common barrier to effective implementation that was mitigated by standard operating procedures and administration support.23 The nascent body of work on surgical patient navigator programs suggests that these programs can promote health equity by addressing health-related social needs that underly social determinants of health for surgical patients.
Our study has limitations. First, the retrospective nature, while appropriate for assessing implementation outcome, relies on documentation of EHR and our patient navigator’s clinical records, which may not uniformly capture all relevant data points. Second, the retrospective design without a comparator group limits the interpretability of findings and introduces the potential for referral bias, as only patients whose providers identified and referred them to the navigation program were included. Patients with similar barriers who were not referred could not be reliably identified from existing records, and it is therefore not possible to determine whether they differed systematically in disease severity, motivation, or social support. A historical control group was similarly not feasible due to inconsistent EHR documentation prior to program implementation. These limitations may affect the generalizability of the findings and preclude definitive conclusions about the program’s overall effectiveness. Future prospective studies with a formal control group are warranted to more rigorously evaluate the impact of patient navigation on surgical access and visual outcomes. Additionally, the study period covers a one-year snapshot of the program activity, which may not fully reflect evolving referral patterns or longitudinal trends in the program. Further, as some patients contributed more than one referral need (64 unique patients; 79 referral items), observations were not fully independent. While GEE was used to account for within-patient correlation, the small sample size for certain referral types, particularly financial assistance (n=3), precluded reliable estimation and limits the interpretability of comparisons involving that group. Future studies with larger samples are warranted to confirm these findings across all referrals need types. Additionally, although prior evaluation of the program demonstrated high levels of patient satisfaction, satisfaction metrics specific to surgical referrals was not collected, which may help further guide our future studies. Finally, cost effectiveness and scalability of patient navigator programs remain important areas for future investigation for long-term sustainability.
In summary, a patient navigator program embedded within an academic ophthalmology department facilitated surgical access for 78% of patients with barriers to care. BCVA improved for patients who completed their recommended outpatient ophthalmic procedure through the patient navigator program. Integrated patient navigator programs may mitigate barriers to care and promote health equity in outpatient surgical care.
Abbreviations
ASC, ambulatory surgery center; BCVA, best-corrected visual acuity; CI, confidence interval; EHR, electronic health record; GEE, generalized estimating equations; IQR, interquartile range; IRB, Institutional Review Board; logMAR, logarithm of the minimum angle of resolution; RR, relative risk.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional data governance policies but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the University of Pittsburgh Institutional Review Board (STUDY20080229). Patient informed consent was waived by the IRB.
Consent for Publication
Consent for publication was not required as no identifiable patient images, videos, or recordings are included.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Institutes of Health (NIH) through core grant P30 EY08098, the Henry L. Hillman Foundation, the Eye and Ear Foundation of Pittsburgh, and from an unrestricted grant from Research to Prevent Blindness to the Department of Ophthalmology at the University of Pittsburgh. The funding organizations had no role in the design or conduct of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Williams AM, Sahel JA. Addressing social determinants of vision health. Ophthalmol Ther. 2022;11(4):1371–9.
2. Solomon SD, Shoge RY, Ervin AM, et al. Improving access to eye care: a systematic review of the literature. Ophthalmology. 2022;129(10):e114–e126. doi:10.1016/j.ophtha.2022.07.012
3. Chatterjee A, Amen TB, Khormaee S. Trends in geographic disparities in access to ambulatory surgery centers in New York, 2010 to 2018. JAMA Health Forum. 2022;3(10):e223608. doi:10.1001/jamahealthforum.2022.3608
4. Janeway MG, Sanchez SE, Chen Q, et al. Association of race, health insurance status, and household income with location and outcomes of ambulatory surgery among adult patients in 2 US states. JAMA Surg. 2020;155(12):1123–1131. doi:10.1001/jamasurg.2020.3318
5. Strope SA, Sarma A, Ye Z, Wei JT, Hollenbeck BK. Disparities in the use of ambulatory surgical centers: a cross sectional study. BMC Health Serv Res. 2009;9(1):121. doi:10.1186/1472-6963-9-121
6. Awidi AA, Wang J, Varadaraj V, et al. The impact of social determinants of health on vision loss from cataracts and cataract surgery utilization in the United States: a national health interview survey analysis. Am J Ophthalmol. 2023;254:44–53. doi:10.1016/j.ajo.2023.03.017
7. Ong SS, Tran D, Westlund E, et al. Neighborhood-level social determinants of health and presenting characteristics for rhegmatogenous retinal detachments. JAMA Ophthalmol. 2024;142(9):845–854. doi:10.1001/jamaophthalmol.2024.2889
8. Mehran N, Ojalvo I, Myers JS, Razeghinejad R, Lee D, Kolomeyer NN. Surgical cancellations in glaucoma practice: causes, delays, and effect on patient care and revenue. Ophthalmol Glaucoma. 2021;4(4):427–432. doi:10.1016/j.ogla.2020.12.006
9. Kim AB, Cheng BT, Tanna AP. Delayed medical care due to lack of transportation among US adults with glaucoma. Ophthalmol Glaucoma. 2023;6(4):439–441. doi:10.1016/j.ogla.2023.03.007
10. Wasser LM, Bear TM, Sommers M, Cassidy J, Muir KW, Williams AM. Barriers to care among glaucoma patients with a missed appointment and interest in a navigator program. J Glaucoma. 2024;33(4):297–302. doi:10.1097/IJG.0000000000002330
11. Solomon EM, Wing H, Steiner JF, Gottlieb LM. Impact of transportation interventions on health care outcomes: a systematic review. Med Care. 2020;58(4):384–391. doi:10.1097/MLR.0000000000001292
12. Teng LJ, Goldsmith LJ, Sawhney M, Jussaume L. Hip and knee replacement patients’ experiences with an orthopaedic patient navigator: a qualitative study. Orthop Nurs. 2021;40(5):292–298. doi:10.1097/NOR.0000000000000789
13. Chen M, Wu VS, Falk D, Cheatham C, Cullen J, Hoehn R. Patient navigation in cancer treatment: a systematic review. Curr Oncol Rep. 2024;26(5):504–537. doi:10.1007/s11912-024-01514-9
14. Shusted CS, Barta JA, Lake M, et al. The case for patient navigation in lung cancer screening in vulnerable populations: a systematic review. Popul Health Manag. 2019;22(4):347–361. doi:10.1089/pop.2018.0128
15. Zarnegar A, Cassidy J, Stone A, et al. Effect of a patient navigator program to address barriers to eye care at an academic ophthalmology practice. J Acad Ophthalmol. 2023;15(1):e106–e111. doi:10.1055/s-0043-1768696
16. Mayer N, Cassidy J, Wasser LM, Liu PJ, Williams AM. Seeing the unseen: uncovering health-related social needs through universal screening at an academic ophthalmology practice. Eye. 2025;39(8):1501–1507. doi:10.1038/s41433-025-03690-9
17. Rodgers JT, Purnell JQ. Healthcare navigation service in 2-1-1 San Diego: guiding individuals to the care they need. Am J Prev Med. 2012;43(6 Suppl 5):S450–456. doi:10.1016/j.amepre.2012.08.012
18. Ferrante JM, Cohen DJ, Crosson JC. Translating the patient navigator approach to meet the needs of primary care. J Am Board Fam Med. 2010;23(6):736–744. doi:10.3122/jabfm.2010.06.100085
19. Medical Assistance Transportation Program. Commonwealth of Pennsylvania. Available from: https://www.pa.gov/services/dhs/medical-assistance-transportation-program.
20. Area Agency on Aging. Allegheny County. Available from: https://www.alleghenycounty.us/Services/Human-Services-DHS/DHS-Offices/Area-Agency-on-Aging.
21. Moneme AN, Syvyk S, Bakillah E, et al. Barriers to and facilitators of a novel preprofessional patient navigation program in surgery. J Surg Res. 2025;311:54–63. doi:10.1016/j.jss.2025.03.066
22. Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9
23. Hark LA, Gorroochurn P, Pizzi LT, et al. Patient navigators improve in-office eye exam adherence after community eye screenings in a randomized clinical trial: NYC-SIGHT Study. Am J Ophthalmol. 2025;274:54–66. doi:10.1016/j.ajo.2025.02.030
24. Thompson AA, Foley K, Wothe JK, et al. Patient navigator in trauma survivor follow-up. JAMA Surg. 2025;160(9):1034–1035. doi:10.1001/jamasurg.2025.2561
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Disparities in Rheumatology in the United States
Wright GC, Zueger PM, Copley-Merriman C, Khan S, Costello J, Krumbach A, Reddy P, Tanjinatus O, Wells AF
Open Access Rheumatology: Research and Reviews 2025, 17:1-12
Published Date: 9 January 2025
Social Determinants of Health, Nursing Care Quality, and Patient Outcomes in Neurological Disorders: A Systematic Review
Yuan S, Hou J, Yang X
Risk Management and Healthcare Policy 2026, 19:597958
Published Date: 23 May 2026