Back to Journals » Journal of Pain Research » Volume 18
Immediate Analgesic Efficacy of Acupuncture in Acute Postoperative Pain Following Internal Fixation of Intertrochanteric Femoral Fractures: Protocol for a Randomized Controlled Trial
Authors Wang H ![]() , Wang T, Tang X, Tang X
, Wang T, Tang X, Tang X ![]() , Li C, Deng Y
, Li C, Deng Y ![]() , Li Q, Liang F
, Li Q, Liang F ![]() , Liao J
, Liao J ![]() , Guo T
, Guo T ![]()
Received 2 April 2025
Accepted for publication 23 July 2025
Published 31 July 2025 Volume 2025:18 Pages 3793—3803
DOI https://doi.org/10.2147/JPR.S531794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Hongyang Wang,1,* Tao Wang,2,* Xiaoxia Tang,2 Xin Tang,1 Chunxiang Li,2 Yuanzheng Deng,1 Qifu Li,3 Fanrong Liang,3 Jianglong Liao,2 Taipin Guo1
1School of Second Clinical Medicine, Yunnan University of Chinese Medicine, Kunming, People’s Republic of China; 2Kunming Municipal Hospital of Traditional Chinese Medicine, Kunming, People’s Republic of China; 3College of Acupuncture and Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianglong Liao, Kunming Municipal Hospital of Traditional Chinese Medicine, Kunming, People’s Republic of China, Email [email protected] Taipin Guo, School of Second Clinical Medicine, Yunnan University of Chinese Medicine, Kunming, People’s Republic of China, Email [email protected]
Purpose: Intertrochanteric femur fractures (IFF) undergoing internal fixation often present with persistent, intolerable hip pain after surgery. Therefore, the immediate alleviation of pain constitutes a critical clinical necessity for participants. This study aims to evaluate the immediate analgesic efficacy of acupuncture within 10 minutes of treatment in participants experiencing acute postoperative pain following internal fixation of IFF.
Participants and Methods: From March 2025 to March 2027, 154 postoperative IFF patients (aged 50– 75) at Kunming Municipal Hospital of Traditional Chinese Medicine will be randomized (1:1) into acupuncture or sham acupuncture groups using computer-generated randomization sequences, with allocation concealment ensured through opaque sealed envelopes. Each group will receive a 10-minute treatment session, and the post-treatment evaluation will be performed after 2, 4, 6, 8, and 10 minutes of acupuncture. The primary outcome will be pain intensity measured by the Visual Analogue Scale (VAS) at 10 minutes post-treatment. Secondary outcomes include the pain VAS score at 2, 4, 6, and 8 minutes post-treatment, the blinding assessment, and the treatment effectiveness expectations scale. This analysis will follow the intention-to-treat (ITT) principle.
Discussion: This study is the first randomized controlled clinical trial to assess the immediate analgesic effects of acupuncture in participants experiencing acute postoperative pain following internal fixation for IFF. This study aims to provide a simple, rapid, and effective therapeutic option for clinical pain management after internal fixation for IFF.
Keywords: intertrochanteric femoral fracture, internal fixation, immediate efficacy, acupuncture, protocol
Introduction
Intertrochanteric femoral fracture (IFF) is defined as a fracture occurring between the femoral neck base and the lesser trochanter level.1 Current epidemiological data have shown that this type of fracture is characterized by a high prevalence in the elderly population over 65 years of age, especially in the combined osteoporotic patient population, where approximately 87% of cases are low-energy trauma.2,3 Globally, IFF accounts for approximately 50% of all hip fractures and places a heavy burden on orthopaedic healthcare systems.4 The estimated annual cost of IFF to the US healthcare system reaches $2.63 billion, accounting for 44% of the cost burden from all hip fractures.5 Beyond its economic impact, IFF is associated with significantly elevated risks of subsequent fractures, mortality, and morbidity, including reduced mobility and impaired quality of life, when compared to the general population.6,7
Internal fixation is one of the main clinical treatments for IFF.8–10 However, a substantial subset of patients develop persistent and unbearable pain after surgery, potentially due to surgical trauma or complications, which seriously affects patient’s daily lives. Consequently, achieving rapid analgesia during the acute postoperative phase has become the main need of patients.
Currently, nonsteroidal anti-inflammatory drugs (NSAIDs) are widely used as first-line drugs for postoperative pain management in patients with IFF.11,12 However, they have some limitations, such as extended treatment period, slow onset of action (approximately 30 minutes), and high recurrence rate.13,14 In addition, the use of NSAIDs may cause adverse effects on the digestive and cardiovascular systems.15,16 Therefore, there is an urgent need for an alternative therapy that can rapidly alleviate acute pain symptoms after postoperative internal fixation of IFF. Acupuncture, a non-pharmacological therapy in traditional Chinese medicine, shows potential advantages in managing acute pain disorders.17 A randomized controlled trial on acute renal colic caused by urinary tract stones showed that the acupuncture group had a 47.6% improvement in pain response rate after 10 minutes of treatment compared with the sham acupuncture group.18 A systematic review and meta-analysis further confirmed that acupuncture treatment has a more significant immediate analgesic effect than medication for specific conditions.19 Moreover, in our preclinical practice, we observed that acupuncture can relieve the pain level of patients after IFF with internal fixation in a short period. However, there is a lack of rigorous randomized controlled trials to confirm this finding.
This study’s purpose is to evaluate the immediate analgesic efficacy of acupuncture in managing acute postoperative pain following internal fixation of IFF. Through a rigorously designed randomized controlled trial, the results of this study will provide high-quality evidence for the use of acupuncture in the treatment of acute postoperative pain following internal fixation of IFF.
Materials and Methods
Study Design and Setting
The study protocol was designed according to the standard protocol item: Recommendations in the Guidelines for Interventional Trials (Supplemental Material 1) and follows the principles of the Declaration of Helsinki.20 It was approved by the Medical Ethics Committee of Kunming Municipal Hospital of Traditional Chinese Medicine (2024–2025) and registered with the China Clinical Trial Registry (ITMCTR2025000566).
This single-center, randomized controlled clinical trial will be conducted at Kunming Municipal Hospital of Traditional Chinese Medicine. A total of 154 participants with acute postoperative pain following internal fixation of IFF will be randomly allocated to either an acupuncture group or a sham acupuncture group in a 1:1 ratio. All participants will receive a single 10-minute treatment session. The study flow chart is shown in Figure 1. The enrollment, intervention, and assessment schedules are shown in Table 1.
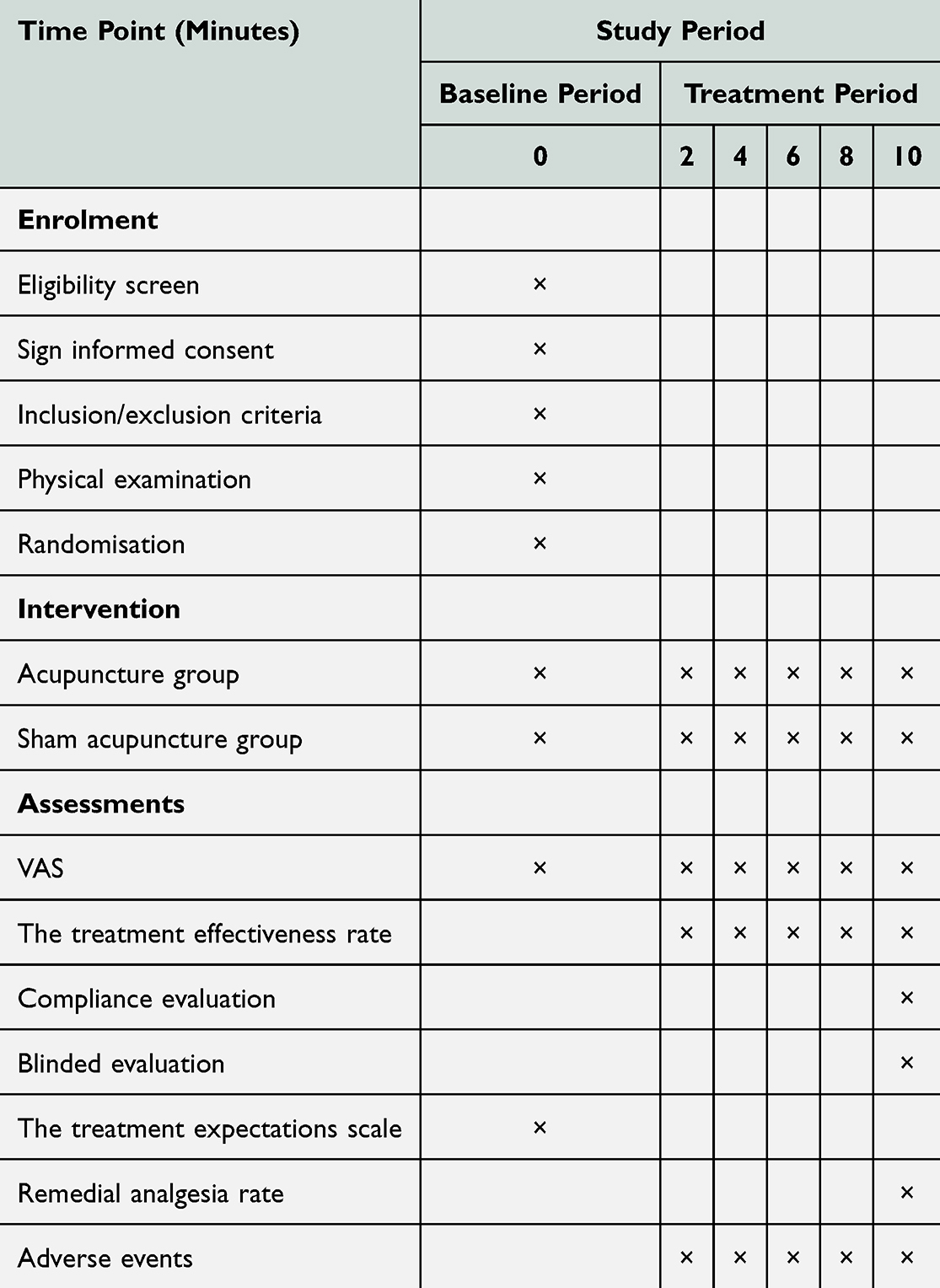 |
Table 1 Study Schedule for Data Measurements |
 |
Table 2 Locations and Manipulations of Acupoints |
 |
Figure 1 Flow diagram. |
Recruitment and Informed Consent
Participant recruitment will be conducted primarily through posters displayed at the Kunming Municipal Hospital of Traditional Chinese Medicine and in the surrounding Kunming community. To ensure accurate diagnosis and eligibility to participate in the study, participants will be diagnosed by a licensed orthopedic surgeon with at least 5 years of clinical experience. Eligible participants must provide written informed consent before randomization into groups. They will have the right to withdraw from the trial at any time without providing any reason.
Inclusion Criteria
Participants who meet all of the following criteria will be included in the analysis:
- Postoperative participants with IFF of internal fixation, male or female.
- Aged between 50 and 75 years;
- Acute pain at the site of application;
- The pain VAS score is between 4 and 9;
- Ability to cooperate actively, complete the clinical study and sign the informed consent form.
Exclusion Criteria
Participants will be excluded from any of the following:
- Participants with multiple fractures or pathologic fractures;
- Combination of serious primary diseases of the cardiovascular, cerebrovascular, hepatic, renal, and hematopoietic systems and other organic diseases, or infections, coagulation disorders, allergies, and skin diseases;
- Participants with comorbid psychiatric disorders such as severe anxiety, depression, insomnia, or intellectual disability who are unable to cooperate with the questionnaire;
- Participants with malignant tumors;
- Participants who have already taken analgesic drugs after surgery;
- Previous history of allergy to opioid analgesics;
- Participants who are intolerant to acupuncture or allergic to acupuncture needles;
- Participants who are participating in other programs.
Removal Criteria
- Participants who did not meet the inclusion criteria and were mistakenly enrolled;
- Participants who were terminated from the trial due to serious adverse events (AEs) or complications and who were inappropriately treated further;
- Participants who chose to withdraw from the study.
Randomisation and Blinding
Participants will be randomly allocated in a 1:1 ratio to either the acupuncture group or the sham acupuncture group. To avoid selection bias, random numbers will be generated by an independent statistician using SPSS V.28.0 (IBM, license code: f56b44b8d8e3562ad8a2), and sealed envelopes will be sequentially numbered from 1 to 154 by the independent investigator in order to hide the group assignment. Participants will be randomly assigned to groups after they have accepted the principle of random assignment. At the end of treatment, both groups will be assessed in a blinded manner. In this trial, participants, researchers, outcome assessors, and statisticians will be blinded. However, due to the specific nature of acupuncture treatment, acupuncturists will not be blinded throughout the study. Blinding can only be revealed in certain situations, such as when the pain does not improve or if it worsens.
Intervention
The interventions in this study have been designed to comply with both the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA). According to Traditional Chinese Medicine (TCM) theory and clinical evidence, the anatomical region of femoral intertrochanteric fractures corresponds to the gallbladder meridian foot Shaoyang. Consequently, two primary acupoints on this meridian have been selected: Yanglingquan (GB34) and Zulinqi (GB41). Meanwhile, to further target the pathological features and local symptoms of the fracture site, we chose to add the Ashi point. Ashi point is an individualized sensitive point, and its selection is based on the actual pain point or pressure point of the patient ‘s fracture area, which can directly stimulate the lesion area and enhance the therapeutic effect of acupuncture on the local lesion. All of the above points were selected for acupuncture with health side. The locations of the acupoints are presented in Table 2 and Figure 2.
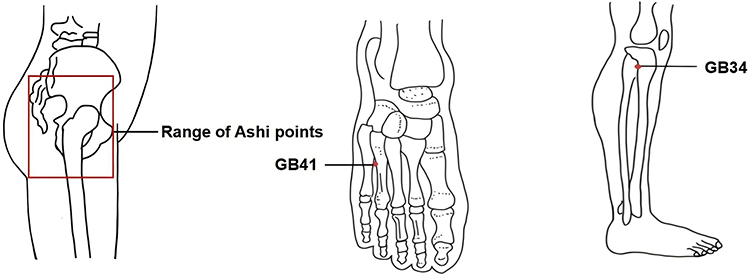 |
Figure 2 Location of acupoint. |
Appliance Selection
Park Sham Acupuncture Device (PSD) (Figure 3): The device includes a transparent catheter (Φ4×20mm), double-sided adhesive tape (Φ1×15mm), and an opaque plastic base. It was manufactured by Suzhou Medical Supplies Factory Ltd, batch number 210401.
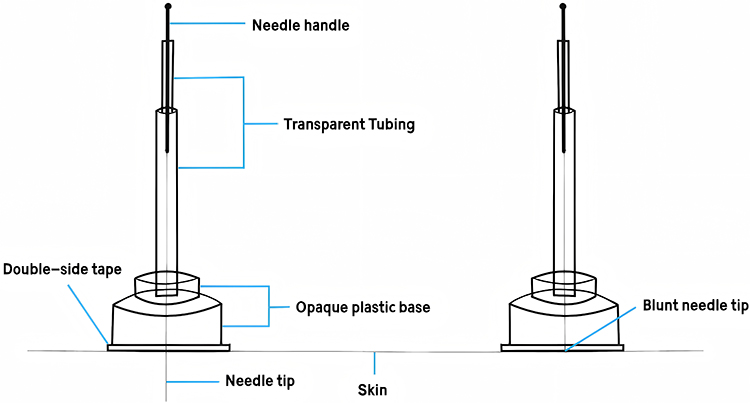 |
Figure 3 Park sham acupuncture device. |
Acupuncture needle (Figure 3): The Huatuo brand disposable acupuncture needles, sized 0.25 mm×40mm and manufactured by Suzhou Medical Supplies Factory, China, will be used. The manufacturer’s licence number is Su Food and Drug Administration of Machinery Production 20010020, and the registration certificate number is 201622770970.
Blunt needle (see Figure 3): Retractable stainless steel blunt needles (0.25×40mm), sourced from Suzhou Medical Supplies Factory, China (lot number 210401), will be used.
Operation
Before the treatment, participants were positioned in a standardized supine position with adequate exposure of the designated acupuncture points. The acupuncturist will disinfect the skin around the acupuncture points. All two groups will use the PSD.
Acupuncture Group
PSD+acupuncture needle will be used. The acupuncturist first sterilized the local skin using a 75% alcohol cotton ball. Subsequently, the adhesive tape on the skin-facing side of the PSD (Placebo Sham Device) was removed, and the needle was inserted into the PSD with its tip exposed. Sterile disposable needles (0.30 mm × 40 mm) were then inserted into the GB41 and GB34 acupoints on the healthy side. The needles were gently rotated and lifted several times to elicit the deqi sensation, a characteristic response in acupuncture indicating effective stimulation. For acupoint Ashi on the healthy side, a sterile disposable needle (0.30mm × 50mm) will be used, and the same method will be used to elicit the deqi response. The depth and angle of the needles are shown in Table 1. Participants in the acupuncture group will receive a single 10-minute session of acupuncture treatment.
Sham Acupuncture Group
PSD+blunt needle will be used. Remove the double-sided tape on the surface of the PSD and introduce a retractable blunt needle. When the tip of the blunt needle touches the skin, the tip will contract back into the hollow handle and will not pierce the skin, but the participant will feel the sensation of being pricked by the needle. The subsequent steps will be the same as in the acupuncture group.
A licensed acupuncturist administered needling procedures of both the acupuncture and sham acupuncture groups with at least 5 years of clinical experience. Before the start of the study, the acupuncturist will receive rigorous training on the location, depth, and angle of needling.
Emergency Treatment
During the study, if a participant’s pain shows no improvement or aggravation, emergency analgesic measures will be administered, including meperidine hydrochloride injection (manufacturer: Qinghai Pharmaceutical Factory Ltd.; Approval Number: H63020021) or other necessary emergency treatment. All treatment details will be meticulously documented in the case report form (CRF).
Outcomes
Primary Outcome
The primary outcome will be the pain VAS score after 10 minutes of treatment.
Secondary Outcomes
Secondary outcomes will include the pain VAS score at other time points (2, 4, 6 and 8 minutes post-treatment), the treatment efficacy rate, blinded assessment, and the treatment effect expectancy scale.
Outcome Measurements
- The VAS is a pain assessment tool that helps measure a participant’s pain level on a 10-centimeter continuum from 0 (no pain) to 10 (severe pain). The higher the VAS score, the more severe the pain.21 The assessment will be conducted six times: at baseline, and 2, 4, 6, 8, and 10 minutes during the treatment process (Supplemental Material 2).
- The treatment efficacy rate was defined as the proportion of participants who exhibited a greater than 50% reduction in pain scores relative to their pre-treatment baseline. The treatment efficacy rate will be evaluated at 2, 4, 6, 8, and 10 minutes during the treatment period.
- The treatment expectations scale will be assessed the participants’ expectations regarding the outcome of the acupuncture treatment. Before the treatment, participants will be required to predict their treatment outcomes by selecting either “effective” or “ineffective” and rate their perception of receiving a positive treatment and the expected outcome on a scale of 0 to 10 (Supplemental Material 3).
- Blinding assessment will be used to assess the validity of the blinding. At the end of the treatment, participants in two groups will be asked whether they believe they received true acupuncture. Additionally, they will be requested to rate their confidence in this belief on an 11-point numerical rating scale ranging from 0 to 10, where 0 indicates “very unsure” and 10 represents “completely sure” (Supplemental Material 4).
- Remedial analgesia rate: At the end of acupuncture treatment, we will calculate the percentage of patients who require additional analgesic medication (Supplementary Material 5).
Sample Size
To our knowledge, no prior experimental studies have directly compared the immediate analgesic effects of acupuncture and sham acupuncture in the context of postoperative pain management following IFF surgery. Therefore, we have referred to a previous study of acupuncture for acute postoperative pain and our own clinical experience to estimate the sample size of this study.22 The change in VAS before and after the treatment of the acupuncture group in the context of postoperative pain management following IFF surgery was 4.7±2.1 and 1.6±1.8 with the sham acupuncture group. We hypothesised that after 10 minutes of treatment, the mean difference in VAS scores before and after treatment was 4.7 points in the acupuncture group and 1.6 points in the sham acupuncture group. Based on an assumed common standard deviation of 2.1, the study was designed to evaluate whether the needling group is superior to the sham group, set α=0.025 (unilateral), β=0.1, Δ=1.2 and K=1. Using the following formula, we calculate the required sample size for both groups:23
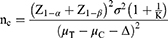
Based on the formula, it is estimated that a minimum of 77 participants will be needed for each group, resulting in 154 participants in total. As only a single treatment session was administered, participant dropout was not considered in the study design.
Statistics
The statistical analyses will be performed using SPSS V.28.0 statistical software (SPSS, Chicago, Illinois, USA). Demographic data analysis will involve independent samples t-tests or Wilcoxon rank sum tests for continuous variables, based on their distribution normality. Significant demographic differences will be incorporated as covariates in efficacy analyses. Categorical variables will be assessed using χ2 or Fisher’s exact tests. Normally distributed continuous variables will be presented as mean ± SD, while non-normally distributed variables will be reported as median (IQR). Adverse event incidence will be compared between groups using χ2 or Fisher’s exact tests. The primary outcome will be evaluated via analysis of covariance, adjusting for baseline pain levels and group allocation. Secondary outcomes, including pain intensity changes at 2, 4, 6, and 8 minutes, will be analyzed using repeated measures ANOVA or Mann–Whitney U-tests, depending on data distribution. Correlations between the pain VAS and the efficacy expectation scores will be examined using Pearson’s or Spearman correlation analyses. All analyses will adhere to the intention-to-treat (ITT) principle, with missing data handled through chained-equation multiple imputation.24
Data Management and Quality Control
Outcome assessors will record initial data in CRFs and promptly enter it into an Excel spreadsheet. Participant identities will be protected, and data collectors will manage, store, and meticulously proofread all data. Investigators will ensure accurate and timely CRF completion, with the research director verifying data authenticity. Personal information will be anonymized to prevent leaks. Data will be securely stored in a locked cabinet for five years post-publication. The Ethics Committee will monitor trial progress, oversee data handling, and make necessary adjustments. The data monitoring committee is independent of the sponsors and has no conflicts of interest. Both acupuncture and sham acupuncture are safe for participants in our trial; therefore, no modifications to the interventions are allowed. Group allocation will be maintained in an Excel file and revealed only after the completion of statistical analysis. Any withdrawals or dropouts will be clearly documented throughout the trial.
AEs Report
During the trial, AEs, including needle fainting, pain, bleeding, hematoma, or infection, may occur. All AEs, whether related to the study or not, must be recorded in CRFs and reported without delay. Affected participants will be provided with timely and adequate care until complete resolution.
Protocol Modification
The study protocol, informed consent form, recruitment materials, and relevant study-related documents have been formally approved by the Medical Ethics Committee of Kunming Municipal Hospital of Traditional Chinese Medicine. The ethical review body will review and approve any subsequent modifications, including changes in study objectives, study design, participant population, sample size, study procedures, etc.
Discussion and Conclusion
Intense pain following internal fixation surgery for IFF is a common complication that severely affects patients’ quality of life.25 As prompt pain management is a critical demand for these patients, the results of this study could provide a simple and rapid-acting treatment for this condition.
Emerging evidence suggests that acupuncture exerts its analgesic effects through a multilevel mechanism involving the stimulation of specific acupoints.26,27 This intervention suppresses spinal glial cell activation (microglia and astrocytes), downregulates pro-inflammatory cytokines (TNF-α, IL-1β), and modulates ascending/descending pain pathways (eg, ACC-PAG-RVM circuitry). These synergistic actions concurrently enhance endogenous opioid signaling while mitigating neuroinflammatory responses, thereby exerting an analgesic effect. Notably, in the acute pain model, significant pain relief can be observed within 10 minutes after acupuncture stimulation.22 Therefore, to quickly reduce pain in participants, a 10-minute intervention period was selected for this study and evaluated every two minutes to more visually assess the immediate analgesic effect of needling.
In clinical practice, pain after internal fixation of IFF is mainly unilateral, so we chose contralateral acupuncture (CAT). CAT, as a traditional acupuncture technique, is meant to work by stimulating healthy side acupuncture points. Modern studies have shown that CAT can directly modulate brain regions, such as the anterior cingulate cortex, to exert its analgesic effects.28 In addition, a growing body of research suggests that CAT is more efficacious when compared to ipsilateral acupuncture.29,30 At the same time, the choice of CAT will not only reduce the risk of postoperative infection after IFF but also avoid the disadvantage of inconveniently selecting acupoints distributed at the surgical site.
To the best of our knowledge, this study is the first high-quality RCT evaluating the efficacy of acupuncture in rapidly relieving postoperative pain after internal fixation of IFF within 10 minutes. In addition, by dynamically assessing VAS scores at multiple time points, this study was able to accurately assess trends in the onset of acupuncture analgesia, identify individual differences, and significantly improve the reliability of the data.31
However, this study has several limitations. First, because of the specific characteristics of the acupuncture operation, the acupuncturist could not be blinded, which may introduce acupuncturist subjective bias. For this reason, we minimized subjective bias by blinding the outcome assessors. Second, this is a single-center study, and its reproducibility needs to be investigated further. Third, the study’s lack of follow-up hindered the assessment of long-term outcomes, which will be addressed in future studies through extended follow-up. Finally, the primary outcome measures in this study rely on subjective indicators without inclusion of objective metrics. Given that pain is inherently a subjective experience that resists objective quantification, patient self-reports remain the gold standard for assessment.
Effective management of acute postoperative pain represents a critical clinical need for participants after internal fixation for IFF. Acupuncture treatment is an effective non-pharmacological therapy, but there is a lack of high-quality research evidence to support it. The findings of this study are expected to provide a simple, rapid, and effective treatment for clinical management.
Abbreviations
IFF, intertrochanteric femoral fracture; VAS, visual Analogue Scale; NSAIDs, nonsteroidal anti-inflammatory drugs; AEs, adverse events; ITT, intention-to-treat; CAT, contralateral acupuncture; CRF, case report form; PSD, Park Sham Acupuncture Device.
Ethics and Dissemination
Ethical approval for this study was obtained from the Medical Ethics Committee of Kunming Municipal Hospital of Traditional Chinese Medicine on 6 December 2024 under the number 2024-015-01. The results of this study will be published in peer-reviewed journals and presented at conferences.
Participant Consent for Publication
Obtained.
Trial Status
The trial is set to initiate recruitment and treatment on 31 March 2025 and is anticipated to be completed by 31 March 2027.
Acknowledgments
We gratefully thank all the collaborating investigators and subjects for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the “Liang Fanrong Expert Workstation” of Yunnan Province-Yunnan Science and Technology Programme (202305AF150072), the Yunnan Ten Thousand Talents Plan Youth Project (YNWR-QNBJ-2019-257).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Attum B, Pilson H. Intertrochanteric femur fracture. StatPearls. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493161/.
2. Gibson-Smith D, Klop C, Elders PJ, et al. The risk of major and any (non-Hip) fragility fracture after hip fracture in the United Kingdom: 2000–2010. Osteoporos Int. 2014;25(11):2555–2563. doi:10.1007/s00198-014-2799-x
3. Li Q, Yang Z, Zhu M, et al. Prevalence and risk factors of osteoporotic fracture among the elderly population in China: a multicenter cross-sectional study. Int Orthop. 2024;48(5):1323–1330. doi:10.1007/s00264-024-06145-0
4. Leer-Salvesen S, Engesæter LB, Dybvik E, Furnes O, Kristensen TB, Gjertsen J-E. Does time from fracture to surgery affect mortality and intraoperative medical complications for hip fracture patients? An observational study of 73 557 patients reported to the Norwegian Hip Fracture Register. Bone Joint J. 2019;101-B(9):1129–1137. doi:10.1302/0301-620X.101B9.BJJ-2019-0295.R1
5. Adeyemi A, Delhougne G. Incidence and economic burden of intertrochanteric fracture: a medicare claims database analysis. JB JS Open Access. 2019;4(1):e0045. doi:10.2106/JBJS.OA.18.00045
6. Nazrun AS, Tzar MN, Mokhtar SA, Mohamed IN. A systematic review of the outcomes of osteoporotic fracture patients after hospital discharge: morbidity, subsequent fractures, and mortality. Ther Clin Risk Manag. 2014;10:937–948. doi:10.2147/TCRM.S72456
7. Xu BY, Yan S, Low LL, Vasanwala FF, Low SG. Predictors of poor functional outcomes and mortality in patients with hip fracture: a systematic review. BMC Musculoskelet Disord. 2019;20(1):568. doi:10.1186/s12891-019-2950-0
8. Kaplan K, Miyamoto R, Levine BR, Egol KA, Zuckerman JD. Surgical management of hip fractures: an evidence-based review of the literature. II: intertrochanteric fractures. J Am Acad Orthop Surg. 2008;16(11):665–673. doi:10.5435/00124635-200811000-00007
9. Hongku N, Woratanarat P, Nitiwarangkul L, Rattanasiri S, Thakkinstian A. Fracture fixation versus hemiarthroplasty for unstable intertrochanteric fractures in elderly patients: a systematic review and network meta-analysis of randomized controlled trials. Orthop Traumatol Surg Res. 2022;108(1):102838. doi:10.1016/j.otsr.2021.102838
10. Ding K, Zhu Y, Li Y, et al. Triangular support intramedullary nail: a new internal fixation innovation for treating intertrochanteric fracture and its finite element analysis. Injury. 2022;53(6):1796–1804. doi:10.1016/j.injury.2022.03.032
11. Pommier W, Minoc EM, Morice PM, et al. NSAIDs for pain control during the peri-operative period of hip fracture surgery: a systematic review. Drugs Aging. 2024;41(2):125–139. doi:10.1007/s40266-023-01074-w
12. Hatano M, Sasabuchi Y, Ishikura H, et al. Outcomes after hip fracture surgery in patients receiving non-steroidal anti-inflammatory drugs alone, acetaminophen alone, or both. Bone Joint J. 2024;106-B(8):849–857. doi:10.1302/0301-620X.106B8.BJJ-2024-0183.R1
13. Fine M. Quantifying the impact of NSAID-associated adverse events. Am J Manag Care. 2013;19(14 Suppl):s267–72.
14. Desjardins PJ, Mehlisch DR, Chang DJ, et al. The time to onset and overall analgesic efficacy of rofecoxib 50 mg: a meta-analysis of 13 randomized clinical trials. Clin J Pain. 2005;21(3):241–250. doi:10.1097/00002508-200505000-00007
15. Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821–847. doi:10.18433/j3vw2f
16. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: a current perspective. Biochem Pharmacol. 2020;180:114147. doi:10.1016/j.bcp.2020.114147
17. Eucker SA, Glass O, Knisely MR, et al. An adaptive pragmatic randomized controlled trial of emergency department acupuncture for acute musculoskeletal pain management. Ann Emerg Med. 2024;84(4):337–350. doi:10.1016/j.annemergmed.2024.03.014
18. Cao Y, Qu Z, Zhang S, et al. Early acupuncture intervention for pain relief in emergency department patients with suspected acute renal colic caused by urinary calculi: a randomized clinical trial. QJM. 2025:hcaf011. Doi:10.1093/qjmed/hcaf011
19. Lin H, Wang X, Feng Y, et al. Acupuncture versus oral medications for acute/subacute non-specific low back pain: a systematic review and meta-analysis. Curr Pain Headache Rep. 2024;28(6):489–500. doi:10.1007/s11916-023-01201-7
20. Chan A-W, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346(jan08 15):e7586. doi:10.1136/bmj.e7586
21. Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths and clinical relevance. Scand J Pain. 2016;13:67–75. doi:10.1016/j.sjpain.2016.06.012
22. Tu JF, Cao Y, Wang LQ, et al. Effect of adjunctive acupuncture on pain relief among emergency department patients with acute renal colic due to urolithiasis: a randomized clinical trial. JAMA Network Open. 2022;5(8):e2225735. doi:10.1001/jamanetworkopen.2022.25735
23. Hu J, Li B, Zhang HN, Liu WH, Feng S. Sample size estimation in acupuncture and moxibustion clinical trials. Zhongguo Zhen Jiu. 2021;41(10):1147–1152. doi:10.13703/j.0255-2930.20201020-0002 Chinese.
24. Azur MJ, Stuart EA, Frangakis C, Leaf PJ. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res. 2011;20(1):40–49. doi:10.1002/mpr.329
25. Morrison J, Morrison M. Management of hip fractures. Crit Care Nurs Clin North Am. 2024;36(4):575–584. doi:10.1016/j.cnc.2024.04.007
26. Chen T, Zhang WW, Chu YX, Wang YQ. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(4):793–811. doi:10.1142/S0192415X20500408
27. Wu Q, Yue J, Lin L, et al. Electroacupuncture may alleviate neuropathic pain via suppressing P2X7R expression. Mol Pain. 2021;17:1744806921997654. doi:10.1177/1744806921997654
28. Yan CQ, Huo JW, Wang X, et al. Different degree centrality changes in the brain after acupuncture on contralateral or ipsilateral acupoint in patients with chronic shoulder pain: a resting-state fMRI study. Neural Plast. 2020;2020:5701042. doi:10.1155/2020/5701042
29. Zhang H, Sun J, Xin X, Huo Z, Li D. Contralateral electroacupuncture relieves chronic neuropathic pain in rats with spared nerve injury. Med Sci Monit. 2018;24:2970–2974. doi:10.12659/MSM.909741
30. Li Y, Zhang Z, Chen Y, et al. Clinical efficacy on peripheral facial paralysis at acute stage treated with opposing needling technique. Zhongguo Zhen Jiu. 2015;35(01):7–10. doi:10.13703/j.0255-2930.2015.01.002
31. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Pain and Function in Patients with Nonspecific Low Back Pain: Study Protocol for an Up-to-Date Systematic Review and Meta-Analysis
Li Y, Liu Y, Zhang L, Zhai M, Li L, Yuan S, Li Y
Journal of Pain Research 2022, 15:1379-1387
Published Date: 10 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Effectiveness of Pharmacopuncture in Patients with Lumbar Spinal Stenosis: A Protocol for a Multi-Centered, Pragmatic, Randomized, Controlled, Parallel Group Study
Lee JY, Park KS, Kim S, Seo JY, Cho HW, Nam D, Park Y, Kim EJ, Lee YJ, Ha IH
Journal of Pain Research 2022, 15:2989-2996
Published Date: 23 September 2022
Central Mechanism of Acupuncture Treatment in Patients with Migraine: Study Protocol for Randomized Controlled Neuroimaging Trial
Jia J, Yan C, Zheng X, Shi A, Li Z, Xu L, Hui Z, Chen Y, Cao Z, Wang J
Journal of Pain Research 2023, 16:129-140
Published Date: 18 January 2023
The Opioid-Sparing Effect of Acupuncture After Abdominal Surgery: A Systematic Review and Meta-Analysis Protocol
Joo C, Kim KH, Jang BH, Huang CW, Kang JW, Lee JD, Lee S, Lee S
Journal of Pain Research 2023, 16:1095-1101
Published Date: 29 March 2023