Back to Journals » Patient Preference and Adherence » Volume 19
Illness Perception, Health Literacy, and Medication Adherence in Hypertensive Patients and Their Spouses: An Actor-Partner Interdependence Mediation Model Approach
Authors Han R ![]() , Wu C, Qu GS
, Wu C, Qu GS ![]() , Chen YC, Zeng XW, Xue QH
, Chen YC, Zeng XW, Xue QH
Received 30 June 2025
Accepted for publication 4 November 2025
Published 15 November 2025 Volume 2025:19 Pages 3647—3656
DOI https://doi.org/10.2147/PPA.S547453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Rui Han,* Chan Wu,* Guang-Su Qu, Ying-Chun Chen, Xiu-Wen Zeng, Qiu-Hua Xue
Department of Cardiovascular Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiu-Hua Xue, Department of Cardiovascular Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China, Email [email protected]
Objective: This study aims to investigate the mediating role of health literacy—both in hypertensive patients and their spouses —on the relationship between illness perception and medication adherence, based on the Actor-Partner Interdependence Mediation Model (APIMeM).
Methods: Hypertensive patients and their spouses from a selected region were recruited through convenience sampling between August 2024 and March 2025. Data were collected using the General Information Questionnaire, Brief Illness Perception Questionnaire, Health Literacy Scale for Chronic Disease Patients, Morisky Medication Adherence Scale, and the Caregiver Self-care Contribution Scale.
Results: (1) Regarding the actor effects, patients’ health literacy partially mediated the relationship between their illness perception and medication adherence (effect size: 0.028, 95% CI: 0.007~0.067, P < 0.05). Similarly, spouses’ health literacy partially mediated the effect of their own illness perception on their medication adherence (effect size: 0.240, 95% CI: 0.165~0.324, P < 0.05). (2) For the partner effects, patients’ health literacy partially mediated the relationship between their spouse’s illness perception and the patient’s medication adherence (effect size: 0.042, 95% CI: 0.018~0.084, P < 0.05). Meanwhile, the spouse’s health literacy fully mediated the effect of the patient’s illness perception on the spouse’s medication adherence (effect size: 0.139, 95% CI: 0.020~0.302, P < 0.05).
Conclusion: A bidirectional actor-partner effect exists between illness perception and medication adherence among hypertensive patients and their spouses. Health literacy plays a significant mediating role in these relationships. These findings suggest that clinical interventions should target both patients and their spouses simultaneously, enhancing health literacy, strengthening disease knowledge, improving illness perception, and thereby promoting better medication adherence.
Keywords: high blood pressure, health literacy, illness perception, medication adherence, actor-partner interdependence model, mediation model
Introduction
Hypertension is one of the most prevalent and preventable causes of mortality worldwide. According to the Global Report on Hypertension 2023, approximately 1.42 billion individuals are currently affected globally, with projections indicating a rise to 1.56 billion1 by 2030. In China, the adult prevalence exceeds 25.2% among individuals aged 18 and above, and rises to over 50% in those older than 60. Prevalence is notably higher in northern regions than in the south, with a narrowing gap between urban and rural areas. Major risk factors include high dietary salt intake—about twice the WHO recommended level—abdominal obesity (over 30%), sedentary behavior, smoking, and aging, which increases risk fivefold in individuals over 65 years old.2,3 Hypertension significantly elevates the risk of cardiovascular diseases, such as stroke and myocardial infarction, as well as kidney and retinal complications.4 Globally, hypertension-related diseases are responsible for around 10 million deaths annually, and in China, over 40% of cardiovascular and cerebrovascular fatalities are directly attributed to hypertension.5,6 Current prevention and management strategies emphasize early detection, lifestyle modification (eg, salt reduction, weight control, smoking cessation), and adherence to standardized pharmacologic regimens. However, medication adherence rates remain suboptimal globally—below 50%7,8—and improving adherence among hypertensive patients is an urgent clinical challenge.
Mueller et al9 found that individuals with higher health literacy were better able to comprehend medication instructions, resulting in improved adherence. Illness perception refers to a patient’s subjective understanding of their disease, shaped by personal knowledge and experiences. According to Chen et al,10 a stronger perception of illness severity correlates with heightened risk awareness and increased motivation for self-management, which in turn enhances adherence to prescribed medications. Moreover, health literacy may mediate this relationship, as patients’ comprehension of their illness influences their capacity to seek, understand, and apply health information effectively. Kenny’s Actor–Partner Interdependence Mediation Model (APIM), developed in 1999,11 emphasizes the interdependent nature of dyadic relationships—particularly among close pairs such as spouses—and their influence on emotional, cognitive, and behavioral health outcomes. APIM allows simultaneous examination of an individual’s influence on their own outcomes (actor effect) and their influence on their partner’s outcomes (partner effect), as illustrated in Figure 1.12
Traditional hypertension research has predominantly focused on the individual level, employing univariate statistical methods that often overlook the close interactions and emotional bonds between patients and their caregivers (such as spouses). This non-independence of data frequently leads to statistical biases and limitations in conclusions. The introduction of the Actor-Partner Interdependence Model (APIM) effectively addresses this gap. Its core lies in simultaneously estimating both the “actor effect” (the influence of an individual’s own variables on their own outcomes) and the “partner effect” (the influence of an individual’s variables on their partner’s outcomes), thereby revealing bidirectional interaction pathways within dyadic relationships.
In hypertension management, medication adherence, emotion regulation, and illness perception in patients and their spouses are often intertwined. For instance, a patient’s depressive mood may increase the caregiver burden on the spouse, while supportive behaviors from the spouse can, in turn, influence the patient’s blood pressure control outcomes and treatment adherence. APIM provides a rigorous framework for analyzing such dyadic interactions. It is particularly suited for exploring shared management mechanisms within couples or patient-caregiver dyads, thus promoting a theoretical expansion in hypertension research from an individual-oriented to a relationship-oriented perspective. Furthermore, it lays the groundwork for developing intervention strategies targeted at the dyad as a whole.
Given the mutual influence of patients and spouses on each other’s health literacy and illness perception, these dynamics may jointly affect medication adherence. Therefore, this study employs an extended APIMeM framework to explore the interactive relationships among illness perception, health literacy, and medication adherence in patient-spouse dyads. The objective is to clarify the mediating pathways and provide a scientific basis for dyadic interventions aimed at improving treatment adherence in hypertensive populations.
Subjects and Methods
Subjects
From August 2024 to March 2025, hypertensive patients and their spouses were recruited via convenience sampling from a designated district.
Inclusion criteria for patients were: (1) clinically diagnosed with hypertension; (2) currently married with a living spouse; (3) aged between 18 and 85 years; (4) capable of basic comprehension and communication; (5) provided informed consent and voluntarily participated in the study.
Exclusion criteria for patients were: (1) a history of psychiatric disorders; (2) severe comorbidities or critical illnesses, such as heart failure, respiratory failure, or malignancies.
Inclusion criteria for spouses were: (1) aged 18–85 years; (2) primary caregiver of the hypertensive patient; (3) mentally alert and able to complete the questionnaire independently; (4) provided informed consent and voluntarily participated.
Exclusion criteria for spouses included the presence of serious physical or mental illness.
Based on the actor-partner interdependence model (APIM), with an expected actor and partner effect size of 0.25, α = 0.05, and 1-β = 0.9, the minimum required sample size was 171 dyads.13 Structural equation modeling (SEM), however, requires at least 200 cases. Considering these factors and accounting for a 10% attrition rate, the target sample size was set at 223 dyads. Ultimately, 274 hypertensive patient-caregiver pairs were surveyed, and 256 valid and complete questionnaire sets were recovered, yielding a response rate of 93.43%.
This study was finally approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (No:2024–070025).
Survey Tools
(1) General Information Questionnaire
Designed by the research team, this questionnaire collected demographic and clinical data, including age, gender, education level, living arrangements, income, duration of hypertension, medication type, and number of comorbidities for patients. Spouse-related data such as age, gender, education, and economic status were also collected.
(2) Brief Illness Perception Questionnaire (BIPQ)
Originally developed by Broadbent et al.,14 the Chinese version of the BIPQ was used to assess illness perception in both patients and spouses. The scale comprises three dimensions: cognitive (5 items), emotional (2 items), and illness understanding (4 items), along with four open-ended items on perceived etiology. Items were rated on an 11-point Likert scale (0–10), with items 3, 4, and 7 reverse-scored. The total score ranges from 0 to 80, with higher scores indicating stronger illness perception. Cronbach’s α coefficients in this study were 0.810 (patients) and 0.833 (spouses).
(3) Health Literacy Management Scale (HeLMS) for Chronic Disease Patients
Developed by Jordan et al.,15 and adapted into Chinese by Sun Haolin et al, this instrument evaluates the health literacy of chronic disease patients. It contains 24 items across four dimensions: information acquisition (9 items), communication ability (9 items), health improvement willingness (4 items), and financial support willingness (2 items). Items are rated on a 5-point Likert scale from “very difficult” (1) to “not difficult at all” (5), with total scores ranging from 24 to 120. Scores ≤72 indicate severely limited health literacy; 73–95 suggest limited literacy, and ≥96 indicate adequate literacy. The tool was also adapted to assess spouses’ health literacy. Cronbach’s α was 0.891 for patients and 0.856 for spouses.
(4) Chinese Medication Adherence Scale (CMAS)
Translated into Chinese by Si Zaixia et al,16 this 8-item scale evaluates medication adherence. Items 1–4 and 6–7 are scored 1 point for “No” and 0 for “Yes.” Item 5 is reverse-scored. Item 8 uses a 5-point Likert scale, scoring from 0 to 1. Total scores range from 0 to 8, with scores ≤6 considered poor adherence and >6 considered good. The Cronbach’s α coefficient in this study was 0.814.
(5) Caregiver Contribution to Self-Care of Chronic Illness Inventory (CC-SC-CII)
Developed by Vellone et al17 and translated into Chinese by Chen et al in 2021, this scale assesses caregivers’ contributions to patients’ self-care. It includes three dimensions: self-care maintenance, monitoring, and management, totaling 19 items. Each dimension is scored on a 0–100 scale, with scores >70 indicating adequate caregiver involvement. The Cronbach’s α coefficient in this study was 0.860.
Data Collection Methods
All questionnaires were administered by trained research personnel. Before distribution, participants were briefed on the study objectives and procedures and signed informed consent forms. Patients and their spouses completed the questionnaires independently in separate rooms. Completed forms were collected immediately and checked for completeness. In cases where participants had difficulties understanding or completing the questionnaires, trained investigators provided one-on-one verbal guidance and recorded responses accurately based on participant input.
Statistical Methods
Data analysis was conducted using SPSS 27.0. Continuous variables conforming to normal distribution were expressed as mean ± standard deviation, while categorical data were presented as frequencies and percentages. Harman’s single-factor test was employed to assess common method bias. Pearson correlation analysis was used to evaluate variable relationships. The APIMeM model was constructed using AMOS 29.0 with maximum likelihood estimation for model fitting. The bootstrap method was applied to test the significance of mediation effects. A two-tailed P-value <0.05 was considered statistically significant.
Results
General Information of Respondents
A total of valid questionnaires were collected in this study, and the basic information at admission is shown in Table 1.
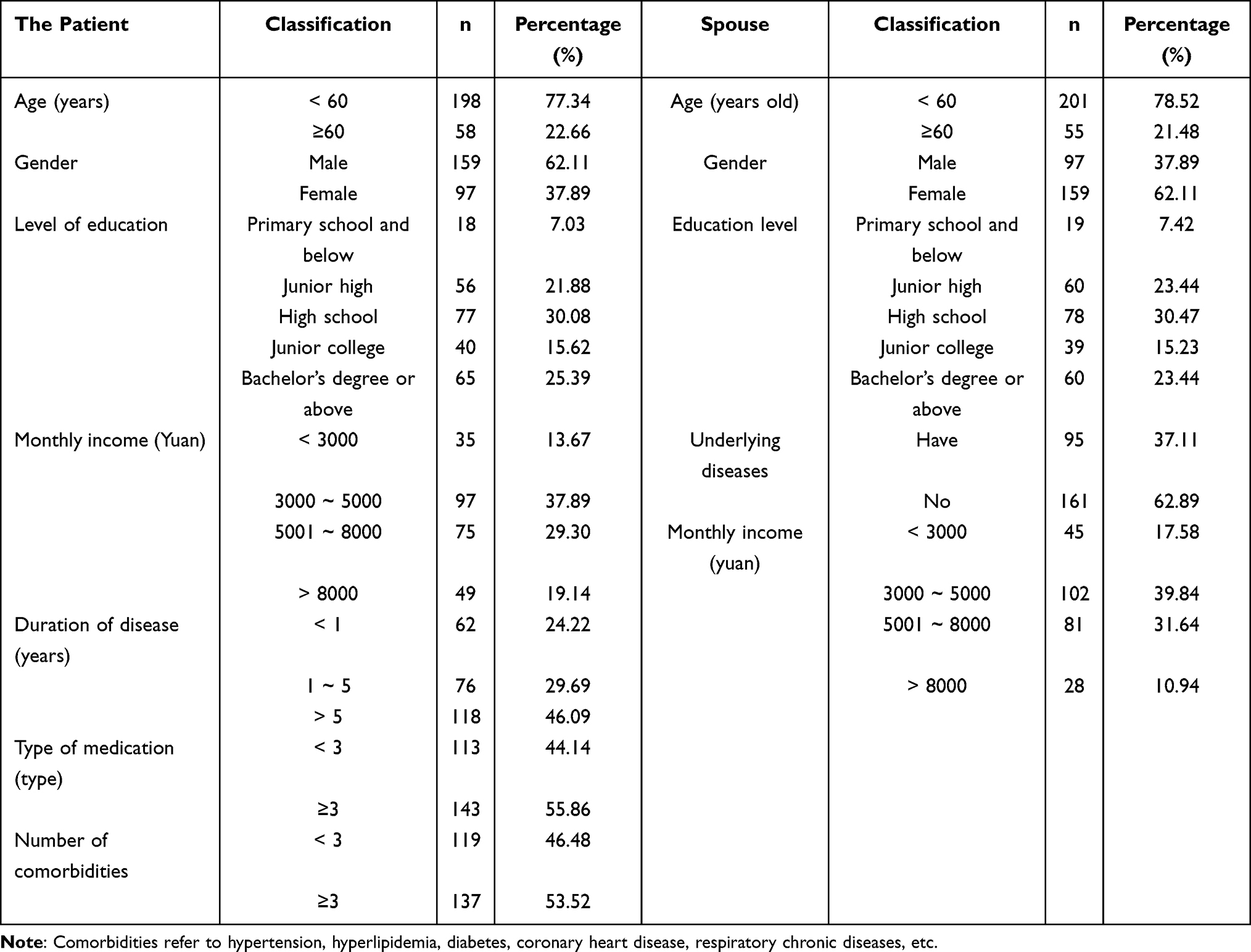 |
Table 1 General Information of the Subjects (n = 256) |
Common Method Bias Test
The results showed that there were 22 factors had eigenvalues greater than 1, with the first factor accounting for 22.32% of the variance. For spouses, 19 factors had eigenvalues greater than 1, with the first factor explaining 26.79% of the variance. As both values were below the critical threshold of 40% there was no significant evidence of common method bias in this study,18 indicating that there was no serious common method bias in this study.
Scores and Correlation Analysis of Illness Perception, Health Literacy, and Medication Adherence in Hypertensive Patients and Their Spouses
The descriptive statistics and correlation analyses of illness perception, health literacy, and medication adherence are presented in Table 2. All correlations were statistically significant (P < 0.05), suggesting meaningful associations among the variables for both patients and spouses. The scores of each scale are shown in Table 2, and the correlation was significant (P < 0.05).
 |
Table 2 Scores and Correlation Analysis of Health Literacy in Illness Perception and Medication Adherence of Hypertension Patients and Their Spouses (r Value, n = 256) |
Host-Object Interdependence Mediating Model Analysis of Illness Perception, Health Literacy and Medication Adherence of Hypertension and Their Spouses
In this study, illness perception was used as the independent variable, health literacy as the mediating variable, and medication adherence as the dependent variable to construct a mediation model of subject-object interdependence. Model fitting results showed and excellent fit with a saturated model (χ2 (15) = 916.89, P < 0.001), CFI, GFI and NFI were all 1, RMSEA < 0.001. The model is shown in Figure 1. Bootstrap repeated sampling 5000 times was used to estimate the 95% confidence interval to test the mediating role of health literacy between illness perception and medication adherence. If the confidence interval did not include 0, the mediating effect was established. Regarding the actor effects, patients’ health literacy partially mediated the relationship between their illness perception and medication adherence (effect size: 0.028, 95% CI: 0.007~0.067, P < 0.05). Similarly, spouses’ health literacy partially mediated the effect of their own illness perception on their medication adherence (effect size: 0.240, 95% CI: 0.165~0.324, P < 0.05). (2) For the partner effects, patients’ health literacy partially mediated the relationship between their spouse’s illness perception and the patient’s medication adherence (effect size: 0.042, 95% CI: 0.018~0.084, P < 0.05). Meanwhile, the spouse’s health literacy fully mediated the effect of the patient’s illness perception on the spouse’s medication adherence (effect size: 0.139, 95% CI: 0.020~0.302, P < 0.05). The results of the mediation effect test are shown in Table 3 and Figure 2.
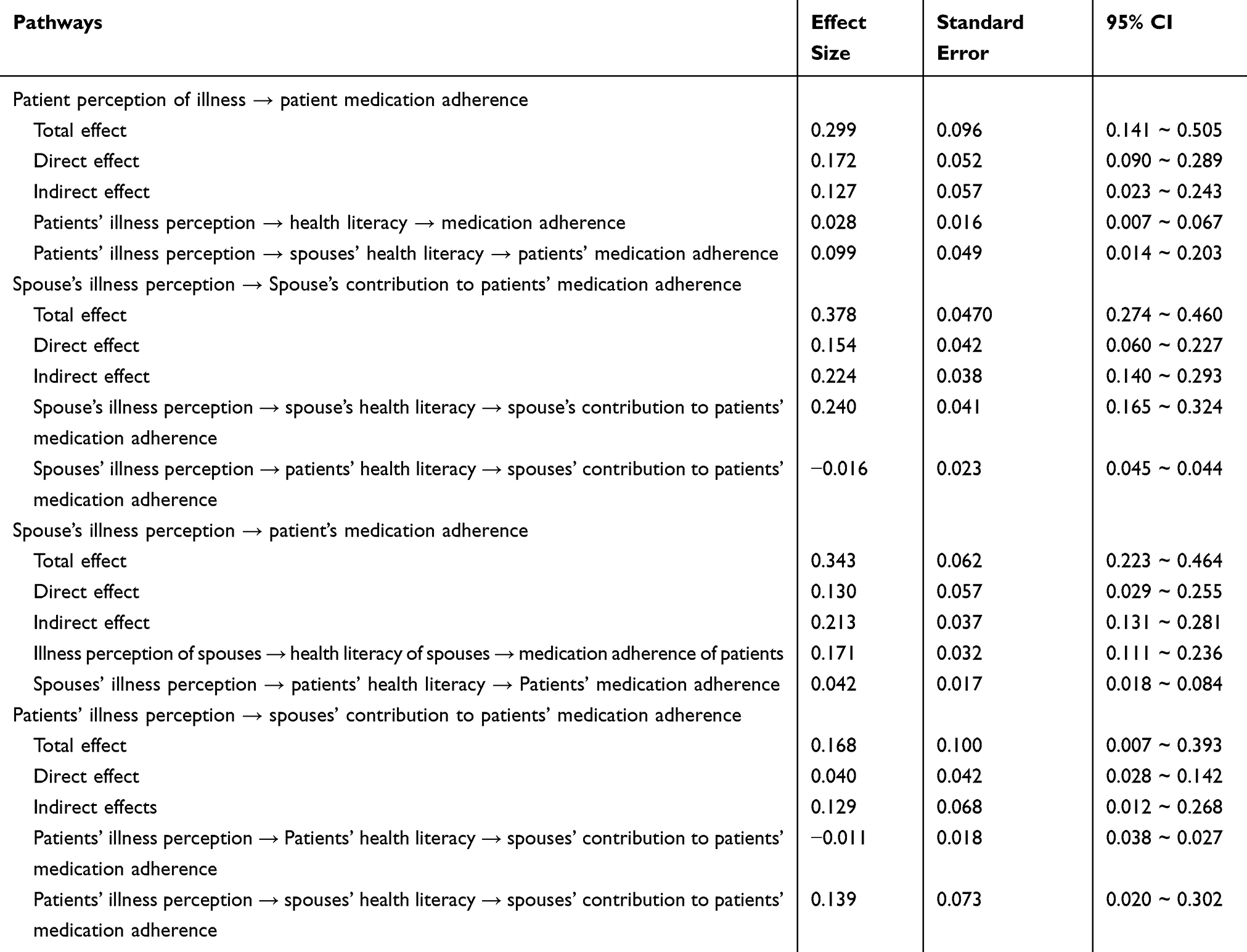 |
Table 3 Mediating Effect Size Analysis of Health Literacy on Illness Perception and Medication Adherence (n = 256) |
 |
Figure 1 Standard model diagram. Notes: C1, Y1 and Y2 are the dependent variables, E1 and E2 are the residuals, Y1 and Y2 are the parts of Y1 and Y2 that are not explained by X1 and X2, respectively. C2 is the correlation between them, which accounts for other factors related to the relationship between the couple. a1 and a2 are the subject effect. P12 and P21 is object effect. |
 |
Figure 2 Path analysis model diagram of illness perception, medication adherence and health literacy of hypertensive patients and their spouses. Note: Dashed line indicates path coefficient P > 0.05; Solid lines indicate path coefficient P < 0.05. |
Discussion
The findings of this study reveal that both hypertensive patients and their spouses exhibit moderate levels of illness perception, consistent19,20 with previous studies. However, health literacy levels in both groups were relatively low, lower than those reported by Lor et21 al. Medication adherence among patients was also suboptimal. This may be attributed to the adaptive cognitive mechanisms commonly found in chronic disease contexts. Over time, patients and their spouses may develop a “cognitive equilibrium”—recognizing the potential risks of hypertension while maintaining a controlled sense of threat through limited behavioral adjustments. While this adaptation may mitigate anxiety, it can also result in superficial health knowledge. Many patients, for instance, are aware of the importance of “taking medicine on time” but lack deeper understanding of the underlying pathophysiology (eg, endothelial damage) or personal risk factors (eg, genetic predisposition), ultimately leading to insufficient health literacy. Additional contributors include limited personalized communication from healthcare providers, minimal behavioral guidance, and the spouses’ reliance on informal, non-professional information sources. These factors reinforce cognitive limitations and hinder effective disease management. Medication adherence suffers not only from low health literacy but also from conflicting illness perceptions—ranging from fear-induced hypervigilance to complacency due to underestimation of risk. Passive spousal support and underutilization of community resources (eg, health lectures) further exacerbate poor adherence outcomes.22,23
Given these insights, clinical interventions should be designed to address both patients and their spouses. Tailored educational programs targeting disease mechanisms and complications should be offered to patients, while training to enhance support capabilities can be provided to spouses. Family-based management strategies—such as joint diet planning—should be encouraged, and medical communication tools (eg, visual aids, local dialects) can be utilized to improve comprehension. Integrating community resources, such as regular skill-based training at primary care centers, may help compensate for low health literacy. Moreover, dynamic assessments of illness perception (eg, using motivational interviewing to correct distorted beliefs) and coordinated family support strategies may improve overall medication adherence by aligning cognitive, behavioral, and environmental factors. The positive correlations observed among illness perception, health literacy, and medication adherence between patients and their spouses (P < 0.05) may reflect shared cognitive environments and behavioral reinforcement within the household. Spouses often have similar exposures to health information and may influence each other’s disease understanding and communication efficacy. Furthermore, spousal support contributes directly to medication adherence, while high adherence by one partner may reinforce the other’s confidence in disease management through reciprocal feedback.24 These findings suggest that incorporating spouses into chronic disease management programs—through family-based education, skills training, and collaborative goal-setting—may significantly enhance treatment outcomes and long-term adherence.
In this study, the illness perception and health literacy of patients and their spouses positively affect the medication adherence of patients. The actor-effect analysis revealed that the patient’s health literacy played a partial mediating role between their illness perception and medication adherence (effect value 0.028, P < 0.05), indicating that illness perception influences medication-taking behavior through the mediating mechanism of health literacy. However, the relatively weak pathway effect suggests certain limitations in the transformation from individual cognition to behavior. In contrast, the spouse’s health literacy also exhibited a partial mediating effect between their own illness perception and the patient’s medication adherence (effect value 0.240, P < 0.05), with a significantly stronger effect size than that of the patient. This reflects that spouses more effectively promote patient adherence through means such as proactively learning about the disease, providing behavioral modeling, or offering emotional support. This implies that spouses who perceive the illness as serious may be more likely to acquire caregiving knowledge and, through behavioral modeling or emotional encouragement, indirectly enhance the patient’s adherence. As previous literature suggests,25 this stronger mediating effect emphasizes that the spouse’s health literacy functions as a critical link between illness perception and medication adherence. In many cases, the spouse assumes an active role as a “co-manager” in the family’s health-related decision-making. Thus, any improvement in their health literacy has a direct, measurable impact on the patient’s adherence behavior. In contrast, the relatively weak mediating role of the patient’s own health literacy reflects the limitations individuals may face in applying health knowledge to self-management. The dominant influence of the spouse’s literacy underscores the importance of a robust familial support structure in chronic disease care.
From a clinical perspective, interventions should simultaneously aim to strengthen the patient’s cognitive understanding of hypertension and build the spouse’s practical caregiving competencies—such as medication tracking and health coaching—to improve household-level disease management. In terms of partner (object) effects, two key findings emerged: First, the patient’s health literacy partially mediated the influence of the spouse’s illness perception on the patient’s medication adherence (effect value = 0.042, P < 0.05). This implies that a spouse’s heightened illness awareness may indirectly promote the patient’s adherence through an improvement in the patient’s health literacy, although the direct partner effect remains more prominent. Second, the spouse’s health literacy completely mediated the effect of the patient’s illness perception on the spouse’s own medication adherence (effect value = 0.139, P < 0.05). This finding further reinforces the pivotal role of the spouse’s health literacy as the central pathway connecting the patient’s disease awareness to the spouse’s adherence behavior. The limited mediating effect of patient literacy again highlights the constraint of individual knowledge translation, while the significant role of spousal literacy points to the proactive caregiving role spouses often play. This underlines the need for clinical practices to actively enhance the caregiving skills of spouses, especially in medication support, to optimize intervention outcomes.
Furthermore, spousal health literacy plays a partial mediating role between the patient’s illness perception and medication adherence (effect value: 0.099, 95% CI: 0.014–0.203, P < 0.05), as well as between the spouse’s own illness perception and the patient’s medication adherence (effect value: 0.171, 95% CI: 0.111–0.236, P < 0.05). This indicates that spousal health literacy acts as a crucial bridge linking the patient’s perception of illness to their medication-taking behavior. When spouses possess higher health literacy—that is, the ability to access, comprehend, and apply health information to make appropriate decisions—they can more accurately understand the patient’s condition and treatment regimen. Consequently, they are better equipped to provide effective emotional support, medication reminders, and daily supervision, thereby helping the patient develop a more accurate perception of the illness and improve medication-taking behavior. Simultaneously, the spouse’s own perception of the illness also influences their motivation and approach to participating in the patient’s health management. High health literacy enables them to more scientifically translate this awareness into concrete supportive actions, which positively affects the patient’s adherence. This underscores the importance of enhancing spousal health literacy in chronic disease management to optimize overall family health behaviors and treatment outcomes.
Summary
This study employed the Actor–Partner Interdependence Mediation Model (APIMeM) to examine the mediating role of health literacy in the relationship between illness perception and medication adherence from a dyadic (patient–spouse) perspective. The findings confirmed that health literacy serves as a significant mediator between illness perception and medication adherence in both actors and partners. Clinical practice requires the development of intervention strategies from a dyadic synergy perspective: The primary focus is strengthening the spouse’s role as a “collaborator” through training in medication management, blood pressure monitoring, and emotional support skills, translating their health literacy into practical supportive actions. Concurrently, patient self-management should be optimized with personalized medication guidance (eg, simplifying regimens, combination therapies) and health literacy education to address limitations in their cognition-behavior transformation. Finally, a family support system must be constructed by establishing long-term follow-up mechanisms that include spouses, utilizing digital tools for health data sharing, ultimately maximizing the effectiveness of patient-spouse collaborative management. However, this study employed a convenience sampling method, which may limit the generalizability of the findings. Additionally, the use of patient-reported outcomes may increase the risk of reporting bias. Finally, due to the limitations inherent in the cross-sectional design, it is not possible to dynamically observe change trajectories or longitudinal effects. Future research could involve multi-center, large-sample longitudinal studies to further explore the interactive effects among these three factors.
Ethics Statement
This study was finally approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (No:2024-070025). Informed consent was obtained from all patients in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dzau VJ, Hodgkinson CP. Precision Hypertension. Hypertension. 2024;81(4):702–708. doi:10.1161/HYPERTENSIONAHA.123.21710
2. Zhang M, Shi Y, Zhou B, et al. Prevalence, awareness, treatment, and control of hypertension in China, 2004-18: findings from six rounds of a national survey. BMJ. 2023;380:e71952.
3. Zhao Y, Zhang H, Liu X, et al. The prevalence of cardiometabolic multimorbidity and its associations with health outcomes among women in China. Front Cardiovasc Med. 2023;10:922932. doi:10.3389/fcvm.2023.922932
4. Franco C, Sciatti E, Favero G, et al. Essential hypertension and oxidative stress: novel future perspectives. Int J Mol Sci. 2022;23(22):14489. doi:10.3390/ijms232214489
5. Hu Y, Wang Z, He H, et al. Prevalence and patterns of multimorbidity in China during 2002-2022: a systematic review and meta-analysis. Ageing Res Rev. 2024;93:102165. doi:10.1016/j.arr.2023.102165
6. Guo C, Liu Z, Fan H, et al. Associations of healthy lifestyle and three latent socioeconomic status patterns with physical multimorbidity among middle-aged and older adults in China. Prev Med. 2023;175:107693. doi:10.1016/j.ypmed.2023.107693
7. Gavrilova A, Bandere D, Rutkovska I, et al. Knowledge about disease, medication therapy, and related medication adherence levels among patients with hypertension. Medicina. 2019;55(11):715. doi:10.3390/medicina55110715
8. Yang Y, R LI. The application value of internet health popularization for community patients with hypertension. Altern Ther Health Med. 2024;30(7):34–39.
9. Mueller CM, Ward L, O’keefe G. Health literacy, medication adherence, and quality of life in patients with uveitis. Ocul Immunol Inflamm. 2022;30(5):1060–1067. doi:10.1080/09273948.2020.1861304
10. Chen YL, Xie YQ, Wei MY, et al. Clinical effects of detailed nursing management interventions on medication adherence and disease perception in patients with drug-resistant tuberculosis. World J Clin Cases. 2024;12(20):4191–4198. doi:10.12998/wjcc.v12.i20.4191
11. Kenny DA, Ledermann T. Detecting, measuring, and testing dyadic patterns in the actor-partner interdependence model. J Fam Psychol. 2010;24(3):359–366. doi:10.1037/a0019651
12. Wang H, Yue H, Ren M, et al. Dyadic effects of family-functioning and resilience on quality of life in advanced lung cancer patients and caregivers: an actor-partner interdependence mediation model. Eur J Oncol Nurs. 2021;52:101963. doi:10.1016/j.ejon.2021.101963
13. Wolff JC, Thomas SA, Hood E, et al. Application of the actor-partner interdependence model in parent-adolescent emotion regulation and depression. J Affect Disord. 2020;277:733–741. doi:10.1016/j.jad.2020.08.075
14. Broadbent E, Petrie KJ, Main J, et al. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
15. Jordan JE, Buchbinder R, Osborne RH. Conceptualising health literacy from the patient perspective. Patient Educ Couns. 2010;79(1):36–42. doi:10.1016/j.pec.2009.10.001
16. Zaixia SI, Lingxia GUO, Zhou MIN, et al. The revised morisky medication adherence scale for the detection of reliability and validity in patients undergoing anticoagulation therapy. J Nurs. 2012;27(22):23–26.
17. Vellone E, LorinI S, Ausili D, et al. Psychometric characteristics of the caregiver contribution to self-care of chronic illness inventory. J Adv Nurs. 2020;76(9):2434–2445. doi:10.1111/jan.14448
18. Wingate S, Sng E, Loprinzi PD. The influence of common method bias on the relationship of the socio-ecological model in predicting physical activity behavior. Health Promot Perspect. 2018;8(1):41–45. doi:10.15171/hpp.2018.05
19. Sovariova SM, Suchanova R, Parova V, et al. association between illness perception and adherence to treatment in slovak patients with hypertension: a cross-sectional study. J Cardiovasc Nurs. 2023;38(5):433–442. doi:10.1097/JCN.0000000000000913
20. de Santana Silva, de Santana SJ H, Silva G, et al. Illness perception and self-care in hypertension treatment: a scoping review of current literature. BMC Health Serv Res. 2024;24(1):1529. doi:10.1186/s12913-024-12001-z
21. Lor M, Koleck TA, Bakken S, et al. Association between health literacy and medication adherence among hispanics with hypertension. J Racial Ethn Health Disparities. 2019;6(3):517–524. doi:10.1007/s40615-018-00550-z
22. Shawler C, Edward J, Ling J, et al. Impact of mother-daughter relationship on hypertension self-management and quality of life: testing dyadic dynamics using the actor-partner interdependence model. J Cardiovasc Nurs. 2018;33(3):232–238. doi:10.1097/JCN.0000000000000448
23. Crapo JS, Turner JJ, Bradford K, et al. An actor-partner interdependence model of parenting difficulties over time in stepfamilies. Fam Process. 2023;62(2):653–670. doi:10.1111/famp.12786
24. Su F, Chao J, Zhang B, et al. Couples’ cognition, intimacy, and activity engagement: an actor-partner interdependence model analysis. Clin Gerontol;2023. 1–13. doi:10.1080/07317115.2023.2274524
25. Xu M, Johnson LN, Anderson SR, et al. Emotion dysregulation and couple relationship satisfaction of clinical couples: an actor-partner interdependence model. Fam Process. 2023;62(4):1555–1573. doi:10.1111/famp.12828
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review of the Hill-Bone Compliance to Blood Pressure Therapy Scale
Commodore-Mensah Y, Delva S, Ogungbe O, Smulcer LA, Rives S, Dennison Himmelfarb CR, Kim MT, Bone L, Levine D, Hill MN
Patient Preference and Adherence 2023, 17:2401-2420
Published Date: 28 September 2023
Perceptions and Knowledge of Cholesterol and Lipid-Lowering Medications Among Treatment-Naive Individuals: A Cross-Sectional Study

Kök M, Bostan F, Yacan Kök A
Patient Preference and Adherence 2025, 19:1411-1422
Published Date: 13 May 2025
A Mediation Model of Medication Literacy and Adherence in Type 2 Diabetes During Hospital-Home Transition
Jiang S, Zeng K, Xie S, Huang Y, Li B, Zhang Y
Patient Preference and Adherence 2025, 19:4283-4297
Published Date: 27 December 2025
CT-Based Visual Atherosclerosis Education Improves Secondary Prevention Adherence: A Retrospective Cohort Study Using Cluster Analysis
Hou X, Qiu S, Chen X
Patient Preference and Adherence 2026, 20:561837
Published Date: 15 January 2026
Illness Perception and Medication Adherence Trajectories in Patients with Acute Coronary Syndrome: A 6-Month Longitudinal Study
Xue Q, Wu C, Qu G, Chen Y, Zeng X, Han R
Patient Preference and Adherence 2026, 20:609941
Published Date: 20 May 2026