Back to Journals » Patient Preference and Adherence » Volume 20
Illness Perception and Medication Adherence Trajectories in Patients with Acute Coronary Syndrome: A 6-Month Longitudinal Study
Authors Xue Q, Wu C, Qu G ![]() , Chen Y, Zeng X, Han R
, Chen Y, Zeng X, Han R ![]()
Received 20 March 2026
Accepted for publication 14 May 2026
Published 20 May 2026 Volume 2026:20 609941
DOI https://doi.org/10.2147/PPA.S609941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Qiuhua Xue, Chan Wu, Guangsu Qu, Yingchun Chen, Xiuwen Zeng, Rui Han
Department of Cardiovascular Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Rui Han, Email [email protected]
Objective: To investigate the trajectories of illness perception and medication adherence in patients with acute coronary syndrome, as well as the predictive relationship between the two.
Methods: A total of 311 patients with acute coronary syndrome (ACS) were recruited from the Department of Cardiology, The Second Affiliated Hospital of Chongqing Medical University, using convenience sampling. Participants were assessed at three time points: T1 (within 1 week post-admission), T2 (3 months post-onset), and T3 (6 months post-onset). Data were collected using the Brief Illness Perception Questionnaire (BIPQ) and the Medication Adherence Rating Scale (MARS). Cross-lagged panel modeling (CLPM) and parallel latent growth modeling (LGM) were constructed to analyze the causal relationship between illness perception and medication adherence.
Results: A total of 287 valid questionnaires were returned (valid response rate: 92.28%). From baseline (T1) to 6-month follow-up (T3), illness perception scores significantly decreased from 61.71 ± 7.05 to 36.59 ± 6.56 (F=41.667, P< 0.001), while medication adherence scores declined from 6.92 ± 0.89 to 6.02 ± 1.13 (F=35.223, P< 0.001). Cross-lagged analysis revealed significant reciprocal relationships: illness perception at each time point positively predicted subsequent medication adherence (T1→T2: β=0.425, P< 0.01; T2→T3: β=0.389, P< 0.001), and vice versa (T1→T2: β=0.430, P< 0.001; T2→T3: β=0.427, P< 0.001). Parallel latent growth modeling indicated that higher initial levels of illness perception negatively predicted its own slope (β=− 0.306, P=0.012) and the slope of medication adherence (β=− 0.318, P=0.024). Similarly, the intercept of medication adherence negatively predicted its own slope (β=− 0.301, P=0.012). Furthermore, the slope of illness perception positively predicted the slope of medication adherence (β=0.329, P=0.002).
Conclusion: The illness perception and medication adherence of patients with acute coronary syndrome are on the rise, and illness perception and medication adherence can predict each other.
Keywords: acute coronary syndrome, illness perception, medication adherence, correlation, cross-lag model, parallel latent variable model
Introduction
Acute coronary syndrome (ACS) is one of the leading causes of death worldwide. There are over 20 million new ACS patients globally each year, and approximately 1 million new ACS patients are diagnosed in China annually.1 There are regional and gender differences in the incidence of ACS. The mortality rate in developed countries is declining, whereas the incidence in developing countries is rising rapidly.2,3 Without timely treatment, the patient mortality rate can be as high as 30%. With normative treatment, although the total in-hospital mortality rate in China has dropped to 5%–6%.4 There is an upward trend in the incidence among people under 45 years of age. After being discharged from the hospital following an acute coronary syndrome, the risk of another coronary event is more than 10 times higher than during the first episode, and secondary prevention is essential.5,6
Maintaining a high level of medication adherence is critical for patients with acute coronary syndromes. Studies have shown that subsequent treatment with secondary preventive medications (eg, dual antiplatelet therapy) can significantly reduce the risk of recurrent major adverse cardiovascular events (MACE), such as myocardial reinfarction, stroke, or death.7,8 Good adherence can reduce the risk of MACE by 34% and the need for repeat revascularization by 55%.9
Illness perception refers to an individual’s cognition and understanding of disease-related information, which plays a decisive role in the behavior orientation of coping with the disease, such as medication adherence.10 ACS patients’ perception of the physical burden of the disease has a direct impact on their medication adherence. When patients have a high perceived burden of the disease, they may be more inclined to strictly abide by the drug treatment plan to alleviate the burden.11 Conversely, if the perceived body burden is low or they lack vigilance towards the symptoms, they may neglect or interrupt the medication.
This association may be mediated by the patients’ subjective assessment of disease severity. That is, high burden awareness strengthens the cognition of the disease threat and promotes compliance behavior.12 However, medication adherence is a complex behavior influenced by multidimensional factors. Beyond illness perception, it is inevitably confounded by factors such as the complexity of treatment regimens (eg, daily pill burden and dosage), healthcare system support (eg, frequency of follow-ups), and psychosocial determinants (eg, family social support and economic status).13,14 Previous studies have often treated these elements as background noise, with limited effective control or discussion of these confounders within their models.
Therefore, understanding the development trajectory and related predictive relationship between illness perception and medication adherence in ACS patients after illness is helpful in identifying the time nodes of low adherence among patients and providing active intervention. This has a positive effect on improving the drug adherence of patients with acute coronary syndrome and reducing the risk of adverse cardiovascular events.
However, current domestic and international studies on illness perception and medication adherence in patients with acute coronary syndrome mostly focus on cross-sectional surveys, which fail to capture the dynamic patterns of the changes in these two factors over time. They mainly discuss the static correlation, lacking an understanding of how the disease trajectory can affect dynamic changes. Subsequently, there is a lack of in-depth exploration of how the trajectory and feedback of drug compliance and adherence influence the subsequent trajectory of illness perception. Traditional cross-sectional studies merely offer a ‘snapshot’ at a single time point, making it difficult to infer causal direction and leaving them vulnerable to survivor bias. In contrast, longitudinal designs track intra-individual dynamic changes, thereby clarifying the temporal sequence between variables and more accurately elucidating the underlying causal mechanisms and reciprocal pathways linking illness perception and medication adherence.
Therefore, this research intends to adopt a vertical tracking design, using the latent variable growth model for data modeling analysis in patients with acute coronary syndrome. It aims to identify the different time-trajectory models of disease awareness and drug compliance in patients with acute coronary syndrome. It also intends to further explore the correlation between the two trajectories, with special attention to whether the illness perception trajectory has a predictive effect on the medication adherence trajectory in subsequent periods, and whether the medication adherence trajectory has a lagged effect on the subsequent evolution of the illness perception trajectory.
Subjects and Methods
Subjects
A total of 311 patients with acute coronary syndrome admitted to the Department of Cardiology of the Second Affiliated Hospital of Chongqing Medical University from July 2024 to December 2024 were selected as the survey subjects using the convenience sampling method. The study protocol was approved by the Ethics Committee of The Second Affiliated Hospital of Chongqing Medical University (ID: 2024060025). Written informed consent was obtained from all participants prior to enrollment. All research activities were conducted in accordance with the Declaration of Helsinki.
Inclusion Criteria
- Meeting the 2019 version of the rapid diagnosis and treatment guidelines for acute coronary syndrome.
- Having normal spiritual intelligence.
- Giving informed consent and voluntarily participating in this study, with all patients signing an informed consent form.
Exclusion Criteria
- Patients with severe cognitive impairment.
- Those with language communication disorder.
- Patients unable to cooperate with the investigation due to severe illness.
- Patients with a questionnaire missing > 1 time.
Sample Size Calculation
This study was conducted using repeated measures with sample:15

Specifically, with α=0.05 and 1-β=0.90, Uα/2 and Uβ represent the upper quantiles of the standard normal distribution corresponding to α and β, respectively.  denotes the sample size inflation factor. Based on a pilot study involving 25 cases, measurements were taken three times; thus, K=3, repeated measurement error
denotes the sample size inflation factor. Based on a pilot study involving 25 cases, measurements were taken three times; thus, K=3, repeated measurement error  =124.333, conditional correlation coefficient
=124.333, conditional correlation coefficient  = 0.710, and individual difference variance
= 0.710, and individual difference variance  = 181.667, n=194. Considering the high dropout rate of longitudinal study samples, the dropout rate was calculated as 20%, n=194/0.80=243. Considering the high dropout rate of longitudinal study, the dropout rate was calculated as 20%, 194/0.80 = 243. A total of 311 patients were included in this study.
= 181.667, n=194. Considering the high dropout rate of longitudinal study samples, the dropout rate was calculated as 20%, n=194/0.80=243. Considering the high dropout rate of longitudinal study, the dropout rate was calculated as 20%, 194/0.80 = 243. A total of 311 patients were included in this study.
Survey Instrument
General Information Questionnaire
The general information questionnaire was designed by the researchers. It included the patient’s age, gender, education level, occupation, living situation, residence, type of medical insurance, number of comorbidities, smoking history, and drinking history.
Brief Illness Perception Questionnaire (BIPQ)
The questionnaire was compiled by Broadbent et al16 In this study, the Chinese version of BIPQ, which was translated by Mei Yaqi et al,17 was used. It included three dimensions: the cognitive dimension (including items 1, 2, 3, 4, and 5), the emotional dimension (including items 6 and 8), and the understanding dimension (item 7). For items 1 to 8, respondents choose one option from low to high on a scale of 0 to 10 points. Item 9 is an open-ended question and does not count towards the total score. Items 3, 4, and 7 were scored in the reverse direction, and the total score ranged from 0 to 80, with higher scores indicating a more negative perception and more severe symptoms. The Cronbach’s α coefficients in this study were 0.814, 0.805, and 0.825.
Medication Adherence Rating Scale (MARS)
The Medication Adherence Scale is a self-developed instrument consisting of 10 items. Each item is scored 1 point for “No” and 0 points for “Yes”, with a total score ranging from 0 to 10. A higher score indicates better medication adherence. The scale demonstrated a content validity index (CVI) of 0.82 and a Cronbach’s α coefficient of 0.94 during its validation phase. In the present study, Cronbach’s α coefficients for the scale were 0.880, 0.902, and 0.856.
Data Collection Methods
All questionnaires were administered by trained investigators after enrollment. The questionnaires included the basic information questionnaire, BIPQ, and MARS. The basic information questionnaire was obtained from patients admitted to the hospital for the first time. The access times for the BIPQ and MARS were as follows: after the condition was relatively stable (T1), within 1 week after admission; 3 months after the incidence (T2); and 6 months after the onset (T3). The questionnaires at T2 and T3 were administered during patients’ visits. For patients who could not be followed-up in person, phone or WeChat voice communication was used to conduct the information questionnaire.
This study followed the principle of voluntariness, and patients with acute coronary syndrome voluntarily filled in and answered the questionnaire. Before distributing the questionnaire, the purpose and main contents of the survey were explained to the patients, and informed consent was obtained from them.
Statistical Methods
SPSS 26.0 software and Mplus 8.0 software were employed for statistical analysis and data testing. Count data were presented as cases and percentages (%), while measurement data were presented as mean ± standard deviation (±S). Repeated Measures ANOVA was utilized to examine the dynamic change trend of illness perception and medication adherence at the T1, T2, and T3 time points. When it failed to meet the spherical test, Greenhouse-Geisser correction was applied. To further explore the dynamic interaction between illness perception and medication adherence, Mplus 8.0 was used to construct a dual-model system. The Cross-Lagged Panel Model (CLPM) was employed to test the bidirectional predictive relationship between illness perception and medication adherence, while controlling for the interference of age and gender. The chi-square degree of freedom ratio (χ2/df), comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) were used for evaluation. Values of χ2/df < 5.000, CFI > 0.900, TLI > 0.900, RMSEA < 0.080, and SRMR < 0.100 indicated a good fit. P< 0.05 was considered statistically significant. Multiple imputation was performed to address missing data, and sensitivity analyses confirmed the robustness of the results, with path coefficient fluctuations remaining below 10%.
Results
General Demographic Data
A total of 287 valid questionnaires were collected, with an effective recovery rate of 92.28%. The demographic data of 287 patients with acute coronary syndrome are as follows: aged 34 to 90 years, with an average age of (65.76±11.53); there were 217 males (75.61%) and 70 females (24.39%). The specific information is shown in Table 1.
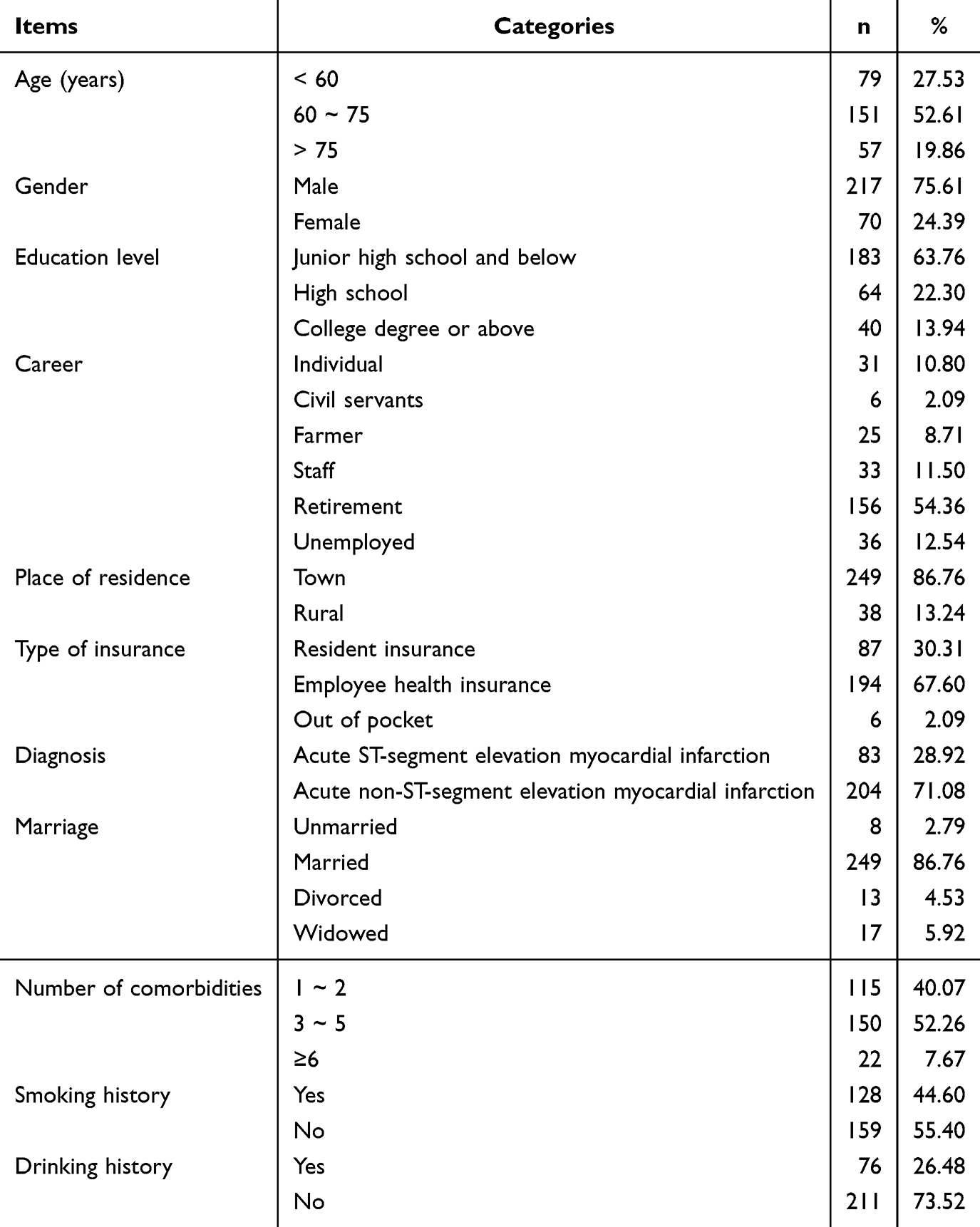 |
Table 1 General Information of Respondents (n=287) |
Common Method Deviation Test
There were 12, 11, and 11 factors with characteristic roots >1 in the T1, T2, and T3 tests, respectively. The variances of the three measurements were 18.24%, 20.56%, and 23.19%, respectively, all of which were less than the critical value level of 40%. The results indicated that there was no obvious common method bias in this study.18
Trends of Illness Perception and Medication Adherence at Three Time Points
Overall, a declining trend was observed for both illness perception and medication adherence scores from T1 to T3. Specifically, illness perception scores decreased significantly from baseline (61.71 ± 7.05) to follow-up (36.59 ± 6.56) (F=41.667, P<0.001), while medication adherence scores also declined from (6.92 ± 0.89) to (6.02 ± 1.13) (F=35.223, P<0.001). Detailed data are presented in Table 2, Figures 1 and 2.
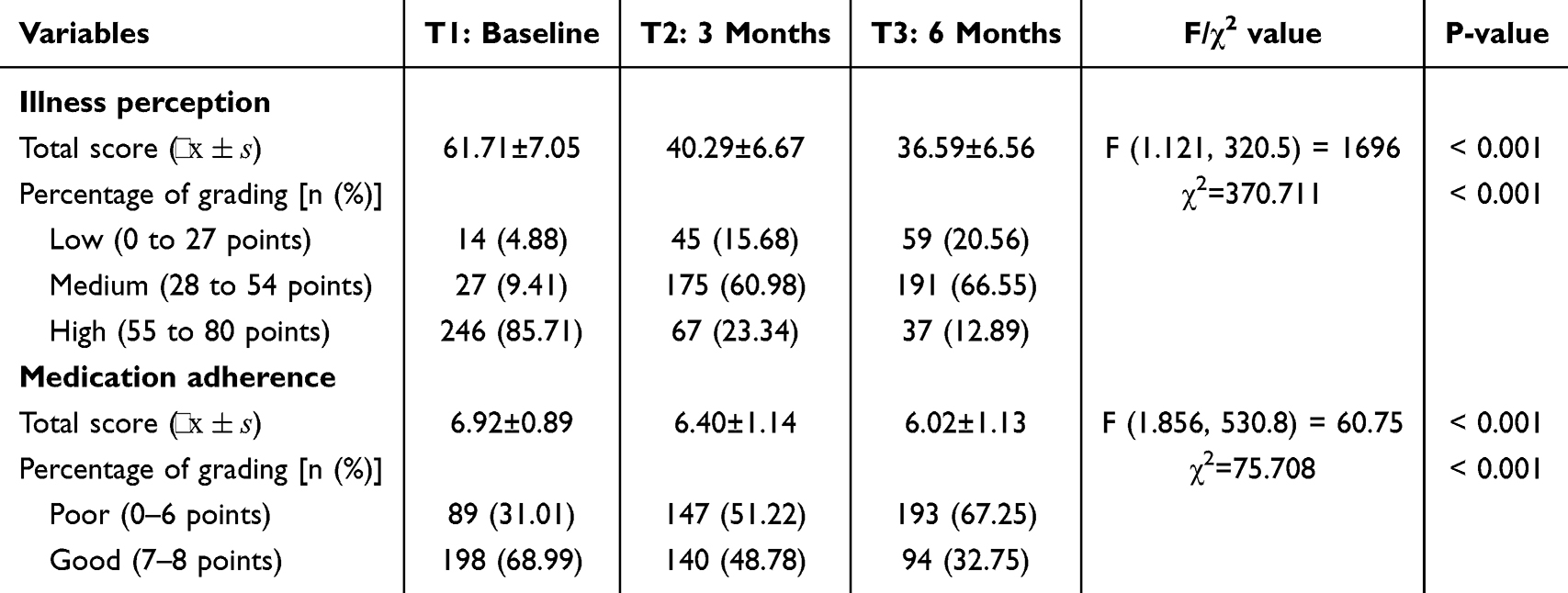 |
Table 2 Dynamic Changes of Illness Perception and Medication Adherence in Patients with Acute Coronary Syndrome (n=287) |
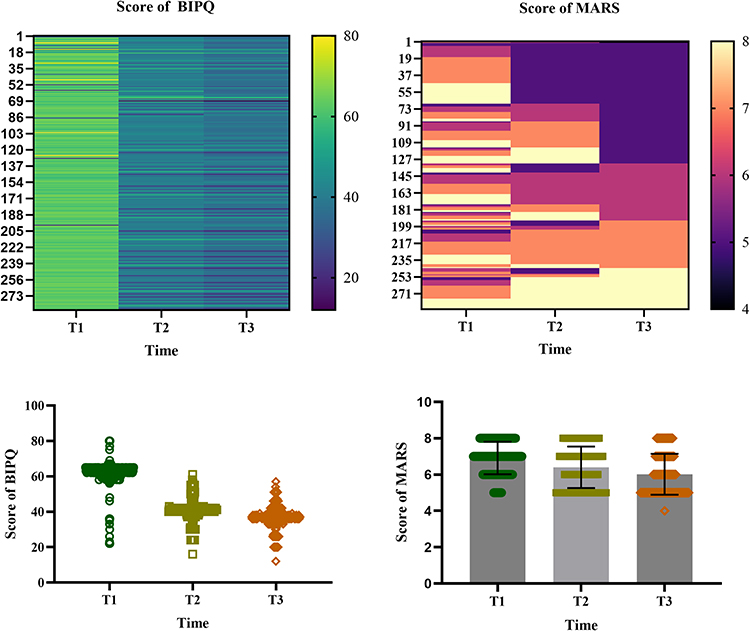 |
Figure 1 Heat map and dot plot distribution of illness perception and medication adherence in patients with acute coronary syndrome. |
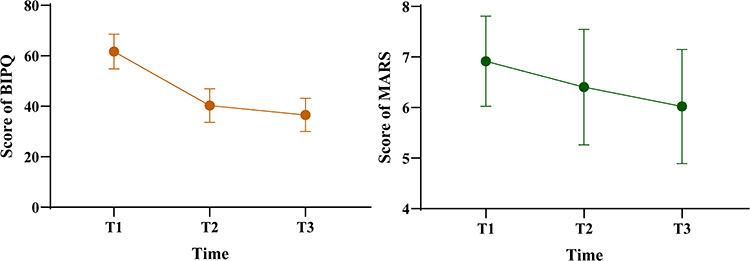 |
Figure 2 Different time trend diagram of illness perception and medication adherence in patients with acute coronary syndrome. |
Correlation Analysis of Illness Perception and Medication Adherence in Patients with Acute Coronary Syndrome at Three Time Points
Pearson correlation analysis was used to examine the illness perception and medication adherence at three time points. The results showed that there was a significant correlation between the two at the three time points (P < 0.05), which met the premise of the cross-lag model. The matrix relationship is presented in Table 3.
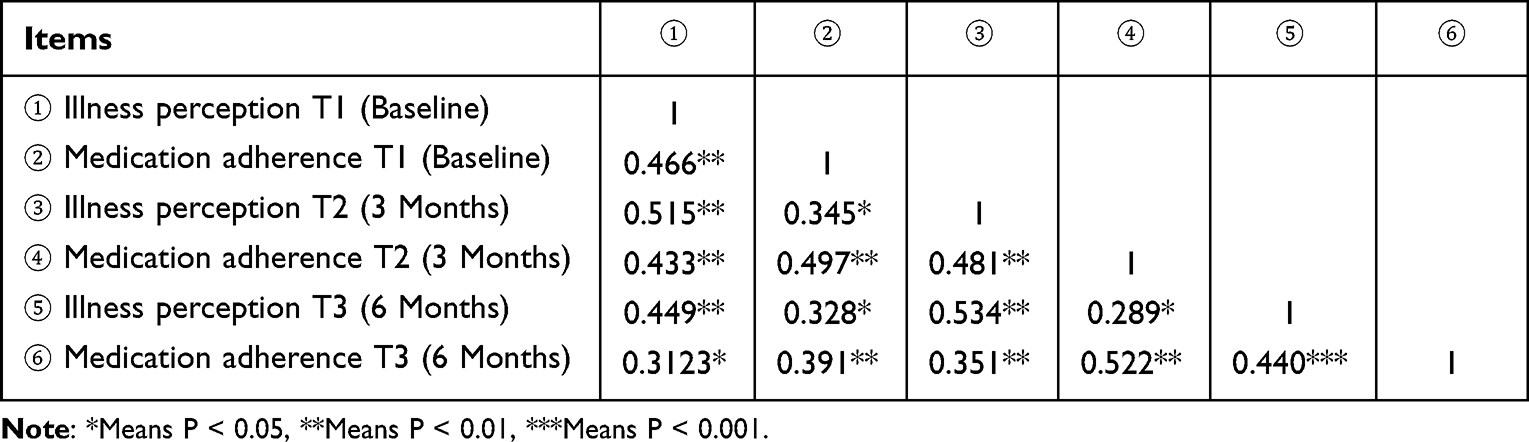 |
Table 3 Scores and Correlation Coefficient Matrix of Illness Perception and Medication Adherence at Three Time Points in Patients with Acute Coronary Syndrome (r Value, n=287) |
Cross-Lag Model of Illness Perception and Medication Adherence in Patients with Acute Coronary Syndrome
Four path models (M1–M4) were constructed to test the causal relationship between illness perception and medication adherence:
- M1 (baseline model): An autoregressive path (T1 → T2 → T3) containing only illness perception and medication adherence.
- M2 (one-way prediction model): On the basis of M1, the prediction path of illness perception on medication adherence at the next time point was added (T1_illness perception → T2_medication adherence, T2_illness perception → T3_medication adherence).
- M3 (reverse prediction model): On the basis of M1, the prediction path of medication adherence to illness perception at the next time point (T1_medication adherence → T2_illness perception, T2_medication adherence → T3_illness perception) was added.
- M4 (two-way full model): It includes both the bidirectional path of illness perception → medication adherence and medication adherence → illness perception.
Robust maximum likelihood estimation (MLR) was used, and model fit comparisons are shown in Table 4. Among them, M4 was significantly better than M1, M2, and M3 (Δχ2 = 153.316, P < 0.001), and the fitting was the best (CFI > 0.98, RMSEA < 0.05), supporting the hypothesis of interaction between them.
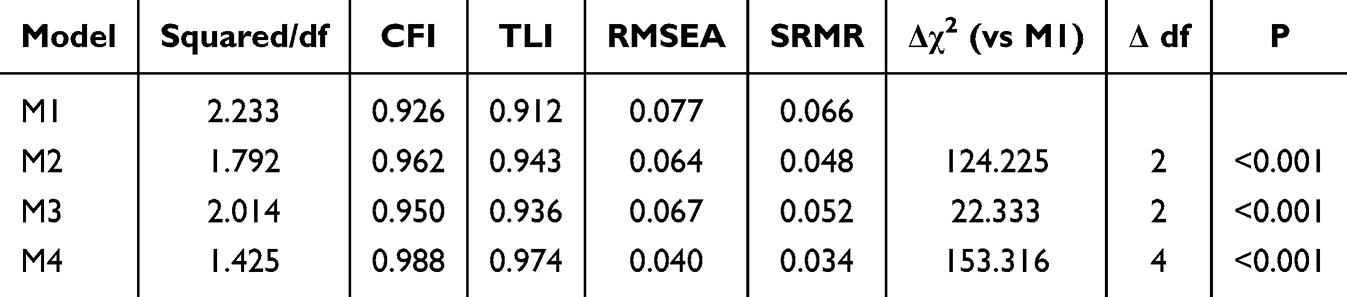 |
Table 4 Comparison of Model Fit |
Specifically
- Autoregressive stability: Both illness perception and medication adherence showed time persistence, and the autoregression coefficient of illness perception was higher (T1 → T2: β = 0.515, T2 → T3: β = 0.534), indicating that the stability of illness perception was stronger than that of medication adherence (the autoregression coefficient of medication adherence T1 → T2: β = 0.497, T2 → T3: β = 0.522).
- Bidirectional cross-temporal prediction: Illness perception → medication adherence path: For every 1 standard deviation (SD) increase in baseline illness perception, medication adherence increased by 0.425 SD (β = 0.425) after 3 months, and the T3 effect was still significant but weakened to β = 0.389.
- Correlation dynamics: Illness perception and medication adherence at the same time point showed a strong positive correlation (T1: β = 0.466, T2: β = 0.481, T3: β = 0.440), and the correlation strength reached the peak at T2.
A cross-lag model was established to investigate the mutual predictive relationship between illness perception and medication adherence. The model fitted well (χ2/df=1.425, GFI=0.988, TLI=0.974, RMSEA=0.040). The level of illness perception positively predicted the medication adherence at the next node (T1→T2: β = 0.425, P < 0.01; T2→T3: β = 0.389, P < 0.001). The level of medication adherence positively predicted the illness perception at the next node (T1→T2: β = 0.389, P < 0.001; T2→T3: β = 0.427, P < 0.001), and the specific path is shown in Figure 3.
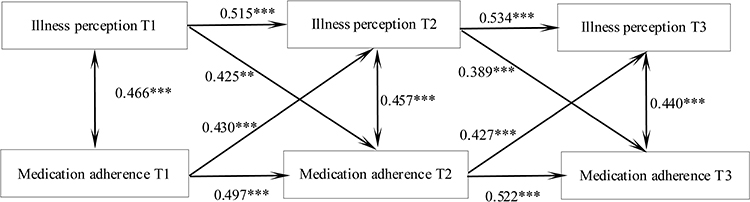 |
Figure 3 The predictive pathways of Illness perception and Medication adherence in patients with acute coronary syndrome at three time points. Notes: Controlling for age, gender, etc.; **Indicates P < 0.01, ***Indicates P < 0.001. |
A Parallel Latent Variable Model of Illness Perception and Medication Adherence in Patients with Acute Coronary Syndrome
A parallel latent variable growth model of illness perception and medication adherence in patients with acute coronary syndrome was constructed. The fitting indicators were as follows: χ2/df = 1.667, GFI = 0.985, TLI = 0.973, RMSEA = 0.0468, SRMR = 0.037, and the degree of fitting was good.
At the initial level, illness perception was positively correlated with medication adherence (r = 0.465, P = 0.005). The intercept of illness perception could negatively predict the slope of self-medication adherence (β = -0.306, P = 0.012), and the intercept of illness perception could also negatively predict the slope of self-medication adherence (β = -0.318, P = 0.024). The intercept of medication adherence could negatively predict the slope of self (β = -0.301, P = 0.012), and the slope of illness perception could positively predict the slope of medication adherence (β = 0.329, P = 0.002). The path of action is shown in Figure 4.
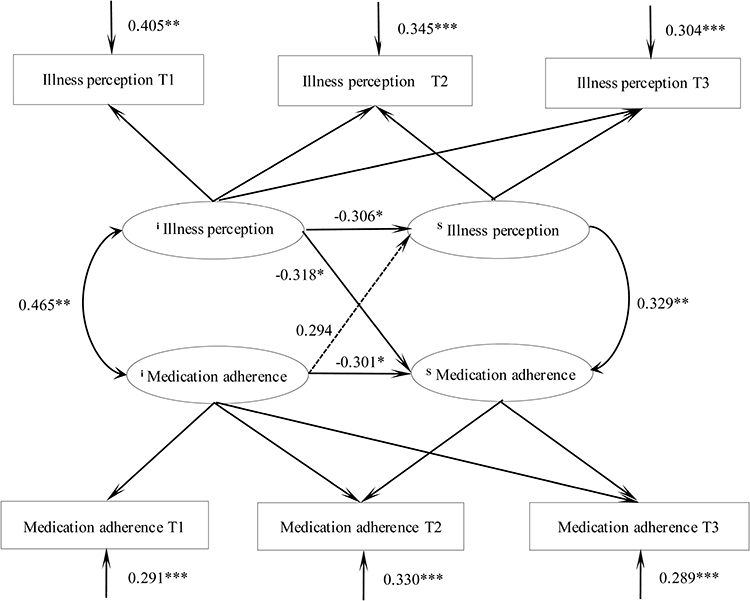 |
Figure 4 Parallel latent variable model of illness perception and medication adherence in patients with acute coronary syndrome. Notes: i denotes the intercept and s denotes the slope. ***Indicates P < 0.001, **Indicates P < 0.01, and *Indicates P < 0.05. |
Discussion
This study found that the illness perception and medication adherence of patients with acute coronary syndrome declined within 6 months after illness. Trends in medication adherence were previously reported in a study by Thomson et al19 This is mainly due to the combined action of many factors. As the acute phase passes, the patient’s body gradually adapts, or the perception of symptoms (such as chest pain and chest tightness) that are prominent in the early stage weakens. Additionally, some symptoms may be alleviated by treatment, which easily leads patients to have the illusion of “the disease has improved”, thereby relaxing their vigilance.20 In terms of medication adherence, patients need to take multiple drugs (such as antiplatelet drugs, statins, etc.) for a long time. The complex medication regimens and potential side effects may directly reduce their willingness to adhere to the medication in the long term. Meanwhile, patients’ perception of the severity of the disease may fade over time, especially when there is no physical emergency, and their subjective emphasis on the importance of secondary prevention may decrease.21,22 Moreover, financial burden, inconvenience of taking medication, and lack of continuous rehabilitation guidance and supervision were also key factors leading to the decline in compliance over time.23 The dual decline of illness perception and adherence undoubtedly increases the risk of long-term recurrence of cardiovascular events.
By constructing a cross-lag model, this study found that the level of illness perception positively predicted the medication adherence at the next time point, and the level of medication adherence also positively predicted the level of illness perception at the next time point. This revealed that there was a dynamic and mutually reinforcing bidirectional predictive relationship between the two. Chen et al pointed out that at a higher level of illness perception, patients perceived the physical burden of the disease more strongly. The pain experience and concern about health status prompted patients to adhere more strictly to medication in subsequent stages to relieve symptoms and control disease progression, reflecting the lagged effect of illness perception on adherence.24
On the other hand, when patients maintain good medication adherence, the secondary prevention drug treatment they receive can effectively stabilize the plaque and improve myocardial blood supply. This can reduce the severity and attack frequency of physical symptoms such as angina pectoris and chest at subsequent time points, showing the lagged improvement effect of medication adherence on symptoms.25
In this study, by constructing the parallel latent variable model, it was found that at the initial level, illness perception is positively correlated with medication adherence. That is, the higher the patient’s illness perception level, the higher the medication adherence level, which also explains the reason in the above discussion. The intercept of illness perception can negatively predict its own slope. That is, the higher the initial level of illness perception, the slower the subsequent decline of illness perception. The higher the initial level of illness perception, the more severe the symptoms, the more complex the pathological basis, and the more difficult the symptom relief, so the decline rate of illness perception is relatively slower.26 The intercept of illness perception can negatively predict the slope of self-medication adherence. That is, the higher the initial level of illness perception, the slower the subsequent decline of medication adherence. For patients with severe initial symptoms, their motivation to maintain medication behavior decays more slowly due to continuous symptom reminders and possible stronger disease concerns, so the rate of decline in medication adherence is also slower. The intercept of medication adherence negatively predicted its slope. That is, patients with a higher initial level of medication adherence had a slower decline in subsequent medication adherence. Patients with a higher initial level of medication adherence often established better medication habits or had more positive beliefs about their treatment, which helped to counteract possible lapses over time and thus maintained their adherence levels for longer and with a slower decline.27,28 The slope of illness perception positively predicted the slope of medication adherence. That is, patients with a faster decline in illness perception had a faster decline in subsequent medication adherence. Patients with a faster decline in illness perception may have their conditions more quickly controlled or have obvious improvement in subjective feelings, which may weaken their motivation to continue to take medication strictly, leading to an accelerated decline in medication adherence.
Limitations
Despite elucidating the dynamic interaction mechanism between illness perception and medication adherence in ACS patients, this study has several limitations that warrant careful consideration. First, the sample was derived from a single-center convenience sampling method, resulting in relatively homogeneous geographical and healthcare resource coverage, which limits the generalizability of the results to broader populations and primary care settings. Second, both illness perception and medication adherence data relied solely on self-reported questionnaires, which are susceptible to social desirability bias and recall bias, lacking validation against objective adherence metrics such as electronic medication monitoring or pharmacy refill records. Third, although demographic variables were controlled for, the models did not incorporate potential confounding factors such as treatment regimen complexity, comorbidity burden, and economic strain, which may independently influence the developmental trajectories of both variables. Finally, the 6-month follow-up duration was relatively limited, restricting the ability to capture the long-term (eg, >1 year) natural evolution of illness perception and adherence, as well as their association with clinical endpoints such as major adverse cardiovascular events (MACE).
Conclusions
Illness perception and medication adherence in patients with acute coronary syndrome are increasing, and illness perception and medication adherence can predict each other. Clinical medical staff should pay attention to the evaluation of illness perception in patients with acute coronary syndrome and make rational use of the interaction between illness perception and medication adherence. This has a positive effect on improving the medication adherence of patients with acute coronary syndrome and reducing the risk of adverse cardiovascular events. Based on these findings, this study holds significant clinical implications and suggests directions for future research. At the clinical level, given the bidirectional reinforcing effect between illness perception and adherence, healthcare professionals should abandon singular medication counseling models in favor of a comprehensive integrated mind-body intervention strategy. Specifically, for patients exhibiting excessively high or low initial illness perceptions, cognitive behavioral therapy is recommended to correct biased cognitions regarding disease severity. Clinicians should leverage the vigilance dividend offered by high illness perception to optimize medication motivation, while simultaneously guarding against adherence decline induced by symptom alleviation. Furthermore, future intervention studies should focus on modulating the deceleration of illness perception slopes to indirectly sustain long-term medication adherence. Potential strategies include developing mHealth-based reminder systems or constructing peer support groups to disrupt the vicious cycle of declining perception, eroding adherence, and functional deterioration.
Ethics and Consent Statements
This study was finally approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University. Informed consent was obtained from all patients in this study.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Zhou S, Zhang Y, Dong X, et al. Regional variations in management and outcomes of patients with acute coronary syndrome in China: evidence from the National Chest Pain Center Program. Sci Bull. 2024;69(9):1302–11. doi:10.1016/j.scib.2024.03.010
2. Wu Y, Yu X, Zhu Y, et al. Integrating depression and acute coronary syndrome care in low resource hospitals in China: the I-CARE randomised clinical trial. Lancet Reg Health West Pac. 2024;48:101126. doi:10.1016/j.lanwpc.2024.101126
3. Dong X, Ding F, Zhou S, et al. Optimizing an emergency medical dispatch system to improve prehospital diagnosis and treatment of acute coronary syndrome: nationwide retrospective study in China. J Med Internet Res. 2022;24(11):e36929. doi:10.2196/36929
4. Li S, Dong X, Li D, et al. Inequities in ambulance allocation associated with transfer delay and mortality in acute coronary syndrome patients: evidence from 89 emergency medical stations in China. Int J Equity Health. 2022;21(1):178. doi:10.1186/s12939-022-01777-3
5. Lin YW, Huang JL, Wei XB, et al. Estimated glomerular filtration rate derived from different formulas and prognosis in acute coronary syndrome: findings from the improving care for cardiovascular disease in China-acute coronary syndrome project. Am J Med Sci. 2022;364(5):565–574. doi:10.1016/j.amjms.2021.10.034
6. Yan Y, Gong W, Huang X, et al. Dual loading antiplatelet therapy in patients with acute coronary syndrome and high bleeding risk undergoing percutaneous coronary intervention: findings from the improving care for cardiovascular disease in china project. Front Cardiovasc Med. 2022;9:774123. doi:10.3389/fcvm.2022.774123
7. Chow CK, Klimis H, Thiagalingam A, et al. Text messages to improve medication adherence and secondary prevention after acute coronary syndrome: the TEXTMEDS randomized clinical trial. Circulation. 2022;145(19):1443–1455. doi:10.1161/CIRCULATIONAHA.121.056161
8. Bots SH, Inia JA, Peters S. Medication adherence after acute coronary syndrome in women compared with men: a systematic review and meta-analysis. Front Glob Womens Health. 2021;2:637398. doi:10.3389/fgwh.2021.637398
9. Bagyawantha N, Coombes ID, Gawarammana I, et al. Impact of a clinical pharmacist on optimising the quality use of medicines according to the acute coronary syndrome (ACS) secondary prevention guidelines and medication adherence following discharge in patients with ACS in Sri Lanka: a prospective non-randomised controlled trial study protocol. BMJ Open. 2023;13(2):e59413.
10. Cheng Y, Tang X, Wu Y, et al. Mediating effect of health belief on illness perception and medication adherence in patients with non-valvular atrial fibrillation. J Pract Cardio-Cerebro-Pulmonary Vasc Dis. 2023;31(5):106–111.
11. Pitanupong J, Sammathit J. Knowledge and attitudes on medication adherence and residual symptoms in individuals with depression: a survey at a University Hospital. BMC Psychiatry. 2023;23(1):210. doi:10.1186/s12888-023-04706-y
12. Alqarni AA, Aldhahir AM, Siraj RA, et al. Asthma medication adherence, control, and psychological symptoms: a cross-sectional study. BMC Pulm Med. 2024;24(1):189. doi:10.1186/s12890-024-02995-x
13. Ingersoll KS, Cohen J. The impact of medication regimen factors on adherence to chronic treatment: a review of literature. J Behav Med. 2008;31(3):213–224. doi:10.1007/s10865-007-9147-y
14. Choudhry NK, Fischer MA, Avorn J, et al. The implications of therapeutic complexity on adherence to cardiovascular medications. Archiv Intern Med. 2011;171(9):814–822. doi:10.1001/archinternmed.2010.495
15. Li X, Liu GF, He DD, et al. Estimation of sample size in repeated measurement design. China Health Statist. 2001;18(4):204–206.
16. Broadbent E, Petrie KJ, Main J, et al. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
17. Mei YQ, Li HP, Yang YJ, et al. Reliability and validity of simplified Chinese version of Illness Perception Questionnaire in female breast cancer patients. Nurs J. 2015;24:11–14.
18. Tang D, Wen Z. Common method bias testing: problems and suggestions. Psychol Sci. 2020;43(01):215–223.
19. Thomson P, Rushworth GF, Andreis F, et al. Longitudinal study of the relationship between patients’ medication adherence and quality of life outcomes and illness perceptions and beliefs about cardiac rehabilitation. BMC Cardiovasc Disord. 2020;20(1):71. doi:10.1186/s12872-020-01378-4
20. Cziraky MJ, Reddy VS, Luthra R, et al. Clinical outcomes and medication adherence in acute coronary syndrome patients with and without type 2 diabetes mellitus: a longitudinal analysis 2006–2011. J Manag Care Spec Pharm. 2015;21(6):470–477. doi:10.18553/jmcp.2015.21.6.470
21. Chinwong S, Doungsong K, Channaina P, et al. Association between medication adherence and cardiovascular outcomes among acute coronary syndrome patients. Res Soc Adm Pharm. 2021;17(9):1631–1635. doi:10.1016/j.sapharm.2021.01.003
22. Liyanage-Don NA, Cornelius T, Romero EK, et al. Association of Hispanic ethnicity and linguistic acculturation with cardiovascular medication adherence in patients with suspected acute coronary syndrome. Prev Med Rep. 2021;23:101455. doi:10.1016/j.pmedr.2021.101455
23. Ho PM, Lambert-Kerzner A, Carey EP, et al. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: a randomized clinical trial. JAMA Intern Med. 2014;174(2):186–193. doi:10.1001/jamainternmed.2013.12944
24. Chen YL, Xie YQ, Wei MY, et al. Clinical effects of detailed nursing management interventions on medication adherence and disease perception in patients with drug-resistant tuberculosis. World J Clin Cases. 2024;12(20):4191–4198. doi:10.12998/wjcc.v12.i20.4191
25. Wang V, Liu CF, Bryson CL, et al. Does medication adherence following a copayment increase differ by disease burden? Health Serv Res. 2011;46(6pt1):1963–1985. doi:10.1111/j.1475-6773.2011.01286.x
26. Guo Z, Zheng L, Fu M, et al. Effects of the full coverage policy of essential medicines on inequality in medication adherence: a longitudinal study in Taizhou, China. Front Pharmacol. 2022;13:802219. doi:10.3389/fphar.2022.802219
27. Wabe N, Lee A, Wechalekar M, et al. Factors associated with medication adherence in a longitudinal study of rheumatoid arthritis patients. Int J Clin Pract. 2019;73(7):e13375. doi:10.1111/ijcp.13375
28. Wang X, Fu Q, Zhou M, et al. How integrated digital tools can improve tuberculosis medication adherence: a longitudinal study in China. Telemed J E Health. 2024;30(2):490–498. doi:10.1089/tmj.2023.0084
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Medication Non-Adherence and Early and Late Readmission Rates for Patients with Acute Coronary Syndrome
Murad H, Basheikh M, Zayed M, Albeladi R, Alsayed Y
International Journal of General Medicine 2022, 15:6791-6799
Published Date: 25 August 2022
Perceptions and Knowledge of Cholesterol and Lipid-Lowering Medications Among Treatment-Naive Individuals: A Cross-Sectional Study

Kök M, Bostan F, Yacan Kök A
Patient Preference and Adherence 2025, 19:1411-1422
Published Date: 13 May 2025
Illness Perception, Health Literacy, and Medication Adherence in Hypertensive Patients and Their Spouses: An Actor-Partner Interdependence Mediation Model Approach
Han R, Wu C, Qu GS, Chen YC, Zeng XW, Xue QH
Patient Preference and Adherence 2025, 19:3647-3656
Published Date: 15 November 2025