Back to Journals » Patient Preference and Adherence » Volume 20
CT-Based Visual Atherosclerosis Education Improves Secondary Prevention Adherence: A Retrospective Cohort Study Using Cluster Analysis
Authors Hou X ![]() , Qiu S
, Qiu S ![]() , Chen X
, Chen X ![]()
Received 27 August 2025
Accepted for publication 30 December 2025
Published 15 January 2026 Volume 2026:20 561837
DOI https://doi.org/10.2147/PPA.S561837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xiaomeng Hou, Shulin Qiu, Xiaochen Chen
Department of Health Care, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Xiaomeng Hou, Peking Union Medical College Hospital (Dongdan Campus), Chinese Academy of Medical Sciences and Peking Union Medical College, No. 1 Shuaifuyuan Wangfujing Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +8613651268681, Email [email protected]
Purpose: Suboptimal adherence to pharmacotherapy for modifiable atherosclerotic risk factors (hypertension, dyslipidaemia, and diabetes) remains a major barrier to effective secondary prevention, particularly in newly diagnosed middle-aged individuals.
Patients and Methods: This retrospective cohort study evaluated the effects of a novel visually aided atherosclerosis education intervention in which clinicians used computed tomography (CT) images to show atherosclerotic calcification and explain plaque progression on adherence. Non-smoking males aged 45– 60 years (n = 153) who underwent health screening at Peking Union Medical College Hospital (March–October, 2024) were stratified into educated (CT-based visualisation of atherosclerotic calcification progression and risk factor education, n = 76) and non-educated (n = 77) groups. K-means cluster analysis was used to classify participants based on low-density lipoprotein cholesterol (LDL-C), glycated haemoglobin (HbA1c), and systolic blood pressure (SBP) control as a proxy for adherence. Group differences in cluster distribution (reflecting adherence patterns) were assessed using the chi-square test.
Results: Cluster analysis identified four distinct adherence patterns: cluster 1 (Optimal Control, 67 patients), cluster 2 (Suboptimal Lipid Control, 61 patients), cluster 3 (Suboptimal Glycaemic Control, 14 patients), and cluster 4 (Suboptimal BP Control, 11 patients). The educated group had significantly more individuals in Cluster 1 (Optimal Control: 53.9% vs 33.8% in the uneducated group, p = 0.012) and fewer suboptimally controlled risk factors (46.1% vs 66.2%, p = 0.012).
Conclusion: Structured, visually aided atherosclerosis education significantly improved adherence to secondary prevention measures and optimised risk factor control. Integrating this evidence-based intervention into routine clinical practice may enhance patient engagement and improve long-term outcomes.
Keywords: medication adherence, atherosclerosis secondary prevention, visual health education, cardiovascular risk factors, health literacy
Introduction
The onset and incidence of hypertension, hyperlipidaemia, and diabetes in middle-aged and older populations are critical factors that contribute to atherosclerosis development and subsequent cardiovascular events.1–3 Timely control of these modifiable risk factors confers substantial benefits in preventing atherosclerosis progression and reducing cardiovascular morbidity and mortality.4,5
Despite the proven benefits of secondary prevention, adherence to suboptimal medications remains a pervasive challenge that undermines its effectiveness. Globally, poor adherence to cardiovascular medications is widespread, with studies estimating that approximately 50% of patients do not take their prescribed medications, leading to inadequate risk factor control and worse clinical outcomes.6–8 Traditional educational methods, which often rely on verbal instructions or pamphlets, may fail to sufficiently motivate behavioural change by making the abstract threat of atherosclerosis feel less immediate.
The literature confirms that improving medication adherence necessitates multifaceted approaches that incorporate digital tools, personalised counselling, behavioural interventions, and barrier mitigation to enhance compliance and reduce cardiovascular risk.9–12 In this context, visual aids have emerged as potent tools for enhancing comprehension and risk perception. By making invisible pathological processes tangible, visual-based interventions can directly influence key determinants of health behaviour, such as perceived susceptibility and severity, as outlined in the Health Belief Model.13,14 For instance, systematic reviews increasingly underscore the value of personalised risk communication, which can be powerfully facilitated by visualising individual pathologies using techniques such as vascular ultrasound or computed tomography (CT) imaging.8,15 However, evidence on the specific impact of CT-based visual education on adherence in the middle-aged population, where early intervention is crucial, remains limited.
Therefore, this study aimed to evaluate the impact of a novel visually aided atherosclerosis education intervention using CT images to illustrate individual calcified plaques and their potential progression on adherence to secondary prevention measures in this key demographic region.
Materials and Methods
Ethical Considerations
This study was approved by the Institutional Review Board of the Peking Union Medical College Hospital (PUMCH; approval no. I-24PJ1686). The requirement for informed consent was waived due to the retrospective design and anonymised nature of the data. The study adhered to the principles of the Declaration of Helsinki.
Study Setting
Beginning in March 2023, a visually aided atherosclerosis education episode was integrated into health examination feedback sessions for patients. This standardised session, delivered by the attending physicians during the feedback consultation, typically lasted 5–7 minutes. During CT scan interpretation, clinicians demonstrate atherosclerotic calcifications in the mediastinal window of the aorta, its major branches, and the coronary arteries. Serial imaging illustrating calcified plaque progression over time was used to educate patients on modifiable risk factors (smoking, hypertension, dyslipidaemia, and diabetes mellitus), emphasising the need to control these risk factors through pharmacotherapy when indicated.
This retrospective cohort study evaluated the impact of visually aided atherosclerosis education on adherence to secondary prevention measures, with participants stratified into an educated group (those receiving the education module during their 2023 health feedback session) and a non-educated group (those not receiving this intervention). Group assignment was definitively determined by whether the patient had received a specific feedback consultation in 2023, during which time the novel visual atherosclerosis education was delivered.
Inclusion and Exclusion Criteria
Health examination reports of contracted members from the Department of Health Medicine were consecutively enrolled, with the following inclusion criteria applied to mitigate the confounding effects of sex and smoking status on glucose metabolism, blood pressure, and lipid profiles:16 never-smoking males aged 45–60 years who completed a comprehensive health screening package between March 1 2024 and October 31 2024. This selective inclusion was intended to enhance the internal validity of educational effects by reducing known confounding factors, although it may limit the generalisability of the findings. Participants with clinically significant unstable comorbidities (eg, active malignancies or systemic infections) during screening were excluded.
Data Collection
Health examination data were retrospectively abstracted for consecutively enrolled non-smoking male members (aged 45–60 years) undergoing comprehensive screening at Peking Union Medical College Hospital between March 1 and October 31, 2024, with the following parameters extracted: glycemic control metrics including fasting blood glucose (FBG) and glycated hemoglobin (HbA1c); lipid profile comprising triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and total cholesterol (TC); and blood pressure measurements (systolic [SBP] and diastolic [DBP]).
Statistical Analysis
K-means cluster analysis was applied to the baseline LDL-C, HbA1c, and SBP values as key pharmacotherapeutic targets for dyslipidaemia, diabetes, and hypertension. This study identified distinct patterns of risk factor control, reflecting the overall adherence to atherosclerotic secondary prevention. Continuous variables are expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]) for normally and non-normally distributed data, respectively (Table 1). The association between educational status (educated vs uneducated) and clustered adherence patterns was assessed using the chi-square test (Table 2). Analyses were performed using the Statistical Package for the Social Sciences (SPSS) Modeller (Professional Authorised User V 18.4, IBM).
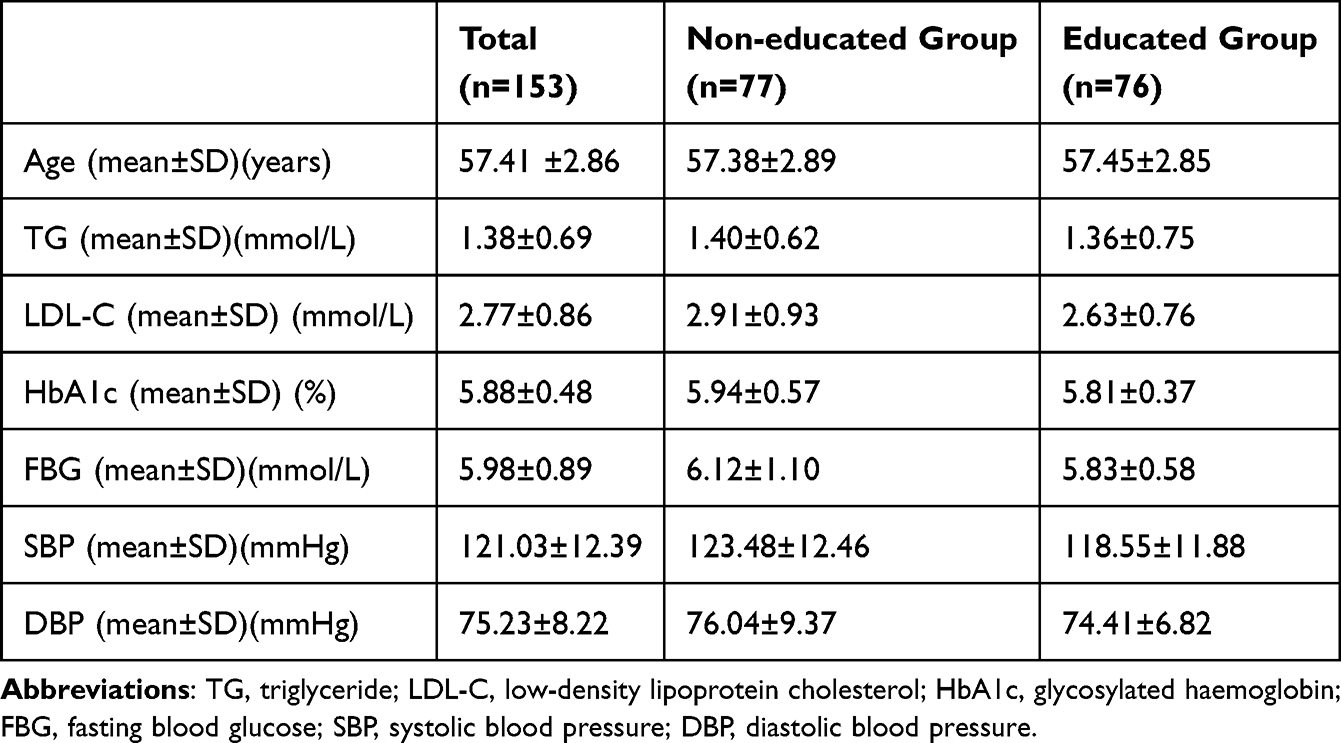 |
Table 1 Distribution of Metabolic Indicators |
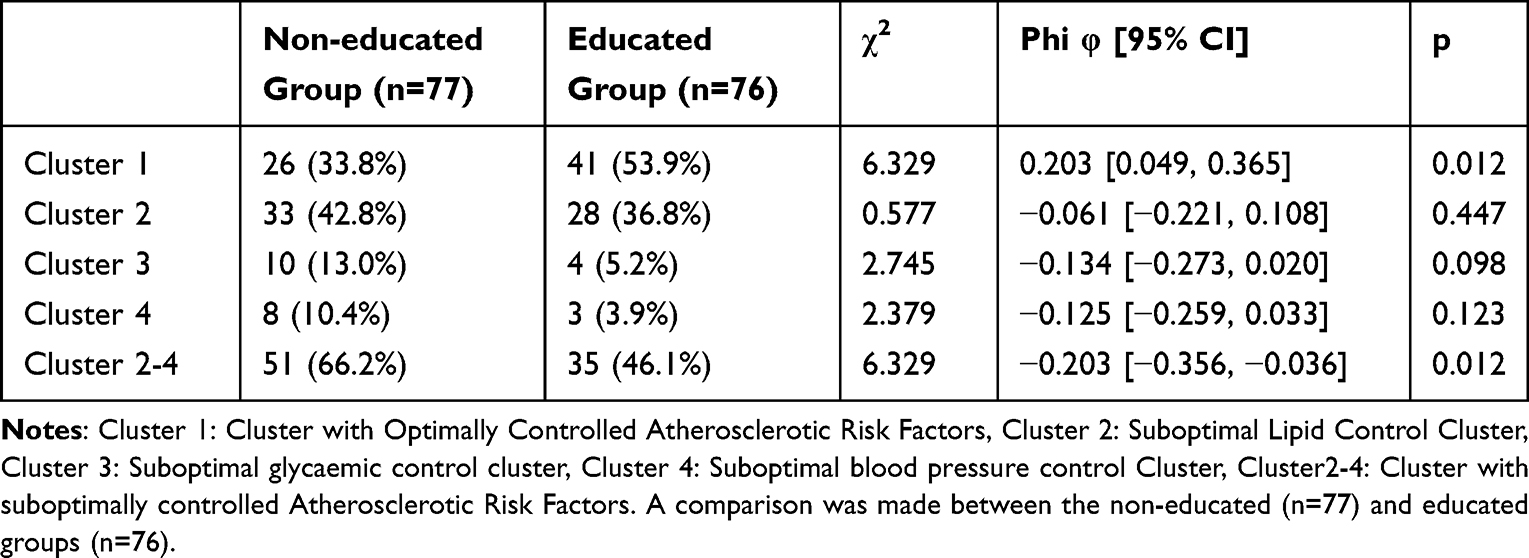 |
Table 2 Association Between Education Status and Clustered Adherence Patterns |
Results
Baseline Characteristics of Participants
Data of 153 male patients with an average age of 57.41 years were included in this study. There were 77 uneducated participants with an average age of 57.38, and 76 educated participants with an average age of 57.45. The metabolic indicators of each group are listed in Table 1, which shows that the two groups were comparable at baseline.
Cluster Analysis of Atherosclerotic Risk Factors
K-means cluster analysis was performed for LDL-C, HbA1c, and SBP levels. The optimal number of clusters (K = 4) was determined by evaluating solutions from three to nine clusters and selecting the one that best met the clinical validity and technical adequacy, as supported by a silhouette coefficient of 0.5. The predictors were LDL-C (1.0), HbA1c (0.70), and SBP (0.48) (Figure 1).
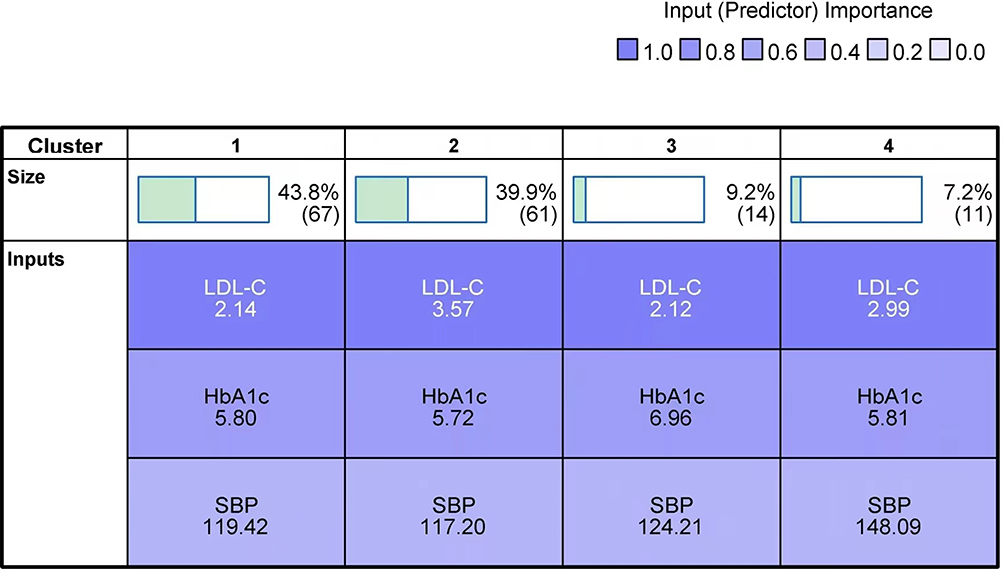 |
Figure 1 Clustering of Atherosclerotic Risk Factors. Notes: Predictor importance of the three variables (LDL-C, HbA1c, and SBP) in the K-means cluster analysis. The analysis identified LDL-C as the most important discriminator among the clusters. |
The four distinct adherence patterns are summarised as follows (Table 2):
Cluster 1: Optimal Control (n = 67): This group achieved all three risk factor targets (LDL-C <2.6 mmol/L, HbA1c <6.3%, SBP ~119.42 mmHg) (Figure 2).
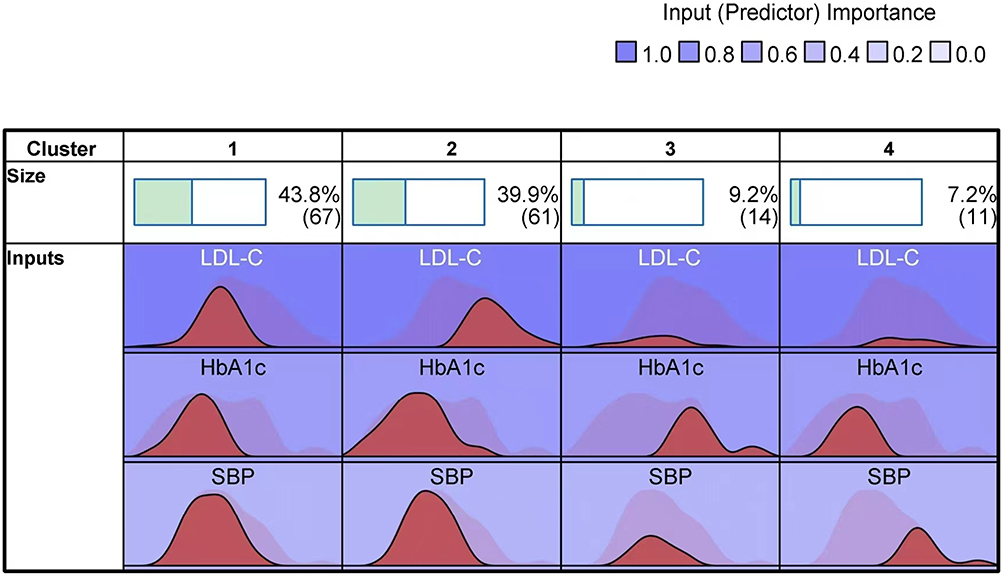 |
Figure 2 Distribution of Risk Factors in Different Clusters. Notes: Radar chart illustrating values of LDL-C, HbA1c, and SBP across the four identified clusters. Cluster 1 (Optimal Control) shows good performance for all three parameters. |
Cluster 2: Suboptimal Lipid Control (n = 61): Characterised by inadequately controlled LDL-C (>2.6 mmol/L) despite controlled HbA1c and SBP (Figure 3).
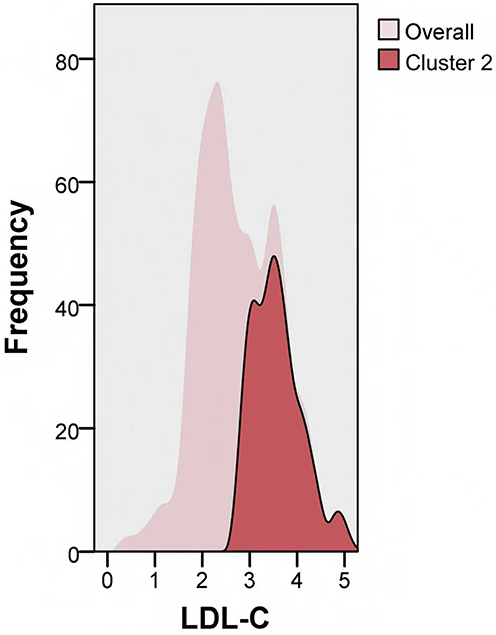 |
Figure 3 Distribution of LDL-C in Cluster 2. Notes: Distribution of low-density lipoprotein cholesterol (LDL-C) levels for the 61 participants in Cluster 2 (Suboptimal Lipid Control). |
Cluster 3: Suboptimal glycaemic control (n=14): elevated HbA1c (>6.3%) with optimal LDL-C and normotensive status (Figure 4).
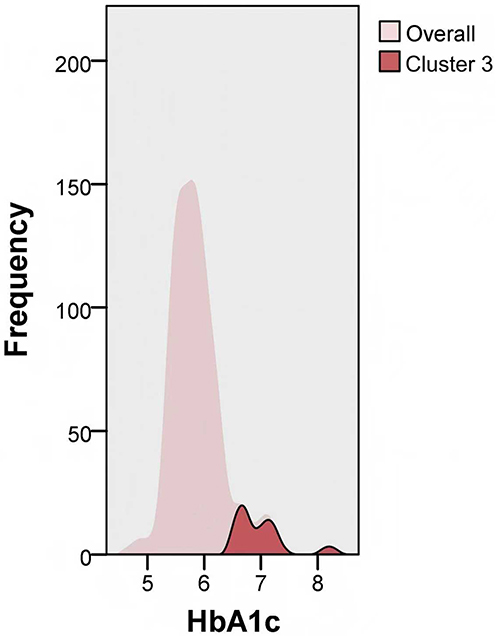 |
Figure 4 Distribution of HbA1c in Cluster 3. Notes: Distribution of glycated haemoglobin (HbA1c) levels for the 14 participants in Cluster 3 (Suboptimal Glycemic Control). |
Cluster 4: Suboptimal Blood Pressure control (n=11): poorly controlled SBP (>140 mmHg) with suboptimal LDL-C, while HbA1c was controlled (Figure 5).
 |
Figure 5 Distribution of SBP in Cluster 4. Notes: Distribution of systolic blood pressure (SBP) levels for the 11 participants in Cluster 4 (Suboptimal Blood Pressure Control). |
A schematic flowchart illustrating the participant grouping and resulting clusters is presented in Figure 6, which provides a visual summary of the study cohort.
 |
Figure 6 Flowchart of Participant Grouping and Cluster Analysis. Notes: This flowchart illustrates the participant grouping and cluster analysis process. The final cohort of 153 never-smoking males was stratified into Educated and Non-educated groups based on the receipt of visual atherosclerosis education. All participants subsequently underwent K-means cluster analysis based on LDL-C, HbA1c, and SBP, resulting in four distinct clusters of risk factor control. |
Distribution of Clusters Among Education Groups
Chi-square analysis revealed a differential cluster distribution based on the recipient of education on visually aided atherosclerosis treatment. Compared to non-recipients, education recipients had significantly more individuals with Optimally Controlled Atherosclerotic Risk Factors (53.9% vs 33.8%, χ2=6.329, p=0.012; Phi φ = 0.203, 95% CI [0.049, 0.365]). Non-recipients tended to have a higher proportion of Suboptimal Blood Pressure Control (SBPC) (10.4% vs 3.9%) and a greater representation of suboptimal glycaemic control (13.0% vs 5.2%). When clusters with suboptimal risk factor control were combined into a single group due to limited sample sizes in individual clusters, clinically significant differences emerged: non-recipients had significantly more individuals with Suboptimally Controlled Atherosclerotic Risk Factors (66.2% vs 46.1%, χ2=6.329, p=0.012; Phi φ = −0.203, 95% CI [−0.356, −0.036]).
Discussion
Atherosclerotic risk factors include non-modifiable factors (genetics, age, and sex) and modifiable factors (smoking, hypertension, dyslipidaemia, and diabetes). The most modifiable risk factors typically emerge during middle age.17,18 Following diagnosis, standardised pharmacotherapy is often challenging for previously healthy middle-aged individuals to accept.19 This study focused on the critical importance of adherence to the secondary prevention of atherosclerosis. To identify improvement strategies, the effects of a novel visually aided atherosclerosis education intervention were evaluated on adherence to secondary prevention measures.
For example, the global hypertension epidemic remains largely uncontrolled, with hypertension persisting as the leading cause of noncommunicable disease mortality worldwide.18 Suboptimal adherence, manifested as a failure to initiate pharmacotherapy, take prescribed medications, or maintain long-term therapy, is a well-established contributor to poor blood pressure control.6,7 Their subjective health beliefs may influence patient acceptance of medical advice. Self-perceived control over blood pressure reduction may decrease medication reliance and subsequently increase nonadherence. Notably, Cluster 4 in this study represented this self-determined blood pressure management group, which was characterised by untreated or inadequately treated hypertension. Consequently, lipid control is suboptimal, owing to poor medication adherence.
Medication compliance is paramount in managing chronic conditions such as dyslipidaemia and diabetes. Poor compliance leads to uncontrolled glucose levels, elevated cholesterol levels, increased stroke, myocardial infarction, and an increased risk of complications.20 Newly diagnosed patients with dyslipidaemia often prefer non-pharmacological approaches (dietary modification and exercise), although evidence confirms their limited efficacy in achieving lipid targets.21,22 Delays in observing non-pharmacological effects prolong vascular exposure to hyperlipidaemia, thereby increasing the risk of cardiac events, stroke, and other cardiovascular outcomes.23 Effective diabetes management typically requires multidrug regimens. This often leads to reluctance among older patients.24 Cluster 2 represented patients undergoing excessive lipid observation periods, whereas Cluster 3 comprised patients with inadequate self-monitoring and pharmacotherapy for diabetes.
The beneficial effects of the intervention can be understood through psychological models of health behaviours. The CT-based visualisation directly operationalises components of the Health Belief Model by making the invisible threat of atherosclerosis visible and tangible.13,14 It enhances perceived susceptibility (by showing “this is happening in my body”) and perceived severity (by illustrating plaque progression), thereby motivating action to reduce the threat through improved adherence. These findings align with those of other studies utilising personalised motivational interventions, which have shown promise in improving risk factor control.12 However, this approach of using routine CT scans to demonstrate calcification offers a novel and readily integrated method for standard health screening.
Higher education levels correlate with better adherence, because educated patients better comprehend their condition and the need for treatment.13 Health literacy, the capacity to understand health information and make informed decisions, is equally critical.14 Providing clear, concise condition- and medication-related information improves compliance, as does health coaching.25 Therefore, the visually aided atherosclerosis education positively guided patients in terms of disease cognition and awareness of complications. Visualisation reduced therapeutic inertia in Cluster 1 by enhancing the perceived threat of plaque progression. The recipients demonstrated significantly higher rates of Optimally Controlled Atherosclerotic Risk Factors (53.9%, P =0.012). Conversely, non-recipients exhibited substantially more individuals who were suboptimally controlled for atherosclerotic risk factors (66.2%, p=0.012). It is important to note that this was a retrospective study, and the results indicate a strong association between education and improved risk factor control.
This study has several limitations. First, its single-centre retrospective design and homogeneous cohort of non-smoking Chinese males, while strengthening internal validity by reducing confounding factors, limit the generalisability of the findings to other populations, including women and smokers. Second, the sample size, which encompassed all eligible patients during the study period, limited the precision of the estimates for the smaller clusters (eg Clusters 3 and 4) and precluded a formal prospective power calculation. Finally, the lack of long-term follow-up data prevented assessment of the durability of the intervention’s effect on adherence and hard cardiovascular outcomes.
Conclusion
This retrospective cohort study demonstrated that CT-based visual atherosclerosis education was strongly associated with improved control of key atherosclerotic risk factors. CT-based visualisation directly targets the “perceived threat” component of the Health Belief Model, bridging the intention-behaviour gap in adherence. Therefore, this study recommends the integration of this evidence-based visual intervention into routine health-screening feedback sessions. Future prospective randomised controlled trials are warranted to confirm the causal efficacy of this intervention and to assess its long-term impact on cardiovascular events.
Acknowledgments
We would like to thank Editage (www.editage.cn) for the English language editing.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Committee ADAPP. 10. cardiovascular disease and risk management: standards of care in diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S179–10.
2. Boehme AK, Esenwa C, Elkind MSV. Stroke risk factors, genetics, and prevention. Circ Res. 2017;120(3):472–495. doi:10.1161/CIRCRESAHA.116.308398
3. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
4. Joseph JJ, Deedwania P, Acharya T, et al. Comprehensive management of cardiovascular risk factors for adults with type 2 diabetes: a scientific statement from the American Heart Association. Circulation. 2022;145(9). doi:10.1161/CIR.0000000000001040
5. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
6. Akoko BM, Fon PN, Ngu RC, et al. Knowledge of hypertension and compliance with therapy among hypertensive patients in the Bamenda health district of Cameroon: a cross-sectional study. Cardiol Ther. 2017;6(1):53–67. doi:10.1007/s40119-016-0079-x
7. Burnier M, Egan BM. Adherence in Hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
8. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
9. Requena M, Montiel E, Baladas M, et al. Farmalarm. Stroke. 2019;50(7):1819–1824. doi:10.1161/STROKEAHA.118.024355
10. Shen Q, He P, Wen M, et al. Secondary prevention of coronary heart disease: the effect of a nursing intervention using Cox’s interaction model of client health behaviour. J Adv Nurs. 2021;77(10):4104–4119. doi:10.1111/jan.14930
11. Johnson C, Lane H, Barber PA, et al. Medication compliance in ischaemic stroke patients. Intern Med J. 2012;42(4):e47–52. doi:10.1111/j.1445-5994.2010.02209.x
12. Boulmpou A, Kartas A, Farmakis I, et al. Motivational interviewing to support LDL-C therapeutic goals and lipid-lowering therapy compliance in patients with acute coronary syndromes (IDEAL-LDL) study: rationale and design. Hellenic J Cardiol. 2019;60(4):249–253. doi:10.1016/j.hjc.2018.10.002
13. Kamran A, Kamran A, Ahari S, et al. Determinants of patient’s adherence to hypertension medications: application of health belief model among rural patients. Ann Med Health Sci Res. 2014;4(6):922–927. doi:10.4103/2141-9248.144914
14. Persell SD, Karmali KN, Lee JY, et al. Associations between health literacy and medication self-management among community health center patients with uncontrolled hypertension. Patient Prefer Adherence. 2020;14:87–95. doi:10.2147/PPA.S226619
15. Whitmore K, Zhou Z, Chapman N, et al. Impact of patient visualization of cardiovascular images on modification of cardiovascular risk factors: systematic review and meta-analysis. JACC Cardiovasc Imaging. 2023;16(8):1069–1081. doi:10.1016/j.jcmg.2023.03.007
16. Zhong H, Ni X, Chen R, et al. Smoking contribution to the global burden of metabolic disorder: a cluster analysis. Med Clin. 2024;163(1):14–20. doi:10.1016/j.medcli.2024.02.001
17. Zaman S, Wasfy JH, Kapil V, et al. The Lancet Commission on rethinking coronary artery disease: moving from ischaemia to atheroma. Lancet. 2025;405(10486):1264–1312. doi:10.1016/S0140-6736(25)00055-8
18. Jones DW, Jones DW, Ferdinand KC, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation and management of high blood pressure in adults: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212–e316. doi:10.1161/HYP.0000000000000249
19. Larsen J, Andersen M, Kragstrup J, et al. High persistence of statin use in a Danish population: compliance study 1993–1998. Br J Clin Pharmacol. 2002;53(4):375–378. doi:10.1046/j.1365-2125.2002.01563.x
20. Sappok T, Faulstich A, Stuckert E, et al. Compliance with secondary prevention of ischemic stroke: a prospective evaluation. Stroke. 2001;32(8):1884–1889. doi:10.1161/01.STR.32.8.1884
21. Thuraisingham S, Tan KH, Chong KS, et al. A randomised comparison of simvastatin versus simvastatin and low cholesterol diet in the treatment of hypercholesterolaemia. Int J Clin Pract. 2000;54(2):78–84. doi:10.1111/j.1742-1241.2000.tb11854.x
22. Alwhaibi M, Altoaimi M, AlRuthia Y, et al. Adherence to statin therapy and attainment of LDL cholesterol goal among patients with type 2 diabetes and dyslipidemia. Patient Prefer Adherence. 2019;13:2111–2118. doi:10.2147/PPA.S231873
23. Llanes EJB, Thongtang N, Lee Z-V, et al. Addressing adherence challenges in long-term statin treatment among Asian populations: current gaps and proposed solutions. Am J Prev Cardiol. 2025;23:101019. doi:10.1016/j.ajpc.2025.101019
24. Esteghamati A, Larijani B, Aghajani MH, et al. Diabetes in Iran: prospective analysis from First Nationwide Diabetes Report of National Program for Prevention and Control of Diabetes (NPPCD-2016). Sci Rep. 2017;7(1):13461. doi:10.1038/s41598-017-13379-z
25. Thom DH, Willard-Grace R, Hessler D, et al. The impact of health coaching on medication adherence in patients with poorly controlled diabetes, hypertension, and/or hyperlipidemia: a randomized controlled trial. J Am Board Fam Med. 2015;28(1):38–45. doi:10.3122/jabfm.2015.01.140123
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Illness Perception, Health Literacy, and Medication Adherence in Hypertensive Patients and Their Spouses: An Actor-Partner Interdependence Mediation Model Approach
Han R, Wu C, Qu GS, Chen YC, Zeng XW, Xue QH
Patient Preference and Adherence 2025, 19:3647-3656
Published Date: 15 November 2025