Back to Journals » International Journal of General Medicine » Volume 15
The Association Between Medication Non-Adherence and Early and Late Readmission Rates for Patients with Acute Coronary Syndrome
Authors Murad H ![]() , Basheikh M, Zayed M
, Basheikh M, Zayed M ![]() , Albeladi R, Alsayed Y
, Albeladi R, Alsayed Y
Received 3 June 2022
Accepted for publication 15 August 2022
Published 25 August 2022 Volume 2022:15 Pages 6791—6799
DOI https://doi.org/10.2147/IJGM.S376926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hussam Murad,1,2 Mohammed Basheikh,3 Mohamed Zayed,4,5 Roaa Albeladi,6 Yousef Alsayed6
1Department of Pharmacology, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia; 2Department of Pharmacology, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Department of Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Physiology, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia; 5Department of Physiology, Faculty of Medicine, Menoufia University, Menoufia, Egypt; 6Medical Students, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Hussam Murad, Department of Pharmacology, Faculty of Medicine, Rabigh, King Abdulaziz University, Jeddah, 21589, Saudi Arabia, Tel +966541541341, Fax +966024223031, Email [email protected]
Purpose: Unplanned hospital readmission forms costly, but preventable burdens on healthcare system. This study was designed to evaluate cardiovascular-related readmission rate after discharge of acute coronary syndrome (ACS) patients and its relationship with medication adherence at a university hospital, Saudi Arabia.
Methods: A total of 370 consecutive patients presenting with ACS were involved. The inclusion criteria were clinical and coronary angiography diagnostic data of ACS. Exclusion criteria included heart valve disease, myocarditis, hepatic disease, and history of acute infection during the previous two weeks. Patients were divided into index admission group (n = 291) and unplanned readmission group (n = 79). Readmission and medication adherence rates were evaluated during 1– 30, 31– 180, 181– 365, and 366– 548 days post-ACS discharge. Medication adherence was estimated with a (yes/no) questionnaire.
Results: The overall readmission rate was 21.4%; individual rates were 30.4%, 38.0%, 27.8%, and 3.8% and the overall medication adherence rate was 62.03%, while individual rates were 54.2%, 70.0%, 63.6%, and 33.3% during the four periods, respectively. There were strong correlations between medication non-adherence and readmission rates. Heart failure, ST-elevated myocardial infarction, unstable angina, cerebrovascular accident, and arrhythmia represented the top causes. Body mass index was higher in readmission group. There were significant correlations between smoking, hypertension, cerebrovascular accident, ischemic heart disease, previous stent, instent restenosis, and LDL-cholesterol as predictor factors and readmission rate.
Conclusion: The cardiovascular-related unplanned readmission rate post-ACS discharge was 21.4%, and medication non-adherence rate was 37.97%. There were strong correlations between them in the time frames from 1-month to 1.5-year post-discharge. The individual rates decreased by time, but the first month showed lower rates than the following 5 months and this indicated the role of factors other than medication non-adherence in readmission. The rates are generally consistent with the international levels but utilizing technology can further improve medication adherence and reduce readmission rates.
Keywords: medication adherence, readmission rate, acute coronary syndrome, Saudi Arabia
Introduction
The unplanned hospital readmission forms a costly burden on the healthcare system, thus guidelines were implemented to reduce it through recognizing its causes, improving transitional care, and engaging patients.1 Broadly defined, the index admission is the initial (original) hospital admission with a main diagnosis of “a specified condition that meets the inclusion and exclusion criteria for that measure”, while any subsequent admission is called readmission. Readmission within 30 days is used in many studies as an indicator of the quality of care received at the hospital, while readmissions occurring later may be more related to the outpatient care.2 The Hospital Readmission Reduction Program executes a financial penalty for hospitals with excess rates of 30-day readmissions for four conditions with high volume and costs among Medicare beneficiaries which are acute myocardial infarction (AMI), congestive heart failure (CHF), chronic obstructive pulmonary disease, and pneumonia. Readmissions may or may not be related to the original cause for index admission.3
The acute ischemic syndrome (myocardial infarction and unstable angina) patients receive hospital-based acute care therapy; then, they are discharged with secondary prevention medications for chronic therapy. Unfortunately, some patients suffer again for a short duration and are readmitted to hospital. The readmission rates at 30 days and one year of acute coronary syndrome (ACS) discharge were 34.3%, and 61.7%. Kidney disease and diabetes mellitus predicted all-cause readmissions at the first month and first year, but there were no strong predictor factors of cardiovascular-related readmissions. Many readmissions were not related to the index admission and thus were not easily predicted with the common clinical parameters.4 The 30-day readmission post-ACS discharge is common and associated with increased mortality, but due to the patients’ and diseases’ variations, making a certain association with the index admission is elusive and not simply predicted. Therefore, 30-day readmission rates remain controversial as measures of healthcare quality.5
Strong adherence to the secondary prevention medications, used to prevent a second attack of acute coronary syndrome, decreases morbidity and mortality after ACS.6 Medication adherence is “the extent to which a patient takes treatments as prescribed by their healthcare providers and is often quantified as the percentage of prescribed treatments that are taken by the patient”.7 Unfortunately, the definitions and quantifying methods of medication adherence vary across trials, making it difficult to compare results.8 Non-adherence to a medication could be a failure to begin, a premature cessation, or not taking it as scheduled.9 In a clinical trial, “good adherence” to statins was defined as using statins without decline of dosage up to 6 months post discharge, while “poor adherence” was identified as using statins at discharge but with either stoppage or dosage decline at 6 months post discharge.10 Adherence to antiplatelets after coronary intervention among patients with myocardial infarction was evaluated by asking patients whether they took the antiplatelet as prescribed.11 The direct measurements of medication adherence include observed administration and measuring blood concentration of a medication, while the indirect measurements include patient self-report, pill count, pharmacy refills, and electronic monitoring.12 The direct methods are more precise, but difficult and costly while indirect methods are easier but less reliable.13 Medication non-adherence is estimated to account for about 10% of hospitalizations in the United States annually.8 Unfortunately, variations in the quantifying methods of medication adherence make the comparison among studies difficult and an exact estimation of the costs somewhat impossible. Thus, “standardization of the estimating measures and development of a streamlined approach to quantify costs is required”.14
Taken together, this study was designed to evaluate the cardiovascular-related early and late unplanned readmission rate after acute coronary syndrome (ACS) discharge during four time frames; equivalent to 1–30, 31–180, 181–365, and 366–548 days post-discharge; and its relationship with the adherence rate to the secondary prevention medications in patients presenting with ACS at Coronary Care Unit at a university hospital, Western Saudi Arabia.
Materials and Methods
Subjects and Study Design
This cross-sectional observational study was approved by KAU-Research Ethics Committee (Ref. No. 467–21) and was performed in accordance with the Helsinki Declaration. All participants’ names have been changed to numbers. A total of 370 consecutive patients presenting with acute coronary syndrome (ACS) were recruited from the Coronary Care Unit at King Abdulaziz University Hospital from September 2020 to March 2022. The patients underwent coronary angiography and presented ACS according to American Heart Association guidelines.15 The inclusion criteria were clinical and coronary angiography diagnostic data of ACS. The exclusion criteria included heart valve disease, myocarditis, hepatic disease, and history of acute infection during the previous two weeks. The early and late unplanned readmission rates post ACS discharge were evaluated throughout four time frames; equivalent to 1–30, 31–180, 181–365, and 366–548 days; post-ACS discharge. The demographic data and clinical criteria of the patients, including age, gender, weight, height, body mass index (BMI), smoking, hypertension, diabetes mellitus, dyslipidemia (low-density lipoprotein (LDL) cholesterol level, were considered optimal if <2.58 mmol/L),16 and creatinine levels were collected.
Medication adherence was measured indirectly through patient self-reporting. Patients were asked (yes/no) questions about proper use of medications in the following wording (do you take your medications as prescribed by your physician?). The medication adherence questionnaire included questions about the post-ASC medications including antithrombotics, antihypertensives, and statins. During the four time frames of the study, the medication adherence was measured as previously described where the proportion of days covered (PDC); which is the number of days that the medication was taken by the patient; was calculated. The patient was defined to be a full adherent if he had a PDC of at least 80%.17
Statistical Analysis
Data were analyzed using SPSS software (version 22, SPSS Inc., IL, USA). Continuous variables were presented as Mean ± SD. The independent samples t test and ANOVA followed by Tukey’s post-hoc test were used for comparing the different groups. The correlations between readmission and the demographic and clinical data were determined by the linear regression analysis. Spearman correlation was used to analyze relationships between medication adherence in the early and late periods between index admission and readmission in the ACS patients. A multivariate regression model with readmission as the dependent variable and medication non-adherence as the predictor variable was conducted with adjustment for cardiovascular disease risk factors. P values less than 0.05 were considered significant.
Results
Relation Between Readmission Rate and Demographic and Clinical Criteria
Of the 370 patients admitted at the study period, 79 had unplanned readmissions; thus, the patients were divided into index admission group (n = 291, 78.6%) and readmission group (n = 79, 21.4%). Of the 79 readmitted patients, the cardiovascular-related causes of readmission were heart failure, ST-elevated myocardial infarction, unstable angina, cerebrovascular accident, and arrhythmia accounting for 22, 10, 39, 5, and 3 cases, respectively. Table 1 shows the participants’ demographic characteristics and risk factors. The body mass index (BMI) was significantly higher in the readmission group. Table 2 shows the linear regression analysis between age, gender, weight, height, BMI, smoking, hypertension, diabetes mellitus, and low-density lipoprotein (LDL) level as predictor variables and readmission rate as a dependent variable. The coefficient of determination (R2) showed significant values with smoking, hypertension, cerebrovascular accident, ischemic heart disease, previous stent, and instent restenosis, while they showed non-significant values with the other predictors indicating absent or poor correlation.
 |
Table 1 The Participants’ Demographic and Clinical Criteria |
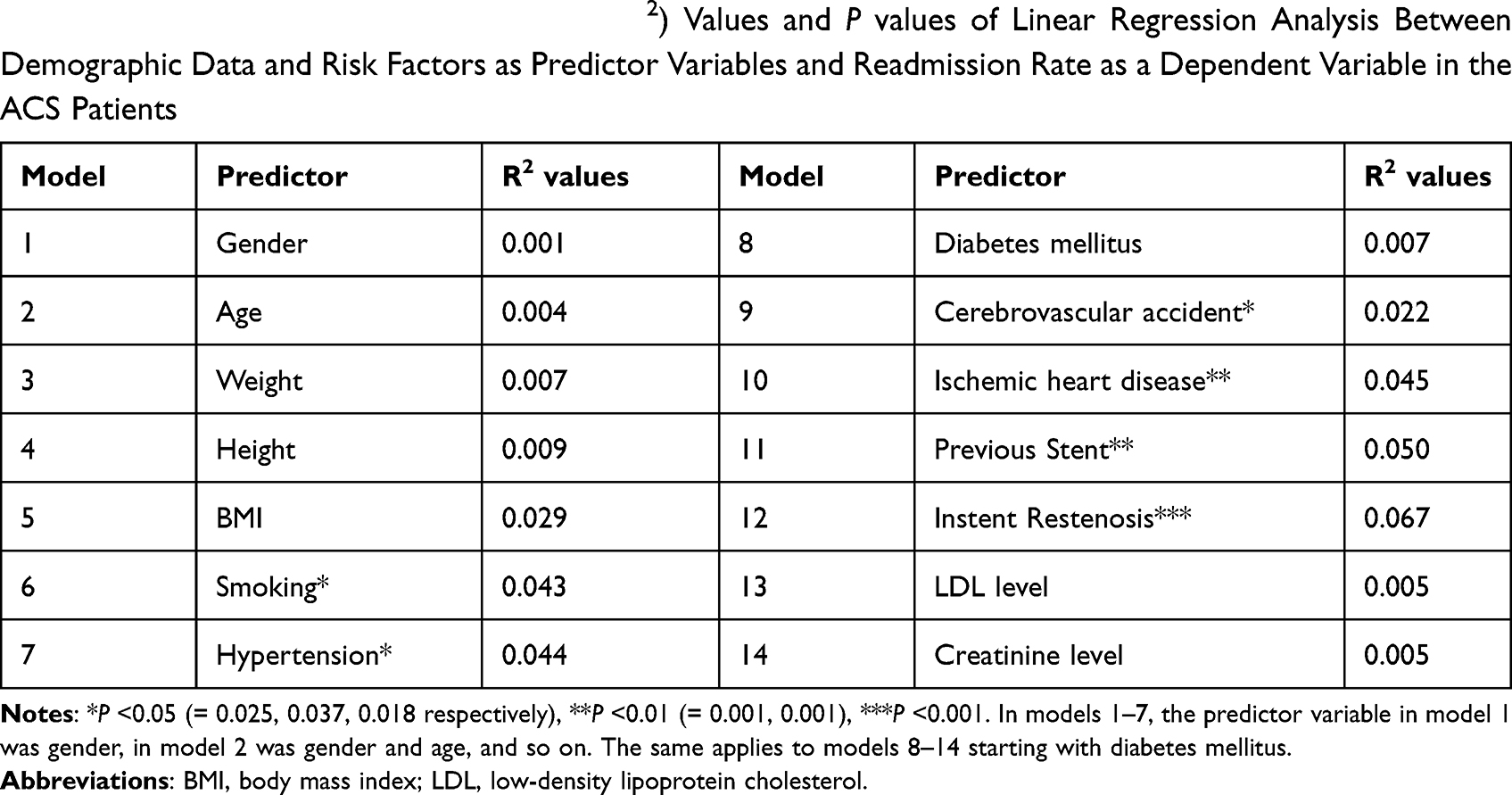 |
Table 2 The Coefficient of Determination (R2) Values and P values of Linear Regression Analysis Between Demographic Data and Risk Factors as Predictor Variables and Readmission Rate as a Dependent Variable in the ACS Patients |
Relation Between Readmission During the Four Post-ACS Discharge Time Frames and Medication Adherence
The overall medication adherence rate was 62.03% and the individual adherence rates decreased with time during the late three post-ACS discharge periods, but the adherence rate in the early first period was lower than that of the second period. Similarly, the individual readmission rates decreased with time during the late three post-ACS discharge periods, but the readmission rate in the early first period was lower than that of the second period. There was a strong significant correlation between the overall medication non-adherence rate and readmission rate. Also, strong significant correlations were detected between the individual medication non-adherence rates and readmission rates during the four post-ACS discharge periods (Table 3 and Figure 1).
 |
Table 3 The Frequencies and Percentages of Medication Adherence and Readmission Rates During the Four Post-ACS Discharge Periods |
 |
Figure 1 Frequencies of medication adherence and readmission rates during the four post-ACS discharge periods. |
In addition, in the readmission group, a multivariate regression model analysis with readmission as the dependent variable and medication non-adherence as the predictor variable was made with adjustment for cardiovascular disease risk factors. The analysis showed smaller values of Wilks lambda and significant values with ischemic heart disease and LDL level indicating more discriminatory ability of these predictors (Table 4).
 |
Table 4 The Wilks Lambda (WL) and P values of Multivariate Regression Model Analysis Between Readmission Rate as the Dependent Variable and Medication Non-Adherence as the Predictor Variable with Adjustment to Cardiovascular Disease Risk Factors in the Readmission Group (n = 79) |
Discussion
Hospital readmission of patients with ACS is related to numerous factors including type of treatment and adherence to secondary prevention medications. Data from 48 Ministry of Health hospitals in Saudi Arabia from 2016 to 2019 showed that ischemic heart disease was the most prevalent cardiovascular cause of readmission. A machine-learning model can be utilized to identify cardiovascular patients with a high risk of readmission.18 In patients over 65 years with acute myocardial infarction, the readmission rate within one year of hospital discharge was 49.9% and the amounts of readmission and mortality were higher in the early months post-discharge but decreased later. The risk trajectories varied by discharge diagnosis and outcome and thus to reduce adverse outcomes, patients should stay vigilant for health deterioration post discharge with proper medical support.19
In a retrospective study conducted to determine the rate and risk factors for 30-day readmission in internal medicine department at King Abdulaziz University Hospital, 678 of 3838 patients (18%) had readmission. Patients were 52 ± 21.2 years-old and more likely females. The risk factors included DM, hypertension, bed sores, stroke, and sepsis.20 In a retrospective study for patients admitted for heart failure to King Abdulaziz Medical City in Saudi Arabia, the 30 and 90-day readmission amounts of HF were 39.6% and 37.6%. The significant predictors for 30-day readmission were hypertension, chronic kidney disease, hypothyroidism, and pulmonary diseases, while those for 90-day readmission included BMI, dyslipidemia, renal dysfunction, dysrhythmias, and lung diseases.21 Another cross-sectional study at Prince Sultan Military Medical City, Saudi Arabia with 213 patients showed that the rate of readmission to hospital by home health care patients was 43.66%. Most of the readmitted patients were 75–85 years old and nearly 60% of them were males. Polypharmacy and diabetes mellitus (DM) were the most frequent causes of readmission.22 In a recent retrospective study, the medication-related readmissions within 30 days post discharge in older patients (≥65 years) were common accounting for 20–40% of hospital readmissions. The risk factors included polypharmacy and potentially inappropriate medication therapy or regimens. This indicates the importance of care planning before discharge and managing medications post discharge to decrease the rate of medication-related readmissions.23
Disappointingly, the patient adherence to the secondary prevention medications after ACS is low, ranging between 40% and 75% in different studies.24,25 Many factors are responsible including lack of motivation and education about medications, forgetfulness, polypharmacy, and low practical support. Utilizing technology like computer-based education and mobile phone reminders is an evolving strategy to improve adherence in patients with ACS.6 In a recent systematic review, it was reported that adherence to secondary prevention medications after ACS is suboptimal. Women with ACS had poorer adherence to statins than men, but no gender-related differences were reported regarding adherence to antiplatelets, inhibitors of the renin angiotensin system, and beta blockers.26 In another study, ACS patients with 90% adherence to beta blockers had a lower risk of major adverse cardiovascular events compared to those with <90% adherence, but no significant associations were found between non-adherence to statins or the renin angiotensin system inhibitors and the adverse outcomes.27 In a study on 216 patients to identify the predictors for readmission to help in planning and guiding hospital discharge, the incidence of readmission was 15.7% and only 50% of the patients were highly adherent to medications. Most patients were males with a mean age of 60 years and the risk factors were sedentary lifestyle and hypertension. Surgical treatment was the only independent predictive factor for readmission.28 A recent study showed that 1 in 7 and 3 in 4 patients were readmitted after percutaneous coronary intervention within 30 days and beyond 3 years. Interventions like discharge checklists and assessment of medication adherence at follow-up should be implemented to decrease readmissions.29 In a pilot randomized clinical trial, the four-item Morisky Medication Adherence Scale was used to evaluate medication adherence at 30 days and one year post discharge. The medication adherence decreased after the first month and readmission and mortality rates were related to low adherence.30 In a cross-sectional study on 250 patients with ACS, it was found that 5.6%, 58%, and 36.4% of the patients had high, moderate, and poor medication adherence post-discharge indicating that the medication adherence rate was mostly poor to moderate.31 Low adherence to medications significantly affects the frequency of readmissions and mortality.30 In a study of 536 patients with ACS, the readmission rate was 21.4% with ACS and heart failure as the main causes of readmission. However, using a hospital-based sample without complete follow-up data is a limitation, thus patients should remain vigilant for health deterioration post ACS discharge.32 More successful therapy will reduce clinical deterioration which requires hospital re-admissions.33
Generally, barriers to medication adherence include patient-related, medication-related, and disease-related factors in addition to socioeconomic and healthcare system factors.34 Improving medication adherence in cardiovascular medicine improves clinical outcomes and decreases healthcare costs.35 Providing reminders via smartphones, repeat contacts (visits/follow up) with the patients, and reducing medication cost seemed to be effective methods to improves adherence.8 The guidelines of the American College of Cardiology and American Heart Association give a class I recommendation for patients with ischemic heart diseases to have treatment plans promoting medication adherence during hospitalization, before discharge, and at follow-up visits.36,37 Also, the 2018 guideline on management of blood cholesterol gives a class I recommendation for interventions to improve adherence like telephone reminders and simplification of the drug regimen.38 These recommendations indicate importance of medication adherence in ischemic heart diseases, however implementation of these guidelines into clinical practice requires strong resource commitment from healthcare providers to significantly affect adherence and clinical outcomes.8
Adherence to antiplatelets among ACS patients was quite high at the first month, but begins to decline by 6 months, 12 months, and more than 12 months. The patients who have average monthly income, can easily reach the hospital, and have timely re-examination, were more adherent to therapy.11 However, even with relatively comprehensive claims data on patients, physicians, and costs, the ability to explain adherence is still poor indicating that administrative data most likely do not capture numerous complicated mechanisms underlying adherence.17
Strengths of this work included study of readmission over four time frames extending from the first month to 1.5 years post-ACS discharge. Secondly, all potential confounders including age, sex, and clinical characteristics were adjusted. Also, we used a common measure of adherence; the proportion of days covered (PDC); which is the number of days that the medication was taken by the patient. However, the study has important limitations. First, medication adherence was assessed by a single question at readmission, and not by using the Morisky Medication Adherence Scale30 or the Brief Medication Questionnaire39 because there are no validated Arabic versions of these scales. However, using a single question could be a suitable way for screening, for example, a single-question test for drug use was validated as a screening test in a sample of primary care patients.40 Second, patient self-reporting is an easier but less reliable measure compared with the direct method of estimating medication non-adherence and thus misclassification of some patients may have occurred, and this underestimates the strength of the associations observed. Side effects of medications were not recorded because this work did not aim to detect the causes of medication non-adherence, however this is considered a third limitation of the study. A fourth limitation is that lipoprotein (a) is not estimated because its levels are extremely variable, under strict genetic control, and are difficult to manipulate.41 Finally, the results of the current study were limited by the cross-sectional study design, the relatively short duration (1.5 year), and the relatively small sample size.
Conclusion
The cardiovascular-related readmission rate after discharge of acute coronary syndrome patients was 21.4%. The causes were heart failure, ST-elevated myocardial infarction, unstable angina, cerebrovascular accident, and arrhythmia. The increased body mass index, smoking, hypertension, and cerebrovascular accident, ischemic heart disease, previous stent, instent restenosis, and LDL-cholesterol were significant risk factors. The overall medication adherence rate was 62.03%. The individual adherence rates and readmission rates in the periods of 1–18 months after discharge decreased by time, but in the first month, both rates were lower than the following 5 months indicating that factors other than medication non-adherence play important roles in readmission. Finally, although the rates are generally acceptable and compatible with the reported international rates, utilizing technology like computer-based education and mobile phone reminders can improve medication adherence in patients with ACS and reduce readmission rates.
Abbreviations
ACS, acute coronary syndrome; AMI, acute myocardial infarction; CHF, congestive heart failure; BMI, body mass index; LDL, low-density lipoprotein.
Data Sharing Statement
Data supporting the results reported in the manuscript can be obtained from the corresponding author on a reasonable request.
Acknowledgments
Disclosure
The authors declare that they have no conflicts of interest.
References
1. LaPointe J. Strategies to reduce hospital readmission rates, costs; 2019.
2. Centers for Medicare & Medicaid Services. 2015 measure information about the 30-day all-cause hospital readmission measure, calculated for the value-based payment modifier program; 2018.
3. Fingar K, Washington R. Trends in Hospital Readmissions for Four High-Volume Conditions, 2009–2013: Statistical Brief #196. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006.
4. Southern DA, Ngo J, Martin BJ, et al. Characterizing types of readmission after acute coronary syndrome hospitalization: implications for quality reporting. J Am Heart Assoc. 2014;3(5):e001046. doi:10.1161/JAHA.114.001046
5. Chin DL, Bang H, Manickam RN, et al. Rethinking thirty-day hospital readmissions: shorter intervals might be better indicators of quality of care. Health Affairs. 2016;35(10):1867–1875. doi:10.1377/hlthaff.2016.0205
6. Cheng K, Ingram N, Keenan J, et al. Evidence of poor adherence to secondary prevention after acute coronary syndromes: possible remedies through the application of new technologies. Open Heart. 2015;2(1):e000166. doi:10.1136/openhrt-2014-000166
7. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
8. Simon ST, Kini V, Levy AE, et al. Medication adherence in cardiovascular medicine. BMJ. 2021;374:n1493. doi:10.1136/bmj.n1493
9. Rosenbaum L. Beyond belief–how people feel about taking medications for heart disease. N Engl J Med. 2015;372(2):183–187. doi:10.1056/NEJMms1409015
10. Xie G, Sun Y, Myint PK, et al. Six-month adherence to Statin use and subsequent risk of major adverse cardiovascular events (MACE) in patients discharged with acute coronary syndromes. Lipids Health Dis. 2017;16(1):155. doi:10.1186/s12944-017-0544-0
11. Luu NM, Dinh AT, Nguyen TTH, et al. Adherence to antiplatelet therapy after coronary intervention among patients with myocardial infarction attending Vietnam national heart institute. Biomed Res Int. 2019;2019:6585040. doi:10.1155/2019/6585040
12. Tomaszewski M, White C, Patel P, et al. High rates of non-adherence to antihypertensive treatment revealed by high-performance liquid chromatography-tandem mass spectrometry (HP LC-MS/MS) urine analysis. Heart. 2014;100(11):855–861. doi:10.1136/heartjnl-2013-305063
13. Kubica A, Kosobucka A, Fabiszak T, et al. Assessment of adherence to medication in patients after myocardial infarction treated with percutaneous coronary intervention. Is there a place for newself-reported questionnaires? Curr Med Res Opin. 2019;35(2):341–349. doi:10.1080/03007995.2018.1510385
14. Cutler RL, Fernandez-Llimos F, Frommer M, et al. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
15. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. doi:10.1016/j.jacc.2013.05.019
16. Arnold SV, Spertus JA, Tang F, et al. Statin use in outpatients with obstructive coronary artery disease. Circulation. 2011;124(22):2405–2410. doi:10.1161/CIRCULATIONAHA.111.038265
17. Chan DC, Shrank WH, Cutler D, et al. Patient, physician, and payment predictors of statin adherence. Med Care. 2010;48(3):196–202. doi:10.1097/MLR.0b013e3181c132ad
18. Alzeer AH, Althemery A, Alsaawi F, et al. Using machine learning to reduce unnecessary rehospitalization of cardiovascular patients in Saudi Arabia. Int J Med Inform. 2021;154:104565. doi:10.1016/j.ijmedinf.2021.104565
19. Dharmarajan K, Hsieh AF, Kulkarni VT, et al. Trajectories of risk after hospitalization for heart failure, acute myocardial infarction, or pneumonia: retrospective cohort study. BMJ. 2015;350:h411. doi:10.1136/bmj.h411
20. Fallatah HI, Bajunaid NF, Jawa HA, et al. Readmission within 30-day as a key indicator for academic hospital performance: rate and risk factors. Saudi J Internal Med. 2019;9(1):29–35. doi:10.32790/sjim.2019.9.1.5
21. Aldihan DA, Alghafees MA, Alharbi RO, et al. Readmission rates of heart failure and their associated risk factors in a tertiary academic medical city in Riyadh, Saudi Arabia. J Nat Sci Med. 2021;4(1):64. doi:10.4103/JNSM.JNSM_57_20
22. Alruwaili L, Alsaid T, Kofi M. Risk factors for hospital readmission among home health care patients at PSMMC, Riyadh, Saudi Arabia. Age. 2019;18(25):6.
23. Glans M, Kragh Ekstam A, Jakobsson U, et al. Medication-related hospital readmissions within 30 days of discharge—A retrospective study of risk factors in older adults. PLoS One. 2021;16(6):e0253024. doi:10.1371/journal.pone.0253024
24. Desai NR, Choudhry NK. Impediments to adherence to post myocardial infarction medications. Curr Cardiol Rep. 2013;15(1):322. doi:10.1007/s11886-012-0322-6
25. Jackevicius CA, Li P, Tu JV. Prevalence, predictors, and outcomes of primary nonadherence after acute myocardial infarction. Circulation. 2008;117(8):1028–1036. doi:10.1161/CIRCULATIONAHA.107.706820
26. Bots SH, Inia JA, Peters SAE. Medication adherence after acute coronary syndrome in women compared with men: a systematic review and meta-analysis. Front Glob Women’s Health. 2021;2:637398. doi:10.3389/fgwh.2021.637398
27. Chinwong S, Doungsong K, Channaina P, et al. Association between medication adherence and cardiovascular outcomes among acute coronary syndrome patients. RSAP. 2021;17(9):1631–1635. doi:10.1016/j.sapharm.2021.01.003
28. Lopes J, Russomanno L, Lopes C. Factors related to hospital readmission of patients with acute coronary syndrome: a prospective cohort study. Eur Heart J. 2021;42(Supplement_1):
29. Kwok CS, Narain A, Pacha HM, et al. Readmissions to hospital after percutaneous coronary intervention: a systematic review and Meta-analysis of factors associated with readmissions. Cardiovasc Revascul Med. 2020;21(3):375–391. doi:10.1016/j.carrev.2019.05.016
30. Oliveira-Filho AD, Morisky DE, Costa FA, et al. Improving post-discharge medication adherence in patients with CVD: a pilot randomized trial. Arq Bras Cardiol. 2014;103(6):503–512. doi:10.5935/abc.20140151
31. Dianati M, Taghadosi M. Medication adherence rate and related factors in patients with acute coronary syndrome after discharge from Shahid Beheshti Hospital in Kashan during 2017–2018. KAUMS J. 2019;23(2):201–208.
32. Oliveira L, Costa I, Silva DGD, et al. Readmission of patients with acute coronary syndrome and determinants. Arq Bras Cardiol. 2019;113(1):42–49. doi:10.5935/abc.20190104
33. Mansur AJ. Hospital readmissions after acute coronary syndromes. Arq Bras Cardiol. 2019;113(1):50–51. doi:10.5935/abc.20190136
34. World Health Organization. Sabate E: Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland; 2009.
35. Sokol MC, McGuigan KA, Verbrugge RR, et al. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43(6):521–530. doi:10.1097/01.mlr.0000163641.86870.af
36. Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929–1949. doi:10.1016/j.jacc.2014.07.017
37. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with Non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228. doi:10.1016/j.jacc.2014.09.017
38. Williams B, Mancia G, Spiering W, et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC task force for the management of arterial hypertension. J Hypertens. 2018;36(12):2284–2309. doi:10.1097/HJH.0000000000001961
39. Turner RM, Yin P, Hanson A, et al. Investigating the prevalence, predictors, and prognosis of suboptimal statin use early after a non-ST elevation acute coronary syndrome. J Clin Lipidol. 2017;11(1):204–214. doi:10.1016/j.jacl.2016.12.007
40. Smith PC, Schmidt SM, Allensworth-Davies D, et al. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170(13):1155–1160. doi:10.1001/archinternmed.2010.140
41. McCormick SP. Lipoprotein(a): biology and clinical importance. Clin Biochem Rev. 2004;25(1):69–80.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Illness Perception and Medication Adherence Trajectories in Patients with Acute Coronary Syndrome: A 6-Month Longitudinal Study
Xue Q, Wu C, Qu G, Chen Y, Zeng X, Han R
Patient Preference and Adherence 2026, 20:609941
Published Date: 20 May 2026