Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Identification of the MC4R start lost mutation in a morbidly obese Brazilian patient
Authors Fonseca ACP ![]() , Abreu GM, Zembrzuski VM
, Abreu GM, Zembrzuski VM ![]() , Campos Junior M
, Campos Junior M ![]() , Carneiro JRI
, Carneiro JRI ![]() , Magno FCCM, Rosado EL
, Magno FCCM, Rosado EL ![]() , Nogueira Neto JF
, Nogueira Neto JF ![]() , Cabello GMK
, Cabello GMK ![]() , Cabello PH
, Cabello PH ![]()
Received 2 October 2018
Accepted for publication 15 November 2018
Published 21 February 2019 Volume 2019:12 Pages 257—266
DOI https://doi.org/10.2147/DMSO.S189455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Ana Carolina Proença da Fonseca,1 Gabriella de Medeiros Abreu,1 Verônica Marques Zembrzuski,1 Mario Campos Junior,1 João Regis Ivar Carneiro,2 Fernanda Cristina C Mattos Magno,3 Eliane Lopes Rosado,3 José Firmino Nogueira Neto,4 Giselda Maria Kalil de Cabello,1 Pedro Hernán Cabello1,5
1Human Genetics Laboratory, Oswaldo Cruz Institute, Oswaldo Cruz Foundation (FIOCRUZ), Rio de Janeiro, Brazil; 2Clementino Fraga Filho University Hospital, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; 3Institute of Nutrition Carlos Chagas Filho, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; 4Department of Pathology and Laboratory, Rio de Janeiro State University, Rio de Janeiro, Brazil; 5Human Genetics Laboratory, Grande Rio University, Rio de Janeiro, Brazil
Background: Melanocortin 4 receptor gene (MC4R) is an important regulator of food intake, body weight, and blood pressure. Mutations in MC4R are associated with the most common form of nonsyndromic monogenic obesity. MC4R variations have an autosomal co-/dominant model of inheritance. MC4R screening could reveal individuals previously unrecognized with Mendelian form of obesity for further clinical management and genetic counseling. However, there are limited data regarding MC4R variants in patients with obesity from Brazil. The aim of this study was to screen the coding region of the MC4R gene in a Brazilian cohort of severely obese adults and to investigate the phenotype–genotype correlation within MC4R variant carriers.
Methods: This study comprised 157 adult participants, stratified according to the period of obesity onset. The first group included 97 patients with childhood-onset obesity (0–11 years) and the second group comprised 60 subjects with adolescence/youth-onset obesity (12–21 years). The entire coding region of MC4R gene was screened by Sanger sequencing.
Results: As a result, five previously described variants (Met1?, Ser36Thr, Val103Ile, Ile98=, and Phe202Leu) were identified. Met1? is a start lost codon variant, which affects the translation of MC4R. It was found in a female patient with childhood-onset obesity. We also compared the anthropometric and metabolic parameters between patients with MC4R missense variants (Ser36Thr, Val103Ile, and Phe202Leu) and noncarriers. Patients carrying MC4R variants had higher median of waist–hip ratio when compared to noncarriers (P=0.048). These missense variants were also associated with hypertension (P=0.014). Additionally, Val103Ile carriers had lower diastolic blood pressure and lower systolic blood pressure compared to noncarriers (P=0.020 and P=0.065, respectively). Val103Ile was also associated with hypertension (P=0.003).
Conclusion: This study showed the prevalence of MC4R variants in a cohort of Brazilian adults with severe obesity. We also identified significant phenotype differences between carriers and noncarriers of missense variants in our sample, suggesting an important role of MC4R on body fat distribution and blood pressure.
Keywords: MC4R, severe obesity, mutation, start lost, blood pressure
Introduction
Obesity is an increase in the body fat mass defined by a body mass index (BMI) >30 kg/m2. This disease has emerged as a major public health problem worldwide, affecting populations from developed and developing countries. In 2016, there were >650 million adults and 124 million children and adolescents with obesity in the world.1 In Brazil, 11.9 million men and 18.0 million women were obese in 2014.2 Clinically severe or morbid obesity is characterized as BMI ≥35 kg/m2 with at least one obesity-related comorbidity (such as type 2 diabetes, metabolic syndrome, and hypertension); or BMI ≥40 kg/m2.3 It affects 0.64% (0.46–0.86) of men and 1.6% (1.3–1.9) of women in the world.2 This extreme BMI causes a substantial increased risk for comorbidities and mortality, lowering the life expectancy of the patients in 6.5–13.7 years.1,2,4
The etiology of obesity is multifactorial, caused by an interaction of environmental factors with many variants of minor effect in multiple genes; however, rare monogenic forms caused by mutations with major effect in a single gene were also identified.5 Among the monogenic types of nonsyndromic obesity, mutations in melanocortin 4 receptor gene (MC4R) are considered the most common cause of this disorder (OMIM*155541).6 MC4R variations have an autosomal co-/dominant model of inheritance, with a high degree of expressivity and penetrance.5
MC4R gene is localized on chromosome 18q21.3. It spans >1.6 kb and its only one exon encodes a 332 amino acid G-protein-coupled seven-transmembrane-domain receptor. MC4R is expressed in several areas of the brain, including the hypothalamus, which has an important role on food intake and body weight regulation. Activation of MC4R by α-melanocyte-stimulating hormone increases satiety signaling in the brain and decreases appetite.7,8 In this context, the dysfunctions of MC4R result in hyperphagia and early-onset obesity, making it a potential drug target for the treatment of obesity.9,10
In addition, activation of central nervous system melanocortin pathway appears to contribute to the development of hypertension in obese subjects.11 Rodents with hypertension have reduced arterial pressure when MC4R was blocked, despite exhibiting hyperphagia and obesity.12 Furthermore, acute central administration of MC4R agonist increased blood pressure and heart rate.13 In humans, MC4R-deficient individuals showed lower blood pressure, heart rate, and prevalence of hypertension when compared to controls. This study also showed that MC4R agonist increases the blood pressure in overweight and obese subjects. These higher levels were sustained during the 7 days of the drug’s administration.14 All these findings suggest that MC4R has an important role in regulating not only the energy balance but controlling the blood pressure as well.15
Epidemiologic data have estimated that 0.05% individuals have variations in MC4R in general population.16,17 Furthermore, the prevalence of MC4R variants in adult with obesity is 0.2% and ~5%–6% in patients with severe early-onset obesity.18,19 However, the prevalence of these mutations varies according to the ethnic composition of the population studied.20 Currently, data available regarding rare genetic variants in MC4R gene and their associations with monogenic obesity in the Brazilian population are limited. Therefore, the aim of this study was to determine the prevalence of MC4R variants in a cohort of severely obese adults, which developed obesity during the childhood or adolescence/youth. We also investigated the phenotype–genotype correlation within MC4R variant carriers.
Materials and methods
Study population
This study comprised 157 unrelated individuals (71.1% female and 22.9% male), aged 18–65 years (median of age, 36.0 [28.0; 43.0]), from Rio de Janeiro, southeast of Brazil. The selection criteria were severe/morbid obesity (BMI ≥35 kg/m2 with at least one obesity-related comorbidity or BMI ≥40 kg/m2) with childhood onset (0–11 years) or adolescence/youth onset (12–21 years). The period of onset was self-reported. The exclusion criteria were pregnancy; lactation; the use of medication to lose or gain weight; and the presence of known symptoms suggestive of obesity-related syndromes. The cohort was divided in two groups according to the age of onset. The first group comprised 97 patients with childhood-onset obesity and the second group comprised 60 patients with adolescence/youth-onset obesity. All participants were recruited from a nongovernmental organization, called Rescue Group to Self-Esteem and Citizenship of the Obese (in Portuguese, “Grupo de Resgate à Autoestima e Cidadania do Obeso”). Those patients are candidates to undergo bariatric surgery in Brazil. The study was carried out according to the Declaration of Helsinki (1964) and the protocol was approved by Ethics Committee of the Oswaldo Cruz Foundation. All participants have consented to participate and provided written informed consent prior to their inclusion in this study.
Biochemical, anthropometric, and blood pressure measurements
The measurement of height, body weight, and waist and hip circumferences was made according to classical methods.21 Briefly, waist circumference was evaluated at the midpoint between the iliac crest and the last costal arch and hip circumference was measured at the level of the greater trochanters. BMI and waist–hip ratio (WHR) were then calculated for each participant.
Glucose, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), and triglyceride (TG) were measured by oxidase-peroxidase method (BioSystems), after an overnight fast. C-reactive protein was evaluated using latex agglutination method and hemoglobin glycated was measured by turbidimetric inhibition immunoassay. Low-density lipoprotein cholesterol (LDL-c) was calculated by Friedewald formula (LDL-c = TC – HDL-c – TG/5). Participants using medication for these biochemical parameters had their levels excluded from statistical analysis. We also measured blood pressure with the subject seated using wrist blood pressure monitor. Hypertension was diagnosed by blood pressure ≥140 × 90 mm Hg, or use of antihypertensive drug therapy.22 In addition, we also used the new classification, in which adults with blood pressure ≥130 × 80 mm Hg are considered having stage 1 hypertension.23 Additional information was obtained from patients with pathogenic MC4R variants, including dietary intake; physical activity; binge eating assessment; and insulin, leptin, and ghrelin measurements. This information was obtained as described by Magno et al.21
Screening of MC4R gene
Genomic DNA was extracted from peripheral blood using QIAamp Blood Kit (Qiagen, Valencia, CA, USA). The coding region of MC4R gene was screened using Sanger automatic sequencing. These regions were amplified using two sets of custom-designed primers with Primer3Plus software (Table S1). Reactions were carried out in a total volume of 10 µL, which included 10–20 ng of genomic DNA, 1 unit of AmpliTaq Gold (Thermo Fisher Scientific, Waltham, MA, USA), 1× AmpliTaq buffer, 0.2 mmol/L of each DNTP, 0.3 pmole of each primer, and 2 mmol/L MgCl2. Amplification of the first set of primers was performed under following conditions: 95°C for 10 minutes, followed by 35 cycles of 94°C for 1 minute, 60°C for 1 minute, and 72°C for 1 minute; then an elongation step of 72°C for 10 minutes. For the second set of primers, the only difference was in the annealing temperature step, which was 62°C. Amplicons were visualized on 1.5% agarose gels and purified using Sweep Clean up kit (Thermo Fisher Scientific).
The products of PCR were directly sequenced using Big Dye Terminator kit v.3.1 on 3730xl DNA analyzer (Thermo Fisher Scientific). Reactions were carried out in a final volume of 10 µL, containing 10–40 ng of PCR products, 1× sequencing buffer, 1.0 µL Big Dye, and 0.32 pmole of primer. The sequencing of products was performed by following conditions: 40 cycles of 94°C for 10 seconds, 50°C for 5 seconds, and 60°C for 4 minutes. DNA sequences were analyzed and aligned with the reference sequence provided by the National Center for Biotechnology Information (Accession number: NM_005912.2) using the software SeqScape version 2.1 (Thermo Fisher Scientific). Detected MC4R mutations were confirmed by bidirectional sequencing of a second PCR reaction.
Bioinformatic tools
MC4R genomic, transcript, and protein sequences were obtained through the National Center for Biotechnology Information (https://www.ncbi.nlm.nih.gov/) and Ensembl database (http://www.ensembl.org/). The pathogenicity of variants was evaluated using Polyphen (Polymorphism Phenotyping) and SIFT (Sorting Intolerant From Tolerant) softwares and interpreted according to current standards and guidelines.24 Additionally, open reading frames (ORFs) were explored using prediction interface in ORFinder (https://www.ncbi.nlm.nih.gov/orffinder/).
Statistical analyses
Descriptive statistics were expressed as median (IQR 25%–75%) and n (%). Mann–Whitney and chi-squared tests were used to compare quantitative and qualitative variables, respectively. P-value <0.05 was considered statistically significant. Data were analyzed using SPSS statistical package (IBM Corporation, Chicago, IL, USA).
Results
Basic characteristics of study population
Subject characteristics from the 157 patients are shown in Table 1. No differences of anthropometric, biochemical, and blood pressure measurements were observed between the categorized groups.
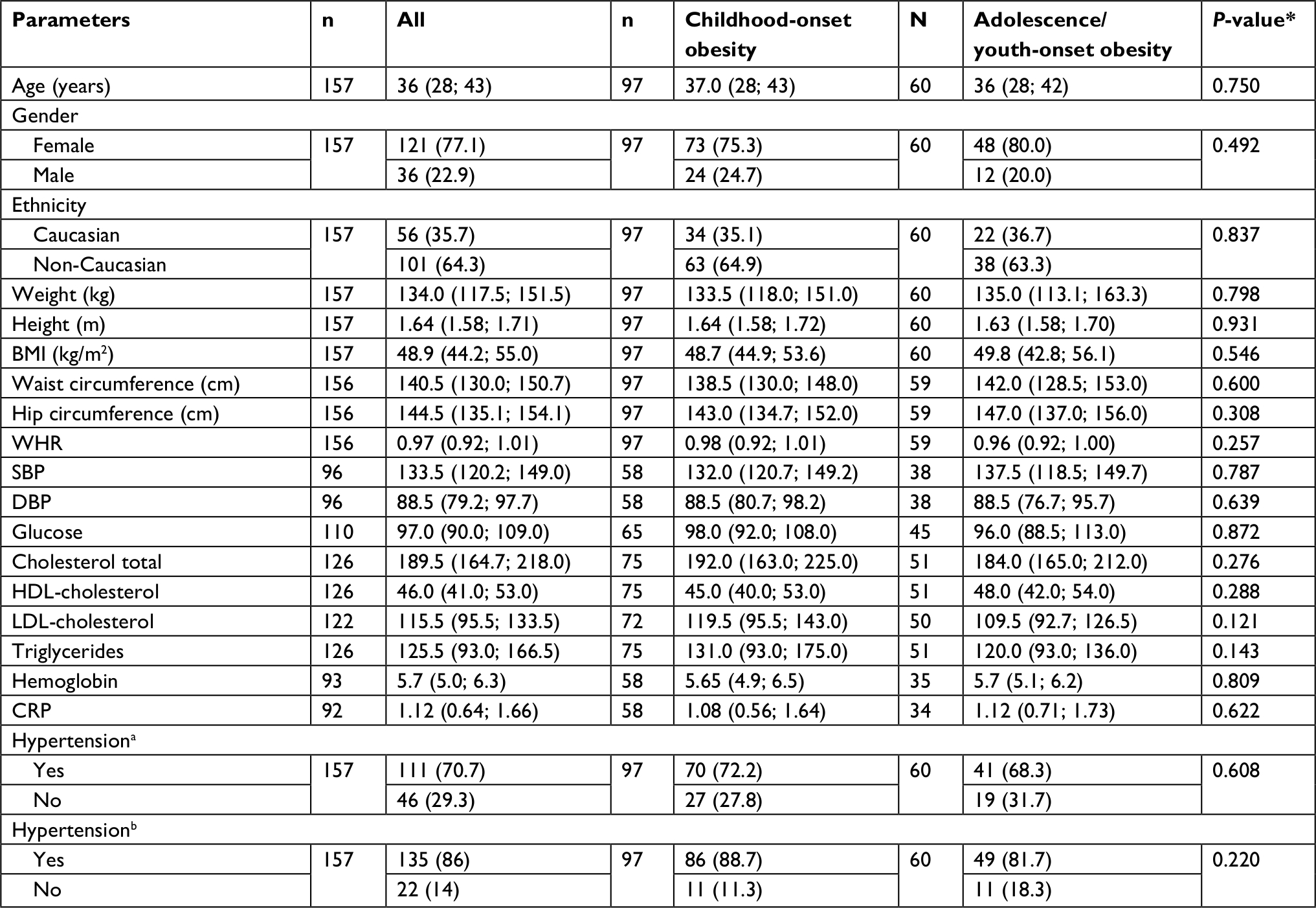 | Table 1 Clinical characterization of the study participants from Brazilian cohort Notes: Data are presented as median values (IQR 25%–75%) for continuous traits and n (%) for categorical traits. Data were analyzed by Mann–Whitney test (for non-normally distributed variables) or chi-squared test (for categorical variables). aHypertension – based on blood pressure ≥140 × 90 mm Hg. bHypertension – based on blood pressure ≥130 × 80 mm Hg. *P-value for differences between case and control subjects. Abbreviations: BMI, body mass index; CRP, C-reactive protein; DBP, diastolic blood pressure; HDL-cholesterol, high-density lipoprotein-cholesterol; LDL-cholesterol, low-density lipoprotein-cholesterol; SBP, systolic blood pressure; WHR, waist–hip ratio. |
Prevalence of MC4R variants in Brazilian adults with severe obesity
A total of five variants were detected, including one silent variant (Ile98=), three missense mutations (Ser36Thr, Val103Ile, and Phe202Leu), and one start codon mutation (Met1?) (Table 2). The electropherogram of these variants is shown in Figure 1. Two of those alterations (Val103Ile and Ile98=) are common polymorphisms. All individuals, except one participant, were heterozygous for the five variants. Two patients were compound heterozygous (Ile198=/Phe202Leu and Met1?/Val103Ile). In silico prediction was performed in order to evaluate the impact of these variants on MC4R. The effect of the Ser36Thr, Val103Ile, and Phe202Leu variants was reported as “Benign” and “Tolerated” by Polyphen and SIFT, respectively. Nevertheless, Met1? variant was predicted to be “deleterious” and “benign” by SIFT and Polyphen, respectively. The potential impact of this variant was also interpreted according to current standards and guidelines, which suggested that variant is pathogenic.24 To evaluate the impact of this mutation on MC4R synthesis, we have also analyzed the potential effect on ORFs using NCBI Bioinformatic tools. This analysis suggested that this variant impacts on original ORF, resulting in a second ORF that starts 8 amino acids (24 nucleotides) later.
 | Table 2 Identified variants in the coding region of MC4R gene Abbreviations: NA, not available; SIFT, Sorting Intolerant From Tolerant. |
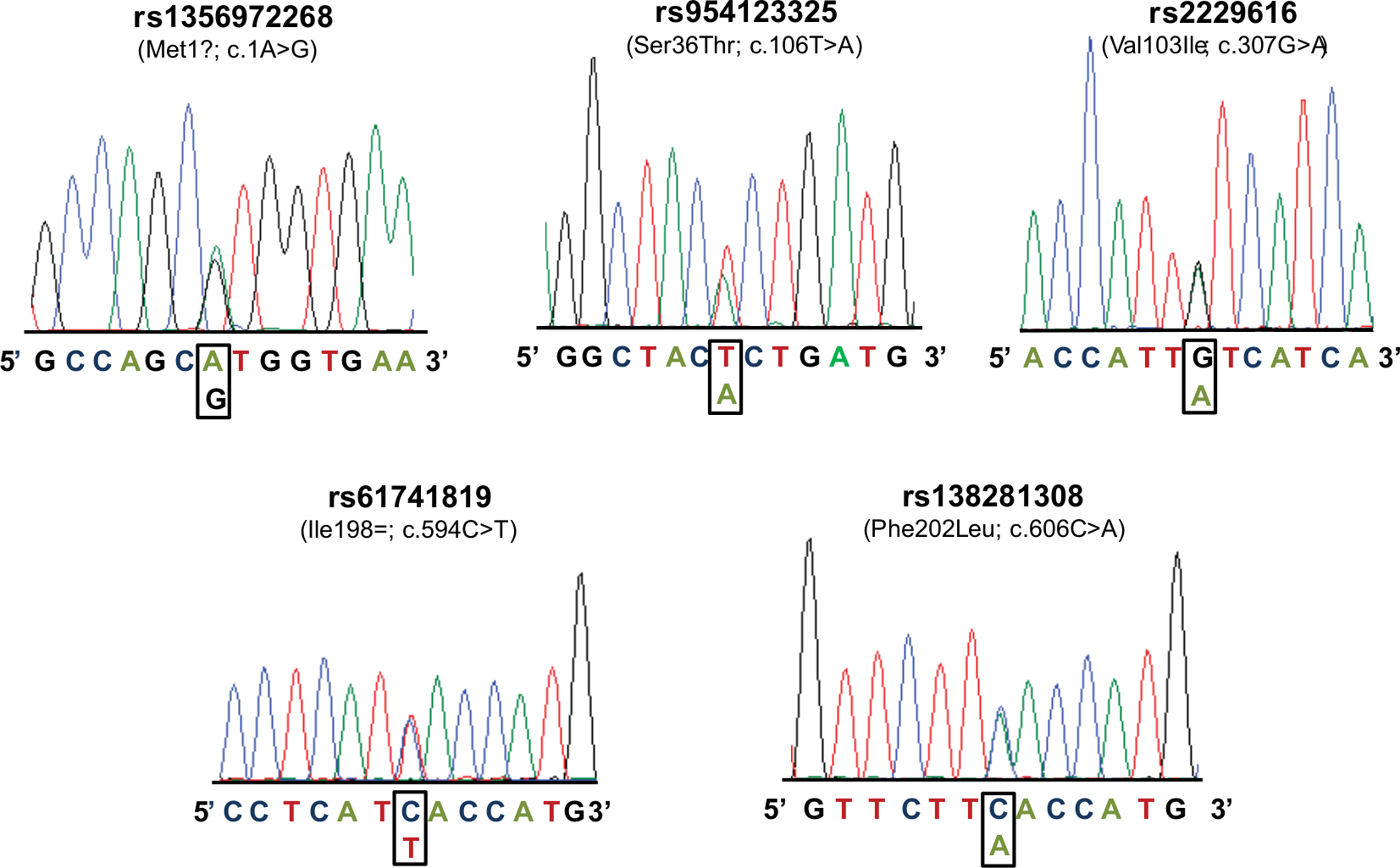 | Figure 1 Electropherogram of MC4R variants identified in this study. |
Phenotype–genotype correlation within MC4R variant carriers
A comparison of missense variants frequency (Ser36Thr, Val103Ile, and Phe202Leu) in patients with childhood vs adolescence/youth-onset obesity did not show any significant differences (3.1% vs 4.2%; P=0.651). Of these three mutations, two were specific for patients with childhood-onset obesity (Ser36Thr and Phe202Leu) and one was found in both groups (Val103Ile). The prevalence of Val103Ile polymorphism was higher in patients with adolescence/youth-onset obesity (4.2%) than in childhood-onset obesity (2.1%); however, this result was not significant (P=0.277).
We compared the anthropometric, biochemical, and blood pressure measurements, and the presence of hypertension among the carriers (n=10) and noncarriers (n=147) for the identified missense mutations. Our results showed that carriers had higher median WHR (0.99 [0.96; 1.05], n=10) than noncarriers (0.97 [0.92; 1.00], n=146) (P=0.048). No differences were found between the groups in biochemical and blood pressure measurements. We also observed that these missense variants were associated with hypertension (P=0.014) (Table S2). The same analyses were carried out using only the Val103Ile carriers (n=8), because it has the higher frequency in our sample. The results showed that individuals carrying the missense mutation had lower median diastolic blood pressure (DBP) (73.0 [68.0; 90.0], n=7) when compared to noncarriers (89.0 [81.0; 98.5]; n=89) (P=0.020). Interestingly, a similar tendency was also observed in systolic blood pressure (SBP),, in which Val103Ile carriers (116.0 [107.0; 140.0], n=7) had lower median than noncarriers (135.0 [121.5; 150.0]; n=89) (P=0.065). This variant was also associated with hypertension (P=0.003). No differences were found between the groups in anthropometric and biochemical parameters (Table S2).
Phenotypic characterization of the Met1?, Ser36Thr, and Phe202Leu carriers
Met1? was identified in a 29-year-old female patient with childhood-onset obesity. On anthropometric examination, her current and maximum weight was 116.8 kg; height, 1.54 m; BMI, 49.2 kg/m2; waist circumference, 137 cm; hip circumference, 143 cm; WHR, 0.96; and neck circumference, 36.5 cm. Her blood pressure was 124/74 mm Hg. We also analyzed biochemical parameters. Her glucose was 86 mg/dL; TC, 182 mg/dL; HDL-c, 49 mg/dL; LDL-c, 115 mg/dL; and TGs, 91 mg/dL. Serum leptin, ghrelin, and insulin levels were 27.1 pg/mL, 18.9 pg/mL, and 13.1 mcU/mL, respectively. She did not exhibit any comorbidities associated with obesity, such as metabolic syndrome, hypertension, and type 2 diabetes mellitus. She did not take any medicine. The patient reported family history of obesity. Her older sister underwent the bariatric surgery. The patient presented a moderate binge-eating disorder (BED) and was physically inactive. According to 3-day dietary records, the patient has consumed a median of 4,900 calories per day, distributed as 36.24% carbohydrates, 20.86% proteins, and 42.90% total fats (27% saturated fatty acid and 700 mg cholesterol). She has consumed low quantity of vitamins and minerals, with exception for sodium (10 g).
Ser36Thr mutation was found in a 59-year-old female patient with childhood-onset obesity. On clinical examination, her current and maximum weight was 112.9 kg; height, 1.55 m; BMI, 47 kg/m2; waist circumference, 136 cm; hip circumference, 127.5 cm; WHR, 1.07; and neck circumference, 50 cm. The blood pressure was 147/86 mm Hg. We also obtained biochemical measurements, in which TC, 144 mg/dL; HDL-c, 38 mg/dL; LDL-c, 72 mg/dL; and TGs, 171 mg/dL. The patient exhibited type 2 diabetes mellitus, metabolic syndrome, and hypertension. She takes medicine to control blood pressure and glucose. The patient reported family history of obesity (mother and son).
We also detected the Phe202Leu variant in a 41-year-old male patient with early-onset obesity. His current weight was 127 kg; however, the maximum weight was 207 kg. His BMI was 40.1 kg/m2; waist circumference, 138 cm; hip circumference, 125 cm; and WHR, 1.10. The blood pressure was 140/100 mm Hg. The biochemical measurements were not available. The patient exhibited hypertension and reported family history of obesity (sibling).
Discussion
The prevalence of obesity in Brazil has increased at alarming rates.1 Common forms of obesity, which are found in most patients, are caused by interaction of environmental factors and genetic variants with minor effect. However, it has been characterized that single gene mutation can cause a rare form of nonsyndromic obesity in human, being the MC4R deficiency considered the most common form in general population.5 Several rare variants were described in the coding region of MC4R gene, including deletions (n=6), frameshift (n=21), nonsense (n=24), and missense mutations (n=318).9 Pathogenic mutations could lead to complete or partial loss of function, which may impair receptor signaling through intracellular retention of the protein, reduced ligand binding, or reduced downstream signaling.9,25,26 In this present study, we aimed to investigate the prevalence of MC4R variants in a cohort of Brazilian patients. To our knowledge, this is the first study carrying a screening of the entire coding region of MC4R gene in our population.
As result, we identified five variants (Met1?, Ser36Thr, Val103Ile, Ile98=, and Phe202Leu) in our cohort of severely obese individuals, resulting in a carrier prevalence of 5.4%. Ser36Thr was found in one female patient with childhood-onset obesity (BMI: 47.0 kg/m2). Ser36Thr is located in the N-terminal domain of MC4R and was only found in obese individuals, suggesting a possible impact on MC4R functionality. Nevertheless, the effect of this variation on cAMP activity was shown to be neutral.27,28 We also detected the Phe202Leu variant in a male patient with childhood-onset obesity (BMI: 40.1 kg/m2). This variant is located in the fifth transmembrane domain of MC4R and was found in compound heterozygosity with Ile98=. Previous functional study showed that Phe202Leu decreased basal receptor activity.29 In contrast, Xiang et al30 reported that this variant has no effect on cell surface expression levels or MC4R activity. Additionally, Phe202Leu was found in both obese and nonobese subjects.17,29 The effect of these missense variants was classified as non-disease causing by in silico softwares. All these findings associated with our Bioinformatic analyses suggest that these two mutations are not associated with nonsyndromic monogenic obesity.
Interestingly, Val103Ile has been considered an obesity-protective polymorphism and was observed in both groups, being the most frequent variant identified in our sample (2.9%). This observation is similar to previous studies in a Polish cohort and a sample of the South American population.17,31,32 Wang et al31 have performed a meta-analysis using six East Asian studies, where they found that the frequency of this variant was 2.9% (n=19,882) in subjects with obesity and 3.9% (n=35,373) in nonobese individuals. Two previous functional analyses of MC4R harboring Val103Ile variant did not show a difference to the wild-type receptor.33,34 Nevertheless, Xiang et al30 showed that the Val103Ile has a significant decrease in antagonist hAGRP potency when compared to MC4R wild type. Further functional analyses are necessary to investigate these divergent results.
The synonymous mutation (Ile198=) was identified in five individuals with childhood-onset obesity. The frequency of Ile198= was 1.59% in our sample. Hinney et al18 found this variant in only one subject (0.2%) in a large German sample. Larsen et al27 also reported that this mutation was identified in five different Danish patients with childhood-onset obesity (1.6%) and it was considered to possess normal receptor function.
We also identified a start codon lost variant (Met1?) in a 29-year-old woman, who developed obesity during childhood and her current BMI is 49.1 kg/m2. The patient exhibited a moderate BED and high calories consumed per day. Interestingly, Branson et al35 have reported that BED is a major phenotype of MC4R mutation carriers. Bonnefond et al have also described that functional MC4R variant carriers presented higher prevalence of BED; however, this association was not observed in another study.28,36 This divergent result may be explained by inclusion sample criteria, since Hebebrand et al36 selected individuals with common polymorphisms (V103I or I251L) and Bonnefond et al28 selected participants with pathogenic mutations. Besides binge disorder, our patient did not present any other phenotypic abnormality, including hypertension. Her blood pressure levels were still lower than suggested for the new guideline.23 We also examined her biochemical levels and found that her values of glucose, TGs, leptin, ghrelin, and insulin were lower than that observed in women with morbid obesity from Brazil.21 We suggest a future study comparing this information with controls.
This mutation is located in the initiation codon ATG (c.1A>G; Met1?), which may affect the translation process and impair the MC4R production. Our Bioinformatic analyses suggested that this variant disrupts the original ORF, resulting in a second ORF, which starts eight amino acids later. It is not clear whether this second ORF is functional resulting in a truncated receptor, because it would be necessary that all transcriptional and translation sequences and regulation work correctly. Further functional analyses are necessary to elucidate the impact of Met1? on MC4R.
Met1? is found in dbSNP database (https://www.ncbi.nlm.nih.gov/SNP/); however, it was not reported in any other study. This variant was absent in 1000 genome, EXAC database, predicted to be causative by at least one of the Bioinformatic tools and was interpreted to be pathogenic by current standards and guidelines.24 Unfortunately, we were unable to evaluate the effect of this variant on the gene expression and the familial segregation. Collet et al9 have also reported two complete loss-of-function mutations in the same codon (c.3G>A and c.3G>C; Met1Ile). None of the other previous described pathogenic mutations was identified in our sample.
The prevalence of pathogenic variants is consistent with earlier studies carried out in adult populations. For example, Jacobson et al37 have screened the coding region of MC4R gene in Swedish sample and showed that the prevalence was 0.5%, being one of the lowest frequencies in Europe. They also did not find any of the previous reported null alleles. Most recently, Stanikova et al38 identified two loss-of-function variants in obese Slovak children (0.7%). Interestingly, Lubrano-Berthelier et al25 found a higher frequency of MC4R pathogenic mutations (2.6%) in French adult subjects with severe obesity. Tunç et al6 also reported an elevated prevalence of MC4R mutations (8.5%) in obese children and adolescence from Turkey. These findings suggest that the high frequency of MC4R mutation associated with nonsyndromic monogenic obesity occurs only in certain ethnic groups.
Phenotypic characteristics were different among MC4R missense mutation carriers and noncarriers. Our study showed that the patients carrying the missense mutations (Ser36Thr, Val103Ile, and Phe202Leu) had higher median of WHR and lower prevalence of hypertension. Furthermore, Val103Ile carriers had lower median of DBP and the same tendency was also observed in SBP. This polymorphism was also negatively associated with hypertension, based on the new guideline.23 Interestingly, previous functional studies indicated that Val103Ile has no implications on MC4R binding or signaling.33 However, Rosmond et al39 showed that heterozygous carriers of Val103Ile had lower WHR and trends for lower BMI when compared to noncarriers in a Swedish men cohort. Brönner et al40 also reported that heterozygous carriers had lower TG levels in cardiovascular patients undergoing cardiac catheterization, suggesting that the Val103Ile polymorphism influences lipid metabolism in a Germany population. Heid et al41 have analyzed a large cohort of German adults (7,888 participants) and found that the presence of isoleucine is associated with decreased waist circumference, decreased glycosylated hemoglobin, and increased HDL-c. They also observed that the Ile103 carriers have reduced risk of having three or more components of metabolic syndrome. Additionally, mutated allele has been negatively associated with obesity, which indicates a protective effect.31 These findings suggest that Val103Ile might have a slight effect on metabolism without affecting the MC4R function in vitro.27 Based on literature, we suggest that Val103Ile is negatively associated with hypertension due to protective effect on body weight and obesity. Our results suggest that blood pressure may be influenced in subjects carrying mutated allele; however, previous studies did not observe this relationship.40,41 Our findings showed a different result and the discrepancies may be explained by differences in genetic background and the sample criteria to select the participants. Further case–control studies with large cohort are necessary to confirm these results.
Conclusion
In summary, our results showed for the first time the prevalence of variants in the coding region of MC4R in a cohort of Brazilian severely obese adults. Assessment of MC4R variants could be beneficial for future treatment strategies. Recently, an MC4R agonist (Setmelanotide) has shown to be effective in the treatment of obese patients with MC4R deficiency.9 We identified five variants; one abolishes the normal translation initiation codon. It was found in a female patient with childhood-onset obesity (c.1A>G; Met1?). Further functional or expression analyses are necessary to confirm the pathogenicity of this variant. We also observed significant phenotypic differences among missense variant carriers and noncarriers, suggesting that MC4R genetic variations may impact body fat distribution and blood pressure.
Acknowledgments
The author would like to thank the patients who kindly agreed to participate in this study. We are grateful to Nereida Proença da Fonseca for her great technical assistance with the participants and Rosimere Lima for her excellent work with patients in Self-Esteem and Citizenship of the Obese Group ([Grupo de Resgate à Autoestima e Cidadania do Obeso]; GRACO). This work was supported by the Oswaldo Cruz Foundation (FIOCRUZ, Rio de Janeiro, Brazil), National Council for Scientific and Technological Development (CNPq), and Coordination for the Improvement of Higher Education Personnel (CAPES).
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Obesity and overweight; 2018. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed August 22, 2018. | ||
NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. 2016;387(10026):1377–1396. | ||
Dixon JB, Zimmet P, Alberti KG, Rubino F; International Diabetes Federation Taskforce on Epidemiology and Prevention. Bariatric surgery: an IDF statement for obese type 2 diabetes. Diabet Med. 2011;28(6):628–642. | ||
Kitahara CM, Flint AJ, de Gonzalez AB, et al. Association between class III obesity (BMI of 40-59 kg/m2) and mortality: a pooled analysis of 20 prospective studies. PLoS Med. 2014;11(7):e1001673. | ||
da Fonseca ACP, Mastronardi C, Johar A, Arcos-Burgos M, Paz-Filho G. Genetics of non-syndromic childhood obesity and the use of high-throughput DNA sequencing technologies. J Diabetes Complications. 2017;31(10):1549–1561. | ||
Tunç S, Demir K, Tükün FA, et al. Melanocortin-4 receptor gene mutations in a group of Turkish obese children and adolescents. J Clin Res Pediatr Endocrinol. 2017;9(3):216–221. | ||
Larder R, Lim CT, Coll AP. Genetic aspects of human obesity. Handb Clin Neurol. 2014;124:93–106. | ||
Morton GJ, Cummings DE, Baskin DG, Barsh GS, Schwartz MW. Central nervous system control of food intake and body weight. Nature. 2006;443(7109):289–295. | ||
Collet T, Dubern B, Mokrosinski J. Evaluation of a melanocortin-4 receptor (MC4R) agonist (setmelanotide) in MC4R deficiency. Mol Metab. 2017;6(10):1321–1329. | ||
Delhanty PJ, Bouw E, Huisman M, et al. Functional characterization of a new human melanocortin-4 receptor homozygous mutation (N72K) that is associated with early-onset obesity. Mol Biol Rep. 2014;41(12):7967–7972. | ||
da Silva AA, do Carmo J, Dubinion J, Hall JE. The role of the sympathetic nervous system in obesity-related hypertension. Curr Hypertens Rep. 2009;11(3):206–211. | ||
da Silva AA, Kuo JJ, Hall JE. Role of hypothalamic melanocortin 3/4-receptors in mediating chronic cardiovascular, renal, and metabolic actions of leptin. Hypertension. 2004;43(6):1312–1317. | ||
Ni XP, Butler AA, Cone RD, Humphreys MH. Central receptors mediating the cardiovascular actions of melanocyte stimulating hormones. J Hypertens. 2006;24(11):2239–2246. | ||
Greenfield JR, Miller JW, Keogh JM, et al. Modulation of blood pressure by central melanocortinergic pathways. N Engl J Med. 2009;360(1):44–52. | ||
do Carmo JM, da Silva AA, Wang Z, Fang T. Role of the brain melanocortins in blood pressure regulation. Biochim Biophys Acta Mol Basis Dis. 2017;1863:2508–2514. | ||
Alharbi KK, Spanakis E, Tan K, et al. Prevalence and functionality of paucimorphic and private MC4R mutations in a large, unselected European British population, scanned by meltMADGE. Hum Mutat. 2007;28(3):294–302. | ||
Logan M, Van der Merwe MT, Dodgen TM, et al. Allelic variants of the melanocortin 4 receptor (MC4R) gene in a South African Study Group. Mol Genet Genomic Med. 2016;4(1):68–76. | ||
Hinney A, Bettecken T, Tarnow P, et al. Prevalence, spectrum, and functional characterization of melanocortin-4 receptor gene mutations in a representative population-based sample and obese adults from Germany. J Clin Endocrinol Metab. 2006;91(5):1761–1769. | ||
Farooqi IS, Keogh JM, Yeo GS, Lank EJ, Cheetham T, O’Rahilly S. Clinical spectrum of obesity and mutations in the melanocortin 4 receptor gene. N Engl J Med. 2003;348(12):1085–1095. | ||
Mackenzie RG. Obesity-associated mutations in the human melanocortin-4 receptor gene. Peptides. 2006;27(2):395–403. | ||
Magno F, Guaraná HC, Fonseca ACP, et al. Influence of FTO rs9939609 polymorphism on appetite, ghrelin, leptin, IL6, TNFα levels, and food intake of women with morbid obesity. Diabetes Metab Syndr Obes. 2018;11:199–207. | ||
Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–1252. | ||
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. | ||
Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405–423. | ||
Lubrano-Berthelier C, Dubern B, Lacorte JM, et al. Melanocortin 4 receptor mutations in a large cohort of severely obese adults: prevalence, functional classification, genotype-phenotype relationship, and lack of association with binge eating. J Clin Endocrinol Metab. 2006;91(5):1811–1818. | ||
Tan KM, Ooi SQ, Ong SG, et al. Functional characterization of variants in MC4R gene promoter region found in obese children. J Clin Endocrinol Metab. 2014;99(5):E931–935. | ||
Larsen LH, Echwald SM, Sørensen TI, Andersen T, Wulff BS, Pedersen O. Prevalence of mutations and functional analyses of melanocortin 4 receptor variants identified among 750 men with juvenile-onset obesity. J Clin Endocrinol Metab. 2005;90(1):219–224. | ||
Bonnefond A, Keller R, Meyre D, et al. Eating behavior, low-frequency functional mutations in the melanocortin-4 receptor (MC4R) gene, and outcomes of bariatric operations: a 6-year prospective study. Diabetes Care. 2016;39(8):1384–1392. | ||
Tao YX, Segaloff DL. Functional analyses of melanocortin-4 receptor mutations identified from patients with binge eating disorder and nonobese or obese subjects. J Clin Endocrinol Metab. 2005;90(10):5632–5638. | ||
Xiang Z, Proneth B, Dirain ML, Litherland SA, Haskell-Luevano C. Pharmacological characterization of 30 human melanocortin-4 receptor polymorphisms with the endogenous proopiomelanocortin-derived agonists, synthetic agonists, and the endogenous agouti-related protein antagonist. Biochemistry. 2010;49(22):4583–4600. | ||
Wang D, Ma J, Zhang S, et al. Association of the MC4R V103I polymorphism with obesity: a Chinese case-control study and meta-analysis in 55,195 individuals. Obesity (Silver Spring). 2010;18(3):573–579. | ||
Nowacka-Woszuk J, Cieslak J, Skowronska B, et al. Missense mutations and polymorphisms of the MC4R gene in Polish obese children and adolescents in relation to the relative body mass index. J Appl Genet. 2011;52(3):319–323. | ||
Gu W, Tu Z, Kleyn PW, et al. Identification and functional analysis of novel human melanocortin-4 receptor variants. Diabetes. 1999;48(3):635–639. | ||
Hinney A, Hohmann S, Geller F, et al. Melanocortin-4 receptor gene: case-control study and transmission disequilibrium test confirm that functionally relevant mutations are compatible with a major gene effect for extreme obesity. J Clin Endocrinol Metab. 2003;88(9):4258–4267. | ||
Branson R, Potoczna N, Kral JG, Lentes KU, Hoehe MR, Horber FF. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. N Engl J Med. 2003;348(12):1096–1103. | ||
Hebebrand J, Geller F, Dempfle A, et al. Binge-eating episodes are not characteristic of carriers of melanocortin-4 receptor gene mutations. Mol Psychiatry. 2004;9(8):796–800. | ||
Jacobson P, Ukkola O, Rankinen T, et al. Melanocortin 4 receptor sequence variations are seldom a cause of human obesity: the Swedish obese subjects, the heritage family study, and a Memphis cohort. J Clin Endocrinol Metab. 2002;87(10):4442–4446. | ||
Stanikova D, Surova M, Ticha L, et al. Melanocortin-4 receptor gene mutations in obese Slovak children. Physiol Res. 2015;64(6):883–890. | ||
Rosmond R, Chagnon M, Bouchard C, Björntorp P. A missense mutation in the human melanocortin-4 receptor gene in relation to abdominal obesity and salivary cortisol. Diabetologia. 2001;44(10):1335–1338. | ||
Brönner G, Sattler AM, Hinney A, et al. The 103I variant of the melanocortin 4 receptor is associated with low serum triglyceride levels. J Clin Endocrinol Metab. 2006;91(2):535–538. | ||
Heid IM, Vollmert C, Kronenberg F, et al. Association of the MC4R V103I polymorphism with the metabolic syndrome: the KorA study. Obesity (Silver Spring). 2008;16(2):369–376. |
Supplementary materials
 | Table S1 Primers used to amplify the coding region of MC4R |
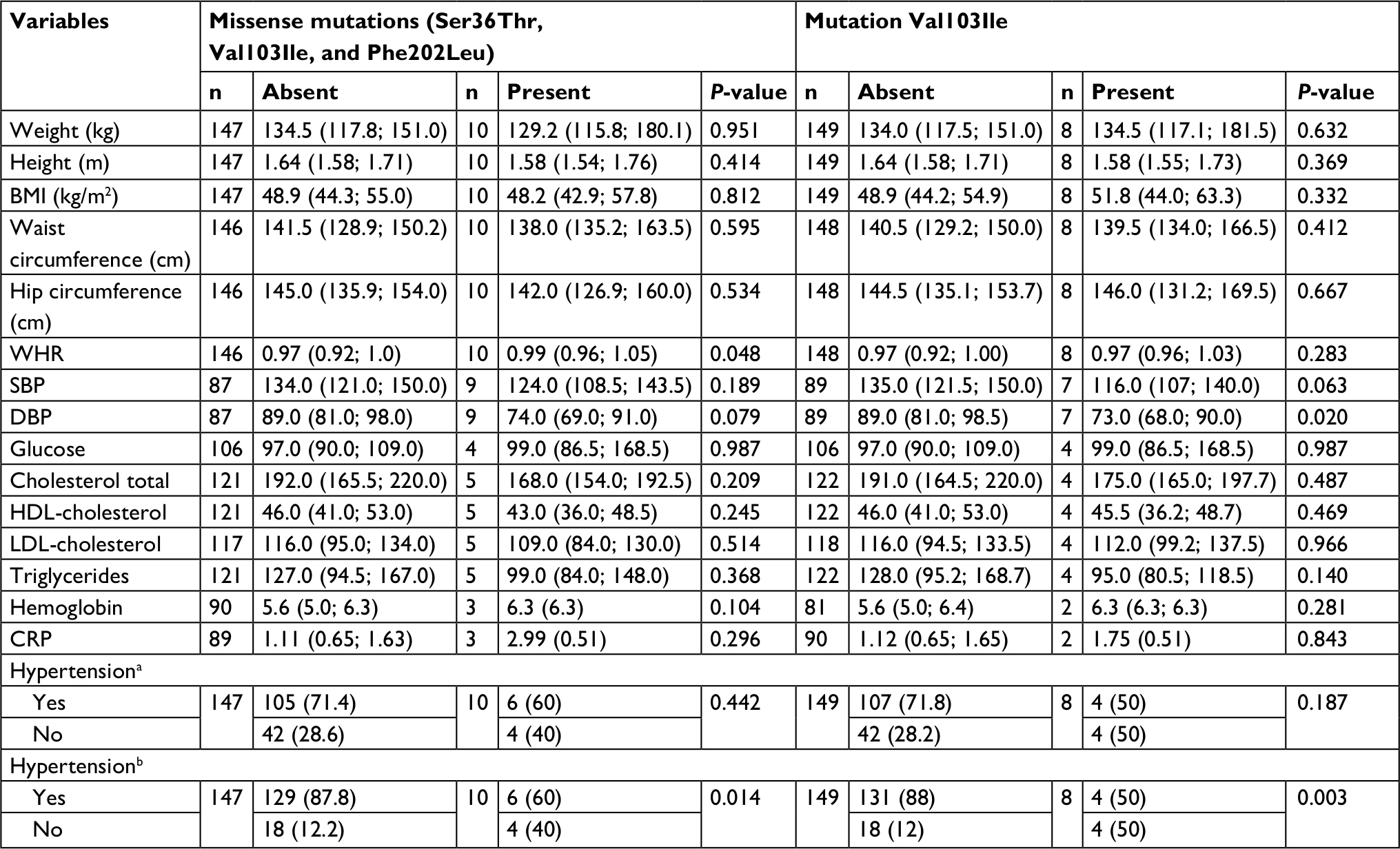 | Table S2 Influence of MC4R mutations on anthropometric, biochemical, and pressure parameters Notes: Data are presented as median values (IQR 25%–75%) for quantitative traits and n (%) for qualitative traits. Data were analyzed by Mann–Whitney test (for non-normally distributed variables) or χ2 test (for categorical variables). aHypertension – based on blood pressure ≥140 × 90 mm Hg. bHypertension – based on blood pressure ≥130 × 80 mm Hg. *P-value for differences between mutated and nonmutated subjects. Abbreviations: BMI, body mass index; CRP, C-reactive protein; DBP, diastolic blood pressure; HDL-cholesterol, high-density lipoprotein-cholesterol; LDL-cholesterol, low-density lipoprotein-cholesterol; SBP, systolic blood pressure; WHR, waist–hip ratio. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.