")
Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 6
Idelalisib therapy of indolent B-cell malignancies: chronic lymphocytic leukemia and small lymphocytic or follicular lymphomas
Authors Madanat Y, Smith M, Almasan A , Hill B
Received 17 December 2015
Accepted for publication 5 January 2016
Published 15 March 2016 Volume 2016:6 Pages 1—6
DOI https://doi.org/10.2147/BLCTT.S73530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Dingli
Yazan F Madanat,1 Mitchell R Smith,2 Alexandru Almasan,3 Brian T Hill2
1Department of Internal Medicine, 2Department of Hematology and Medical Oncology, Taussig Cancer Institute, 3Department of Cancer Biology, Lerner Research Institute, Cleveland Clinic, Cleveland, OH, USA
Abstract: Chronic lymphocytic leukemia, small lymphocytic lymphoma, and follicular lymphoma are indolent B-cell lymphoproliferative disorders that mainly affect an older population. Although the majority of patients in need of treatment derive significant benefit from conventional chemotherapeutic agents as well as monoclonal antibodies, less toxic and more effective treatments are needed. Novel agents that inhibit the B-cell receptor signaling pathway have shown promising outcomes in these disorders. Idelalisib is a potent selective oral inhibitor of phosphatidylinositol 3-kinase delta and has shown significant clinical activity in B-cell malignancies. In this review, we summarize the clinical trial data using idelalisib as monotherapy or in combination with rituximab for the treatment of relapsed/refractory disease. The adverse effect profile includes autoimmune disorders such as transaminitis, colitis, and pneumonitis. Given the efficacy and manageable toxicity profile of idelalisib, it is being increasingly incorporated into the management of indolent B-cell malignancies.
Keywords: idelalisib, PI3Kδ inhibitors, chronic lymphocytic leukemia, follicular lymphoma
Introduction
Chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma (SLL), and follicular lymphoma (FL) are common B-cell lymphoproliferative disorders. CLL is the most common leukemia, and FL is the most common indolent B-cell lymphoma.1,2 CLL/SLL and FL affect the older population, with a median age of 65 years at diagnosis for FL and 71 years for CLL/SLL.3–5 The first-line treatment for CLL with greatest efficacy consists of chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab (FCR). This has shown an overall response rate (ORR) of greater than 95% and complete remission of 72% for patients without the high risk 17p deletion.6,7 However, this treatment is not an option for elderly patients or those with significant comorbidities. Although bendamustine with rituximab (BR) is a less-toxic alternative with equivalent progression-free survival (PFS) for patients 65 years or older, neither FCR nor BR are attractive options in the relapsed setting in this population due to cumulative toxicities.8 This has posed difficulties in managing these patients, and there has been an unmet need for less-toxic treatment options.
In the case of FL, front-line treatment consists of rituximab usually in combination with chemotherapy. Common regimens include R-CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) and R-CVP (cyclophosphamide, vincristine, and prednisone), with ORRs nearing 90%.9 More recently, a trial comparing BR to R-CHOP for front-line treatment of indolent non-Hodgkin’s lymphomas (iNHL) including FL demonstrated a longer PFS with less toxicity with BR compared to R-CHOP (median PFS of 69 vs 31 months, respectively).10 Although initial response rates are high, treatment is not curative, and there is decreased efficacy with retreatment. In addition, there are cumulative toxic effects to chemotherapy, including myelosuppression, cardiomyopathy, and secondary malignancies. This necessitates alternative options.
More in-depth understanding of the dependence of B-cell malignancies on the B-cell receptor (BCR) signaling pathway has led to the development of novel orally-bioavailable small-molecule inhibitors of several kinases downstream of the BCR. These include two compounds that have been approved to date, the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib, as well as idelalisib, a potent selective inhibitor of a key kinase, the phosphatidylinositol 3-kinase (PI3K) delta isoform. Idelalisib will be reviewed here, highlighting data from recent clinical trials.
Kinase inhibitors and BCR signaling
BCR activation triggers a cascade of downstream events involving sequential activation of intracellular transduction molecules with kinase function that ultimately modulate cell proliferation, cell survival, differentiation, and function. Several orally-bioavailable small-molecule inhibitors of these kinases have been developed.11,12 Ibrutinib, the first approved BTK inhibitor demonstrated impressive clinical activity in high-risk patients with previously treated CLL with a reported PFS of 75% and an overall survival (OS) of 83% at 26 months. Side effects are generally manageable, but some cases of clinically significant bleeding and atrial fibrillation occur.13,14
Another BCR pathway member that is critical to both CLL and FL cell survival is PI3K. Idelalisib (formerly GS-1101, CAL-101) is a first-in-class, reversible, potent, selective PI3Kδ inhibitor. Idelalisib was approved by the US Food and Drug Association in 2014 for treatment of relapsed/refractory CLL and FL.15
PI3Ks are signal transduction enzymes, found in four isoforms p110 (alpha, beta, gamma, and delta).16 Though the p110 alpha and beta isoforms are expressed widely, gamma and delta isoforms of PI3K are restricted to hematopoietic cells.15,17,18 The delta isoform is expressed in B-cell malignancies, while the gamma isoform is also expressed in T-cells, macrophages, and mesenchymal stromal cells. The activation of the gamma isoform promotes chemotactic signals and maintains the tumor microenvironment.19
PI3K promotes activation of protein kinase B (Akt) by phosphorylation of its threonine/serine molecules, which in turn activate the mammalian target of rapamycin pathway. This cascade promotes cell differentiation and prolongs survival in lymphocytes.20 The activation of BCR can occur through antigen-dependent or through tonic (antigen-independent) pathways, both of which involve PI3K. Both cascades are upregulated in CLL and FL cells.18,21 Idelalisib induces cell cycle arrest in G0/G1 phase, thus inhibiting proliferation; furthermore, it induces apoptosis in B-cells by caspase activation.
Mode of action and pharmacokinetic profile of idelalisib
Based on the Phase I trial and its pharmacokinetic profile, the approved dose of idelalisib is 150 mg orally every 12 hours. A reduced dose of 100 mg twice daily is recommended when clinically indicated. Its elimination half-life is 8.2 hours. The time-to-peak plasma concentration increased from 2 to 4 hours with food; however, this was not clinically significant. It is metabolized primarily by aldehyde oxidase (AO), and to a lesser extent by cytochrome P450 3A (CYP3A), to its inactive metabolite GS-563117. Although drug–drug interactions with CYP3A inducers and/or inhibitors could theoretically affect plasma concentration of idelalisib, these may not be clinically significant as the major metabolizing enzyme is AO. Both idelalisib and its metabolite GS-563117 are highly protein-bound at 94% and 99%, respectively. Excretion is mostly hepatobiliary, with 78% of the drug found in feces and only 15% in urine. Given the minimal urinary excretion, dose adjustment in renal impairment is not necessary.22
Recent clinical trials and efficacy
Chronic lymphocytic leukemia
The Phase I trial of idelalisib monotherapy in 54 patients with relapsed or refractory CLL showed an ORR of 72% and a median PFS of 15.8 months.23 This supported conducting a Phase III, randomized, double-blind, placebo-controlled trial on 220 patients with previously treated CLL in 90 centers in the USA and Europe between May 2012 and August 2013. The patients were randomized to receive rituximab (R) in combination with idelalisib (150 mg BID) or R with placebo twice daily. High-risk patients with del17p, TP53 mutation, or lack of hypermutation in the immunoglobulin heavy chain (IGHV) were included. This study was terminated early given the superior efficacy of idelalisib. The PFS in the idelalisib vs placebo groups at 24 weeks was 93% vs 46% (P<0.001), and OS at 12 months was 92% vs 80% (P=0.02), respectively.24
A recent Phase II trial investigating the role of idelalisib in combination with R in 64 treatment-naïve patients over 65 years old with CLL (n=59) or SLL (n=5) reported an ORR of 96.9%. Patients with high-risk disease, that is del17p/TP53 mutations or unmutated IGHV, had similar ORRs as well. The median duration of response and PFS were not reached by the time of the analysis, with PFS at 24 months being 92.9% and 82% at 36 months (Table 1).25
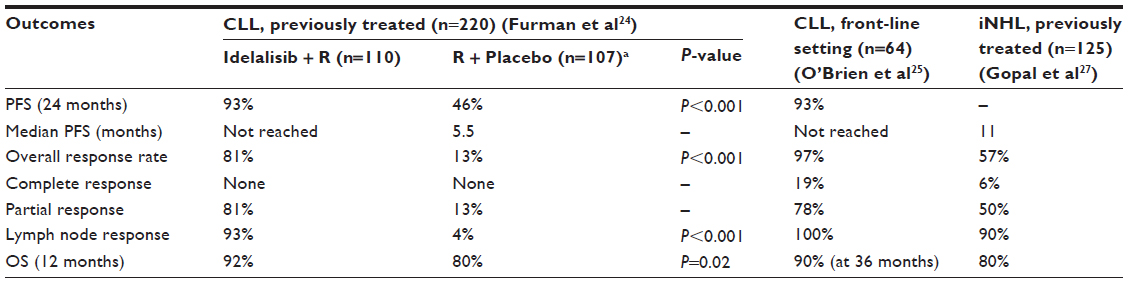 | Table 1 Efficacy of idelalisib |
At the 2015 Annual Society of Hematology Meeting, results of a Phase III randomized study of BR vs BR + idelalisib for relapsed/refractory CLL, including patients with del17p, demonstrated significantly improved PFS and OS for addition of idelalisib to BR. The safety profile did not demonstrate any new or unexpected adverse events.26
Indolent B-cell lymphoma
The role of idelalisib as monotherapy in relapsed iNHL was investigated in a Phase II study involving 125 patients from April 2011 to October 2012. Subtypes of iNHL included were FL (n=72), SLL (n=28), marginal-zone lymphoma (n=15), and lymphoplasmacytic lymphoma (n=10). Eligible patients were considered refractory to treatment with both rituximab and an alkylating agent. ORR was 57%. Response rates were comparable within the subgroups of iNHL (ORR: 47%–80%). The median duration of response was 12.5 months, and the median PFS duration was 11 months. Median OS was 20.3 months with 80% OS at the end of the study (Table 1).27
Safety and adverse events
The adverse effects (AE) associated with idelalisib combining the three most recent clinical trials are summarized in Table 2. In the relapsed CLL trial, the most common AE in the idelalisib + R treatment group were fatigue (24%), nausea (24%), diarrhea (19%), fever (29%), and chills (22%). Serious adverse effects (SAE) included pneumonia (6%), febrile neutropenia (5%), diarrhea (3%), pyrexia (6%), and dyspnea (1%). Laboratory abnormalities included elevation in alanine transaminase/aspartate transaminase, which mostly occurred within the first 12 weeks of treatment. Others include anemia, neutropenia, and thrombocytopenia. In addition, lymphocytosis, which is an observed class effect of BCR pathway inhibitors, was seen.23 Idelalisib-associated lymphocytosis peaked at week 2 and resolved by week 12; however, in combination with rituximab, idelalisib did not show prominent lymphocytosis.24
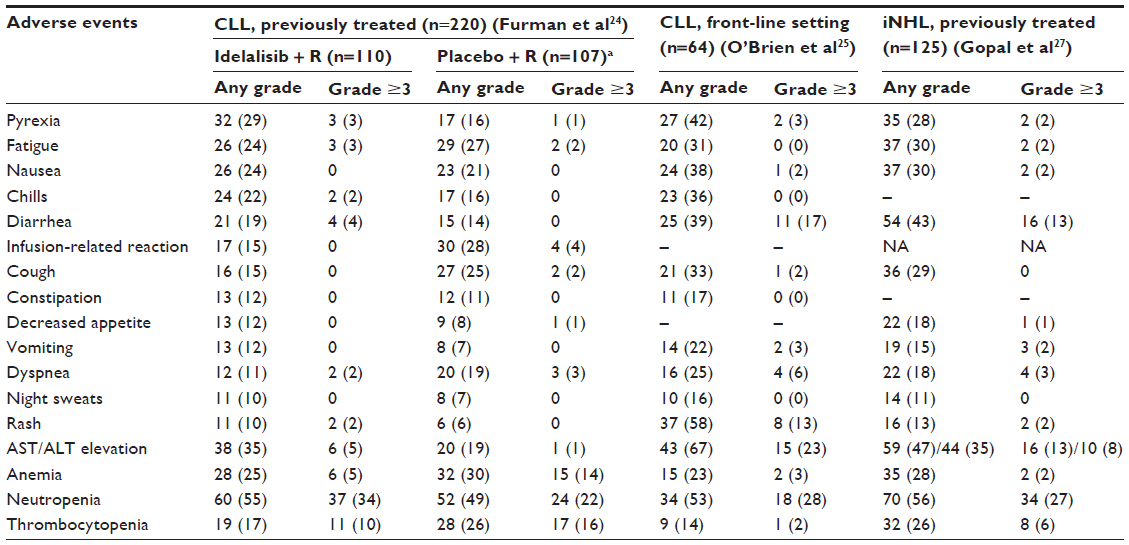 | Table 2 Adverse events and lab abnormalities |
In the relapsed/refractory iNHL trial, the most common AE with idelalisib monotherapy included diarrhea (13%) and pneumonia (7%). Dose reduction from 150 mg BID to 100 mg BID was necessary in 34% of patients due to AE (hepatotoxicity, colitis, and pneumonitis/pneumonia).27
In the treatment-naïve CLL trial, SAE were higher with diarrhea/colitis at 42.2% and pneumonia at 18.8%, presumably reflecting a more intact immune system.25
Idelalisib prescribing information provides a black box warning for serious and/or fatal toxicities. These included grade ≥3 diarrhea/colitis (14%), hepatotoxicity (14%), pneumonitis, and intestinal perforation. In the setting of SAE, idelalisib is withheld until resolution of AE, and then dose reduction to 100 mg BID is recommended. Recurrence of AE after dose reduction or occurrence of a life-threatening AE warrants permanent treatment discontinuation. Corticosteroids are recommended for treatment of severe colitis/pneumonitis.28
AE leading to idelalisib discontinuation were lower when used in the relapsed setting vs front-line setting. Nine patients (8%) discontinued treatment in the relapsed CLL trial due to gastrointestinal and skin side effects, while 25 patients (20.8%) discontinued idelalisib in the relapsed iNHL trial due to hepatotoxicity, colitis, and pneumonia.24,27 However, 29 patients (45.3%) discontinued idelalisib in treatment-naïve CLL patients. The most reported AE in the front-line setting included diarrhea/colitis (18.8%), dyspnea (4.7%), and rash (4.7%).25
Given the activity of idelalisib in the relapsed setting, a Phase II clinical trial of idelalisib plus ofatumumab for treatment-naïve CLL patients was launched. Preliminary results presented at the 2015 Annual Society of Hematology Meeting revealed a high rate of hepatic toxicity, suggesting that patients without exposure to prior immunosuppressive chemotherapy may be insufficiently immunocompromised to tolerate idelalisib therapy as front-line treatment.29
A recent retrospective analysis examined the incidence of colitis in 50 patients treated with idelalisib continuously for 3 months. Of the 23 patients who developed diarrhea, eight patients had severe symptoms. Twelve of 14 patients who underwent a colonoscopy with biopsies had histological evidence of colitis with intraepithelial lymphocytosis and crypt apoptosis. Eleven of 50 patients had to discontinue treatment due to severity of symptoms, while nine patients were successfully treated with steroids.30 It has been noted that idelalisib-induced diarrhea may be poorly responsive to antimotility agents, lasting up to 1 month after treatment discontinuation.28
Patient adherence
There are many factors influencing patient adherence; the ease of administration, a tolerable side effect profile, and acceptable drug–drug interactions make idelalisib an encouraging medication for patient adherence. However, the average wholesale price of a 28-day supply is estimated at $8,862 at the recommended full dose.31
Future directions
Idelalisib is an active agent in indolent B-cell leukemia/lymphoma. We foresee further investigation in combination with other chemo- and immunotherapies, as well as studies trying to replace chemoimmunotherapy in various indications. The utility of this agent in other settings such as aggressive B-cell lymphoma needs investigation. Given the cumulative burden of cost, immune toxicities, and unknown long-term AE, studies comparing stopping treatment, perhaps in a minimal residual disease state, vs continuous therapy would be worthwhile. Enthusiasm of moving this effective therapy to the front-line setting may be tempered by the preliminary data for front-line treatment, which is concerning for a high incidence of autoimmune complications.
Concurrent inhibition of multiple isoforms of the PI3K enzyme demonstrated theoretical benefit in vitro studies.32 Duvelisib (IPI-145) is a novel oral inhibitor of both PI3K delta and gamma isoforms that is in clinical development.33
Recent data demonstrated that PI3K pathway inhibition by idelalisib sensitized malignant B-cells to overcome resistance to the Bcl-2 inhibitor venetoclax (formerly ABT-199) through downregulation of myeloid cell leukemia 1 and Bcl-2-associated X protein activation, paving the way for rational combination therapies.34
Conclusion
In conclusion, idelalisib is a highly efficacious new targeted therapy for the treatment of patients with iNHL and CLL/SLL, producing high rates of durable responses, with favorable PFS and OS. Combinations with BR chemotherapy in the relapsed/refractory CLL population demonstrate safety with both a PFS and OS benefit. The somewhat unique toxicity profile requires careful monitoring of patients treated with this agent. Targeted therapies such as idelalisib already play a pivotal role in the current treatment of CLL/iNHL, and this role is expected to expand as many clinical trials are ongoing.
Disclosure
AA was supported by the CA127264 research grant from National Institutes of Health. BTH has served on an advisory boards with both Genentech and Pharmacyclics. MRS has served on advisory boards with Genentech, Spectrum, and Celgene. The authors report no other conflicts of interest in this work.
References
Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the united states, 1992–2001. Blood. 2006;107:265–276. | |
Gribben JG. How I treat indolent lymphoma. Blood. 2007;109:4617–4626. | |
Junlen HR, Peterson S, Kimby E, et al. Follicular lymphoma in Sweden: nationwide improved survival in the rituximab era, particularly in elderly women: a Swedish lymphoma registry study. Leukemia. 2015;29:668–676. | |
Redaelli A, Laskin BL, Stephens JM, Botteman MF, Pashos CL. The clinical and epidemiological burden of chronic lymphocytic leukaemia. Eur J Cancer Care (Engl). 2004;13:279–287. | |
Diehl LF, Karnell LH, Menck HR. The American college of surgeons commission on cancer and the American cancer society. The National Cancer Data Base report on age, gender, treatment, and outcomes of patients with chronic lymphocytic leukemia. Cancer. 1999;86:2684–2692. | |
Tam CS, O’Brien S, Wierda W, et al. Long-term results of the fludarabine, cyclophosphamide, and rituximab regimen as initial therapy of chronic lymphocytic leukemia. Blood. 2008;112:975–980. | |
Goede V, Hallek M. Pharmacotherapeutic management of chronic lymphocytic leukaemia in patients with comorbidities: new agents, new hope. Drugs Aging. 2015;32(11):877–886. | |
Eichhorst B, Fink AM, Busch R, et al. Frontline chemoimmunotherapy with fludarabine (F), cyclophosphamide (C), and rituximab (R)(FCR) shows superior efficacy in comparison to bendamustine (B) and rituximab (BR) in previously untreated and physically fit patients (pts) with advanced chronic lymphocytic leukemia (CLL): final analysis of an international, randomized study of the german CLL study group (GCLLSG)(CLL10 study) [abstract 19]. Abstract presented at: 56th American Society of Hematology (ASH) Annual Meeting and Exposition, December 6–9, 2014, San Francisco, CA. | |
Lunning MA, Vose JM. Management of indolent lymphoma: where are we now and where are we going. Blood Rev. 2012;26:279–288. | |
Rummel MJ, Niederle N, Maschmeyer G, et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet. 2013;381:1203–1210. | |
Stevenson FK, Caligaris-Cappio F. Chronic lymphocytic leukemia: revelations from the B-cell receptor. Blood. 2004;103:4389–4395. | |
Davids MS, Brown JR. Targeting the B cell receptor pathway in chronic lymphocytic leukemia. Leuk Lymphoma. 2012;53:2362–2370. | |
Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369:32–42. | |
Wang Y, Zhang LL, Champlin RE, Wang ML. Targeting Bruton’s tyrosine kinase with ibrutinib in B-cell malignancies. Clin Pharmacol Ther. 2015;97:455–468. | |
Markham A. Idelalisib: first global approval. Drugs. 2014;74:1701–1707. | |
Vanhaesebroeck B, Guillermet-Guibert J, Graupera M, Bilanges B. The emerging mechanisms of isoform-specific PI3K signalling. Nat Rev Mol Cell Biol. 2010;11:329–341. | |
Puri KD, Gold MR. Selective inhibitors of phosphoinositide 3-kinase delta: modulators of B-cell function with potential for treating autoimmune inflammatory diseases and B-cell malignancies. Front Immunol. 2012;3:256. | |
Dong S, Guinn D, Dubovsky JA, et al. IPI-145 antagonizes intrinsic and extrinsic survival signals in chronic lymphocytic leukemia cells. Blood. 2014;124:3583–3586. | |
Sciavolino PJ. A tale of two isoforms: PI3K delta and gamma. Targeted Oncology [serial online, cited December 1, 2015] April 30, 2015. Available from: http://www.targetedonc.com/publications/targeted-therapies-cancer/2015/april-2015/a-tale-of-two-isoforms-pi3k-delta-and-gamma. Accessed November 10, 2015. | |
Bernal A, Pastore RD, Asgary Z, et al. Survival of leukemic B cells promoted by engagement of the antigen receptor. Blood. 2001;98:3050–3057. | |
Young RM, Staudt LM. Targeting pathological B cell receptor signalling in lymphoid malignancies. Nat Rev Drug Discov. 2013;12:229–243. | |
Ramanathan S, Jin F, Sharma S, Kearney BP. Clinical pharmacokinetic and pharmacodynamic profile of idelalisib. Clin Pharmacokinet. Epub August 15, 2015. | |
Brown JR, Byrd JC, Coutre SE, et al. Idelalisib, an inhibitor of phosphatidylinositol 3-kinase p110delta, for relapsed/refractory chronic lymphocytic leukemia. Blood. 2014;123:3390–3397. | |
Furman RR, Sharman JP, Coutre SE, et al. Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med. 2014;370:997–1007. | |
O’Brien SM, Lamanna N, Kipps TJ, et al. A phase 2 study of idelalisib plus rituximab in treatment-naive older patients with chronic lymphocytic leukemia. Blood. 2015;126(25):2686–2694. | |
Zelenetz AD, Robak T, Coiffier B, et al. Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory chronic lymphocytic leukemia: results of a phase 3 randomized double-blind placebo-controlled study [late breaking abstract 5]. Abstract presented at: 57th American Society of Hematology (ASH) Annual Meeting and Exposition, December 5–8, 2015, Orlando, FL. | |
Gopal AK, Kahl BS, de Vos S, et al. PI3Kdelta inhibition by idelalisib in patients with relapsed indolent lymphoma. N Engl J Med. 2014;370:1008–1018. | |
Zyledig® [prescribing information]. Foster City, CA: Gilead Sciences, Inc.; 2014. Available from: http://www.gilead.com/~/media/Files/pdfs/medicines/oncology/zydelig/zydelig_pi.pdf. Accessed November 28, 2015. | |
Lampson BL, Matos T, Kim HT, et al. Idelalisib given front-line for the treatment of Chronic lymphocytic Leukemia Results in frequent and severe immune-mediated toxicities [abstract 497]. Abstract presented at: 57th American Society of Hematology (ASH) Annual Meeting and Exposition, December 5–8, 2015, Orlando, FL. | |
Weidner AS, Panarelli NC, Geyer JT, et al. Idelalisib-associated colitis: histologic findings in 14 patients. Am J Surg Pathol. 2015; 39(12):1661–1667. | |
Butler T, Maravent S, Boisselle J, Valdes J, Fellner C. A review of 2014 cancer drug approvals, with a look at 2015 and beyond. P T. 2015; 40:191–205. | |
Blunt MD, Steele AJ. Pharmacological targeting of PI3K isoforms as a therapeutic strategy in chronic lymphocytic leukaemia. Leuk Res Rep. 2015;4:60–63. | |
Balakrishnan K, Peluso M, Fu M, et al. The phosphoinositide-3-kinase (PI3K)-delta and gamma inhibitor, IPI-145 (duvelisib), overcomes signals from the PI3K/AKT/S6 pathway and promotes apoptosis in CLL. Leukemia. 2015;29:1811–1822. | |
Choudhary GS, Al-Harbi S, Mazumder S, et al. MCL-1 and BCL-xL-dependent resistance to the BCL-2 inhibitor ABT-199 can be overcome by preventing PI3K/AKT/mTOR activation in lymphoid malignancies. Cell Death Dis. 2015;6:e1593. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.