Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
How Effective are Mentoring Programs for Improving Health Worker Competence and Institutional Performance in Africa? A Systematic Review of Quantitative Evidence
Authors Feyissa GT ![]() , Balabanova D, Woldie M
, Balabanova D, Woldie M ![]()
Received 4 September 2019
Accepted for publication 27 November 2019
Published 5 December 2019 Volume 2019:12 Pages 989—1005
DOI https://doi.org/10.2147/JMDH.S228951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Garumma Tolu Feyissa,1,2 Dina Balabanova,3 Mirkuzie Woldie2,4
1Department of Health, Behavior and Society, Jimma University, Jimma, Ethiopia; 2Ethiopian Evidence Based Healthcare: JBI Center of Excellence, Jimma University, Jimma, Ethiopia; 3Department of Health Policy and Management, London School of Hygiene and Tropical Medicine, London, UK; 4Department of Global Health and Population, T.H. Chan Harvard School of Public Health, Addis Ababa, Ethiopia
Correspondence: Garumma Tolu Feyissa
Department of Health, Behavior and Society, Jimma University, P.o.box 378, Jimma, Ethiopia
Email [email protected]
Introduction: Mentoring programs are frequently recommended as innovative and low-cost solutions, and these have been implemented in many healthcare institutions to tackle multiple human resource-related challenges. This review sought to locate, appraise and describe the literature reporting on mentorship programs that were designed to improve healthcare worker competence and institutional performance in Africa.
Methods: This review searched and synthesized reports from studies that assessed the effectiveness of mentorship programs among healthcare workers in Africa. We searched for studies reported in the English language in EMBASE, CINAHL, COCHRANE and MEDLINE. Additional search was conducted in Google Scholar.
Results: We included 30 papers reporting on 24 studies. Diverse approaches of mentorship were reported: a) placing a mentor in health facility for a period of time (embedded mentor), b) visits by a mobile mentor, c) a mentoring approach involving a team of mobile multidisciplinary mentors, d) facility twinning, and e) within-facility mentorship by a focal person or a manager.
Implication for practice: Mentoring interventions were effective in improving the clinical management of infectious diseases, maternal, neonatal and childhood illnesses. Mentoring interventions were also found to improve managerial performance (accounting, human resources, monitoring and evaluation, and transportation management) of health institutions. Additionally, mentoring had improved laboratory accreditation scores. Mentoring interventions may be used to increase adherence of health professionals to guidelines, standards, and protocols. While different types of interventions (embedded mentoring, visits by mobile mentors, facility twinning and within-facility mentorship by a focal person) were reported to be effective, there is no evidence to recommend one model of mentoring over other types of mentoring.
Implications for research: Further research—experimental methods measuring the impact of different mentoring formats and longitudinal studies establishing their long-term effectiveness—is required to compare the effectiveness and cost-effectiveness of different models of mentoring. Further studies are needed to explore why and how different mentoring programs succeed and the meaningfulness of mentoring programs for the different stakeholders are also required.
Keywords: mentoring, Africa, institutional performance, health worker competence, systematic review
Introduction
Accessible, qualified and responsive human resources for health (HRH) are critical determinants of a well-functioning health system and thus improving the health of populations.1 However, skill and competency gaps continue to present major problems among some healthcare professionals in Africa1 Centralized and off-site training programs are either ineffective or expensive.2 A number of strategies have sought to tackle the problems arising from the scarcity of highly qualified HRH, in low- and middle-income countries. Among these initiatives are supportive supervision, provision of tools and aids, quality improvement methods, coaching and mentoring.3 Mentoring is one of the innovative short-term solutions that have been in place in many healthcare institutions to tackle human resource-related challenges in low- and middle-income countries (LMICs).4,5
Clinical mentoring is defined as “a system of practical training and consultation that fosters ongoing professional development” (pp.4).6 Mentoring entails career support provided by an experienced, knowledgeable, skillful, empathetic and committed individual or a mentor to another less experienced individual or a mentee.7 It involves a reciprocal relationship between the mentor and the mentee and hence improves the career outcomes of both.7 Clinical mentoring is an approach for in-service training seeking to facilitate the dissemination of evidence-based practices.8 It is aimed to increase the competence of health professionals and is seen as a part of continuous professional development.9 Mentoring helps to establish an independent and productive service professional.10 It also assists the mentee in establishing clear learning goals and professional relationships.10 It stimulates the mentees to acquire both theoretical knowledge and practical skills and encourages the immediate application of the learning at work settings.11
Mentoring is different from supervision which is hierarchical and managerially oriented, and aimed at evaluating performance based on predetermined criteria or to assess facility infrastructure.6,12 Mentoring does not involve hierarchical relationship between the mentor and mentee, rather it is a relationship involving a shared power model, mutually beneficial and a professional development activity aimed at improving professional skills of mentees based on their needs. In this process, goals are set mutually both by the mentee and mentor, whereas in supervision, goals are set by the supervisor or are guided by regulatory guidelines.9,12 The mentor assumes the role of a counselor.10 Mentorship is also different from coaching, which is the process that involves instructing or guiding a person to develop a specific skill.13 Mentor usually provides feedback to the mentee in a less directive way to enable the mentee develop independence,9,12 and competence, focusing on skills related to specific service.9 Although mentoring is sometimes used interchangeably with preceptorship, it is different in that it involves a longer period and deeper relationship between mentor and mentee than preceptor and preceptee. Unlike mentors, preceptors have less experience and seniority.14
Clinical mentoring usually follows a didactic coursework.12,15 It is, therefore, considered as a continuum of professional development.12,16 Mentoring assists in implementing guidelines and standards by addressing gaps in knowledge and skills of the clinicians.15 Mentoring may include clinical case review, bedside teaching, journal club, and morbidity and mortality rounds.16
Mentoring has been used as a tool to reduce providers’ turnover rates and increase professional satisfaction, thus improving retention.17,18 On-site mentoring also reduces unnecessary absences of staff for centralized training programs and shifts the focus to practice-based learning at job sites.2,11 Researchers reported that mentorship will be effective only if they are conducted with sufficient duration and frequency.19 A systematic review of qualitative studies found that the interpersonal skills, personality and professional status of mentors affect the success of mentorship programs. The review also indicated that for mentorship interventions to be effective, mentees should be committed and proactive. The importance of both personal and professional relationships was also shown.20 In general, mentors should provide psychosocial support, career support and role modeling to the mentees.7
However, no standard duration and frequency of mentorship program is universally accepted. While it is recommended that mentorship interventions should also allow enough time to ensure independent operation by the mentees,19 it may be challenging for mentors to integrate themselves into institutional activities. Hence, it is essential to increase their involvement and recognition as members of the organization they are mentoring by arranging frequent organizational staff meetings.19 In addition, standard measures of performance are required in order to measure progress and effectiveness of the mentorship program.19
Globally, there is emerging evidence that some mentoring programs have reduced turnover rates, employee turnover costs and medical negligence rates and improved job satisfaction, communication skills and professional identity.21 Primary research from several African countries has indicated that mentorship interventions are effective in improving the quality of integrated management of neonatal and childhood illness (IMNCI) services,22 increasing knowledge and competence in the management of human immune-deficiency syndrome virus (HIV) and tuberculosis (TB),4,8 reproductive health,4 antenatal care, labor, and delivery.19
However, the experience of implementing mentorship programs in Africa has not been systematically appraised and synthesized to inform policy and practice. Hence, there is only limited evidence providing clarity on how to design well-performing mentorship programs and integrate these into the structure of health systems.3 The approaches to delivery of the programs, the selection criteria for mentors and frequency and nature of interaction between mentor and mentee required for mentorship programs may affect the effectiveness of mentorship programs, and it is imperative to employ types of mentorship programs that are found to be effective. Through a preliminary search in PubMed, CINAHL, EMBASE, Cochrane database of systematic reviews (CDSR), Database of abstracts of reviews of effectiveness (DARE), JBI Database of systematic reviews and implementation reports, we did not find any systematic review addressing effectiveness of mentorship interventions in African countries, especially for the African context.
Recognizing this knowledge gap, this review sought to locate, appraise and synthesize evidence published in the international literature reporting on the effectiveness of mentorship programs in improving clinical competence of the healthcare workers and the performance of health facilities in Africa. Based on the evidence generated from this review, mentorship programs could be designed to assist health facilities in improving health facility leadership and governance for better service management and delivery.
Methods and Participants
The report included in this systematic review was prepared using PRISMA reporting guidelines (Supplementary material 1) for systematic reviews.23 The review was conducted based on an a-priori protocol registered on PROSPERO (Registration number: CRD42018096366). During the conduct of the review, we considered the following inclusion criteria.
Population
In this review, health professionals of any type and any education level working in any type of healthcare facility acting as a mentee or mentor were considered for inclusion. Only in-service health professionals were included. Pre-service mentees or mentors were not considered for inclusion.
Intervention
Mentoring program of any type was considered for inclusion. Mentorship is defined as “a flexible learning and teaching process that serves specific objectives of a health program”.24 The review did not consider mentorship programs and interventions conducted during pre-service training. It did not include preceptorship interventions or orientations for newly hired professionals.
Comparator
This review considered studies that compared mentorship interventions to programs without mentorship or studies that compared different approaches of mentorship.
Outcomes
The review considered studies that include the following outcomes: competence (knowledge and skills, adherence to standard protocols), and institutional/staff performance. Patient outcomes were not included in the review.
Context
This review considered mentorship interventions conducted in healthcare facilities in all African countries.
Types of Studies
This review considered all studies with comparative designs, such as randomized controlled trials, quasi-experimental studies and before and after studies. Both published and grey literatures published in English language were included.
Search Strategy
The search strategy aimed to identify both published and unpublished studies and it involved three-steps. An initial limited search of CINAHL and MEDLINE was undertaken followed by an examination of the text words contained in the title and abstract, and of the index terms used to describe the articles. A second search using all identified keywords and index terms was then undertaken across all included databases. Third, the reference list of all identified reports and articles was searched for additional studies. Both published and unpublished papers reported in English were searched with no restriction according to age, country, and date of publication. The databases searched were: EMBASE, CINAHL, CENTRAL, and MEDLINE. Additional search was conducted in Google Scholar. A detailed search strategy for each database is reported in Supplementary materials 2. The search was conducted by GTF. The search was conducted from Feb 7 to Feb 9, 2018. Similar key terms were used across all databases. The search in PubMed was conducted with the following MESH terms, keywords and limits.
(“Mentors”[Mesh] OR “Educational outreach” [tw] OR “Onsite training” [tw] OR “mentors”[tw] OR “mentor”[tw]) AND (((“Africa”[Mesh] OR “Africa South of the Sahara”[Mesh] OR “South Africa”[Mesh] OR “Africa, Western”[Mesh] OR “Africa, Southern”[Mesh] OR “Africa, Northern”[Mesh] OR “Africa, Eastern”[Mesh] OR “Africa, Central”[Mesh] OR “Namibia”[Mesh] OR “Mozambique”[Mesh]))) AND (“humans”[MeSH Terms] AND English[lang])
Study Selection
Following the above search procedure, all identified citations were loaded into EndNote and duplicates were removed. Titles and abstracts were screened by two independent reviewers for assessment against the inclusion criteria for the review. The full texts of potentially eligible studies were retrieved and assessed in detail against the inclusion criteria by two independent reviewers.
Risk of Bias Assessment
The papers retrieved were critically appraised by two reviewers independently using the Joanna Briggs Institute (JBI) appraisal checklists (Supplementary material 3). Any potential disagreements were settled by discussion. Since there was no unsettled dispute between the two reviewers, there was no need for a third reviewer.
Data Collection and Analysis
Quantitative data were extracted from papers included in the review using the standardized data extraction tool developed by the JBI (Supplementary material 4). Where necessary, we asked the first authors to provide additional information on the articles. Effect measures reported in the form of mean difference and standard deviation (for continuous variables) and relative risk, odds ratio and their confidence intervals (for dichotomous variables) were extracted and reported. Since the intervention methods, outcomes and populations of interests were heterogeneous, narrative synthesis of the findings was carried out to address the review questions under relevant thematic areas. Summary tables are provided as appropriate.
The outcomes reported in the current review were measured differently across different studies and across different areas of practice such as; laboratory accreditations, institutional performance management, infectious disease management, maternal and child health services and family planning. Hence, we did not conduct quality assessment using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE)25 approach.
Findings
The search yielded a total of 496 records. After removing duplicates, 413 records were screened. After reading the titles and abstracts, 163 records were retained for further examination, out of which 30 articles reporting on 24 studies met eligibility criteria. After a critical appraisal, all 24 articles were included in the analysis (Figure 1).
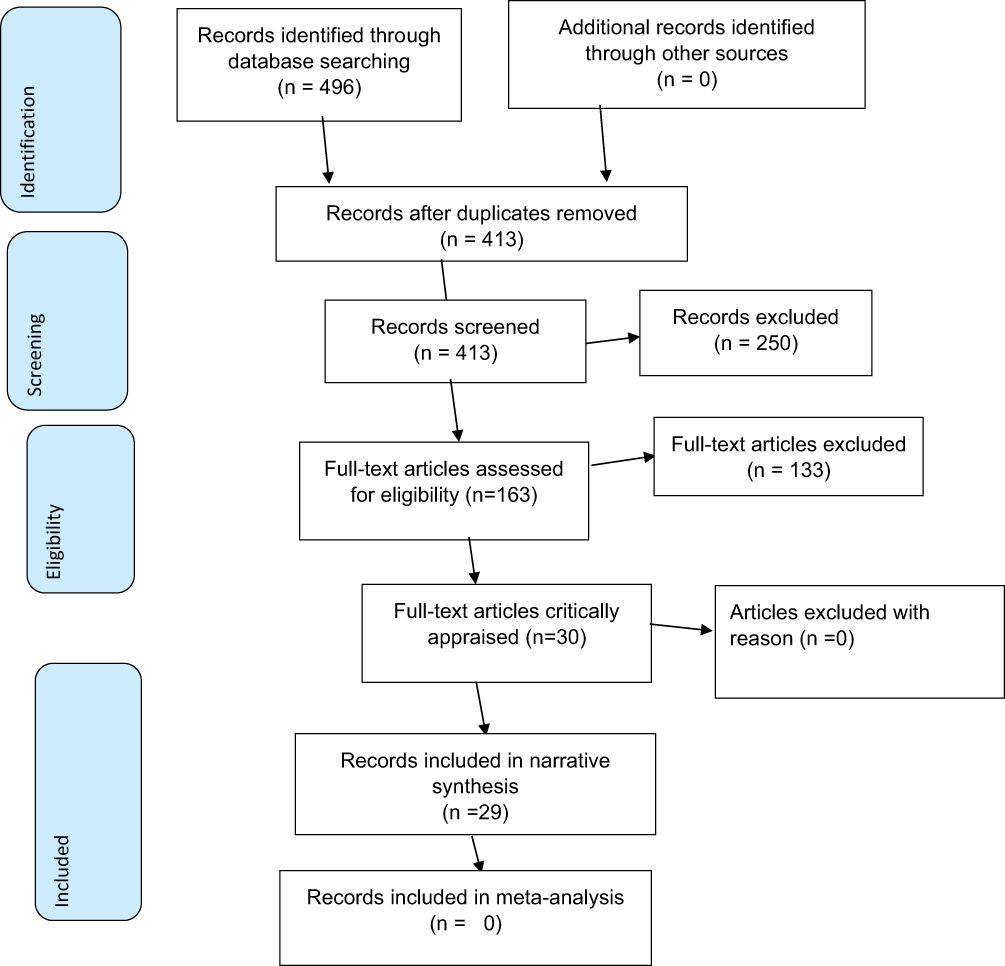 |
Figure 1 Study selection process (Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097). |
Characteristics of the Included Studies
Out of the included records, two26,27 addressed mentorship in healthcare facility managerial performance, six records28–33 addressed mentorship in laboratory setting, and the remaining 21 records2,4,8,11,22,34–48 addressed mentorship in clinical performance. Seven of the included records8,34–39 reported on different aspects of one cRCT, 18 records2,22,26–30,32,33,41,43–45,47,49,50 were quasi-experimental studies, four40,42,46,48 were cohort studies and two4,11 were comparative cross-sectional studies.
Six studies26,28,35,40–42 were conducted in Ethiopia. Two2,22 studies were conducted in Rwanda and reported on different aspects of the same study. Two50,51 were conducted in Malawi. Six records8,34–39 reported on different aspects of the same study that was conducted in Uganda and two studies43,44 were conducted in Nigeria. Two studies29,30 were conducted in Lesotho. One study45 was a multicounty study conducted in African and Asian countries, and only reports related to African countries were extracted. The other studies were conducted in Cameroon,32,46,47 Kenya,49 Zimbabwe,33 Mozambique,27 South Africa4 and Botswana48 (Table 1).
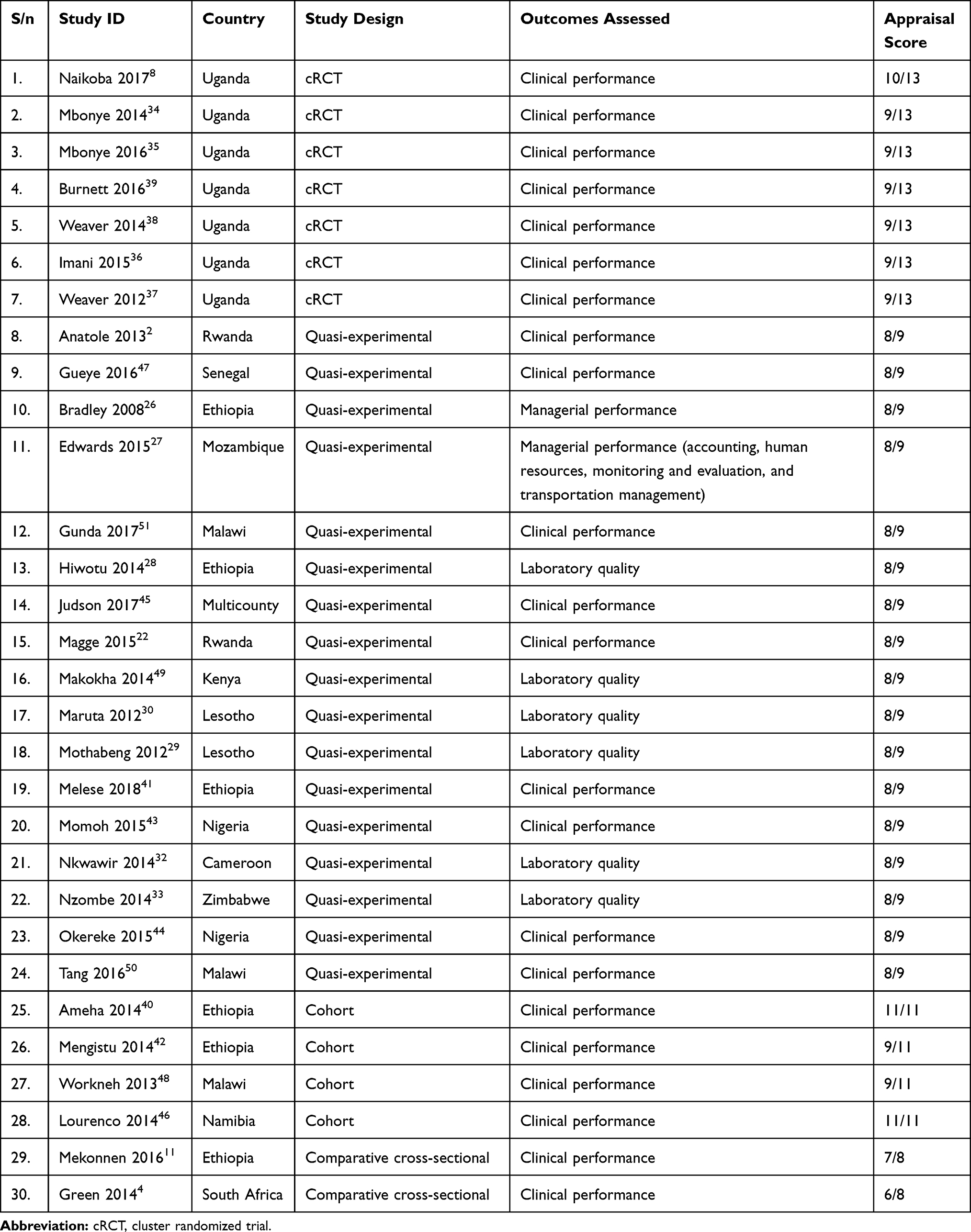 |
Table 1 Characteristics of the Included Studies |
One of the included clustered randomized trials8 received an appraisal score of 11/13. The trial utilized a random generator number to randomize the facilities and independent clinicians who were blinded to assess the outcomes. In the trial treatment allocation was not concealed. The trial did not describe whether participants and mentors (treatment administrators) were blinded or not. The second trial36 used random numbers generated by Stata to randomize the groups but did not blind assessors and mentors (treatment providers) and did not conceal treatment allocation from the project staff. The trial was assigned with an appraisal score of 9/13. For similar reasons, the third trial35 was also assigned an appraisal score of 9/13.For the intervention and outcomes of interest to the current review (one-on-one mentoring), these trials used cRCT design. Two studies34,35 reported on similar outcomes, the difference being one34 reporting on subgroups of populations (categorizing into 0 to 5 years and 5 years and above). In order to avoid duplication, we did not report findings from one of the two studies.34
Sixteen of the quasi-experimental studies2,4,22,26–30,32,33,41,43–45,47,49 did not include control groups and received appraisal scores of 8/9. Two of the cohort studies40,46 scored 11/11, while the other two42,48 scored 9/11 because they did not identify and control for confounders. One cross-sectional study4 did not identify and deal with confounding factors and hence it received 6/8. The other comparative cross-sectional study10 did not control for confounding factors, had control and experimental groups having different characteristics and did not take multiple measurements and received a score of 7/8.
Findings of the Included Studies
The included studies reported on the following major approaches to mentoring: mentoring by mobile team,8,34–39 twining higher performing institution with lower performing institution,26,45,49 embedded mentor support,30,32 providing mentoring support through e-mails and phone calls,43 visits by a single mobile mentor,51 and within-facility mentorship provided by a focal person, experienced or senior person or a manager.50 The included studies assessed the effectiveness of mentorship interventions in three areas: a) clinical competence and performance, b) managerial competence and performance, and c) laboratory quality. We report our findings in relation to these three outcomes in the section below.
Mentorship Interventions Designed to Improve Clinical Competence and Performance
Mentorship interventions reported under these outcomes were infectious disease management, integrated community case management, maternal, neonatal and child health services and family planning services.
Mentorship to Improve Infectious Disease Management
Seven articles reported the finding of one clustered randomized trial on the effect of mobile mentoring on knowledge and clinical competence in the management of infectious diseases8,34–39 The studies reported significant improvement in majority of the measured outcomes. One study8 reported that after the 9 months of mentorship intervention, the mean change in knowledge score in managing HIV and TB (as measured by case scenario) among providers in the intervention group was significantly higher when compared to that of providers in the control group (mean difference (MD) =14.5% (95% confidence interval (CI=8.2% to 20.8%)) (p<0.01)).8
Mbonye et al34 reported an increment in the proportion of patients that received an appropriate antimalarial that was 1.38 (99% CI: 0.89, 2.13) times higher among those prescribed any antimalarial in arms exposed to both onsite mentorship and integrated management of infectious diseases training (IMID) when compared to that of the arms exposed to IMID alone. It also reported that the proportion of patients with a negative diagnostic test result for malaria that was prescribed an antimalarial was 30% (adjusted relative risk ratio (aRRR)=0.70; 99% CI: 048, 1.00) lower in arm A when compared to that of arm B.34 In addition, Mbonye et al35 reported an increment in the proportion of emergency patients who received at least one appropriate treatment that was two times (aRRR=2.00; 99% CI=1.11–3.79, p<0.01) higher in the intervention arm (an arm exposed to both onsite mentorship and IMID training) when compared to that of the control arm (integrated management of infectious diseases training alone). The proportion of patients with a negative malaria test result that were prescribed an antimalarial was 35% (aRRR=0.65, 99% CI=0.44–0.98, p<0.01) lower in the intervention arm compared to that of the control arm.35
Similarly, Burnett et al39 reported that staff in the intervention arm (an arm exposed to both onsite mentorship and IMID training) performed significantly better than the control arm (an arm exposed to IMID training alone) in correctly completing laboratory procedures for HIV rapid testing (an adjusted relative risk (adj RR) (95% CI=1.18 (1.10–1.26) (p<0.01), TB sputum microscopy 1.29 (1.21–1.40), and malaria microscopy 1.19 (1.11–1.27) (P<0.01)).
Imani et al 36 reported 1.18 (aRRR=1.18; 95% CI=1.06–1.31) and 1.27 (adj RR=1.27; 95% CI=1.02–1.59) (p<0.01) times higher improvement in patient history taking and physical examination tasks, respectively, among professionals exposed to both IMID training and onsite support (mentoring) intervention when compared to that of a group exposed to IMID training alone. Surprisingly, Weaver 201237 found that only the combined effect of training and mentorship was statistically significant (not the mentorship alone). To the contrary, Weaver et al (2014)38 reported that mentoring intervention alone was effective in improving one indicator (emergency patients receiving at least one appropriate treatment) compared to training. In addition, it reported that mentoring combined with IMDI training was effective in improving six (three emergency triads (two on malaria and one on HIV)) indicators. The findings from these trials are summarized in Table 2.
 |
Table 2 Findings of Clustered Randomized Trials for Mentorship Support to Improve Infectious Disease Management |
Like the RCTs reported earlier, observational studies also reported significant improvements on several outcomes. A before-and-after study41 that evaluated the effect of mentoring program and placing supervisory tool for supervisors from 2011 to 2015 reported an increment in the proportion of health facilities with 100% data accuracy for all forms of TB from a baseline level of 55.1% to an end line level of 96.5%. Additionally, it reported an improvement in the TB cure rate from 71% at baseline level to 91.1% after the intervention. The treatment success rate increased from 88% at baseline to 95.3% after the intervention.
A retrospective cohort study46 evaluated the effect of onsite mentoring program on appropriate prescription of Artmesin-based combination therapy (ACT) that was complemented by enhanced training and educational SMS message sent on daily basis for two months. The study reported a reduction in the number of patients inappropriately receiving ACT after a negative test from 1046 before the mentorship intervention to 26 six months after the mentorship intervention (p<0.05).
A before-and-after study52 that evaluated the quality of ART management before and after mentoring reported improvements in drawing required bloods (91% at baseline vs 99% after the intervention, p<0.05), assessing adherence (50% vs 78%, p<0.001) and WHO staging (63% vs 91%, p<0.01). A study from Malawi48 conducted a monthly outreach mentorship visit by either a pediatrician or a medical officer experienced in provision of comprehensive pediatric HIV care or an experienced nurse mentor. The study reported that two outreach mentoring sites showed an improvement in documentation of pill count, viral load results, and correct laboratory monitoring and correct ART dosing (p<0.01 for all outcomes). At one of outreach mentoring sites, it found that improvements were made in pill count (0% to 25%) (p<0.05), disclosure (0% to 7%) (p>0.05) CD4 documentation (from 53% to 96%) (p<0.001), viral load (51% to 77%) (p<0.05). At another outreach mentoring site, it reported improvement only in viral load documentation (22% to 49%) (p<0.05) and correct ART dosing showing improvements (p<0.01). Findings from observational studies reporting on the effect of mentoring on clinical performance are summarized in Table 3.
 |
Table 3 Findings of Observational Studies for Mentorship in Clinical Performance |
Mentoring Intervention to Improve Maternal, Neonatal and Child Health Services
One aspect of the mentoring reported to under this theme was mentoring aiming to increase integrated community case management (ICCM). Two retrospective studies40,42 evaluated the effect of performance review and clinical mentoring meetings (PRCMM) on ICCM. One of the studies40 reported an improvement in the consistency of case management for pneumonia, malaria, and diarrhea from 23%, 26%, and 14%, respectively, at baseline to 70%, 69%, and 61% after the intervention. The study also reported a dose–response relationship between the intervention and its effect on ICCM. Similarly, another study42 found an increment in the consistency in classification for pneumonia (from 54.1% [95% CI: 47.7–60.5%] to 78.2% [73.9–82.5%]), malaria (from 50.8% [42.9–58.7%] to 78.9% [73.4–84.4%]), and diarrhea (from 33.7% [27.9–39.5%] to 70.0% [64.7–75.3%]).
A before-and-after study51 that aimed to promote retention among infants and mothers through mother-infant pair clinic by providing integrated care for HIV, maternal and childhood illnesses evaluated the effect of mentorship support to clinics. The study reported an improvement in mentoring score from 3.0 at quarter one of 2015 to 4.2 at quarter one of 2016. Another before-and-after study5 reported an improvement in correct IMNCI classification from 56.0% at baseline to 91.5% at the end line (p<0.01), correct treatment from the baseline level of 78.3% to 98.2% at end line (p<0.01).
Mentoring Intervention to Improve Antenatal Care Services
Anatole et al2 found an increment in the total number of antenatal care consultations from 200 at baseline to 749 after the intervention. Besides that, the study reported an increment in the number of assessments completed from the total of 60.1% (SD= 28) at baseline to 73.2% (SD=25.9) after the mentorship intervention. Though not statistically significant, the study also reported increment in the percentage of consultation that was correctly classified from 99.4% (166) at baseline to 99.2% (607) after the mentorship intervention (p=0.77).
A before-and-after study44 conducted in Nigeria evaluated the effect of mentoring on knowledge scores of maternal, newborn and child health such as the use of magnesium sulfate for preeclampsia, causes of anemia, management of postpartum hemorrhage (PPH), normal labor, obstetric emergency, and newborn resuscitation. The study reported an increment in the mean percentage of knowledge score significantly from 56±2.1 before mentoring intervention to 74.7±1.7 (p<0.01) six months after the intervention.
Another study11 reported on the effect of placing senior midwife mentors in district health offices on health workers’ performance in ANC, PNC, delivery and family planning. The study reported improvement in several maternal and newborn related outcomes following the mentoring intervention. After the mentoring program, 100% of the observed mentees in the implementation districts checked fundal height and fetal heartbeat and/or fetal movement, compared to only 75% and 88%, respectively, in the non-intervention districts. The proportion of healthcare workers in intervention districts who checked if the mothers had edema was 37% higher when compared to the healthcare workers in control districts. The proportion of healthcare workers in intervention districts who provided advice on using insecticide-treated nets in malaria zones was 18.75% higher when compared to healthcare workers in control districts. The study also reported that the use of partograph in the intervention districts was 29% higher when compared to that of the health workers in control districts. Additionally, the proportion of mentees who checked the weight of the newborn babies and signs of umbilical infection were 7% and 14% higher, respectively, in the intervention districts when compared to those health workers in the control districts.
Mentoring Intervention to Improve Emergency Obstetrics and Neonatal Care
A before-and-after study from Malawi50 reported a significant increment in knowledge scores following hospital-based mentoring intervention on emergency obstetrics and neonatal care knowledge and skills that was maintained after six months from the intervention (p<0.01).
Mentoring Intervention to Improve Family Planning Service Provision
A before-and-after study47 assessed the effect of mentoring on long-acting contraceptive service provision. It reported that the percentage of clinical providers with acceptable LARC performance (at least 80% of the observation checklist items correct) doubled from 32% in the baseline to 67% after the two mentoring visits.
Mentoring to Improve Cataract Surgeries
A before-and-after study45 reported an increment in average cataract surgeries per surgeon from 340 (range=200–566) to 786 (range=561–1181) after institutional mentorship, with 131% increase over four years ($ 11.44 spent per additional surgery).
Mentoring to Improve Managerial Performance and Advocacy Skills
A pre–post-descriptive study26 conducted in 14 hospitals in Ethiopia reported improvement in 45 of the 75 (60%) key management indicators between August 2006 and May 2007 following mentoring embedded mentoring program. It also reported a mean change in the management indicator of 7.5 (SD=5.9). Another before and after study27 reported a significant improvement in health system performance (accounting, human resources, monitoring and evaluation, and transportation management) following a one-year site-based health management mentorship. It also reported increment in the percentage of high quality (timely and accurate) reports from 75.0% at baseline (quarter 1) to 96.7% in quarter 2, 89.2% in Q3, and 91.7% in Q4. Similarly, a one group, pre and posttest study43 that assessed the effect of reproductive advocacy mentoring intervention for NGO staff in Nigeria reported an increment in the mean knowledge score on advocacy and policy issues from 39.1±17.6 at baseline to 76.2±14.2 six months after the intervention (p<0.01) (Table 4).
 |
Table 4 Findings of Observational Studies on Mentorship for Managerial Performance of Healthcare Institutions and Advocacy Skills Health Professionals |
Mentorship for Strengthening Laboratory Management Towards Accreditation
A before-and-after study29 assessed the effect of Strengthening Laboratory Management toward Accreditation (SLMTA) program on laboratory accreditation scores. Two methods were used to implement SLMTA. The first method is a “three workshops” approach lasting for 11 months. The second approach was twinning SLMTA with mentorship, which involved an intensive follow-up visit that lasted for 9 months. At the final assessment, 8 laboratories attained one star, 5 achieved two stars, and 4 achieved three stars from the baseline level where all but one laboratory was zero score. Another before-and-after study49 conducted in Kenya paired three laboratories, with nearby accredited research laboratories to provide institutional mentorship, with the other five receiving standard mentorship. The study reported an average of 12 additional percentage points among twinned laboratories compared to the increment of 28 additional percentage points in non-twinned laboratories.
A study32 that assessed the impact of a mentoring program that followed a workshop on the cross-cutting, productivity management, quality assurance, and documents and records management modules. The study reported increment in performance from baseline (18%) to 8 months after completion of the three workshops (85%). In addition, a before-and-after study33 conducted in Zimbabwe evaluated the effect of four model mentorship of laboratory quality using the revised version of the WHO AFRO Laboratory Accreditation Checklist. Model one (mentorship by the laboratory manager), model two (a monthly mentorship by national quality assurance program), model three (cyclical embedded mentorship after SLMTA where the national quality assurance was embedded in the laboratory for six weeks, away for eight weeks and back for another four weeks) and model four (cyclical embedded mentorship incorporated with SLMTA). The study found similar median improvements (from pre-SLMTA to post-mentorship) for all four models.
A before-and-after study28 that assessed the effect of Strengthening Laboratory Management toward Accreditation program on laboratory accreditation scores reported a 15% increase in Stepwise Laboratory Quality Improvement Process towards Accreditation audit score. The intervention also increased the number of laboratories with one to four-star scores from 0 level at baseline to 61% (n = 14/23) (for the cohort I) and 48% (n = 10/21) (for cohort II laboratories) at end line. Another before-and-after study30 conducted in Lesotho reported a significant improvement in average scores (182.3; p< 0.05) following a 10 weeks laboratory mentorship that was separated by 6–8 weeks that was conducted in four hospital laboratories reported Findings of the studies reporting on the effect of mentoring on improving laboratory quality are summarized in Table 5.
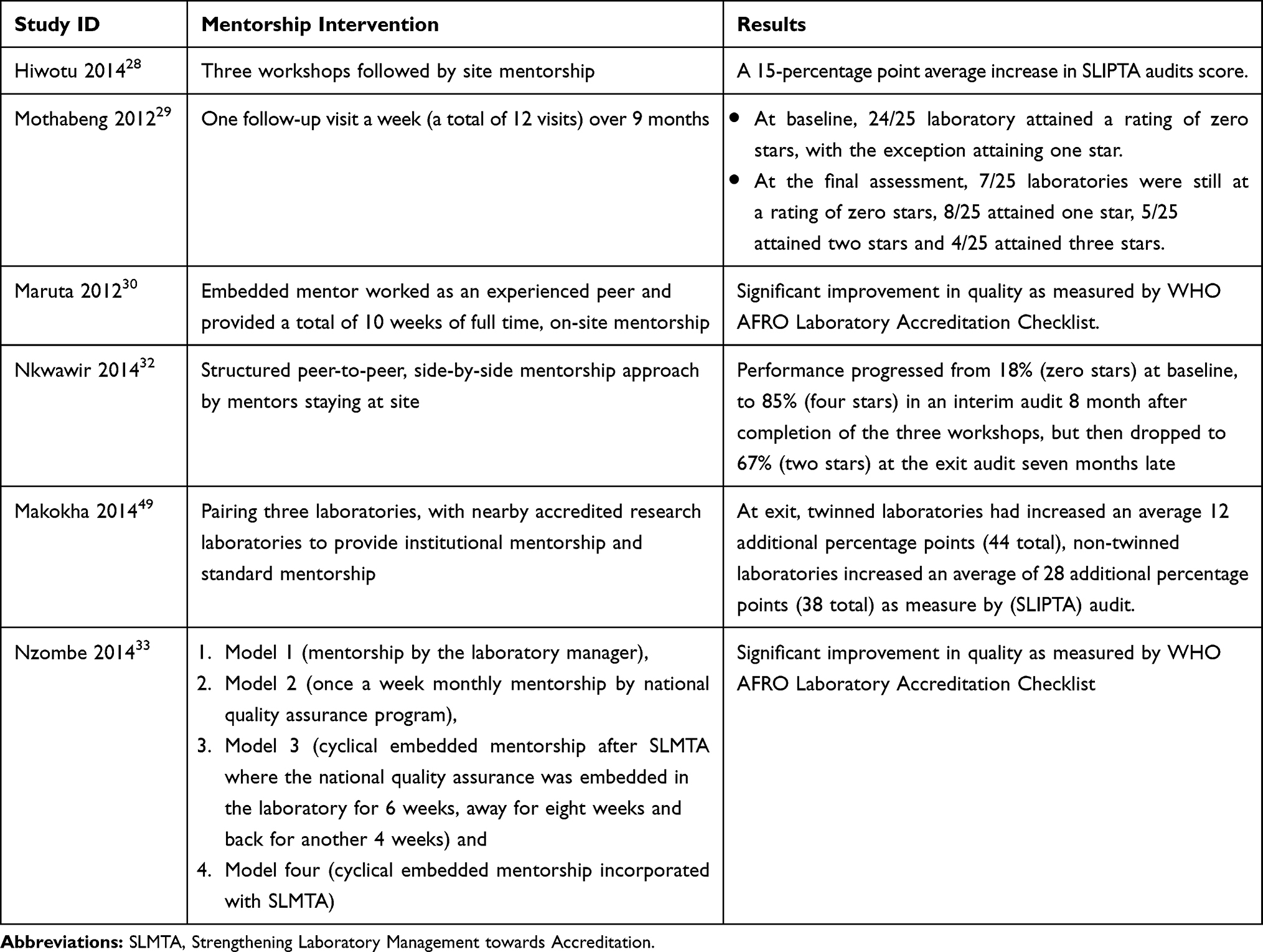 |
Table 5 Findings for Mentorship for Strengthening Laboratory Management Toward Accreditation (SLAMTA) |
Discussion
This review sought to locate, critically appraise and analyze the findings of studies reporting on the nature and outcomes of mentorship interventions conducted across a range of African countries. The studies included in the review addressed different approaches to mentorship interventions. Thus, mentorship has been utilized to strengthen laboratory services,28–30,32,33,49 to increase health workers competence in the management of different health problems, such as HIV, malaria, TB and maternal and child health problems.2,4,8,11,22,26,34–48 Mentorship interventions have also been utilized to improve health system management skills.26,27
Mentorship comes in many forms. The major approaches to mentorship reported in the included studies were: mentorship support by a mobile mentor or a mobile multidisciplinary team,8,34–39 within-facility mentorship approach provided by staff in managerial position,50 embedded mentors support,11 remote mentorship intervention and twinning institutions to facilitate the support of more experienced institution to that of less experienced institution26,45,49 and remote mentorship through phone and e-mail communications.43
Though the indirect findings from one study indicated that mentorship programs that followed didactic training were more effective compared to mentorship programs alone,37 the included studies did not generally compare one type of mentorship intervention with another type. This remains an outstanding knowledge gap.
Suboptimal healthcare practices usually emanate from limited competence of health workers and the lack of management support.53,54 Almost all the studies included in this review reported significant improvement in one or more of the outcomes of interest such as health professional knowledge and skills, health professional performance and facility performance.8,34–39 In relation to health worker performance, mentorship interventions were effective as reported in several of the included studies. These findings show that continued in-service professional development contributes to the quality health services delivered.55 This ensures that health professionals, apart from reciting what they already know, have the opportunity to get updates on new developments in their fields and provide evidence informed clinical care. Specifically, the interventions increased the adherence of healthcare workers to standard protocols.2,22,47 This implies that mentorship programs offer a significant potential to introduce new policies, protocols, and guidelines.56 Moreover, the mentorship interventions in this review addressed various health programs including HIV, TB, infectious diseases, maternal and child health services. This implies that program implementers and policy makers can utilize mentorship interventions to improve the quality of services and performance of healthcare workers.
Additionally, mentorship programs were found to be effective in improving the managerial skills of health managers.27,57 This is critical, because the commitment and support by the management may affect the implementation of best practices independently from the presence of competent health professionals.58,59 However, from what we found in this review it is evident that the effect of mentorship interventions in improving facility leadership, management and governance (LMG) is not well studied. The studies addressing this outcome of interest were only three and these studies have addressed only a limited number of indicators related to LMG. Hence, further studies evaluating the contribution of mentorship interventions improving health facility and health systems LMG are required.
Notably, we found that mentorship interventions were effective in improving the quality and rating of laboratory services.28–30,32,33,49 Since use of standard protocols (SOPs) is characteristic of laboratory services, it follows that the effect of mentorship interventions is much more palpable in this area of work in the health facility. The findings from the included studies showed that mentorship was used to introduce new services or improve already existing services in the laboratories. This implies that mentorship interventions are more effective in areas where what is executed by the professional is skill based and governed by more structured procedures.
One study included in the current review demonstrated that remote mentorship through phone and e-mail communications were effective in improving knowledge score on advocacy and policy issues at pre-test and posttest.43 This has policy implications in designing health services for remote health facilities were there are huge gaps in skill and competency of healthcare professionals.1
A closer look at the nature of the mentorship interventions reported in the included studies reveals that there is a lack of uniformity in how the interventions are designed and implemented. This is problematic for two reasons. First, this makes difficult, if not impossible, any intention of creating a link between mentorship interventions and any of the outcomes of interest. Second, given this variation recommendation of any of the mentorship approaches for adoption or adaptation in similar settings is not straightforward. Therefore, further evidence is required to adequately identify the nature of interventions which are particularly effective in improving any of the outcomes of interest.
While the current review provided helpful information that may help policy makers for making evidence-informed decisions, it is worth to consider the limitations of the current review. Given that the mentoring interventions, the participants or the fidelity of the mentoring interventions reported in the studies reported in the current review were different across the included studies, we could not conduct meta-analysis of the findings. Additionally, the outcomes of interests were measured differently across the studies. The methodological qualities of the included studies were poor. Therefore, further research—experimental methods measuring the impact of different mentorship formats and longitudinal studies establishing their longer-term effectiveness—is required to compare the effectiveness and cost-effectiveness of one model of mentorship over the other. Another limitation of the current review is that it did not address contextual factors – resources, supportive structures and other factors that may determine why mentoring interventions were effective or not. Therefore, studies addressing why and how different mentoring programs succeeded and the meaningfulness of the mentoring interventions for the different participants should be further investigated. Furthermore, the outcomes reported in the current review were measured differently across different studies and across different areas of practice. Hence, GRADE assessment was not conducted.
Conclusions
A variety of different approaches of mentorship were reported: a) placing a mentor in healthcare facility for some time (embedded mentor), b) visits by a mobile mentor, c) mentorship by a team of mobile multidisciplinary mentors, d) facility twinning, e) within-facility mentorship by a focal person or a manager. These mentorship interventions were effective in improving clinical competence, institutional managerial performance, and laboratory quality improvement. Almost all of the included studies reported that mentorship interventions were effective in improving all or many of the outcomes of interest. Mentoring interventions were used as a mechanism for improving maternal, neonatal, child services and strengthening laboratory management towards accreditation. Mentoring interventions, when combined with training, have resulted in higher competence of clinicians in the management of infectious diseases compared to traditional training interventions alone. Mentoring interventions were also found to improve managerial performance (accounting, human resources, monitoring and evaluation, and transportation management) of health institutions.
Implication for Practice
Mentorship interventions may be used to increase adherence of health professionals to guidelines, standards, and protocols. While different types of interventions (embedded mentoring, visits by mobile mentors, facility twinning and within-facility mentorship by a focal person) were reported to be effective, there is no evidence to support recommendation of one model of mentorship over other approaches.
Implication for Research
We did not find any study that compared one approach of mentorship with the other and future research should address this gap. The qualities of the included studies were poor. Hence, future studies should use high-quality research designs such as randomized controlled studies. Further research is also needed to compare the cost-effectiveness of mentorship interventions. The health systems structures and resources—resources, institutional mechanisms to support career progression—mentorship need to be captured as well given their significance for the outcomes. Moreover, the feasibility, applicability, and meaningfulness of mentoring interventions to different participants and contexts should be further investigated.
Acknowledgments
Authors acknowledge the feedback provided by Dr. Daniel Burssa of Federal Ministry of Health, Ethiopia. The authors are grateful to Jimma University Rapid Review Response Center: AHPSR/WHO Center of Excellence for sponsoring this review.
Author Contributions
GTF performed the formal analysis, was responsible for project administration, and wrote the original draft of the manuscript. All authors contributed to conception of the study, methodology, data curation, validation, visualization, data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflict of interest.
References
1. Bhutta ZA, Lassi ZS, Mansoor N. Systematic Review on Human Resources for Health Interventions to Improve Maternal health Outcomes: Evidence from Developing Countries. World health organization (WHO); 2010.
2. Anatole M, Magge H, Redditt V, et al. Nurse mentorship to improve the quality of health care delivery in rural Rwanda. Nurs Outlook. 2013;61(3):137–144. doi:10.1016/j.outlook.2012.10.003
3. Vasan A, Mabey DC, Chaudhri S, Brown Epstein H-A, Lawn SD. Support and performance improvement for primary health care workers in low-and middle-income countries: a scoping review of intervention design and methods. Health Policy Plan. 2017;32(3):437–452. doi:10.1093/heapol/czw144
4. Green A, de Azevedo V, Patten G, Davies MA, Ibeto M, Cox V. Clinical mentorship of nurse initiated antiretroviral therapy in Khayelitsha, South Africa: a quality of care assessment. PLoS One. 2014;9(6):e98389.
5. Manzi A, Magge H, Hedt-Gauthier BL, et al. Clinical mentorship to improve pediatric quality of care at the health centers in rural Rwanda: a qualitative study of perceptions and acceptability of health care workers. BMC Health Serv Res. 2014;20(14):275. doi:10.1186/1472-6963-14-275
6. World Health Organization. WHO Recommendations for Clinical Mentoring to Support Scale-Up of HIV Care, antiretroViral Therapy and preVention in Resource-Constrained Settings. Geneva, Switzerland: WHO; March 7-8 2005.
7. Ghosh R, Rejo TG. Career benefits associated with mentoring for mentors: a meta-analysis. J Vocat Behav. 2013;83:106–116. doi:10.1016/j.jvb.2013.03.011
8. Naikoba S, Senjovu KD, Mugabe P, et al. Improved HIV and TB knowledge and competence among mid-level providers in a cluster-randomized trial of one-on-one mentorship for task shifting. J Acquir Immune Defic Syndr. 2017;75(5):e120–e127. doi:10.1097/QAI.0000000000001378
9. Schwerdtle P, Morphet J, Hall H. A scoping review of mentorship of health personnel to improve the quality of health care in low and middle-income countries. Global Health. 2017;13(77). doi:10.1186/s12992-017-0301-1
10. Republic of Kenya Ministry of Health. Strengthening RH/HIV Integration Services: National Mentorship Guidelines.
11. Mekonnen Y, Haddis L, Asefa S, Kefale M. A study into the effectiveness of the midwives’ mentorship for improving maternal and new born health care programme in Ethiopia. 2016. Available from : https://www.jarrco.info/uploads/36678796657d2baa64b8098.30952292.pdf. Accessed December 2, 2019.
12. Republic of Zambia Ministry of Health. Guidelines for Clinical Mentorship of Health Care Workers in Zambia. Health. RoZMo; 2012.
13. McKenna LS. Introduction to Teaching and Learning in Health Professions. Sydney: Lippincott Williams and Wilkins; 2013.
14. Wensel T. Mentor or preceptor: what is the difference? Am J Health-System Pharm. 2006;63(17):1597. doi:10.2146/ajhp060121
15. National Department of Health, Republic of South Africa. Clinical Mentorship Guideline for Integrated Services. National Department of Health RoSA; January 2011.
16. World Health Organization. WHO Recommendations for Clinical Mentoring to Support Scale-Up of HIV Care, Antiretroviral Therapy and Prevention in Resource-Constrained Settings. Kampala, Uganda; June 16–18 2005.
17. Kanaskie ML. Mentoring–a staff retention tool. Crit Care Nurs Q. 2006;29(3):248–252. doi:10.1097/00002727-200607000-00010
18. Zhang Y, Qjan Y, Wu J, Wen F, Zhang Y. The effectiveness and implementing a mentoring program for a newly graduated nurses: a systematic review. Nurse Educ Today. 2016;37:136–144. doi:10.1016/j.nedt.2015.11.027
19. Maruta T, Rotz P, Peter T. Setting up a structured laboratory mentoring programme. Afr J Lab Med. 2013;2(1). doi:10.4102/ajlm.v2i1.77
20. Sambunjak D, Straus SE, Marusic A. A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine. J Gen Intern Med. 2010;25(1):72–78. doi:10.1007/s11606-009-1165-8
21. Chen C, Lou M-F. The effectiveness and application of mentorship programmes for recently registered nurses: a systematic review. J Nurs Manag. 2014;22(1):433–442. doi:10.1111/jonm.12102
22. Magge H, Anatole M, Cyamatare FR, et al. Mentoring and quality improvement strengthen integrated management of childhood illness implementation in rural Rwanda. Arch Dis Child. 2015;100(6):565–570.
23. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
24. Belrhiti Z, Booth A, Marchal B, Verstraeten R. To what extent do site-based training, mentoring, and operational research improve district health system management and leadership in low- and middle-income countries: a systematic review protocol. Syst Rev. 2016;5(1):70. doi:10.1186/s13643-016-0239-z
25. GRADEpro G. GRADEpro Guideline Development Tool [Software]. McMaster University; 2015.
26. Bradley E, Hartwig KA, Rowe LA, et al. Hospital quality improvement in Ethiopia: a partnership-mentoring model. Int j Qual Health Care. 2008;20(6):392–399. doi:10.1093/intqhc/mzn042
27. Edwards LJ, Moises A, Nzaramba M, et al. Implementation of a health management mentoring program: year-1 evaluation of its impact on health system strengthening in Zambezia Province, Mozambique. Int j Health Policy Manage. 2015;4(6):353–361. doi:10.15171/ijhpm.2015.58
28. Hiwotu TM, Ayana G, Mulugeta A, et al. Laboratory system strengthening and quality improvement in Ethiopia. Afr J Lab Med. 2016;3(2):1–6.
29. Mothabeng D, Lebina M, Maruta T, Wanyoike J, Lewis K, Mengstu Y. Strengthening laboratory management towards accreditation: the Lesotho experience. Afr J Lab Med. 2012;1(1):1–7.
30. Maruta T, Rotz PJ, Wanyoike J, Peter T, Motebang D, Mathabo L. Impact of mentorship on WHO-AFRO strengthening laboratory quality improvement process towards accreditation (SLIPTA). Afr J Lab Med. 2012;1(1):1–8.
31. Nkwawir SC, Batumani NN, Awasom CN, Maruta T. From grass to grace: how SLMTA revolutionised the Bamenda regional hospital laboratory in Cameroon. Afr J Lab Med. 2016;3(2):1–6.
32. Nkwawir S, Batumani N, Maruta T, Awasom C. From grass to grace: how SLMTA revolutionised the Bamenda Regional Hospital Laboratory in Cameroon. Afr J Lab Med. 2014;3(2):
33. Nzombe P, Luman E, Shumba E. Maximising mentorship: variations in laboratory mentorship models implemented in Zimbabwe. Afr J Lab Med. 2014;3(2):241.
34. Mbonye MK, Burnett SM, Burua A, et al. Effect of integrated capacity-building interventions on malaria case management by health professionals in Uganda: a mixed design study with pre/post and cluster randomized trial components. PLoS One. 2014;9(1):e84945.
35. Mbonye MK, Burnett SM, Naikoba S, et al. Effectiveness of educational outreach in infectious diseases management: a cluster randomized trial in Uganda. BMC Public Health. 2016;16(1):714. doi:10.1186/s12889-016-3375-4
36. Imani P, Jakech B, Kirunda I, Mbonye MK, Naikoba S, Weaver MR. Effect of integrated infectious disease training and on-site support on the management of childhood illnesses in Uganda: a cluster randomized trial. BMC Pediatr. 2015;15(1):103. doi:10.1186/s12887-015-0410-z
37. Weaver MR, Crozier I, Eleku S, et al. Capacity-building and clinical competence in infectious disease in Uganda: a mixed-design study with pre/post and cluster-randomized trial components. PLoS One. 2012;7(12):e51319.
38. Weaver MR, Burnett SM, Crozier I, et al. Improving facility performance in infectious disease care in Uganda: a mixed design study with pre/post and cluster randomized trial components. PLoS One. 2014;9(8):e103017.
39. Burnett SM, Mbonye MK, Martin R, et al. Effect of on-site support on laboratory practice for human immunodeficiency virus, tuberculosis, and malaria testing. Am J Clin Pathol. 2016;146(4):469–477. doi:10.1093/ajcp/aqw138
40. Ameha A, Karim AM, Erbo A, et al. Effectiveness of supportive supervision on the consistency of integrated community cases management skills of the health extension workers in 113 districts of Ethiopia. Measurements. 2013;52:65–71.
41. Melese M, Habte D, Girma B, et al. Use of indicators of standards of care to improve tuberculosis program management in Ethiopia. J Clin Tuberc Other Mycobact Dis. 2018;10:17–23. doi:10.1016/j.jctube.2017.12.001
42. Mengistu B, Karim AM, Eniyew A, et al. Effect of performance review and clinical mentoring meetings (PRCMM) on recording of community case management by health extension workers in Ethiopia. Ethiop Med J. 2014;52(Supp. 3):73–81.
43. Momoh GT, Oluwasanu MM, Oduola OL, Delano GE, Ladipo OA. Outcome of a reproductive health advocacy mentoring intervention for staff of selected non-governmental organisations in Nigeria. BMC Health Serv Res. 2015;15:314. doi:10.1186/s12913-015-0975-0
44. Okereke E, Tukur J, Oginni AB, Obonyo B. Evaluating health workers’ knowledge following the introduction of clinical mentoring in Jigawa State, Northern Nigeria. Afr J Reprod Health. 2015;19(3):118–125.
45. Judson K, Courtright P, Ravilla T, Khanna R, Bassett K. Impact of systematic capacity building on cataract surgical service development in 25 hospitals. BMC Ophthalmol. 2017;17(1):96. doi:10.1186/s12886-017-0492-5
46. Lourenço C, Kandula D, Haidula L, Ward A, Cohen JM. Strengthening malaria diagnosis and appropriate treatment in Namibia: a test of case management training interventions in Kavango Region. Malar J. 2014;13(1):508.
47. Gueye B, Wesson J, Koumtingue D, et al. Mentoring, task sharing, and community outreach through the tutoratplus approach: increasing use of long-acting reversible contraceptives in Senegal. Global Health. 2016;4(Suppl 2):S33–S43.
48. Workneh G, Scherzer L, Kirk B, et al. Evaluation of the effectiveness of an outreach clinical mentoring programme in support of paediatric HIV care scale-up in Botswana. AIDS Care. 2013;25(1):11–19. doi:10.1080/09540121.2012.674096
49. Makokha EP, Mwalili S, Basiye FL, et al. Using standard and institutional mentorship models to implement SLMTA in Kenya. Afr J Lab Med. 2014;3(2). doi:10.4102/ajlm.v3i2.220
50. Tang JH, Kaliti C, Bengtson A, et al. Improvement and retention of emergency obstetrics and neonatal care knowledge and skills in a hospital mentorship program in Lilongwe, Malawi. Int j Gynaecol Obstetr. 2016;132(2):240–243. doi:10.1016/j.ijgo.2015.06.062
51. Gunda A, Jousset A, Tchereni T, Joseph J, Mwapasa V. Integrating HIV and maternal, neonatal and child health services in rural Malawi: an evaluation of the implementation processes and challenges. J Acquir Immune Defic Syndr. 2017;75:S132–S139. doi:10.1097/QAI.0000000000001367
52. Green A, de Azevedo V, Patten G, Davies M-A, Ibeto M, Cox V. Clinical mentorship of nurse initiated antiretroviral therapy in Khayelitsha, South Africa: A quality of care assessment. PLoS One. 2014;9(6):e98389. doi:10.1371/journal.pone.0098389
53. Harrison MB, Légaré F, Graham ID, Fervers B. Adapting clinical practice guidelines to local context and assessing barriers to their use. Can Med Assoc J. 2010;182(2):E78–E84. doi:10.1503/cmaj.081232
54. Legare F, Ratte S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision making in clinical practice: update of a systematic review of health professionals’ perceptions. Patient Educ Couns. 2008;73:526–535. doi:10.1016/j.pec.2008.07.018
55. Opiyo N, Mike E. In-service training for health professionals to improve care of seriously ill newborns and children in low-income countries. Cochrane Database Syst Rev. 2015;2015(5):
56. Grimshaw J, Eccles M, Tetroe J. Implementing clinical guidelines: current evidence and future implications. J Contin Educ Health Prof. 2004;24(S1):S31–S37. doi:10.1002/chp.1340240506
57. Hartwig K, Pashman J, Cherlin E, et al. Hospital management in the context of health sector reform: a planning model in Ethiopia. Int J Health Plann Manage. 2008;23(3):203–218. doi:10.1002/hpm.915
58. Michie S, Pilling S, Garety P, et al. Difficulties implementing a mental health guideline: an exploratory investigation using psychological theory. Implement Sci. 2007;2. doi:10.1186/1748-5908-2-8
59. French SD, Green SE, O’Connor DA, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the Theoretical Domains Framework. Implement Sci. 2012;7(1):38. doi:10.1186/1748-5908-7-38
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.