Back to Journals » International Medical Case Reports Journal » Volume 19
Honey Phonophoresis as an Adjunctive Multimodal Intervention in Knee Osteoarthritis: A Case Report
Authors Ahmed MM ![]() , Alomairy N
, Alomairy N ![]() , Elbendary EY, Al Areefy AA, Elnaeem M, Ayoub A, Amin WM
, Elbendary EY, Al Areefy AA, Elnaeem M, Ayoub A, Amin WM ![]()
Received 6 January 2026
Accepted for publication 4 March 2026
Published 10 March 2026 Volume 2026:19 592408
DOI https://doi.org/10.2147/IMCRJ.S592408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Mohamed M Ahmed,1,2,* Nada Alomairy,3,* Ehab Yones Elbendary,4,5,* Azza A Al Areefy,4,6,* Mozdalifah Elnaeem,3,* Abdulraouf Ayoub,1,* Wafaa Mahmoud Amin1,7,*
1Department of Physical Therapy, College of Nursing and Health Sciences, Jazan University, Jazan, 82817, Saudi Arabia; 2Department of Basic Science in Physical Therapy, Faculty of Physical Therapy, Beni Suef University, Beni Suef, 62511, Egypt; 3Diagnostic Radiography Technology Department, College of Nursing and Health Sciences, Jazan University, Jazan, 82817, Saudi Arabia; 4Clinical Nutrition Department, Nursing and Health Sciences, Jazan University, Jazan, 82817, Saudi Arabia; 5Specialized Medical Hospital, Faculty of Medicine, Mansoura University, Mansoura, 35516, Egypt; 6Department of Nutrition and Food Science, Faculty of Home Economics, Helwan University, Helwan, 1171, Egypt; 7Department of Basic Science for Physical Therapy, Faculty of Physical Therapy, Cairo University, Giza, 12613, Egypt
*These authors contributed equally to this work
Correspondence: Wafaa Mahmoud Amin, Department of Physical Therapy, College of Nursing and Health Sciences, Jazan University, P.O. Box. 114, Jazan, 82817, Saudi Arabia, Tel +966596211342, Email [email protected]
Purpose: To clarify the clinical, imaging, and laboratory changes after application of honey phonophoresis combined with conventional physiotherapy in a patient with knee osteoarthritis (OA).
Patients and Methods: A 55-year-old male with Grade II medial knee osteoarthritis presented with chronic pain, morning stiffness, and functional limitations. Baseline assessment included pain intensity, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), musculoskeletal ultrasound (MSK-US) evaluation of medial femoral cartilage thickness, and systemic inflammatory markers. The patient underwent a four-week multimodal physiotherapy program consisting of honey phonophoresis applied to the medial tibiofemoral compartment, transcutaneous electrical nerve stimulation (TENS), and supervised quadriceps strengthening exercises.
Results: Following the intervention, pain intensity decreased from 8/10 to 4/10, and the total WOMAC score improved from 58/96 to 43/96. MSK-US demonstrated increased medial femoral cartilage thickness on both longitudinal (0.26 to 0.30 cm) and transverse (0.20 to 0.26 cm) posterior views. Systemic inflammatory markers also improved, with C-reactive protein decreasing from 8.08 to 5.2 mg/L and erythrocyte sedimentation rate from 29 to 18 mm/h. No adverse events were observed.
Conclusion: Integration of honey phonophoresis with conventional physiotherapy in this single case may be associated with improvements in the patient’s reported outcomes, cartilage ultrasound assessment, and inflammatory biomarkers in OA. Causal relationships cannot be inferred from a single case due to the uncontrolled, multimodal design; thus, imaging changes should be interpreted cautiously. The findings of this case are exploratory and hypothesis-generating, supporting further investigation through well-designed randomized controlled trials.
Keywords: knee osteoarthritis, honey phonophoresis, musculoskeletal ultrasound, cartilage thickness, c-reactive protein, erythrocyte sedimentation rate
Introduction
Osteoarthritis (OA) is the most prevalent chronic joint disorder and a leading cause of pain, disability, and reduced quality of life worldwide, particularly among older adults. Although traditionally viewed as a purely degenerative mechanical condition, OA is now widely recognized as a complex, whole-joint disease characterized by low-grade inflammation, oxidative stress, synovial activation, subchondral bone remodeling, and progressive cartilage degradation. These interconnected pathological processes contribute to pain sensitization, functional limitations, and gradual structural deterioration of the joint.1,2 Knee OA symptoms vary significantly, with notable day-to-day pain fluctuations observed in cohort studies, highlighting the challenges in interpreting short-term symptom changes.3 Also, structural alterations in the menisci are associated with osteoarthritis severity, underscoring OA as a complex joint disease beyond cartilage deterioration.4
Articular cartilage has a limited intrinsic capacity for repair due to its avascular and abneural nature, making disease modification in OA particularly challenging. Consequently, conservative management strategies remain the first-line approach and primarily focus on symptom reduction, functional improvement, and slowing disease progression rather than true biological restoration. Physiotherapy interventions, including therapeutic exercise and electro-physical modalities, are strongly recommended in clinical guidelines and play a central role in OA management. However, there is increasing interest in adjunctive therapies that may influence inflammatory and biological pathways underlying OA pathophysiology rather than focusing solely on biomechanics.1,5
Honey is a natural substance with a complex biochemical composition, containing a wide range of polyphenols, flavonoids, phenolic acids, and other bioactive compounds. Experimental and translational research has demonstrated that honey possesses antioxidant, anti-inflammatory, antimicrobial, and tissue-protective properties. Emerging evidence suggests that specific honey-derived flavonoids may exert chondroprotective effects by reducing oxidative stress, modulating inflammatory mediators, and supporting cartilage homeostasis, all of which are highly relevant to OA pathology. Despite these promising biological properties, the clinical application of honey in musculoskeletal and joint disorders remains limited, and its potential role as a biologically active adjunct in OA has not been sufficiently explored.6–11
Recent research in osteoarthritis emphasizes regenerative and disease-modifying strategies that target inflammatory and cartilage repair pathways, suggesting that osteoarthritis may be a modifiable condition.12–15
Phonophoresis is a non-invasive therapeutic technique that uses ultrasound to enhance the transdermal delivery of topically applied agents by increasing tissue permeability through acoustic cavitation and microstreaming. Phonophoresis has been successfully employed to improve the clinical effectiveness of various pharmacological and biologically active substances in musculoskeletal conditions, including knee OA. In addition, recent experimental studies have demonstrated that ultrasound exposure may enhance the bioavailability and antioxidant capacity of honey, potentially amplifying its biological activity when used as a coupling medium during ultrasound therapy.16–18
From a multidisciplinary perspective, integrating a biologically active natural substance with a physical delivery modality and conventional physiotherapy represents a translational approach that bridges rehabilitation science, imaging, and inflammation biology. To our knowledge, published clinical reports have investigated the use of honey phonophoresis in knee osteoarthritis, while simultaneously assessing patient-reported outcomes and objective structural changes using musculoskeletal ultrasound; systemic inflammatory biomarkers have not been assessed. Addressing this gap is particularly relevant for multidisciplinary healthcare settings, where accessible, safe, and cost-effective interventions with potential biological benefits are highly desirable.
Phonophoresis and biologically active topical agents are mentioned in musculoskeletal rehabilitation,2,19 but there is limited data integrating clinical outcomes, ultrasound-based cartilage assessment, and inflammatory biomarkers in a single-case context, highlighting the need for careful exploratory studies. Therefore, the purpose of this case report is to explore the clinical, structural, and biological effects of honey phonophoresis combined with conventional physiotherapy in a patient with knee osteoarthritis. This case report does not propose a novel therapeutic modality but aims to provide exploratory observations integrating clinical, imaging, and laboratory parameters within a descriptive case framework on the role of honey phonophoresis as an adjunctive intervention in OA management.
Materials and Methods
Case Description
The patient was a 55-year-old male office worker (height: 169 cm; weight: 71 kg; body mass index: 24.9 kg/m2) who presented with a six-month history of progressively worsening pain localized to the medial aspect of the left knee. The patient reported associated morning stiffness, a subjective sense of weakness, and increasing difficulty performing activities of daily living, particularly sit-to-stand transfers, stair negotiation, and prolonged ambulation. These functional complaints are commonly reported in individuals with knee osteoarthritis and reflect the combined impact of pain, stiffness, and neuromuscular impairment on daily function.1
Methodology
At the time of initial assessment, the patient rated his maximum pain intensity as 8 out of 10 on the Numeric Pain Rating Scale during weight-bearing activities involving the affected knee. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was used to assess disease severity and functional status. Baseline WOMAC scores revealed a pain subscale score of 11 out of 20, stiffness score of 5 out of 8, and physical function score of 42 out of 68, resulting in a total WOMAC score of 58 out of 96, indicative of moderate knee osteoarthritis–related disability. The WOMAC index is a validated, widely used outcome measure for evaluating pain, stiffness, and functional limitations in individuals with knee osteoarthritis.6
The patient had not sought prior medical consultation for his knee symptoms and was not receiving pharmacological treatment at the time of referral to physical therapy. There was no reported history of previous knee surgery, acute trauma, inflammatory arthropathy, or systemic disease affecting the musculoskeletal system. Clinical examination revealed localized tenderness along the medial joint line of the left knee and reduced quadriceps strength, findings frequently associated with symptomatic knee osteoarthritis and contributing to functional impairment.20
Baseline laboratory investigations demonstrated elevated markers of systemic inflammation, with serum C-reactive protein (CRP) measured at 8.08 mg/L and erythrocyte sedimentation rate (ESR) at 29 mm/h. Although osteoarthritis is not classically considered a systemic inflammatory disease, low-grade elevations in inflammatory biomarkers have been reported. They are thought to reflect synovial inflammation and disease activity in subsets of patients with knee osteoarthritis.5 Inflammatory biomarkers were collected during routine clinical assessments and subsequently used for research purposes, without any additional invasive procedures.
Musculoskeletal ultrasound (MSK-US) examination of the left knee was performed using posterior longitudinal and transverse approaches to assess medial femoral cartilage thickness. All examinations were conducted by experienced radiology specialists using consistent techniques and standardized protocols for proper probe positioning and anatomy identification. The same radiologist performed the pre- and post-MSK-US; she positioned the patient in the prone position, with the knee fully extended and relaxed, and scanned the popliteal fossa to assess the posterior portions of the femoral condyles.19 Ultrasound imaging revealed reduced cartilage thickness over the medial tibiofemoral compartment, measuring 0.26 cm on the longitudinal view (Figure 1) and 0.20 cm on the transverse view (Figure 2). MSK-US is increasingly recognized as a reliable, non-invasive imaging modality for evaluating cartilage morphology and structural changes in knee osteoarthritis, particularly in the medial compartment.11,18
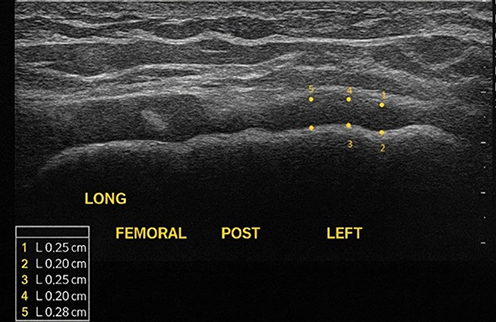 |
Figure 1 Longitudinal posterior musculoskeletal measurements of femoral cartilage (pretreatment), with five sequential measurement points (1–5) marked in yellow. Cartilage thickness values, shown in centimeters, are indicated in the measurement panel (L = length measurement). |
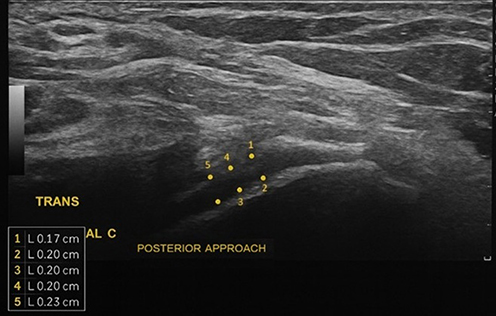 |
Figure 2 Transverse posterior musculoskeletal measurements of femoral cartilage (pretreatment), with five sequential cartilage thickness measurements indicated by numbered yellow markers (1–5). The thickness values in centimeters are shown in the embedded measurement panel, with “L” indicating length. |
A 14 MHZ linear transducer was used to perform both longitudinal and transverse scanning to evaluate the posterior aspect of the medial femoral condyle. Ensuring the ultrasound beam was kept as perpendicular as possible to the cartilage surface to minimize anisotropy artifacts and obtain accurate thickness measurements.18
Three adjacent (2 mm) cartilage thicknesses were measured from a thin hyper-echoic line at the soft tissue-cartilage interface to the hyper-echoic line at the cartilage–bone interface. These three values were averaged to comprise a single thickness value, which was representative of the middle medial femoral condyle cartilage thickness.11,18
Based on the clinical presentation, functional assessment, laboratory findings, imaging results, and the Kellgren–Lawrence grading system, the patient was diagnosed with Grade II left knee osteoarthritis, which is characterized by noticeable osteophyte formation and possible joint space narrowing.21
Ethical Approval and Consent
The case was conducted in accordance with the Declaration of Helsinki. Per our institutional regulations, approval was required for the publication of patient clinical details and imaging findings. Ethical approval to publish the case details was obtained from the Institutional Review Board of Jazan University, the Standing Committee for Scientific Research (HAPO-10-Z-001; approval reference REC-45/05/851), Gizan, Saudi Arabia. Written informed consent was obtained for participation and publication of anonymized clinical information and images.
Intervention
The intervention program was delivered over four weeks and consisted of three treatment sessions per week on alternate days, for a total of twelve sessions. This treatment frequency and duration are consistent with commonly applied physiotherapy protocols for knee osteoarthritis and have been reported to produce clinically meaningful improvements in pain and function.2,5 The intervention was designed as a multimodal physiotherapeutic approach combining honey phonophoresis, transcutaneous electrical nerve stimulation (TENS), and supervised therapeutic exercises.
Honey phonophoresis was applied to the medial tibiofemoral compartment of the left knee using therapeutic ultrasound. Ultrasound was delivered in continuous mode at 1 MHz and 1 W/cm2 for 10 minutes per session.2,19,22 Original, locally sourced Sedr honey collected from the Jazan region in the southern area of the Kingdom of Saudi Arabia was used as the coupling medium. The knee was positioned at approximately 25 degrees of flexion during ultrasound application to optimize access to the medial femoral cartilage region Figure 3. Phonophoresis has been reported to enhance transdermal delivery of topical agents by increasing tissue permeability through acoustic cavitation and microstreaming, thereby improving the local penetration of biologically active substances.2,19,22
 |
Figure 3 Application of phonophoresis on the left knee from 25 degrees of knee flexion. |
In addition to honey phonophoresis, transcutaneous electrical nerve stimulation (TENS) was applied during each session to modulate pain. TENS was delivered using four surface electrodes placed around the medial aspect of the knee joint. Stimulation parameters included a frequency of 80 Hz and a treatment duration of 20 minutes, with intensity adjusted to produce a strong but comfortable sensory perception without muscle contraction. High-frequency TENS has been associated with reduced pain and improved function in individuals with knee osteoarthritis and is widely incorporated into rehabilitation programs.5
A supervised quadriceps strengthening program was implemented as a core component of the intervention, given the established association between quadriceps weakness and functional limitations in knee osteoarthritis. Exercises were performed during each treatment session and consisted of three sets of ten repetitions at the patient’s ten-repetition maximum. The exercise program included quadriceps setting over a bolster, seated knee extensions, straight-leg raises, and resisted knee extension using an elastic band within the outer range of motion. Progressive quadriceps strengthening has been associated with reduced pain, improved function, and positively influenced knee joint loading in patients with medial knee osteoarthritis.5,20
Throughout the intervention period, the patient was instructed not to use specialized footwear, orthotic devices, or knee braces, and no additional physical therapy modalities or pharmacological treatments were introduced. This approach was adopted to minimize confounding variables and to isolate better the combined effects of honey phonophoresis, TENS, and exercise therapy. The patient was monitored during each session, and no adverse events or treatment-related complications were reported.
Results
Statistical analysis was not conducted due to the single-case design, and values are presented descriptively without inferential interpretation. Outcome assessment was performed at baseline and immediately following completion of the four-week intervention period. Clinical, functional, structural, and biological outcomes were evaluated using validated patient-reported outcome measures, musculoskeletal ultrasound imaging, and laboratory inflammatory markers.
Pain intensity was assessed using the Numeric Pain Rating Scale (NPRS), a reliable and valid measure for quantifying pain severity in musculoskeletal conditions.16 At baseline, the patient reported a maximum pain intensity of 8 out of 10 during weight-bearing activities involving the affected knee. Following the intervention, pain intensity decreased to 4 out of 10, representing a substantial reduction in perceived pain severity.16
Functional status and disease severity were evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), a validated outcome measure for knee osteoarthritis.6 Post-intervention assessment demonstrated improvement across all WOMAC subscales. The pain subscale score improved from 11 out of 20 to 6 out of 20, the stiffness score decreased from 5 out of 8 to 3 out of 8, and the physical function score improved from 42 out of 68 to 34 out of 68. Consequently, the total WOMAC score decreased from 58 out of 96 at baseline to 43 out of 96 following treatments, reflecting improvement in knee-related symptoms and functional performance.
Structural assessment of the knee joint was performed using musculoskeletal ultrasound (MSK-US) to measure medial femoral cartilage thickness.11,18 Post-intervention ultrasound imaging demonstrated increased cartilage thickness compared with baseline. Longitudinal posterior measurements increased from 0.26 cm at baseline to 0.30 cm following treatment Figure 4, while transverse posterior measurements increased from 0.20 cm to 0.26 cm Figure 5. Musculoskeletal ultrasound is a non-invasive imaging modality for assessing morphological changes in knee cartilage in osteoarthritis.11,18
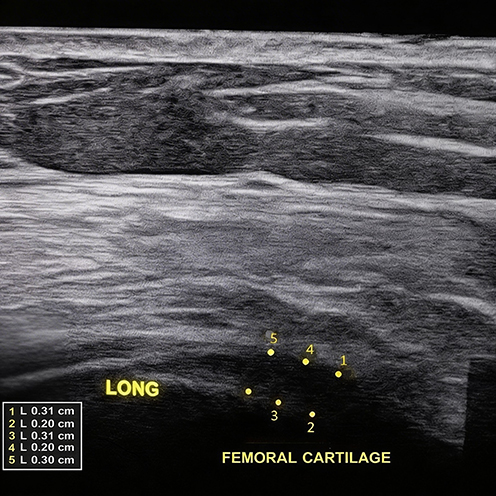 |
Figure 4 Longitudinal posterior musculoskeletal measurements of femoral cartilage (post-treatment), with five sequential measurement points (1–5) marked in yellow. Cartilage thickness values, shown in centimeters, are indicated in the measurement panel (L = length measurement). The imaging changes observed in osteoarthritis should be interpreted cautiously, recognizing it as a whole-joint condition involving cartilage, menisci, synovium, and periarticular structures. |
 |
Figure 5 Transverse posterior musculoskeletal measurements of femoral cartilage (post-treatment), with five sequential cartilage thickness measurements indicated by numbered yellow markers (1–5). The thickness values in centimeters are shown in the embedded measurement panel, with “L” representing length measurement. Structural variations in osteoarthritis should be viewed as part of the multifactorial, whole-joint context rather than as isolated changes in cartilage. |
Systemic inflammatory status was evaluated using serum C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). At baseline, CRP was elevated at 8.08 mg/L, and ESR measured 29 mm/h, reflecting low-grade systemic inflammatory activity.10 Following the intervention, CRP decreased to 5.2 mg/L, and ESR decreased to 18 mm/h. Although these biomarkers are not specific to osteoarthritis, reductions in CRP and ESR may reflect changes in systemic inflammatory status and have been associated with symptom improvement in subsets of patients with knee osteoarthritis.10,12
No adverse events, treatment-related complications, or symptom exacerbations were reported throughout the intervention period. The patient tolerated all treatment components well, and complete adherence to the prescribed intervention protocol was achieved.
Discussion
This case report provides preliminary clinical, structural, and biological evidence supporting the potential role of honey phonophoresis as an adjunct to conventional physiotherapy in the management of knee osteoarthritis. Following a four-week multimodal intervention, the patient demonstrated meaningful improvements in pain, functional performance, femoral cartilage thickness, and systemic inflammatory markers. From a multidisciplinary healthcare perspective, these findings are relevant as they integrate rehabilitation science, imaging-based structural assessment, and inflammatory biology within a single conservative treatment framework.
The observed reduction in pain intensity and improvement in WOMAC scores are consistent with established benefits of physiotherapy-based interventions in knee osteoarthritis. Therapeutic exercise and electro-physical modalities, such as TENS, have been associated with reduced pain, enhanced neuromuscular control, and improved functional capacity in individuals with knee OA.5,20 However, the magnitude of improvement noted in this case may also reflect an additive or synergistic effect of honey phonophoresis, particularly given the concurrent improvements observed in inflammatory biomarkers and cartilage-related outcomes.
Honey contains a diverse range of bioactive compounds, including polyphenols and flavonoids, which have been shown to exert antioxidant and anti-inflammatory effects in experimental and translational studies.1,9 These bioactive molecules may modulate inflammatory mediators, reduce oxidative stress, and have been investigated for chondrocyte effects, all of which are central to osteoarthritis pathophysiology.1,23 The reduction in serum C-reactive protein and erythrocyte sedimentation rate observed in this case supports the hypothesis that honey-based interventions may influence low-grade systemic inflammation associated with knee osteoarthritis.23
Phonophoresis has been reported to provide analgesic and anti-inflammatory benefits in certain musculoskeletal disorders,19 but evidence for its direct impact on cartilage structure is limited,10 and the underlying biological mechanisms for regenerative effects are not well established.18 Phonophoresis may further enhance the therapeutic potential of honey by facilitating transdermal delivery of its bioactive constituents. Ultrasound-induced cavitation and microstreaming increase tissue permeability, allowing deeper penetration of topically applied agents.17 Additionally, experimental evidence suggests that ultrasound exposure may enhance the antioxidant capacity and phenolic content of honey, potentially amplifying its biological activity when used as a coupling medium.18 Although the exact tissue distribution of honey-derived compounds cannot be determined in this case, the combined clinical and biomarker improvements observed lend support to this mechanistic rationale.
The increase in medial femoral cartilage thickness detected by musculoskeletal ultrasound is a notable finding. MSK-US is increasingly recognized as a non-invasive modality for assessing cartilage morphology in knee osteoarthritis, particularly within the medial compartment.18 These short-term increases in cartilage thickness may reflect reduced inflammation, decreased joint effusion, temporary changes in cartilage hydration, mechanical unloading, or variability in ultrasound measurements.10,18 Additionally, improvements in inflammatory biomarkers could have influenced the joint microenvironment, affecting tissue appearance without confirming structural regeneration. Due to operator-dependent factors and the lack of formal reliability assessments in this single case report, minor short-term fluctuations in cartilage thickness on MSK-US should be interpreted cautiously. Therefore, these findings should be viewed as exploratory and hypothesis-generating rather than confirmatory.11,12 Cartilage remodeling remains biologically complex and usually requires long-term interventions; therefore, the structural gains observed should be interpreted cautiously, especially given the short intervention duration. Further controlled studies with long-term imaging are needed to determine the permanence of the observed changes.
Importantly, this case aligns with the evolving conceptualization of osteoarthritis as a potentially modifiable condition rather than an inevitably progressive degenerative disease.10,14 Contemporary translational research is focused on biologically targeted and regenerative approaches to modulate inflammation and improve cartilage homeostasis, though robust clinical validation is still underway.10,12
Emerging evidence suggests that early interventions targeting inflammatory and metabolic pathways may influence disease trajectory.12 From this perspective, honey phonophoresis represents a low-cost, accessible, and theoretically plausible adjunctive strategy that may complement established physiotherapy approaches, but the clinical evidence supporting disease modification remains limited.23
Several limitations must be acknowledged. This report describes a single patient, limiting generalizability and precluding causal inference. The multimodal nature of the intervention prevents isolation of the specific effects attributable to honey phonophoresis. Due to the multimodal nature of the intervention and the lack of a control condition, the specific impact of honey phonophoresis cannot be applied separately from the exercise therapy, TENS, or inherent clinical variability. Although no adverse events occurred during treatment sessions, standardized safety reporting protocols were not used, indicating the need for broader safety evaluations in larger controlled studies. Additionally, imaging and biomarker assessments were limited to pre- and post-intervention measurements, with no long-term follow-up. Future research should include randomized controlled trials with larger sample sizes, standardized phonophoresis protocols, and extended follow-up periods. Incorporation of advanced imaging and biochemical markers may further elucidate underlying mechanisms.
Despite these limitations, the present case offers valuable translational insight for multidisciplinary healthcare practice. By demonstrating concurrent improvements in patient-reported outcomes, imaging-based structural measures, and inflammatory biomarkers, this report supports further investigation of honey phonophoresis as a novel adjunctive intervention in the management of knee osteoarthritis.
Conclusion
Following a four-week intervention of honey phonophoresis combined with conventional physiotherapy in these single cases, there were concurrent reductions in pain intensity and WOMAC scores, accompanied by increases in femoral cartilage thickness on musculoskeletal ultrasound and decreases in inflammatory markers.
Although causal relationships cannot be established from a single case, the multimodal nature of the intervention limits isolation of individual treatment effects. The imaging changes observed should be interpreted cautiously, as they may reflect reduced inflammation, altered cartilage hydration, or temporary adaptive responses rather than permanent structural changes.
No direct clinical practice recommendations can be derived from this single-case report, as it is intended to generate hypotheses rather than establish a therapeutic effect; accordingly, the results of this study should be interpreted within this context. Further research in the form of well-designed randomized controlled trials with standardized imaging protocols, appropriate control groups, larger sample sizes, and long-term follow-up is required to confirm efficacy, determine the durability of effects, and clarify underlying mechanisms.
Acknowledgments
We acknowledge the patient’s valuable participation in this study and express our gratitude to the Department of Physical Therapy at Jazan University Hospital for its support and cooperation.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Alvarez-Suarez J, Giampieri F, Battino M. Honey as a source of dietary antioxidants: structures, bioavailability and evidence of protective effects against human chronic diseases. Curr Med Chem. 2013;20(5):621–10. doi:10.2174/092986713804999358
2. Ahmed MAS, Saweeres ESB, Abdelkader NA, Abdelmajeed SF, Fares AR. Improved pain and function in knee osteoarthritis with dexamethasone phonophoresis: a randomized controlled trial. Indian J Orthop. 2019;53(6):700–707. doi:10.4103/ortho.IJOrtho_639_18
3. Vivekanantham A, Selby D, Lunt M, et al. Day-to-day variability of knee pain and the relationship with physical activity in people with knee osteoarthritis: an observational, feasibility study using consumer smartwatches. BMJ Open. 2023;13(3):e062801. doi:10.1136/bmjopen-2022-062801
4. Atik I, Gul E, Atik S. Evaluation of the relationship between knee osteoarthritis and meniscus pathologies. Malawi Med J. 2024;36(1):48–52. doi:10.4314/mmj.v36i1.8
5. Atamaz FC, Durmaz B, Baydar M, et al. Comparison of the efficacy of transcutaneous electrical nerve stimulation, interferential currents, and shortwave diathermy in knee osteoarthritis: a double-blind, randomized, controlled, multicenter study. Arch Phys Med Rehabil. 2012;93(5):748–756. doi:10.1016/j.apmr.2011.11.037
6. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the Hip or knee. J Rheumatol. 1988;15(12):1833–1840.
7. Ayhan E. Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J Orthop. 2014;5(3):351–361. doi:10.5312/wjo.v5.i3.351
8. Ciulu M, Spano N, Pilo M, Sanna G. Recent advances in the analysis of phenolic compounds in unifloral honeys. Molecules. 2016;21(4):451. doi:10.3390/molecules21040451
9. da Silva PM, Gauche C, Gonzaga LV, Costa ACO, Fett R. Honey: chemical composition, stability and authenticity. Food Chem. 2016;196:309–323. doi:10.1016/j.foodchem.2015.09.051
10. Di Nicola V. Degenerative osteoarthritis a reversible chronic disease. Regen Ther. 2020;15:149–160. doi:10.1016/j.reth.2020.07.007
11. Aydemir Ekim A, Bakılan F, Gönüllü E, Hamarat H. Ultrasonographic evaluation of femoral cartilage thickness in patients with familial Mediterranean fever. Turkish J Phys Med Rehabil. 2021;67(4):416–420. doi:10.5606/tftrd.2021.6094
12. Bahari Golamkaboudi A, Vojoudi E, Babaeian Roshani K, Porouhan P, Houshangi D, Barabadi Z. Current non-surgical curative regenerative therapies for knee osteoarthritis. Stem Cell Rev Rep. 2024;20(8):2104–2123. doi:10.1007/s12015-024-10768-6
13. Davis S, Karali K, Zekonyte J, Roldo M, Blunn G. 3D full‐field strain distribution across the osteochondral unit during osteoarthritis progression. VIEW. 2025;6(6):e20250062. doi:10.1002/VIW.20250062
14. Rasekh M, Arshad MS, Ahmad Z. Advances in drug delivery integrated with regenerative medicine: innovations, challenges, and future frontiers. Pharmaceutics. 2025;17(4):456. doi:10.3390/pharmaceutics17040456
15. Popov VL. Personalized regenerative rehabilitation of osteoarthritis based on mechanical loading and mechanoregulation. Spectr Mech Eng Oper Res. 2025;2(1):147–153. doi:10.31181/smeor21202540
16. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short‐Form McGill Pain Questionnaire (SF‐MPQ), Chronic Pain Grade Scale (CPGS), Short Form‐36 Bodily Pain Scale (SF‐36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(S11):S240–S252.
17. Gośliński M, Nowak D, Kłębukowska L. Antioxidant properties and antimicrobial activity of manuka honey versus Polish honeys. J Food Sci Technol. 2020;57(4):1269–1277. doi:10.1007/s13197-019-04159-w
18. Kauppinen K, Casula V, Zbýň Š, Blanco Sequeiros R, Saarakkala SS, Nevalainen MT. Ultrasonographic assessment of the normal femoral articular cartilage of the knee joint: comparison with 3D MRI. Sci World J. 2021;2021:1–6. doi:10.1155/2021/9978819
19. Luksurapan W, Boonhong J. Effects of phonophoresis of piroxicam and ultrasound on symptomatic knee osteoarthritis. Arch Phys Med Rehabil. 2013;94(2):250–255. doi:10.1016/j.apmr.2012.09.025
20. Lim B, Hinman RS, Wrigley TV, Sharma L, Bennell KL. Does knee malalignment mediate the effects of quadriceps strengthening on knee adduction moment, pain, and function in medial knee osteoarthritis? A randomized controlled trial. Arthritis Care Res. 2008;59(7):943–951. doi:10.1002/art.23823
21. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
22. Mitragotri S, Kost J. Low-frequency sonophoresis. Adv Drug Deliv Rev. 2004;56(5):589–601. doi:10.1016/j.addr.2003.10.024
23. Martinez-Armenta C, Camacho-Rea MC, Martínez-Nava GA, et al. Therapeutic potential of bioactive compounds in honey for treating osteoarthritis. Front Pharmacol. 2021;12:642836. doi:10.3389/fphar.2021.642836
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated C-Reactive Protein and Erythrocyte Sedimentation Rate Correlates with Depression in Psoriasis: A Chinese Cross-Sectional Study
Tan M, Luo Y, Hu J, Hu K, Li X, Yang J, Chen J, Zhu W, Kuang Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:397-405
Published Date: 13 February 2023
The Utility of Synovial Fluid Interleukin-10 in Diagnosing Chronic Periprosthetic Joint Infection: A Prospective Cohort Study
Zou Y, Yang Y, Yang J, Zhang Y, Zhao C, Qin L, Hu N
Infection and Drug Resistance 2025, 18:533-542
Published Date: 28 January 2025
Exploring the Relationship Between Inflammatory Biomarkers and Anthropometric Measures of Obesity in Healthy Adults: A Case Control Study
El-Aghbary DA, Thabet RA, Almorish MA, AlSayaghi KM, Elkhalifa AME
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3403-3414
Published Date: 9 September 2025