Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
High versus Medium Dose of Inhaled Corticosteroid in Chronic Obstructive Lung Disease: A Systematic Review and Meta-Analysis
Authors Archontakis Barakakis P ![]() , Tran T, You JY, Hernandez Romero GJ, Gidwani V, Martinez FJ
, Tran T, You JY, Hernandez Romero GJ, Gidwani V, Martinez FJ ![]() , Fortis S
, Fortis S
Received 16 December 2022
Accepted for publication 27 March 2023
Published 6 April 2023 Volume 2023:18 Pages 469—482
DOI https://doi.org/10.2147/COPD.S401736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Paraschos Archontakis Barakakis,1 Thuonghien Tran,2 Jee Young You,3 Gabriel J Hernandez Romero,4 Vipul Gidwani,1 Fernando J Martinez,5 Spyridon Fortis2,6
1Northeast Internal Medicine Associates, LaGrange, IN, USA; 2Division of Pulmonary, Critical Care, and Occupational Medicine, Department of Internal Medicine, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, IA, USA; 3Department of Pulmonary and Critical Care Medicine, Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA; 4Department of Medicine, Albert Einstein College of Medicine/Jacobi Medical Center, Bronx, NY, USA; 5Departments of Medicine and Genetic Medicine, Weill Cornell Medicine, New York, NY, USA; 6Veterans Rural Health Resource Center, VA Office of Rural Health, and Center for Access and Delivery Research and Evaluation (CADRE) at the Iowa City VA Healthcare System, Iowa City, IA, USA
Correspondence: Paraschos Archontakis Barakakis, Northeast Internal Medicine Associates, 4344 Love Grass Lane, Fort Wayne, LaGrange, IN, 46845, USA, Tel +1 929-422-4589, Email [email protected]
Background: Inhaled corticosteroids (ICSs) combined with bronchodilators have been identified to improve outcomes in COPD but also to be associated with certain adverse effects.
Objective: We performed a systematic review and meta-analysis to compile and summarize data on the efficacy and safety of dosing levels (high versus medium/low) of ICS alongside ancillary bronchodilators following PRISMA guidelines.
Data Sources: Medline and Embase were systematically searched until December 2021. Randomized, clinical trials (RCTs) that met predefined inclusion criteria were included.
Data Extraction: Risk ratios (RRs) with 95% confidence intervals (CI) were extracted. Any acute exacerbation of COPD (AECOPD) risk was chosen as the primary efficacy outcome, mortality rate as the primary safety outcome, moderate/severe AECOPD risk as the secondary efficacy outcome and pneumonia risk as the secondary safety outcome. Subgroup analyses of individual ICS agents, of patients with baseline moderate/severe/very severe COPD and of patients with recent COPD exacerbation history were also performed. A random-effects model was used.
Results: We included 13 RCTs in our study. No data on low doses were included in the analysis. High dose ICS was not associated with a statistically significant difference in any AECOPD risk (RR: 0.98, 95% CI: 0.91– 1.05, I2: 41.3%), mortality rate (RR: 0.99, 95% CI: 0.75– 1.32, I2: 0.0%), moderate/severe AECOPD risk (RR: 1.01, 95% CI: 0.96– 1.06, I2: 0.0%) or pneumonia risk (RR: 1.07, 95% CI: 0.86 − 1.33, I2: 9.3%) compared to medium dose ICS. The same trend was identified with the several subgroup analyses.
Conclusion: Our study collected RCTs investigating the optimal dosing level of ICS prescribed alongside ancillary bronchodilators to patients with COPD. We identified that the high ICS dose neither reduces AECOPD risk and mortality rates nor increases pneumonia risk relative to the medium dose.
Keywords: chronic obstructive lung disease, acute COPD exacerbation, mortality, pneumonia, inhaled corticosteroids
Introduction
Chronic obstructive pulmonary disease (COPD) is a medical condition that has a significant morbidity, mortality and financial toll globally.1,2 Since their first iteration, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines have offered a stepwise approach to pharmacologic management of COPD in its stable state via the use of different inhaled medication classes.3 The use of an inhaled corticosteroid (ICS) is not the initial recommendation but a possible subsequent one thus building double and triple therapies.
The use of ICS is dictated by an individualized risks and benefits calculation. On one hand, they are effective in decreasing acute exacerbations of COPD (AECOPDs).4 AECOPDs are considered the most serious complication5–7 and a prevalent cause of mortality for patients with COPD alongside cardiovascular causes and malignancies.8 On the other hand, ICSs have also been associated in a dose-dependent manner with potentially significant side effects, most importantly pneumonia but also others such as bone fractures and cataract.9,10 An effect on cardiovascular mortality has not yet been definitively established11 and some evidence of all-cause mortality benefit associated with their use has recently become available.12,13
A consensus on the optimal ICS dosing regimen has not been reached. Different study groups investigated a number of different agents and an even larger number of dosing regimens. We performed a systematic review of this literature and meta-analyzed the results of randomized, clinical trials (RTCs) that provided details on efficacy outcomes (risk of any AECOPD and risk of moderate/severe AECOPD) and safety outcomes (mortality rate and risk of pneumonia development) in patients with COPD in order to investigate and quantify the effect profile of different ICS doses.
Methods
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.14 The study was registered with the International Prospective Register of Systematic Reviews (Identifier: CRD42021276365). The PRIMSA Checklist corroborating our methodology is presented in our Supplementary Material.
Study Selection and Eligibility Criteria
The algorithm used for the Medline and Embase databases was:
(Inhaled AND ((glucocorticosteroids OR glucocorticoids OR corticosteroids OR steroids) OR (fluticasone OR budesonide OR mometasone OR beclomethasone OR ciclesonide))) AND (COPD OR (chronic AND obstructive AND pulmonary AND disease) OR. (chronic AND bronchitis))
In addition and in order to identify further eligible studies, manual searches of the references list of the included studies and pertinent reviews were performed.
The processing of studies proceeded with pre-specified inclusion criteria: i) RCT, ii) study population being adults (>18 years old) suffering from COPD, iii) final form of publication available online in English, iv) study comparing a high dose of ICS to a low/medium dose of the same ICS, v) concurrent use of at least one (LABA or LAMA) ancillary medication to the ICS, vi) clear definition of AECOPD and clear definition of stratification of AECOPD, if one is used, vii) studies providing outcome results as participant counts or participant groups Risks or participant groups Risk Ratio (RR) with 95% Confidence Intervals (CI) or data that would allow the calculation of counts or RR with 95% CI.
We excluded articles for the following reasons: i) duplicate reports, ii) studies that included patients without COPD, for example asthma, iii) studies that did not include COPD exacerbation as an outcome, v) studies that only included a single dose of inhaled corticosteroid, vi) studies that compared two or more different ICSs.
The databases and references review started in January 2021 and was completed in December 2021 by two researcher teams led by PAB and TT. A third independent investigator (SF) was involved as needed to reach consensus.
Data Extraction and Outcomes
Two independent reviewers (JYY and GJHR) blinded to each other extracted data from the included studies using for all pertinent variables in a predefined data collection form. Discrepancies were resolved with the involvement of a third reviewer (PAB). Data for the following baseline variables were extracted: first author, year of publication, time period of trial interventions, nature of population enrolled, definition of AECOPD used in the study, type and dosage of ICS, type of accompanying LABA/LAMA, number of participants enrolled, age of participants, gender distribution of participants, distribution of pack-years of smoking, mean forced expiratory volume in the first second (FEV1), number of participants with COPD severity of stage 2–4 according to GOLD, number of participants with recent AECOPD.
We chose our study’s outcomes focusing on clinically meaningful outcomes as well as outcomes with the lowest possible exposure to different types of bias. As such, our primary efficacy endpoint was the RR with 95% CI of any AECOPD between the ICS dose levels during the investigational period and the secondary efficacy endpoint was the RR with 95% CI of moderate/severe AECOPD. Our primary safety endpoint was the RR with 95% CI of mortality between the ICS dose levels during the investigational period and our secondary safety endpoint was the RR with 95% CI of development of pneumonia. The definition of AECOPD and pneumonia was accepted as provided by the authors of the primary study.
The ICS steroid levels were classified as per usual medical practice with the maximal dose representing the “High” dose for our investigational purposes and everything less than that representing the “Low/Medium” dose. We collected counts, risks or RRs with 95% CI both for our main data collection but also for a pre-determined number of subgroups of interest. The first analysis was performed on subgroups based on the individual ICS agent used, the second on the subgroup of patients with moderate/severe/very severe COPD at baseline (as per GOLD classification) and the third on the subgroup of patients with a recent AECOPD (within 1 year from study enrollment).
Risk of Bias Assessment
Two independent reviewers (TT, VG) assessed the risk of bias of the included studies using the Revised Cochrane risk-of-bias tool (RoB 2) for randomized studies.15
Data Synthesis and Statistical Analysis
The utmost care was dedicated to ensure that the dosing regimens, including corticosteroid dosing equivalency, were appropriately classified as a high or a low/medium dose. Furthermore, the definitions of AECOPDs and the definitions of severity stratification of AECOPDs were verified to ensure the appropriate pooling of data.
A random effects model was selected a priori because the included studies had heterogeneous study design and baseline patients’ characteristics.16 Forest plots were used to illustrate the individual study findings and the random effects meta-analysis results. The I-square statistic (I²) was used to assess for heterogeneity among the studies17,18 and a cut-off of 50% was used to indicate statistically significant heterogeneity. The Q statistic and the p value for the Q statistic were also calculated. Dichotomous outcomes were calculated as risk ratios (RRs) with 95% confidence intervals (CIs) for the primary and secondary outcomes. Statistical analysis was conducted with R version 4.2.1 with R studio version 2022.02.3.
Certainty of Evidence
The quality of the evidence was assessed via the use of the GRADE approach and primarily based on the Risk of bias of included RCTs and calculation of heterogeneity.19
Results
Studies Selection and Characteristics
In total, 5448 records were screened and 296 full text articles were assessed for eligibility. Of these, 13 studies met all the inclusion criteria and were advanced to qualitative and quantitative analysis.13,20–31 A PRISMA flow diagram with the selection process was created to depict this work (Figure 1).
 |
Figure 1 PRISMA Flowchart. |
Extensive information on the methodology of each study, including the type of ICS and type of ancillary bronchodilator used, the locations where the study was performed, the primary outcomes investigated and the AECOPD definition, as well as on the baseline characteristics of their included population samples were collected. This data is presented in Table 1 and ETable 1.
 |
Table 1 Baseline Characteristics of Study Populations in the Included RCTs |
Of note, all our comparisons were performed between high and medium dose of ICS combinations.
Primary Efficacy Outcome
There were 12,219 patients included in the analysis of our primary efficacy outcome. The any AECOPD risk varied substantially between the studies with the risk for the high dose ranging from 6.8% to 48% and for the medium dose from 6.4% to 47.8%. Cumulatively, no statistically significant difference was identified between the high and medium dose ICS groups (RR: 0.98, 95% CI: 0.91–1.05, I2: 41.3%) (Figure 2).
 |
Figure 2 Comparison of Any AECOPD Risk between patients with COPD using High Dose ICS versus Medium ICS as part of maintenance therapy. |
The certainty of evidence for this comparison was calculated to be “Moderate” because of low risk of bias of included RCTs, low-to-intermediate heterogeneity among the included studies and thus low-to-intermediate inconsistency and absence of imprecision.
Primary Safety Outcome
There were 13,557 patients included in the analysis of our primary safety outcome. The mortality rate was low in all studies and a relatively high variability was appreciated with mortality for the high dose ranging from 0.5% to 3.8% and for the medium dose from 0.3% to 3.2%. Cumulatively, no statistically significant mortality difference was identified between the high and medium dose ICS groups (RR: 0.99, 95% CI: 0.75–1.32, I2: 0.0%) (Figure 3).
 |
Figure 3 Comparison of Mortality Risk Rate between patients with COPD using High Dose ICS versus Medium ICS as part of maintenance therapy. |
The certainty of evidence for this comparison was calculated to be “Low” because of low risk of bias of included RCTs, low heterogeneity among the included studies, absence of inconsistency but moderate possibility of imprecision as per few deaths in each study.
Secondary Efficacy Outcome
There were 11,190 patients included in the analysis of our secondary efficacy outcome. The moderate or severe AECOPD risk varied substantially between the studies with the risk for the high dose ranging from 6.8% to 48% and for the medium dose from 6.4% to 47.8%. Cumulatively, no statistically significant difference was identified between the high and medium dose ICS groups (RR: 1.01, 95% CI: 0.96–1.06, I2: 0.0%) (Figure 4).
 |
Figure 4 Comparison of Moderate/Severe AECOPD Risk between patients with COPD using High Dose ICS versus Medium ICS as part of maintenance therapy. |
The certainty of evidence for this comparison was calculated to be “High” because of low risk of bias of included RCTs, low heterogeneity among the included studies, absence of inconsistency or imprecision.
Secondary Safety Outcome
There were 13,567 patients included in the analysis of our secondary safety outcome. The pneumonia risk also varied substantially between the studies with the risk for the high dose ICS ranging from 0.7% to 8.0% and for the medium dose from 0.4% to 7.2%. Cumulatively, no statistically significant difference was identified between the high and medium dose ICS groups (RR: 1.07, 95% CI: 0.86 −1.33, I2: 9.3%) (Figure 5).
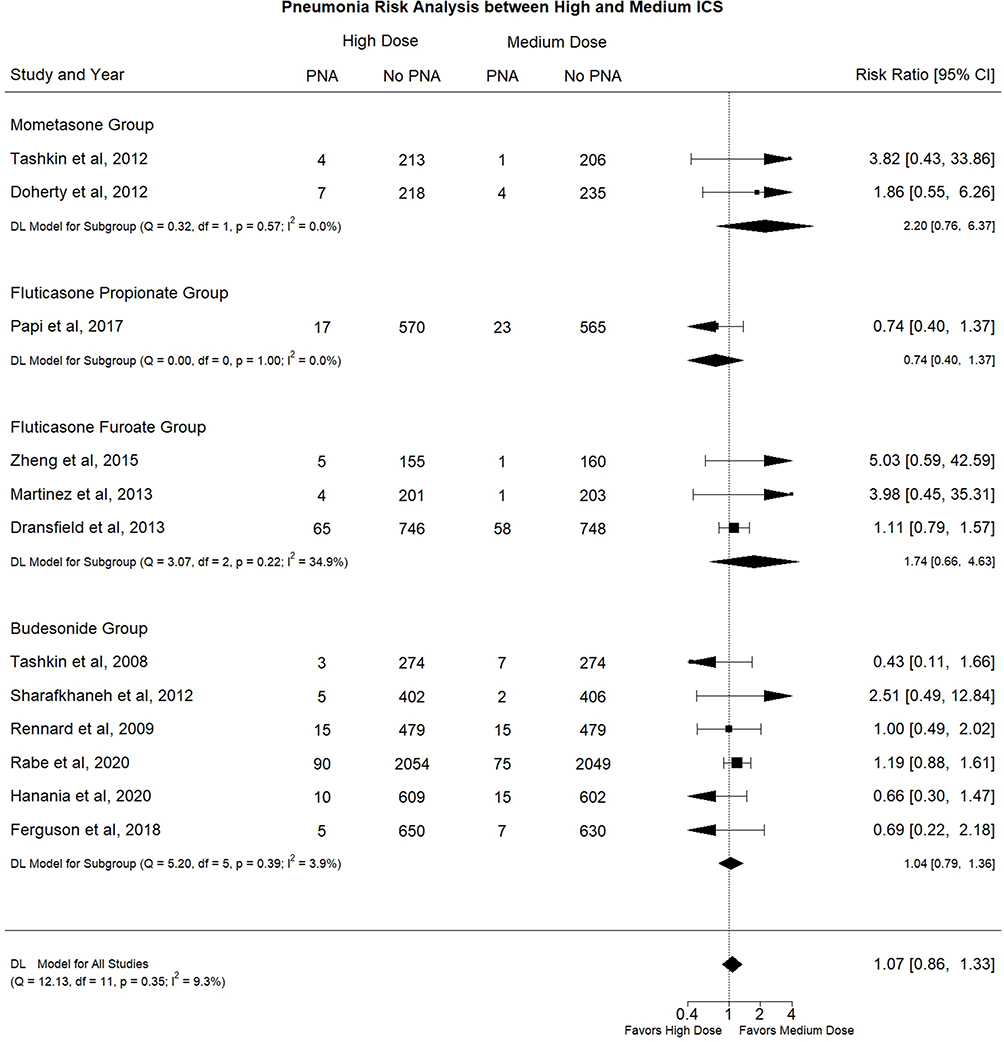 |
Figure 5 Comparison of Pneumonia risk between patients with COPD using High Dose ICS versus Medium ICS as part of maintenance therapy. |
The certainty of evidence for this comparison was calculated to be “Moderate” because of low risk of bias of included RCTs, low heterogeneity among the included studies and thus low-to-intermediate inconsistency and absence of imprecision.
Type of Inhaled Corticosteroid Subgroup
When focusing on separate inhaled corticosteroids agents, the high dose of mometasone was not associated with a statistically significant difference in any AECOPD risk (2 studies, RR: 0.95, 95% CI: 0.61–1.46, I2: 80.4%), mortality rate (2 studies, RR: 3.07, 95% CI: 0.84–11.28, I2: 0.0%), moderate/severe AECOPD risk (2 studies, RR: 0.90, 95% CI: 0.47–1.70, I2: 64.5%), pneumonia risk (2 studies, RR: 2.20, 95% CI: 0.76–6.37, I2: 0.0%) compared to the medium dose of mometasone. (Figures 2–5) The certainty of evidence was calculated as “Low” for the ones with low heterogeneity and “Very Low” for the ones with high heterogeneity.
The high dose of fluticasone propionate was not associated with a statistically significant difference in any AECOPD risk (2 studies, RR: 0.74, 95% CI: 0.33–1.66, I2: 89.7%), mortality rate (1 study), moderate/severe AECOPD risk (1 study) or pneumonia risk (1 study) compared to the medium dose of fluticasone propionate (Figures 2–5). The certainty of evidence for the one comparison was calculated as “Very Low” as per high heterogeneity.
The high dose of fluticasone furoate was not associated with a statistically significant difference in any AECOPD risk (3 studies, RR: 0.99, 95% CI: 0.89–1.11, I2: 0.0%), mortality rate (3 studies, RR: 1.23, 95% CI: 0.59–2.58, I2: 0.0%), moderate/severe AECOPD risk (3 studies, RR: 1.10, 95% CI: 0.95–1.29, I2: 0.0%) or pneumonia risk (3 studies, RR: 1.74, 95% CI: 0.66–4.63, I2: 34.9%) compared to the medium dose of fluticasone furoate (Figures 2–5). The certainty of evidence was calculated as “High” for any and moderate/severe AECOPD comparisons and “Low” for the Mortality and pneumonia comparisons as per low documented counts.
Finally, the high dose of budesonide was not associated with a statistically significant difference in any AECOPD risk (4 studies, RR: 0.99, 95% CI: 0.94–1.04, I2: 0.0%), mortality rate (6 studies, RR: 0.82, 95% CI: 0.56–1.19, I2: 0.0%), moderate/severe AECOPD risk (4 studies, RR: 0.99, 95% CI: 0.94–1.04, I2: 0.0%) or pneumonia risk (6 studies, RR: 1.04, 95% CI: 0.79–1.36, I2: 3.9%) compared to the medium dose of budesonide (Figures 2–5). The certainty of evidence was calculated as “High” for any and moderate/severe AECOPD comparisons, “Moderate” for pneumonia and “Low” for the mortality comparison as per low documented counts.
Patients with Moderate, Severe or Very Severe COPD Subgroup
In the subgroup of patients suffering from moderate, severe or very severe COPD, no statistically significant difference was identified between the high and medium ICS dose in any AECOPD risk (RR: 1.01, 95% CI: 0.94–1.07, I2: 22.5%), mortality rate (RR: 0.93, 95% CI: 0.68–1.28, I2: 0.0%), moderate/severe AECOPD risk (RR: 1.01, 95% CI: 0.96–1.06, I2: 0.0%) or pneumonia risk (RR: 1.02, 95% CI: 0.77–1.36, I2: 13.83%). (EFigure 1A–D) The certainty of evidence was calculated as “High” for any, moderate/severe AECOPD and pneumonia comparisons and “Low” for the mortality comparison as per low documented counts.
Patients with Recent Exacerbation Subgroup
In the subgroup of patients with recent AECOPD, no statistically significant difference was identified between the high and medium ICS dose in any AECOPD risk (RR: 1.00, 95% CI: 0.95–1.00, I2: 0.0%), mortality rate (RR: 0.88, 95% CI: 0.61–1.26, I2: 0.0%) or moderate/severe AECOPD risk (RR: 1.01, 95% CI: 0.96–1.06, I2: 0.0%) or pneumonia risk (RR: 1.11, 95% CI: 0.91–1.37, I2: 0.0%). (EFigure 2A–D) The certainty of evidence was calculated as “High” for any, moderate/severe AECOPD and pneumonia comparisons and “Low” for the mortality comparison as per low documented counts.
Publication Bias
Funnel plots were constructed for all outcomes and no major evidence of publication bias was appreciated. These Funnel plots are presented in EFigure 3A–L.
Other Risks of Bias Assessment
Our risk of bias assessment was based on the appropriate tool, RoB2 for RCTs, and did not reveal any major source of bias for any of the included studies (EFigure 4).
Discussion
This study was a systematic review and meta-analysis of 13 RCTs comparing the efficacy and safety profile of two different dosage levels (high versus medium) of ICS in combination with at least one bronchodilator (LABA, LAMA or both) in COPD.
Assessing the methodology of the included studies, a significant alignment is appreciated. Initially, there is agreement on the specific ICS dosing between studies using the same ICS and on the dosing equivalency between studies using different agents. Second, there are significant similarities in the methodology of patient population selection and of outcome assessment, including their definitions of AECOPD and AECOPD severity levels. Third, the investigational period is deemed relatively similar between studies and generally spanning from 6 to 12 months. All in all, our decision to pool the results of the studies is deemed methodologically appropriate.
Our results indicate that i) the use of high dose ICS was not associated with a statistically significant difference in any AECOPD risk, ii) the use of high dose ICS was not associated with a statistically significant difference in mortality rate, iii) the use of high dose ICS was not associated with a statistically significant difference in moderate or severe AECOPD risk, iv) the use of high dose ICS was not associated with a statistically significant difference in pneumonia risk, v) no difference on any AECOPD risk, mortality rate, moderate/severe AECOPD risk or pneumonia risk was identified with individual ICS agent subgroup analysis, vi) no difference on any AECOPD risk, mortality rate, moderate/severe AECOPD risk or pneumonia risk was identified with patients suffering from moderate, severe or very severe COPD subgroup analysis, vii) no difference on any AECOPD risk, mortality rate, moderate/severe AECOPD risk or pneumonia risk was identified with patients with recent AECOPD history subgroup analysis.
Our results provide a possibly significant contribution to the decision-making process of clinicians providing care to patients with COPD. According to the most recent GOLD guidelines,3 one of the main treatment goals for these patients is to tailor their inhaler maintenance regimen to prevent AECOPD, as per their multilevel detrimental effects.32,33 Combined ICS and bronchodilator therapy has been associated with improvement in lung function and health status as well as reduction in exacerbations.3 Additionally, ICS combinations have been associated with all-cause mortality benefit. Two recent large RCTs (IMPACT and ETHOS) showed reduction in all-cause mortality when ICS is added to dual bronchodilator therapy relative to dual bronchodilation therapy alone.34,35 The same conclusion was reached by a recently published meta-analysis that investigated all-cause mortality as the primary outcome.12 Finally, it is important to mention the effect of ICS combinations on cardiovascular events. Again, the IMPACT trial identified a reduced risk of cardiovascular mortality and the ETHOS trial identified a reduced risk for major adverse cardiovascular events. However, it is important to underline that the effect was not corroborated by the equally large and oriented to cardiovascular events SUMMIT trial.11 According to the above and pending further elaboration, COPD guidelines suggest adding ICS in patients with a history of COPD-related hospitalization, ≥2 moderate exacerbations the last year, blood eosinophil counts >300 cells/μL, and/or a history of asthma.3
Despite the aforementioned and significant benefits, ICS use has been linked with several safety concerns and thus ICS use is not recommended in patients with low eosinophil counts (<100 cells/μL), history of mycobacterial infection, and those with several pneumonias.3 Elaborating on these concerns, the risk of pneumonia development with the use of this medication class has been investigated by RCTs, with the majority identifying an increased risk22,26,28,36–38 and a minority a similar risk,4,21,27,29 by observational studies39 and by meta-analyses of RCTs, with the majority again identifying an increased risk40–42 and a minority a similar risk.43 Second, the risk of onset or deteriorated control of Diabetes Mellitus has been associated with ICS use. Evidence of such effect has been demonstrated by both randomized and observational studies28,44 but a significant number of studies have been unable to prove a difference.13,20,30,45–47 Finally, ICS have been associated with deleterious effects on bone health (either decreased bone density or fractures) with mixed results from different studies once again with some studies identifying deleterious effects22,27 while others not identifying a connection.13,21,48,49 As per the above, a significant level of ambiguity is appreciated with the adverse effects linked to ICS use. In this setting and considering the dose-dependent nature of some of these side effects,9,10 the use of the lowest possible dose of ICS becomes very clinically relevant. As a consequence, our study provides pertinent information on the appropriate dosing of ICS by assessing the benefits and detriments of the different dosing levels.
Strengths and Weaknesses
Our study demonstrates a number of strengths. Specifically, we strictly adhered to the systematic review methodology from start to finish, we narrowly focused on one primary efficacy, one primary safety, one secondary efficacy and one secondary safety outcome avoiding a more nebulous spectrum of outcomes. Second, these outcomes were identified as clinically relevant for all practitioners providing care to patients with COPD and as unambiguous in nature thus avoiding introduction of bias to our study. Third and because of this methodology, we were able to search, collect, screen and analyze a significant number of studies and thus a substantial patient population size.
Our study demonstrates certain weaknesses as well. First, our goal to pool low and medium dose was not achieved as all included studies used the medium dose of respective ICS and none used the low dose. Second, we considered 640mcg/day and 320mcg/day of budesonide as high and low/moderate dose respectively based on US regulatory labelling although these doses have been categorized as medium and low by other organizations.50 Alongside the budesonide dosing intensity topic, the approved ICS doses in the United States reach medium intensity only, most high doses of ICS are not used even in a RCT setting and thus the possibility of region-specific results is introduced in our study. Third, the methods used to identify, quantify, and present AECOPD in our source material were not uniform. Although data on the outcome were available in all of them, it was impossible in some cases to use it because we were unable to mathematically convert it to our statistic of choice, such as when extracting COPD exacerbations per person-year. On the other hand, some studies did not provide data on all severity levels of exacerbation and instead focused on the most clinically relevant moderate or severe ones. In this scenario, we included these counts in our primary outcome. Finally, we did not investigate the contribution of eosinophil count measurement to the effect of the dosing levels on the outcomes of choice, a research point of interest recently.
Conclusion
The high ICS dose combined with bronchodilator therapy neither reduces AECOPD and mortality rates nor increases pneumonia risk relative to the medium dose. Further research might be needed to investigate whether low ICS doses can provide similar benefits with fewer adverse events than medium or high ICS doses to patients with COPD.
IRB Review
This study is a review and meta‐analysis, which does not require IRB review.
Data Sharing Statement
Our data is derived from public domain resources. All data source material that supports the findings of this study are available on Medline and Embase.
Author Contributions
PAB was involved in the study execution, data analysis and data interpretation and was involved in the manuscript drafting and writing.
TT was involved in the study design, study execution and acquisition of data and was involved in substantially revising the article.
JYY, GJHR and VG were involved in the study execution, acquisition of data and were involved in substantially revising the article.
FJM was involved in the study conception, data (result) interpretation and was involved in substantially revising and critically reviewing the article.
SF was involved in the study conception, study design, study execution and was involved in article writing, substantially revising and critically reviewing the article.
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
FJM reports grants from NHLBI, National Institutes of Health, personal fees from Continuing Education, personal fees from Forest Laboratories, Janssen, GlaxoSmithKline, Nycomed/Takeda, AstraZeneca, Boehringer Ingelheim, Bellerophon (formerly Ikaria), Genentech, Novartis, Pearl, Roche, Sunovion, Theravance, CME Incite, Annenberg Center for Health Sciences at Eisenhower, Integritas, InThought, National Association for Continuing Education, Paradigm Medical Communications, LLC, PeerVoice, UpToDate, Haymarket Communications, Western Society of Allergy and Immunology, Proterixbio (formerly Bioscale), Unity Biotechnology, ConCert Pharmaceuticals, Lucid, Methodist Hospital, Columbia University, Prime Healthcare Ltd, WebMD, PeerView Network, California Society of Allergy and Immunology, Chiesi, Puerto Rico Thoracic Society, outside the submitted work. He is also a part of the event adjudication committee for Medtronic. SF has received grants from American Thoracic Society and Fisher & Paykel; personal fees from Hospital Medicine (SHM) and has consulted Genentech. The authors report no other conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR.; Collaborators GBDCRD. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. doi:10.2147/CEOR.S34321
3. Global strategy for prevention, diagnosis and management of COPD: 2022 Report. GOLD Reports Web site. Available from: https://goldcopd.org/2022-gold-reports-2/.
4. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
5. Lindenauer PK, Dharmarajan K, Qin L, Lin Z, Gershon AS, Krumholz HM. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/rccm.201709-1852OC
6. Wang Y, Stavem K, Dahl FA, Humerfelt S, Haugen T. Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2014;9:99–105. doi:10.2147/COPD.S51467
7. Darnell K, Dwivedi AK, Weng Z, Panos RJ. Disproportionate utilization of healthcare resources among veterans with COPD: a retrospective analysis of factors associated with COPD healthcare cost. Cost Eff Resour Alloc. 2013;11:13. doi:10.1186/1478-7547-11-13
8. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
9. Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;2014(3):CD010115. doi:10.1002/14651858.CD010115.pub2
10. Suissa S, Patenaude V, Lapi F, Ernst P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68(11):1029–1036. doi:10.1136/thoraxjnl-2012-202872
11. Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomised controlled trial. Lancet. 2016;387(10030):1817–1826. doi:10.1016/S0140-6736(16)30069-1
12. Chen H, Deng ZX, Sun J, et al. Association of inhaled corticosteroids with all-cause mortality risk in patients with COPD: a meta-analysis of 60 randomized controlled trials. Chest. 2023;163(1):100–114. doi:10.1016/j.chest.2022.07.015
13. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
14. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi:10.1371/journal.pmed.1000100
15. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:15.
16. Riley RD, Higgins JP, Deeks JJJB. Interpretation of random effects meta-analyses. BMJ. 2011;342:d549. doi:10.1136/bmj.d549
17. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
18. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
19. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
20. Cheng SL, Su KC, Wang HC, Perng DW, Yang PC. Chronic obstructive pulmonary disease treated with inhaled medium- or high-dose corticosteroids: a prospective and randomized study focusing on clinical efficacy and the risk of pneumonia. Drug Des Devel Ther. 2014;8:601–607. doi:10.2147/DDDT.S63100
21. Doherty DE, Tashkin DP, Kerwin E, et al. Effects of mometasone furoate/formoterol fumarate fixed-dose combination formulation on chronic obstructive pulmonary disease (COPD): results from a 52-week Phase III trial in subjects with moderate-to-very severe COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:57–71. doi:10.2147/COPD.S27320
22. Dransfield MT, Bourbeau J, Jones PW, et al. Once-daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: two replicate double-blind, parallel-group, randomised controlled trials. Lancet Respir Med. 2013;1(3):210–223. doi:10.1016/S2213-2600(13)70040-7
23. Ferguson GT, Papi A, Anzueto A, et al. Budesonide/formoterol MDI with co-suspension delivery technology in COPD: the TELOS study. Eur Respir J. 2018;52(3):1801334. doi:10.1183/13993003.01334-2018
24. Hanania NA, Papi A, Anzueto A, et al. Efficacy and safety of two doses of budesonide/formoterol fumarate metered dose inhaler in COPD. ERJ Open Res. 2020;6:2. doi:10.1183/23120541.00187-2019
25. Martinez FJ, Boscia J, Feldman G, et al. Fluticasone furoate/vilanterol (100/25; 200/25 mug) improves lung function in COPD: a randomised trial. Respir Med. 2013;107(4):550–559. doi:10.1016/j.rmed.2012.12.016
26. Papi A, Dokic D, Tzimas W, et al. Fluticasone propionate/formoterol for COPD management: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2017;12:1961–1971. doi:10.2147/COPD.S136527
27. Rennard SI, Tashkin DP, McElhattan J, et al. Efficacy and tolerability of budesonide/formoterol in one hydrofluoroalkane pressurized metered-dose inhaler in patients with chronic obstructive pulmonary disease: results from a 1-year randomized controlled clinical trial. Drugs. 2009;69(5):549–565. doi:10.2165/00003495-200969050-00004
28. Sharafkhaneh A, Southard JG, Goldman M, Uryniak T, Martin UJ. Effect of budesonide/formoterol pMDI on COPD exacerbations: a double-blind, randomized study. Respir Med. 2012;106(2):257–268. doi:10.1016/j.rmed.2011.07.020
29. Tashkin DP, Doherty DE, Kerwin E, et al. Efficacy and safety of a fixed-dose combination of mometasone furoate and formoterol fumarate in subjects with moderate to very severe COPD: results from a 52-week Phase III trial. Int J Chron Obstruct Pulmon Dis. 2012;7:43–55. doi:10.2147/COPD.S27319
30. Tashkin DP, Rennard SI, Martin P, et al. Efficacy and safety of budesonide and formoterol in one pressurized metered-dose inhaler in patients with moderate to very severe chronic obstructive pulmonary disease: results of a 6-month randomized clinical trial. Drugs. 2008;68(14):1975–2000. doi:10.2165/00003495-200868140-00004
31. Zheng J, de Guia T, Wang-Jairaj J, et al. Efficacy and safety of fluticasone furoate/vilanterol (50/25 mcg; 100/25 mcg; 200/25 mcg) in Asian patients with chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Curr Med Res Opin. 2015;31(6):1191–1200. doi:10.1185/03007995.2015.1036016
32. Williams NP, Coombs NA, Johnson MJ, et al. Seasonality, risk factors and burden of community-acquired pneumonia in COPD patients: a population database study using linked health care records. Int J Chron Obstruct Pulmon Dis. 2017;12:313–322. doi:10.2147/COPD.S121389
33. Fortis S, Wan ES, Kunisaki K, et al. Increased mortality associated with frequent exacerbations in COPD patients with mild-to-moderate lung function impairment, and smokers with normal spirometry. Respir Med X. 2021;3:100025.
34. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/rccm.201911-2207OC
35. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. a randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
36. Ferguson GT, Anzueto A, Fei R, Emmett A, Knobil K, Kalberg C. Effect of fluticasone propionate/salmeterol (250/50 microg) or salmeterol (50 microg) on COPD exacerbations. Respir Med. 2008;102(8):1099–1108. doi:10.1016/j.rmed.2008.04.019
37. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
38. Wedzicha JA, Calverley PM, Seemungal TA, et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med. 2008;177(1):19–26. doi:10.1164/rccm.200707-973OC
39. Ernst P, Gonzalez AV, Brassard P, Suissa S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am J Respir Crit Care Med. 2007;176(2):162–166. doi:10.1164/rccm.200611-1630OC
40. Drummond MB, Dasenbrook EC, Pitz MW, Murphy DJ, Fan E. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(20):2407–2416. doi:10.1001/jama.2008.717
41. Nannini LJ, Lasserson TJ, Poole P, Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829. doi:10.1002/14651858.CD006829.pub2
42. Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219–229. doi:10.1001/archinternmed.2008.550
43. Rojas-Reyes MX, Garcia Morales OM, Dennis RJ, Karner C. Combination inhaled steroid and long-acting beta(2)-agonist in addition to tiotropium versus tiotropium or combination alone for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;2016(6):CD008532. doi:10.1002/14651858.CD008532.pub3
44. Suissa S, Kezouh A, Ernst P. Inhaled corticosteroids and the risks of diabetes onset and progression. Am J Med. 2010;123(11):1001–1006. doi:10.1016/j.amjmed.2010.06.019
45. Blackburn D, Hux J, Mamdani M. Quantification of the risk of corticosteroid-induced diabetes mellitus among the elderly. J Gen Intern Med. 2002;17(9):717–720. doi:10.1046/j.1525-1497.2002.10649.x
46. Dendukuri N, Blais L, LeLorier J. Inhaled corticosteroids and the risk of diabetes among the elderly. Br J Clin Pharmacol. 2002;54(1):59–64. doi:10.1046/j.1365-2125.2002.01610.x
47. O’Byrne PM, Rennard S, Gerstein H, et al. Risk of new onset diabetes mellitus in patients with asthma or COPD taking inhaled corticosteroids. Respir Med. 2012;106(11):1487–1493. doi:10.1016/j.rmed.2012.07.011
48. Ferguson GT, Calverley PMA, Anderson JA, et al. Prevalence and progression of osteoporosis in patients with COPD: results from the towards a revolution in COPD health study. Chest. 2009;136(6):1456–1465. doi:10.1378/chest.08-3016
49. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, Phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
50. Global strategy for asthma management and prevention. Global Initiative for Asthma Web site; 2022. Available from: http://www.ginasthma.org/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.