Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Healthcare Utilization in Patients with Chronic Obstructive Pulmonary Disease Discharged from Coronavirus 2019 Hospitalization
Authors Puebla Neira D ![]() , Zaidan M, Nishi S, Duarte A, Lau C, Parthasarathy S, Wang J, Kuo YF, Sharma G
, Zaidan M, Nishi S, Duarte A, Lau C, Parthasarathy S, Wang J, Kuo YF, Sharma G
Received 9 May 2023
Accepted for publication 6 August 2023
Published 22 August 2023 Volume 2023:18 Pages 1827—1835
DOI https://doi.org/10.2147/COPD.S415621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Video abstract presented by Daniel Puebla Neira.
Views: 105
Daniel Puebla Neira,1 Mohammed Zaidan,2 Shawn Nishi,2 Alexander Duarte,2 Christopher Lau,1 Sairam Parthasarathy,3 Jiefei Wang,4 Yong-Fang Kuo,4 Gulshan Sharma2
1Division of Pulmonary, Critical Care and Sleep Medicine, University of Arizona College of Medicine-Phoenix, Phoenix, AZ, USA; 2Division of Pulmonary Critical Care and Sleep Medicine, University of Texas Medical Branch, Galveston, TX, USA; 3Division of Pulmonary, Critical Care and Sleep Medicine, University of Arizona College of Medicine-Tucson, Tucson, AZ, USA; 4Department of Biostatistics & Data Science, University of Texas Medical Branch, Galveston, TX, USA
Correspondence: Daniel Puebla Neira, Division of Pulmonary, Critical Care and Sleep Medicine, University of Arizona College of Medicine-Phoenix, 1111 E McDowell Road, Phoenix, AZ, 85006, USA, Email [email protected]
Rationale: There is concern that patients with chronic obstructive pulmonary disease (COPD) are at greater risk of increased healthcare utilization (HCU) following Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-COV-2) infection.
Objective: To assess whether COPD is an independent risk factor for increased post-discharge HCU.
Methods: We conducted a retrospective cohort study of patients with COPD discharged home from a hospitalization due to Coronavirus Disease 2019 (COVID-19) between April 1, 2020, and March 31, 2021, using Optum’s de-identified Clinformatics® Data Mart Database (CDM). COVID-19 was identified by an International Classification of Diseases, tenth revision, clinical modification (ICD-10-CM) diagnosis code of U07.1. The primary outcome was HCU (ie, emergency department (ED) visits, readmissions, rehabilitation/skilled nursing facility (SNF) visits, outpatient office visits, and telemedicine visits) nine months post-discharge after COVID-19 hospitalization (from here on “post-discharge”) in patients with COPD compared to HCU of patients without COPD. Poisson regression modeling was used to calculate relative risk (RR) and confidence interval (CI) for COPD, adjusted for the other covariates.
Results: We identified a cohort of 160,913 patients hospitalized with COVID-19, with 57,756 discharged home and 14,622 (25.3%) diagnosed with COPD. Patients with COPD had a mean age of 75.48 years (± 9.49); 55.5% were female and 70.9% were White. Patients with COPD had an increased risk of HCU in the nine months post-discharge after adjusting for the other covariates. Risk of ED visits, readmissions, length of stay during readmission, rehabilitation/SNF visits, outpatient office visits, and telemedicine visits were increased by 57% (RR 1.57; 95% CI 1.53– 1.60), 50% (RR 1.50; 95% CI 1.46– 1.54), 55% (RR 1.55; 95% CI 1.53– 1.56), 18% (RR 1.18; 95% CI 1.14– 1.22), 16% (RR 1.16; 95% CI 1.16– 1.17), and 28% (RR 1.28; 95% CI 1.24– 1.31), respectively. Younger patients (ages 18 to 65 years), women, and Hispanic patients with COPD showed an increased risk for post-discharge HCU.
Conclusion: Patients with COPD hospitalized with COVID-19 experienced increased HCU post-discharge compared to patients without COPD.
Keywords: COPD, Healthcare Utilization disease, COVID-19
Introduction
The medical literature has contradicting reports on the outcomes of patients with chronic obstructive pulmonary disease (COPD) infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). At the beginning of the COVID-19 pandemic, patients with COPD were observed to have low rates of hospitalization due to COVID-19. As the pandemic evolved, some studies indicated an association of worse outcomes (eg, higher rates of admission to ICU, use of non-invasive and invasive positive pressure ventilation, and worse mortality) in patients with COPD hospitalized with COVID-19,1–4 but other studies did not show this association.5–8 Many of these studies evaluated hospitalization and ICU use rates and/or mortality as surrogates for healthcare utilization (HCU).1,9 The post-discharge HCU of patients with COPD hospitalized due to COVID-19, however, has not been well studied.
Prior to the COVID-19 pandemic, patients with COPD were reported to have higher rates of HCU compared to patients without COPD.10–13 Patients with COPD are more likely to receive care in the emergency department (ED) or be hospitalized at least once per year, and they tend to have longer average length of stay and higher cost of inpatient care.14 Patients with COPD also have a higher risk of post-discharge readmissions, and those readmitted are at increased risk of death.15,16 COPD is a leading reason for office-based visits.10,14,17 Moreover, HCU of patients with COPD is greater in current smokers with advanced age, greater number of comorbidities, and worse airflow obstruction.10–14,18–21
The aim of this study was to evaluate whether COPD is an independent risk factor for increased post-discharge HCU after COVID-19 hospitalization. A better understanding of the risk of post-discharge HCU in patients with COPD and COVID-19 could help prioritize and implement healthcare policies for this population, such as aggressive preventive measures (eg, non-pharmacologic interventions to mitigate the risk of infection) and proactive COVID-19 vaccination. Some of the content of this work has been previously presented in the form of a conference abstract.22
Methods
Data Source
In this retrospective cohort study, we used Optum’s Clinformatics® Data Mart Database (CDM), a statistically de-identified and HIPAA-compliant database of administrative health claims for over 67 million people from all 50 states in the United States. CDM contains claims data from individuals with commercial and Medicare Advantage insurance plans. The University of Texas Medical Branch Institutional Review Board approved this study (IRB# is 20–0180). Written informed consent was not required due to the de-identified nature of the patient data.
Cohort
The study cohort consisted of patients hospitalized with a primary diagnosis of COVID-19 between April 1, 2020, and March 31, 2021, as identified by an ICD-10-CM diagnosis code of U07.1. We excluded patients <18 years old; patients not discharged to home; patients with incomplete information on gender, region, or race/ethnicity; and patients with continuous enrollment <12 months before hospitalization or whose enrollment ended before the discharge date (Figure 1).
 |
Figure 1 Flow diagram of our cohort selection process. Our cohort was obtained from Optum’s de-identified Clinformatics® Data Mart Database (CDM). It consists of 57,756 patients who were discharged home from a hospitalization due to COVID-19 from April 2020 until March 2021. From this, 14,622(25.3%) were identified as having COPD. COPD was defined as having at least one inpatient or two outpatient diagnoses in the one year prior to COVID-19 diagnosis (see Table S1). |
Variables
The index date was defined as the date of discharge from hospitalization due to COVID-19. The primary outcome was HCU nine months after the index date in patients with COPD. Subsequently, HCU was compared to patients without COPD during the same period. HCU included ED visits, readmissions, and length of stay during readmissions, rehabilitation/skilled nursing facility (SNF) visits, outpatient office visits, and telemedicine visits. The main independent variable of interest was COPD, which was defined as having experienced one inpatient or two outpatient visits for COPD in the year prior to the index date (Table S1). Other independent variables included age, gender, race/ethnicity, region, COVID-19 hospitalization length of stay, and number of comorbidities. HCU was measured in person-days, which was calculated as the number of days between the index date and the end of the study, death, or the end of enrollment, whichever came first.
Statistical Analysis
Patient and clinical characteristics were summarized by COPD status as frequencies, percentages, or mean ±standard deviation (SD). Comparison between COPD and non-COPD groups was performed using chi-square statistics or t-tests as appropriate. The HCU of patients with COPD after COVID-19 hospitalization was measured in 10,000 (10k) person-days and compared with patients without COPD. A Poisson regression was used to determine if COPD was an independent risk factor for HCU after adjustment for other variables. The outcomes were the number of post-discharge ED visits, readmissions, and length of stay during readmission, rehabilitation/SNF visits, outpatient office visits, and telemedicine visits in the nine months after the index date. Person-days were included in the Poisson model as an offset to account for the different subject follow-up times. The interactions between COPD and age, gender, and race/ethnicity were examined in the Poisson model. The Poisson model was stratified by age, gender, or race/ethnicity to show the impact of COPD on HCU in each subgroup if the interaction term was found to be significant at the 5% nominal level. As a sensitivity analysis, to evaluate the influence of individual comorbidities in the relative risk of HCU in patients with COPD, the multivariable model was built including each of the comorbidities independently rather than grouping them in a composite measure (Comorbidities ≥3) (Tables S2–S5). Baseline HCU of patients with COPD in 2019 is shown in Table S6. All analyses were performed with SAS 9.4 (SAS, Inc., Cary, North Carolina). P-value <0.05 was considered significant.
Results
We had a cohort of 160,913 patients admitted with the principal diagnosis of COVID-19, of which 57,756 patients were discharged home. Of these patients, 25.3% (14,622) had a diagnosis of COPD. Patients with COPD had a mean age of 75.48 ± 9.49, 55.5% were female, and 70.9% were White. Most patients with COPD (91.8%) had three or more comorbidities, and 35% of these patients received care in the intensive care unit (Table 1).
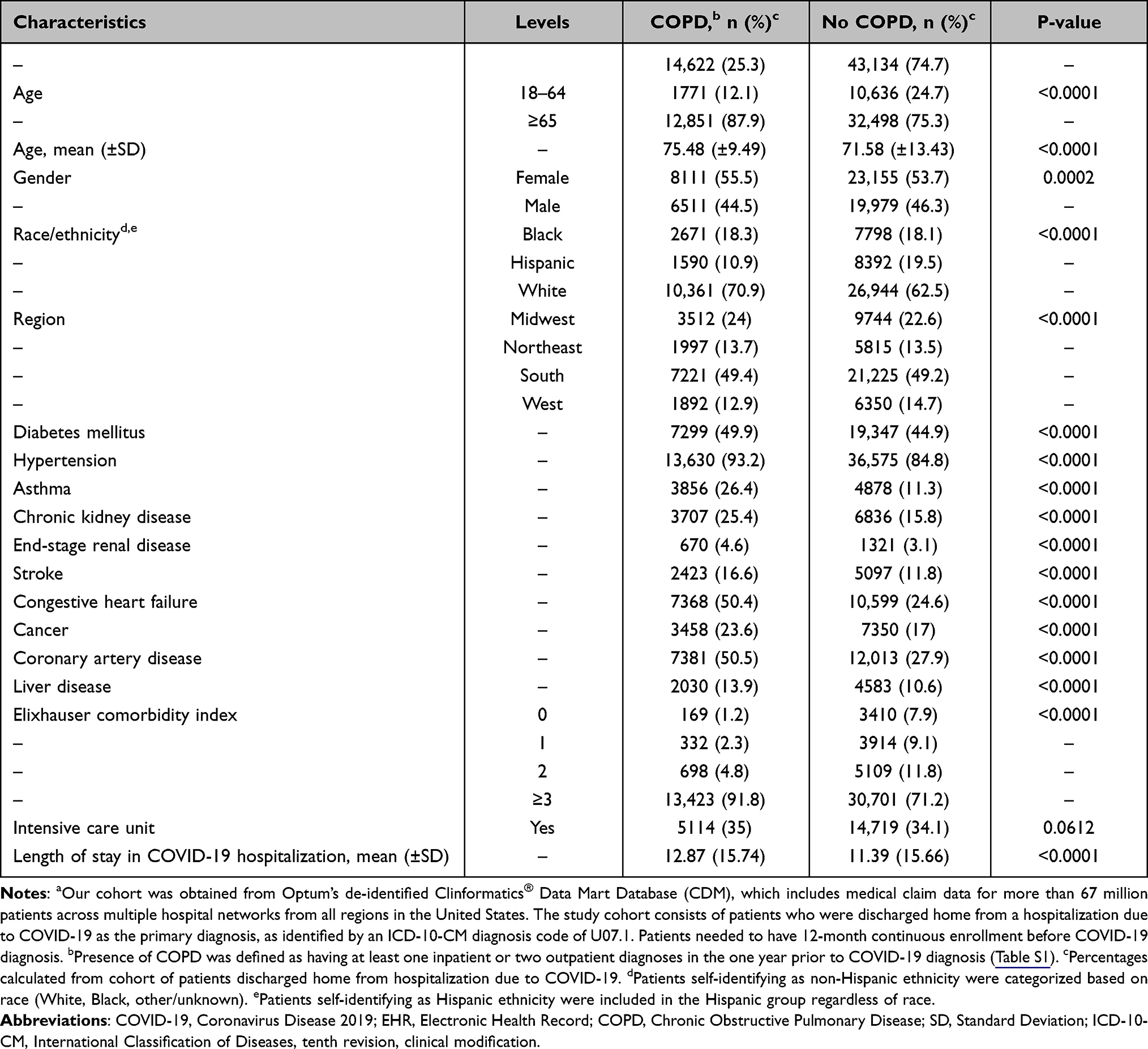 |
Table 1 Characteristics of Patients with and without COPD Discharged Home from Hospitalization Due to COVID-19 in the United States from April 2020 Until March 2021a |
In the nine months post-discharge, patients with COPD had significantly higher HCU than patients without COPD. Post-discharge ED visits, readmissions, length of stay during readmission, rehabilitation/SNF visits, outpatient office visits, and telemedicine visits relatively increased by 78.7%, 57.9%, 69.4%, 46.5%, 22.5%, and 38.2%, respectively (Table 2). Results from the multivariable Poisson regression model showed that patients with COPD are at increased risk for HCU in the nine months post-discharge. The risk of ED visits, readmissions, length of stay during readmissions, rehabilitation/SNF visits, outpatient office visits, and telemedicine visits were increased by 57% (RR 1.57; 95% CI 1.53–1.60), 50% (RR 1.50; 95% CI 1.46–1.54), 55% (RR 1.55; 95% CI 1.53–1.56), 18% (RR 1.18; 95% CI 1.14–1.22), 16% (RR 1.16; 95% CI 1.16–1.17), and 28% (RR 1.28; 95% CI 1.24–1.31), respectively (Table 3).
 |
Table 2 Healthcare Utilizationa Comparison in Patientsb with and without COPDc Within Nine Months Post-Discharge Home from COVID-19 Hospitalization |
 |
Table 3 Multivariable Model of the Risk of HCUa,b in Patients with COPDc,d Post-Discharge Home from COVID-19 Hospitalization |
We analyzed interactions between COPD and age, COPD and gender, and COPD and race/ethnicity in HCU outcomes. We conducted a stratified Poisson regression model, stratifying by age, gender, and race/ethnicity, when the corresponding interaction term was significant. We also included in the model each of the comorbidities independently rather than grouping them into a composite measure (Comorbidities ≥3) (Tables S3–S5). Both younger (age 18–64 years) and older (age ≥65 years) patients with COPD showed an increased relative risk of all measures of HCU post-COVID-19 hospitalization. Interestingly though, younger patients with COPD had 62% increased risk of ED visits (RR 1.62; 95% CI 1.54–1.70), 28% increased risk of readmissions (RR 1.28; 95% CI 1.19-1.36), and 50% greater risk of a longer length of stay during readmissions (RR 1.50; 95% CI 1.44–1.52) compared to patients without COPD. Also, this younger group showed 37% higher risk for telemedicine visits (RR1.37; 95% CI 1.30–1.50) and 13% increased risk for office visits (RR 1.13; 95% CI 1.11–1.20) (Table S3).
Although both men and women with COPD had an increased risk of HCU post-COVID compared to patients without COPD, the analysis of interactions between COPD and sex in HCU outcomes revealed that women with COPD had 40% increased risk for readmissions (RR 1.40; 95% CI 1.30–1.41) and 42% risk for longer length of stay during readmission (RR 1.42; 95% CI 1.40–1.44). Men’s risk of readmissions and longer length of stay during readmission was 30% (RR 1.30; 95% CI 1.22–1.32) and 28% (RR 1.40; 95% CI 1.30–1.41) (Table S4).
Similarly, HCU was worse in patients with COPD post-COVID-19 discharge across all examined races/ethnic backgrounds. The analysis of the interaction between COPD and race/ethnicity in HCU showed that Hispanic patients with COPD have a higher risk of HCU across the board (Table S5).
Discussion
In this retrospective study of patients with COPD who were discharged home after COVID-related hospitalization, patients with COPD had greater HCU than patients without COPD over a 9-month period. HCU was measured as a composite of ED visits, readmissions, length of stay during readmissions, admission to rehabilitation or skilled nursing facilities, outpatient office visits, and telemedicine visits. Moreover, as shown previously, the diagnosis of COPD was independently associated with greater HCU. Our main findings were the association between higher HCU and a diagnosis of COPD in patients younger than 65 years old, women, and patients with Hispanic ethnicity. The findings of greater healthcare utilization following a COVID-related hospitalization are similar to that observed in studies demonstrating an association between healthcare utilization following hospitalization for an acute exacerbation of COPD (AECOPD).12,15,23
AECOPD is usually caused by viral and/or bacterial infections, and patients with COPD discharged home after hospitalization for COPD exacerbation are at increased risk of mortality, readmissions, and greater HCU.10–13 These outcomes are mediated by age13 and comorbidities24–26 and are reported in the older population with COPD. Similarly, our findings indicate that patients with COPD have a greater risk of ED visits and readmissions. Importantly, our findings demonstrating 62% increased risk of ED visits and 28% increased risk of readmissions in younger patients with COPD (<65 years old) deserve careful attention. This finding has major implications for health resource planning considering that ~30% of the associated health burden may be due to COVID-19 related disability and HCU.27–30
Our second main finding corresponds to the high risk of HCU in women with COPD post-discharge from COVID-19. In general, women appeared to be protected from the adverse effects of SARS-COV-2 infection, showing better outcomes than male patients.31,32 However, women with COPD who are hospitalized with COVID-19 may have an increased risk of mortality,1 and, based on our findings, those who survive may be at risk of high HCU post-discharge (ie, 36% increased risk for ED visits, 40% increased risk for readmissions, and 42% risk for longer length of stay during readmission, etc.) (Table S4). The differences in HCU in women with COPD post COVID-19 infection may be explained by social rather than biological variables.33
Our third main finding was the racial/ethnic differences in the HCU of patients with COPD post-COVID-19 hospitalization (Table S5). There are known disparities in care, such as higher odds of being undiagnosed, greater barriers to access care and possibly worse outcomes for Black and Hispanic patients with COPD.34–40 In our study we found that Black and Hispanic patients with COPD discharged home after a COVID-19 hospitalization have an increased risk for HCU compared to patients without COPD (Table S5). But Hispanic patients’ 40% increased risk of ED visits and readmissions should be noticed. This is because, historically, Hispanic patients have had lower odds of readmission and mortality due to COPD, raising the concept of the “Hispanic paradox”.41–43 The observed higher HCU in our study could be explained by higher clinical risk profiles, for example, more comorbidities, more prior acute stays, more ICU admissions, and longer lengths of stay,43 but variations in smoking patterns, environmental exposures, genetic susceptibility, and healthcare access may also play a role.44
We are uncertain as to whether the observed increase in HCU in patients with COPD reflects increased susceptibility to post-acute sequelae of SARS-CoV-2 infection (also known as post-acute COVID-19 syndrome) or other factors.45 With an increasing number of COVID-19 survivors,9 post-acute COVID-19 syndrome has emerged as a disorder of ongoing healthcare use.46,47 This syndrome is described in patients who continue to have signs and symptoms of the illness four weeks after the initial diagnosis of the SARS-CoV-2 infection, which are not explained by other causes.45,48 Symptoms can vary, including chronic cough, persistent or worsening shortness of breath, palpitations, neuropathy, cognitive impairment, fatigue, and anxiety.48 Observational studies have shown that the prevalence of post-acute sequelae of SARS-CoV-2 infection is between 10% and 30% in the general population, with symptoms lasting for several months.30,48 This syndrome is more common in older individuals, patients with pre-existing conditions, and patients who have required hospital admission for acute SARS-CoV-2 infection.49
Our study has several strengths, including a large sample size and a nine-month post-discharge follow-up after COVID-19 hospitalization. Limitations include the retrospective design that can only evaluate associations and does not infer causality. Thus, the increased risk in HCU observed in patients with COPD could be related to other unmeasured confounding variables.13,24–26 Additionally, increased HCU is linked to the degree of airflow obstruction in patients with COPD25,26 and our administrative database did not provide spirometry data, thus we were unable to determine the degree of airflow obstruction. Yet, investigators have examined HCU of patients with COPD using administrative claims data and assessed disease severity in the absence of spirometry measurements.50–52 Similarly, HCU in COPD is linked to increased age and number of comorbidities, and we found an increased risk of HCU in the older population (age 65 years and older) with more comorbid conditions. Notably, the finding of high HCU (after adjusting for comorbidities) in the younger population with COPD, who may have less comorbidities, is intriguing and may be examined in future investigations. The potential interactions between COPD, comorbid conditions, and increased HCU remain relevant.26
Conclusion
Patients with COPD hospitalized with COVID-19 experienced increased HCU post-discharge.
Abbreviations
CAD, Coronary Artery Disease; CHF, Congestive Heart Failure; CKD, Chronic Kidney Disease; COPD, Chronic Obstructive Pulmonary Disease; COVID-19, Coronavirus Disease 2019; DM, Diabetes Mellitus; ED, Emergency Department; ESRD, End-Stage Renal Disease; HCU, healthcare utilization; HTN, Hypertension; ICD-10-CM, International Classification for Diseases, tenth revision, clinical modification; ICU, Intensive Care Unit; LOS, length of stay; PCP, Primary Care Provider, SNF, skilled nursing facility, SD, Standard Deviation.
Author Contributions
All authors made a significant contribution to the work reported in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
Dr. Puebla Neira reports support from NHLBI Advanced Respiratory Research for Equity (AiRE) - AZ-PRIDE Program grant (5R25HL126140-09) during the conduct of this study. Dr. Parthasarathy reports personal fees from Jazz Pharmaceuticals, Inc., UpToDate, Inc., grants from NIH (R25-HL126140, R33-HL151254; OT2-HL161847; R21-HD109777; C06-OD028307; HL140144; HL138377; 1OT2HL156812; OT2-HL156912 and OT2HL158287), grants from PCORI (DI-2018C2-13161, CER-2018C2-13262), grants from Department of Defense (W81XWH20C0051 and W81XWH2110025), grants from Pima County Health Department (CPIMP211275), grants from Arizona Commerce Authority (LTR DTD 021822), grants from Sergey Brin Foundation, grants from Philips, Inc. (0483-06-161311-73077), grants from Sommetrics, Inc., grants from American Academy of Sleep Medicine Foundation (AASMF; 169-SR-17), grants from Regeneron, Inc., grants from Centers for Disease Control (CDC FR Doc. 2021–19050), personal fees from AbbVie, Inc., and SaiOx, Inc., outside the submitted work; in addition, Dr. Parthasarathy has a patent US20160213879A1 licensed to SaiOx, Inc. Dr. Kuo reports grants from the UTMB Claude D. Pepper Older Americans Independence Center during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Puebla Neira DA, Watts A, Seashore J, et al. Outcomes of patients with COPD hospitalized for coronavirus disease 2019. Chronic Obstr Pulm Dis. 2021;8(4):517–527. doi:10.15326/JCOPDF.2021.0245
2. Zhao Q, Meng M, Kumar R, et al. The impact of COPD and smoking history on the severity of COVID-19: a systemic review and meta-analysis. J Med Virol. 2020;92(10):1915–1921. doi:10.1002/JMV.25889
3. Gerayeli FV, Milne S, Cheung C, et al. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:100789. doi:10.1016/J.ECLINM.2021.100789
4. Attaway AA, Zein J, Hatipoğlu US. SARS-CoV-2 infection in the COPD population is associated with increased healthcare utilization: an analysis of Cleveland clinic’s COVID-19 registry. EClinicalMedicine. 2020;26:100515. doi:10.1016/J.ECLINM.2020.100515
5. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369. doi:10.1136/bmj.m1966
6. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
7. Hippisley-Cox J, Young D, Coupland C, et al. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: cohort study including 8.3 million people. Heart. 2020;106(19):1503–1511. doi:10.1136/heartjnl-2020-317393
8. Zheng M, Romero GF, Marron RM, et al. Impact of chronic obstructive pulmonary disease and emphysema on outcomes of hospitalized patients with COVID-19 pneumonia. Chronic Obstr Pulm Dis. 2021;8(2):255–268. doi:10.15326/JCOPDF.2020.0200
9. McNaughton CD, Austin PC, Sivaswamy A, et al. Post-acute health care burden after SARS-CoV-2 infection: a retrospective cohort study. CMAJ. 2022;194(40):E1368–E1376. doi:10.1503/CMAJ.220728
10. Grasso ME, Weller WE, Shaffer TJ, Diette GB, Anderson GF. Capitation, managed care, and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158(1):133–138. doi:10.1164/AJRCCM.158.1.9710041
11. Regueiro CR, Hamel MB, Davis RB, Desbiens N, Connors AF, Phillips RS. A comparison of generalist and pulmonologist care for patients hospitalized with severe chronic obstructive pulmonary disease: resource intensity, hospital costs, and survival*. Am J Med. 1998;105:366–372. doi:10.1016/S0002-9343(98)00290-3
12. Connors AF, Dawson NV, Thomas C, et al. Outcomes following acute exacerbation of severe chronic obstructive lung disease. Am J Respir Crit Care Med. 1996;154(4 I):959–967. doi:10.1164/AJRCCM.154.4.8887592
13. Cydulka RK, Mcfadden ER, Emerman CL, Sivinski LD, Pisanelli W, Rimm AA. Patterns of hospitalization in elderly patients with asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1997;156(6):1807–1812. doi:10.1164/AJRCCM.156.6.9611008
14. Mapel DW, Hurley JS, Frost FJ, Petersen HV, Picchi MA, Coultas DB. Health care utilization in chronic obstructive pulmonary disease: a case-control study in a health maintenance organization. Arch Intern Med. 2000;160(17):2653–2658. doi:10.1001/ARCHINTE.160.17.2653
15. Lindenauer PK, Dharmarajan K, Qin L, Lin Z, Gershon AS, Krumholz HM. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/rccm.201709-1852OC
16. Puebla Neira DA, Hsu ES, Kuo YF, Ottenbacher KJ, Sharma G. Readmissions reduction program: mortality and readmissions for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(4):437–446. doi:10.1164/rccm.202002-0310OC
17. Verbrugge LM, Patrick DL. Seven chronic conditions: their impact on US adults’ activity levels and use of medical services. Am J Public Health. 1995;85(2):173–182. doi:10.2105/AJPH.85.2.173
18. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
19. Vilkman S, Keistinen T, Tuuponen T, Kivela SL. Survival and cause of death among elderly chronic obstructive pulmonary disease patients after first admission to hospital. Respiration. 1997;64(4):281–284. doi:10.1159/000196687
20. Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalization for exacerbation of COPD. Chest. 2006;129(3):536–544. doi:10.1378/CHEST.129.3.536
21. Au DH, Udris EM, Fihn SD, McDonell MB, Curtis JR. Differences in health care utilization at the end of life among patients with chronic obstructive pulmonary disease and patients with lung cancer. Arch Intern Med. 2006;166(3):326–331. doi:10.1001/ARCHINTE.166.3.326
22. Puebla Neira D, Zaidan MF, Duarte AG, et al. Health Care Utilization of Patients with Chronic Obstructive Pulmonary Disease Post-Discharge from Coronavirus Disease 2019 Hospitalization. American Thoracic Society; 2023.
23. Hartnett J, Donga P, Ispas G, et al. Risk factors and medical resource utilization in US adults hospitalized with influenza or respiratory syncytial virus in the hospitalized acute respiratory tract infection study. Influenza Other Respi Viruses. 2022;16(5):906–915. doi:10.1111/IRV.12994
24. Lin PJ, Shaya FT, Scharf SM. Economic implications of comorbid conditions among Medicaid beneficiaries with COPD. Respir Med. 2010;104(5):697–704. doi:10.1016/j.rmed.2009.11.009
25. Gerdtham UG, Andersson LF, Ericsson Å, et al. Factors affecting chronic obstructive pulmonary disease (COPD)-related costs: a multivariate analysis of a Swedish COPD cohort. Eur J Heal Econ. 2009;10(2):217–226. doi:10.1007/S10198-008-0121-6/TABLES/5
26. Simon-Tuval T, Scharf SM, Maimon N, Bernhard-Scharf BJ, Reuveni H, Tarasiuk A. Determinants of elevated healthcare utilization in patients with COPD. Respir Res. 2011;12(1):1–8. doi:10.1186/1465-9921-12-7/TABLES/7
27. NIHR N. Themed review: living with Covid19 – second review; 2021.
28. McAlister FA, Dong Y, Chu A, et al. The risk of death or unplanned readmission after discharge from a COVID-19 hospitalization in Alberta and Ontario. CMAJ. 2022;194(19):E666–E673. doi:10.1503/CMAJ.220272
29. Tartof SY, Malden DE, Liu I-LA, et al. Health care utilization in the 6 months following SARS-CoV-2 infection. JAMA Netw Open. 2022;5(8):e2225657–e2225657. doi:10.1001/JAMANETWORKOPEN.2022.25657
30. Daugherty SE, Guo Y, Heath K, et al. Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study. BMJ. 2021:373. doi:10.1136/BMJ.N1098
31. Haitao T, Vermunt JV, Abeykoon J, et al. COVID-19 and sex differences: mechanisms and biomarkers. Mayo Clin Proc. 2020;95(10):2189–2203. doi:10.1016/j.mayocp.2020.07.024
32. Klein SL, Morgan R. The impact of sex and gender on immunotherapy outcomes. Biol Sex Differ. 2020;11(1):1–13. doi:10.1186/s13293-020-00301-y
33. Connor J, Madhavan S, Mokashi M, et al. Health risks and outcomes that disproportionately affect women during the Covid-19 pandemic: a review. Soc Sci Med. 2020;266:113364. doi:10.1016/j.socscimed.2020.113364
34. Mamary AJ, Stewart JI, Kinney GL, et al. Race and gender disparities are evident in COPD underdiagnoses across all severities of measured airflow obstruction. Chronic Obstr Pulm Dis J COPD Found. 2018;5(3):177. doi:10.15326/JCOPDF.5.3.2017.0145
35. Ejike CO, Dransfield MT, Hansel NN, et al. Chronic obstructive pulmonary disease in America’s black population the black population. Am J Respir Crit Care Med. 2019;200(4):423–430. doi:10.1164/rccm.201810-1909PP
36. Gaffney AW, Hawks L, White AC, et al. Health care disparities across the urban-rural divide: a national study of individuals with COPD. J Rural Heal. 2022;38(1):207–216. doi:10.1111/JRH.12525
37. Gaffney AW, Hawks L, Bor D, et al. National trends and disparities in health care access and coverage among adults with asthma and COPD: 1997–2018. Chest. 2021;159(6):2173–2182. doi:10.1016/J.CHEST.2021.01.035
38. Han MLK, Curran-Everett D, Dransfield MT, et al. Racial differences in quality of life in patients with COPD. Chest. 2011;140(5):1169–1176. doi:10.1378/chest.10-2869
39. Arnett MJ, Thorpe RJ, Gaskin DJ, Bowie JV, LaVeist TA. Race, medical mistrust, and segregation in primary care as usual source of care: findings from the exploring health disparities in integrated communities study. J Urban Heal. 2016;93(3):456–467. doi:10.1007/S11524-016-0054-9/TABLES/2
40. Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance—United States, 1999–2011. Chest. 2013;144(1):284–305. doi:10.1378/CHEST.13-0809
41. Bruse S, Sood A, Petersen H, et al. New Mexican Hispanic smokers have lower odds of chronic obstructive pulmonary disease and less decline in lung function than non-Hispanic whites. Am J Respir Crit Care Med. 2011;184(11):1254–1260. doi:10.1164/rccm.201103-0568OC
42. Young RP, Hopkins RJ. A review of the Hispanic paradox: time to spill the beans? Eur Respir Rev. 2014;23(134):439–449. doi:10.1183/09059180.00000814
43. Nastars DR, Rojas JD, Ottenbacher KJ, Graham JE. Race/ethnicity and 30-day readmission rates in medicare beneficiaries with COPD. Respir Care. 2019;64(8):931–936. doi:10.4187/respcare.06475
44. Powell R, Davidson D, Divers J, et al. Genetic ancestry and the relationship of cigarette smoking to lung function and per cent emphysema in four race/ethnic groups: a cross-sectional study. Thorax. 2013;68(7):634–642. doi:10.1136/THORAXJNL-2012-202116/-/DC1
45. Thaweethai T, Jolley SE, Karlson EW, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329(22):1934–1946. doi:10.1001/jama.2023.8823
46. Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–631. doi:10.1038/s41591-021-01292-y
47. Crook H, Raza S, Nowell J, Young M, Edison P. Long covid—mechanisms, risk factors, and management. BMJ. 2021;374. doi:10.1136/BMJ.N1648
48. Sisó-Almirall A, Brito-Zerón P, Ferrín LC, et al. Long covid-19: proposed primary care clinical guidelines for diagnosis and disease management. Int J Environ Res Public Health. 2021;18(8):4350. doi:10.3390/IJERPH18084350/S1
49. Dennis A, Wamil M, Alberts J, et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: a prospective, community-based study. BMJ Open. 2021;11(3):e048391. doi:10.1136/BMJOPEN-2020-048391
50. Mapel DW, Dutro MP, Marton JP, Woodruff K, Make B. Identifying and characterizing COPD patients in US managed care. A retrospective, cross-sectional analysis of administrative claims data. BMC Health Serv Res. 2011;11:11. doi:10.1186/1472-6963-11-43
51. Stanford RH, Nag A, Mapel DW, et al. Validation of a new risk measure for chronic obstructive pulmonary disease exacerbation using health insurance claims data. Ann Am Thorac Soc. 2016;13(7):1067–1075. doi:10.1513/AnnalsATS.201508-493OC
52. Make B, Dutro MP, Paulose-Ram R, Marton JP, Mapel DW. Undertreatment of COPD: a retrospective analysis of us managed care and medicare patients. Int J COPD. 2012;7:1–9. doi:10.2147/COPD.S27032
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.