Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Healthcare System Transition in Kazakhstan and Its Impact on Inguinal Hernia Repair Outcomes: A Multidisciplinary Comparative Analysis of TEP, TIPP, and Open Lichtenstein Procedures
Authors Akkaliyev Y, Kamaliev M ![]() , Karataev MM, Akkaliyev M, Aliyeva S, Tsigengagel О
, Karataev MM, Akkaliyev M, Aliyeva S, Tsigengagel О
Received 18 March 2026
Accepted for publication 14 May 2026
Published 27 May 2026 Volume 2026:19 609610
DOI https://doi.org/10.2147/JMDH.S609610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Yerlan Akkaliyev,1,2 Maksut Kamaliev,2 Madamin Musaevich Karataev,3 Merkhat Akkaliyev,4 Sholpan Aliyeva,1 Оxana Tsigengagel5
1National Hospital of the Medical Center of the President’s Affairs Administration of the Republic of Kazakhstan, Almaty, Kazakhstan; 2Department of Health Management, Kazakhstan Medical University “Kazakhstan School of Public Health”, Almaty, Kazakhstan; 3Department of Public Health, I.K. Akhunbaev Kyrgyz State Medical Academy, Bishkek, Kyrgyzstan; 4Department of Surgical Disciplines, NCJSC Semey Medical University, Semey, Kazakhstan; 5Department of Epidemiology and Biostatistics, Astana Medical University, Astana, Kazakhstan
Correspondence: Оxana Tsigengagel, Department of Еpidemiology and Biostatistics, Astana Medical University, st. Beybitshilik 49a, Astana, 010000, Kazakhstan, Email [email protected]
Background: Management of inguinal hernia repair (IHR) in transition economies remains a challenge where clinical adoption of international guidelines, such as HerniaSurge 2023, is often hindered by legacy funding models. This study evaluates the impact of surgical technique transition on clinical outcomes, cost-utility, and institutional resource turnover in Almaty, Kazakhstan.
Methods: A prospective-retrospective analysis of 505 patients was conducted (January 2021 to December 2023). For clinical comparison, a matched subgroup (n=138) was analyzed, comparing Open Lichtenstein (n=56), Laparoscopic Totally Extraperitoneal (TEP, n=42), and Open Transinguinal Preperitoneal (TIPP, n=40) repairs. Clinical outcomes were quantified via the EuraHS-QoL scale. Economic efficiency was modeled using Quality-Adjusted Life Years (QALY). We introduced the System Burden Index (SBI) — calculated as the ratio of category mean length of stay (LOS) to population average — to identify productivity bottlenecks across financing channels (Commercial, Government Quotas, and City Budget).
Results: Posterior approach techniques (TEP and TIPP) significantly reduced postoperative pain frequency compared to the Lichtenstein group (26.2% and 32.5% vs. 51.8%, p=0.013). TEP was identified as the dominant strategy for cost-utility. Management analysis revealed a significant “Efficiency Gap” across funding sectors: government quota cases showed a mean LOS of 8.31 days (SBI 1.28) compared to 5.37 days (SBI 0.83) in the commercial sector. Our predictive model suggests that transitioning state-funded sectors to rapid-recovery protocols could potentially reclaim 4.7 bed-days per patient.
Conclusion: Transitioning to TEP/TIPP protocols is a key factor for enhancing healthcare capacity in Kazakhstan. Shifting reimbursement logic from bed-day occupancy to value-based outcome packages is essential to align regional practice with global surgical standards and optimize institutional throughput.
Keywords: inguinal hernia, totally extraperitoneal, TEP, transinguinal preperitoneal, TIPP, value-based healthcare, health economics, system burden index, QALY, Kazakhstan, length of stay, resource optimization
Introduction
Inguinal hernia repair (IHR) is among the most frequently performed surgical procedures worldwide, with an estimated annual volume exceeding 20 million operations. Beyond its prevalence, the condition carries a substantial socioeconomic burden, primarily affecting the quality of life and productivity of working-age individuals who often serve as the primary economic support for their households. Recent updates to international standards, specifically the HerniaSurge 2023 guidelines, provide a strong recommendation for laparoscopic techniques, such as Totally Extraperitoneal (TEP) and Transabdominal Preperitoneal (TAPP) repair. These recommendations are based on high-level evidence demonstrating accelerated functional recovery and a reduced incidence of chronic postoperative pain.1,2
Despite this consensus, the integration of minimally invasive techniques into routine clinical practice remains inconsistent, particularly in transition economies.3,4 In such settings, the “clinical gold standard” often encounters structural and economic barriers. In Kazakhstan, the introduction of Compulsory Social Health Insurance (CSHI) has established a hybrid financing model during a period of systemic reform.5 In this evolving environment, reimbursement mechanisms may inadvertently influence clinical workflows. Specifically, funding models historically predicated on bed-day occupancy can create a misalignment where rapid clinical recovery and early discharge might be perceived as an administrative disadvantage.6 This fiscal logic can potentially delay the adoption of evidence-based surgical innovations that prioritize patient-centered outcomes.
In this context, the present study evaluates the implementation of posterior approach repairs specifically laparoscopic TEP and open Transinguinal Preperitoneal (TIPP) as dual-value interventions aimed at restoring patient quality of life while improving institutional resource management. To address the gap between clinical performance and organizational efficiency, we introduce the SBI as an exploratory descriptive tool. The study aims to provide a multidisciplinary analysis of how transitioning from traditional anterior repair (Lichtenstein) to modern preperitoneal techniques can optimize surgical throughput and institutional turnover within a rapidly changing healthcare system.
Materials and Methods
Ethical Statement and Study Design
This study utilized a hybrid prospective - retrospective cohort design to evaluate clinical, functional, and institutional outcomes of inguinal hernia repair. The study was conducted at the Medical Center Hospital of the Presidential Affairs Administration of the Republic of Kazakhstan (Almaty, Kazakhstan) between January 2021 and December 2023.
The study protocol was approved by the Institutional Review Board of Kazakhstan’s Medical University, “Kazakhstan School of Public Health” (Protocol No. A114; approved on December 20, 2019). The study adhered to the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all patients participating in the prospective phase (12-month quality-of-life follow-up). For the retrospective collection of perioperative data, institutional records were de-identified to ensure patient confidentiality.
Patient Selection and Eligibility Criteria
The total study population consisted of 505 adult patients (age ≥18 years) diagnosed with primary unilateral inguinal hernia. Inclusion Criteria: Primary unilateral or bilateral reducible inguinal hernia; ASA (American Society of Anesthesiologists) physical status I–III; and availability of complete 12-month follow-up data. Exclusion Criteria: Recurrent hernias; emergency presentations (incarcerated or strangulated hernias); history of major pelvic or lower abdominal surgery; and patients with cognitive or linguistic barriers preventing the completion of survey instruments.
Surgical Interventions
Patients underwent one of three standardized procedures, performed by senior surgical staff with a median experience of 14 years (range 10–22 years), according to European Her-nia Society (EHS) guidelines:
Lichtenstein Open Repair (LOR): A standard anterior tension-free repair using a polypropylene mesh. This group represents the conventional open approach.
Transinguinal Preperitoneal (TIPP) Repair: An open preperitoneal technique. For this comparative analysis, TIPP is classified as an open procedure and analyzed separately from laparoscopic techniques.
Totally Extraperitoneal (TEP) Repair: A laparoscopic, minimally invasive surgery (MIS) approach performed via a three-port preperitoneal access.
Propensity Score Matching (PSM)
To minimize selection bias and control for confounding variables inherent in non-randomized studies, a matched comparative subgroup of 138 patients was extracted from the total population (N=505). A 1:1:1 nearest-neighbor matching algorithm was employed with a caliper width of 0.2 standard deviations of the logit of the propensity score. Patients were matched based on three key prognostic indicators: age, biological sex (male), and baseline symptom severity (as measured by preoperative EuraHS-QoL scores). The balance of the matched cohorts was verified using Standardized Mean Differences (SMDs), where an SMD < 0.1 was considered indicative of negligible group imbalance.
Clinical and Patient-Reported Outcome Measures (PROMs)
Clinical Outcomes
Data were collected on operative time (minutes), length of stay (LOS, days), and postoperative complications (seroma, hematoma, surgical site infection) classified according to the Clavien-Dindo system.
Functional and Quality of Life (QoL) Metrics
The European Hernia Society Quality of Life (EuraHS-QoL) questionnaire was used to assess functional recovery at 12 months postoperatively. This instrument evaluates three domains: pain intensity, activity restriction, and cosmetic dissatisfaction. Binary outcomes for “activity limitation”, “cosmetic dissatisfaction”, and “postoperative pain frequency” were derived using a predefined cutoff of >3 on a 0–10 Likert scale. The 12-month postoperative follow-up was established through a hybrid approach combining mandatory in-person clinical examinations in the outpatient department and supplementary structured telephonic questionnaires to ensure comprehensive data collection.
Economic Evaluation and Institutional Efficiency
Cost-Utility Analysis
An economic evaluation was performed from the healthcare provider (hospital) perspective. Quality-of-life scores were converted into utility weights using a validated crosswalk method to calculate Quality-Adjusted Life Years (QALYs). Direct medical costs included surgical consumables, anesthesia, and bed-day charges based on 2023 institutional rates. A 12-month time horizon was applied.
System Burden Index (SBI)
To assess resource utilization patterns, we utilized the SBI as an exploratory descriptive indicator. The SBI normalizes the mean LOS of specific subgroups (eg., specific funding models or surgical techniques) against the overall institutional mean LOS for inguinal hernia repair:
An SBI > 1.0 identifies patient cohorts or administrative channels where hospitalization duration exceeds the institutional average, potentially indicating resource consumption driven by reimbursement structures or administrative logistics rather than clinical necessity.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics version 26.0. Continuous variables are reported as mean ± standard deviation (SD). For the three-group comparison, differences were assessed using one-way ANOVA with Bonferroni post-hoc tests for continuous data and Chi-square (χ2) or Fisher’s exact tests for categorical proportions. A p-value < 0.05 was considered statistically significant. For the economic model, Incremental Cost-Effectiveness Ratios (ICERs) were calculated to assess the dominance of MIS over open techniques.
Results
Baseline Patient Demographics and Clinical Characteristics
Baseline equivalence was established across the matched study groups (n=138) to ensure comparability. As demonstrated in Table 1, the Lichtenstein Open Repair (LOR), Totally Extraperitoneal (TEP), and Transinguinal Preperitoneal (TIPP) groups showed no significant differences in age (p=0.312), gender distribution (92.8% male across all groups; p=0.999), or preoperative EuraHS-QoL scores for pain (p=0.189), activity restriction (p=0.409), and cosmetic dissatisfaction (p=0.393). These results confirm that the propensity score matching successfully balanced the cohorts across key prognostic variables before intervention.
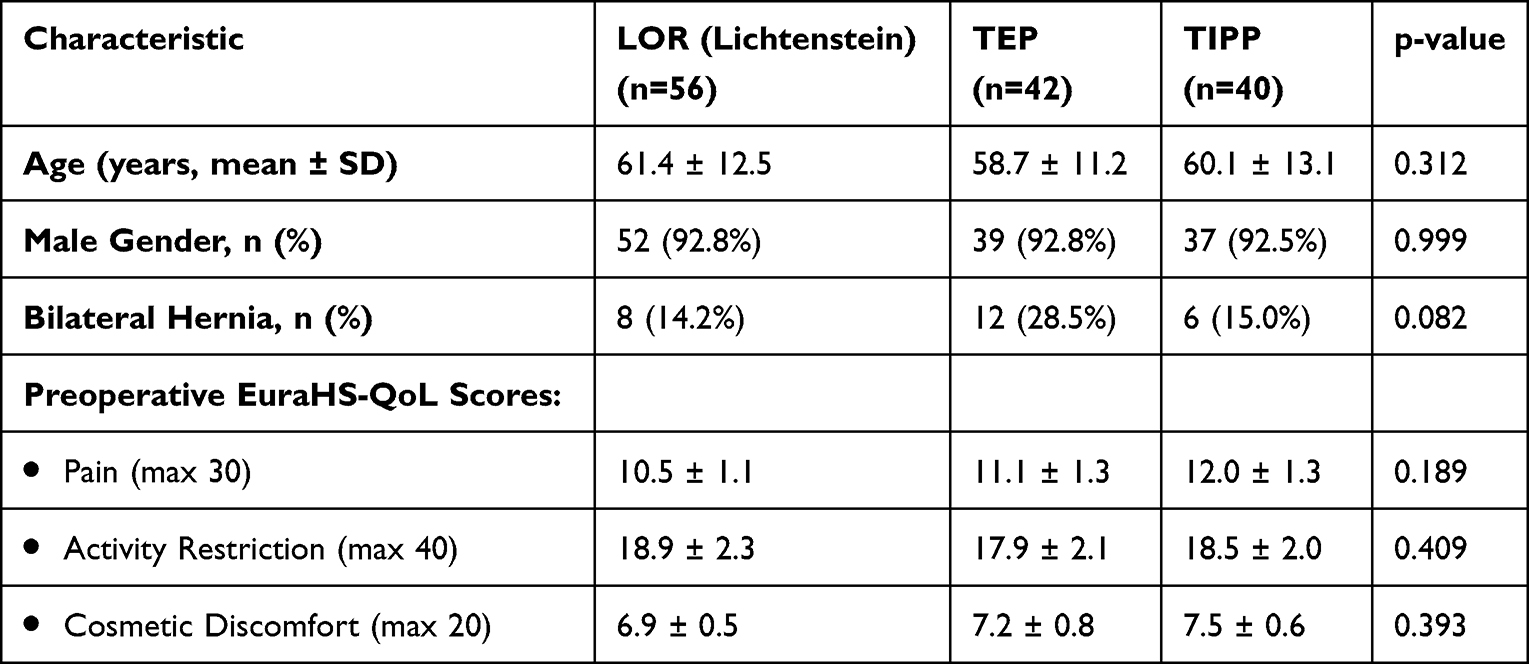 |
Table 1 General Characteristics and Preoperative Quality of Life Profiles (n=138) |
Clinical Safety and Patient-Reported Outcomes
Postoperative outcomes demonstrated significant differences in recovery profiles between the surgical groups (Table 2). Patients in the LOR group reported a significantly higher frequency of postoperative pain at 12 months (51.8%) compared to the TEP group (26.2%, pairwise p=0.013). Functional reintegration followed a similar pattern, with 57.1% of LOR patients reporting activity limitations versus 35.7% in the TEP cohort (p=0.042). Seroma formation occurred in 4.7% (n=2) of the TEP group, 5.0% (n=2) of the TIPP group, and 3.5% (n=2) in the LOR group (p=0.892), with all cases resolving via conservative management.
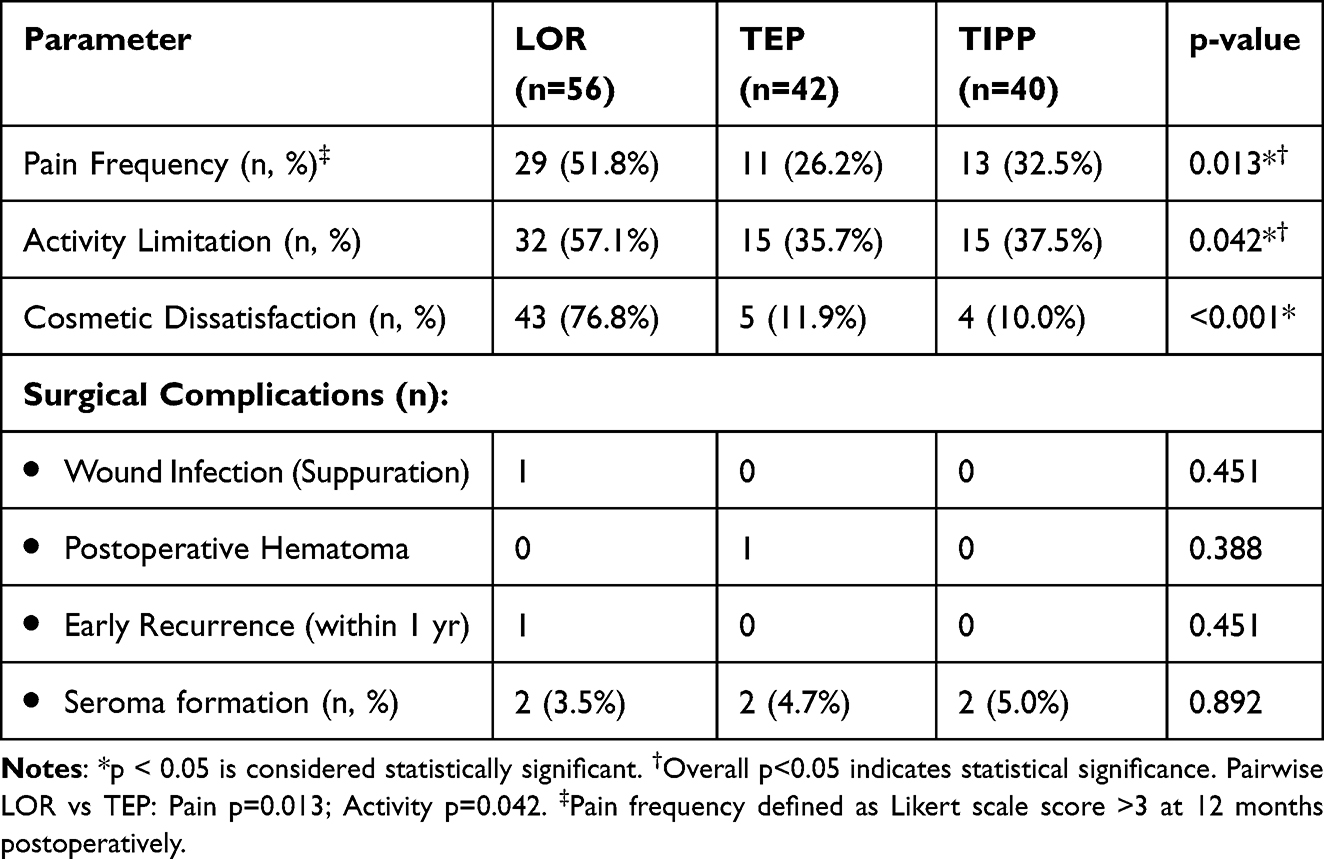 |
Table 2 Postoperative Clinical Outcomes and Complications (n=138) |
Regarding clinical safety, no major early complications or recurrences were recorded in the TEP or TIPP cohorts during the 12-month follow-up. The LOR group experienced one case of wound infection and one early recurrence. Cosmetic dissatisfaction was the most significant differentiator, reported by 76.8% of LOR patients compared to 11.9% in the TEP group and 10.0% in the TIPP group (p<0.001). Figure 1 provides a visual comparison of these functional outcomes, demonstrating the superior functional restoration profile of the TEP and TIPP techniques.
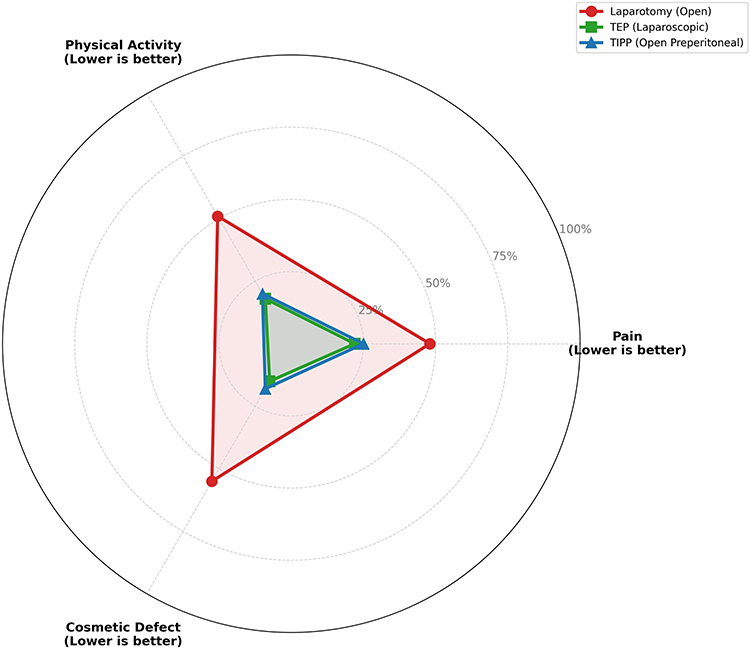 |
Figure 1 Comparison of Patient-Reported Outcomes (LOR, TEP, and TIPP). Radar chart illustrating functional outcomes across three dimensions: Pain, Physical Activity, and Cosmetic Defect. Values are normalized; lower scores indicate superior clinical performance. TEP (Green) and TIPP (Blue) demonstrate a concentrated inner profile, indicating marked superiority in functional restoration compared to the LOR (Red) group. |
Institutional Efficiency and Economics
The analysis of the broader population (N=505) revealed that resource utilization was associated with the funding model (Table 3). Patients treated under Government Quotas experienced the longest hospital stays (8.31 ± 2.1 days), resulting in an SBI of 1.28. In contrast, Paid (Commercial) services demonstrated an SBI of 0.83.
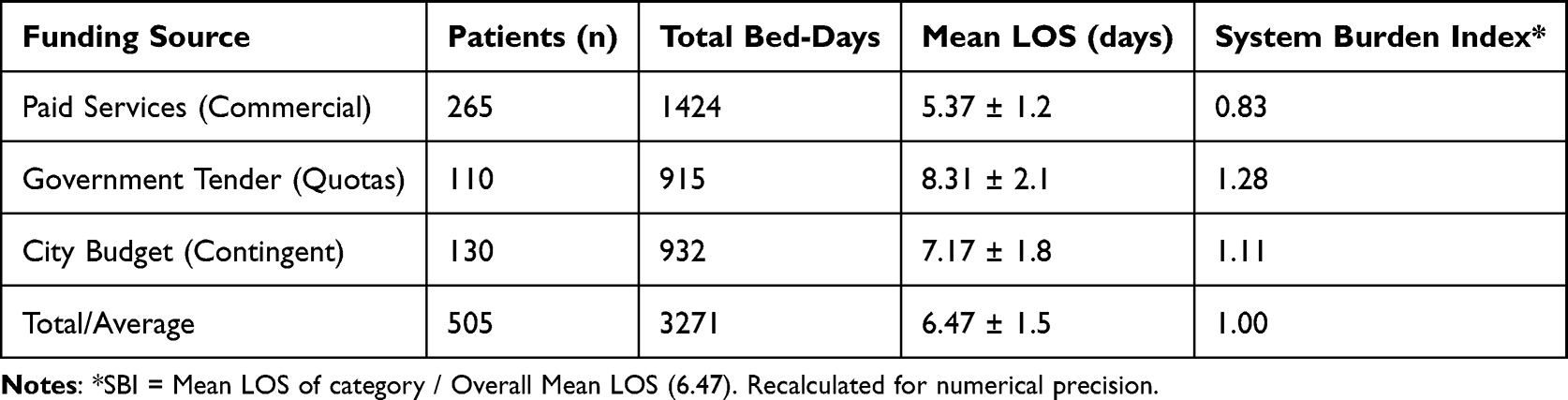 |
Table 3 Resource Utilization and SBI Metrics by Funding Source (N=505) |
Transitioning from the institutional mean LOS (6.47 days) to a standardized laparo-endoscopic protocol (mean TEP LOS: 1.8 days) suggests a theoretical “Bed-Day Recovery” of 4.7 days per patient. Figure 2 illustrates the cost-effectiveness plane, identifying TEP as the dominant strategy, providing maximum health utility gains at op-timal costs.
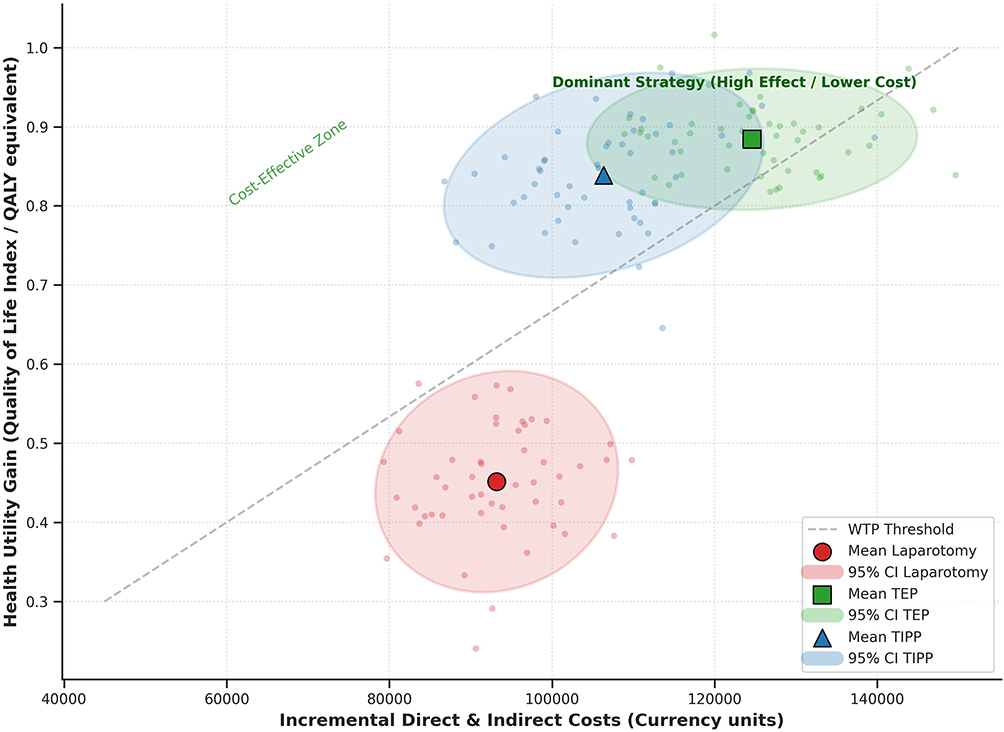 |
Figure 2 Cost-Effectiveness Plane of Inguinal Hernia Repair Techniques. Scatter plot representing 1,000 bootstrap simulations. The y-axis shows health utility gains (QALY equivalents) derived from EuraHS-QoL scores, and the x-axis reflects incremental direct and indirect costs in local currency units. The gray dashed line represents the Willingness-to-Pay (WTP) threshold. TEP (Green square) and TIPP (Blue triangle) are positioned in the “Cost-Effective Zone” (above the WTP threshold). TEP is identified as the dominant strategy, providing the highest health utility gains relative to incremental costs compared to Lichtenstein repair (Red circle).7–10 |
Discussion
The clinical results of this study reinforce the established evidence base suggesting that laparo-endoscopic (TEP) and open preperitoneal (TIPP) repairs offer superior functional recovery and lower postoperative pain compared to the Lichtenstein open anterior repair. While these clinical advantages are well-documented in international guidelines, such as the HerniaSurge 2023 consensus,1 this study provides a novel analysis of how these outcomes intersect with institutional resource utilization and healthcare financing in a transition economy.
A notable finding, beyond the direct clinical comparisons, is the observed mean length of stay (LOS) across all techniques (6.47 days), which remains considerably higher than typically reported in European standards (often less than 24–48 hours for comparable procedures). This prolonged LOS in Kazakhstan is largely attributable to deeply entrenched legacy reimbursement models, where hospital funding is historically tied to bed-day accumulation. Furthermore, a more conservative post-surgical care culture and the current lack of widespread “Day Surgery” or rapid-discharge infrastructure in many public healthcare facilities also contribute to these extended inpatient durations, rather than specific deficiencies in pain management or anesthesia protocols.
A key finding of our analysis is the observed reduction in length of stay (LOS) associated with MIS compared to the institutional mean. The theoretical “bed-day recovery” of 4.7 days (the difference between the institutional mean of 6.47 days and the TEP mean of 1.8 days) suggests a significant opportunity for institutional capacity optimization. In urban centers like Almaty, where surgical volume is often constrained by inpatient bed turnover rather than operating room availability, the transition to standardized MIS protocols could serve as a mechanism to alleviate structural bottlenecks. However, our projections regarding increased hospital throughput remain theoretical capacity models and would require broader logistical adjustments to be realized at scale.
The socio-economic implications are particularly relevant given that 92.8% of the study cohort comprised working-age males. In the context of Kazakhstan’s labor market, faster functional recovery directly correlates with reduced productivity loss. Prolonged hospitalization and delayed vocational reintegration represent a quantifiable economic burden11. Our results suggest that MIS is not merely a technical refinement but a value-based intervention that supports the socio-economic reintegration of surgical patients, aligning with contemporary enhanced recovery after surgery (ERAS) principles foundational to healthcare sustainability.12,13
The exploratory analysis using the SBI identified significant disparities in resource consumption across funding channels. The SBI of 1.28 for government-funded cases (Mean LOS 8.31 days) compared to the commercial sector (SBI 0.83) indicates that public-sector hospitalization duration is 28% higher than the institutional average. This observed “implementation gap” aligns with findings by Aliyeva et al (2025), who reported significant disparities in healthcare satisfaction and delivery patterns between insured and uninsured populations in Almaty, suggesting that financing models are a primary determinant of health system performance and resource distribution in the region.14
While these results suggest that reimbursement models predicated on bed-day occupancy may inadvertently disincentivize rapid discharge, they should be interpreted with caution. Potential confounders, such as differences in patient comorbidity burden, social support factors, and administrative referral patterns between government and private sectors, were not fully adjusted for in this analysis. Nevertheless, the data support the ongoing transition in Kazakhstan toward outcome-based surgical packages to better align financial incentives with clinical recovery milestones.15,16
Regarding clinical safety, the absence of recurrence in the TEP and TIPP cohorts over the 12-month follow-up period reflects the technical standardization of preperitoneal mesh placement.17 However, we acknowledge that a 12-month horizon is insufficient to definitively establish long-term recurrence rates. Laparo-endoscopic proficiency also provides a technical foundation for managing future surgical complexity, such as chronic pain or complex mesh issues, which are increasingly managed through minimally invasive salvage procedures.13,18 The successful adoption of these techniques in Kazakhstan is contingent upon a professional culture of clinical accountability and the ongoing modernization of institutional protocols.19
Limitations
Several limitations must be acknowledged. First, the study was conducted at a single medical center in Almaty, which may limit the generalizability of the findings to rural or lower-tier healthcare facilities in Kazakhstan. Second, the hybrid prospective–retrospective design and non-randomized patient allocation introduce the risk of selection bias, although we utilized propensity score matching to mitigate this. Third, the study was not powered to detect significant differences in rare outcomes, such as long-term recurrence or chronic mesh infection. Finally, the (SBI) is an exploratory indicator developed for this study; it has not been externally validated and should be treated as a descriptive normalization of LOS rather than a definitive performance metric.
Conclusion
This study demonstrates that laparo-endoscopic TEP and open preperitoneal TIPP techniques provide superior functional outcomes and higher patient satisfaction compared to the Lichtenstein open repair in a transition-economy setting. Beyond individual clinical benefits, these techniques facilitate significant reductions in hospital bed-day consumption.
The findings highlight an “implementation gap” between international clinical evidence and local institutional resource utilization, particularly within government-funded sectors.20 The exploratory SBI identifies public-sector resource turnover as a primary target for institutional reform. To achieve the theoretical gains in hospital throughput, healthcare policy should prioritize a shift from reimbursement logic based on bed-day occupancy toward value-based care models. Standardizing minimally invasive inguinal hernia repair is a key strategy for optimizing institutional capacity and improving the socio-economic efficiency of surgical services in Kazakhstan.
Institutional Review Board Statement
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The Ethics Committee of Kazakhstan’s Medical University, “Kazakhstan School of Public Health” (Almaty, Kazakhstan), approved the study before its commencement (approval number: A114; approved on 20 December 2019).
Informed Consent Statement
Informed consent was obtained electronically from all participants before participation in the study.
Abbreviations
IHR, Inguinal Hernia Repair; MIS, Minimally Invasive Surgery; TEP, Totally Extraperitoneal (Laparoscopic); TAPP, Transabdominal Preperitoneal (Laparoscopic); TIPP, Transinguinal Preperitoneal (Open); QoL, Quality of Life; EuraHS-QoL, European Registry for Abdominal Wall Hernias Quality of Life; QALY, Quality-Adjusted Life Year; ICER, Incremental Cost-Effectiveness Ratio; WTP, Willingness-to-Pay; SBI, System Burden Index; LOS, Length of Stay; CSHI, Compulsory Social Health Insurance (Kazakhstan Context); OR, Odds Ratio; CI, Confidence Interval; SD, Standard Deviation; PROM, Patient-Reported Outcome Measure; JCI, Joint Commission International.
Data Sharing Statement
The data assessed and reported in this study are available from the corresponding author upon reasonable request, adhering to ethical and privacy principles.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Stabilini C, van Veenendaal N, Aasvang E, et al. Update of the international HerniaSurge guidelines for groin hernia management. BJS Open. 2023;7(5):zrad080. doi:10.1093/bjsopen/zrad080
2. HerniaSurge Group. International guidelines for groin hernia management. Hernia. 2018;22(1):1–9.
3. Liu J, Shen J, Liu N, et al. Comparison of open and laparoscopic preperitoneal tension-free repair of groin hernia: a prospective nonrandomized controlled study. Surg Endosc. 2025;39(9):5889–5898. doi:10.1007/s00464-025-11913-z
4. Yilmaz AH, Ulutas ME. A retrospective comparative study of the enhanced view-totally extraperitoneal technique versus the traditional totally extraperitoneal technique in managing recurrent inguinal hernias. BMC Surg. 2025;25(1):355. doi:10.1186/s12893-025-03105-2
5. World Health Organization. Health systems in action: kazakhstan: 2022 edition [Internet] 2020. Available online: https://www.who.int/europe/publications/i/item/9789289059145.
6. Damaskos C, Garmpis N, Lamprinos D, et al. Surgery on the road to the land of promise–ιmpact of the refugee crisis on the greek healthcare system: results from a surgical department of a tertiary hospital. Healthcare. 2025;13(9):975. doi:10.3390/healthcare13090975
7. Sharma P, Boyers D, Scott N, et al. 2015; The clinical effectiveness and cost-effectiveness of open mesh repairs. HTA. 19(92). https://www.ncbi.nlm.nih.gov/books/NBK326920/.
8. Chen J, Zheng Y, Lin C. Comparison of short- and long-term efficacy and economic indicators between transabdominal preperitoneal and open tension-free repair for inguinal hernia in adults: a meta-analysis of randomized controlled trials. Hernia. 2025;29(1:248. doi:10.1007/s10029-025-03435-3
9. Kulkarni M, Dongre P. Determining efficacy of inpatient care for select surgeries at a large tertiary care hospital with average length of stay as a measure. Hosp Top. 2023;101(1):48–53. doi:10.1080/00185868.2022.2097972
10. Campbell JA, Hensher M, Davies D, et al. Long-term inpatient hospital utilisation and costs (2007-2008 to 2015-2016) for publicly waitlisted bariatric surgery patients in an Australian public hospital system based on australia’s activity-based funding model. Pharmacoecon Open. 2019;3(4):599–618. doi:10.1007/s41669-019-0140-5
11. Pogorelić Z, Ljubić N, Rađa M, Mrklić I, Vidović S. Parental satisfaction after pediatric inguinal hernia repair: day surgery versus conventional hospitalization. Healthcare. 2025;13(23):3088. doi:10.3390/healthcare13233088
12. Lloyd M, Ademi Z, Harris IA, et al. Implementing an enhanced recovery from surgery pathway to reduce hospital length of stay for primary hip or knee arthroplasty: a budget impact analysis. BMC Health Serv Res. 2024;24(1):1540. doi:10.1186/s12913-024-11871-7
13. Posthuma JJ, Sandkuyl R, Sloothaak DA, et al. Transinguinal preperitoneal (TIPP) vs endoscopic total extraperitoneal (TEP) procedure in unilateral inguinal hernia repair: a randomized controlled trial. Hernia. 2023;27(1):119–125. doi:10.1007/s10029-022-02651-5
14. Aliyeva S, Lokshin V, Kamaliev M, Sarmuldayeva S, Kaldybayev G, Tsigengagel O. Exploring disparities in satisfaction with obstetric-gynecological care among insured and uninsured women in Almaty, Kazakhstan: a comparative cross-sectional study. Front Glob Womens Health. 2025;6:1580888. doi:10.3389/fgwh.2025.1580888
15. Hurel R, Bouazzi L, Barbe C, et al. Lichtenstein versus TIPP versus TAPP versus TEP for primary inguinal hernia, a matched propensity score study on the French Club Hernie Registry. Hernia. 2023;27(5):1165–1177. doi:10.1007/s10029-023-02737-8
16. Bökkerink WJV, Koning GG, Vriens PWHE, et al. Open preperitoneal inguinal Hernia repair, TREPP versus TIPP in a randomized clinical trial. Ann Surg. 2021;274(5):698–704. doi:10.1097/SLA.0000000000005130
17. Sanderson R, DE-Marchi DD, Cesário JCB, Sanderson LGD, Zilberstein B. quality of life using eurahs-qol scores after surgical treatment of inguinal hernia: laparoscopic transabdominal preperitoneal (tapp) and lichtenstein techniques. Arq Bras Cir Dig. 2024;37:e1798. doi:10.1590/0102-672020240005e1798
18. Özveri E, Gök H, Tekcan Sanli DE, Ertem M. Laparoscopic mesh removal in inguinal hernia surgery: evaluating patient satisfaction and surgical outcomes. Hernia. 2025;30(1:5. doi:10.1007/s10029-025-03496-4
19. Alchimbayeva M, Glushkova N, Mammadov V, et al. The intention to disclose medical errors among health professionals in Kazakhstan. Int J Healthcare Manage. 2024;17(2):409–415. doi:10.1080/20479700.2023.2190635
20. Tigora A, Radu PA, Garofil DN, et al. Modern perspectives on inguinal Hernia repair: a narrative review on surgical techniques, mesh selection and fixation strategies. J Clin Med. 2025;14(14):4875. doi:10.3390/jcm14144875
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.