")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Health-Related Quality of Life Among Type 2 Diabetes Mellitus Patients Using the 36-Item Short Form Health Survey (SF-36) in Central Ethiopia: A Multicenter Study
Authors Esubalew H , Belachew A, Seid Y , Wondmagegn H , Temesgen K , Ayele T
Received 20 November 2023
Accepted for publication 27 February 2024
Published 29 February 2024 Volume 2024:17 Pages 1039—1049
DOI https://doi.org/10.2147/DMSO.S448950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Habtamu Esubalew,1 Ayele Belachew,2 Yimer Seid,2 Habtamu Wondmagegn,3 Kidus Temesgen,1 Tsegazeab Ayele3
1School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 2School of Public Health, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Human Anatomy, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Habtamu Esubalew, School of Public Health, College of Medicine and Health Sciences, Arba Minch University, P.O. Box 21, Arba Minch, Ethiopia, Tel +251 931547322, Email [email protected]
Introduction: Diabetes, one of the major global health emergencies of the 21st century, can affect a patient’s quality of life. A compromised quality of life has adverse effects on self-care practices, resulting in inadequate glycemic control and an increased susceptibility to complications. In Ethiopia, there is a paucity of information regarding the quality of life of patients with type 2 diabetes mellitus. Therefore, this study aimed to assess health-related quality of life in type 2 diabetes mellitus patients.
Methods: A cross-sectional study was conducted among type 2 diabetes mellitus patients attending diabetes follow-up clinics in selected public hospitals in Addis Ababa using short form- 36 (SF-36) health survey measures. Descriptive statistics were used to summarize the characteristics of the study participants. Simple and multiple linear regressions were done to identify significantly associated factors with health-related quality of life.
Result: A total of 309 patients participated in this study. The mean scores of the physical and mental component summaries were 40.15 (SD = 7.27) and 48.11 (SD = 8.87), respectively. Being old, being overweight or obese, living with type 2 diabetes mellitus for more than fifteen years, taking combined medication, having diabetes-related complications, and having comorbidities were factors that reduced the mean score of the physical component summary (p-value< 0.05). Being obese and diabetes related complication were factors that negatively affect mental component summary (p-value < 0.05). On the other hand, being married was factors that positively affect mental component summary (p-value < 0.05).
Conclusion: Older age, being married, obesity, overweight, longer duration of diabetes, using combined medications, diabetic-related complications, and co-morbidities were factors associated with health-related quality of life. Healthcare providers should strengthen counseling patients on lifestyle modifications such as diet modifications, and weight reduction.
Keywords: health-related quality of life, type 2 diabetes mellitus, short-form-36 health survey
Introduction
Diabetes is a serious chronic disease that occurs either when the pancreas does not produce enough insulin (a hormone that regulates blood glucose) or when the body cannot effectively use the insulin it produces.1 By 2011, the world leaders recognized diabetes mellitus (DM) as an important cause of premature death and disability, and it is one of four priorities non-communicable disease (NCD) in the prevention and control of NCD.2
According to the 2021 International Diabetic Federation (IDF) report, 537 million people worldwide, or 10.5% of the adult population (20–79 years), are estimated to have diabetes, with almost half unaware that they are living with the condition. This number is projected to reach 643 million by 2030, and 783 million by 2045.3 Type 2 diabetes mellitus (T2DM) accounts for more than 90% of cases worldwide.4 About three in four adults with diabetes live in low and middle-income countries, including Ethiopia. Diabetes accounted for 12.2% of global all-cause mortality among people aged between 20 and 79 years.3 A 2018 World Health Organization (WHO) country report estimated that the prevalence of diabetes mellitus in Ethiopia was 3.8%.5 A systematic review conducted in Ethiopia found that the prevalence of diabetes differed across the country, running from 0.3% at Debre Berhan Referral Hospital to 7.0% in Harar town.6
Diabetes is one of the major global health emergencies of the 21st century. Diabetes, if not well controlled, may cause blindness, kidney failure, lower limb amputation, and several other long-term consequences that impact significantly on the quality of life.7 Just as diabetes can affect a patient’s quality of life, a patient’s quality of life can affect their diabetes. A compromised quality of life has adverse effects on self-care practices, resulting in inadequate glycemic control and an increased susceptibility to complications.8 When patients experience overall satisfaction and well-being in their lives, including their life with diabetes, they are more motivated to effectively manage their diabetes. This increased self-care leads to improved day-to-day well-being and long-term health outcomes. The positive effects of feeling better and maintaining good health further enhance their quality of life.9,10 Therefore, a good quality of life activates a self-reinforcing positive cycle.4
WHO defines the quality of life as individuals’ “perception of their position in life in the context of the culture and value systems in which they live and about their goals, expectations, standards, and concerns”. It is a broad-ranging concept affected in a complex way by the person’s physical health, psychological state, personal beliefs, social relationships, and relationship to salient features of their environment.11 Health-related quality of life (HRQOL) measures make it possible to demonstrate scientifically the impact of health on quality of life, going well beyond the old paradigm that was limited to what can be seen under a microscope.12
HRQOL in T2DM patients is affected by socio-demographic and disease-related factors. According to previous studies, HRQOL is associated with sex, age, marital status, education, occupation, and income.13–17 Furthermore, HRQOL is associated with body mass index (BMI),15,18,19 hemoglobin A1c (HbA1c),20 duration of DM,21 treatment modality,16 diabetes complications22 and co-morbidities.19,23 Even though assessing HRQOL in T2DM patients is a critical contribution for decision-makers, policymakers, and clinicians, as well as in the improvement of guidelines, there is a paucity of studies regarding the quality of life of T2DM patients and its determinants using the SF-36 in Ethiopia, which is one of the top four African countries with the highest adult diabetic populations. As a result, the purpose of this study was to assess HRQOL and its determinants among type 2 diabetes patients attending diabetes follow-up clinics at public hospitals in Addis Ababa.
Methods and Materials
Study Design and Study Area
Institution-based multi-center cross-sectional study design was implemented. The study was conducted at three randomly selected public hospitals located in Addis Ababa, namely Tikur Anbessa Specialized Hospital (TASH), St. Paul’s Millennium Medical College, and Yekatit 12 Hospital.
Study Participants
The study population was all patients with T2DM in Addis Ababa who were attending the diabetes follow-up clinic of selected public hospitals during the study period and fulfilled the inclusion criteria. The study units were individuals with a diagnosis of T2DM.
Inclusion Criteria
Patients who have had T2DM for at least one year, who are at least 18 years old and who are willing to participate in the study, were included in the study.
Exclusion Criteria
Patients diagnosed with T2DM but who were seriously ill during the data collection or cognitively impaired were excluded from the study.
Sample Size Determination and Sampling Procedures
The sample size was determined using a single population mean formula (n = z2σ2/d2), considering a Z-value of 1.96 with a 95% confidence level, a margin of error of 5, and a standard deviation (43) taken from the previous study.24 By assuming a non-response rate of 10%, the final sample size we calculated was 313. We selected study hospitals using a simple random sampling method and proportionally allocated the sample to the selected hospitals. Finally, study participants were selected using a systematic random sampling technique from each hospital.
Data Collection Procedures
The data were collected by trained nurses through face-to-face interviews with structured questionnaires. Information regarding sex, age, marital status, religion, education, occupation, and income were obtained using a socio-demographic questionnaire. BMI (kg/m2) was determined by dividing the weight (kg) by the height (m) squared. The weight and height of the patients were measured using standardized height and weight measurements for adults. Data on diabetes-related conditions and medications (duration of diabetes, HbA1c, treatment modality, diabetes-related complications, and co-morbidities) were collected using questions adopted from the literature22–24 and the patient’s medical records. Information regarding HRQOL was collected through face-to-face interviews using an SF-36 health survey.
Measurement
We used a validated Amharic version of the short form-36 (SF-36) questionnaire to measure HRQOL in T2DM patients.25 The short form 36- (SF-36) health survey is one of the standard, short, and practical evaluation tools used to measure HRQOL, and it possesses good psychometric properties. The SF-36 health survey tool consists of 36 items that measure HRQOL in the past four weeks in eight domains, namely: physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH). All responses were re-coded to a linear 0–100 scale, with higher scores (scores approaching 100) indicating better HRQOL.26 The two summary scores —the “physical component summary” (PCS) and the “mental component summary” (MCS) —were calculated using the SF-36 physical and mental health summary scales user’s manual.27
Data Processing and Statistical Analysis
The data were entered in EpiData version 3.1, and analysis was done using SPSS version 25. The characteristics of the study population were described using descriptive statistics. The determinate factors for the two summary measures (PCS and MCS) were determined using the linear regression model. Before analysis, the fulfillment of assumptions for linear regression was checked. The diagnostic tests conducted on the data indicated that the assumptions necessary for regression analysis have been met. The plot of standardized residuals versus standardized predicted values displayed no discernible funneling, suggesting homoscedasticity. Additionally, the P-P plot revealed that the dots were closely aligned with the diagonal line, indicating conformity to normality assumptions. Multicollinearity was assessed through collinearity statistics, which demonstrated no significant multicollinearity among independent variables, as evidenced by VIF scores below 4 and tolerance scores above 0.1. P-values less than 0.25 in simple linear regression were used as a cutoff point for selecting independent variables that have to be eligible for multiple linear regressions. A p-value less than 0.05 in the multiple linear regression analysis was considered an independently associated factor for health-related quality of life.
Results
Socio-Demographic Characteristics
Of the 313 participants who were approached in the study, four potential respondents refused to participate in the study, and 309 participants were interviewed, which makes the response rate 98.7%. One hundred and eighty-two (58.9%) were females, and the mean age of participants was 52.28 (SD=12.9) years. Two hundred and ten (68%) were married, and two hundred and forty-three (78.6%) were orthodox Christians. One hundred and six (34.3%) attended secondary school, and ninety-nine (32%) were housewives. The mean monthly income in ETB was 3027.57 (SD=2818.08). The mean BMI was 25.85 (SD=3.77) (Table 1).
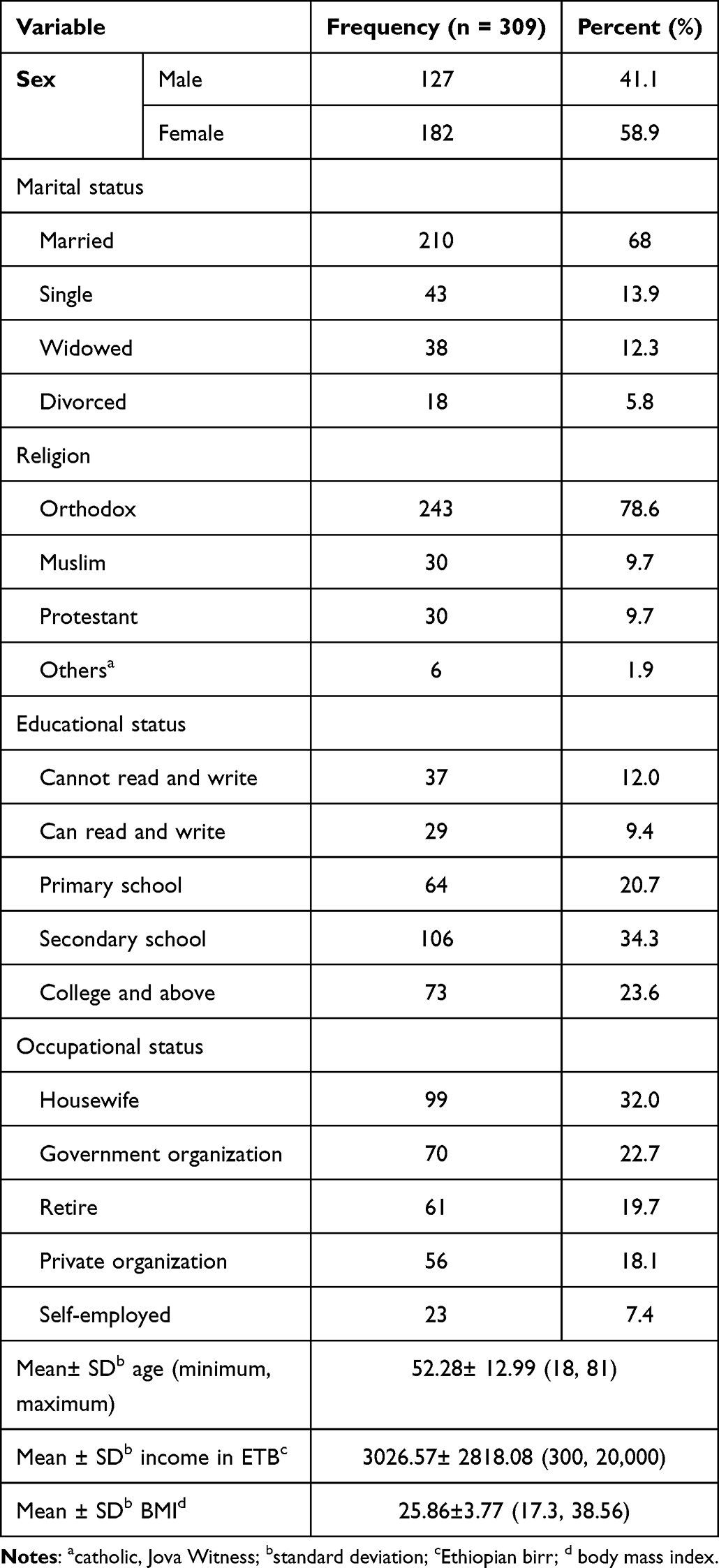 |
Table 1 Socio-Demographic Characteristics of Study Participants in Selected Public Hospitals, Addis Ababa, Ethiopia |
Diabetes-Related Characteristics of Type 2 Diabetes Patients
The mean duration of T2DM illness since diagnosis was 10.17 (SD = 7.88) years, and one hundred and twenty-nine (41.7%) used oral anti-diabetic medication. The mean levels of HbA1c and cholesterol were 8.42% (SD = 1.9) and 188.27 mg/dl (SD = 48.01), respectively. Ninety-two patients (30.1%) developed one or more complications. Of the complications recorded, the most frequent was peripheral neuropathy, which occurred in forty-two patients (13.6%), followed by retinopathy in forty-one patients (13.3%), nephropathy in twenty-six patients (8.4%), and diabetic foot ulcers in nine patients (2.9%). One hundred and seventy-nine patients (57.9%) presented with co-morbidity. Of the co-morbidities, the most frequent was hypertension, which was recorded in one hundred and fifty-seven patients (49.5%) (Table 2).
 |
Table 2 Diabetes-Related Characteristics of Study Participants in Selected Public Hospitals, Addis Ababa, Ethiopia |
Levels of Health-Related Quality of Life (HRQOL) of the Study Participants
Among the domains of the SF-36 health survey, the domain with the highest mean score was mental health functioning, with a mean and standard deviation of 72.7 (SD = 15.13), followed by social functioning (M = 64.52 (SD = 19.22)) and role emotional (M = 61.60 (SD = 29.29). The domain with the lowest score was role-playing, with a mean score of 52.91 (SD = 24.33). In addition, the mean scores for the physical component summary (PCS) and the mental component summary (MCS) were 40.15 (SD = 7.27) and 48.11 (SD = 8.87), respectively (Table 3).
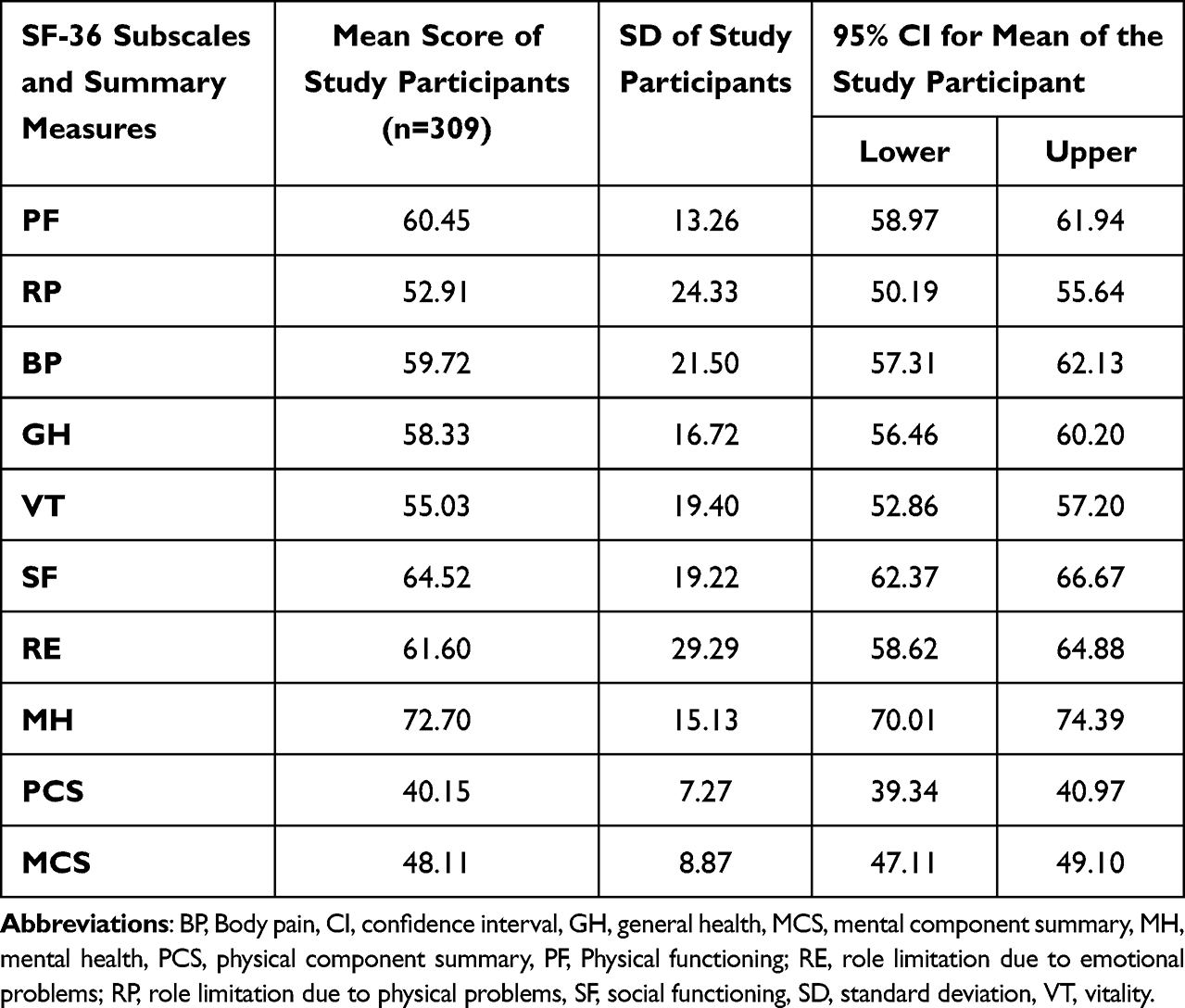 |
Table 3 Mean Scores for the Eight SF-36 Domains and the Two Summary Measures (PCS and MCS) of the Study Participants |
Factors Associated with PCS and MCS
Multiple linear regression results indicated that being old, being overweight or obese, living with T2DM for more than fifteen years, taking combined medication, having one or more T2DM-related complications, and having comorbidities were significantly associated factors that reduced the mean score of PCS (p-value<0.05). Patients who are living with one or more comorbidities had significantly lower mean scores in MCS compared to those patients without co-morbidities (p<0.05). On the other hand, married T2DM patients had a good mean score in the MCS compared to those patients who were single (p<0.05) (Table 4).
 |
Table 4 Regression Coefficients of the Determinate Factors for Summary Measures of SF-36 Resulted from Multiple Linear Regressions in Addis Ababa, Ethiopia |
Discussion
Health-related quality of life is important in many aspects for diabetes patients and healthcare providers. This study aimed to assess the level of health-related quality of life and its determinants among T2DM patients and factors associated with HRQOL. We found that the age of the patients, marital status, educational status, BMI, duration of diabetes, treatment modality, diabetic-related complications, and co-morbidities were independent factors significantly associated with one or more domains of SF-36 and the two summary measures (PCS and MCS) of HRQOL.
In the current study, we found lower mean scores in almost all domains of the SF-36 health survey, except in MH. Contrary to our findings, the result of a study conducted in the Netherlands showed higher mean scores in all domains of SF-36.28 A study conducted in Greece with the same tool also reported higher scores in most of the domains of SF-36 (PF, RP, BP, VT, SF, and RE).13 The lower scores observed in our study may be attributed to the participants’ lower educational status, leading to inadequate self-discipline in terms of diet and physical activity. Additionally, the provision of substandard health care services for patients might have resulted in the early development of complications. Furthermore, socio-demographic factors could also contribute to the observed differences.
In our study, we found mean scores of 40.15 and 48.11 for PCS and MCS, respectively. In contrast to our findings, studies conducted in China and Romania found higher mean scores in the two summary measures.18,19,29 This difference might be observed due to differences in socio-demographic characteristics, access to healthcare resource, including medications and regular medical check-ups, and access to education and support programs.
However, the result from our study showed higher scores in six domains of SF-36 (such as PF, RP, BP, GH, RE, and MH) and the MCS when we compared it to a study conducted in Ethiopia among T2DM patients with peripheral neuropathic pain.24 The reason why we observed higher scores in most SF-36 domains in the current study might be the difference in the study population, which means they include patients with peripheral neuropathic pain, which affects the patient’s quality of life.
We also tried to compare our findings with a study conducted in Butajira, rural Ethiopia, among general populations, and we observed lower scores in all domains (except MH) and two summary measures among T2DM patients.25 This difference might be observed due to the risk of developing or the presence of long-term complications, the presence of other chronic disease conditions, the burden of diabetes medications, the psychosocial toll of living with diabetes that can affect self-care behavior, and glycemic control among diabetic patients. In addition, the reason for lower scores might be because there is a higher proportion of the elderly in our study.
We found a significant association between age and the PCS measure. In line with this, other studies conducted in China18 and Ethiopia24 found a significant association between age and the PCS measure. The reason why elders have a lower score in the PCS measure might be because elders are at risk of developing complications and may have co-morbid diseases like hypertension and dyslipidemia, economic difficulties, and hard living conditions. However, some studies reported no relationship between age and HRQOL among T2DM patients.13,15
Likewise, when we compared the relationship between marital status and HRQOL of the patients with T2DM, we found a higher score in MCS measures among married T2DM patients. Consistent with our findings, a study conducted in China found single patients scored a lower mean in the MCS measure compared to married subjects.18 The justification for this might be happening because of the point of view of society toward single individuals, a lack of social support, and living alone. However, another study showed no association between the two summary measures and marital status.24
BMI was another factor that was significantly associated with PCS and MCS. We found that the PCS mean scores of overweight and obese patients were significantly lower than those patients with a normal BMI. Obese patients had lower mean scores in the MCS compared to those patients with normal BMI. A study conducted in China showed a negative relationship between BMI and PCS score which is consistent with our findings.18 The suggestions for this might be that overweight or obese patients may have difficulty with daily physical functioning due to shortness of breath, pain of the weight-bearing joints, low energy level or reduced mobility, and presence of psychological concerns such as low self-esteem and disturbance of body image.
Patients who have been living with T2DM for more than 15 years have worsened HRQOL than those who were living with it for 5 years or less. Similar findings were reported in studies conducted in Turkey and Mexico.15,21 The justification for this might be that when patients live with the illness for a long time, they might start to develop complications and may have other co-morbidities that add stress to the management and control of their blood glucose level. This leads to a poor quality of life.
The type of medication the patients use to control blood glucose levels affects their health-related quality of life. In the current study, we found that patients who used combined medication had lower mean scores in the PCS measures. In consistence with our findings, other studies also found a significant association between treatment modality and HRQOL.15,16 The suggestions for this might be that when the patients are on combined medication, their treatment adherence may be compromised, which leads to poor control of blood glucose and the development of a complication, which then affects their quality of life.
In the current study, we found that T2DM patients with any kind of diabetic-related complication have a lower HRQOL than those with T2DM with no complications. In line with our findings, diabetic-related complications have been shown to have a significant association with HRQOL in other studies.15,17,24 Another study also showed a relationship between diabetic microvascular complications such as peripheral neuropathy, nephropathy, retinopathy, and cardiovascular diseases and HRQOL.22 The suggestions for this might be because patients with diabetic-related complications have poor prognoses or disease outcomes, use various treatments, and have new signs and symptoms or pathological changes that affect their quality of life.
Co-morbidities impose a negative effect on the HRQOL of T2DM patients. The current study showed that co-morbidities were significantly associated with the PCS measures. Consistent with our findings, studies conducted in the Netherlands and China found that the presence of co-morbidities has a negative association with HRQOL.18,23 The suggestions for this might be the presence of co-morbidities leading to a high pill burden, increased morbidity, and poor outcomes, which end up with a low health-related quality of life. The limitations of this study were that we assessed patients’ HRQOL using a generic instrument, not a disease-specific one, and we used a cross-sectional study design because, due to its nature, it shows an association, not a causal relationship.
Conclusion
In conclusion, the result of this study indicated that the HRQOL of T2DM patients was low. Old age, being overweight or obese, longer duration of T2DM, taking combined medication, the presence of diabetic-related complications, and the presence of co-morbidities were significantly associated factors that negatively affected the PCS measure. On the other hand, being obese and the presence of diabetic-related complications were significantly associated factors that negatively affected the MCS measure, and being married was a significantly associated factor that positively related to the MCS measure. Understanding the effect of diabetes on HRQOL is important for day-to-day clinical management to improve the HRQOL and health outcomes of those with diabetes. Therefore, healthcare providers should strengthen the provision of information and/or counseling for patients about lifestyle modifications such as diet modification, weight reduction, and physical exercise.
Abbreviations
BMI, body mass index; BP, body pain; CI, confidence interval; DM, diabetes mellitus; GH, general health perceptions; HRQOL, Health-Related Quality of Life; MCS, mental component summary; MH, mental health; PCS, physical component summary; PF, physical functioning; RE, role limitations due to emotional problems; RP, role limitations due to physical health problems; T2DM, type 2 diabetes mellitus.
Data Sharing Statement
The data that support the findings of this study are not openly available and are available from the corresponding author upon reasonable request.
Ethical Approval
Before starting the study, Ethical approval has been obtained from the Institutional Review Board (IRB) of the Addis Ababa University, College of Health Sciences, St. Paul’s Hospital Millennium Medical College, Tikur Anbessa Specialized Hospital and Addis Ababa Public Health Research and Emergency Management Directorate. All procedures have been conducted following the principles stated in the Declaration of Helsinki. The study’s objectives and purposes were explained to the study’s participants. All data collected during the study were handled with the utmost confidentiality. Participants were informed that their participation in the study was completely voluntary and they can withdraw from the study anytime they want. Prior to the interview, written informed consent was taken from each study participant.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We are thankful to Addis Ababa University, data collectors, supervisors, study participants, Tikur Anbessa Specialized Hospital, St Paul’s Millennium Medical College, and Yekatit 12 Hospital directors and staff for their cooperation. This paper is based on the thesis of Habtamu Esubalew. The original thesis was not peer reviewed and has only been published in Addis Ababa University institutional repository for thesis.30
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, stud design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alberti KGMM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabetic Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
2. World Health Organization. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. New York: 66th Session of the Unites Nations General Assembly, WHO; 2011.
3. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
4. Roglic G. WHO Global report on diabetes: a summary. Int J Noncommunicable Dis. 2016;1(1):3. doi:10.4103/2468-8827.184853
5. World Health Organization. Diabetes Country Profiles, 2016. Diabetes [Internet]. 2016.
6. Abebe N, Kebede T, Addise D. Diabetes in Ethiopia 2000–2016 prevalence and related acute and chronic complications; a systematic review. Afr J Diabetes Med. 2017;25(2):7–12.
7. Saeedi P, Salpea P, Karuranga S, et al. Mortality attributable to diabetes in 20–79 years old adults, 2019 estimates: results from the International Diabetes Federation Diabetes Atlas. Diabetes Res Clin Pract. 2020;162:108086. doi:10.1016/j.diabres.2020.108086
8. Garratt AM, Schmidt L, Fitzpatrick R. Patient-assessed health outcome measures for diabetes: a structured review. Diabet Med. 2002;19(1):1–11. doi:10.1046/j.1464-5491.2002.00650.x
9. Fadli A. The Impact of Self-Management-Based Care Interventions on Quality of Life in Type 2 Diabetes Mellitus Patients: a Philosophical Perspective. med Rxiv. 2022;
10. Malini H, et al. Self-Care And Quality of Life People With Type 2 Diabetes During the Covid-19: cross-Sectional Study. J Diabetes Metab Disord. 2022;21(1):785–790.
11. Group W. The development of the World Health Organization quality of life assessment instrument (the WHOQOL). In: Quality of Life Assessment: International Perspectives. Springer; 1994:41–57.
12. Taylor VR. Measuring healthy days; population assessment of health-related quality of life. 2000.
13. Papadopoulos AA, Kontodimopoulos N, Frydas A, et al. Predictors of health-related quality of life in type II diabetic patients in Greece. BMC Public Health. 2007;7(1):186. doi:10.1186/1471-2458-7-186
14. Mikailiūkštienė A, et al. Quality of life in relation to social and disease factors in patients with type 2 diabetes in Lithuania. Med Sci Monit. 2013;19:165–174. doi:10.12659/MSM.883823
15. Altınok A, Marakoğlu K, Kargın N. Evaluation of quality of life and depression levels in individuals with Type 2 diabetes. J Family Med Prim Care. 2016;5(2):302–308. doi:10.4103/2249-4863.192358
16. Al Hayek AA, Robert AA, Al Saeed A, et al. Factors Associated with Health-Related Quality of Life among Saudi Patients with Type 2 Diabetes Mellitus: a Cross-Sectional Survey. Diabetes Metab J. 2014;38(3):220–229. doi:10.4093/dmj.2014.38.3.220
17. Verma SK, Luo N, Subramaniam M, et al. Impact of depression on health related quality of life in patients with diabetes. Ann Acad Med Singap. 2010;39(12):913–917. doi:10.47102/annals-acadmedsg.V39N12p913
18. Wong CK, Lo YYC, Wong WHT, et al. The associations of body mass index with physical and mental aspects of health-related quality of life in Chinese patients with type 2 diabetes mellitus: results from a cross-sectional survey. Health Qual Life Outcomes. 2013;11(1):1–9. doi:10.1186/1477-7525-11-142
19. Rejeski WJ, Lang W, Neiberg RH, et al. Correlates of health‐related quality of life in overweight and obese adults with type 2 diabetes. Obesity. 2006;14(5):870–883. doi:10.1038/oby.2006.101
20. Qaseem A, Vijan S, Snow V, et al. Glycemic Control and Type 2 Diabetes Mellitus: the Optimal Hemoglobin A 1c Targets. A Guidance Statement from the American College of Physicians. Ann Intern Med. 2007;147(6):417–422. doi:10.7326/0003-4819-147-6-200709180-00012
21. Zurita-Cruz JN, Manuel-Apolinar L, Arellano-Flores ML, et al. Health and quality of life outcomes impairment of quality of life in type 2 diabetes mellitus: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):94. doi:10.1186/s12955-018-0906-y
22. Quah JH, Luo N, Ng WY, et al. Health-related quality of life is associated with diabetic complications, but not with short-term diabetic control in primary care. Ann Acad Med Singap. 2011;40(6):276–286. doi:10.47102/annals-acadmedsg.V40N6p276
23. Adriaanse MC, Drewes HW, van der Heide I, et al. The impact of comorbid chronic conditions on quality of life in type 2 diabetes patients. Qual Life Res. 2016;25(1):175–182. doi:10.1007/s11136-015-1061-0
24. Degu H, Wondimagegnehu A, Yifru YM, et al. Is health related quality of life influenced by diabetic neuropathic pain among type II diabetes mellitus patients in Ethiopia? PLoS One. 2019;14(2):e0211449. doi:10.1371/journal.pone.0211449
25. Kebede D, Alem A, Shibre T, et al. Health related quality of life (SF-36) survey in Butajira, rural Ethiopia: normative data and evaluation of reliability and validity. Ethiop Med J. 2004;42(4):289–297.
26. Ware JE. SF-36 Health Survey: Manual and Interpretation Guide. Health Institute; 1993.
27. Ware J, Kosinski M, Keller S, SF-36 physical and mental health summary scales. A user’s manual, 2001; 1994.
28. Verhulst MJ, Teeuw W, Gerdes V, et al. Self-reported oral health and quality of life in patients with type 2 diabetes mellitus in primary care: a multi-center cross-sectional study. Dia meta synd Obesi. 2019;12:883. doi:10.2147/DMSO.S207087
29. Grigorescu ED, Lăcătușu C-M, Crețu I, et al. Self-Reported Satisfaction to Treatment, Quality of Life and General Health of Type 2 Diabetes Patients with Inadequate Glycemic Control from North-Eastern Romania. Int J Environ Res Public Health. 2021;18(6):3249. doi:10.3390/ijerph18063249
30. Esubalew H. Assessment of Health-Related Quality of Life and Its Determinants Among Type II Diabetes Mellitus Patients in Selected Public Hospitals of Addis Ababa, Ethiopia. Addis Ababa University; 2021. orginal.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.