Back to Journals » Clinical Interventions in Aging » Volume 18
Frequency and Correlates of Multimorbidity Among the Oldest Old: Study Findings from the Representative “Survey on Quality of Life and Subjective Well-Being of the Very Old in North Rhine-Westphalia (NRW80+)”
Received 3 September 2022
Accepted for publication 14 December 2022
Published 11 January 2023 Volume 2023:18 Pages 41—48
DOI https://doi.org/10.2147/CIA.S388469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
André Hajek, Hans-Helmut König
Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Hamburg Center for Health Economics, Hamburg, Germany
Correspondence: André Hajek, Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Martinistr. 52, Hamburg, 20246, Germany, Tel +49 40 7410 52877, Fax +49 40 7410-40261, Email [email protected]
Purpose: Our aim was to clarify the frequency and correlates of multimorbidity among the oldest old.
Patients and Methods: We used data from the representative “Survey on quality of life and subjective well-being of the very old in North Rhine-Westphalia (NRW80+)” covering participants ≥ 80 years living in private households and in institutionalized settings in North Rhine-Westphalia (n = 1484, mean age was 86.3 years). Multimorbidity is defined as the co-occurrence of at least two chronic conditions. Sociodemographic, lifestyle-related, and health-related (including health literacy) correlates were included in regression analysis.
Results: About 79% of the participants were multimorbid. Logistic regressions showed that the likelihood of multimorbidity significantly increased with living in a private household, having a larger network size, worse self-rated health, higher functional impairment, and more depressive symptoms, whereas the remaining sociodemographic and lifestyle-related factors as well as health literacy were not significantly associated with multimorbidity.
Conclusion: A large proportion of participants in very late life is multimorbid. Apart from health-related factors, also two sociodemographic factors (ie, living situation and network size) were associated with multimorbidity among the oldest old. This knowledge may help to identify individuals at risk for multimorbidity in very late life.
Keywords: 80 and over, depression, functional status, multimorbidity, multiple chronic conditions, health literacy, loneliness, social isolation, network size, technology, physical activity, institutionalization, nursing home
Introduction
There is a steady increase in the number of individuals in late life (particularly among the oldest old individuals aged 80 years and over). Since age is commonly associated with the number of chronic conditions, the number of individuals with multimorbidity (co-existence of at least two chronic conditions) is also expected to rise. For example, a systematic review stated that the prevalence of multimorbidity in late life varied from 55% to 98% among individuals aged 60 years and over.1 Only one2 of the studies mentioned in this former systematic review1 additionally focused on individuals aged 80 years and over and identified a prevalence of 74% among men and 80% in women in this age group (based on data from a general practice setting). In Europe, about 50 million individuals had multimorbidity.3 Additionally, multimorbidity is also a challenge in low- and middle-income countries.4
Multimorbidity is also an increasing challenge because it is associated with, eg, feelings of loneliness,5 higher pain,6 a high economic burden,7 nursing home admission8 and even mortality.9 For example, multimorbidity may affect loneliness by decreasing the quality of the relationships.5 Moreover, certain chronic conditions (eg, chronic low back problems combined with gout, chronic gastritis or cardiac insufficiency) can contribute to higher pain levels.10 Furthermore, multimorbidity commonly reflects an increased need for healthcare use (eg, GP visits11) – which refers to a high economic burden.7 Additionally, certain chronic conditions (such as stroke, Parkinson’s disease, hip fracture) as part of multimorbidity may drive the association between multimorbidity and nursing home admission as well as longevity.8
Moreover, multimorbidity is a risk factor of elder abuse/mistreatment12 and can contribute to low grip strength.13 Hence, it is important to identify the correlates of multimorbidity. This is of particular importance as various critical events take place in this age bracket (eg, marked decrease in health, feelings of isolation, admission to nursing or old age home). Therefore, studying the frequency and correlates of multimorbidity exclusively in this age bracket is important.
Most of the existing studies mainly examined the frequency and correlates of multimorbidity in older age (eg,14–19). For example, one of these studies by Sakib et al used baseline data from the Canadian Longitudinal Study on Aging (45–85 years) to investigate the correlates of multimorbidity using multiple logistic regressions.15 Another study by Zhang et al used data from the China Health and Retirement Longitudinal Study (CHARLS).19 Both studies showed that a higher likelihood of multimorbidity was significantly associated with, among other things, higher age, and being female, whereas one study showed that it was associated with lower education.19
However, there is a lack of knowledge regarding the frequency and correlates of multimorbidity exclusively among the oldest old – based on large, representative samples (and including individuals living in institutionalized settings). Thus, our aim was to fill this gap in our current knowledge. Our findings may be important to address individuals at increased risk of multimorbidity which in turn is important because it can contribute to successful ageing and longevity in late life.20
Materials and Methods
Sample
Data for our study were taken from the “Survey on quality of life and subjective well-being of the very old in North Rhine-Westphalia (NRW80+)”. In the most populous state in Germany (North Rhine-Westphalia), this study took place from August 2017 to February 2018. It is a representative sample of individuals ≥ 80 years in this state (with men and individuals aged 85 years and older being oversampled). More precisely, a multistage sampling design was applied. First, 120 sampling points were defined. These sampling points were located in 94 communities. It should be noted that communities that have a high proportion of individuals aged 80+ had multiple sampling points. In sum, 400 addresses were chosen at random from the population registries for each sampling point. Second, a sample of 8040 target individuals who were approached for an interview was chosen using a disproportionate sampling strategy with stratification by age groups (80–84, 85–89, and 90+ years) and gender. Fieldwork was carried out by the renowned company Kantar public.
Several topics were included in this study (eg, health-related factors, socioeconomic-factors). Main inclusion criteria were as follows: Having a registered main residence in this state (including both individuals in private households and individuals in institutionalized settings) and being 80 years or older. It should be noted that the response rate was 23.4%. Main reasons for non-participation were a lack of willingness to participate and the inability to participate for health reasons. However, the response rate should be put into perspective against the background of the age bracket of the participants (including participants in institutionalized settings), and a mean interview duration of about 90 minutes. Moreover, prior research has shown that, eg, gender, age group or living situation were not associated with the likelihood of non-response.21 As also stated by Kuppler and Wagner (referring to the response rate of the NRW 80+): “[…] a low response rate does not necessarily imply low representativeness of the sample”.22 Moreover, the response rate has to be seen in the light of the age bracket, the general low participation rate in Germany and the mean interview duration. Further details are given by Wagner et al.21
The sample consists of 1863 individuals (1687 self-report interviews and 176 proxy interviews). In our analytical sample, n equaled 1484 individuals due to missings.
The NRW80+ was approved by the ethics committee of the Medical Faculty of the University of Cologne (No. 17–169). Informed consent was obtained from all participants or their legal representatives.
Outcome: Multimorbidity
In accordance with a previous multimorbidity index,23 based on self-reports 19 chronic illnesses were assessed (for each illness: 0 = absence, 1 = presence): myocardial infarction, heart failure, hypertension, stroke, mental illness, cancer, diabetes, respiratory or pulmonary disease, back pain, gastric or intestinal disease, kidney disease, liver disease, blood disease, joint or bone disease, bladder disease, sleep disorder, eye disease or visual disorder, ear disease or hearing impairment, and neurological disease. Multimorbidity was defined as the co-occurrence of at least two of these aforementioned chronic illnesses.
Independent Variables
Based on previous research14–19 and theoretical considerations, independent variables were chosen. Several sociodemographic, lifestyle and health-related factors were included in regression analysis: sex, age, marital status (distinguishing between single; divorced; widowed; married, living together with spouse; married, living together with spouse), living situation (living in a private household; living in an institutionalized setting), the level of education (ISCED-9724 classification: low, medium or high), size of social network and loneliness (from 1= never/almost never to 4 = almost or almost always; with higher values corresponding to higher loneliness levels).
With regard to lifestyle-related factors, we included a score which counts the frequency of 16 activities (eg, sports, traveling, cinema, volunteering, or walks), ranging from 1 to 5 (with higher values corresponding to a higher frequency). Moreover, we included the number of technologies in use (based on six items, eg, computer/laptop, internet, smartphone; in each case: 0=no, 1=yes). By averaging the items, a score was calculated (higher values indicate a higher number of technologies in use).
With regard to health-related factors, we included: self-rated health (from 1 = very bad to 4 = very good), functional impairment, depressive symptoms and health literacy. A modified Lawton and Brody IADL scale (with seven items, each case: 0 = only possible with help to 2 = no help needed)25 was used to quantify functional impairment. The score was calculated by averaging the seven items (0–2, higher values indicating lower functional impairment).
The “depression in old age scale” (DIA-S)26,27 was used to assess depressive symptoms, consisting of four items (each case: no or yes). A sum score was calculated (ranging from 0 to 4, with higher values corresponding to more depressive symptoms). The DIA-S has favorable psychometric properties.26,27 By averaging two items, a score was used to quantify health literacy (from 1 to 4, higher values correspond to higher health literacy).
Statistical Analysis
In a first step, sample characteristics are shown stratified by the presence of multimorbidity (no or yes). Chi² tests or independent t-tests were conducted, as appropriate. Additionally, the frequency of multimorbidity is displayed stratified by age group. Moreover, effect sizes (Cohen’s d) were calculated. Thereafter, multiple binary logistic regressions were used to identify the correlates of multimorbidity. The statistical significance was defined as p value of ≤0.05. Stata 16.1 was used for statistical analyses (Stata Corp., College Station, Texas).
Results
Sample Characteristics
In Table 1, sample characteristics stratified by multimorbidity are given. In total, mean age was 86.3 years (SD: 4.5, ranging from 80 to 102 years) and about 49% were female. In sum, about 79% of the individuals were multimorbid. In bivariate analysis, multimorbidity was significantly associated with higher age, higher loneliness levels, both lifestyle factors (activities and technology usage), and all health-related factors (self-rated health, functional impairment, depressive symptoms, as well as health literacy). Further details are shown in Table 1. Furthermore, the frequency of multimorbidity is displayed stratified by age group (Table 2).
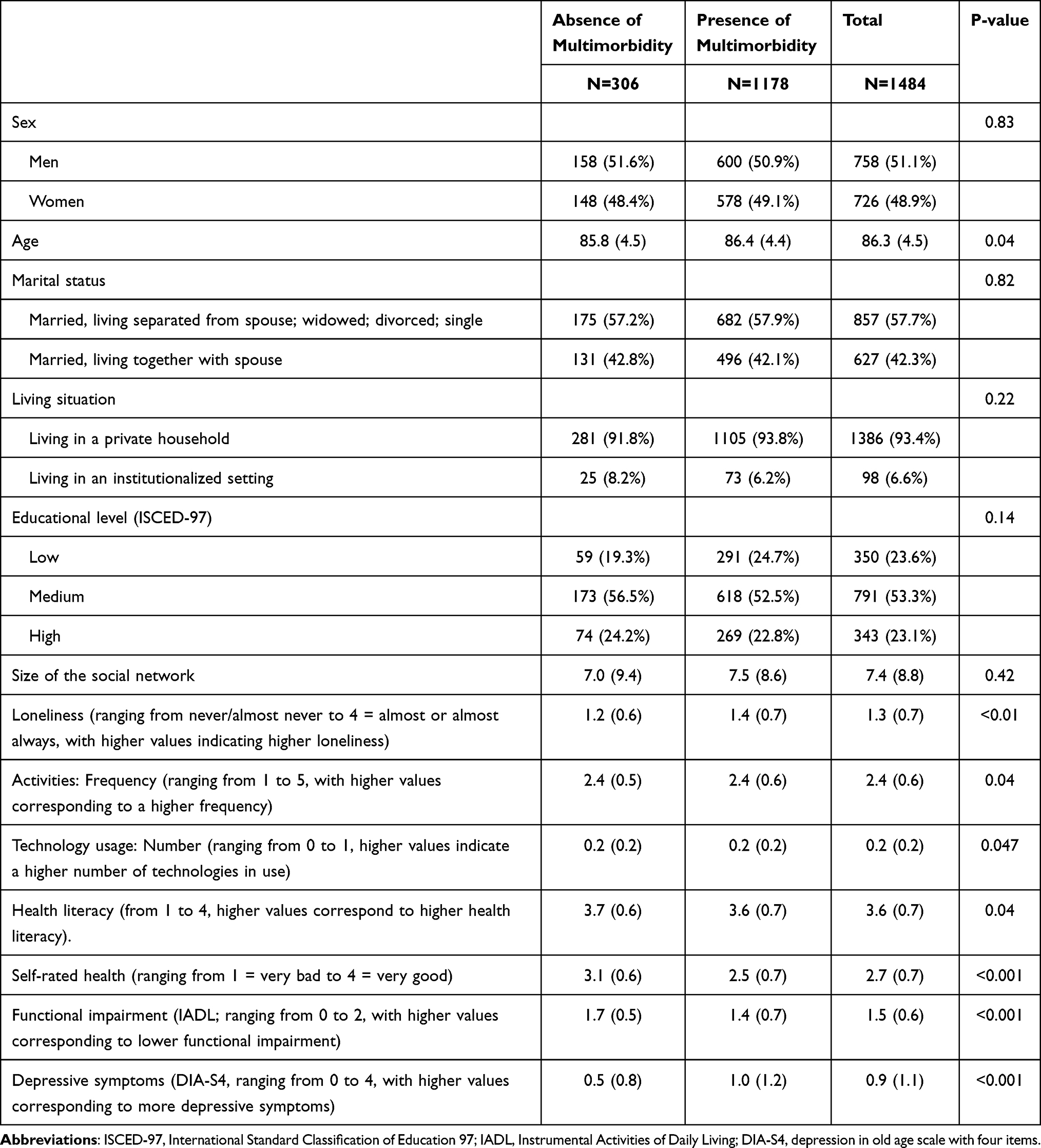 |
Table 1 Sample Characteristics (for the Analytical Sample), Stratified by Multimorbidity (n=1484) |
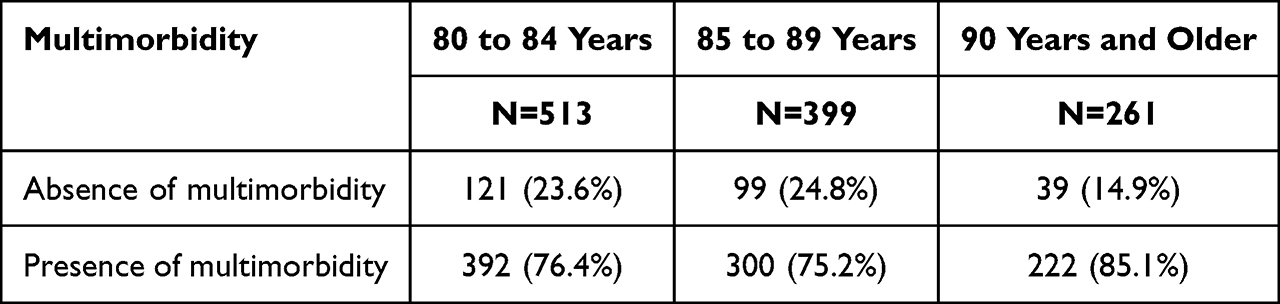 |
Table 2 Frequency of Multimorbidity (by Age Group) |
Comparably high effect sizes (according to Cohen’s d) were identified for the association between multimorbidity with self-rated health (d=0.76), functional impairment (d=0.50), and depressive symptoms (d=−0.51).
Regression Analysis
Results of logistic regressions are given in Table 3. Logistic regressions showed that the likelihood of multimorbidity significantly increased with living in a private household (OR: 0.39, 95% CI: 0.21–0.69), having a larger network size (OR: 1.02, 95% CI: 1.00–1.04), worse self-rated health (OR: 0.39, 95% CI: 0.31–0.49), higher functional impairment (OR: 0.40, 95% CI: 0.29–0.57), and more depressive symptoms (OR: 1.34, 95% CI: 1.12–1.59).
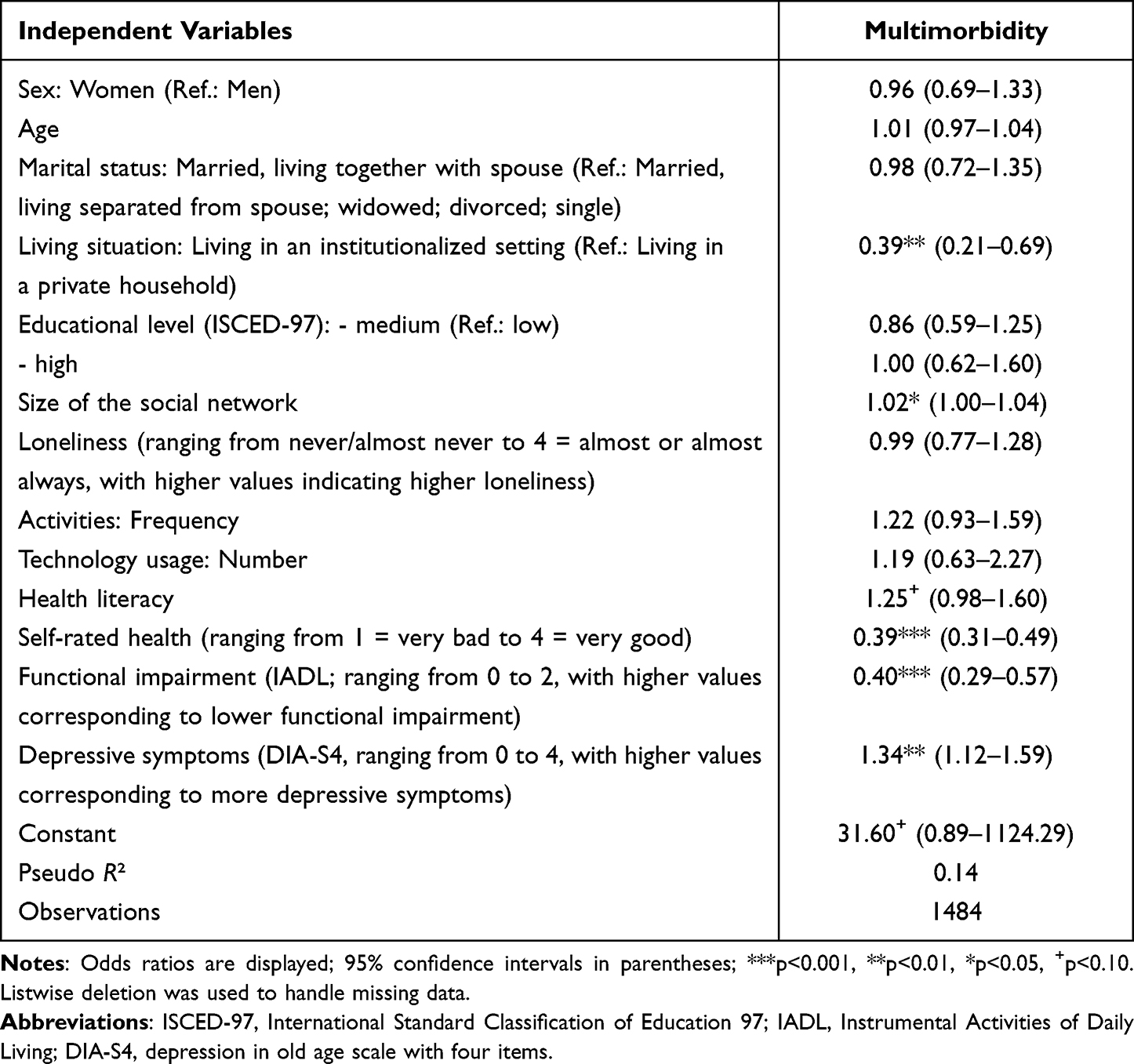 |
Table 3 Correlates of Multimorbidity. Results of Binary Logistic Regressions (0 = Absence of Multimorbidity, 1 = Presence of Multimorbidity) |
In contrast, sex, age, marital status, educational level, loneliness, activities, technology usage, and health literacy were not significantly associated with the likelihood of multimorbidity.
Because (particularly a high number of) depressive symptoms can reflect a mental illness, depressive symptoms were removed from the main regression model. These results are displayed in Table 4. In terms of effect size and significance, all findings remained nearly the same (compared to our main model). However, in this additional model, the association between health literacy and multimorbidity achieved statistical significance (OR: 1.28, 95% CI: 1.02–1.60; main model: 1.25, 95% CI: 0.98–1.60).
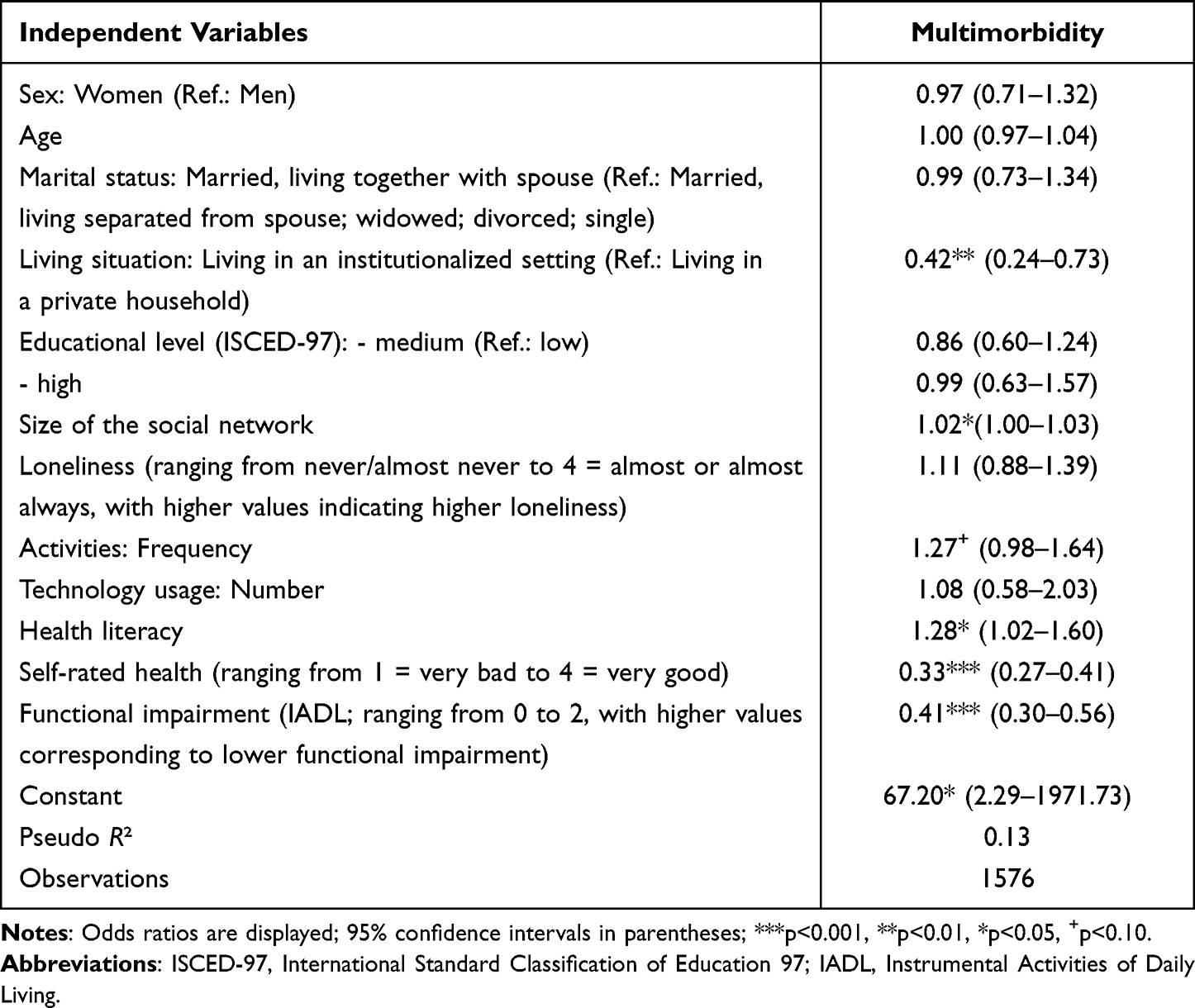 |
Table 4 Correlates of Multimorbidity. Results of Binary Logistic Regressions (0 = Absence of Multimorbidity, 1 = Presence of Multimorbidity) – without Depressive Symptoms as Independent Variable |
Discussion
Main Findings
The goal of our current study was to identify the frequency and correlates of multimorbidity in highest age using data from a large, representative sample. In total, 79% of the individuals were multimorbid. Regressions revealed that the likelihood of multimorbidity significantly increased with living in a private household, having a larger network size, worse self-rated health, higher functional impairment, and more depressive symptoms, whereas the remaining sociodemographic and lifestyle-related factors as well as health literacy were not significantly associated with multimorbidity. Based on (1) representative data exclusively from the (2) oldest old ((3) also covering individuals living in institutionalized settings) and using (4) valid tools, our study thus extends previous knowledge in multimorbidity research.
Previous Research and Possible Explanations
The association between a larger network size and a higher likelihood of multimorbidity which was found in our study may seem counterintuitive at first glance. However, it confirms previous research based on middle-aged and older adults in Germany.28,29 As stated by Kristensen et al,28,29 this association may reflect the fact that individuals with multimorbidity are in higher need of care and could therefore enlarge their social network. Previous qualitative research has also demonstrated that individuals with multimorbidity described their networks frequently as fulfilling and diverse.30
Our study showed that health-related factors (worse self-rated health, higher functional impairment, and more depressive symptoms) were significantly associated with multimorbidity among the oldest old. This appears very plausible and stresses the importance of health-related factors for multimorbidity. Furthermore, it is in accordance with previous research examining individuals in older age in China.19
Surprisingly, individuals living in private households have a higher likelihood of multimorbidity compared to individuals living in institutionalized settings. However, it should be noted that institutionalization is particularly associated with cognitive or functional impairment, but not increased chronic conditions in Germany.31,32 Oldest old individuals living in private households may suffer from social exclusion or may miss communication with others – particularly when living alone – as stated before.19 These factors could in turn lead to multimorbidity in Germany.5
Strengths and Limitations
Some strengths and limitations are worth noting when interpreting our data. It should be noted that data were used from a rarely examined population (individuals ≥80 years). Additionally, data were taken from a large, representative sample – also covering individuals living in institutionalized settings, whereas existing studies were mainly limited to community-dwelling individuals. Furthermore, valid tools were used to quantify the variables. While the response rate was rather low, the NRW80+ is considered as representative for individuals aged 80 years and over living in North Rhine-Westphalia.21 Nevertheless, as also acknowledged by Kuppler and Wagner:22 individuals with high care needs may be underrepresented. One consequence may be that the actual frequency of multimorbidity is somewhat higher among individuals ≥ 80 years living in North Rhine-Westphalia. Valid tools were used to assess the correlates. Moreover, an established tool was used to quantify multimorbidity. However, it should be noted that it is based on self-reports. Due to the cross-sectional design, the directionality of the associations should be treated with caution.
Conclusion and Future Research
It is worth repeating that a large proportion of individuals in very late life is multimorbid. Apart from health-related factors, also two sociodemographic factors (living situation and network size) were associated with multimorbidity among the oldest old. In conclusion, this knowledge may help to identify individuals at risk for multimorbidity in very late life. Specifically addressing these individuals at risk can contribute to successful ageing among the oldest old. From a public health perspective, this knowledge may ultimately assist in reducing the prevalence of multimorbidity in very late life.
Future research is required to clarify the correlates of different multimorbidity patterns in this age bracket. Moreover, research from other regions and longitudinal studies are both required to confirm our findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. doi:10.1016/j.arr.2011.03.003
2. Van den Akker M, Buntinx F, Metsemakers JF, Roos S, Knottnerus JA. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J Clin Epidemiol. 1998;51(5):367–375. doi:10.1016/S0895-4356(97)00306-5
3. Rijken M, Struckmann V, Dyakova M, Melchiorre MG, Rissanen S, van Ginneken E. ICARE4EU: improving care for people with multiple chronic conditions in Europe. Eurohealth. 2013;19(3):29–31.
4. Arokiasamy P, Uttamacharya U, Jain K, et al. The impact of multimorbidity on adult physical and mental health in low-and middle-income countries: what does the study on global ageing and adult health (SAGE) reveal? BMC Med. 2015;13(1):1–16. doi:10.1186/s12916-015-0402-8
5. Hajek A, Kretzler B, König -H-H. Multimorbidity, loneliness, and social isolation. A systematic review. Int J Environ Res Public Health. 2020;17(22):8688. doi:10.3390/ijerph17228688
6. Nakad L, Booker S, Gilbertson-White S, Shaw C, Chi N-C, Herr K. Pain and multimorbidity in late life. Curr Epidemiol Rep. 2020;7(1):1–8. doi:10.1007/s40471-020-00225-6
7. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev. 2011;68(4):387–420. doi:10.1177/1077558711399580
8. Halonen P, Raitanen J, Jämsen E, Enroth L, Jylhä M. Chronic conditions and multimorbidity in population aged 90 years and over: associations with mortality and long-term care admission. Age Ageing. 2019;48(4):564–570. doi:10.1093/ageing/afz019
9. Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, van den Bos GA. Causes and consequences of comorbidity: a review. J Clin Epidemiol. 2001;54(7):661–674. doi:10.1016/S0895-4356(00)00363-2
10. Scherer M, Hansen H, Gensichen J, et al. Association between multimorbidity patterns and chronic pain in elderly primary care patients: a cross-sectional observational study. BMC Fam Pract. 2016;17(1):1–8. doi:10.1186/s12875-016-0468-1
11. Buczak-Stec E, Hajek A, van den Bussche H, et al. Frequent attendance in primary care in the oldest old: evidence from the AgeCoDe-AgeQualiDe study. Aging Clin Exp Res. 2020;32(12):2629–2638. doi:10.1007/s40520-020-01495-2
12. Sathya T, Nagarajan R, Selvamani Y. Multimorbidity as a risk factor of elder abuse/mistreatment in India: a cross-sectional study. J Interpers Violence. 2022;37(11–12):NP9191–NP9213
13. Yorke AM, Curtis AB, Shoemaker M, Vangsnes E. The impact of multimorbidity on grip strength in adults age 50 and older: data from the health and retirement survey (HRS). Arch Gerontol Geriatr. 2017;72:164–168. doi:10.1016/j.archger.2017.05.011
14. Gu J, Chao J, Chen W, et al. Multimorbidity in the community-dwelling elderly in urban China. Arch Gerontol Geriatr. 2017;68:62–67. doi:10.1016/j.archger.2016.09.001
15. Sakib MN, Shooshtari S, St John P, Menec V. The prevalence of multimorbidity and associations with lifestyle factors among middle-aged Canadians: an analysis of Canadian longitudinal study on aging data. BMC Public Health. 2019;19(1):243. doi:10.1186/s12889-019-6567-x
16. Sindi S, Pérez LM, Vetrano DL, et al. Sleep disturbances and the speed of multimorbidity development in old age: results from a longitudinal population-based study. BMC Med. 2020;18(1):382. doi:10.1186/s12916-020-01846-w
17. Singh A, Contreras Suarez D, You E, Fleitas Alfonzo L, King T. Role of social support in the relationship between financial hardship and multimorbidity-a causal mediation analysis. Eur J Public Health. 2021;31(3):482–487. doi:10.1093/eurpub/ckab015
18. Steeves JA, Shiroma EJ, Conger SA, Van Domelen D, Harris TB. Physical activity patterns and multimorbidity burden of older adults with different levels of functional status: NHANES 2003–2006. Disabil Health J. 2019;12(3):495–502. doi:10.1016/j.dhjo.2019.02.005
19. Zhang Y, Zhou L, Liu S, et al. Prevalence, correlates and outcomes of multimorbidity among the middle-aged and elderly: findings from the China health and retirement longitudinal study. Arch Gerontol Geriatr. 2020;90:104135. doi:10.1016/j.archger.2020.104135
20. Brijoux T, Woopen C, Zank S. Multimorbidity in old age and its impact on life results. Z Gerontol Geriatr. 2021;54(S2):108–113. doi:10.1007/s00391-021-01920-9
21. Wagner M, Rietz C, Kaspar R, et al. Quality of life of the very old. Z Fur Gerontol Geriatr. 2018;51(2):193–199. doi:10.1007/s00391-017-1217-3
22. Kuppler M, Wagner M. Effect of regional long-term care service supply on choice of care arrangement in old age. J Popul Ageing. 2022;15(2):337–361. doi:10.1007/s12062-020-09299-y
23. Diederichs C, Berger K, Bartels DB. The measurement of multiple chronic diseases—a systematic review on existing multimorbidity indices. J Gerontol a Biol Sci Med Sci. 2011;66(3):301–311. doi:10.1093/gerona/glq208
24. UNESCO. International Standard Classification of Education. ISCED 1997.
25. Lawton M, Brody E, Médecin U. Instrumental activities of daily living (IADL). Gerontologist. 1969;9:179–186. doi:10.1093/geront/9.3_Part_1.179
26. Heidenblut S, Zank S. Entwicklung eines neuen Depressionsscreenings für den Einsatz in der Geriatrie. Z Fur Gerontol Geriatr. 2010;43(3):170–176. doi:10.1007/s00391-009-0067-z
27. Heidenblut S, Zank S. Screening for depression with the Depression in Old Age Scale (DIA-S) and the Geriatric Depression Scale (GDS15): diagnostic accuracy in a geriatric inpatient setting. GeroPsych. 2014;27(1):41–49. doi:10.1024/1662-9647/a000101
28. Kristensen K, König -H-H, Hajek A. The association of multimorbidity, loneliness, social exclusion and network size: findings from the population-based German ageing survey. BMC Public Health. 2019;19(1):1–10. doi:10.1186/s12889-019-7741-x
29. Kristensen K, König HH, Hajek A. The longitudinal association of multimorbidity on loneliness and network size: findings from a population-based study. Int J Geriatr Psychiatry. 2019;34(10):1490–1497. doi:10.1002/gps.5158
30. McKinlay E, McDonald J, Darlow B, Perry M. Social networks of patients with multimorbidity: a qualitative study of patients’ and supporters’ views. J Prim Health Care. 2017;9(2):153–161. doi:10.1071/HC16062
31. Hajek A, Brettschneider C, Lange C, et al. Longitudinal predictors of institutionalization in old age. PLoS One. 2015;10(12):e0144203. doi:10.1371/journal.pone.0144203
32. Hajek A, Luppa M, Brettschneider C, et al. Correlates of institutionalization among the oldest old—evidence from the multicenter AgeCoDe-AgeQualiDe study. Int J Geriatr Psychiatry. 2021;36(7):1095–1102. doi:10.1002/gps.5548
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of an Electronic Tool to Assess Patient Preferences in Geriatric Polypharmacy (PolyPref)
Eidam A, Roth A, Frick E, Metzner M, Lampert A, Seidling HM, Haefeli WE, Bauer JM
Patient Preference and Adherence 2022, 16:1733-1747
Published Date: 23 July 2022
Health Priorities in Chronic Obstructive Pulmonary Disease Patients with Multimorbidity: A Qualitative Study
Cai M, Cui M, Nong Y, Qin J, Mo S
Patient Preference and Adherence 2022, 16:2521-2531
Published Date: 13 September 2022
Bidirectional Association Between Probable Depression and Multimorbidity Among Middle-Aged and Older Adults in Thailand
Pengpid S, Peltzer K, Anantanasuwong D
Journal of Multidisciplinary Healthcare 2023, 16:11-19
Published Date: 7 January 2023
Facilitators and Barriers of Integrated Care for Older Adults with Multimorbidity: A Descriptive Qualitative Study
Wu J, Xue E, Huang S, Fu Y, Chen D, Shao J, Zhang H, Tang L, Ye Z
Clinical Interventions in Aging 2023, 18:1973-1983
Published Date: 29 November 2023
Classification of Elderly Patients with Comorbidities and Their Subtypes: A Data-Driven Cluster Analysis
Qiao X, Chen X, Wang W, Guo L, Pan Q
Clinical Interventions in Aging 2025, 20:1671-1680
Published Date: 3 October 2025