Back to Journals » Advances in Medical Education and Practice » Volume 12
Health-Care Providers’ Knowledge, Attitudes, and Practices Regarding Adult Cardiopulmonary Resuscitation at Debre Markos Referral Hospital, Gojjam, Northwest Ethiopia
Authors Abebe TA, Zeleke LB ![]() , Assega MA, Sefefe WM, Gebremedhn EG
, Assega MA, Sefefe WM, Gebremedhn EG ![]()
Received 24 November 2020
Accepted for publication 17 February 2021
Published 14 June 2021 Volume 2021:12 Pages 647—654
DOI https://doi.org/10.2147/AMEP.S293648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Temesgen Agegnehu Abebe,1 Liknaw Bewket Zeleke,2 Mulunesh Alemayehu Assega,3 Worku Mekonnen Sefefe,1 Endale Gebreegziabher Gebremedhn4
1Department of Surgery, School of Medicine, Debre Markos University, Gojjam, Ethiopia; 2Department of Public Health, College of Health Sciences, Debre Markos University, Gojjam, Ethiopia; 3Department Public Health, College of Health Sciences, Debre Markos University, Gojjam, Ethiopia; 4Department of Anaesthesia, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Temesgen Agegnehu Abebe
School of Medicine, Debre Markos University, PO Box 269, Gojjam, Ethiopia
Tel +251 91-881-2675
Email [email protected]
Background: Cardiac arrest is one of the leading causes of death worldwide. Good knowledge, attitudes, and practices of health-care providers regarding cardiopulmonary resuscitation are vital to improve patient outcomes after cardiac arrest. This study aimed to assess knowledge, attitudes, and practices with regard to management of adult patients with cardiac arrest among health-care providers at Debre Markos Referral Hospital, Debre Markos, northwest Ethiopia in 2019.
Methods: A hospital-based cross-sectional study was conducted from January to February, 2019 at Debre Markos Referral Hospital. All health-care providers who fulfilled the inclusion criteria were enrolled in the study. A pretested structured questionnaire was used for data collection. Data were entered into EpiData 3.1 and transferred to SPSS 20 for analysis.
Results: Of the 352 health-care providers, 324 participated in the study for a response rate of 92%. Amajority (63%) were male. The age of male (80%) was 26– 35 years old, with a mean of 29.28± 4.8 years. A majority (77.8%) had inadequate knowledge about cardiopulmonary resuscitation. Almost all (97.8%) had no knowledge about cardiocerebral resuscitation. More than half (64.2%) had unfavorable attitudes toward CPR. Moreover, 288 (88.9%) had unsafe practices regarding cardiopulmonary resuscitation. The site and depth of chest compression was answered correctly by only 33 (10.2%) and 59 (18.2%) of participants, respectively.
Conclusion: Health-care providers’ knowledge, attitudes, and practices were inadequate, unfavorable, and unsafe regarding the management of cardiac arrest. Training on the assessment of critically ill patients, cardiopulmonary resuscitation, and cardiocerebral resuscitation should be provided for health-care providers. Additionally, resuscitation equipment like defibrillators and emergency drugs should be available in all wards and emergency rooms.
Keywords: cardiac arrest, cardiopulmonary resuscitation, knowledge, attitudes, practices
Background
Cardiovascular disease is one of the most common causes of death worldwide, accounting for 30% of deaths.1 Nearly 50% of cardiovascular deaths are due to sudden cardiac death secondary to cardiac arrest.1 Therefore, cardiac arrest is a major public health problem, and most people who have a cardiorespiratory arrest die.1 In the vast majority, cardiac arrest is due to primary cardiac arrest (nonasphyxial arrest), which is usually a loss of functioning cardiac electrical activity, whereas secondary cardiac arrest (asphyxial arrest) results from respiratory insufficiency characterized by lack of oxygen in the blood and occurs in drowning and choking victims and in other circumstances like drug overdoses, which are less common, but still a major public health problem.2 Therefore, preparing meticulous evidence-based guidelines is important to improve the survival of patients with cardiac arrest.3,4 National and international guidelines recommend cardiopulmonary resuscitation (CPR) for both primary and secondary cardiac arrests.3,4 CPR is an emergency procedure used to treat victims of cardiac arrest.3,4
Even in developed nations, society’s and health professionals’ knowledge, attitudes, and practices regarding CPR is not without challenge.3,4 Although immediate response to a cardiac arrest is challenging in resource-limited and developing countries, having basic knowledge, skills, and attitude is an essential part of medical service providers.3,4 A study conducted in India among medical and nursing interns showed that 36% of nursing interns and 46% of medical interns had poor knowledge and 42% of medical interns and 52% of nursing interns poor practices.5 Almost all participants (99%) had positive attitudes toward CPR.5 Another study conducted in Spain showed that 64.7% of hospital staff had attended at least one CPR course and 7% of nursing staff had not had CPR training to American Heart Association standards.6 A study conducted in India indicated that 17.6% of dental interns and 13% of dental postgraduate students had poor knowledge of CPR.7
A study conducted in Malaysia showed that junior doctors lacked the much-needed confidence when it came to an actual resuscitation case.8 It is important to address this issue, as junior doctors are often the frontline doctors called to manage ward emergencies before the arrival of more senior doctors.8 A study carried out in Ethiopia at Jimma University medical students on CPR showed that a majority of students’ knowledge, attitudes, and practices regarding CPR were not sufficiently favorable or safe.9 The current study was designed to assess health-care providers’ knowledge, attitudes, and practices regarding adult CPR and cardiocerebral resuscitation (CCR).
Methods
A descriptive cross-sectional study design was used.
The source population was all health-care providers working at Debre Markos Referral Hospital (DMRH), while the
study population comprised all health-care providers working at DMRH who were available during the data-collection period.
Exclued were new employees and those on annual/maternal leave or seriously ill during the data-collection period. All administrative and supporte staff were also excluded.
Data-Collection Techniques
Data were collected using a pretested standardized self-administered questionnaire. The questions on CPR were adopted from studies in Malaysia and Turkey.8,10 Four medical interns were trained and collected the data. Data collection was supervised by the investigators.
Variables
The dependent variables were knowledge, attitudes, and practices (adequate/inadequate). Independent variables comprised socio-demographic characteristics (age, sex, education, profession), facility-related factors (lack of training opportunities, lack of protocols and guidelines, lack of seminars, and lack of such equipment as electrocardiography [ECG] machines and defibrillators]), and worker factors (experience with cardiac arrest, attendance at training and seminars, reading habits, and media consumption).
Data Compilation and Analysis
Completed questionnaires were checked for completeness and consistency by the investigators. Data were cleaned, entered into EpiData 3.1 transferred to and analyzed with SPSS 20. Descriptive statistics used were means ± SD and percentages to describe the study population in relation to relevant variables. Results are presented in the form of text, graphs, and tables.
Operational and Standard Definition of Terms
- “Basic life support” refers to maintaining the airway, breathing, and circulation for patients with cardiac arrest without using drugs or equipment.
- “Advanced life support” comprises advanced interventions after basic life support had started and appropriate use of automated external defibrillators (AEDs) and drugs.
- “Attitudes” refers to the affective domain of “learner” values, beliefs, and role expectations that may influence the management of patients: eight questions assessed attitudes of respondents toward cardiac arrest management, with those scoring ≥70% deemed to have favorable attitudes and those scoring <70% unfavorable attitudes.8
- “Cardiac arrest” refers to abrupt cessation of cardiac mechanical function that may be reversible by prompt intervention, the lack of which will lead to death.
- For “knowledge”, based on ten questions assessing the knowledge of respondents about cardiac arrest management, those scoring ≥70% were deemed to have adequate knowledge and those scoring <70% inadequate knowledge.8
- “Myocardial infarction” refers to an acute episode of heart disease marked by the death or damage of heart muscle due to insufficient blood supply to the heart muscle, usually as a result of coronary thrombosis or coronary occlusion, characterized especially by chest pain — also called “heart attack”.
- “Practice” refers to actual ability to put specific knowledge into practice: four questions assessd practices of respondents with regard to cardiac arrest management, with those scoring ≥3 deemed to practice safely and those scoring <3 unsafely.
- “Sudden cardiac death” is defined as natural death due to cardiac causes in a person who may or may not have previously recognized heart disease, but in whom the time and mode of death are unexpected.
Quality Assurance
To assure data quality, high emphasis was placed on the data-collection tool. This was a structured questionnaire in English adapted from various literature, and questions were reviewed by experts and senior staff. Before data collection, a pretest of the questionnaire was performed randomly on 20 health-care providers at a nearby hospital (Lumame Primary Hospital). The questionnaire was the modified and utilized for data collection. Training was also given for four data collectors, supervisors, and principal investigators prior to data collection. Supervision was conducted by two supervisors and the principal investigators.
Ethics
This study was conducted in accordance with the Declaration of Helsinki. Ethics clearance was obtained from the ethical review committee of Debre Markos University. All DMRH staff members selected for the study were asked about their willingness to participate. All reasons for subjects being chosen and why the research was being conducted were explained in the questionnaire. Written informed consent was obtained from each participant before commencement of the study. Confidentiality of all data was ensured by avoiding personal identifiers and locking the questionnaire.
Results
Sociodemographic Characteristics of Study Participants
A total of 324 of 352 health-care providers were included in the study, for a response rate of 92%. Nine (2.6%) refused to participate, and 15 (4.3%) were not available during data collection because of annual/maternal leave and training. The age of a majority (80%) of the respondents was 26–35 years, with a mean of 29.28±4.8 years. A majority (63%) were males. The majority (n=194, 59.9%) were nurses and 36 pharmacists (11.1%), followed by midwifery and laboratory personnel, each accounting for 27 (8.3%, Table 1), and 23 (7.1%) were general practitioners. With regard to qualifications, 217 (67%) were BSc holders, 77 (23.8%) had diplomas, five (1.5%) had MSc, and 23 (7.1%) were medical doctors.
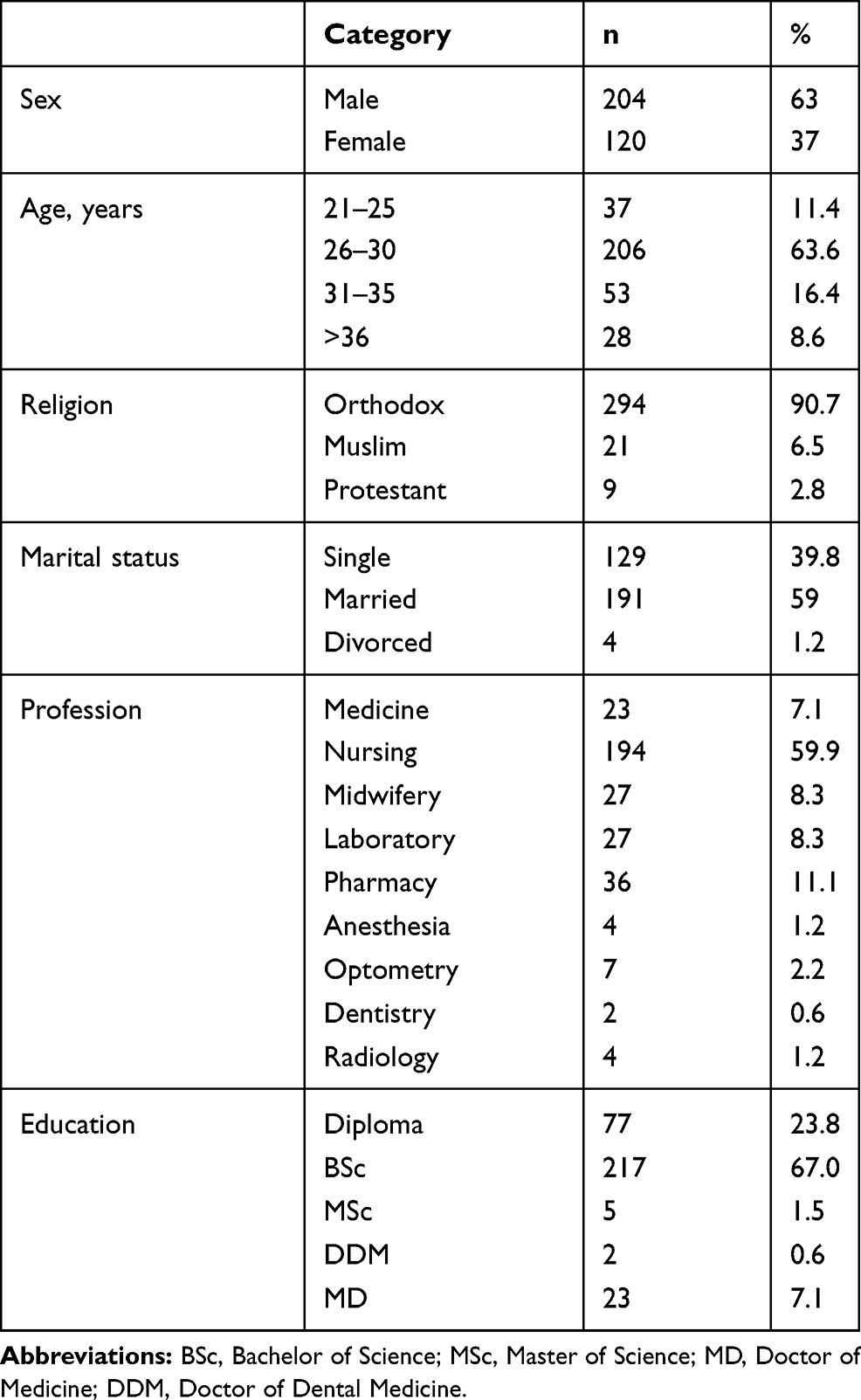 |
Table 1 Sociodemographic characteristics of study participants |
Knowledge of Respondents about Cardiopulmonary Resuscitation
A majority of health-care providers (n=196, 60.5%) knew the compression:ventilation ratio. Additionally, 178 (54.9%) knew the rate of rescue breathing. Only 133 (41%) answered correctly on the importance of uninterrupted chest compression, and 156 (48.1%) knew the correct rate of chest compression (Table 2).
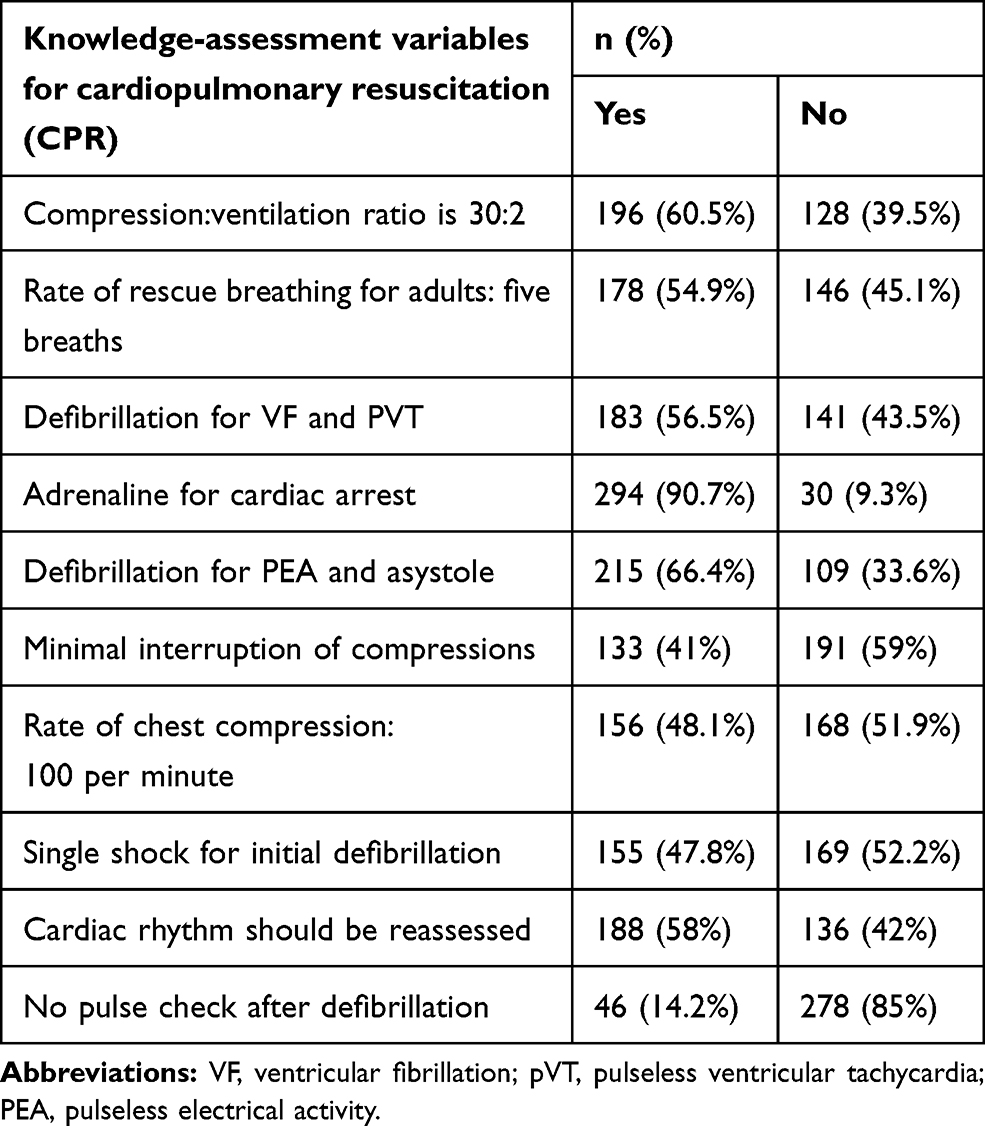 |
Table 2 Health-care providers’ responses to questions to assess knowledge on management of cardiac arrest with CPR |
With regard to profession, more than half (n=13, 56.5%) of the medical doctors had adequate knowledge. A majority of nurses (82%) had inadequate knowledge. All anesthetists (100%) had adequate knowledge. On the contrary, all optometry and radiology health-care providers had inadequate knowledge (Table 3).
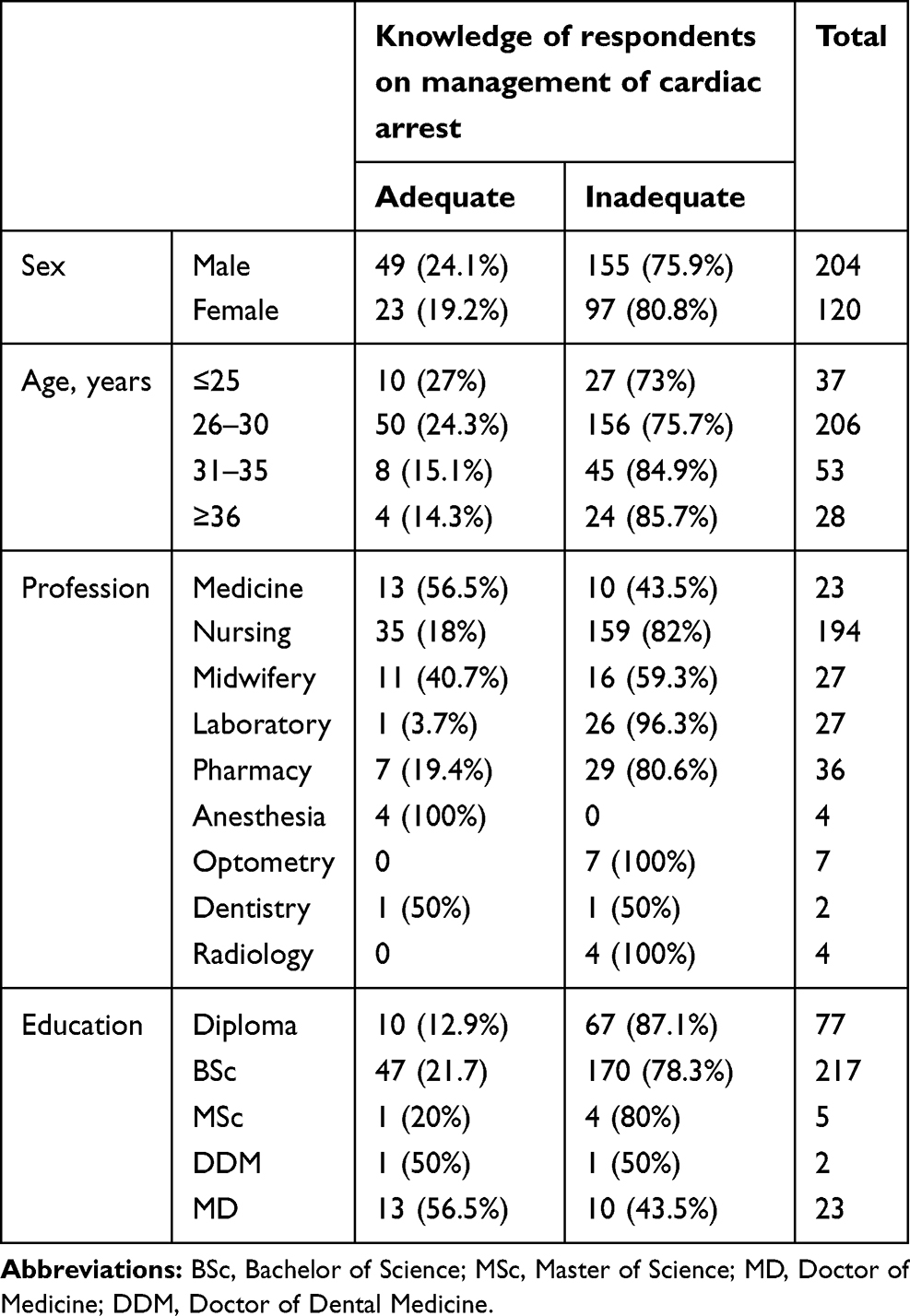 |
Table 3 Knowledge levels of health-care providers |
Knowledge of Respondents about Cardiocerebral Resuscitation
A majority of participants (95.7%) did not know the difference between primary and secondary cardiac arrest (Table 4). Additionally, a majority (n=280, 86.4%) had never heard of CCR. More than half (54.9%) answered that if they saw a person collapsed on the road, they would first ventilate him/herwith mouth to mouth, then start chest compression immediately.
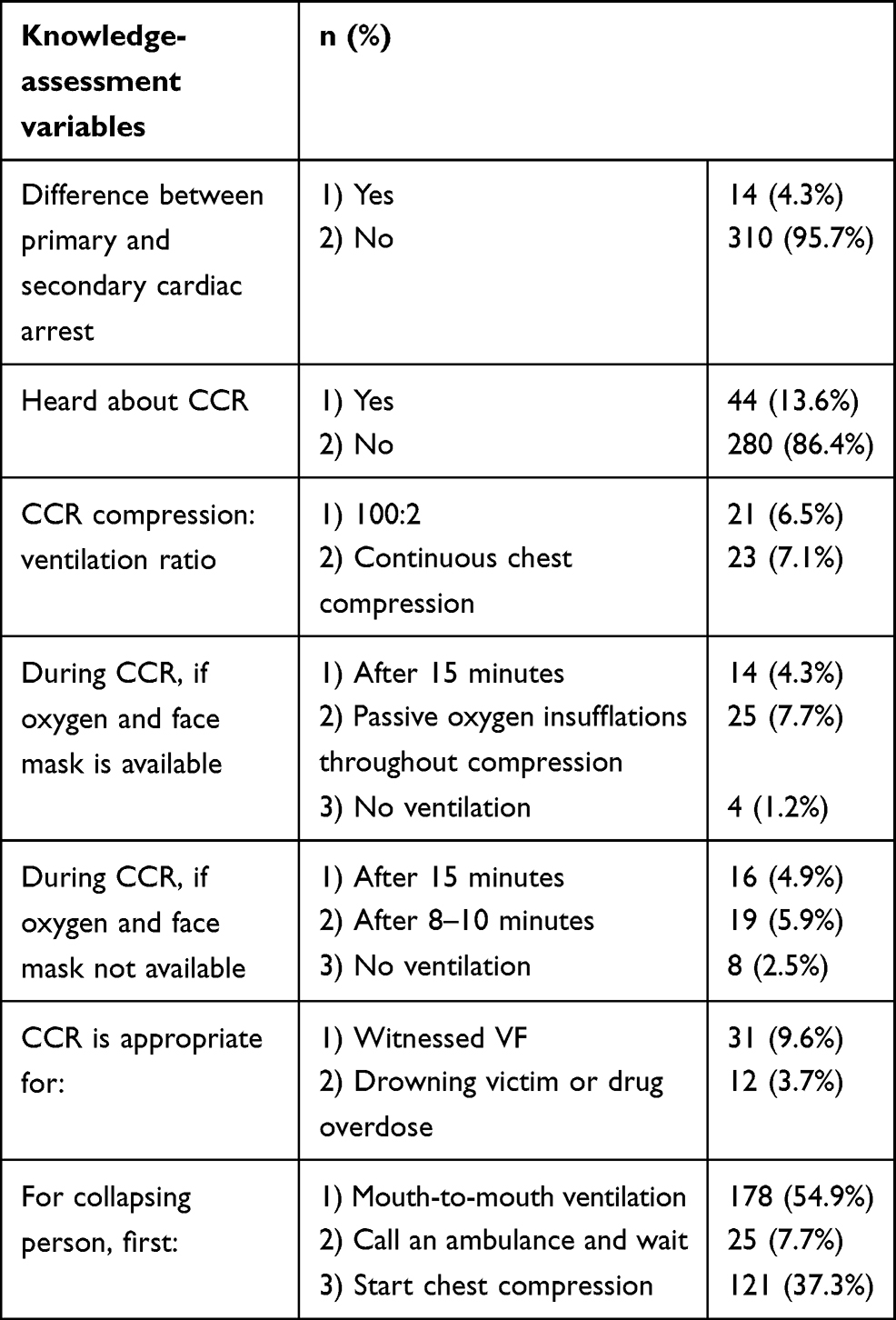 |
Table 4 Health-care providers’ responses to knowledge questions on management of cardiac arrest with cardiocerebral resuscitation (CCR) |
Almost all health care providers (n=317, 97.8%)had inadequate knowledge of CCR, and seven (2.2%) had adequate knowledge (Figure 1).
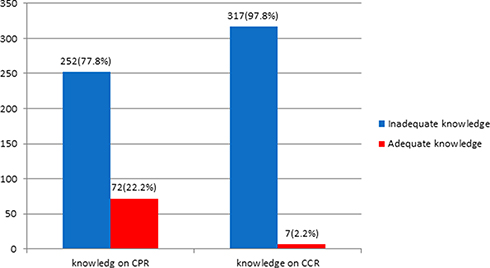 |
Figure 1 Knowledge level of healthcare providers on the management of cardiac arrest with CPR and CCR at Debre Markos Referral Hospital, northwest Ethiopia, 2019. |
Attitudes of Study Participants Toward Cardiopulmonary Resuscitation
More than half (n=208, 64.2%) the health-care providers had unfavorable attitudes toward CPR. Only 116 (35.8%) had favorable attitudes on the management of cardiac arrest. Of the 324 respondents, 239 (73.8%) felt that they had had no adequate training to handle CPR confidently, and 277 (85.5%) and 262 (80.9%) responded that basic life support and advanced cardiac life-support training, respectively should be provided to all health-care workers before practice. More than half (62.7%) responded that they did not understand the principles behind interventions during CPR (Table 5).
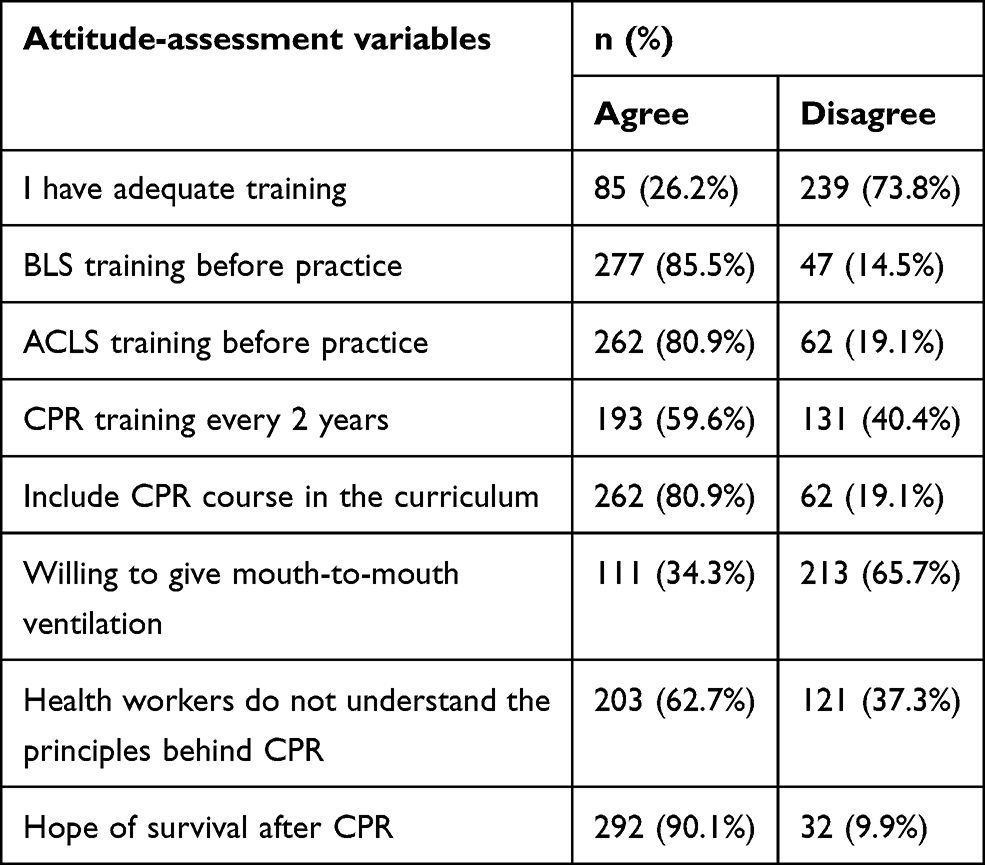 |
Table 5 Health-care providers’ attitudes toward management of cardiac arrest |
Practices of Respondents for Cardiopulmonary Resuscitation
Of the 342 health-care providers, 164 (50.6%) responded correctly that they performed chest compression at a rate of 100 per minute, and 162 (50%) responded correctly on how they ventilated and compressed the chest. However, the site and depth of chest compression were answered correctly by only 33 (10.2%) and 59 (18.2%), respectively (Table 6).
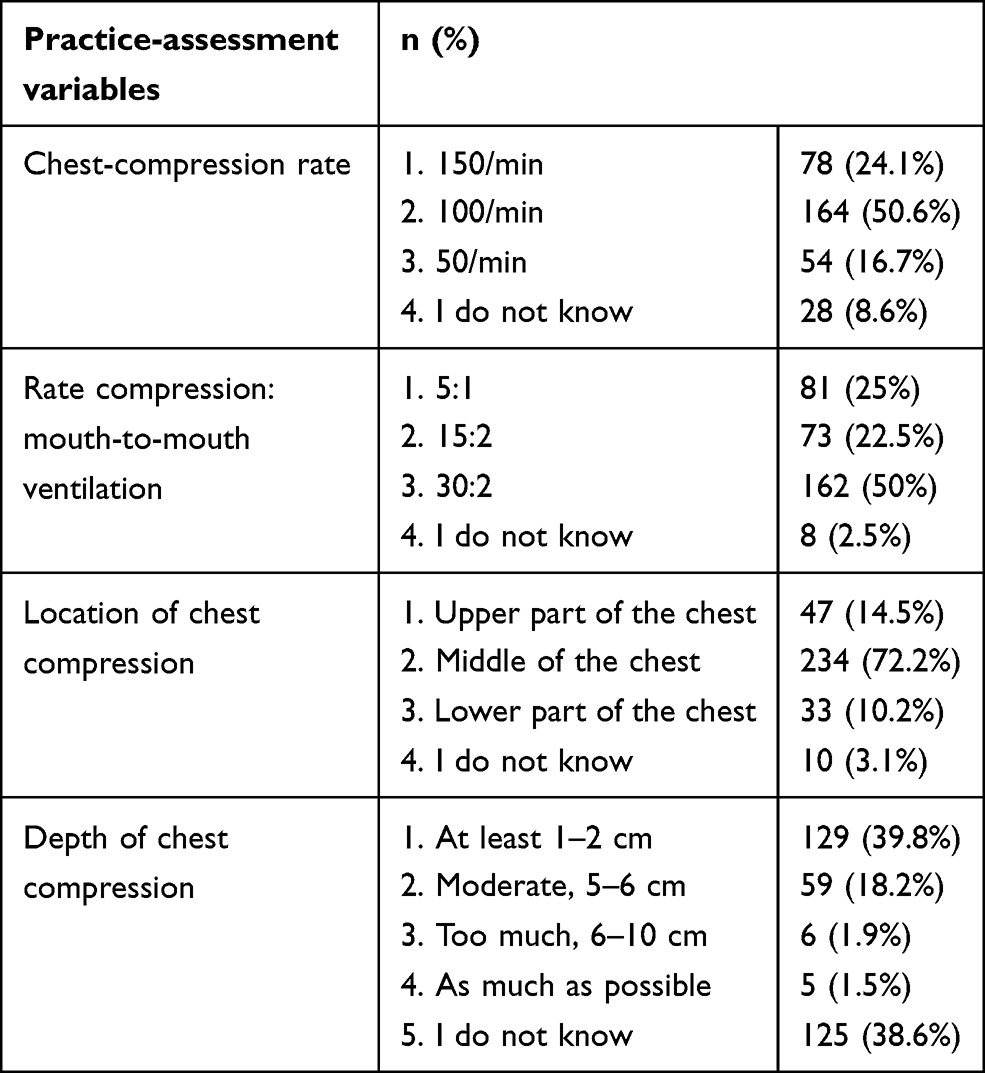 |
Table 6 Health-care provider’s responses for practice questions on the management of cardiac arrest |
With regard to profession, more than half (n=14, 60.9%) of the medical doctors had safe practices. All anesthetists (n=4) had safe practices. However, a majority (91.8%) of nurses had unsafe practices for CPR (Table 7).
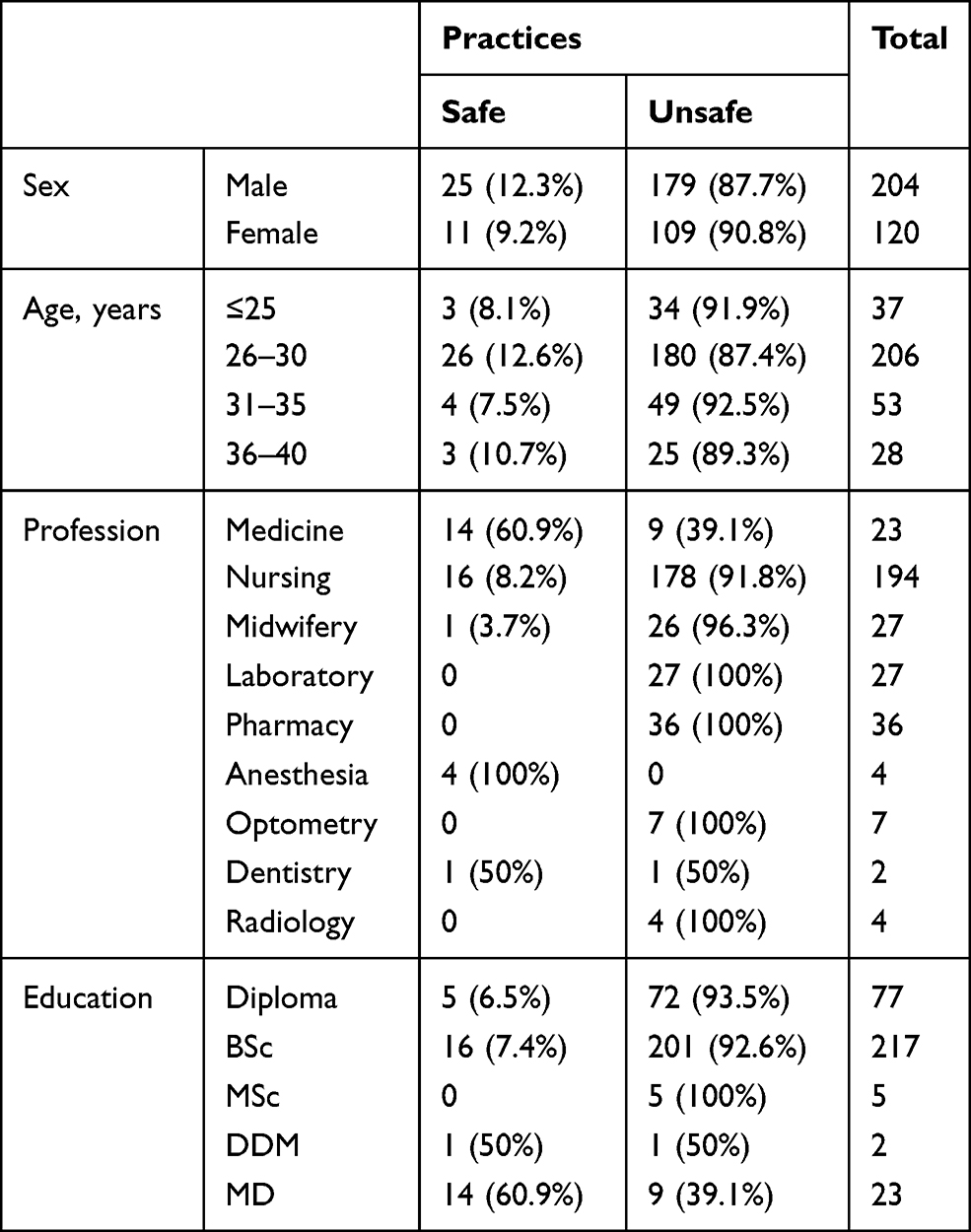 |
Table 7 Health-care providers’ practices in managing cardiac arrest. |
Discussion
In the current study, the knowledge, attitudes, and practices of health-care providers regarding CPR and CCR were substandard. Only 196 (60.5%) knew the compression:ventilation ratio of 30:2. This finding was relatively high compared with a Nigerian study, where the reported knowledge level was 53.85%.11 Additionally, 156 (48%) of the respondents knew the rate of chest compression, whereas in the Nigerian study this was 40%.11 The discrepancy between the present and Nigerian study could be to differences in CPR training, refresher courses, and frequency of exposure to CPR cases. This shows that the hospital should arrange updated training for staff every 6 months and audit the numbers of cardiac arrests and outcomes every month.
The question on the chest compression:ventilation ratio was answered correctly by 21 (91.3%) of the medical doctors. This finding was higher than in a study conducted in Malaysia — 51 (72.9%).8 Additionally, only eight (34.8%) of them knew the rate of rescue breathing, lower than in the Malaysian study — 36 (51.4%).8 Under 60% of participants knew the indication for defibrillation and common ECG rhythms of cardiac arrest, which was low compared with the Malaysian study (70%).8 This difference could be due to discrepancies in the training, availability of facilities for CPR, and exposure to CPR cases. This warrants updated training on CPR and regular auditing of cardiac arrest cases and outcomes very month.
Staff get CPR training rarely, and AEDs are available in some operation theaters only. Staff are exposed to cardiac arrest very often, as there are may trauma cases, in addition to other medical and surgical cases. Unfortunately, there is no out-of-hospital CPR-service system in the catchment area.
In this study, 58.8% and 51.5% of nurses knew about the compression:ventilation ratio and rate of chest compression, respectively. This finding was higher than that in a study conducted in India among nurses, where the reported knowledge level in their study was 14% and 37%, respectively.12 Only 72 (22.2%) of DMRH healthcare providers had adequate knowledge on the management of cardiac arrest. This might be due to the difference in sample size and lack of training opportunities, seminars, and availability of necessary equipment like defibrillators and ECG machines. This indicates that the hospital should purchase resuscitation equipment, such as AEDs, ECG machines, bag-valve masks, and emergency drugs. Additionally, simulation training for CPR should be provided and locally applicable guidelines should be developed.
Regarding knowledge on the assessment of CCR, recently CCR or compression-only CPR has become recommended practice for primary cardiac arrest, since it has a survival benefit over conventional CPR and avoids unnecessary compression interruptions and procedures like mouth-to-mouth ventilation.1,13 However, among the health-care workers at DMRH, only 14 (4.3%) knew the difference between primary and secondary cardiac arrest, and 280 (86.4%) had never heard of CCR. Therefore, almost all the health-care workers (317, 97.8%) had no knowledge about CCR at DMRH. This might be due to lack of training, availability of necessary facilities for CCR, and limited exposure to CCR.
The knowledge level of anesthetists about cardiac arrest management was 100%. This was high compared to a study conducted in Addis Ababa, Ethiopia, where 93.3% of anesthetists scored <84%.14 This could be due to differences in training, refresher courses, and frequency of exposure to CPR cases.
With regard to attitudes, only five (21.7%) DMRH medical doctors felt that they had adequate training or skills in handling CPR. This was lower than the study conducted in Malaysia, where the reported attitude level was 20 (28.6%). Additionally, 20 (86.9%) and 18 (78.3%) DMRH medical doctors believed that basic life support (BLS) and advanced cardiovascular life support (ACLS) training should be provided to all health-care workers, lower than the Malaysian study, where reported attitudes toward training were 69 (98.6) and 66 (94.3%), respectively.8 In this study, among nursing staff, only 82.5% believe that ACLS training should be given to health-care workers, which was very low compared with a study done in India, where support for further ACLS training was 97.4%. Only 116 (35.8%) had favorable attitudes toward cardiac arrest management. This might be due to lack of training and experience with cardiac arrest management.
Practices of health-care providers for cardiac arrest management were insufficent. Half (n=164, 50.6%) knew the rate of chest compression, only 59 (18.2%) knew the depth of chest compression, and 33 (10.2%) knew the correct site of chest compression. This finding was low compared with a study conducted in India which was 59.8%.12 Only 59 (18.2%) knew the proper depth of chest compression. Just one in ten 36 (11.1%) DMRH clinical staff had safe practices for cardiac arrest management. This might be due to lack of training, refresher courses, and local resuscitation guidelines. It should be underlined that the training provided during undergraduate study only may not be sufficient, and regular simulation training and refresher courses should be provided.
Limitation
The limitation of this study is that it was a survey assessment only,where there may be limited correlation between the survey responses and the actions of respondents in real life.
Conclusion
Knowledge, attitudes, and practices of health-care providers regarding the management of cardiac arrest were substandard. For CPR, few participants knew the rate of rescue breathing, defibrillation indications, procedures during CPR. With regard to knowledge about CCR, a majority did not know the difference between primary and secondary cardiac arrest, and almost none had heard of CCR.
The majority of health-care providers at DMRH had positive attitudes toward BLS training and incorporating CPR courses in the undergraduate curriculum. However, the majority of respondents felt that they had no adequate training to manage cardiac arrest confidently. Most felt that they did not understand the principles behind CPR.
As for cardiac arrest management, the majority of respondents did not know the site or depth of chest compressions, which revealed unsafe practices for cardiac arrest management.
It is recommended that refresher courses and simulation training on CPR and CCR should be provided for health-care providers. Locally applicable CPR and CCRguidelines should be developed. Resuscitation equipment like defibrillators and emergency drugs should be purchased and made available in emergency rooms and all wards. Furthermore, there should be regular auditing of cardiac arrest cases and outcomes every month.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ewy GA. The cardiocerebral resuscitation protocol for treatment of out-of-hospital primary cardiac arrest. Scand J Trauma Resusc Emerg Med. 2012;20:65. doi:10.1186/1757-7241-20-65
2. Ewy GA. Cardiocerebral and cardiopulmonary resuscitation - 2017 update. Acute Med Surg. 2017;4(3):227–234. doi:10.1002/ams2.281
3. Neumar RW, Shuster M, Callaway CW, et al. 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18):S315–S367. doi:10.1161/CIR.0000000000000252
4. Ewy GA. Chest compression only cardiopulmonary resuscitation for primary cardiac arrest. Circulation. 2016;134:695–697. doi:10.1161/CIRCULATIONAHA.116.023017
5. Mendhe HG, Burra L, Singh D, et al. Knowledge, attitude and practice study on cardiopulmonary resuscitation among medical and nursing interns. Int J Community Med Public Health. 2017;4(8):3026. doi:10.18203/2394-6040.ijcmph20173366
6. García S, Blen A, Alemán F, et al. Assessment of the knowledge level and its relevance in terms of CPR in medical personnel of the hospital emergency medical system of the autonomous community of the region of Murcia. Enfermeria Glob. 2015;14:230.
7. Narayan DP, Biradar SV, Reddy MT, et al. Assessment of knowledge and attitude about basic life support among dental interns and postgraduate students in Bangalore city, India. World J Emerg Med. 2015;6(2):118–122. doi:10.5847/wjem.j.1920-8642.2015.02.006
8. Chew KS, Hashairi FM, Zarina Z, et al. A survey on the knowledge, attitude and confidence level of adult cardiopulmonary resuscitation among junior doctors in Hospital Universiti Sains Malaysia and Hospital Raja Perempuan Zainab II, Kota Bharu, Kelantan, Malaysia. Med J Malaysia. 2011;66(1).
9. Tsegaye W, Tesfaye M, Alemu M. Knowledge, attitude and practice of cardiopulmonary resuscitation and associated factors in Ethiopian University medical students. J Gen Pract. 2015;3:4. doi:10.4172/2329-9126.1000206
10. Ozbilgin S, Akan M, Hanci V, et al. Evaluation of public awareness, knowledge and attitudes about cardiopulmonary resuscitation: report of Izmir. Turk J Anaesthesiol Reanim. 2015;43(6):396–405. doi:10.5152/TJAR.2015.61587
11. Olajumoke TO, Afolayan JM, Raji SA, et al. Cardiopulmonary resuscitation - knowledge, attitude & practices in OSUN STATE, Nigeria. J West Afr Coll Surg. 2012;2(2):23–32.
12. Pillai SV, Ramesh B, Koshy RC. Knowledge, attitude and practice of current cardiopulmonary resuscitation guidelines – a survey among nurses. IOSR J Nurs Health Sci. 2016;5(2).
13. Bobrow BJ, Clark LL, Ewy GA, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299(10):1158–1165. doi:10.1001/jama.299.10.1158
14. Weji BG, Goshu EM, Melese KG. Assessment of knowledge, attitude and associated factors of cardiopulmonary resuscitation among anesthetists working in governmental and private hospitals in Addis Ababa. Int J Med Med Sci. 2017;9(3):17–21. doi:10.5897/IJMMS2017.1291
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.