Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Glycemic Control and Associated Factors Among Children and Adolescents with Type 1 Diabetes Mellitus, Southwest Ethiopia
Authors Abrahim AM ![]() , Tilahun T, Gelana B
, Tilahun T, Gelana B ![]()
Received 24 April 2023
Accepted for publication 27 June 2023
Published 4 July 2023 Volume 2023:16 Pages 2025—2037
DOI https://doi.org/10.2147/DMSO.S412529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Aneso Mohammed Abrahim,1 Tsion Tilahun,1 Beshea Gelana2
1Department of Pediatrics and Child Health, Jimma University, Jimma, Ethiopia; 2Department of Health Policy and Management, Jimma University, Jimma, Ethiopia
Correspondence: Beshea Gelana, Department of health policy and management, Jimma University, Jimma, Ethiopia, Tel +251 921833996, Email [email protected]
Purpose: Type 1 diabetes mellitus is the most common endocrine disorder among children and adolescents worldwide. Glycemic control is the ultimate goal of management of diabetes. Poor glycemic control is shown to be associated with complications of diabetes. Only a few studies have addressed the problem in Ethiopia, and this study aimed to determine the level of glycemic control and factors associated among children and adolescents with type 1 diabetes mellitus on follow up.
Methods: Institution based cross sectional study design was conducted on a total of 158 children and adolescents with type 1 diabetes on follow up at Jimma Medical Center from July to October 2022. Data were collected using structured questionnaire and entered into Epi Data 3.1 then exported to SPSS for analysis. Glycemic control was assessed based on glycosylated hemoglobin (HbA1c) level. Descriptive and inferential statistics were employed, and a p-value < 0.05 was considered to declare statistical significance.
Results: The mean glycosylated hemoglobin of the participants was 9.67 ± 2.28%. Of the total study participants, 121 (76.6%) had poor glycemic control. In multivariable logistic regression, guardian or father as a primary caregiver [guardian (AOR=4.45, 95%, p=0.045), father (AOR=6.02, 95%, p=0.023)], minimal involvement of caregiver in insulin injection (AOR=5.39, 95%, p=0.002), poor blood glucose monitoring adherence (AOR=4.42, 95%, p=0.026), faced problems at health facility (AOR=4.42, 95%, p=0.018) and being admitted to hospital in the past 6 months (AOR=7.94, 95%, p=0.004) were the variables significantly associated with poor glycemic control.
Conclusion: Majority of children and adolescents with diabetes had poor glycemic control. Whereas, primary caregiver other than mother, minimal involvement of caregiver in insulin injection, and poor adherence to glucose monitoring were among the contributing factors for poor glycemic control. Therefore, adherence counseling and the participation of caregivers in diabetes management is recommended.
Keywords: adolescents, children, diabetes, Ethiopia, glycemic control, Jimma
Introduction
Type 1 diabetes mellitus is one of the most common endocrine disorders among children and adolescents, having significant consequences on physical and emotional development. It is an autoimmune disease characterized by low or absent level of endogenously produced insulin and by dependence on exogenous insulin to prevent development of ketoacidosis, an acute life-threatening complication of T1DM. Although most symptoms of T1DM are non-specific, the most important clue is an inappropriate polyuria and poor weight gain. T1DM in children and adolescents are diagnosed in the presence of random blood glucose ≥200mg/dL (11.1mmol/L) with typical symptoms like polyuria, polydipsia, and unexplained weight loss with glucosuria and ketonuria.1
According to the International Diabetes Federation (IDF) estimation, there were an estimated 1.1 million children 0–14 years in 2021 globally. In Ethiopia, the estimated prevalence of T1DM among children and adolescents of 0–19 years old is 2.4 per 100,000 per year.2
In patients with diabetes the morbidity and mortality are usually due to the acute metabolic derangements and chronic complications such as nephropathy, retinopathy, ischemic heart disease, neuropathy, and arterial occlusion with gangrene of the extremities.1 Glycemic control is an important part of management of diabetes. It is the strongest modifiable predictor of chronic complications of diabetes. It was shown that strict glycemic control delayed the onset and also slowed the progression of chronic complications of diabetes.3
Glycemic control can reliably be determined by measuring level of glycosylated hemoglobin (HbA1c) which reflects the level glycaemia over the preceding two to three months. As a result, measurement of HbA1c is often recommended to be done every three months.1 According to the recommendations of the ADA and the International Society for Pediatric and Adolescent Diabetes (ISPAD), children and adolescents who have access to comprehensive diabetes care should aim to achieve a target of HbA1c <7.0% (53mmol/mol). However, a higher HbA1c target (<7.5%[58mmol/mol]) is appropriate in settings where there is lack of access to analog insulins, advanced insulin delivery technology, ability to regularly check blood glucose and continuous glucose monitoring.4,5
Despite continuous improvement means and development of supported protocols, majority of children and adolescents with T1DM failed to achieve optimal glycemic control. According to ADA only 21% of adolescents with T1DM achieved optimal glycemic goals. This situation is even alarming in low income countries due to lack of adequate financial human resources. This failure to meet optimal glycemic control can have significant consequences on health outcomes and can contribute to early development of chronic complications of diabetes.6
Various factors and challenges have been identified that are associated with the level of glycemic control. Some of these factors include socio-demographic variables like age of the child, family structure and socioeconomic status. Other diabetes related factors that were found to affect glycemic control includes duration of diabetes, adherence and involvement of caregiver in the diabetes management.7–11
In a study done in Ethiopia it was found that more than fifty percent of children and adolescents with diabetes had poor glycemic control. However, in that study the HbA1c cutoff used for defining poor glycemic control was >10% (86mmol/mol) which is higher than the recommended target HbA1c; and the study did not identify factors associated with glycemic control.12 Another recent study in Ethiopia also documented that the mean HbA1c was 9.6 ± 2.4% and concluded that the majority of children and adolescents had poor glycemic control. However, in that study the HbA1c measurement was not uniformly done at the time of data collection, rather it was taken from the medical records of patients. Therefore, this study aimed to determine the level of glycemic control and identify factors associated among children and adolescents with T1DM on follow-up at a pediatric chronic follow up clinic in Jimma Medical Center, Jimma, Ethiopia.
Materials and Methods
Study Area and Period
The study was conducted at pediatric chronic follow up clinic of Jimma Medical Center, Jimma, South-west Ethiopia. Jimma Medical Center is located in Jimma town which is located in southwestern part of Ethiopia, Oromia region, 352km from Addis Ababa. It serves as a referral hospital for southwestern part of the country. It gives service in different specialty and subspecialty fields, among these pediatrics and child health is one of them. The service given at pediatrics and child health include inpatient treatment and outpatient treatment including emergency, ambulatory and follow up service. Children and adolescents with T1DM attend their regular follow up at pediatrics follow up clinic and the care given include evaluation by pediatrics residents, medication refill, diabetes education etc. The study was conducted from July 10 to October 10, 2022.
Study Design and Population
An institution-based cross-sectional study was conducted among children and adolescents with type 1 diabetes mellitus on follow up at pediatric follow-up clinic at Jimma Medical Center.
Sampling and Eligibility Criteria
There were a total of 173 children and adolescents with type 1 diabetes mellitus on regular visits at pediatrics follow-up clinic of Jimma Medical Center. The calculated final sample size before performance the study become 107 by using single population proportion formula. However, as the sample size is manageable and also to increase the precision, we decided to include all sample fulfilling the inclusion criteria as the final sample size.
All children and adolescents ≤ 18 years of age, diagnosed with type 1 diabetes mellitus, on medication for at least 3 months, and on follow up at pediatric follow up clinic were consecutively included. Those children and adolescents who are on treatment for less than 3 months and those who refuse to participate in the study were excluded.
Study Variables
The dependent variable is the level of glycemic control. The independent variables in this study were divided into two categories. They were: a) socio-demographic- this category included variables such as age, gender and educational status of child/adolescent, age, gender, educational status, marital status of primary caregivers, average family monthly income, place of residence and relationship of primary caregivers with the child and adolescent; and b) diabetes, medication and health facility related factors-this category included variables such as Age at diagnosis, Duration of diabetes, Anthropometric parameters, Insulin Storage, Missed Insulin doses, Frequency of blood glucose monitoring, Caregiver involvement in Insulin injections and supervision and blood glucose monitoring (BGM), presence of comorbidity, Caregiver’s diabetes knowledge status, health education given during visit, problems faced during follow up visit and frequency of hospital admission in the past 6 month.
Data Collection and Measurements
Data Collection Instruments
Diabetes knowledge of the caregiver was assessed using validated structured questionnaire of diabetes knowledge test adapted from Michigan University tools for health professionals and modified to the context of Ethiopian diet.13,14 It contains 23 items, correct answer to the question was given a score of 1 and incorrect or I do not know answer was given score of 0. Additionally, to capture important information about the sociodemographic information of the child and caregiver, duration of diabetes, anthropometric assessments, insulin dose, regimen, storage and missed doses, frequency of blood glucose monitoring, caregiver involvement in insulin injections and BGM, level of HbA1c, comorbidity and health facility/service related factors were prepared after reviewing literatures.
Data Collection Procedures
Participants and their caregivers were interviewed using structured questionnaires. The anthropometric assessment was done and standardized using WHO curve for nutritional assessment. Chart of the patient reviewed to capture duration of DM, insulin regimen and dosage. Blood sample for HgbA1c determination collected by trained nurses, the code written on the sample collection tube (EDTA), and then it was given to the assigned laboratory technician at the main laboratory. Results were collected and documented on questionnaire. HgbA1C was done using Roche HITACHI (Cobas 6000) machine at the main laboratory. The questionnaire was prepared in English and translated to Afaan Oromo and Amharic language which are most commonly used by the study population. Data quality was assured during data collection, coding, entry and analysis. To increase the quality of data internal consistency, reliability test was done for the tool used. The Cronbach’s alpha for Diabetes knowledge test was (α=0.79). The completeness and consistency of collected data was checked on daily basis.
Operational Definition
Missed insulin doses: this was determined by the number of insulin doses missed in the past 1 week.
Insulin storage: this the place where the family or caregiver regularly keep the Insulin after using this can be refrigeration, storage in a pot of cold water, storage at room temperature or others.
Blood glucose monitoring (BGM) adherence: This was determined by the frequency of blood glucose measurement in a week. It was graded as, Good: ≥3 times per week, Average: 1–2 times per week and Poor: none.7,15
Caregiver involvement in diabetes management: includes involvement in insulin injections and involvement in BGM. This was assessed by using a scale graded as minimal, moderate or optimal involvement. This was adapted from study done in Tanzania on glycemic control and associated factors.7
Involvement in insulin injection was determined by the number of insulin doses injected or supervised by caregiver in the last 24hr:
Minimal: none
Moderate: 1 injection
Optimal: all injections
Involvement in BGM was determined by the degree of participation of caregiver in the task of blood glucose determination:
Minimal: No participation
Moderate: Reminds the child to check blood glucose, Enters glucose level in the diary or Asks the child about the blood glucose level
Optimal: Sets up the glucometer, Does the finger prick or Supervises the task
Level of Glycemic control: In this study, Good glycemic control: HbA1c <7.5% and Poor Glycemic control: HbA1c ≥7.5%.
Caregiver: an individual, such as a family member or guardian who takes care of a child or adolescent.
Guardian: an individual other than the parents who takes care of a child or adolescent.
Adolescents: from 12 to 18 years old
Children: up to 12 years old
Overweight: defined as BMI b/n 2SD and 3SD or WFA b/n 2SD and 3SD
Obese: defined as BMI > 3SD or WFA >3SD.
Wasting: Moderate wasting = defined by WHO curve as WFH/L b/n −2SD and −3SD, BMI b/n −2SD and −3SD and Severe wasting: defined by WFH/L <-3SD, BMI < −3SD.
Stunting: Severe stunting= defined by using WHO curve as L/HFA less than −3SD and Moderate stunting= Defined as L/HFA b/n −2SD and −3SD.
Comorbidities: are a problem identified after onset of diabetes and usually related to as complication either due to disease progression or treatment related complication or chronic illnesses like epilepsy, RVI.
Diabetes Knowledge: includes components like knowledge of diabetic diet, diabetic test, general diabetes knowledge, physical exercise and diabetes and about diabetic complication.
From the 23 knowledge test questions
Poor Knowledge: participants who scored below the mean value were considered as having poor knowledge towards T1DM.
Good Knowledge: participants who scored above the mean value were considered as having good knowledge or knowledgeable towards T1DM.
Data Processing and Analysis
Collected data were checked for completeness and clarity and variables were categorized then cleaned, coded, and entered into Epi-Data 3.1, exported to SPSS version 25.0 for analysis. Frequencies, percentage, mean and standard deviation were used to summarize descriptive statistics. Univariate, bivariate, and multivariate analyses were also done. Candidate variables on binary logistic regression (p-value ≤0.25) were analyzed by multivariable logistic regression to identify significant predictor for poor glycemic control. Variables having p-value <0.05 in the multivariate logistic regression model were considered as statistically significant. The odds ratio was also used to determine the strength of association between independent variables and the outcome variable.
Results
Socio-Demographic Characteristics
A total of 158 children and adolescents with T1DM on follow up at pediatrics follow up clinic of JMC fulfilling the inclusion criteria were included in the study during the study period. This study revealed that the mean and standard deviation of the age of the participants were 12.05 ± 3.74 years with minimum and maximum age of 1 and half year and 18 years old respectively. More than half 86 (54.4%) of the study participants were males. Regarding educational status of the study participants 68 (43.0%) were attending elementary school. This study also revealed that the mean and standard deviation age of primary caregiver was 39.33± 10.25 years. About 93 (58.9%) of the primary caregivers were females and 86 (54.4%) of caregivers were children’s mother. Additionally, the majority 93 (58.9%) participants were from rural. One-fourth of the primary caregivers ha attended primary education. Based on this study 55 (34.8%) of the study participants were having ≤1500 ETB of family monthly income (See Table 1).
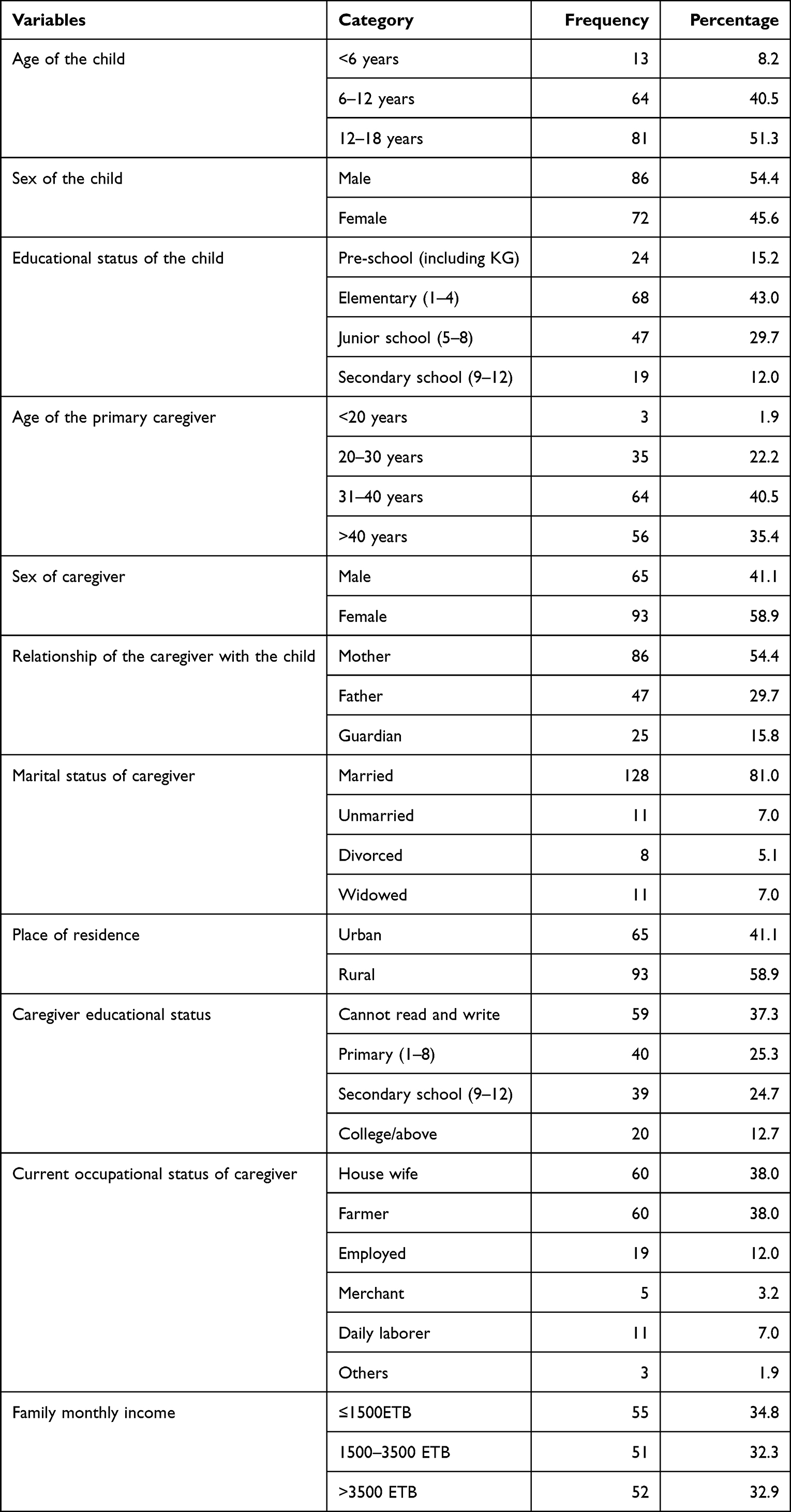 |
Table 1 Socio-Demographic Characteristics of Children and Adolescents with Type 1 DM at Pediatric Follow Up Clinic, JMC, Southwest Ethiopia, 2022 |
Diabetes and Medications Related Factors
This study revealed that the mean and standard deviation age in years at diagnosis was 8.62 ±3.56 years. About 71 (44.9%) participants age at diagnosis was between 5 and 10 years of age. The mean and standard deviation of duration of diabetes in years was 3.43±2.76 years. Similarly, about 79 (50%) respondents duration of diabetes was between 1 and 5 years. This study revealed that all children and adolescents with type 1 diabetes were using an intermediate-acting NPH insulin mixed with regular insulin administered twice daily. This study revealed that half 79 (50.0%) of the patients stored the medication in pot of cold water followed by 59 (37.3%) of them stored insulin in refrigerator. Regarding caregiver involvement in insulin injection, only 40 (25.3%) of them had optimal and 14 (8.9%) of them were having moderate caregiver involvement in the tasks. Whereas 41 (25.9%) of participants were having optimal caregiver involvement with regard to insulin injection supervision. Sixty (38.0%) study participants had good adherence to blood glucose monitoring. Regarding the role/involvement of caregivers in measurement of blood glucose, only 47 (29.7%) caregivers had optimal involvement in the task (See Table 2).
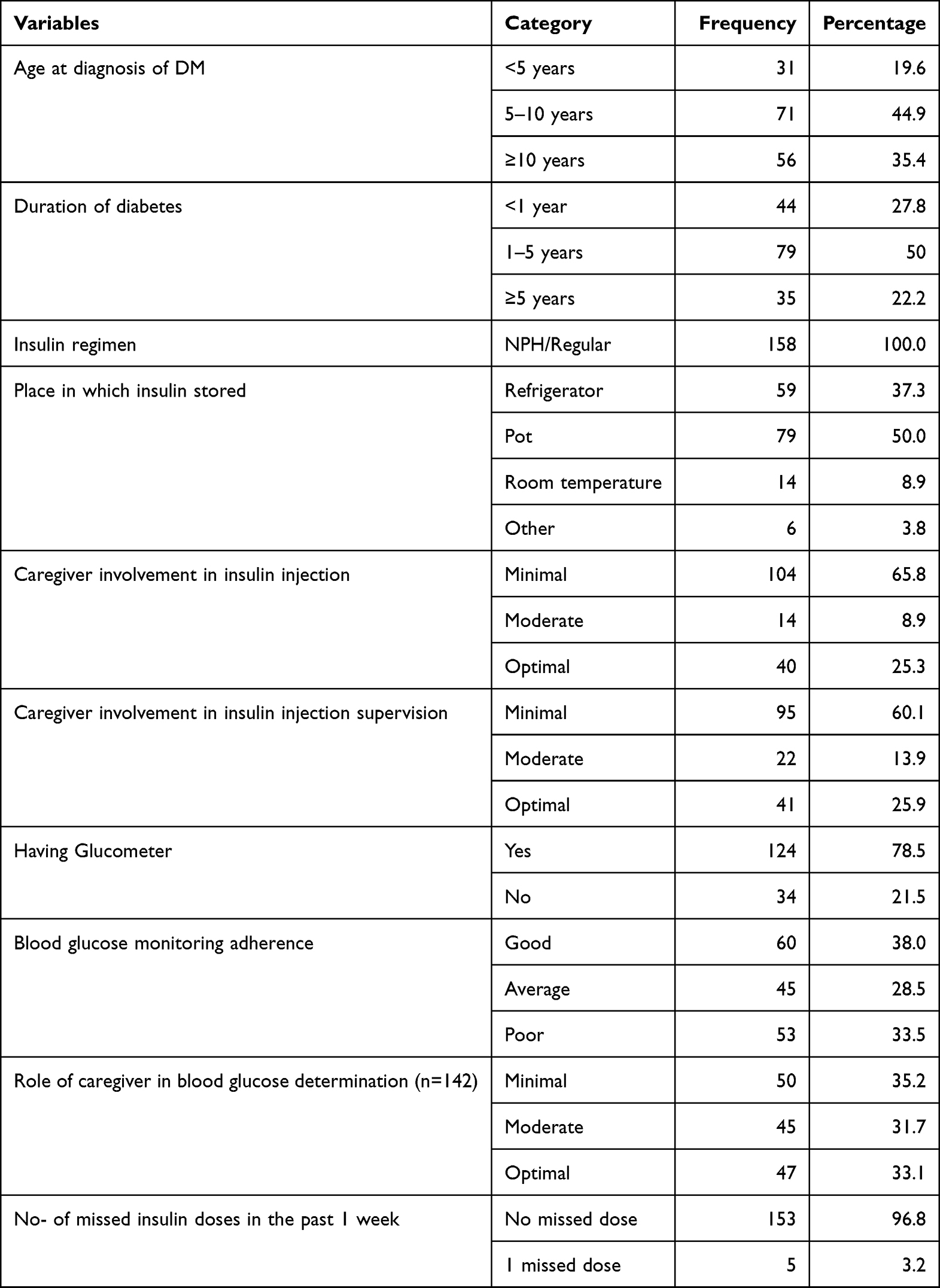 |
Table 2 Diabetes and Medication Related Characteristics of Children and Adolescents with Type 1 DM at Pediatric Follow Up Clinic, JMC, Southwest Ethiopia, 2022 |
Nutritional Status of Children and Adolescents
This study showed that 8 (5.1%) participants were reported as being underweight. Similarly, moderate stunting was reported among 27 (17.1%) children and severe stunting was reported among 8 (5.1%) children. Based on the BMI for age result 13 (8.2%) children had moderate wasting and 2 (1.3%) children were reported as having severe wasting. Additionally, 20 (12.7%) respondents had moderate wasting based on MUAC for age value (See Table 3).
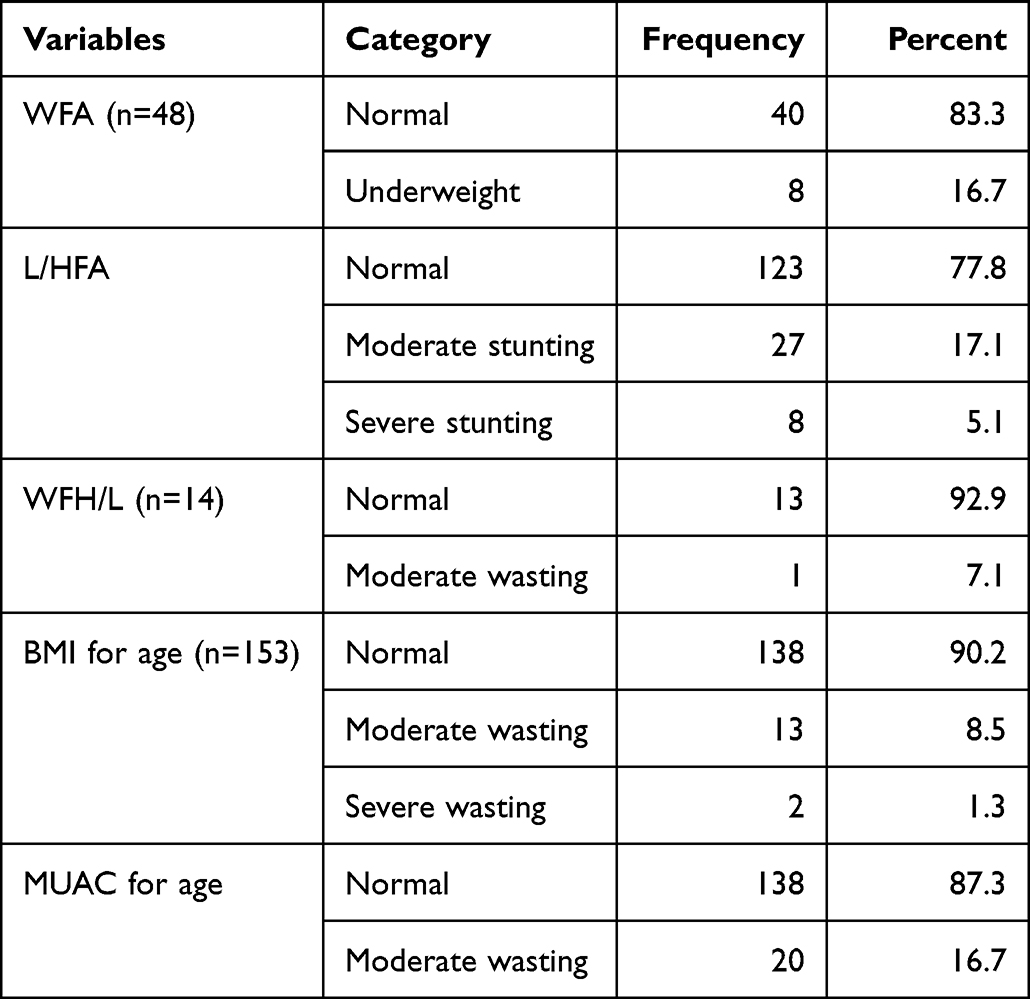 |
Table 3 Anthropometric Parameters of Children and Adolescents with Type 1 DM at Pediatric Follow Up Clinic, JMC, Southwest Ethiopia, 2022 |
Health Facility/Service Related Factors
This study revealed that 145 (91.8%) study participants have received health education and/or advice about diabetes during any of their visits to health facility. This study also revealed that half 81 (51.3%) of study participants faced problems in the hospital during health care delivery. Among problems faced during health care delivery shortage of insulin was reported among 79 (50.0%) children. Similarly, 42 (26.6%) of children with Type 1 DM attending their follow up at Pediatric clinic of JUMC have been admitted to hospital in the past 6 months. Among admitted children 36 (85.7%) of them were admitted for 1 time and the rest 6 (14.3%) of children were admitted to hospital 2 times in the last 6 months (See Table 4).
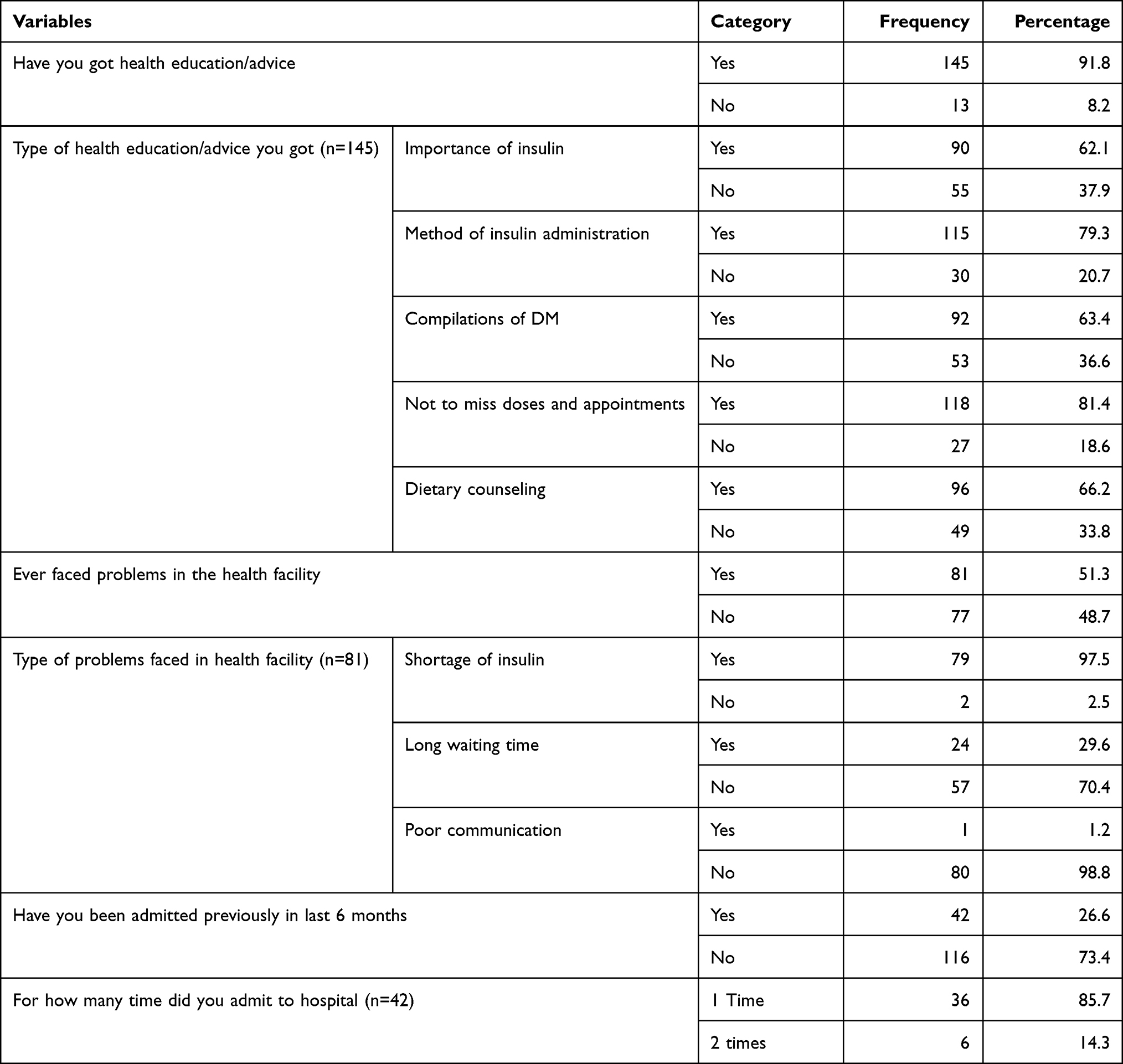 |
Table 4 Health Facility Related Characteristics of Children and Adolescents with Type 1 DM at Pediatric Follow Up Clinic, JMC, Southwest Ethiopia, 2022 |
Caregivers’ Diabetes Knowledge Status
This study revealed that the mean and standard deviation of diabetes knowledge score among caregivers towards diabetic knowledge was 8.48 ±3.58 with minimum and maximum knowledge score of 2 to 17 out of 23 knowledge items.
Level of Glycemic Control
Regarding the level of HgbA1C; the mean and standard deviation of HgbA1C was 9.67 ± 2.28%. According to this study about 3/4th of the study participants were having poor glycemic control (See Figure 1).
 |
Figure 1 Glycemic control among children and adolescents with type 1 DM at pediatric follow up clinic, JMC, Southwest Ethiopia, 2022. |
Factors Associated with Poor Glycemic Control
In multivariate logistic regression model caregivers relationship with child, involvement of caregiver in insulin injection supervision, blood glucose monitoring adherence, faced problems at hospital during health care delivery, and having previous admission in last six months were found to be significant variables associated with poor glycemic control at p-value <0.05 with 95% CI of AOR.
So, this study revealed that children having guardian as primary caregiver were 4.4 times more likely to have poor glycemic control compared to mother as primary caregiver for a child (AOR=4.45 95%, p=0.045). Similarly, children having father as primary were 6 times more likely to have poor glycemic control compared to mother as primary caregiver for a child (AOR=6.02, 95%, p=0.023).
The odds of having poor glycemic control was 5.4 times higher among participants who had minimal caregiver involvement in insulin injection supervision compared to children who had optimal caregiver involvement (AOR=5.39, 95%, p=0.002). The odds of having poor glycemic control was 4.4 times higher among children who had poor blood glucose monitoring adherence as compared to children who had good adherence (AOR=4.42, 95%, p=0.026).
Participants who had faced problems at hospital while seeking health service was 3.4 times more likely to have poor glycemic control compared to their counterparts (AOR=4.42, 95%, p=0.018). Similarly, this study revealed that the odds of having poor glycemic control was 7.9 times higher among children who had history of previous admission in the last six months as compared to their counterparts (AOR=7.94, 95%, p=0.004) (See Table 5).
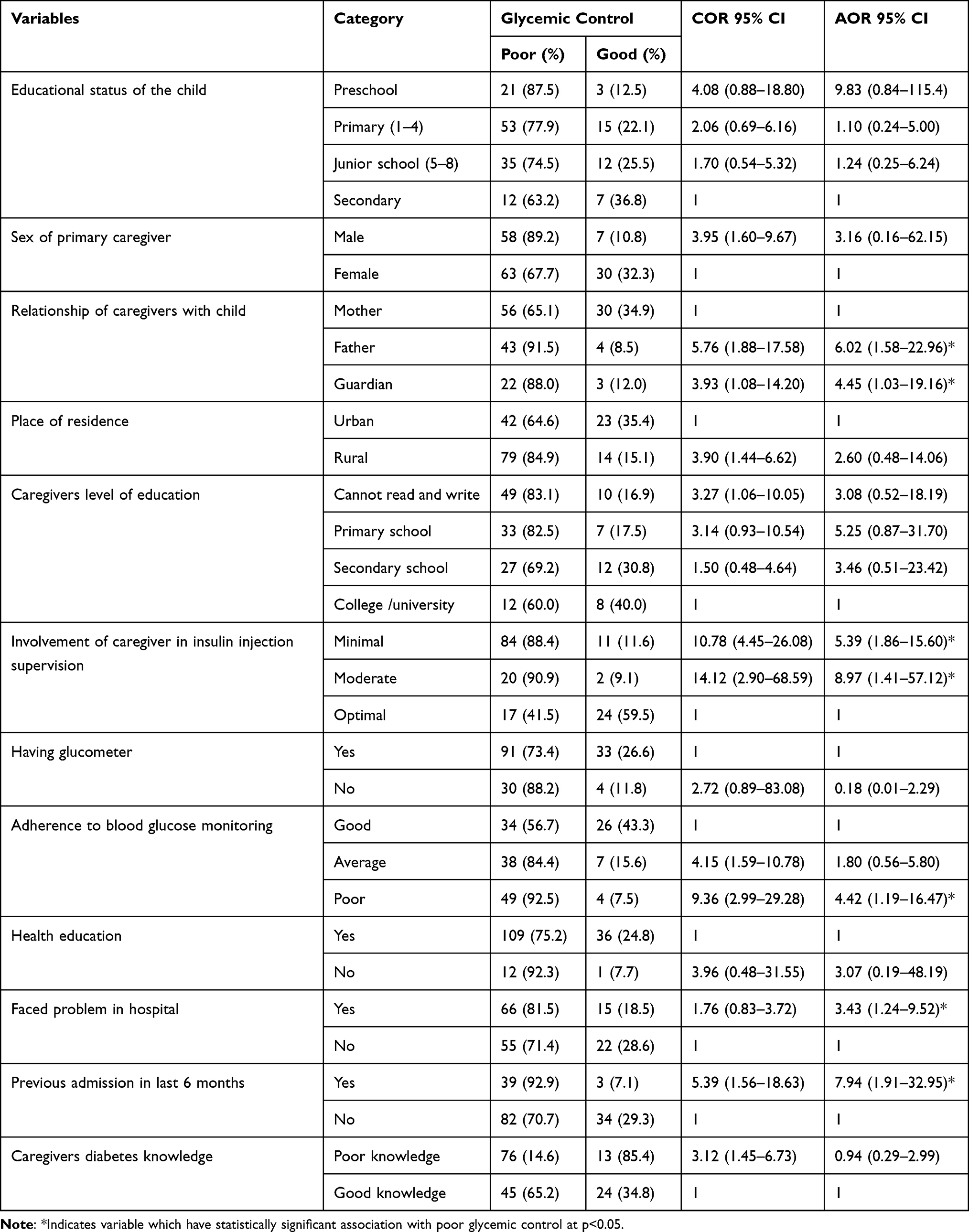 |
Table 5 Binary and Multivariable Logistic Regression Model to Identify Factors Associated with Poor Glycemic Control Among Children and Adolescents with Type 1 DM at Pediatric Follow Up Clinic, JMC, Southwest Ethiopia, 2022 |
Discussion
This study revealed that significant numbers of participants were having poor glycemic control, which accounts about 76.6%. The mean HbA1c in this study was 9.67 ± 2.28%, which is higher than the recommended target [7.5%]. This is alarming because children and adolescents with poor glycemic control are at risk of multiple complications of diabetes. This finding is in line with the studies done in Ethiopia (mean HbA1c was 9.6 ± 2.4%) and other resource-limited settings like Cameroon (mean HbA1c was 9.2% ± 2.5), Tanzania (mean HbA1c 11.1 ± 2.1%), and Southeast Niger (mean HbA1c was 10.5%). It is also consistent with the finding of study done in Sudan which showed the prevalence of poor glycemic control of 76%.7–9,11,16 This similarity in glycemic control could be due to the same poor socioeconomic status in these countries as poor socioeconomic status contributes to poor glycemic control through its undesired effects on quality of diabetes care, treatment adherence, and provision of adequate and healthy nutrition.17
According to this study regarding the nutritional status of children and adolescents with diabetes, about 22.2% were stunted. This finding is lower than study done in Rwanda, which showed the prevalence of stunting was 30.9%. This difference could be due to the sample size difference. This study is also consistent study done in Pune, India. The effect of diabetes on the nutritional status could be explained by the fact that insulin is an important regulator of growth hormone-related factors, specifically insulin-like growth factor (IGF-1) and insulin-like growth factor binding protein (IGFBP-3), disorders of insulin production can result in poor growth. In our study, there is no association between stunting and glycemic control, which is in line with the study done in Rwanda.18
This study revealed that more than half of the caregivers (56.3%) had poor level of diabetes knowledge, and this shows that many caregivers may have difficulty in managing their children’s diabetes, which might lead to many types of complications. This result is consistent with an Ethiopian study demonstrating the same finding.14 It is also in line with study from Tanzania, which mentioned that mothers had limited knowledge about diabetes mellitus though they did not mention the exact knowledge level. There is no statistically significant association between diabetes knowledge of caregiver and poor glycemic control, which is in line with the above study.7
In the current study, a primary caregiver other than the mother were one of the factors significantly associated with poor glycemic control. This is in line with the study done in Tanzania.7 This could be explained by the role that parents play in caring for sick children in the African societies, where it is the primary responsibility of the mother to care for sick children.
Minimal caregiver involvement in insulin injection supervision was also significantly associated with poor glycemic control. This is in line with study done in Southeast Nigeria, on sociodemographic determinants of glycemic control among children with type 1 diabetes, and found caregivers’ involvement in diabetes management was the only strong determinant for optimal glycemic control.8 This could be explained by some children may not take doses accurately when they take without supervision by the caregiver.
In this study, poor blood glucose monitoring adherence was associated with poor glycemic control. This is consistent with the study done in Tanzania.7 This might be due to the fact that participants who measure their blood glucose less frequently may not detect episodes of hyperglycemia or hypoglycemia and take necessary measures. In our setting due to limited resources, it could be because of lack of continuous supply of glucometer strips or the fact that most of the participant’s glucometer was not functional but this is just the observation of the authors and needs further studies on factors affecting the adherence to blood glucose monitoring.
Problems faced in the health facility were one of the variables that were significantly associated with glycemic control. Children who had faced problems which was mainly lack of insulin medication at hospital while seeking health service were more likely to have poor glycemic control. This might be the lack of insulin supply, which happens sometimes in the hospital because of limited availability of economic resources in our setup and obviously most of the parents in our setting may not afford to buy from the private pharmacies.
Admission to the hospital in the past 6 months were significantly associated with the poor glycemic control. This could be explained by the fact that admission to hospital by itself could be because of poor glycemic control. Children and adolescents should be monitoring their blood glucose level and health professionals and caregivers must work in integrity to support admitted children and adolescents with diabetes.
The strength of this study included that HbA1 measurements were done using the same machine for all participants and used many independent variables to look associations with outcome variable. However, this study does have some limitations. The cross-sectional nature of the study design and being conducted at a single follow-up site limiting the generalizability of these findings to all children and adolescents with diabetes are the main limitations of this study.
Conclusion
In conclusion, this study found that the level of glycemic control is poor in children and adolescents with type 1 diabetes mellitus. Factors associated with poor glycemic control include a caregiver other than the mother, minimal caregiver involvement in insulin injection, poor adherence to blood glucose-monitoring, problems faced during health care seeking and having history of hospital admission in the past 6 months.
Health education and counseling should be sustainable and long lasting; emphasis needs to be given to adherence counseling and active participation of caregiver in diabetes management tasks. Regular monitoring of glycemic control should be strengthened. We also recommend that health care constraints in our setting like lack of continuous supply of the insulin and lack of access to technologies such as continuous glucose monitoring and insulin pumps shall be solved. Additionally, putting strategies to sustain insulin supply shall also be considered. We also recommend more multicenter studies with a large number of participants.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; JMC, Jimma Medical Center; T1DM, Type 1 diabetes mellitus; HbA1c. Hemoglobin A1C (Glycated hemoglobin); WHO, World Health Organization; BMI, Body Mass Index; MUAC, Mid Upper Arm Circumference; ADA, American Diabetes Association; ETB, Ethiopian Birr; IDF, International Diabetes Federation; SPSS, Statistical Package for the Social Sciences; mg/dL, milligram per deciliter; mmol, millimole; RBS, random blood sugar; BGM, blood glucose monitoring; ISPAD, International Society for Pediatric and Adolescent Diabetes.
Ethics Approval and Informed Consent
Ethical clearance was obtained from Jimma University Institutional Review Board and permission to conduct the study was obtained from administration of Jimma Medical Center. After explaining the purpose of the study, written informed consent was obtained from each study participant’s caregiver. Assent was also obtained from adolescent participants. Confidentiality was assured by collecting data anonymously. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We are grateful to Jimma University for funding the study and also the study participants and data collectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. David R, Weber NJ. Nelson textbook of pediatrics. In: Diabetes Mellitus in Children. Vol. 21. Philadelphia: Saunders; 2007:2405.
2. Webber S. International Diabetes Federation; 2021.
3. Nathan DM. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37(1):9–16. doi:10.2337/dc13-2112
4. Care D, Suppl SS. 6. Glycemic targets: standards of medical care in diabetes. American Diabetes Association. Diabetes Care. 2022;42(January):S61–S70.
5. DiMeglio LA, Acerini CL, Codner E, et al. ISPAD clinical practice consensus guidelines 2018: glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes. Pediatr Diabetes. 2018;19:105–114. doi:10.1111/pedi.12737
6. McLarty RP, Alloyce JP, Chitema GG, Msuya LJ. Glycemic control, associated factors, acute complications of type 1 diabetes mellitus in children, adolescents and young adults in Tanzania. Endocrinol Diabetes Metab. 2021;4(2):1–8. doi:10.1002/edm2.200
7. Noorani M, Ramaiya K, Manji K. Glycaemic control in type 1 diabetes mellitus among children and adolescents in a resource limited setting in Dar es Salaam- Tanzania. BMC Endocr Disord. 2016;16(1):1–8. doi:10.1186/s12902-016-0113-y
8. Ogugua CF, Chikani UN, Okiche CY, Ibekwe UM. Sociodemographic determinants of glycemic control among children with type 1 diabetes in south eastern Nigeria. Pan Afr Med J. 2021;38:1–13. doi:10.11604/pamj.2021.38.250.19790
9. Taha Z, Eltoum Z, Washi S. Predictors of glucose control in children and adolescents with type 1 diabetes: results of a cross-sectional study in Khartoum, Sudan. Open Access Maced J Med Sci. 2018;6(11):2035–2039. doi:10.3889/oamjms.2018.423
10. Niba L, Aulinger B, Mbacham W, Parhofer K. Determinants of outcome of children with type 1 diabetes in Cameroon. Horm Res Paediatr. 2015;84:185.
11. Shibeshi MS, Daba AK, Meiso KM, Tadesse BT. Glycemic control among children and adolescents with diabetes in Southern Ethiopia: a cross-sectional study. BMC Endocr Disord. 2022;22(1):1–7. doi:10.1186/s12902-022-01070-y
12. Shibeshi MS, Fantahun B, Kebede T, Tilahun B. Pediatric diabetic retinopathy: experience of a tertiary hospital in Ethiopia. BMC Res Notes. 2016;9(1):1–6. doi:10.1186/s13104-016-1941-6
13. Meranti DIK. Michigan diabetes research and training center’s revised diabetes knowledge test; 2015. Available from: https://medicine.umich.edu/dept/diabetes/affiliated-centers/michigan-diabetes-research-center/resources/tools-health-professionals/survey-instruments.
14. Fenta F, Radie Y. Knowledge level of type 1 diabetes mellitus and associated factors among caregivers of children attending diabetic clinic in public hospitals of Addis Ababa City, Ethiopia, 2016; 2016.
15. Anderson B, Ho J, Brackett J, Finkelstein D, Laffel L. Parental involvement in diabetes management tasks: relationships to blood glucose monitoring adherence and metabolic control in young adolescents with insulin-dependent diabetes mellitus. J Pediatr. 1997;130(2):257–265. doi:10.1016/s0022-3476(97)70352-4
16. Djonou C, Tankeu AT, Dehayem MY, Tcheutchoua DN, Mbanya JC, Sobngwi E. Glycemic control and correlates in a group of sub Saharan type 1 diabetes adolescents 11 medical and health sciences 1117 public health and health services. BMC Res Notes. 2019;12(1):1–5. doi:10.1186/s13104-019-4054-1
17. Brown AF, Ettner SL, Piette J, et al. Socioeconomic position and health among persons with diabetes mellitus: a conceptual framework and review of the literature. Epidemiol Rev. 2004;26:63–77. doi:10.1093/epirev/mxh002
18. Endocrinologist P. Assessment of growth among children with type 1 diabetes mellitus: a cross-sectional study of factors contributing to stunting; 2016.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exposure to Atmospheric Ozone Disruption and Altitude Over 3500 m.a.s.l. are Associated with a Higher Prevalence of Photodermatoses in Pediatric Population of High-Altitude in Peru
Ramos W, Gutierrez EL, De La Cruz-Vargas JA, Díaz J, Hurtado J, Ronceros G, de Vries E
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1779-1786
Published Date: 31 August 2022
Management of Chronic Migraine in Children and Adolescents: Where are We in 2022?
Gibler RC, Knestrick KE, Reidy BL, Lax DN, Powers SW
Pediatric Health, Medicine and Therapeutics 2022, 13:309-323
Published Date: 9 September 2022
Body Image Dissatisfaction and Aggressive Behavior Among Chinese Children at Different Pubdertal Stages: A Path Analysis
Peng X, Cao R, Wang Y, Yao R, Han H, Han M, Fu L
Psychology Research and Behavior Management 2022, 15:2573-2586
Published Date: 14 September 2022
Evaluation of Risk Factors for Diabetic Peripheral Neuropathy Among Saudi Type 2 Diabetic Patients with Longer Duration of Diabetes
Alshammari NA, Alodhayani AA, Joy SS, Isnani A, Mujammami M, Alfadda AA, Siddiqui K
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3007-3014
Published Date: 28 September 2022
Lived Experiences of Newly Diagnosed Type 1 Diabetes Mellitus Children and Adolescents in Uganda
Nsamba J, Nabirye G, Hense S, Drenos F, Mathews E
Journal of Multidisciplinary Healthcare 2022, 15:2647-2665
Published Date: 18 November 2022