Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Global Trends of Cognition-Targeted Interventions in Chronic Lung Disease: A Bibliometric and Visualized Analysis
Authors Zhang J ![]() , Sun N, He C
, Sun N, He C ![]() , Liu L, Wan C, Luo J, Wu L, Zhang R, Lu J, Liu Z, Zhang W, Fang B
, Liu L, Wan C, Luo J, Wu L, Zhang R, Lu J, Liu Z, Zhang W, Fang B
Received 16 September 2025
Accepted for publication 25 January 2026
Published 10 March 2026 Volume 2026:21 567846
DOI https://doi.org/10.2147/COPD.S567846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Jirong Zhang,1,* Ning Sun,2,3,* Chenming He,1,* Liang Liu,1 Chuanqi Wan,1 Jielian Luo,1 Linguangjin Wu,1 Runze Zhang,1 Jiamin Lu,1 Zhankui Liu,4 Wen Zhang,1,* Bangjiang Fang1,4
1Department of Emergency, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Rehabilitation Medicine Center and Institute of Rehabilitation Medicine, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 3Key Laboratory of Rehabilitation Medicine in Sichuan Province, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 4Institute of Critical Care, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bangjiang Fang, Email [email protected] Wen Zhang, Email [email protected]
Purpose: To map the research landscape and synthesize randomized evidence on cognitive interventions for adults with chronic lung disease (CLD).
Methods: This two-stage study involved: (i) bibliometric mapping of Web of Science Core Collection (WOSCC) (Jan 2005–May 2025) to evaluate output, collaboration, and thematic trends via VOSviewer, CiteSpace, and Bibliometrix; and (ii) narrative synthesis of Randomized Controlled Trials (RCTs) in adults (≥ 18 y) with chronic lung diseases and validated cognitive outcomes, identified from WOSCC, Scopus, and PubMed (to May 1, 2025). Screening, data extraction, and RoB 2 assessment were conducted in duplicate.
Results: Bibliometric mapping (2005– 2025) of 3,474 publications showed sustained growth, broad international collaboration, and a shift from epidemiology to mechanisms and patient-centered outcomes. Fifteen RCTs, mostly in stable Chronic Obstructive Pulmonary Disease (COPD), assessed inspiratory-muscle/breathing training, aerobic-resistance or dance exercise, exercise with behavioral/educational components, multimodal cognitive-lifestyle programs, and pharmacological/nutritional or acute physiological therapies Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE) were the most common cognitive measures, alongside executive-function tests. Methodological quality was generally moderate.
Conclusion: Bibliometrics and randomized-trial synthesis reveal a rapidly growing, globally connected CLD-cognition field moving from epidemiology toward mechanistic and patient-centered research. Multimodal PR, especially exercise and inspiratory-muscle training, shows neurotherapeutic promise, but substantial gaps persist in Low and Middle Income Countries (LMICs) and non-COPD populations.
Keywords: chronic lung disease, cognitive impairment, bibliometric analysis, scoping review, lung–brain axis
Introduction
CLDs are a diverse group of respiratory diseases, including COPD, bronchial asthma, bronchiectasis, and interstitial lung disease (ILD), each of which causes substantial morbidity and mortality worldwide. According to the Global Burden of Disease (GBD) study, the prevalence of CLDs has steadily increased between 1990 and 2019,1 and these diseases continue to pose a significant public health burden.2 The GBD 2017 estimated that approximately 544.9 million people worldwide were living with CLDs in 2017, a 39.8% increase compared to 1990.1 The coronavirus disease 2019 (COVID-19) pandemic has resulted in a large number of survivors with persistent lung dysfunction, further expanding the high-risk population.3 Meanwhile, the GBD 2019 update further ranked CLDs as the third leading cause of death worldwide.4 The absolute global burden continues to rise due to an aging population and continued exposure to risk factors such as smoking and ambient air pollution.5,6 Long-term respiratory impairment reduces health-related quality of life and places significant strain on healthcare systems.7,8
Along with the growing burden of CLD, cognitive impairment, including mild cognitive impairment (MCI) and dementia, has become a major and rapidly expanding global health challenge.9 Currently, more than 50 million people worldwide suffer from dementia, and the associated economic costs are expected to increase nearly tenfold from $9.12 trillion in 2015.10 Epidemiological studies estimate that 3%–42% of adults aged 50 years and older have MCI.11 Cognitive impairment impairs functional independence and quality of life12 requires long-term care, and places a significant burden on families and healthcare systems.13 Given these impacts, dementia was ranked as the fifth leading cause of disability and dependency among older adults in 2016.14 Of note, CLD and cognitive impairment share several modifiable risk factors, such as smoking, hypoxemia, systemic inflammation, and vascular comorbidities, raising the possibility of a pathophysiological interaction between lung disease and neurocognitive impairment. Given the systemic nature of CLDs and their impact on oxygenation and inflammation, there is increasing recognition that respiratory impairment may contribute to neurocognitive decline.
There is growing evidence of clinically relevant crosstalk between CLDs and cognitive impairment. A recent meta-analysis of over 40,000 participants showed that decreased lung function increased the risk of MCI and dementia by 1.3 to 1.6 times.15 Population data from the Mayo Clinic Study of Aging confirmed this association, showing that COPD patients were almost twice as likely to develop MCI as age-matched controls.16 When the two diseases coexist, prognosis worsens. A prospective cohort study of community-dwelling older adults showed that patients with both COPD and cognitive impairment had a 55% increased rate of respiratory hospitalization and an 80% increased overall mortality compared with patients with COPD alone.17 Mechanistic hypotheses involve chronic and intermittent hypoxemia;18 systemic inflammation and autonomic dysregulation,19,20 among others. Despite these insights, systematic reviews have highlighted significant heterogeneity in study designs and diagnostic criteria, and a lack of longitudinal mechanistic studies in this interdisciplinary field.21
Therefore, we designed a comprehensive two-step study. In the first phase, bibliometric methods were used to map WOSCC records from 2005 to 2025 to quantify publication growth, focus on topic hotspots, and visualize the global collaborative network connecting CLDs and cognitive impairment research. By integrating macro-level bibliometric mapping with micro-level synthesis of randomized interventions, this study aims to generate a unified, evidence-based framework to guide future mechanistic and clinical research in the pulmonary–neurocognitive axis. Accordingly, we implemented a two-phase approach in which bibliometric mapping provided the structural overview, and trial-level synthesis supplied the clinical granularity needed to construct an evidence-based framework. Based on this, the second phase aggregated all randomized controlled trials (RCTs) found through WOSCC, Scopus, and PubMed, classified their intervention types, summarized key study characteristics, and assessed methodological quality using the RoB 2 tool. By combining macro-scientific mapping with descriptive synthesis of trial design and quality, this study generated a unified knowledge map that illuminated past progress and revealed evidence gaps in the pulmonary-neurocognitive axis. Based on this, the second phase aggregated all RCTs found through WOSCC, Scopus, and PubMed, classified their intervention types, summarized key study characteristics, and assessed methodological quality using the RoB 2 tool. By combining macro-scientific mapping with descriptive synthesis of trial design and quality, this study generated a unified knowledge map that illuminated past progress and revealed evidence gaps in the pulmonary-neurocognitive axis.
Method
In this study, we employed a two-step strategy. First, we conducted a bibliometric analysis of WOSCC records from 2005 to 2025 to map the scope, thematic evolution, and collaboration patterns in research on CLDs and cognitive impairment. The search was performed on 17 May 2025, covering publications from 1 January 2005 to 1 May 2025. It combined free-text and controlled vocabulary terms related to cognitive decline and CLDs, developed based on prior studies22,23 and expert consultation to ensure comprehensiveness. Only English-language articles and reviews were included, resulting in 3,474 records. Extracted data included publication year, country, institution, journal, citation counts, keywords, and co-authorship/co-citation networks. Visualisations of growth trends, thematic clusters, and collaboration maps were generated using VOSviewer 1.6.20, CiteSpace 6.4 R1, and the Bibliometrix package for R (v4.2). Given its descriptive nature, this step did not require risk-of-bias assessment.
Insights from the bibliometric analysis informed a subsequent systematic review of RCTs evaluating interventions targeting cognitive outcomes in adults with CLDs. Using the same lung- and cognition-related terms with an RCT filter, we searched WOSCC, Scopus, and PubMed up to 1 May 2025. Eligible trials enrolled adults (≥18 years) with diagnosed CLDs, compared pharmacological, rehabilitative, behavioural, or device-based interventions against control groups (eg, usual care, sham, placebo, or active comparator), and reported at least one validated cognitive outcome. We restricted inclusion to English-language publications to ensure consistent screening, data extraction, and risk-of-bias assessment across databases. We acknowledge that this language restriction may have excluded relevant non-English studies and could introduce language bias and potential publication bias. Two reviewers independently screened titles, abstracts, and full texts, resolving discrepancies by consensus. For each study, we extracted participant characteristics, intervention type and duration, cognitive outcomes, secondary respiratory or functional measures, and follow-up length; total sample sizes ranged from 20 to 647 participants (median 73.5; IQR 30–83). Risk of bias was assessed using the Cochrane RoB 2 tool. Due to heterogeneity in interventions and outcomes, results were synthesised narratively rather than quantitatively.
Both components followed the PRISMA extension for Scoping Reviews (PRISMA-ScR) and the RCT review also adhered to PRISMA 2020 guidelines. A summary workflow is presented in Figure 1.
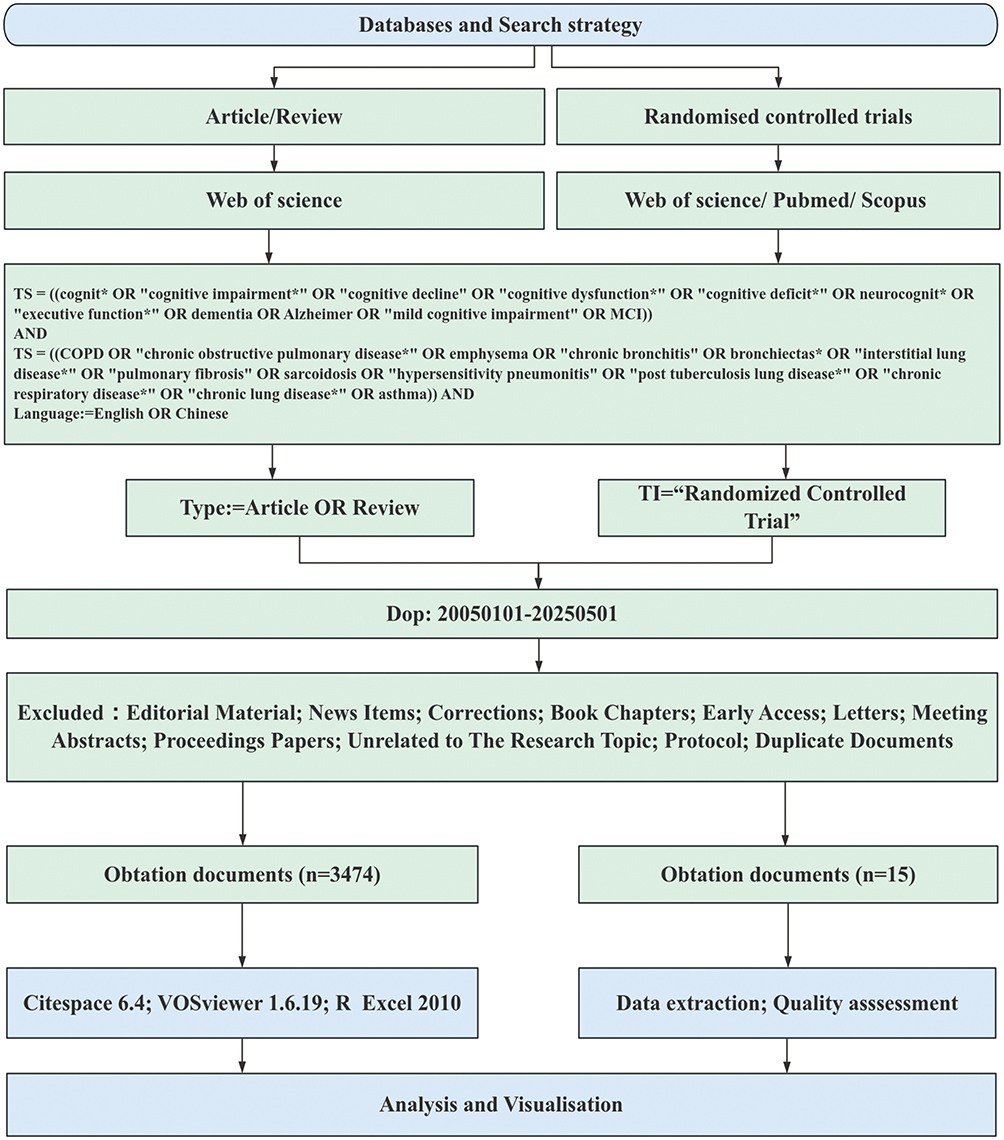 |
Figure 1 Flow chart of the progress of literature screening. |
Results
Quantitative Bibliometric Landscape
Analysis of Publications
Figure 2 shows the bibliometric landscape of CLDs and cognitive impairment from 2005 to 2025. Annual publications rose from 50 in 2005 to peaks of 311 in 2021 and 323 in 2024 (Figure 2A), fitting an exponential growth curve. Citation activity paralleled key milestones, with a sharp surge in 2012 (20,468 citations) and sustained levels above 8,000 through 2021, while recent downturns largely reflect citation lag and partial 2025 data (120 papers, 50 citations). In total, 3,474 publications in 1,291 journals were authored by 19,216 researchers, yielding a 10.3% annual growth rate, an average of 6.98 co-authors per paper, and notable international collaboration in 24.18% of publications. The literature cites 175,494 references, contains 7,107 unique author keywords, and achieves a mean article age of 7.4 years with an average of 44.19 citations per paper (Figure 2B), underscoring the field’s rapid expansion, collaborative ethos, and growing scientific influence.
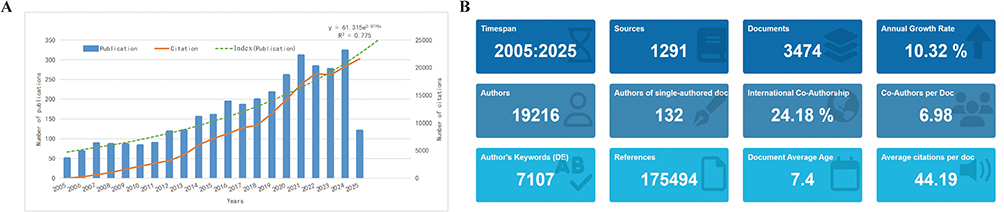 |
Figure 2 Analysis of publications (A) Global trends in research publications on CLDs and cognitive impairment over the past 20 years. (B) Summary of key descriptive bibliometric metrics. |
Geographical and Institutional Landscape
(Figure 3) Research spans 112 countries but is highly concentrated: the United States (1,026; 29.5%), China (418; 12.0%), and the United Kingdom (261; 7.5%) lead. Collaboration is strongest across a U.S.–Western Europe–China triad, with Africa and South America comparatively peripheral. Longitudinally, the US share declined from ~50% to ~33%, while China rose; other high-income countries remain stable Institutionally, Harvard (311), University of London (269), and the University of California system (247) lead, and co-authorship clusters center on Harvard, King’s College London, University of Washington, University of Toronto, and Maastricht University.
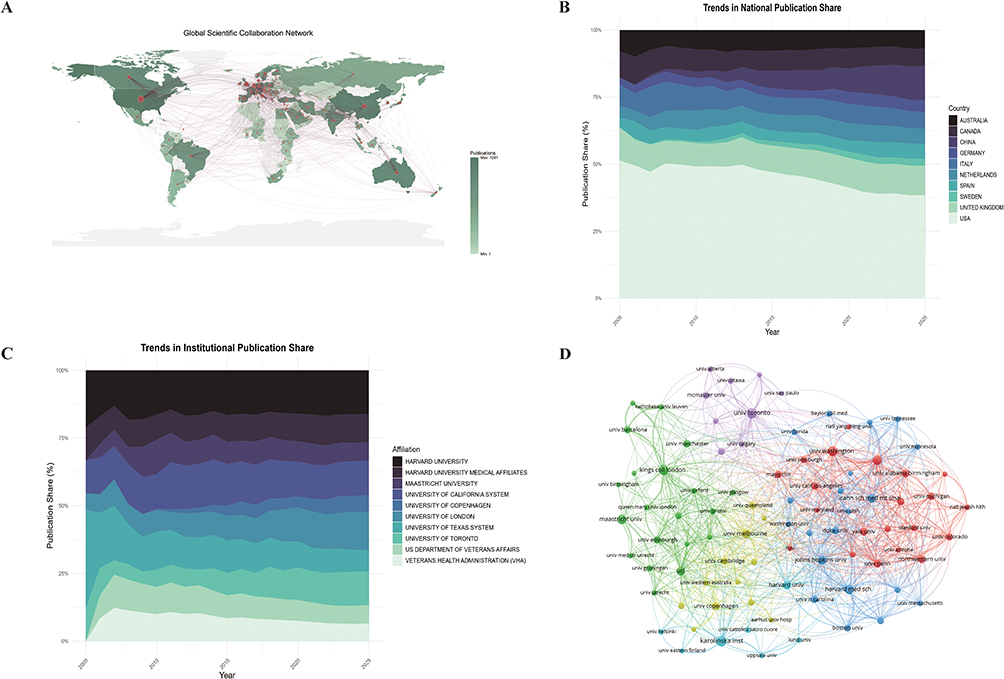 |
Figure 3 Analysis of institutions and Country-area cooperation network (A) National cooperation geographic map (B) Stacked area chart of percentage of publications by country over time (C) Stacked area chart of the percentage of papers published by institutions over time (D) Inter-institutional collaboration network map. |
Analysis of Authors and Co-Cited Authors
Top producers are JANSSEN DJA,24,25 FEDERMAN AD,26,27 and WOUTERS EFM28 (15 papers each; Supplementary Table S1). By co-author citations, PEDONE C,29 CORSONELLO A,30 and WOUTERS EFM lead (Supplementary Table S1). The author network forms six clusters dominated by a large group around JANSSEN DJA (Figure 4A), with smaller, specialized groups around JONES PW,31 CORSONELLO A, and PEDONE C. Country layering highlights the US, China, and UK as primary contributors (Figure 4B).From 2008 to 20255, productivity and citations rose for ZHANG J32 and Liu Y,33 whereas CORSONELLO A34 and PEDONE C35 peaked earlier (Figure 4C).
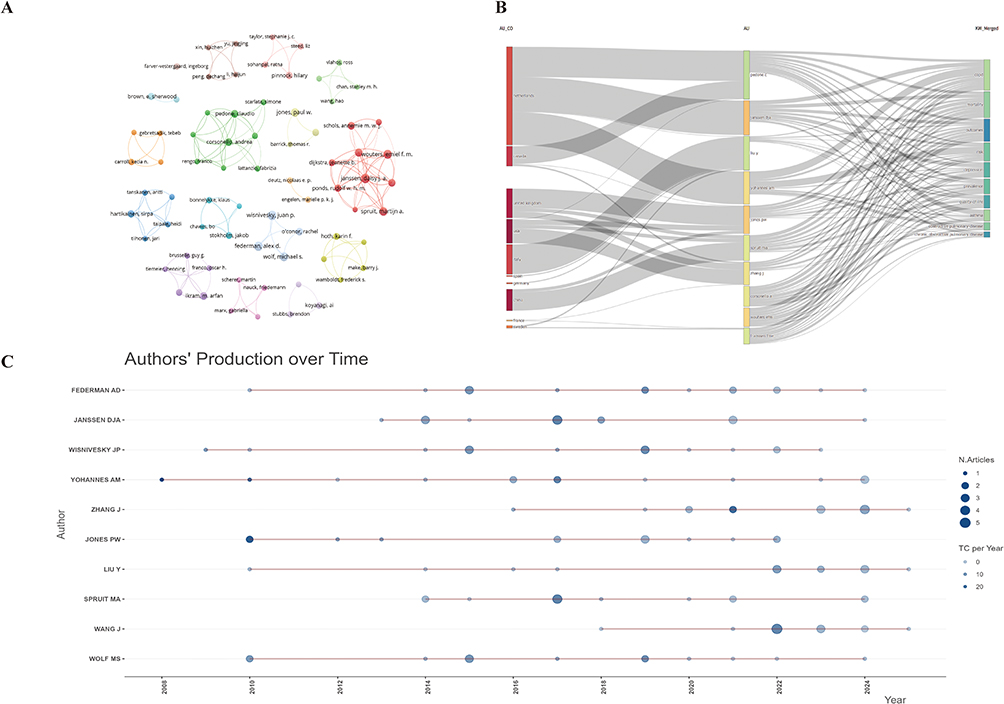 |
Figure 4 Analysis of Authors and co-cited authors. (A) A visual authors cooperation map for VOSviwer network. (B) Three-layer Sankey diagram of country-author-research topic. (C) Authors’ production over time. |
Analysis of References
The co-citation analysis of the top 10 seminal references (Supplementary Table S2) reveals three critical insights into the COPD cognitive dysfunction field. First, JW DODD36 dominates the foundational literature, contributing four high impact studies (Rank #1, #4, #7, #9), including the most cited paper (304 citations; Dodd, 2010) establishing cognitive impairment in stable COPD and its association with brain structure/function. Second, neurobiological mechanisms have received extensive attention, such as ORTA PAMUK37(2006) who found an association between cerebral perfusion defects and cognitive decline, and DODD38 (2012) who used multimodal magnetic resonance imaging (MRI) to detect brain structural changes. Third, these findings have been further confirmed by important clinical studies. RAFFAELE39 (2006) reported that decreased drawing ability was a predictor of mortality in patients with severe COPD, while Chang17 (2012) demonstrated that the coexistence of COPD and cognitive impairment has a compounding adverse effect on the elderly. In summary, these highly cited studies reflect a trend of interdisciplinary research that combines neurobiological insights with clinical outcomes, and these studies are mainly published in high impact journals.
The co-citation network (Figure 5A) identified ten robust clusters (Modularity Q = 0.867; mean Silhouette = 0.953). The largest cluster (#0, “chronic obstructive pulmonary disease”) occupies the hub position and is densely linked to clusters on “cognitive function” (#3), “cognitive behavioural therapy” (#2) and “risk factors” (#4), indicating that COPD-related cognitive mechanisms and interventions form the intellectual core of the field. A colour gradient for node age shows that most items in the “systematic review” cluster (#1) and in cluster #2 are warm coloured (ie, recently published) signalling that evidence syntheses and behavioural treatments are the current research frontier. By contrast, cooler colours dominate the “bronchial asthma” (#8) and “middle income countries” (#7) clusters, reflecting earlier foundational and epidemiological work. Two smaller clusters, “panic attack” (#6) and “common geriatric condition” (#9), highlight emerging extensions into psychiatric and gerontological domains.
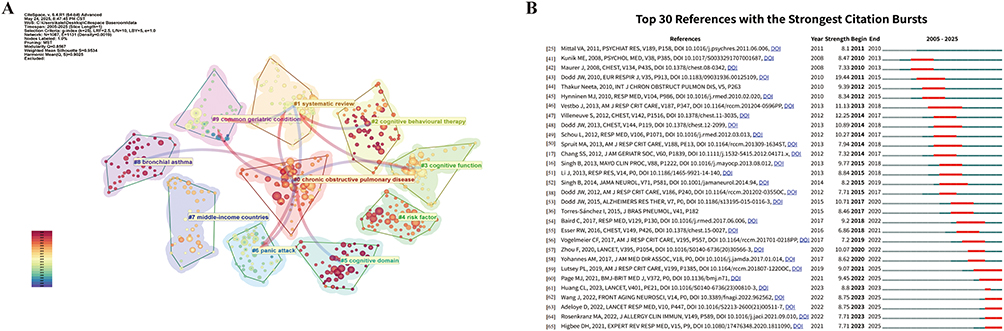 |
Figure 5 Analysis of reference outbursts (A) Citation cluster analysis (B) Top 28 references with the strongest citation bursts. |
Citation burst analysis (Figure 5B) reveals a distinct temporal progression in the evolution of influential literature, comprising three successive phases involving 30 high impact references. The first phase (2011–2015) was driven by DODD JW and MAURER J, who explored cognitive decline in COPD.25,40–43 The second phase (2013–2019) focused on guideline-directed research, risk factors, and PR, with contributions from VESTBO J and SPRUIT MA.16,17,38,44–50 The most recent phase (2020–present) sees the strongest citation bursts, with research centered on post-Covid sequelae, health equity, and methodological standards.36,51–63 These references reflect current research frontiers, particularly in viral sequelae, large-scale epidemiological studies, and evidence synthesis frameworks.
Keywords Analysis
Analysis of keyword evolution from 2005 to 2025 (Figure 6A) shows persistent research themes, such as COPD, Alzheimer’s disease, and oxidative stress, which have remained significant over the years. Recently, emerging topics like animal models, depression, and gene expression reflect increased interest in molecular mechanisms and psychological comorbidities in chronic diseases. The thematic map (Figure 6B) highlights key research areas, with quality of life and care management identified as dominant themes. In contrast, COPD risk, prevalence, asthma, Alzheimer’s disease, and inflammation remain underdeveloped, concentrated in the basic thematic quadrant. Oxidative stress and its related terms, expression and activation, bridge basic biological processes and disease contexts, indicating their growing research importance. Temporal trends in keyword usage (Figure 6C) reveal that while COPD, comorbidity, and chronic disease have maintained strong focus, recent years have seen a rise in anxiety, depression, and quality of life, highlighting a shift towards psychological and patient-centered outcomes. Figure 6D shows that keywords like oxidative stress, Alzheimer’s disease, asthma, and dose effect have experienced notable citation bursts in recent years, marking them as current research hotspots.
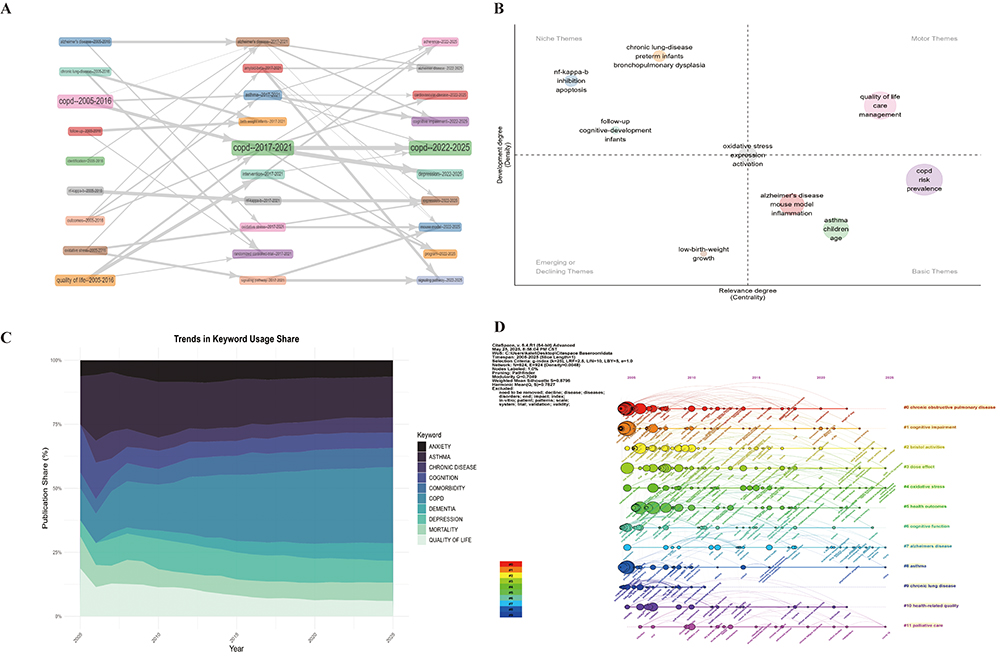 |
Figure 6 Analysis of keywords and keywords with strongest citation burst (A) Evolution of topics in the field of CLDs and cognitive impairment. (B) The thematic map of CLDs and cognitive impairment domains. (C) Keyword frequency percentage stacking chart over time - CLDs and cognitive impairment areas. (D) Timeline of keywords in the field of CLDs and cognitive impairment. |
The top 30 keywords with the strongest citation bursts from 2005 to 2025 (Figure 7) underscore the shifting research priorities. Early bursts were related to clinical and developmental topics such as follow-up, cognitive development, and bronchopulmonary dysplasia, with quality of life showing the highest burst strength (11.67) during 2006–2011. More recent bursts (from 2020 onward) focus on public health concerns like coronavirus disease 2019, global burden, frailty, stress, and model, reflecting growing attention to aging, systemic vulnerability, and post-pandemic health outcomes.
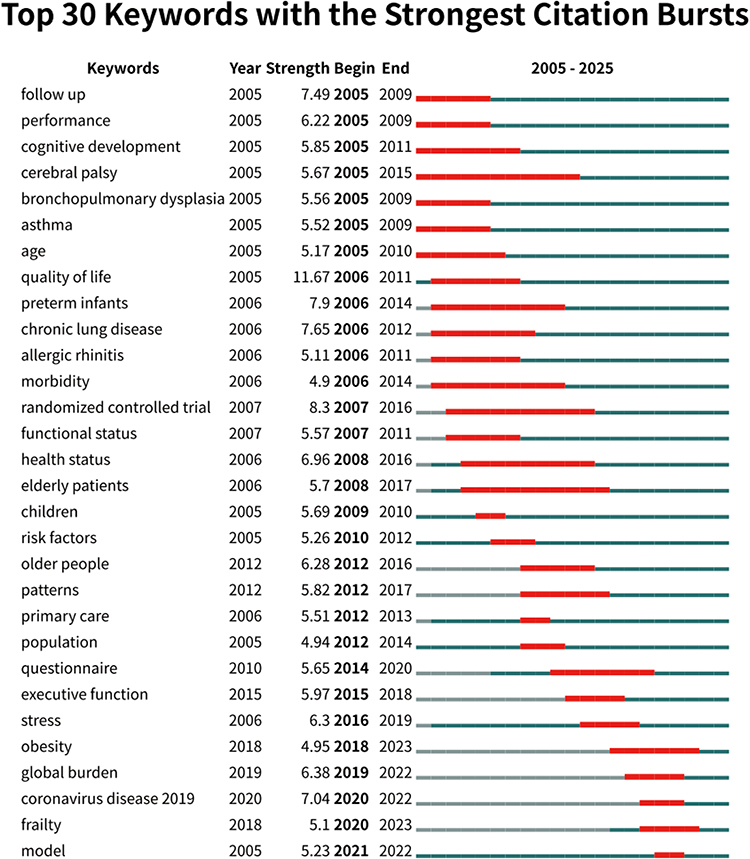 |
Figure 7 Top 30 keywords with the strongest citation bursts. |
Clinical Trial Evidence Synthesis
Study Selection and Participants
Of the 8,377 records retrieved from the three databases, 34 articles were selected after title and abstract screening; full-text review yielded 15 eligible RCTs (Table 1). The sample size of each trial ranged from 20 to 304. All trials, except one study of acute oxygen therapy,64 recruited patients with stable or mild-to-moderate COPD. CHENG65 restricted inclusion to male COPD patients with mild cognitive impairment; another study by SCHOU66 targeted patients within 24 hours of discharge from hospital after an acute exacerbation. Overall, the study population was predominantly male, aged 55–75 years, and heavy smokers, indicating that women and patients with severe hypoxemia were underrepresented. Notably, several trials were small and short-term, which may increase susceptibility to test–retest learning (practice effects) and expectancy effects in brief cognitive screening outcomes; therefore, short-term cognitive gains should be interpreted cautiously.
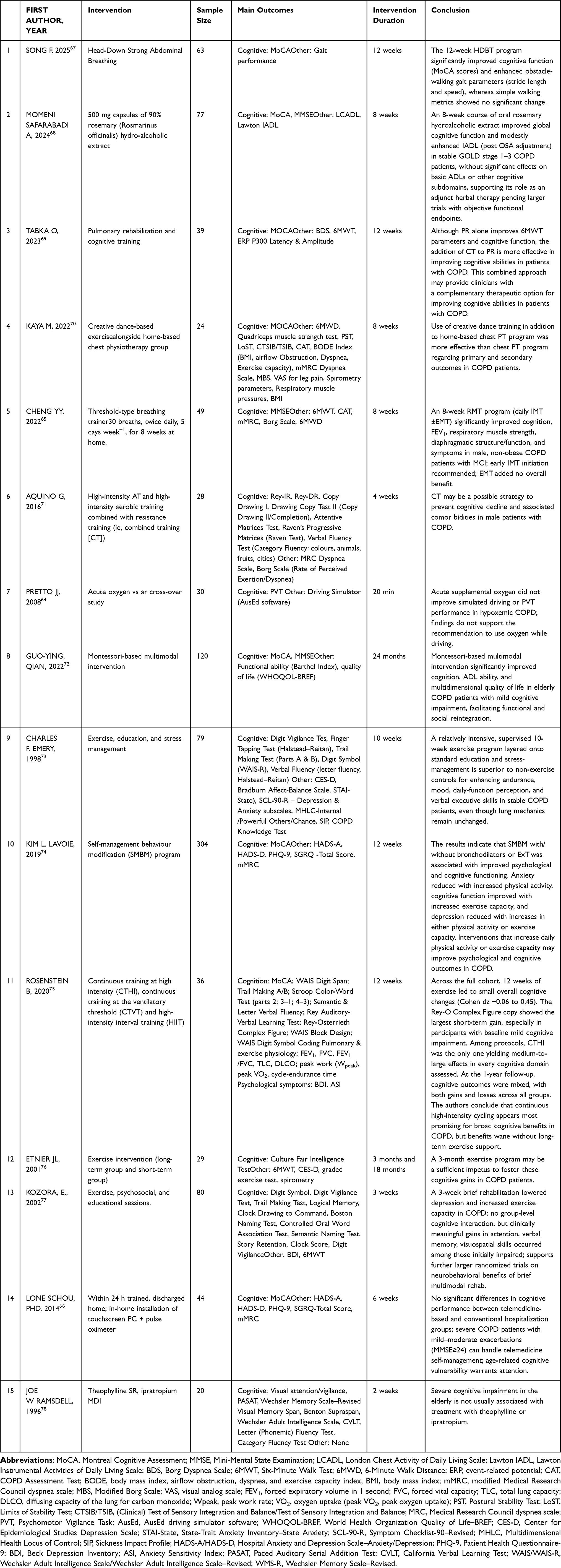 |
Table 1 15 Eligible RCTs |
Intervention Categories
Interventions clustered into five groups:
- Inspiratory muscle/breathing-pattern training (2 trials):65,67 tailored loading or rhythm training to improve ventilatory efficiency.
- Exercise programmes (5 trials):69–71,75,76 moderate- to high-intensity aerobic, resistance or dance training.
- Exercise plus behavioural/psychological/educational components (3 trials):72–74 PR combined with cognitive training, stress management, education or remote self-management.
- Multimodal cognitive-lifestyle intervention (2 trial):66,77 Montessori-based multi-sensory and daily-task training.
- Pharmacological, nutritional or acute physiological therapy (3 trials):64,68,78 antioxidant herbs, brief oxygen supplementation, or bronchodilator optimisation.
Four trials were short-term (≤ 4 weeks), eleven lasted 6–15 weeks, and two reported ≥ 12-month follow-up (Etnier 2001; Rosenstein 2020). The paucity of long-term data limits conclusions about durability of benefit.
Outcomes and Effect Patterns
The MoCA was the primary endpoint in eight trials; the MMSE in three. Executive, attention and memory domains were probed with Trail-Making, Stroop, Digit-Span, Rey and verbal-fluency tests. Functional indices (6-min walk, CAT, mMRC, Borg) were reported in most studies, allowing exploration of cognitive–clinical correlations.
Inspiratory-muscle training and moderate- to high-intensity exercise (interval cycling; combined resistance-aerobic; dance) consistently improved MoCA/MMSE scores and executive–memory domains, accompanied by gains in 6-min walk distance, FEV1, CAT, mood and ADL. Combined exercise-behavioural programmes and the Montessori intervention further enhanced daily function and quality of life. In contrast, single-session oxygen and short-term pharmacotherapy showed no immediate cognitive benefit, suggesting isolated physiological correction is insufficient to drive neuroplastic change.
Risk-of-Bias Assessment
RoB 2 appraisal showed only Pretto 2008 was low risk across all domains (Supplementary Table S3). Six trials (40%) adequately reported randomisation procedures; five (33%) showed low risk of deviations from intended interventions. Missing-data bias was low in seven trials (47%), but few performed sensitivity analyses. Measurement bias was lowest (12/15 trials, 80% low risk) owing to objective scales and assessor blinding. Reporting bias was most frequent (11/15 trials with some concern or high risk) due to absent preregistration and multiplicity adjustments. Overall quality was moderate, highlighting the need for improved random sequence generation, adherence monitoring and transparent reporting.
Discussion
General Information
This study conducted a comprehensive bibliometric analysis using WOSCC to examine the evolving knowledge landscape and research trends in CLDs and cognitive function. A total of 3,474 publications met the inclusion criteria, spanning 546 institutions across 112 countries, reflecting the field’s multidisciplinary and global scope. Publication output increased steadily, peaking in 2021, likely due to heightened public health awareness and the impact of the COVID-19 pandemic. Interestingly, citation frequency peaked in 2012, potentially linked to key publications and rising recognition of lung–brain comorbidity. After a brief decline in 2023—possibly due to shifting focus to pandemic recovery—output rebounded in 2024, perhaps reflecting renewed attention to CLDs and cognitive impairment in aging populations.
Geographically, the United States led with nearly one-third of publications, consistent with its established research infrastructure. Among the top authors, FRIED T.R. (Yale) and FEDERMAN A.D. (Mount Sinai) have notably contributed to advancing research on multimorbidity and cognitive decline. Fried emphasizes aligning care with patients’ cognitive trajectories and functional goals, while Federman highlights how poor health literacy combined with mild cognitive impairment hampers self-management in chronic illness, advocating integrated cognitive and educational support.
China ranked second (12%), the only developing country in the top three, followed by several European nations. Europe’s output reflects its high concentration of developed countries and strong international collaboration. Collaboration patterns showed developed countries tend to partner with each other, while developing countries more often form regional clusters. The marked rise in Chinese publications since 2010 likely reflects growing concern over aging-related health burdens. However, a gap remains in the global influence of institutions from developing regions, underscoring the need for more impactful research and equitable, cross-regional collaboration to address fragmentation in this field. Although we included English-language publications only, cross-validation of the RCT evidence through parallel searches in Scopus and PubMed substantially mitigated the potential bias arising from language restriction and database coverage.
Hotspots and Frontiers
Integrated Mechanism to Evidence Narrative
Evidence from external mechanistic and observational studies suggests that chronic hypoxaemia from asthma, pneumonia, or COPD triggers excess reactive oxygen species (ROS), which stabilise HIF-1α, activate NF-κB, and weaken tight-junction proteins—disrupting the blood–brain barrier (BBB) and priming microglia for neuroinflammation.79
Single-nucleus epigenomic data from Alzheimer’s cortex reveal that HIF-1α–dependent angiogenic stalling and BBB leakage occur early in neurodegeneration,80 while hypoxia induced BACE1 upregulation and Ca2⁺-mediated tau phosphorylation accelerate amyloid and tau pathology.81
Parallel shifts in the low biomass airway microbiome amplify systemic cytokine release and generate neuroactive metabolites that modulate microglial behavior.82
Multimodal MRI demonstrates frontoparietal network disintegration and accelerated grey-matter atrophy in COPD and interstitial lung disease, while rodent models show that interventions such as selective HIF-1α knock-down or ROS scavenging restore synaptic plasticity and memory.83 Fifteen RCTs support that targeting ventilatory mechanics and cardiopulmonary fitness yields cognitive benefits. Aerobic, resistance, or inspiratory-muscle training improved MoCA/MMSE by 1.8–3.5 points and enhanced executive function, walk distance, and FEV1 in COPD cohorts aged 55–75.65,67,69,71 Adding behavioural or cognitive components, such as CBT or creative therapies, amplified effects.67,73 In contrast, single-session oxygen or short pharmacologic treatments were largely ineffective.75
Despite these findings, methodological concerns persist. Only six trials reported robust sequence generation; one-fifth lacked blinding, and most were unregistered, resulting in moderate-to-high risk of bias. Severely hypoxaemic patients and non-smokers were under-represented, and few studies included follow-up beyond one year.
Future trials should adopt stratified randomisation, monitor adherence, apply sensitivity analyses, and use standardised outcome sets capturing both cognition and real-world function. Large, multi-centre trials embedded in standard care, coupled with sub-studies involving spirometry, multi-omics, microbiomics, and advanced neuroimaging, are needed to clarify dose response relationships, identify responders, and validate composite biomarkers for early risk detection along the lung–brain axis.
Multimodal, Patient-Centred Rehabilitation
Keywords such as “oxidative stress”, “cognitive function”, and “health outcomes” have gained prominence, reflecting a shift toward the lived experience of patients with CLDs. These terms align with the Global Alliance against Chronic Respiratory Diseases (GARD) initiative, which prioritises prevention and equity in the context of the Sustainable Development Goals. Topic clustering also highlights increased attention to vulnerable subgroups and end-of-life care. Recent surges in terms like “self-management” and “post-acute care” suggest a growing emphasis on quality of life (QoL), mental health, and sleep, outcomes that patients often value as much as—if not more than—traditional lung function indices.84 Notably, several bibliometric hotspots (eg, frailty, obesity/overweight, and related vulnerability constructs) are increasingly mirrored in the RCT literature. In these trials, pulmonary rehabilitation and multi-component programmes commonly target functional reserve, physical activity, weight/metabolic health, and patient-reported outcomes alongside cognitive measures, thereby strengthening the translational link from research priorities to interventional testing. Specifically, hotspots around hypoxemia/oxidative stress and patient-centred outcomes (eg, quality of life and self-management) are reflected in RCTs testing pulmonary rehabilitation packages, particularly exercise and inspiratory-muscle or breathing training, often supplemented with behavioural or educational components. However, mechanistic hotspots are still rarely incorporated as prespecified trial endpoints. Consistent with this convergence, in RCTs with an approximately 12-week intervention period, heterogeneous intervention packages were generally associated with potentially clinically relevant improvements in global cognition, with MoCA or MMSE increasing by approximately 1–3 points. These findings support the plausibility that multidomain, patient-centred strategies can translate into measurable neurocognitive benefit, although interpretation should remain cautious given between-trial heterogeneity. Patient-centered intervention strategies are increasingly supported by evidence. Community-based PR programmes delivered in non-clinical settings show comparable benefits in exercise capacity and disease-specific QoL to hospital-based care, despite low-to-moderate certainty. Trials such as the multicenter TANDEM study demonstrate that integrating brief cognitive behavioural therapy (CBT) into PR significantly improves anxiety, depression, and health status, without increasing provider burden. Digital approaches—such as smartphone-supervised PR—have reported non-inferior outcomes to centre-based PR, with the greatest benefits observed among highly adherent users and in rural settings.85 Collectively, these findings suggest that accessibility-oriented delivery models can preserve core PR benefits while potentially extending reach to populations facing structural barriers to rehabilitation.
These benefits may extend beyond psychological well-being. For example, a 3-week inpatient PR programme improved functional independence in patients with interstitial lung disease or COPD, indicating that even short, intensive formats may yield meaningful gains in daily function. Innovative formats are also emerging: Singing for Lung Health has been associated with improvements in QoL and well-being comparable to conventional physical training, although effects on core PR outcomes and cognitive endpoints remain uncertain. Taken together, the expanding portfolio of delivery formats and components underscores an ongoing shift from “one-size-fits-all” rehabilitation toward adaptable, preference-sensitive interventions that address physical, psychological, and cognitive domains.
The COVID-19 pandemic intensified interest in neurocognitive sequelae (eg, brain fog, memory loss, accelerated decline) and exposed persistent inequities in respiratory care.86 In low- and middle-income countries (LMICs), fragile health systems, service disruptions, and lockdown-related barriers exacerbated challenges in diagnosis, follow-up, and rehabilitation. Older adults with CLDs faced greater risks of severe infection,87,88 prolonged care gaps, worsened mental health, and potentially faster cognitive decline.87,89,90 Yet despite a rapidly growing burden in LMICs, most research still originates from high-income settings. Bridging this divide will require longitudinal cohorts with sufficiently long follow-up, culturally adapted screening and cognitive outcome measures (including education- and language-sensitive tools), and implementation strategies that embed equity from the outset—spanning community delivery, digital inclusion, workforce training, and context-appropriate models of PR and cognitive support.
Limitation
This study has several limitations. First, literature retrieval was limited to WOSCC due to difficulties standardizing raw data from other databases such as Scopus and PubMed, potentially reducing comprehensiveness. Second, restricting inclusion to English language publications may have introduced language bias. In addition, because the RCT evidence was synthesized narratively and trials were heterogeneous, we did not use funnel plots. Publication bias and selective reporting therefore cannot be excluded. Third, bibliometric analysis may not fully reflect evolving trends in a dynamic research landscape. Future studies should consider integrating multiple databases and qualitative analyses to provide a more comprehensive perspective.
Conclusion
This study provides an integrated view of the lung–brain axis in CLDs by coupling a field-level bibliometric map with a narrative synthesis of randomized trials, thereby extending prior reviews that largely examined epidemiology or clinical associations in isolation. The bibliometric analysis indicates sustained growth led by the United States, Europe, and China, alongside a thematic shift toward mechanisms and patient-centered outcomes, including hypoxemia and oxidative stress, BBB integrity, mood and sleep comorbidities, quality of life, and equity trends; however, LMICs and non-COPD phenotypes remain underrepresented. Across RCTs, multimodal pulmonary rehabilitation was most consistently associated with cognitive and functional improvements. Notably, among trials with a common intervention duration of 12 weeks, heterogeneous intervention packages were generally associated with clinically meaningful gains in global cognition, with MoCA or MMSE improving by approximately 1–3 points. Meanwhile, follow-up was predominantly short (8–12 weeks), and the longest follow-up among included studies was 15 months, limiting inference on durability and long-term decline trajectories. To better address the maintenance and progression of COPD-related cognitive impairment, future intervention studies should extend follow-up to ≥12 months, incorporate harmonized cognitive and functional endpoints, and embed mechanistic measures to link physiological pathways to cognitive change. Preliminary evidence from small trials suggests that community- or digitally delivered pulmonary rehabilitation may be feasible and potentially beneficial, but adequately powered, multicenter, preregistered RCTs with equity-focused implementation strategies are needed to strengthen effectiveness estimates, improve generalizability, and expand reach in LMICs and other underrepresented groups.
Abbreviations
CLDs, chronic lung diseases; WOSMCC, Web of Science Core Collection; COPD, chronic obstructive pulmonary disease; ILD, interstitial lung disease; GBD, Global Burden of Disease; MCI, mild cognitive impairment; ROS, reactive oxygen species; GARD, Global Alliance against Chronic Respiratory Diseases; QoL, quality of life; PR, pulmonary rehabilitation; CBT, cognitive behavioral therapy; PExT, physical exercise training; LMICs, middle-income countries.
Author Contributions
Jirong Zhang, Ning Sun, and Chenming He share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Natural Science Foundation of China (Project No. 82374350); National Traditional Chinese Medicine (TCM) Key Specialty Construction Project (2024YSZKZZYX006); National Natural Science Foundation of China (Project No. 82204890).
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–18. doi:10.1016/S2213-2600(20)30105-3
2. Zimmermann CM, Baldassi D, Chan K, et al. Spray drying siRNA-lipid nanoparticles for dry powder pulmonary delivery. J Control Release. 2022;351:137–150. doi:10.1016/j.jconrel.2022.09.021
3. Michalski JE, Kurche JS, Schwartz DA. From ARDS to pulmonary fibrosis: the next phase of the COVID-19 pandemic? Transl Res. 2022;241:13–24. doi:10.1016/j.trsl.2021.09.001
4. GBD. Chronic respiratory diseases collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
5. Labaki WW, Han MK. Chronic respiratory diseases: a global view. Lancet Respir Med. 2020;8(6):531–533. doi:10.1016/S2213-2600(20)30157-0
6. Quiros KAM, Nelson TM, Ulu A, Dominguez EC, Nordgren TM, Eskandari M. Fibrotic and emphysematous murine lung mechanics under negative-pressure ventilation. Am J Physiol Lung Cell Mol Physiol. 2025;328(3):L443–L455. doi:10.1152/ajplung.00087.2024
7. Sariaslan A, Sharpe M, Larsson H, Wolf A, Lichtenstein P, Fazel S. Psychiatric comorbidity and risk of premature mortality and suicide among those with chronic respiratory diseases, cardiovascular diseases, and diabetes in Sweden: a nationwide matched cohort study of over 1 million patients and their unaffected siblings. PLoS Med. 2022;19(1:e1003864. doi:10.1371/journal.pmed.1003864
8. Ascher K, Shafazand S. Dyspnea and quality of life improvements with management of comorbid obstructive sleep apnea in chronic lung disease. Sleep Med Clin. 2024;19(2):371–378. doi:10.1016/j.jsmc.2024.02.013
9. Gao Q, Zang E, Bi J, et al. Long-term ozone exposure and cognitive impairment among Chinese older adults: a cohort study. Environ Int. 2022;160:107072. doi:10.1016/j.envint.2021.107072
10. Jiang Q, Liu J, Huang S, et al. Antiageing strategy for neurodegenerative diseases: from mechanisms to clinical advances. Signal Transduct Target Ther. 2025;10(1):76. doi:10.1038/s41392-025-02145-7
11. Xu Z, Zhang D, Yip BH, et al. Combined mind-body physical exercise, cognitive training, and nurse-led risk factor modification to enhance cognition among older adults with mild cognitive impairment in primary care: a three-arm randomised controlled trial. Lancet Healthy Longev. 2025;6(4):100706. doi:10.1016/j.lanhl.2025.100706
12. van den Boogaard M, Schoonhoven L, Evers AW, van der Hoeven JG, van Achterberg T, Pickkers P. Delirium in critically ill patients: impact on long-term health-related quality of life and cognitive functioning. Crit Care Med. 2012;40(1):112–118. doi:10.1097/CCM.0b013e31822e9fc9
13. Nikmat AW, Al-Mashoor SH, Hashim NA. Quality of life in people with cognitive impairment: nursing homes versus home care. Int Psychogeriatr. 2015;27(5):815–824. doi:10.1017/S1041610214002609
14. GBD. Dementia collaborators. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(1):88–106. doi:10.1016/S1474-4422(18)30403-4
15. Li QY, Li XM, Hu HY, et al. Associations of lung function decline with risks of cognitive impairment and dementia: a meta-analysis and systematic review. J Alzheimers Dis. 2023;92(3):853–873. doi:10.3233/JAD-221136
16. Singh B, Parsaik AK, Mielke MM, et al. Chronic obstructive pulmonary disease and association with mild cognitive impairment: the mayo clinic study of aging. Mayo Clin Proc. 2013;88(11):1222–1230. doi:10.1016/j.mayocp.2013.08.012
17. Chang SS, Chen S, McAvay GJ, Tinetti ME. Effect of coexisting chronic obstructive pulmonary disease and cognitive impairment on health outcomes in older adults. J Am Geriatr Soc. 2012;60(10):1839–1846. doi:10.1111/j.1532-5415.2012.04171.x
18. Figat M, Wiśniewska A, Plichta J, et al. Potential association between obstructive lung diseases and cognitive decline. Front Immunol. 2024;15:1363373. doi:10.3389/fimmu.2024.1363373
19. Vemuri P, Graff-Radford J, Lesnick TG, et al. White matter abnormalities are key components of cerebrovascular disease impacting cognitive decline. Brain Commun. 2021;3(2):fcab076. doi:10.1093/braincomms/fcab076
20. Ogoh S. Chronic obstructive pulmonary disease-induced autonomic dysfunction may be associated with cerebral blood flow regulation and brain function. Exp Physiol. 2018;103(8):1045–1046. doi:10.1113/EP087173
21. Simargi Y, Mansyur M, Turana Y, et al. Risk of developing cognitive impairment on patients with chronic obstructive pulmonary disease: a systematic review. Medicine. 2022;101(25):e29235. doi:10.1097/MD.0000000000029235
22. Yang Z, Hotterbeex P, Marent PJ, Cerin E, Thomis M, van Uffelen J. Physical activity, sedentary behaviour, and cognitive function among older adults: a bibliometric analysis from 2004 to 2024. Ageing Res Rev. 2024;97:102283. doi:10.1016/j.arr.2024.102283
23. Lee M, Saver JL, Hong KS, et al. Cognitive impairment and risk of future stroke: a systematic review and meta-analysis. CMAJ. 2014;186(14):E536–E546. doi:10.1503/cmaj.140147
24. van Beers M, Mount SW, Houben K, et al. Working memory training efficacy in COPD: the randomised, double-blind, placebo-controlled cogtrain trial. ERJ Open Res. 2021;7(4):00475–2021. doi:10.1183/23120541.00475-2021
25. van Beers M, Janssen DJA, Gosker HR, Schols AMWJ. Cognitive impairment in chronic obstructive pulmonary disease: disease burden, determinants and possible future interventions. Expert Rev Respir Med. 2018;12(12):1061–1074.
26. Moritz G, Becker JH, Ankam JV, et al. Considering different montreal cognitive assessment cutoff scores for older adults with asthma. Allergy Asthma Proc. 2024;45(6):e72–e80. doi:10.2500/aap.2024.45.240045
27. Becker JH, Feldman JM, Arora A, Busse PJ, Wisnivesky JP, Federman AD. Cognition, symptom perception, and medication non-adherence in older adults with asthma. J Asthma. 2022;59(3):607–615. doi:10.1080/02770903.2020.1856867
28. Cleutjens FAHM, Ponds RWHM, Spruit MA, et al. The relationship between cerebral small vessel disease, hippocampal volume and cognitive functioning in patients with COPD: an MRI study. Front Aging Neurosci. 2017;9:88. doi:10.3389/fnagi.2017.00088
29. Tondo G, De Marchi F, Terazzi E, et al. Chronic obstructive pulmonary disease may complicate Alzheimer’s disease: a comorbidity problem. Neurol Sci. 2018;39(9):1585–1589. doi:10.1007/s10072-018-3470-7
30. Antonelli-Incalzi R, Corsonello A, Trojano L, et al. Screening of cognitive impairment in chronic obstructive pulmonary disease. Dement Geriatr Cogn Disord. 2007;23(4):264–270. doi:10.1159/000100773
31. Bajaj MK, Burrage DR, Tappouni A, Dodd JW, Jones PW, Baker EH. COPD patients hospitalized with exacerbations have greater cognitive impairment than patients hospitalized with decompensated heart failure. Clin Interv Aging. 2018;14:1–8. doi:10.2147/CIA.S185981
32. Ji X, Zhu Y, Ahmadizar F, et al. Cognitive decline before and after incident chronic respiratory disease. GeroScience. 2025;1–12.
33. Luo JF, Yang W, Liu Y, et al. Construction and evaluation of nomogram for risk prediction of cognitive impairment in chronic obstructive pulmonary disease comorbidity. BMC Psychology. 2025;13(1):1–15. doi:10.1186/s40359-025-02516-3
34. Incalzi RA, Corsonello A, Pedone C, et al. Construct validity of activities of daily living scale: a clue to distinguish the disabling effects of COPD and congestive heart failure. Chest. 2005;127(3):830–838. doi:10.1378/chest.127.3.830
35. Pedone C, Ercolani S, Catani M, et al. Elderly patients with cognitive impairment have a high risk for functional decline during hospitalization: the GIFA study. J Gerontol a Biol Sci Med Sci. 2005;60(12):1576–1580. doi:10.1093/gerona/60.12.1576
36. Torres-Sánchez I, Rodríguez-Alzueta E, Cabrera-Martos I, et al. Cognitive impairment in COPD: a systematic review. J Bras Pneumol. 2015;41:182–190. doi:10.1590/S1806-37132015000004424
37. Ortapamuk H, Naldoken S. Brain perfusion abnormalities in chronic obstructive pulmonary disease: comparison with cognitive impairment. Ann Nuclear Med. 2006;20(2):99–106. doi:10.1007/BF02985621
38. Dodd JW, Chung AW, van den Broek MD, et al. Brain structure and function in chronic obstructive pulmonary disease: a multimodal cranial magnetic resonance imaging study. Am J Respir Crit Care Med. 2012;186(3):240–245. doi:10.1164/rccm.201202-0355OC
39. Raffaele AI, Andrea C, Claudio P, et al. Drawing impairment predicts mortality in severe COPD. Chest. 2006;130(6):1687–1694. doi:10.1378/chest.130.6.1687
40. Kunik ME, Veazey C, Cully JA, et al. COPD education and cognitive behavioral therapy group treatment for clinically significant symptoms of depression and anxiety in COPD patients: a randomized controlled trial. Psycholog Med. 2008;38(3):385–396. doi:10.1017/S0033291707001687
41. Maurer J, Rebbapragada V, Borson S, et al. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4):43S–56S. doi:10.1378/chest.08-0342
42. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Eur Respir J. 2010;35(4):913–922. doi:10.1183/09031936.00125109
43. Thakur N, Blanc PD, Julian LJ, et al. COPD and cognitive impairment: the role of hypoxemia and oxygen therapy. Int J Chronic Obstr;2010. 263–269. doi:10.2147/copd.s10684
44. Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
45. Villeneuve S, Pepin V, Rahayel S, et al. Mild cognitive impairment in moderate to severe COPD: a preliminary study. Chest. 2012;142(6):1516–1523. doi:10.1378/chest.11-3035
46. Dodd JW, Charlton RA, van den Broek MD, et al. Cognitive dysfunction in patients hospitalized with acute exacerbation of COPD. Chest. 2013;144(1):119–127. doi:10.1378/chest.12-2099
47. Schou L, Østergaard B, Rasmussen LS, et al. Cognitive dysfunction in patients with chronic obstructive pulmonary disease–a systematic review. Respir Med. 2012;106(8):1071–1081. doi:10.1016/j.rmed.2012.03.013
48. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/european respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
49. Li J, Fei GH. The unique alterations of hippocampus and cognitive impairment in chronic obstructive pulmonary disease. Respir Res. 2013;14(1):140. doi:10.1186/1465-9921-14-140
50. Singh B, Mielke MM, Parsaik AK, et al. A prospective study of chronic obstructive pulmonary disease and the risk for mild cognitive impairment. JAMA neurol. 2014;71(5):581–588. doi:10.1001/jamaneurol.2014.94
51. Dodd JW. Lung disease as a determinant of cognitive decline and dementia. Alzheimer’s Res Ther. 2015;7(1):32. doi:10.1186/s13195-015-0116-3
52. Baird C, Lovell J, Johnson M, et al. The impact of cognitive impairment on self-management in chronic obstructive pulmonary disease: a systematic review. Respir Med. 2017;129:130–139. doi:10.1016/j.rmed.2017.06.006
53. Esser RW, Stoeckel MC, Kirsten A, et al. Structural brain changes in patients with COPD. Chest. 2016;149(2):426–434. doi:10.1378/chest.15-0027
54. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
55. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
56. Yohannes AM, Chen W, Moga AM, et al. Cognitive impairment in chronic obstructive pulmonary disease and chronic heart failure: a systematic review and meta-analysis of observational studies. J Am Med Directors Assoc. 2017;18(5):451.e1–451.e11. doi:10.1016/j.jamda.2017.01.014
57. Lutsey PL, Chen N, Mirabelli MC, et al. Impaired lung function, lung disease, and risk of incident dementia. Am J Respir Crit Care Med. 2019;199(11):1385–1396. doi:10.1164/rccm.201807-1220OC
58. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
59. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2023;401(10393):e21–e33. doi:10.1016/S0140-6736(23)00810-3
60. Wang J, Li X, Lei S, et al. Risk of dementia or cognitive impairment in COPD patients: a meta-analysis of cohort studies. Front Aging Neurosci. 2022;14:962562. doi:10.3389/fnagi.2022.962562
61. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
62. Rosenkranz MA, Dean IIIDC, Bendlin BB, et al. Neuroimaging and biomarker evidence of neurodegeneration in asthma. J Allergy Clin Immunol. 2022;149(2):589–598.e6. doi:10.1016/j.jaci.2021.09.010
63. Higbee DH, Dodd JW. Cognitive impairment in COPD: an often overlooked co-morbidity. Exp Rev Respirator Med. 2021;15(1):9–11. doi:10.1080/17476348.2020.1811090
64. Pretto JJ, McDonald CF. Acute oxygen therapy does not improve cognitive and driving performance in hypoxaemic COPD. Respirology. 2008;13(7):1039–1044. doi:10.1111/j.1440-1843.2008.01392.x
65. Cheng Y-Y, Lin SY, Hsu CY, et al. Respiratory muscle training can improve cognition, lung function, and diaphragmatic thickness fraction in male and non-obese patients with chronic obstructive pulmonary disease: a prospective study. J Personaliz Med. 2022;12(3):475. doi:10.3390/jpm12030475
66. Schou L, Østergaard B, Rasmussen LS, et al. Telemedicine-based treatment versus hospitalization in patients with severe chronic obstructive pulmonary disease and exacerbation: effect on cognitive function. A randomized clinical trial. Telemed J e-Health. 2014;20(7):640–646. doi:10.1089/tmj.2013.0224
67. Song F, Ding K, Sun W, et al. Effects of 12 weeks of head-down strong abdominal breathing training on gait and cognitive function in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2025;20:1347–1359. doi:10.2147/COPD.S514766
68. Momeni Safarabadi A, Gholami M, Kordestani-Moghadam P, Ghaderi R, Birjandi M. The effect of rosemary hydroalcoholic extract on cognitive function and activities of daily living of patients with chronic obstructive pulmonary disease (COPD): a clinical trial. Explore. 2024;20(3):362–370. doi:10.1016/j.explore.2023.09.008
69. Tabka O, Sanaa I, Mekki M, Acheche A, Paillard T, Trabelsi Y. Effect of a pulmonary rehabilitation program combined with cognitive training on exercise tolerance and cognitive functions among Tunisian male patients with chronic obstructive pulmonary disease: a randomized controlled trial. Chron Respir Dis. 2023;20:14799731231201643. doi:10.1177/14799731231201643
70. Kaya M, Gurses HN, Ucgun H, Okyaltirik F. Effects of creative dance on functional capacity, pulmonary function, balance, and cognition in COPD patients: a randomized controlled trial. Heart Lung. 2023;58:13–20. doi:10.1016/j.hrtlng.2022.10.017
71. Aquino G, Iuliano E, Di Cagno A, et al. Effects of combined training vs aerobic training on cognitive functions in COPD: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2016;11:711–718. doi:10.2147/COPD.S96663
72. Guoying Q, Haiqin C, Xinhua S, et al. Effects of Montessori multimodal intervention on cognitive function and quality of life in elderly patients with chronic obstructive pulmonary disease and mild cognitive impairment. J Clin Psychiatry. 2022;32(4):297–300.
73. Emery CF, Schein RL, Hauck ER, et al. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol. 1998;17(3):232. doi:10.1037/0278-6133.17.3.232
74. Lavoie KL, Sedeno M, Hamilton A, et al. Behavioural interventions targeting physical activity improve psychocognitive outcomes in COPD. ERJ Open Res. 2019;5(4):00013–2019. doi:10.1183/23120541.00013-2019
75. Rosenstein B, Smyrnova A, Rizk A, et al. Short-and long-term changes in cognitive function after exercise-based rehabilitation in people with COPD: a pilot study. Can J Respir Crit Care Sleep Med. 2021;5(5):300–309. doi:10.1080/24745332.2020.1790060
76. Etnier JL, Berry M. Fluid intelligence in an older COPD sample after short- or long-term exercise. Med Sci Sports Exerc. 2001;33(10):1620–1628. doi:10.1097/00005768-200110000-00002
77. Kozora E, Tran ZV, Make B. Neurobehavioral improvement after brief rehabilitation in patients with chronic obstructive pulmonary disease. J CardiopulmonarRehabi Prev. 2002;22(6):426–430. doi:10.1097/00008483-200211000-00008
78. Ramsdell JW, Henderson S, Renvall MJ, et al. Effects of theophylline and ipratropium on cognition in elderly patients with chronic obstructive pulmonary disease. Ann Allergy Asthma Immunol. 1996;76(4):335–340. doi:10.1016/S1081-1206(10)60034-8
79. Tsartsalis S, Sleven H, Fancy N, et al. A single nuclear transcriptomic characterisation of mechanisms responsible for impaired angiogenesis and blood-brain barrier function in Alzheimer’s disease. Nat Commun. 2024;15(1):2243. doi:10.1038/s41467-024-46630-z
80. Sun X, He G, Qing H, et al. Hypoxia facilitates Alzheimer’s disease pathogenesis by up-regulating BACE1 gene expression. Proc Natl Acad Sci U S A. 2006;103(49):18727–18732. doi:10.1073/pnas.0606298103
81. Kurbatskaya K, Phillips EC, Croft CL, et al. Upregulation of calpain activity precedes tau phosphorylation and loss of synaptic proteins in Alzheimer’s disease brain. Acta Neuropathol Commun. 2016;4:34. doi:10.1186/s40478-016-0299-2
82. Mumaw CL, Levesque S, McGraw C, et al. Microglial priming through the lung–brain axis: the role of air pollution–induced circulating factors. Faseb J. 2016;30(5):1880. doi:10.1096/fj.201500047
83. He FM, Liu Y, Guan Z, Li C, Zhang Z. Neuroimaging insights into lung disease-related brain changes: from structure to function. Front Aging Neurosci. 2025;17:1550319. doi:10.3389/fnagi.2025.1550319
84. Zhu Y, Zhu Y, Zhu Y, Ren Q, Zhou T. An analysis of the dynamic changes in the self-efficacy and quality of life of elderly patients with chronic obstructive pulmonary disease following community-based rehabilitation. Am J Transl Res. 2021;13(4):2745–2751.
85. Gloeckl R, Spielmanns M, Stankeviciene A, et al. Smartphone application-based pulmonary rehabilitation in COPD: a multicentre randomised controlled trial. Thorax. 2025;80(4):209–217. doi:10.1136/thorax-2024-221803
86. Popa E, Popa AE, Poroch M, et al. The molecular mechanisms of cognitive dysfunction in long COVID: a narrative review. Int J Mol Sci. 2025;26(11):5102. doi:10.3390/ijms26115102
87. Liu H, Yao Y, Yang Y, et al. Chronic lung diseases and depressive symptoms in older adults: insights from observational studies and Mendelian randomization. J Multidiscip Healthc. 2025;18:3465–3475. doi:10.2147/JMDH.S515745
88. Zhang X, Anzalone AJ, Dai D, et al. Chronic lung disease as a risk factor for long COVID in patients diagnosed with coronavirus disease 2019: a retrospective cohort study. Open Forum Infect Dis. 2024;11(8):ofae424. doi:10.1093/ofid/ofae424
89. Mekonen ZT, Fenta TG, Nadeem SP, Cho DJ. Global health commodities supply chain in the era of COVID-19 pandemic: challenges, impacts, and prospects: a systematic review. J Multidiscip Healthc. 2024;17:1523–1539. doi:10.2147/JMDH.S448654
90. Terry P, Heidel RE, Wilson AQ, Dhand R. Risk of long COVID in patients with pre-existing chronic respiratory diseases: a systematic review and meta-analysis. BMJ Open Respir Res. 2025;12(1):e002528. doi:10.1136/bmjresp-2024-002528
91. Edition F. Diagnostic and statistical manual of mental disorders. Am Psychiatr Assoc. 2013;21(21):591–643.
92. Hynninen MJ, Bjerke N, Pallesen S, et al. A randomized controlled trial of cognitive behavioral therapy for anxiety and depression in COPD. Respir Med. 2010;104(7):986–994. doi:10.1016/j.rmed.2010.02.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Application of ChatGPT in Medicine: A Scoping Review and Bibliometric Analysis
Wu J, Ma Y, Wang J, Xiao M
Journal of Multidisciplinary Healthcare 2024, 17:1681-1692
Published Date: 18 April 2024