")
Back to Journals » Journal of Pain Research » Volume 16
Global Trends in Research of Perioperative Analgesia Over Past 10 Years: A Bibliometric Analysis
Authors Zhou LZ, Li X, Zhou LM
Received 9 July 2023
Accepted for publication 26 September 2023
Published 19 October 2023 Volume 2023:16 Pages 3491—3502
DOI https://doi.org/10.2147/JPR.S429719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen M Soffin
Lian Zhen Zhou,1,* Xuan Li,2,* Li Min Zhou1
1Department of Anesthesiology, the Second Affiliated Hospital of Shandong First Medical University, Tai’ an, People’s Republic of China; 2Department of Anesthesiology and Pain Clinic, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Min Zhou, Department of Anesthesiology, the Second Affiliated Hospital of Shandong First Medical University, No. 366 Taishan Street, Tai’ an, Shandong Province, 271000, People’s Republic of China, Tel +86-17661211078, Email [email protected]
Background: The postoperative acute pain caused by surgery has been a major problem plaguing anesthesiologists, and even some acute pain progresses to chronic pain syndrome, terribly reducing the quality of life of patients. To this end, increasing attention has been paid to the management of perioperative analgesia. At present, with the increase of research on perioperative analgesia, the understanding and solution of this clinical problem have been further developed. Bibliometrics can estimate research hot-spots and trends of related fields in a certain period of time. However, a systematic bibliometric analysis has not been conducted to explore current research hotspots and future development trends, which is thus the purpose of this study.
Methods: Articles and reviews published from 2012 to 2021 were retrieved from the Web of Science Core Collection (WoSCC) database, and the bibliometric analysis of the keywords and references of articles was performed using VOSviewer1.6.18. Besides, the number of articles related to perioperative analgesia in term of countries, affiliations, authors, and journals were analyzed.
Results: Finally, 3157 articles meeting the screening requirements were retrieved, and it was hereby found that the research on perioperative analgesia had received more attention and interest in the past 10 years, with the United States making more contributions, where there were eight of the top ten affiliations by the number of publications. Kaye AD was the most active researcher in this field. Most related articles were published in Anesthesia and Analgesia, accounting for 2.76% of all literature. Enhanced recovery after surgery, different types of anesthesia and multi-mode analgesic drug intervention were the main trends and hotspots.
Conclusion: Perioperative analgesia has attracted considerable academic interest. In the past decade, the effects of enhanced recovery after surgery, different types of anesthesia and multi-mode analgesic drug intervention on perioperative analgesia have become the research hotspots, which are also likely to be the focus of future study.
Keywords: perioperative analgesia, pain, enhanced recovery after surgery, bibliometrics, VOSviewer
Introduction
Postoperative pain, ie, generally acute pain caused by surgical injury, has always been one of the main problems in the perioperative period, with an incidence of 20–40% in postoperative patients,1 which, fortunately, can be controlled, and most of the pain can be eliminated within a week. However, some of these patients bear acute postoperative pain that lasts longer than the time required for normal tissue healing and becomes chronic postoperative pain (CPSP), with a prevalence of about 10%.2
Both acute pain and chronic pain expose patients to unpleasant emotional experience, physical and even mental pain. Chronic pain greatly reduces the quality of life of patients, making it necessarily important to take preventing measures. Good perioperative analgesia can not only reduce postoperative acute pain, but also effectively prevent the occurrence of chronic pain, thereby improving the quality of life of patients after discharge.
Postoperative pain is inadequately controlled in 80% of patients in the United States, indicating the extraordinary significance of investigations into perioperative analgesic methods.3 At present, the methods of perioperative analgesia include local anesthesia, the use of non-opioid and opioid analgesics, and multi-mode analgesia.4–7 Considering the difficulty of achieving favorable postoperative analgesia effect by using a single drug or a particular anesthetic technique, most doctors adopt multi-mode analgesia in clinical practice. This method refers to the use of several different analgesic drugs or analgesic techniques at the same time to maximize postoperative analgesia through multiple mechanisms and to reduce the use of opioids. Studies have shown that multi-modal analgesia may affect the chain of mechanical events leading to postoperative chronic pain.8
Although some achievements have been made in clinical research, more studies are still needed to evaluate the effect of different perioperative analgesia methods on postoperative analgesia and prevention of long-term chronic pain. Therefore, quantitative analyses of perioperative analgesic related research situation, research hot spot and the future prospects are of great significance to the development of this field.9,10
Bibliometrics represents the study of academic publications that uses statistics to describe trends in the field and to highlight relationships between published works.11 As a convenient method, bibliometrics can estimate the research hot-spots and trends of related fields in a certain period of time and reveal the key research directions by analyzing the characteristics of databases and documents.12 Over the years, the fruits of bibliometric analysis has been extensively used in rheumatism, bone, internal medicine and other fields.13–15 However, bibliometric study on perioperative analgesia remains a void. To this end, literature on perioperative analgesia was hereby systematically analyzed to evaluate the current status and hot spots in this field, so as to provide guidance for the study and selection of perioperative analgesia.
Methods
Data Source and Search Strategies
Herein, SCI-expanded of WoSCC bibliographic database was used as the data source, and the searching was conducted on April 5, 2022. The search term was presented as TS= (PERIOPERATIVE ANALGESIA), and the publication period was set between 2012 and 2021. Articles of the “Article” and “Review” categories were screened, in with those in languages other than English removed. Then, the publication dates of each article on the Web of Science were checked, and articles not published during 2012–2021 were removed. Finally, a total of 3157 articles were acquired. Two researchers independently conducted the primary data search and then discussed any potential differences, the kappa score reached 0.98, showing substantial accordance. All literature data were exported in the form of ‘Full record and cited references’ and imported into the Endnote X 9 software for rechecking. (The detailed screening is shown in Figure 1.)
 |
Figure 1 Flowchart of the screening process. |
Bibliometric Analysis
In this study, number of publications, number of citations without self-citations, H-index and impact factor were chosen as the indexes of bibliometric analysis. Number of publications (Np) was used for measuring productivity, with a higher Np indicating more researchers involved in the field. Number of citations without self-citations (Nc) was used to represent the impact, which was considered a good indicator to evaluate the level of research. H-index assesses the scientific contributions of researchers in relevant fields and predicts future research outcomes by combining the number and impact of publications.16,17 Although originally developed to assess academic achievements of an individual, the H-index could also be extended to describe the output of publications in a country or region, institution, or journal.16,18 Besides, impact factor (IF) is one of the most reliable methods for evaluating the quality of scientific journals and has been widely used in evaluating medical journals.
VOSviewer is a software for building and viewing bibliometric graphs, which can build visual graphs based on the data of co-citation and co-occurrence of keywords.19 The analysis of co-citation and co-occurrence can explore the hot spot and research direction of perioperative analgesia.
Results
An Overview of Publications on Perioperative Analgesia
Based on the search strategy, a total of 3157 articles and reviews published in the past decade were hereby retrieved. The total Nc of the retrieved articles was 45,619, with an average Nc of 14.45 per article, and the H-index was 86 for all publications.
Annual Trends in the Number of Publications
Figure 2A shows the number of publications related to perioperative analgesia over the past decade. Overall, while the number of publications fluctuated over the past decade, the overall number of publications jumped from 142 in 2012 to 507 in 2021. Figure 2B presents the growth trend in the number of publications per year. There was a positive correlation with a correlation coefficient (R2) of 0.9559 between the number of publications and the year indicating an increasing trend in the research of perioperative analgesia. Figure 2C exhibits a comparison of the number of publications published each year in the United States, China, and Canada. The number of publications in the United States and China has been growing rapidly each year, while that in Canada remains relatively stable.
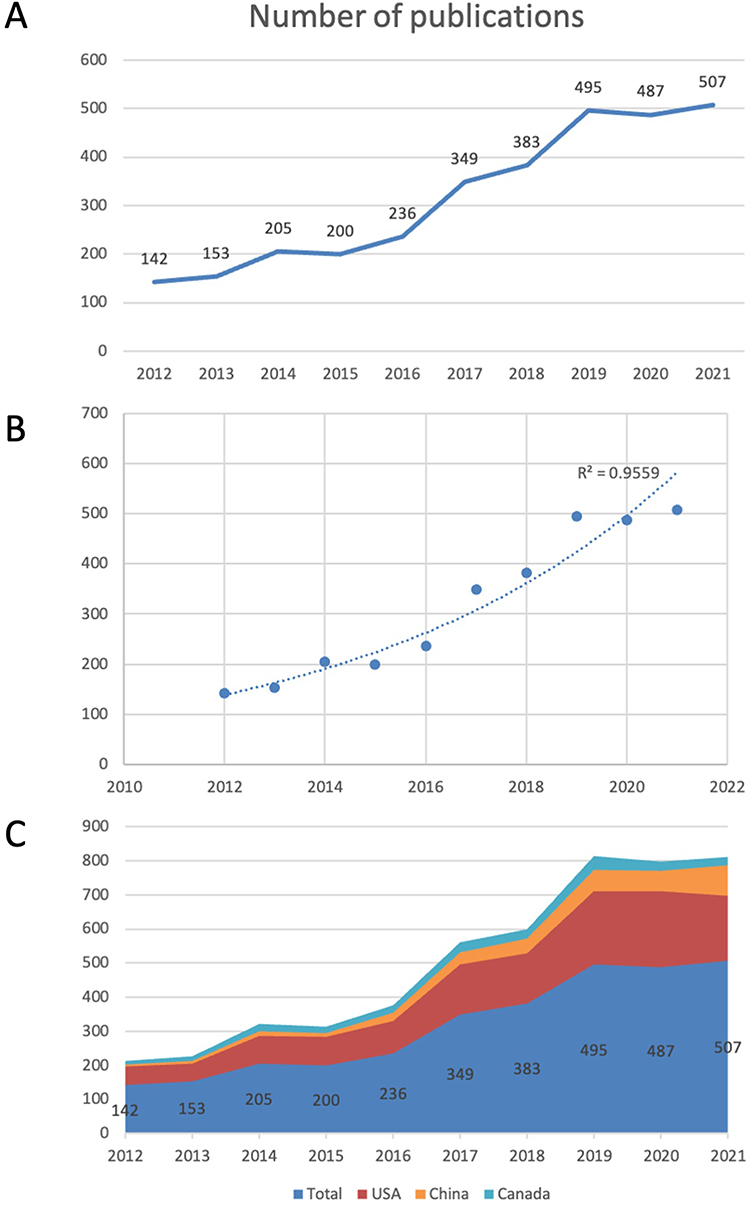 |
Figure 2 (A) The number of articles published annually in this field over the past decade. (B) The fitting curve of the annual number of publications and the year. (C) The top three countries in terms of number of publications. |
Contributions of Countries/Regions to Global Publications
Table 1 shows the top ten countries/regions for publications. Compared with second-place China (358,11.34%) and third-place Canada (233,7.38%), most articles (1,287,40.77%) were published in the United States. In terms of either Nc or H-index, the United States was far ahead of the rest of the world. In comparison, there were fewer publications in Canada and the UK than in China, but both their Nc and H-index outperformed. Meanwhile, Germany had a relatively low circulation and a higher Nc and H-index when compared with India. The same was true of Italy and Australia.
 |
Table 1 The Top 10 Most Productive Countries/Regions |
Analysis of Affiliations
Table 2 shows the top 10 affiliations for the number of publications, where it could be observed that Harvard had the largest number of publications (132), followed by League of European Research Universities (131) and the University of California system (107). The League of European Research Universities had the highest number of non-self-references (8279) and the highest h-index (46). More than half of the institutions in the top 10 were from the United States (8), with the remaining two from Europe (League of European Research Universities) and Canada (University of Toronto).
 |
Table 2 The Top 10 Most Productive Affiliations |
Analysis of Authors
Table 3 presents the authors of the top 10 publications, who published a total of 216 articles, ie, 6.84% of the total number of papers. The largest number of publications was Kaye AD (33), followed by Urman RD (30), Cata JP and Wu CL tied for the third (23). The Nc of Demartines N was the highest (3494). Wu CL, Demartines N and Ljungqvist O tied for first place in the H-index (15). More than half of the top 10 authors are from the United States (6).
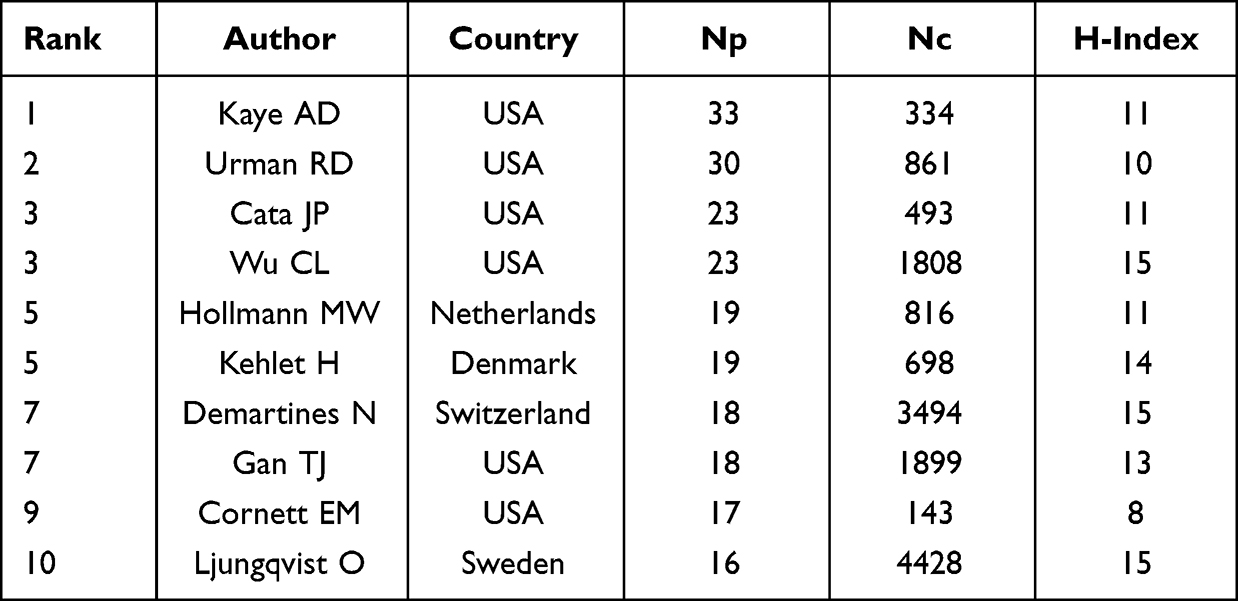 |
Table 3 The Top 10 Most Productive Authors |
Analysis of Journals
Table 4 shows the top 10 journals of publications, involving a total of 556 published articles, ie, 17.61% of the total number of publications. ANESTHESIA AND ANALGESIA (87, IF: 5.178) published the most literature on perioperative analgesia, followed by CURRENT OPINION IN ANESTHESIOLOGY (64, IF: 2.706) and BRITISH JOURNAL OF ANAESTHESIA (58, IF: 9.166). Both Nc (2945) and H-index (33) of ANESTHESIA AND ANALGESIA were in first place. JOURNAL OF CLINICAL ANESTHESIA had the highest IF (9.452). Besides, of the top 10 journals, half had a high IF (defined as more than 5.000).
 |
Table 4 The Top 10 Most Active Journals |
Analysis of Co-Cited References
A co-citation relationship indicates the situation of two (or more) articles citing the same article. Co-citation emphasizes research topics closely related to a particular field. Of the 74,448 references cited in the retrieved papers, the minimum number of references was set to 35, and 133 references were screened for co-citation analysis (Figure 3). A line between the two nodes indicates that both are referenced in a publication, while shorter and thicker lines indicate a closer relationship between the two articles. The size of the node represents the total number of references of the article. In addition, nodes of different colors divide the article into different groups. Herein, Group 1 (Red), consisting of 42 references, focused on enhanced recovery after surgery (ERAS) and explored the efficacy of epidural analgesia as a method of postoperative analgesia;20–32 Group 2 (Green), consisting of 42 references, explored the effects of different adjunctive analgesics on multi-modal postoperative acute pain management;33–45 Group 3 (Blue), consisting of 15 references, focused on the safety and efficacy of intravenous lidocaine for postoperative analgesia and recovery;46–49 Group 4 (Yellow), consisting of 15 references, focused on the exploration of methods to reduce postoperative opioid use;50–56 Group 5 (Purple), consisting of 14 references, highlighted the impact of the selection of perioperative anesthetic methods and the use of analgesics on postoperative recurrence or survival after cancer surgery.57–60 As shown in Figure 3, the co-citation literature of Group 4 was relatively new, indicating the emergence of clinical research on reducing opioid use in recent years. Possibly given Group 5 focused more on postoperative recurrence and survival than on postoperative pain, Group 5 was not closely associated with the other groups.
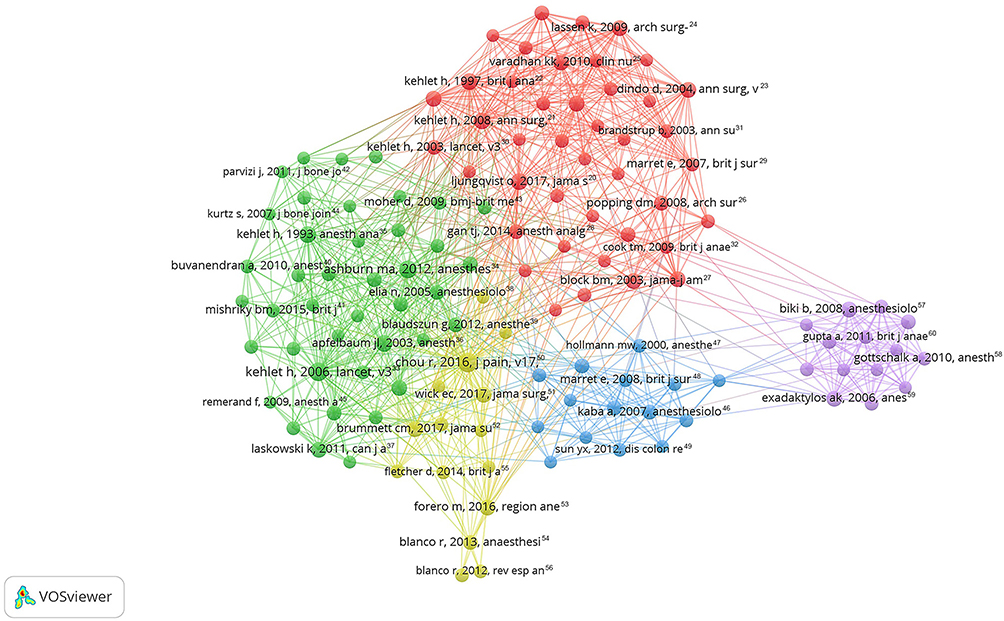 |
Figure 3 Network map of co-cited references. Among the 74,448 references, 133 references (divided into five groups: group 1: Red, group 2: Green, group 3: Blue, group 4: Yellow, group 5: Purple) were cited at least 35 times. |
Analysis of Research Hotspots
Co-occurrence analysis explores recent research hotspots. The co-occurrence of two keywords in a literature is called a co-occurrence relationship. Of the 4788 keywords in the 3157 articles included in the study, the minimum co-occurrence of keywords was set to 30, and 129 keywords were screened out for co-occurrence analysis (Figure 4). Figure 4A shows that the 129 keywords were divided into five groups. Group 1 (Red) focused on the effects of different drugs and perioperative analgesia techniques on postoperative pain; Group 2 (Green) studied the effect of different anesthetics on perioperative analgesia; Group 3 (Blue) studied the effect of different anesthesia methods on the recurrence rate and survival rate after cancer operation; Group 4 (Yellow) explored the effect of ERAS on perioperative recovery and length of hospital stay in patients undergoing different procedures; Group 5 (Purple) highlighted the management of perioperative pain and recovery. The most common keywords were “Analgesia” (751 times), followed by “Surgery” (584 times) and “Postoperative analgesia” (499 times). Figure 4B describes a visualization by VOSviewer of the colors of all keywords by average publication year (APY). The latest keywords were “Dexmedetomidine” (APY: 2018.92), followed by “Enhanced recovery” (APY: 2018.90), “Liposomal bupivacaine” (APY: 2018.74), and “Paravertebral block” (APY: 2018.69). In addition, contrasting Figures 4A and B, “Dexmedetomidine” (APY: 2018.92) became the most recent drug for perioperative analgesia in recent years.
 |
Figure 4 The mapping on keywords related to perioperative analgesia research. (A) 129 keywords were divided into 5 groups by different colors (group 1: Red, group 2: Green, group 3: Blue, group 4: Yellow, group 5: Purple) with the minimum co-occurrence times of 30. The size of the node represents the co-occurrence frequency and the closeness of the co-occurrence relationship with other keywords. (B) Visual network map of keywords according to the APY. The more yellow the node is, the later the keyword occurrences. |
Figure 5 shows the density visualizations and hotspots of co-occurrence keywords. Considering the huge amount of keywords, the minimum number of co-occurrences was set to 50 to highlight the more frequent keywords. Finally, 69 high-frequency keywords were selected. High-frequency words, such as surgery, anesthesia, analgesia, management, and postoperative pain, were still prominent. It should be noted that although the frequency of general-anesthesia, local-anesthesia, regional-anesthesia, epidural-anesthesia and spinal-anesthesia was not particularly high, they were located in the center of the map, indicating their close relationship with other keywords.
 |
Figure 5 Density visualization map for 129 keywords. Each keyword in the density map shows the frequency of its occurrence in related research fields. Red represents the high-frequency keyword, and the position of the keyword is related to the degree of correlation between it and other keywords. The position in the center indicates the stronger correlation with the others. Abbreviations: WoSCC, Web of Science Core Collection; Np, the number of publications; Nc, the number of citations without self-citations; IF, impact factor; ERAS, enhanced recovery after surgery; APY, average publication year. |
Discussion
In this study, a bibliometric analysis of 3157 articles retrieved from the Web of Science Database was conducted, and a visual analysis was carried out with VOSviewer to explore the hotspots and development trend of perioperative analgesia. By fitting the curve, it is found that the number of publications in this field has increased almost exponentially in the last ten years, especially in the last five years, and the number of publications has increased more than three times in the last ten years.
Most of the high-ranking authors and institutions come from the United States, indicating the absolute advantage of researches of the United States in this area. Besides, the United States is the country with the most researches and the most in-depth researches on perioperative analgesia. Although China had the second-largest number of publications in the last decade, its H-index lags far behind that of the UK and Canada, suggesting that Chinese academics and research institutions need to do more in this area of research to balance the quantity and quality of articles in the field. India and Turkey are also facing the same situation.
Among the top 10 authors, Kehlet H is the author of the concept of ERAS and the method of multi-modal analgesia. The article published in 1997 is extensively cited, and in the last decade, it has been cited 104 times, ranking No. 4.22 Meanwhile, the quality and quantity of the author’s articles remain high for nearly a decade, which shows his strong influence in this field. It should be noted that Ljungqvist O, ranking 10th in terms of number of published papers, ranks first in terms of H-index, and has published several high-quality articles on ERAS in recent years. He analyzed the impact of ERAS implementation on patients and the health care system and concluded that ERAS has brought surgery and anesthesia to a new level and has brought significant improvements to patients and the health care system, but further improvements are still needed.20,61
Of note, half of the top 10 journals have high IF, suggesting that it is not challenged to publish research articles on perioperative analgesia in high-quality journals. In addition, a co-citation visualization analysis showed that the most cited article was the clinical guideline for postoperative pain management published by Chou R et al, which was published in 2016 and cited 158 times. To a certain extent, this article has a great impact on the field of research.50 The second is an article published in 2006 by Kehlet H et al (cited 146 times), which describes the risk factors and prevention of postoperative persistent pain, arguing that the intensity of postoperative acute pain is related to the development of a persistent state, and that multi-modal drug interventions may prevent this shift.33 There is a strong co-citation relationship between this article and most of the articles related to perioperative anesthesia and analgesic drugs, which indicates the guiding significance of this research for the future research of multi-mode analgesic drug intervention. In third place is a new report on practice guidelines for acute pain management in the perioperative setting published in 2012.34
The literature on Group 5 in Figure 3 is not closely related to that on other groups. It could thus be concluded that perioperative anesthesia techniques and analgesics are relatively independent of other studies on the prognosis of cancer surgery, and more attention is paid to the long-term and overall recovery of patients than to analgesia, which also suggests the significance of the pursuit of perioperative analgesia. Future researches in this area can increase the long-term effect of postoperative observation of patients.
Terms such as general-anesthesia, local-anesthesia, regional-anesthesia, epidural-anesthesia, and spinal-anesthesia for different types of anesthesia sit in the middle of the mapping, suggesting that studies of perioperative analgesia increasingly revolve around changes in the type of anesthesia, which are likely to become more common in the future.
To some extent, the development trend and research hotspot in this field can be understood based on the bibliometric analysis and visualization of the literature, and references are provided for researchers and clinical doctors in related fields. Increasingly perfect perioperative analgesia can reduce patients’ perioperative pain. However, the present study is still subject to some limitations. First, the search term “PERIOPERATIVE ANALGESIA” searched did not completely search the relevant literature in this field. Second, only the number of citations was relied on to evaluate the impact of an article. Actually, due to the difference in the year of publication, the factors of time should be combined for more comprehensive evaluation. Finally, the VOSviewer can only analyze keywords and co-cited literature, instead of the whole content of the article, making the analysis not comprehensive.
Conclusion
Through bibliometric analysis, the United States has been proven a leading country in the field of perioperative analgesia research. Harvard University and the League of European Research Universities have made outstanding contributions. In the past decade, the effects of enhanced recovery after surgery, different types of anesthesia and multi-mode analgesic drug intervention on perioperative analgesia have become the research hotspots and are likely to be the focus of future study.
Acknowledgments
Lian Zhen Zhou and Xuan Li are co-first authors for this study. We thank the Second Affiliated Hospital of Shandong First Medical University for its support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gerbershagen HJ, Aduckathil S, van Wijck AJM, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944.
2. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546.
3. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–2298.
4. Weinstein EJ, Levene JL, Cohen MS, et al. Local anaesthetics and regional anaesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children. Cochrane Database Syst Rev. 2018;4:CD007105.
5. Chaparro LE, Smith SA, Moore RA, Wiffen PJ, Gilron I. Pharmacotherapy for the prevention of chronic pain after surgery in adults. Cochrane Database Syst Rev. 2013;1(7):CD008307.
6. Viscusi ER, Webster L, Kuss M, et al. A randomized, Phase 2 study investigating TRV130, a biased ligand of the μ-opioid receptor, for the intravenous treatment of acute pain. Pain. 2016;157(1):264–272.
7. Clarke H, Poon M, Weinrib A, Katznelson R, Wentlandt K, Katz J. Preventive analgesia and novel strategies for the prevention of chronic post-surgical pain. Drugs. 2015;75(4):339–351.
8. Huang XZ, Zhao JH, Gao P, et al. Continuous Wound infiltration with local anesthetic is an effective and safe postoperative analgesic strategy: a meta-analysis. Pain Ther. 2021;10(1):525–538.
9. Svider PF, Nguyen B, Yuhan B, Zuliani G, Eloy JA, Folbe AJ. Perioperative analgesia for patients undergoing endoscopic sinus surgery: an evidence-based review. Int Forum Allergy Rhinol. 2018;8(7):837–849.
10. Oh SK, Lim BG, Won YJ, Lee DK, Kim SS. Analgesic efficacy of erector spinae plane block in lumbar spine surgery: a systematic review and meta-analysis. J Clin Anesth. 2022;78:110647.
11. Ninkov A, Frank JR, Maggio LA. Bibliometrics: methods for studying academic publishing. Perspect Med Educ. 2013.
12. Wang S, Zhou HP, Zheng L, et al. Global Trends in Research of Macrophages Associated With Acute Lung Injury Over Past 10 Years: a Bibliometric Analysis. Front Immunol. 2021;12:11.
13. Guler S, Capkin S, Sezgin EA. The evolution of publications in the field of scoliosis: a detailed investigation of global scientific output using bibliometric approaches. Turk Neurosurg. 2021;31(1):124–136.
14. Koo M. Systemic Lupus erythematosus research: a bibliometric analysis over a 50-year period. Int J Environ Res Public Health. 2021;18(13):14.
15. Li N, Wang L, Hu YD, et al. Global evolution of research on pulmonary nodules: a bibliometric analysis. Future Oncol. 2021;17(20):2631–2645.
16. Durieux V, Gevenois PA. Bibliometric Indicators: quality Measurements of Scientific Publication. Radiology. 2010;255(2):342–351.
17. Dorta-Gonzalez P, Dorta-Gonzalez MI. Empirical application of a bibliometric indicator based on the h-index. Cult Educ. 2011;23(2):297–313.
18. Jones T, Huggett S, Kamalski J. Finding a way through the scientific literature: indexes and measures. World Neurosurg. 2011;76(1–2):36–38.
19. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538.
20. Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: a Review. JAMA Surg. 2017;152(3):292–298.
21. Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248(2):189–198.
22. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–617.
23. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213.
24. Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009;144(10):961–969.
25. Varadhan KK, Neal KR, Dejong CHC, Fearon KCH, Ljungqvist O, Lobo DN. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010;29(4):434–440.
26. Pöpping DM, Elia N, Marret E, Remy C, Tramèr MR. Protective effects of epidural analgesia on pulmonary complications after abdominal and thoracic surgery: a meta-analysis. Arch Surg. 2008;143(10):567.
27. Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Wu CL. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290(18):2455–2463.
28. Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2014;118(1):67.
29. Marret E, Remy C, Bonnet F. Meta-analysis of epidural analgesia versus parenteral opioid analgesia after colorectal surgery. Br J Surg. 2007;94(6):665–673.
30. Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. 2003;362(9399):1921–1928.
31. Brandstrup B, Tønnesen H, Beier-Holgersen R, et al. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003;238(5):641–648.
32. Cook TM, Counsell D, Wildsmith JAW. Major complications of central neuraxial block: report on the third national audit project of the royal college of anaesthetists. Br J Anaesth. 2009;102(2):179–190.
33. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625.
34. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116(2):248–273.
35. Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77(5):1048–1056.
36. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–540.
37. Laskowski K, Stirling A, McKay WP, Lim HJ. A systematic review of intravenous ketamine for postoperative analgesia. Can J Anaesth. 2011;58(10):911–923.
38. Elia N, Lysakowski C, Tramèr MR. Does multimodal analgesia with Acetaminophen, nonsteroidal antiinflammatory drugs, or selective cyclooxygenase-2 inhibitors and patient-controlled analgesia morphine offer advantages over morphine alone? Meta-analyses of randomized trials. Anesthesiology. 2005;103(6):1296–1304.
39. Blaudszun G, Lysakowski C, Elia N, Tramèr MR. Effect of perioperative systemic α2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Anesthesiology. 2012;116(6):1312–1322.
40. Buvanendran A, Kroin JS, Della Valle CJ, Kari M, Moric M, Tuman KJ. Perioperative oral pregabalin reduces chronic pain after total knee arthroplasty: a prospective, randomized, controlled trial. Anesth Analg. 2010;110(1):199–207.
41. Mishriky BM, Waldron NH, Habib AS. Impact of pregabalin on acute and persistent postoperative pain: a systematic review and meta-analysis. Br J Anaesth. 2015;114(1):10–31.
42. Parvizi J, Miller AG, Gandhi K. Multimodal pain management after total joint arthroplasty. J Bone Joint Surg Am. 2011;93(11):1075–1084.
43. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
44. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision Hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–785.
45. Remérand F, Le Tendre C, Baud A, et al. The early and delayed analgesic effects of ketamine after total Hip arthroplasty: a prospective, randomized, controlled, double-blind study. Anesth Analg. 2009;109(6):1963–1971.
46. Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lidocaine infusion facilitates acute rehabilitation after laparoscopic colectomy. Anesthesiology. 2007;106(1).
47. Hollmann MW, Durieux ME. Local anesthetics and the inflammatory response: a new therapeutic indication? Anesthesiology. 2000;93(3):858–875.
48. Marret E, Rolin M, Beaussier M, Bonnet F. Meta-analysis of intravenous lidocaine and postoperative recovery after abdominal surgery. Br J Surg. 2008;95(11):1331–1338.
49. Sun Y, Li T, Wang N, Yun Y, Gan TJ. Perioperative systemic lidocaine for postoperative analgesia and recovery after abdominal surgery: a meta-analysis of randomized controlled trials. Dis Colon Rectum. 2012;55(11):1183–1194.
50. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of Postoperative Pain: a Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157.
51. Wick EC, Grant MC, Wu CL. Postoperative Multimodal Analgesia Pain Management With Nonopioid Analgesics and Techniques: a Review. JAMA Surg. 2017;152(7):691–697.
52. Brummett CM, Waljee JF, Goesling J, et al. New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults. JAMA Surg. 2017;152(6):e170504.
53. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The Erector Spinae Plane Block: a Novel Analgesic Technique in Thoracic Neuropathic Pain. Region Anesth Pain Med. 2016;41(5):621–627.
54. Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107–1113.
55. Fletcher D, Martinez V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth. 2014;112(6):56.
56. Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59(9):470–475.
57. Biki B, Mascha E, Moriarty DC, Fitzpatrick JM, Sessler DI, Buggy DJ. Anesthetic technique for radical prostatectomy surgery affects cancer recurrence: a retrospective analysis. Anesthesiology. 2008;109(2):180–187.
58. Gottschalk A, Ford JG, Regelin CC, et al. Association between epidural analgesia and cancer recurrence after colorectal cancer surgery. Anesthesiology. 2010;113(1):27–34.
59. Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. 2006;105(4):660–664.
60. Gupta A, Björnsson A, Fredriksson M, Hallböök O, Eintrei C. Reduction in mortality after epidural anaesthesia and analgesia in patients undergoing rectal but not colonic cancer surgery: a retrospective analysis of data from 655 patients in central Sweden. Br J Anaesth. 2011;107(2):164–170.
61. Ljungqvist O, de Boer HD, Balfour A, et al. Opportunities and Challenges for the Next Phase of Enhanced Recovery After Surgery: a Review. JAMA Surg. 2021;156(8):775–784.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.