Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Global Trends in COPD Self-Management Research: A Dual-Perspective Bibliometric Analysis (January 2005–July 2025)
Authors Huang X ![]() , Feng J
, Feng J ![]() , Gan X
, Gan X ![]() , Wu R, Su C, Zheng L, Deng R
, Wu R, Su C, Zheng L, Deng R
Received 28 August 2025
Accepted for publication 22 December 2025
Published 6 January 2026 Volume 2026:21 563718
DOI https://doi.org/10.2147/COPD.S563718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Xingyu Huang,* Jiacai Feng,* Xiaoting Gan,* Rongqing Wu,* Cui Su,* Luxiong Zheng,* Renli Deng*
Nursing Department, The Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renli Deng, Nursing Department, The Affiliated Hospital of Zunyi Medical University, No. 149, Dalian Road, Huichuan District, Zunyi, Guizhou, 563000, People’s Republic of China, Tel +86 13985616078, Email [email protected]
Purpose: We looked at research articles published from January 2005 to July 1, 2025. We focused on global trends and key research topics in COPD self-management.
Patients and Methods: We searched the Web of Science database thoroughly using the keywords “COPD (Chronic Obstructive Pulmonary Disease)” and “self-management”. Most previous meta-analyses and systematic reviews focused only on mediating effects. This study is different. We use a dual-perspective bibliometric method. Apply CiteSpace for co-citation network analysis, and VOSviewer for collaborative structure mapping. This study will look into how regional research affects self-management practices for COPD. It will closely explore the main gaps in the academic community.
Results: We reviewed roughly 426 papers and observed that this research area has expanded consistently, peaking between 2020 and 2021. Keyword co-occurrence analysis shows a research framework focused on “chronic obstructive pulmonary disease” and “self-management” We statistically reviewed main author groups and identified 76 prolific researchers with consistent relevant outputs. This number aligns with the field’s growing research interest in recent years. Geographically, European and Australian teams prioritize research quality—their work is methodologically rigorous and clinically useful. US, UK and Dutch institutions have more publications and greater academic influence.
Conclusion: Over the past two decades, the field of COPD self-management has made significant progress. This is due to the long-term work of core authors and the collaboration between top research institutions. This study gives key information to optimize COPD self-management strategies, and points out key areas for future research.
Keywords: chronic obstructive pulmonary disease, self-management, bibliometrics, research trends, global collaboration
Introduction
Data from the Global Burden of Disease study shows COPD mortality remains high. It ranks second only to cardiovascular, cerebrovascular diseases and malignant tumors, and is the third leading cause of death worldwide.1 Over the next decade, the disease’s prevalence is projected to rise—data from the 2023 WHO report puts annual deaths at over 3 million. Individual-related factors in patients with COPD (such as insufficient adherence to medication and improper home care measures) result in a clinically common 20% rate of readmission within 30 days. The expenses associated with diagnosis, treatment, and nursing resulting from multiple hospitalizations constitute the core reason for the high medical costs of this disease.2 Clinical studies show about 40% of COPD patients do not take meds as told, and over 60% lack basic self-care skills. The World Health Organization (WHO) Guidelines for Self-Care Interventions for Health and Well-Being state that self-management is key to improving health outcomes,3 and structured interventions are necessary to help individuals manage their health autonomously. The guide also says digital health tools, like mobile health apps and telemedicine platforms, can give important help for good self-care.4 Even with progress in related areas, there’s a big global gap: developed countries’ main problem is patients not taking meds as told, and developing countries struggle to share important knowledge.5
Research on COPD is divided into three stages: early 1800s observations of bronchitis-emphysema connections,6 international diagnostic criteria established by ATS/ERS in the 1970s,7 international diagnostic criteria established by ATS/ERS in the 1970s.8 Self-management concepts emerged from mid-20th-century doctor-patient relationship research—most notably Balint’s theories, and Neighbor’s “shared management”. These parallel developments reflect the lengthy evolutionary path of academic interest in COPD, and self-management. Guidelines released between 2016 and 2023 further define core requirements for effective self-management: personalized support, structured education, and digital tools.
Existing research mainly uses systematic reviews and meta-analyses. Their main job is to pull out practical effects of different interventions, giving direct help for clinical work. From a big-picture view of how the field grows, this way of focusing on small-scale effects has big limits. Over 20 years, related research has built up steadily. Figuring out how knowledge structures change, what global collaboration networks are like and new research frontiers all at once needs good macro-level bibliometric analyses—these are still hard to find. Traditional reviews often fail to provide insights at the strategic level. This study achieves this by utilizing complementary bibliometric methods. By combining three approaches: quantifying research outcomes, visualizing knowledge frameworks, and predicting future directions, we precisely address the shortcomings of traditional methods.9
We got bibliographic data from the Web of Science Core Collection and only included papers indexed in SCI-EXPANDED and SSCI. The study period was January 2005 to July 1, 2025, and there are four clear objectives:
- In global COPD self-management research, do traditional care methods shifting to digital health strategies happen often? What obvious traits show in this field’s research growth over 20 years? How to sort changes in key research topics?
- In the global research on self-management of COPD, which country is leading? Which institutions are at the core and have made prominent contributions as authors? What are the structural characteristics of the collaborative network? How do regional differences in research quality, output quantity, and thematic focus (such as Western digital health and East Asian biomass-related interventions) manifest? Is there a correlation between the geographical distribution of research outcomes and regional differences in medical resource allocation?
- What core keywords and thematic clusters constitute the knowledge system of this field? What key research hotspots (eg, health literacy, self-management support) do these clusters reflect?
- What emerging research frontiers and burst concepts have appeared in recent years? How do these elements reflect the paradigm shift in this field (eg, moving from the standardization of research methods to the enhancement of patients’ capabilities)?
Materials and Methods
Bibliometric Approach
Bibliometrics,10 as a scientific methodology for quantitative analysis of scholarly literature, employs mathematical statistics and visualization techniques to objectively delineate research hotspots, evolutionary trajectories, and collaborative networks. Bibliometrics has shown significant application value in medical research, especially in the field of chronic disease management.11 There are mainly three types of core technologies supporting this method: co - occurrence analysis is used to clarify the core research topics and their interrelationships, citation network analysis can track the academic influence of key publications, and burst point detection can accurately identify emerging research directions.12 Its core advantage lies in using objective means to transform complex academic phenomena into quantifiable indicators. This can reduce the interference of subjective bias and ensure the reliability of research conclusions.13
The Web of Science (WoS) is a globally recognized top.14 We selected relevant literature from January 2005 to July 2025 to build a reliable dataset and use CiteSpace and VOSviewer to draw a knowledge map. By applying co - occurrence, clustering, and burst detection techniques, systematically sort out the characteristics of global research results on COPD self - management and fully present the overall picture of research in this field. Traditional review methods suck at grasping the macro - research trends, and this kind of bibliometric analysis method can totally fill that gap.
Data Source
In the practice of bibliometric research, CiteSpace and VOSviewer are two indispensable core tools. Using them together can fully bring out their synergistic effects. CiteSpace’s time can accurately pinpoint the key milestones and evolution paths in the development process of a discipline. The burst detection algorithm in this tool can efficiently catch emerging research trends.15 Also, it’s compatible with mainstream academic databases like Web of Science and CNKI, and can directly integrate and apply multi - source literature data.16 Chen and others’ research17 has confirmed that a certain Java visualization tool can accurately draw a citation network to present the knowledge structure through co - citation analysis technology, which provides strong support for screening key literature, locating research frontiers, and sorting out knowledge dissemination paths. VOSviewer18 focuses on building scientific cooperation networks. With its optimized visualization engine, it can clearly break down the complex relationship patterns hidden in large - scale bibliometric data.
Both tools share the same core features and use similar visualization techniques.19 Their co-occurrence analysis and clustering algorithms rely on an improved community detection method to identify research topics and academic communities.20 They follow standardized scientometric workflows—like data cleaning, network mapping, and visualization—to deliver complete solutions.21 This coordinated approach makes them essential and complementary in today’s bibliometric research.
This study will explore the following questions through a bibliometric lens:
- Objective 1 (Output Growth and Topic Evolution): Utilize CiteSpace’s time slice analysis and VOSviewer’s keyword co-occurrence analysis to quantify annual publication trends and track the evolution of topics over time.
- Objective 2 (Key Players, Collaborations & Local Resource Ties): Since this field focuses on how teamwork and resource sharing intersect, we used VOSviewer to map out networks among authors, institutions, and countries – clearly showing gaps in research output/quality – and combined it with big-picture stats like national health spending, this helps uncover potential links between resource allocation and how collaboration networks actually work.
- Objective 3 (Knowledge Structure & Hot Topics): Figuring out core theme clusters and their impact through CiteSpace keyword clustering (Q=0.3624, s=0.8439) and VOSviewer co-occurrence analysis (min. keyword frequency 5–10).
- Objective 4 (Emerging Frontiers & Paradigm Shifts): We will pick out high-burst keywords using CiteSpace’s burst detection (γ=0.5), then map how research trends evolve over time. The big shift we are seeing, Moving from standardized methods toward putting patients in the driver’s seat.
Data Screening Process
Raw data extracted from the database often includes duplicate records or irrelevant entries, so a stringent data screening protocol was implemented to uphold analytical rigor. Searches were initially conducted within the Web of Science Core Collection, encompassing both SCI-EXPANDED and SSCI indices—this selection stems from WoS’s two key strengths: comprehensive bibliometric metadata and broad coverage of high-impact academic work in chronic disease research. Data retrieval was restricted to the period spanning January 1, 2005, to July 1, 2025; this time frame balances a thorough portrayal of long-term research trends in the field while mitigating incomplete data issues associated with 2025 remaining unfinished. The search yielded 109,124 publications related to “COPD”, 38,765 focusing on “self-management”, and 1541 publications incorporating both terms.
The screening process involved:
- Restricting document types to research articles and reviews;
- Manual title/abstract screening to exclude off-topic literature;
- Deduplication and record consolidation.
- During the manual screening, publications were excluded based on the following pre-defined criteria:
- The study did not primarily focus on COPD patients.
- The intervention described was not a self-management program (eg, studies on pharmacological treatments or inpatient rehabilitation without a self-management component were excluded).
- The publication was not an original research article or review (eg, editorials, letters, grey literatures or conference abstracts without full text).
The screening process followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines Figure 1, this PRISMA literature screening flow diagram illustrates the entire process of literature selection for COPD self-management research from 2005 to 2025. From 1541 relevant records retrieved from databases, 426 valid articles were finally confirmed for subsequent analysis after duplicate removal, screening and eligibility assessment. The manual screening was conducted independently by two reviewers (Xingyu Huang and Jiacai Feng), To ensure consistency, a pilot screening was performed on a random sample of 50 publications, resulting in an inter-rater reliability (Cohen’s Kappa) of 0.85, indicating excellent agreementAll discrepancies were resolved through consensus with a third senior researcher (Renli Deng).
 |
Figure 1 The PRISMA flow diagram illustrates the literature screening pathway for COPD self-management research from 2005 to 2025, fully demonstrating the entire process of gradually selecting 426 eligible articles from 1541 initial records. |
After carefully sifting through everything, we ended up with a dataset of 426 solid publications to analyze. We wrapped up our literature search on July 1, 2025, focusing on stuff published between January 1, 2005, and that date. Gotta mention, the 2025 papers only reflect what was out by the search date—not the whole year’s publications. That’s pretty standard for bibliometric studies, letting us include the latest research while keeping the timeline crystal clear. To guarantee data integrity, all steps employed dual-independent verification with consensus resolution for discrepancies. The curated dataset provides comprehensive bibliometric metadata, forming a robust foundation for subsequent visualization analyses, Table 1 presents key criteria for data source and selection in COPD self-management research: Web of Science (SCI/SSCI) as the database, 2005–2024 as the search period, English as the language, keywords related to COPD and self-management, articles/reviews as eligible document types, and 426 included samples.
 |
Table 1 Detailed Criteria for Data Source Selection and Literature Screening in COPD Self-Management Research |
A total of 428 studies were finally included in this analysis, with their methodological types showing a distinct “empirical intervention orientation”: As can be seen in Figure 2, randomized controlled trials (RCTs) accounted for 39.3% (168 studies), the highest proportion among all research designs, followed by literature reviews (129 studies, 30.2%) and path analysis (109 studies, 25.5%), while also covering diverse methods such as qualitative research (108 studies, 25.3%) and systematic reviews (69 studies, 16.2%). This methodological distribution aligns well with the research nature of COPD self-management: the core goal of chronic disease self-management is to optimize patients’ daily health behaviors via practical interventions, and RCTs serve as the authoritative research paradigm to verify the effectiveness of such interventions and confirm their clinical feasibility. Thus, RCTs have become the dominant research design in this field, providing key data support for subsequent analysis of the “evolution pattern of hotspots in intervention-related studies”.
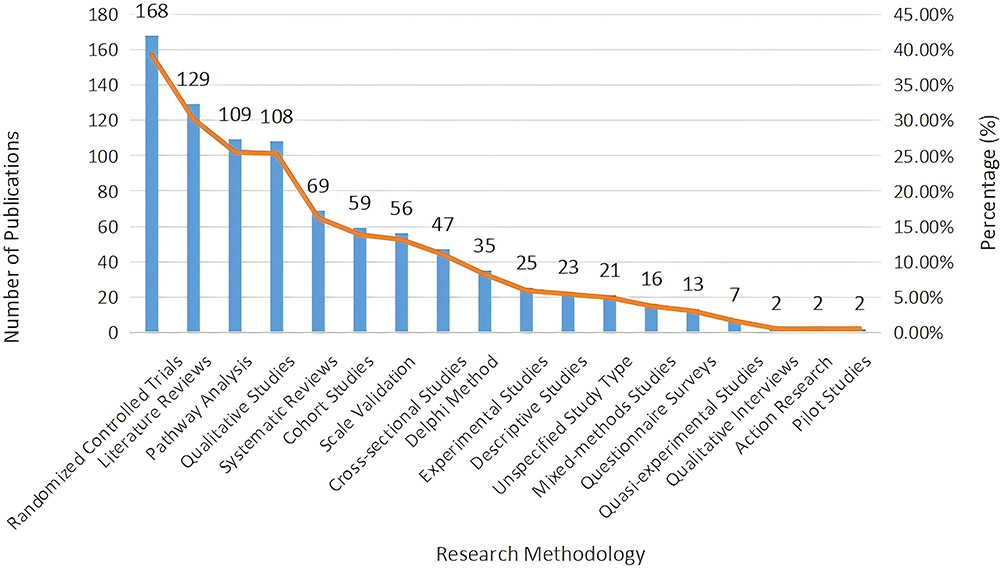 |
Figure 2 Statistics on the distribution of research methodologies in COPD self-management studies show that randomized controlled trials (168 studies) account for the highest proportion among various research designs and serve as the primary research approach in this field. |
Analysis Techniques
This study adopted CiteSpace (v6.4.R1) and VOSviewer (v1.6.20) for complementary analysis: As shown in Table 2, VOSviewer was used to construct collaboration networks and keyword co-occurrence networks; CiteSpace, through co-citation analysis and burst detection, clarified the field’s knowledge base and research frontiers. Specific parameters for each analysis (eg, minimum frequency threshold) followed the conventional default settings of the software for bibliometric mapping.
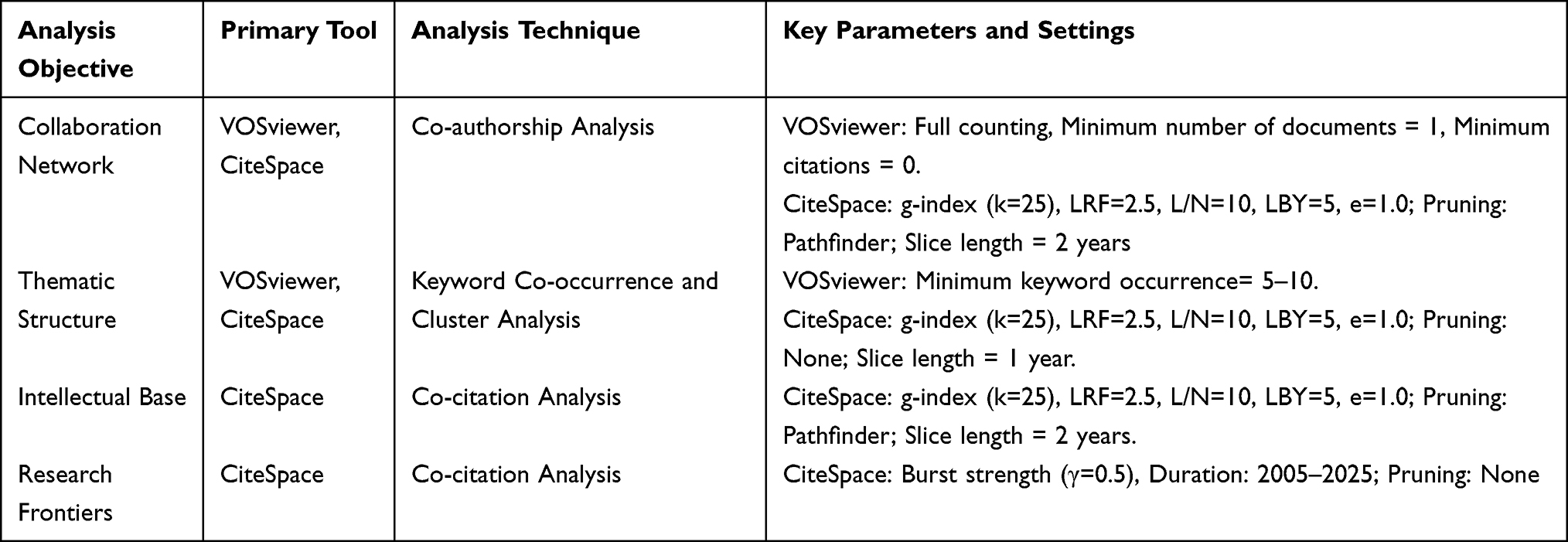 |
Table 2 Bibliometric Analysis Tools, Techniques, and Key Parameter Settings for COPD Self-Management Research |
Rationale for Parameter Settings:
- The minimum occurrence frequency of keywords in VOSviewer is set to 5–10 times, a range determined through preliminary tests: if the frequency is below 5, trivial terms with little analytical value (eg, “case report”) will be included; if it exceeds 10, meaningful keywords (such as “digital health intervention”, which appeared only 8 times before 2020 but represents a key emerging direction) will be excluded.
- The time slice length in CiteSpace is set to a differentiated 1–2 year range: a 2-year slice is used for collaboration network analysis to capture stable cooperative connections, while a 1-year slice is applied for keyword burst detection to accurately identify short-term, rapid shifts in research themes.
- Differentiated Adaptation Logic for Pruning Algorithms:
For CiteSpace analyses of collaboration networks and intellectual bases, the Pathfinder algorithm was selected—connection lines (for cooperation or literature citations) in such networks are typically dense, and the algorithm streamlines redundant lines to make the structure of core clusters (eg, cross-border author collaboration circles, high-citation literature clusters) more intuitively clear; for CiteSpace analyses of thematic structures and research frontiers, no pruning algorithm was enabled (parameter labeled “Pruning: None”)—these analyses cover emerging research directions like “digital health”, where weak connections between keywords or literature often imply frontier dynamics, and retaining the network’s complete lines prevents omitting potential trend-related information.
Data Cleaning
To make sure our data’s solid, we are using a standard cleanup process that goes like this:
- Combining the consistency of the author’s affiliation and the characteristics of the collaborative network, merge the same author with inconsistent name expressions to achieve disambiguation.
- Standardization of key words: Consolidate synonymous expressions and lexical variants (eg, unify and standardize “COPD” and “chronic obstructive pulmonary disease”).
- Standardizing institution names: For variant names of the same institution, use the official standard form (eg, “Univ Twente” becomes “University of Twente”).
- De-duping: We will compare the titles and DOIs in the literature to weed out any duplicate records.
Descriptives Statistics
This study conducted a systematic analysis of 426 peer-reviewed literature. These documents cover an academic collaboration network of 765 institutions and 1841 authors from 46 countries. The relevant results have been published in 139 journals, with a total of 11061 references cited, providing a solid theoretical foundation for this study. 69 high impact articles have been cited over 20 times, laying a pioneering foundation for research in the field of self-management of chronic obstructive pulmonary disease. From the annual publication trend in Figure 3 it can be seen that research in this field has shown a steady growth trend in the past two decades, reaching its peak of development in 2020–2021. This change is closely related to the increasing global attention to chronic disease management and digital health technology during the same period. The cited literature sources cover 3460 journals, fully reflecting the outstanding disciplinary diversity and extensive global academic exchanges in this field.
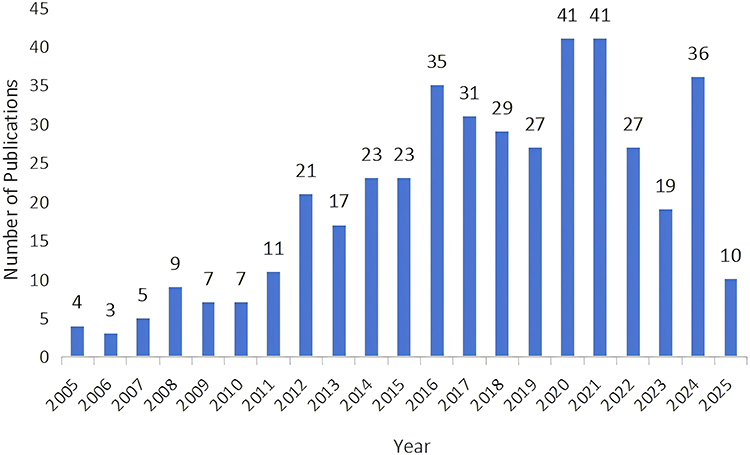 |
Figure 3 The trend chart of annual publication output in COPD self-management research from 2005 to 2025 indicates that the research output in this field presents a steady upward trend, with a publication peak achieved between 2020 and 2021. |
Bibliometric Analysis of the Author
This study takes a systematic look at the current research progress and situation in the area of self-management for chronic obstructive pulmonary disease.
The development trajectory of COPD self-management requires empirical data support. Thisstudy examines the distribution of academic outputs of scholars in this field, with a focus onanalyzing the scope of their academic influence, distilling data-driven core insights, and providing empirical evidence for grasping the development trajectory of the field. We applied Lotka’s Law22 and Price’s Law (See Supplementary Material S1 for detailed methodology, including the application and calculation of Lotka’s Law and Price’s Law). Lotka’s Law enables the precise delineation of high - yield research cohorts and their seminal contributions within the realm of COPD self-management.23 In line with the above-defined criteria, authors who have published no fewer than 4 papers are classified as core authors. This identification method aligns with the core principle of Price’s Law, which stipulates that the volume of literature contributed by the core author group must account for more than 50% of the total number of publications in the field.24
In the field of COPD self-management research, we identified five core authors, each having published no less than nine related papers. Table 3 presents the distribution of high-yield authors (with a publication count of ≥ 9 papers), which is consistent with the academic output characteristics we previously observed. In the field of COPD self-management, Professor Burbo has a prominent academic influence, with 26 related research achievements, he is a highly productive scholar in this field. His research has been cited a total of 935 times, and his academic influence remains consistently stable As a key contributor to the 2016 global expert consensus, he did way more than just publishing papers—that framework literally set the worldwide standard for COPD self-management, solidifying his role as a major shaper of the field’s direction.25 His research shows a clear progression: in the early 2000s, he focused on proving how self-management can actually cut down hospital stays, building up solid evidence along the way. By the 2010s, he shifted gears to standardizing practices in the field, taking the lead to get guidelines rolling,26 Lately, he’s been zeroing in on blending personalized health plans with digital management strategies.27 This journey demonstrates solid academic accumulation and also reflects the extensive transformation of disciplinary paradigms. Dr. Job Van der Palen ranked second with 15 published papers, and his high citation index of 1141 total citations and an average of 76.06 citations per paper highlights the outstanding scientific value and dissemination potential of his research. Dr. Tanja W. Effinger also has a good citation count, with an average of 68.88 citations per paper. Dr. Sally J. Singh and Dr. Hassan Hosseinzadeh both published 9 papers, but their citation counts are different, at 340 and 226 respectively. This indicates that the rigor of research direction or methodology may influence scientific impact.
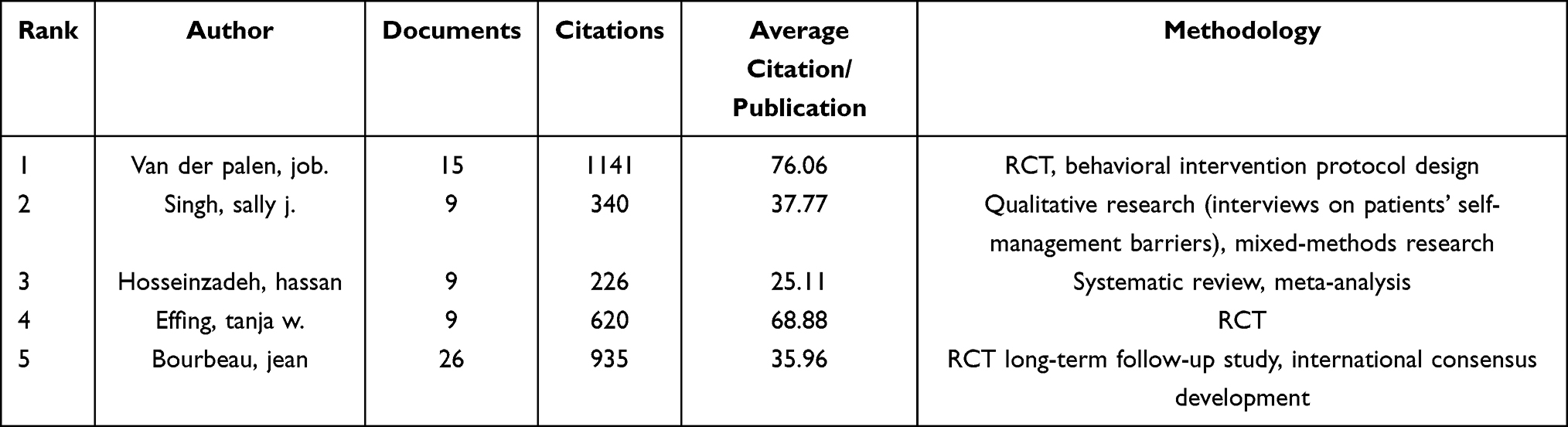 |
Table 3 Important Authors in the Field of COPD Self-Management and Their Methodological Focus |
This visualization in Figure 4 from VOSviewer has 59 nodes, each one standing for an author. The scale of the nodes is directly related to the frequency of collaboration. “Bourbeau, Jean” corresponds to the largest node, confirming that significant publication achievements and active participation in collaboration were prominent during this period. The 76 edges in the graph represent the cooperative relationships among authors, and the thickness of the lines intuitively reflects the differences in the degree of collaboration. The thickest line connects “Bourbeau, Jean” and “van der Palen, Job”, indicating a very close collaboration between the two. Nodes are distinguished by color and divided into 59 research entities, which are further subdivided into 6 major collaboration clusters, each of which has internal cooperative relationships. Bourbeau, Jean is at the core of the red group, which is the largest and most closely-knit in this field, and is the dominant force in it. The blue cluster is led by two core figures, Job Van der Palen and Paul Van der Valk, The team is focused and members work closely together. The green cluster is headed by Sally J. Singh. The team is loose, with members being scattered and having less contact. The purple cluster centered around Rand and Lucia (with 4 members) and the pink cluster led by Wolf and Michael S (with 5 members) are both small in size but highly efficient, concentrating on specialized research in their respective fields. The orange/yellow cluster features the aggregation of multiple small research teams, each forming an independent micro-core and collectively exploring connected topics within the same broad field.
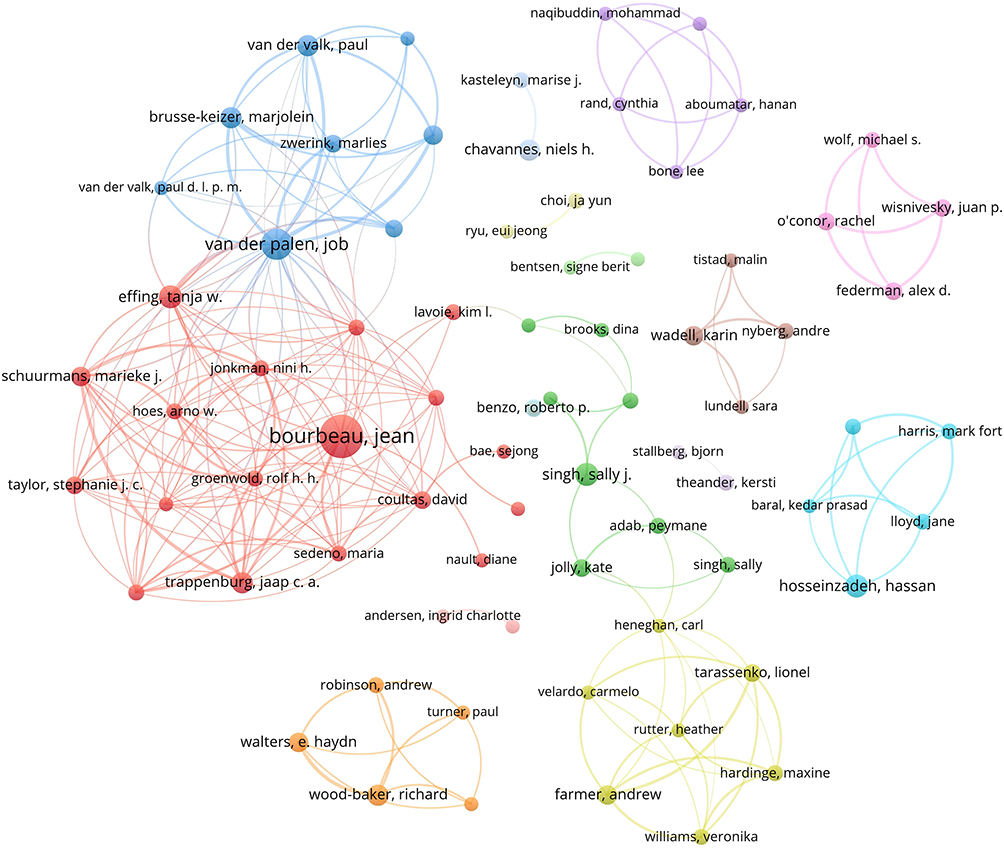 |
Figure 4 Within the author collaboration network developed via VOSviewer, the size of each node corresponds to the frequency of collaboration, the thickness of connecting lines indicates how tight the collaboration is, and Bourbeau, Jean, as the core author, forms a central hub for collaboration. |
Figure 5 presents a co-authorship network visualization of COPD self-management research generated through CiteSpace (version 6.4.R1), spanning January 2005–July 2025 with a temporal slice length of 2 years. Node diameters scale with author publication output, while connecting edges denote collaborative relationships. The chromatic gradient (cool-to-warm tones) temporally maps collaboration evolution.28 It includes a total of 367 nodes and 740 links between the nodes, here is a correlation between the edge density index and the intensity of research collaboration. The weighted average silhouette coefficient reaches 0.9032, which confirms a very high clustering homogeneity (when the value of S approaches 1, the clustering cohesion approaches perfection). The modularity analysis yields Q = 0.7446 (a Q value greater than 0.3 indicates a significant community structure), clearly showing the differences between the sub - research domains. These indicators reflect the academic cooperation model, the temporal dynamics, and the characteristics of the intellectual clusters in the research on self-management of COPD.
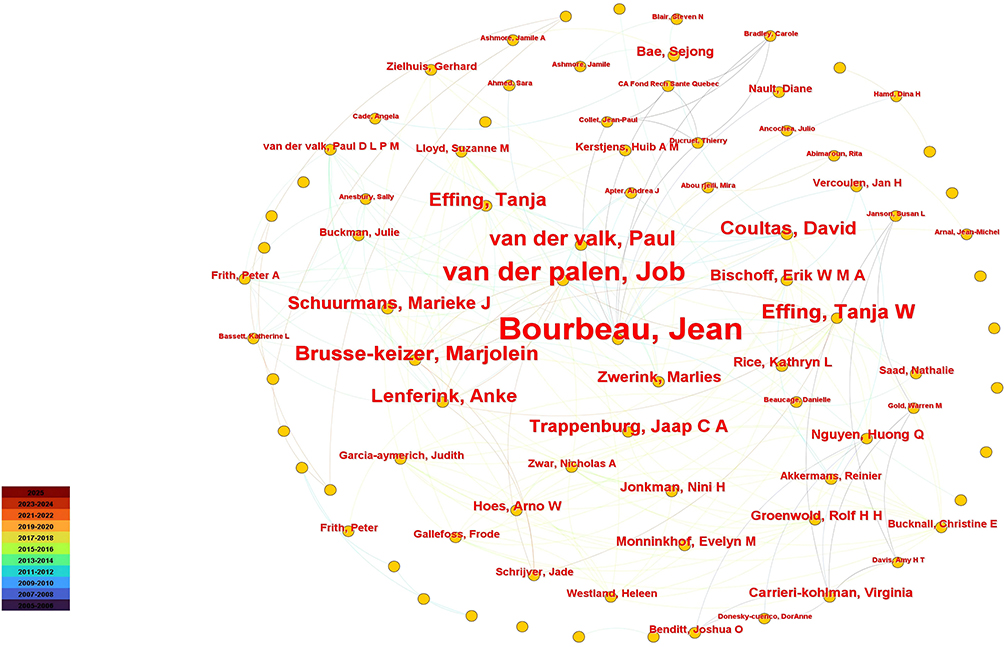 |
Figure 5 The author co-occurrence map generated on the basis of CiteSpace not only clearly exhibits the collaborative links between researchers but also clarifies the distribution features of core collaborative circles at the same time. |
Bibliometric Analysis of the Journal
According to Bradford’s Law,18 a bibliometric analysis of journal distribution revealed that over the past two decades, the majority of publications in this field have been concentrated in chronic disease research, with only a limited number appearing in general medical journals. Table 4 presents the top seven journals by publication volume, derived from an analysis of 426 articles, this chart outlines how journals in the COPD self-management research field are distributed across dimensions like publication output volume, overall academic impact, and the average influence per individual paper.
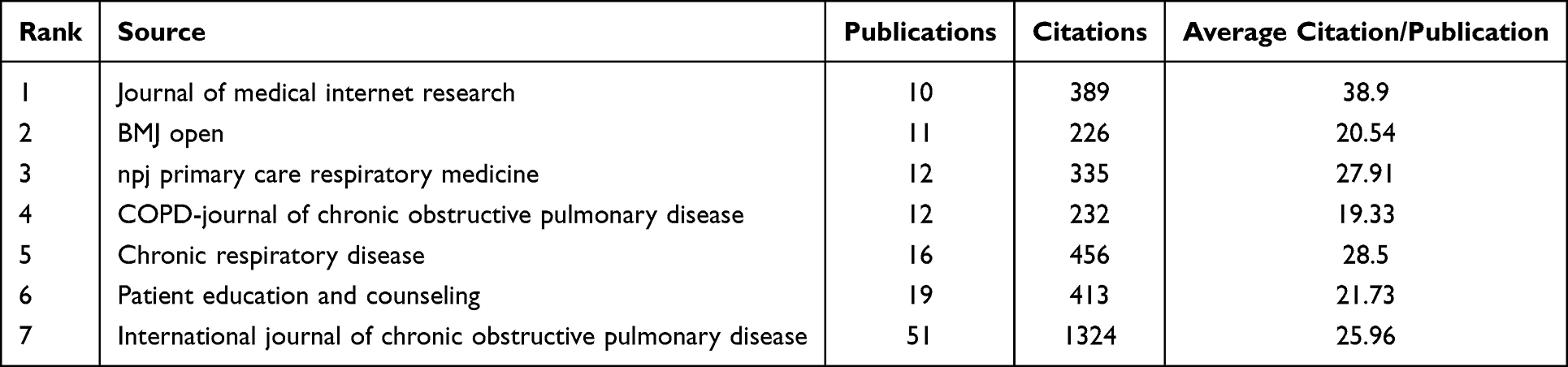 |
Table 4 Analysis of Journals with More Than 7 Publications in the Field of COPD |
Meanwhile, Figure 6 Visualization Chart of Publication Characteristics of Key Journals in COPD Self-Management Research (2005–2025) also reveals the distinct publication patterns among key journals in this field. Three journals demonstrated particularly high productivity: Chronic Respiratory Disease (16 articles), Patient Education and Counseling(19 articles), and International Journal of Chronic Obstructive Pulmonary Disease (leading with 51 publications). Four additional journals published more than 10 articles each: Journal of Medical Internet Research, BMJ Open, npj Primary Care Respiratory Medicine, and COPD: Journal of Chronic Obstructive Pulmonary Disease. Respiratory Medicine, and COPD: Journal of Chronic Obstructive Pulmonary Disease. The Journal of Medical Internet Research, BMJ Open, npj Primary Care Respiratory Medicine, and the International Journal of Chronic Obstructive Pulmonary Disease are all open-access journals, this shows that the continuous development of open-access publishing in recent times has greatly contributed to the promotion of research on the self-management of chronic obstructive pulmonary diseases.
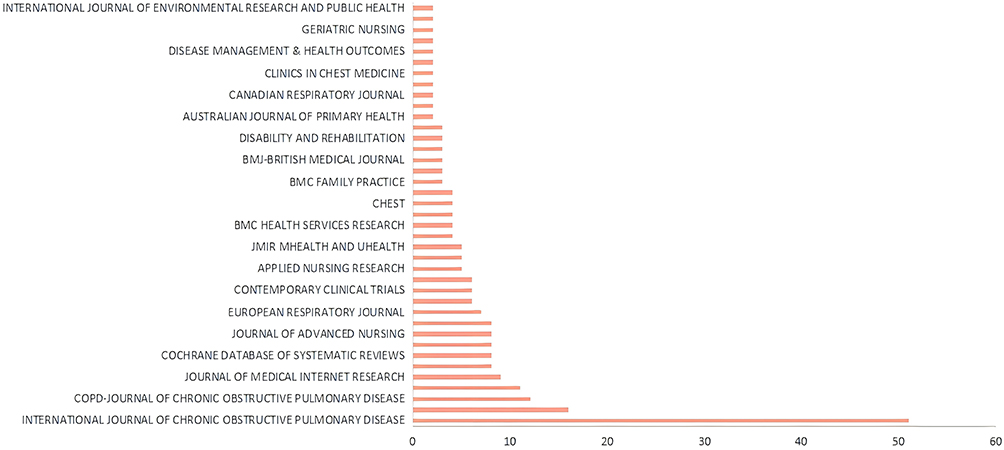 |
Figure 6 The visualization results regarding the publication situation in core journals of the COPD self-management field indicate that International Journal of Chronic Obstructive Pulmonary Disease ranks first in the field in terms of the number of published papers. |
The dual-map overlay illustrates the citation landscape, the left hemisphere corresponds to the cited journals, while the right hemisphere represents the citing journals.21,29 The COPD citation map Figure 7 shows that this kind of research mostly moves forward by blending knowledge from different fields, not just through clinical exploration. And that’s exactly why it works so well for patients’ complex real-world needs—basically, cross-discipline teamwork is its real strength.30
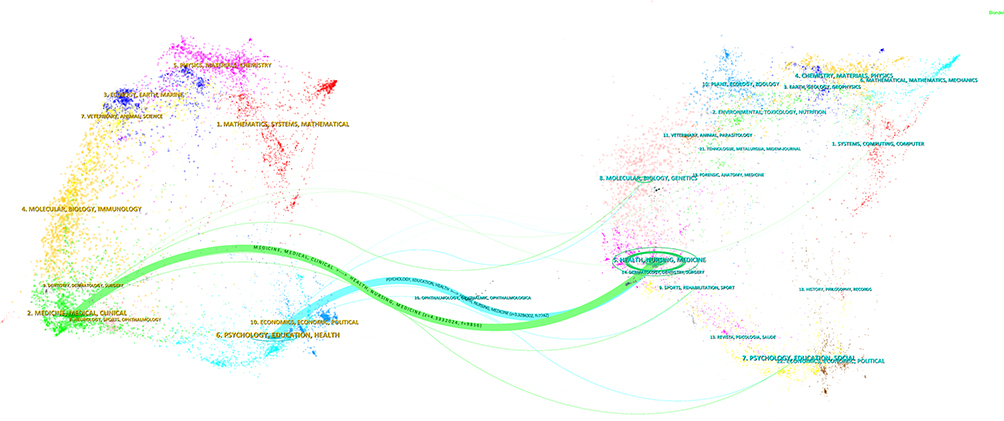 |
Figure 7 The dual-map overlay analysis chart of journals related to the COPD self-management field uncovers both the citation transmission routes of papers in this field and the key traits of interdisciplinary knowledge flow. |
In the map, clusters of different colors stand for distinct disciplines (eg, Medicine/Clinical Medicine, Psychology/Education/Health, Environment/Toxicology/Nutrition). Denser clusters mean more active research in that field; the thickness of the curves linking clusters corresponds to the strength of interdisciplinary ties — thicker curves signal more frequent knowledge exchange. The central Medicine/Clinical Medicine cluster (the green hub) has strong links to Molecular Biology/Genetics (supporting pathophysiology-based self-care), Psychology/Education/Health (guiding behavioral interventions), and Environment/Toxicology/Nutrition (refining context-aware management). Self-management of COPD is not just a simple medical method. It is an integrated practice that combines knowledge from multiple fields such as basic life sciences, social sciences, and environmental sciences.
These cross-disciplinary connections pose challenges to the perception of chronic obstructive pulmonary disease self-management as a single disciplinary field. These interdisciplinary connections precisely highlight the interdisciplinary nature of this field, which requires the breaking down of academic barriers to meet the multi-dimensional needs of patients with COPD in their self-care process, covering biological, behavioral and environmental aspects.
Bibliometric Analysis of the Institutional
We used VOSviewer to build an institutional collaboration network and collected data on the publication output of the organizations involved. As we can see from Table 5, the field of COPD self-management research has a multi-node collaborative structure. This structure is mainly led by academic and medical institutions. The main findings are as follows:
- Institutional composition: The analyses of this study show that among the eight institutions that have published the most articles in this field, all are higher education institutions or medical institutions. Among them, general - oriented universities and specialized medical centers are evenly distributed, each accounting for half.
- Search results by level: The academic outputs of different institutions show obvious level differences. Medisch Spectrum Twente (15 articles), the University of Twente (20 articles), and McGill University (27 articles) together form the first group, and the number of articles published by these three institutions is significantly higher than that of other institutions in this field. The University Medical Center Utrecht, Radboud University Nijmegen (both with 14 papers), the General Hospital for Repatriation (13 papers), and the University Hospitals of Leicester NHS Trust (12 papers), among others, fall into the second tier, with their research output all at a medium level.
- Academic Impact Differences: The Citation Per Paper (CPP) metric reveals notable variations in research quality. Three major Dutch institutions—University Medical Center Utrecht (CPP=91.00), Twente Medical Spectrum (CPP=88.33), and Repatriation General Hospital (CPP=87.69)—stand out for their strong research influence, with CPP values exceeding global averages. By contrast, McGill University (CPP=40.81) shows a disconnect between its publication volume and research quality—its high number of papers has not fully translated into leading citation performance.
- Preeminence of central institutions: The top eight institutions have published a total of 130 articles taking the Medical Center of Utrecht University as an example, the average number of citations per article is 91.00 times. European medical institutions and Australian universities have more pronounced competitive advantages in terms of research results and quality, as evidenced by the Dutch ZonMw, which focuses its funds on clinical translation to improve the relevance of research, while North American institutions have “high output but relatively average quality”. This distribution characteristic may be closely related to the differences in disciplinary emphasis and research investment across different regions. European research led by the Netherlands typically leverages tightly collaborative networks, with a focus on designing patient-centered practical clinical trials. The evidence generated from these studies translates directly to real-world applications— a key driver behind their strong citation performance. On the other hand, the North American system is large - scale and decentralized, supporting research covering a wider range, including many fundamental, methodological or early - stage research, where the citation accumulation rate is slower. This reflects not inferior quality, but differences in research priorities and the scientific division of labor across the global research landscape.
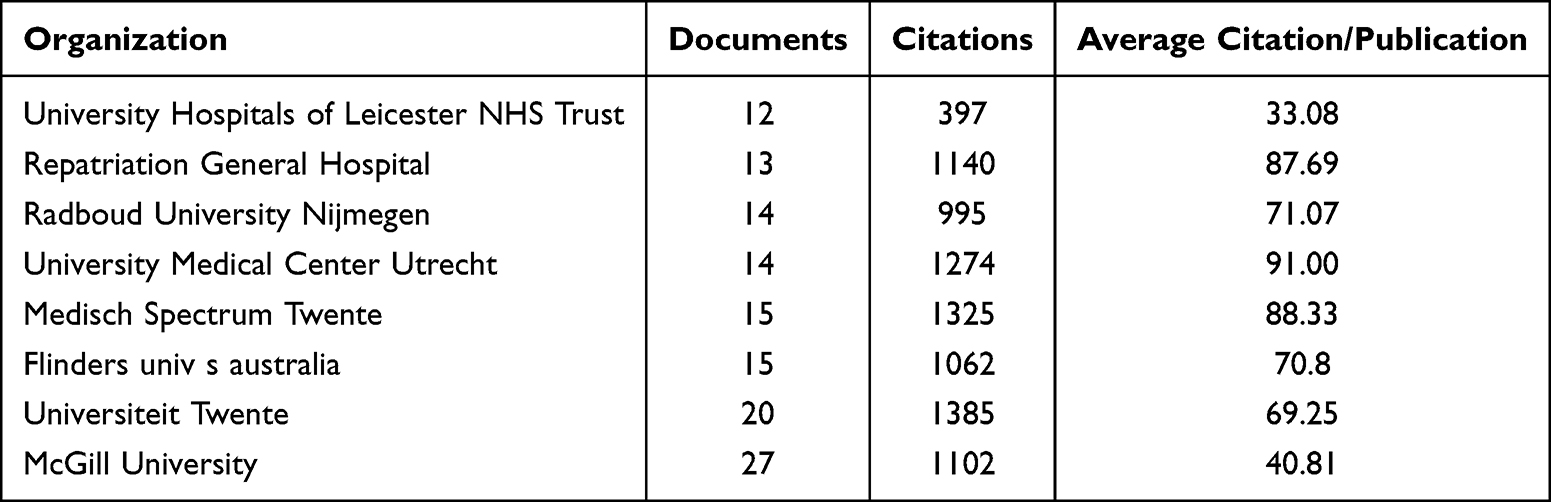 |
Table 5 Analysis of the Top 8 Institutions by Publication Volume in the Field of COPD Patient Self-Management |
VOSviewer builds a research collaboration network for COPD self-management, with over 40 institutions included. Nodes represent these institutions, and their size scales with publication output to offer clear visibility of research outcomes and impact. Links between nodes show collaboration patterns and connection strength. These institutions are grouped into 5 different clusters. Look at Figure 8, each cluster is an alliance of entities formed around a common research focus or a collaboration partnership, this analytical framework can help us precisely identify the main research teams and collaboration networks in the field of self-management of chronic obstructive pulmonary disease.
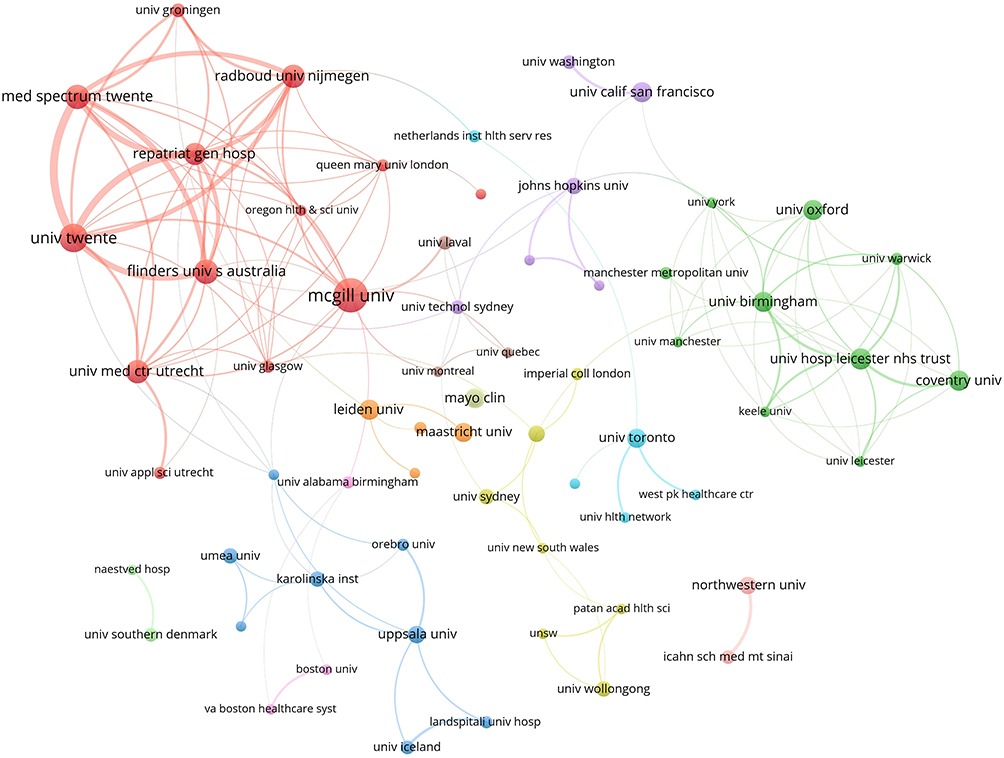 |
Figure 8 The institutional collaboration network diagram constructed by means of VOSviewer shows the collaborative relationships among 765 relevant institutions around the world, among which institutions in Europe and North America serve as the core entities for collaboration. |
An Analysis of the Correlation Mechanism Between Geographical Distribution of Research Output and Regional Resource Allocation
To find out which countries hold key influence in COPD self-management research, this study analyzed relevant publications from 46 countries. Using the data in Table 6, we focused on evaluating the top five countries with over 37 published articles. As shown in the table, this study selected the top five countries that published more than 37 articles for evaluation. The Netherlands particularly stood out, having published a total of 70 relevant articles, which were cited a total of 3394 times, with an average of 48.48 citations per article, reflecting the high quality of their research results. The United States leads in terms of total publication volume, but the number of citations per article is only 27.33, which results in “a large number of publications and average influence”. Australia has 60 COPD self-management articles, 2615 total citations, and 43.58 citations per article on average. England has 75 published articles and 2422 total citations. Both countries show strong research capabilities in this field. Their performance differences reflect how their development models vary in research investment efficiency and academic influence.
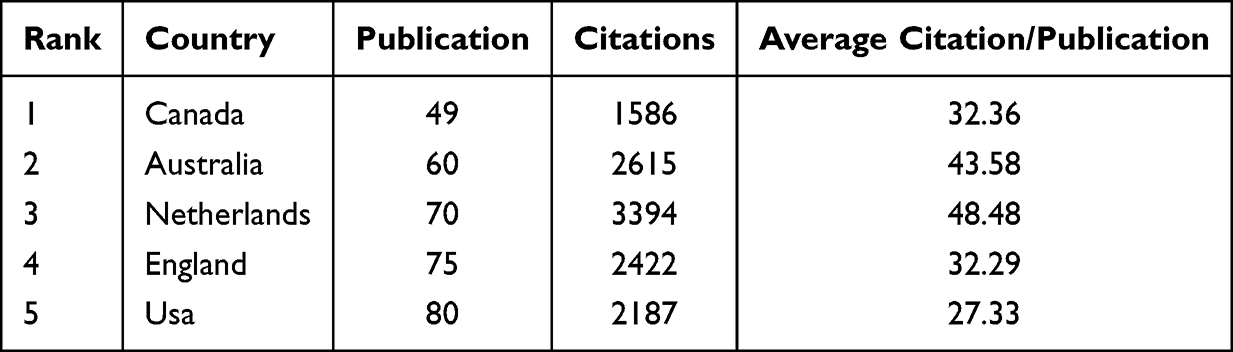 |
Table 6 National Publication Output Analysis for the Field of Chronic Obstructive Pulmonary Disease Self-Management |
Figure 9 international collaboration network shows cross-border collaboration structures in COPD self-management research. A main collaborative community focuses on Europe and North America. Relatively independent collaboration clusters exist in East Asia. This cluster distribution reflects notable regional differences in global research of this field. It affects cross-regional knowledge exchange to some extent. The weighted average silhouette coefficient stands at 0.8439 (surpassing the 0.5 threshold), which confirms that the clustering results are reliable. The network modularity index reaches 0.6346 (going beyond the 0.3 critical value), showing a notable community structure exists within the research network. Node size correlates directly with each country’s publication output. As key hub nodes, the UK and the US have established tight academic collaboration ties with the Netherlands, Canada, and Australia. China and South Korea have established somewhat independent research clusters in East Asia, with fairly limited connections to Western research communities. This observation directly shows variations in research paradigms across different regions. The network density of 0.0531 (a quantitative measure) indicates significant room for global cooperation expansion in this field. The independence of this Sino-Korean cluster might link to language barriers, as well as differences in national healthcare systems and public health priorities. It’s hard to fully show the research situation in this field if we only use the number of papers each country publishes as a statistical measure. The international cooperation trends in this article are the main force that drives global knowledge flow. Research priorities in different regions are often affected by the real challenges they face locally. For example, East Asian researchers pay more attention to things like biomass smoke exposure and population aging. Western researchers, however, tend to focus on digital-related research directions. This difference in research focus directly makes the cooperation network divided. This visualization shows the geopolitical structure of COPD self-management research clearly and provides a foundation for related collaboration.
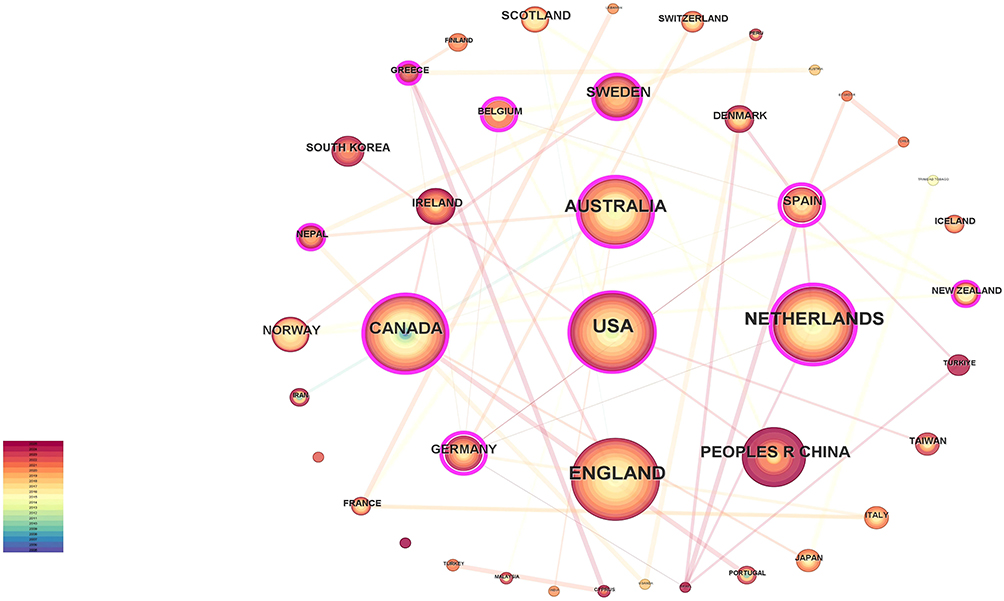 |
Figure 9 The national-level collaboration network diagram for COPD self-management research presents the respective geographical distributions and collaborative features of the Europe-North America core collaboration cluster and the East Asia collaboration cluster. |
The characteristics of resource allocation under geographical distribution are reflected in the research and health investments of the Netherlands and Australia: the total health expenditures of both countries have accounted for 9% to 10% of GDP (World Bank data: 10.1% in the Netherlands and 9.3% in Australia). The corresponding research outputs and influence have been prominent. The Netherlands has published 70 papers, with an average of 48.48 citations per paper. Australia has published 60 papers, with an average of 43.58 citations per paper. The United States, despite having the largest total investment (NIH’s COPD funding increased from USD 97 million to USD 112 million between 2008 and 2019, with an inflation-adjusted actual growth rate of approximately 16%31), has its resources scattered across multiple institutions. As a result, its research features “high output (80 papers) but moderate average citations (27.33 per paper)”, which contrasts with the Netherlands.
Southeast Asian countries have low research output, along with low total health expenditure as a share of GDP and insufficient special funds during the same period. This indicates a positive correlation between the geographical differences in research output and the intensity of regional medical resource investment—resource-rich regions are more likely to conduct high-quality COPD self-management research, while resource-constrained regions mostly focus on basic clinical issues and have insufficient investment in this field.
The East Asian cluster has relatively high health investment (World Bank data: China’s average health R&D expenditure accounts for 2.56%). However, its medical system focuses on “disease treatment” rather than “chronic disease management”, so its research mostly concentrates on “community intervention”, which differs from the Western frontier of “digital health”. This further confirms the correlation between geographical distribution and the resource allocation orientation of the medical system.
Figure 10 is a national collaboration network visualization in the COPD self-management field, intuitively showing the global pattern and core traits of international collaboration here. It covers Europe, America, Asia, Oceania and some developing countries, with dozens of participants—including research and influence leaders like the UK, US, Canada and the Netherlands, European regional players such as Iceland and Finland, and developing nations like Nepal.
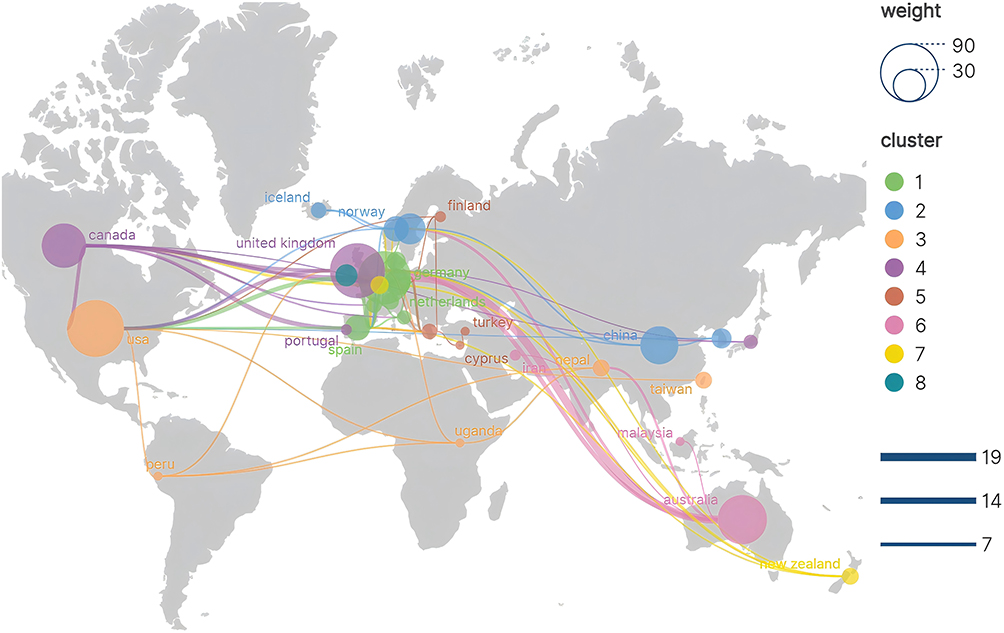 |
Figure 10 The visual analysis chart of the national collaboration network in the field of COPD self-management intuitively displays the weight ratio and cluster membership of countries like Iceland, Finland, and Canada within the collaboration network. |
The “Europe-America Core Cluster” is the most striking clustering trait of this network. The UK and the US act as twin hubs, linking the Netherlands, Australia, and Canada. Within the cluster, cooperation is close and connections stay stable Most participating countries have attained top research quality. Papers from the Netherlands average 48.48 citations each, while those from Australia have an average of 43.58 citations per paper. China and South Korea have together established an “East Asian Independent Cluster”. Nodes in this cluster share basic collaborative ties, yet cross-regional engagement with Western clusters remains limited, resulting in an overall pattern of isolated cooperation. This situation largely stems from East Asia’s focus on local practical needs—such as biomass smoke exposure—and the region’s research approaches differing from the Western “digital health-oriented” model.
The node connection density is positively correlated with the hub status, the higher the density of node connections, the more prominent the hub status usually is. The performance of the United Kingdom and the United States in the network can illustrate this point: the number of connections of the two countries is far more than that of other countries, they are the collaborative core of the European and American clusters, and they have also carried out cross-regional cooperation with countries such as Australia, and are also the key ties of global collaboration. Canada and the Netherlands have quite high research levels. They are important nodes in the Europe-America Core Cluster and connect the center with neighboring countries. Iceland and Finland also belong to this cluster, but their cooperation links are simple. They mainly rely on regional neighboring countries. For developing countries like Nepal, node connections are weak. They usually take part in a “temporary” way and act as peripheral participants. They rarely join core cooperation projects or advanced fields like digital health interventions and customized research.
Global cooperation follows a simple model: European and American countries lead, East Asia works independently, and low-development countries have limited participation. The main reasons are gaps in medical resources, different research priorities, and language and cultural barriers. This model shows that global cooperation has problems with geographical and social inequality. In the future we need to increase developing countries’ participation and improve cross-cluster cooperation efficiency through cross-regional financial alliances, localization support and other means.
Analysis of the Key Keywords
Analysis of Research Domain Vitality
This study collected documents related to the self-management of COPD globally from 2005 to 2025 and extracted 1242 keywords. In the process of keyword extraction, the research methodology proposed by Vladimir Batagelj et al was taken into account. In this study, a keyword co - occurrence network was constructed with the selection threshold of keyword occurrence frequency ≥10 (T≥10). The specific results are shown in Figure 11. In this network, it can be seen that “self - management” and “COPD” are the two core nodes. These nodes are the largest in size and have the thickest corresponding connection lines. Table 7 data shows that research in the COPD field has three central pillars. They are evidence-based structured interventions, patient-centered health outcomes, and care pathways linked to clinical practice. This setup shows that self-management strategies are the central focus and the most basic research theme in this field:
- Multicomponent intervention stands as the key focus of structured intervention in COPD self-management research. Keywords such as “rehabilitation” (227 times), “education” (217 times), and “solution” (207 times) appear with notable frequency, which lends support to this observation. The primary goal of these interventions is to equip patients with the essential skills and knowledge needed to manage their condition effectively.
- “Quality of life” (268 times) and “care” (240 times) are often mentioned in the literature. This tells us that research on patients’ health outcomes is no longer just about physiological indicators. Iit is now focusing on making patients’ daily lives better and improving their real-life experiences.
- In clinical management research, “obstructive pulmonary disease” (372 mentions) connects closely with relevant keywords. “Chronic obstructive pulmonary disease” itself appears 492 times, a notably high frequency. Together, these findings confirm that academic research in this area aligns well with clinical disease management.
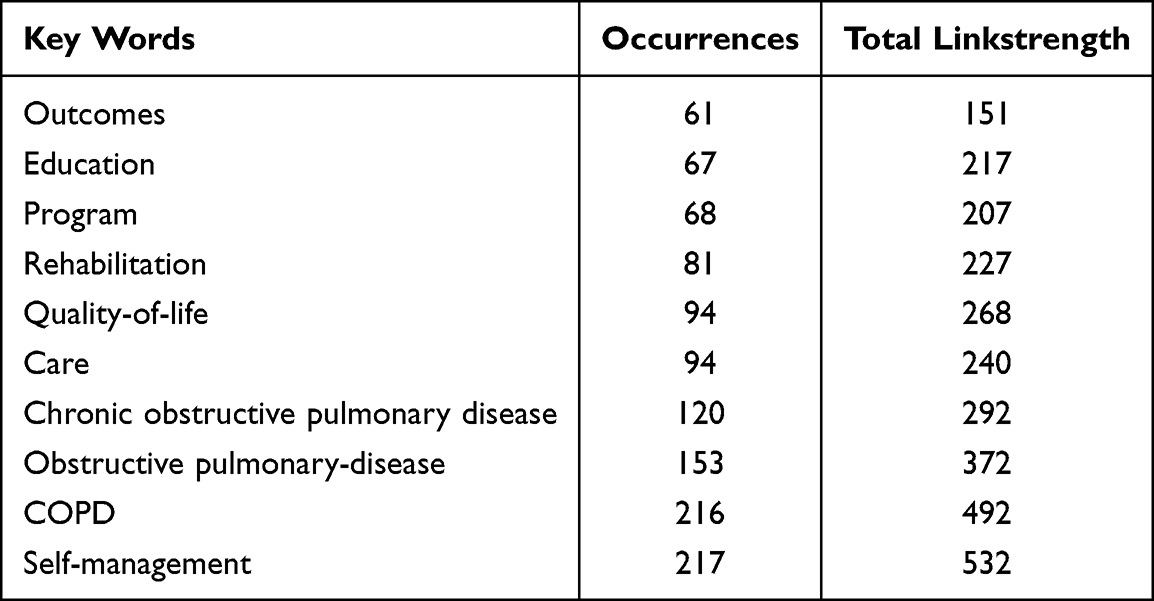 |
Table 7 Core Keyword Frequency & Association Analysis Table for COPD Self-Management Research |
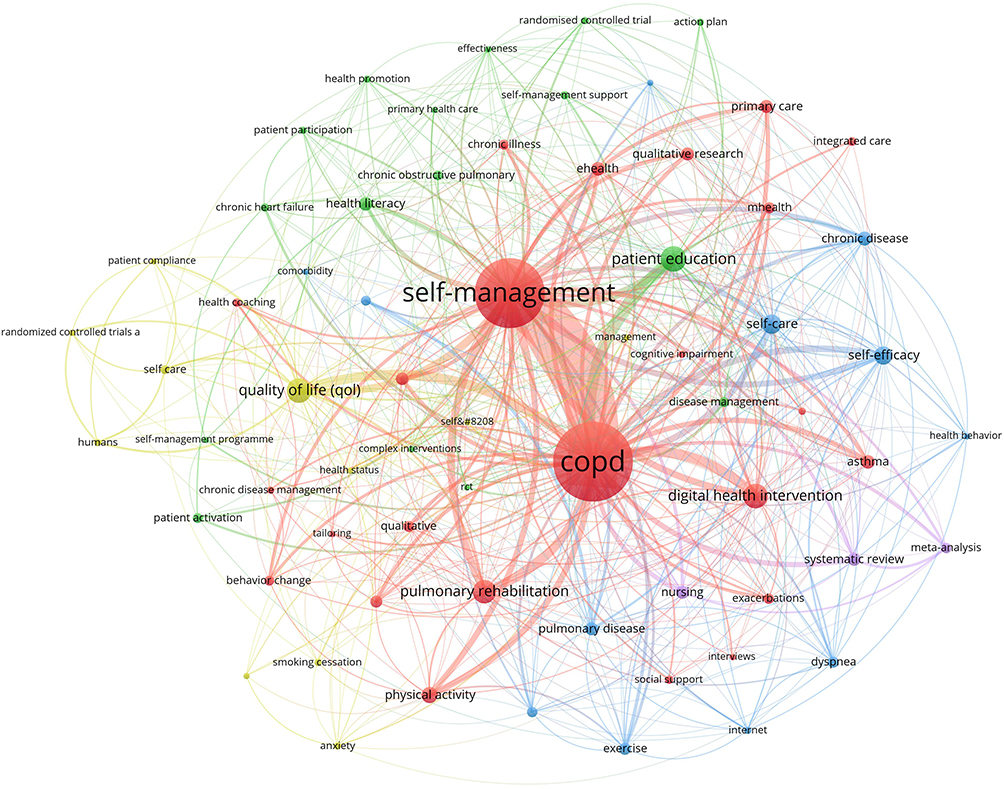 |
Figure 11 The visualization map of core keyword relationships in COPD self-management research intuitively presents the association network among core terms such as “COPD”, “self-management”, and “digital health intervention”, while clearly showing the distribution of research themes in this field. |
Research on COPD self-management has evolved from a general concept into a mature academic area, with existing research frameworks clearly showing that structured interventions offer practical benefits to patients.
Keyword Clustering View Analysis
In this study, we conducted a comprehensive visualization analysis of literature related to chronic disease self-management from 2005 to 2025 using CiteSpace 6.4 software. Figure 12 shows eight major research clusters (modularity Q = 0.3624, silhouette S = 0.8439) with clear, distinct knowledge structures (average memorability = 0.7172). Cluster trajectories visually reflect the inherent research logic: “chronic diseases” (clusters 0 and 1), “health literacy” (cluster 2), and finally “interventions” (cluster 6). The clustering results of this study show good robustness. The silhouette values of central clusters #0, #2, #6, and #7 all exceed 0.81 (S > 0.5 means the clustering is reliable). The overall modularity Q = 0.3624 (Q > 0.3 confirms the clustering structure is significant). Central clusters build the research framework by their functions. Cluster #0 “Diseases” is the basic node. Cluster #1 “Diseases” and Cluster #2 “Health literacy” form the health literacy dimension. Cluster #2 and Cluster #7 “Digital health” have an inter-cluster correlation. Cluster #6 “Intervention measures” forms the clinical practice axis. Secondary clusters add more dimensions to the research. Cluster #3 “Palliative care” and Cluster #5 “Patients with chronic diseases” emphasize the patient-centered orientation. Cluster #4 “Chronic disease management model” stands for the systematic management field. Cluster #8 “Project evaluation” focuses on effectiveness evaluation. Through research on common chronic disease self-management, we identified three core knowledge areas: “chronic disease - health management capacity - intervention measures”. Network density (0.0302) indicates strong connections between nodes. Patient education (#2) serves as a key link between “digital health” and “intervention measures”, supporting the translation of patients’ disease knowledge into clinical practice.
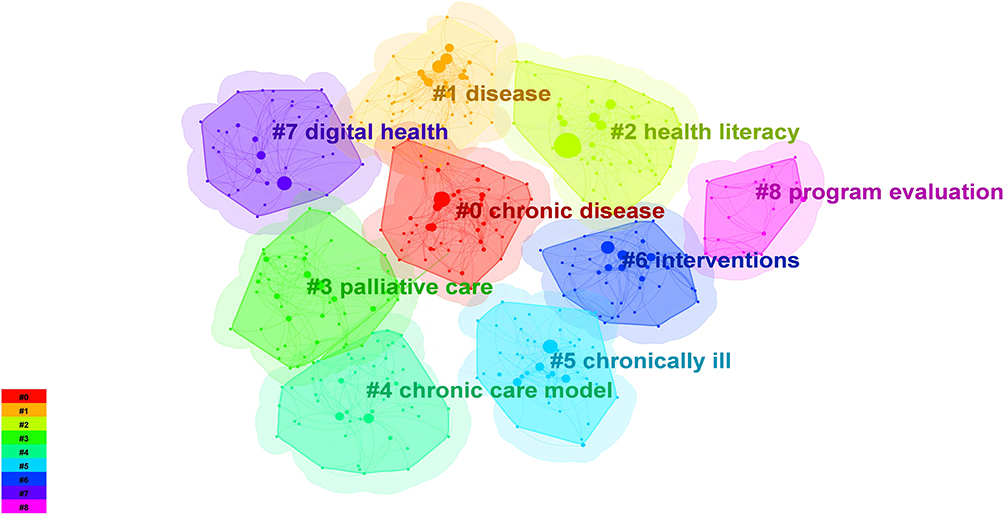 |
Figure 12 The figure visualizes keyword clustering results of COPD self-management research using CiteSpace software, with reliable clustering performance. It includes nine core thematic clusters covering basic research, patient capability enhancement, intervention implementation, and effect evaluation, reflecting inter-theme knowledge flow and the field’s knowledge system. |
We analyzed the core themes of these clusters and their associations with the existing chronic disease management framework. This research focuses on the pathological characteristics of COPD (such as “airway obstruction” and “chronic inflammation”) and important outcomes for patients (such as “health status” and “quality of life”). “Chronic diseases” (#0) and related “diseases” (#1) form the basic categories in this field. This classification also corresponds to the central direction of the academic field that has long emphasized quantifying the burden of diseases and patients. Category 2 “Health literacy” is closely related to Category 6 “Intervention measures” and has significant impact. The core of “Health literacy” can be described with co-occurring terms like “Enhanced awareness” and “Knowledge acquisition”. It plays an important intermediate role in carrying out “Intervention measures” (eg, “Behavioral advice” and “Application of digital tools”). This association matches classic behavioral theories such as the Health Belief Model and Social Cognitive Theory. All these theories stress that knowledge transfer and self-efficacy are key drivers of continuous behavior change in chronic disease management. Our team’s recent case series analysis provides quantitative evidence: a digital health-based health literacy intervention can improve treatment adherence among COPD patients by 18%. This data confirms the practical value of the 7th “Digital Health” cluster and fills the evidence gap on “how digital technologies translate into real improvements in patient outcomes”. It also confirms its central role as an independent research cluster in COPD self-management — the physical intervention dimension it focuses on meets clinicians’ real needs for patient self-management tools. Looking at terminological connections, the frequent co-occurrence of “digital health” with “intervention effectiveness” and “daily management” shows it is not an isolated technical concept. Instead, it is a practical paradigm rooted in behavior reinforcement theory and chronic disease self-efficacy theory. Could this mean future research can focus on the combined use of digital tools and theoretical frameworks to provide new breakthrough directions for optimizing the COPD self-management model. Category 3, “palliative care”, mainly centers on the clinical care requirements of patients with advanced COPD. Related key terms cover “symptom management” and “quality of life maintenance”. Category 8, “project evaluation”, looks into specific ways to improve intervention programs, with a focus on areas like “effectiveness verification” and “cost-effectiveness”. The combined display of these two themes clearly shows the balance in this field between advancing clinical practices and guaranteeing methodological rigor.
Based on the results of keyword clustering analysis in the field of self-management of COPD, this study constructed a keyword clustering timeline knowledge graph. By analyzing the keyword timeline Figure 13, it can be found that the research topics in the field of “self-management of chronic obstructive pulmonary disease” have been constantly changing over time, and have shown multi-dimensional development characteristics at different stages. From 2005 to 2025, research on the self-management of chronic obstructive pulmonary diseases has been actively carried out. As the knowledge map shows, topics such as chronic diseases, self-management, health information comprehension, intervention methods, and primary care have long been at the core of research in this field and continue to attract the attention of the academic community. Analysis shows that core topics in this field include quality of life (qol), acute exacerbation of chronic obstructive pulmonary disease, and randomized controlled trials — all have been studied consistently. Between 2020 and 2025, academics have grown more interested in digital health interventions, self-management support, and project evaluation. These fields are now at the research forefront. From the emerging keyword analysis Figure 14, research hotspots on COPD self-management change across different periods. The key keywords are “randomized controlled trial”, “intervention measures” and “health literacy”. This development drives a shift in research paradigm, with three key focuses: standardizing research methods, applying tools in clinical practice, and enhancing patients’ capabilities.
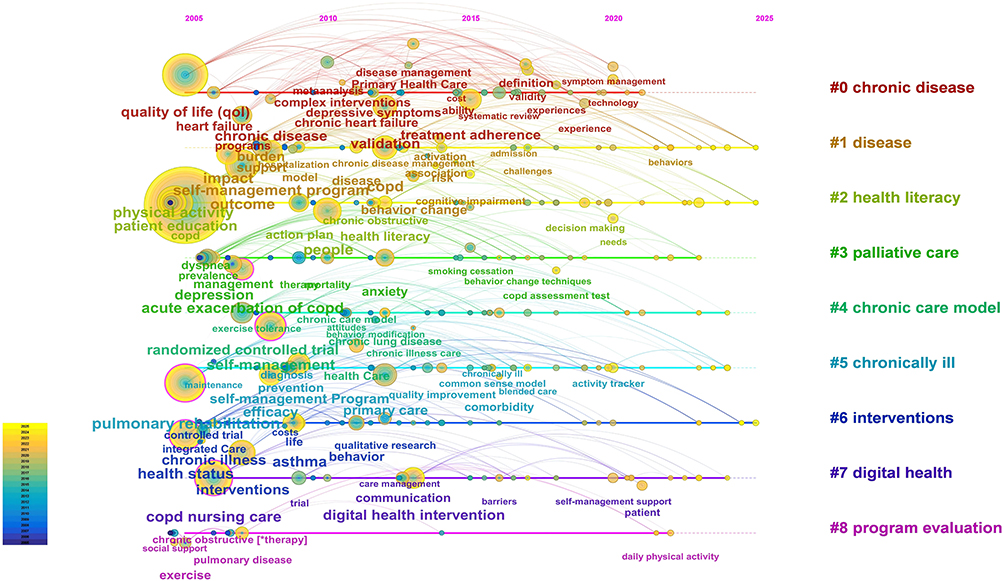 |
Figure 13 The timeline map of keyword clustering in COPD self-management research constructed based on CiteSpace clearly shows the temporal development process of various thematic clusters in this field from 2005 to 2025, as well as the changing trajectory of research hotspots. |
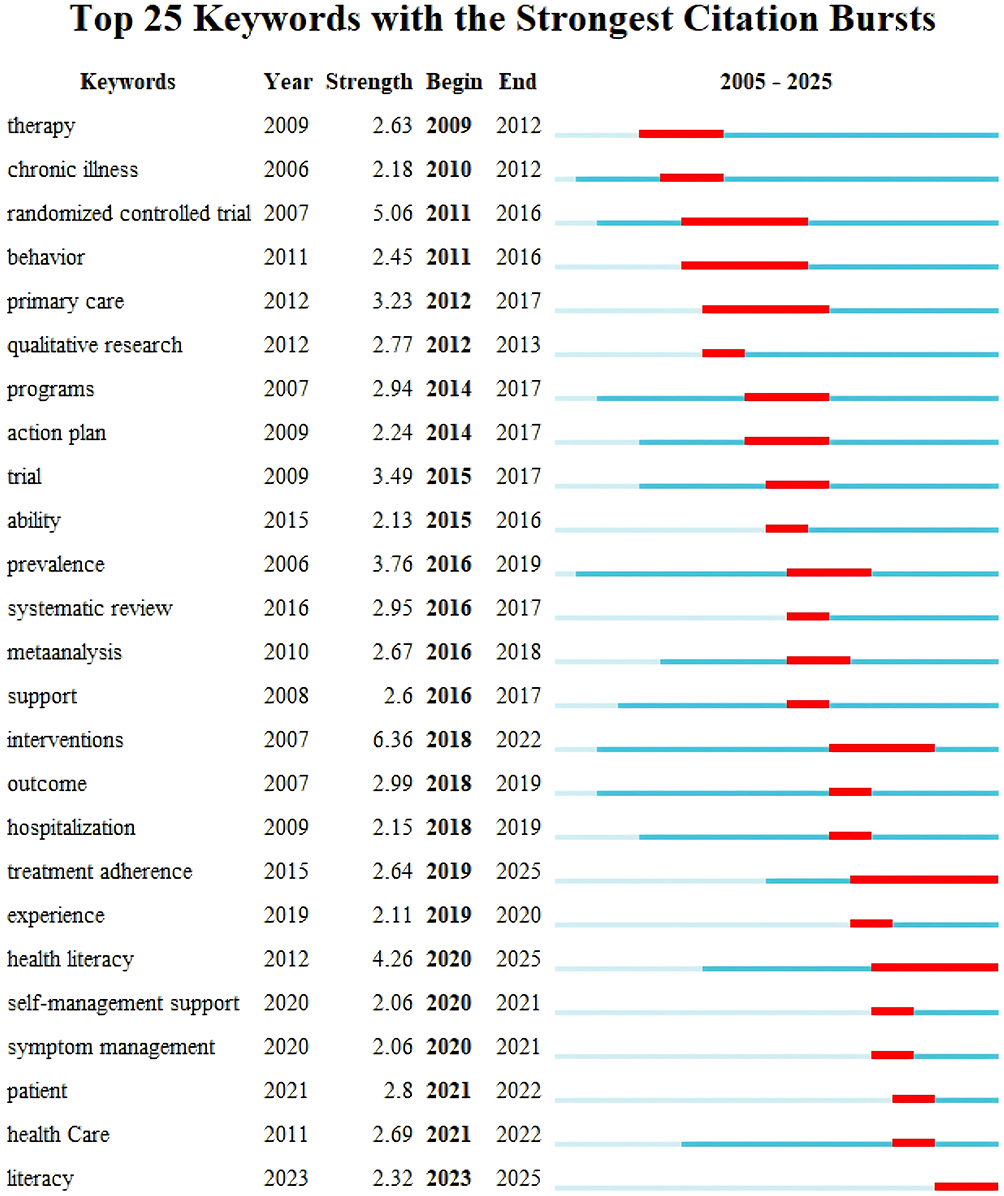 |
Figure 14 The keyword burst analysis map in the field of COPD self-management lists 25 keywords with high burst intensity in detail, and presents the dynamic change trends of research frontiers in this field in different periods through these keywords. |
From 2005 to 2014, research in this field centered on two key topics: “randomized controlled trials” (burst strength 5.06) and “primary care” (burst strength 3.23).
From 2015 to 2019, research focused on intervention themes. Key examples are “intervention measures” (appearance intensity 6.36) and “behavior change” (appearance intensity 3.89).
After 2020, research on patients’ capabilities grew a lot. It focused on areas like “health literacy” (appearance intensity 4.26) and “treatment compliance” (appearance intensity 2.64).
This shift may carry twofold implications:
Research focus is slowly moving to a practical approach, this change itself has positive meaning. Research on COPD self-management develops a methodological framework around standardized verification and application in specific scenarios, with the primary goal of improving patients’ health awareness and treatment compliance. This indicates that the field is developing in a direction that is more in line with clinical needs, pays more attention to individual differences among patients, and attaches greater importance to the sustainability of effects, striving to transform research conclusions into precise programs applicable to daily management.
On the negative side, there is a potential problem of “excessive binding of capability improvement to technology”, and in particular, the tendency of “technology hype” needs to be guarded against. Currently, most studies on “health literacy” and “treatment adherence” rely on digital tools (such as intelligent popular science apps and medication reminder systems) to implement interventions, but this kind of “technology-dependent capability improvement model” needs to be viewed rationally. A key question has not been fully answered: Is the evidence base of existing intervention studies on patients’ capabilities combined with digital technology sufficiently solid? In our dataset, the proportion of large-scale randomized controlled trials (RCTs) with sound design and covering diverse patient groups (such as elderly patients and people with low digital literacy) in relevant studies still needs to be increased. Many studies are still in the stage of small-scale pilots, and their long-term effects of improving health literacy/adherence with the help of digital tools, cost-effectiveness under different medical resource environments, and actual improvement effects on core clinical indicators of COPD (such as acute exacerbation rate) still require verification through larger-scale studies.
To a certain extent, the evolution of this research hotspot is consistent with the “peak of inflated expectations” in the technology maturity curve — this reminds the academic and clinical communities that a balance needs to be struck between the enthusiasm for “digital technology empowerment” and the rigor of “clinical effect first”, so as to avoid over-reliance on technical means to improve patients’ capabilities while ignoring the universality and core clinical value of interventions.
Analysis of Application Distribution and Practical Efficacy of Behavioral Change Theoretical Models
Characteristics of Application Distribution
Drawing on the 426 included studies, we identified the application characteristics and practical effects of behavioral change theoretical models in the field of COPD self-management through keyword co-occurrence, thematic clustering, and content mining, with specific details presented as follows:
Table 8 the Theory of Planned Behavior (TPB) accounts for the highest proportion of applications in this field (66.0%), with its keyword co-occurrence frequency significantly exceeding that of other models. The core reason lies in its ability to accurately align with the logical chain of “behavioral intention - self-management practice” and its strongest association with “health literacy - interventions” in cluster analysis, However, attention should be paid to the limitations of this model—it has relatively weak explanatory power for patients’ “behavior maintenance” (eg, long-term adherence to rehabilitation exercises). In contrast, models such as Motivational Interviewing and Social Cognitive Theory have relatively low application proportions (all less than 2%), yet their co-occurrence frequency with keywords like “digital health interventions” and “personalized care” has shown an upward trend since 2020. In the future, its “observational learning + self-regulation” mechanism can be used to optimize the interactive design of digital interventions and enhance the sustainability of behavioral changes.
 |
Table 8 Application and Efficacy Characteristics of Behavioral Change Theoretical Models in COPD Self-Management |
The efficacy data of each model are derived from specific research scenarios, therefore, in clinical application, personalized selection should be made based on the characteristics of patient groups (such as age and digital literacy) to avoid the “one-size-fits-all” application model.
Analysis of Practical Efficacy
The practical effects of all models have been supported by empirical studies: The Theory of Planned Behavior enhances patients’ willingness to engage in rehabilitation exercises and standardized medication use effectively through the pathway of “attitude - subjective norm - perceived behavioral control”; Motivational Interviewing focuses on “motivation enhancement” and demonstrates outstanding performance in improving patients’ short-term intentions for behaviors such as smoking cessation and physical activity; The Social Cognitive Theory provides a theoretical basis for the design of digital health tool interventions by relying on the “observational learning - self-regulation” mechanism, with its effects being particularly evident in the scenario of remote self-management; The Transtheoretical Model achieves accurate matching of intervention programs by dividing the stages of behavioral change, addressing the drawback of “homogeneity” in traditional interventions.
Citation Analysis of the Literature
Reference citations can, to a certain extent, reflect the core literature within a research field. Through an analysis of 426 articles, a total of 11,061 references were collectively cited. As presented in Figure 15, an examination of publications cited no fewer than 10 times (T ≥ 10) identified 201 highly influential articles, this map centers on key highly cited papers like Zwerink (2014) and Bourbeau (2003) as nodes, clustering them into themed groups—red for self-management, blue for theoretical frameworks and behavioral intervention mechanisms, green for clinical intervention, etc.—to show how research in this field connects and diverges, from long-term disease management to digital-based interventions, from which a co-citation network graph was subsequently generated.
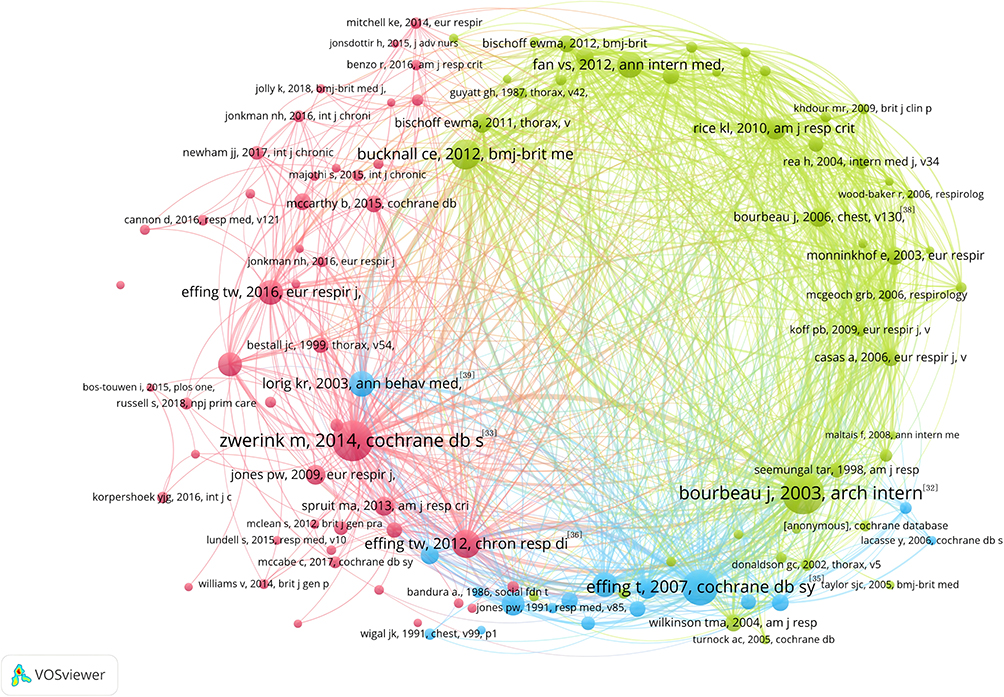 |
Figure 15 The co-citation analysis map of COPD self-management literature generated with the help of VOSviewer can present the co-citation association relationships among high-impact literatures in this field, and at the same time show the clustering characteristics of these literatures. |
A comprehensive analysis was conducted on the top 10 most-cited publications meeting the threshold of citations ≥ 53 (T ≥ 53), which are widely regarded as seminal works in this field. The analytical findings are presented in Table 9. These highly influential papers provide critical insights into the research priorities and evolutionary trajectories of the discipline, this table ranks the top 10 most-cited publications in the COPD self-management field by their citation counts: Bourbeau j’s 2003 work takes first place with 104 citations, while zwerink m’s 2014 publication comes in second with 100 citations.
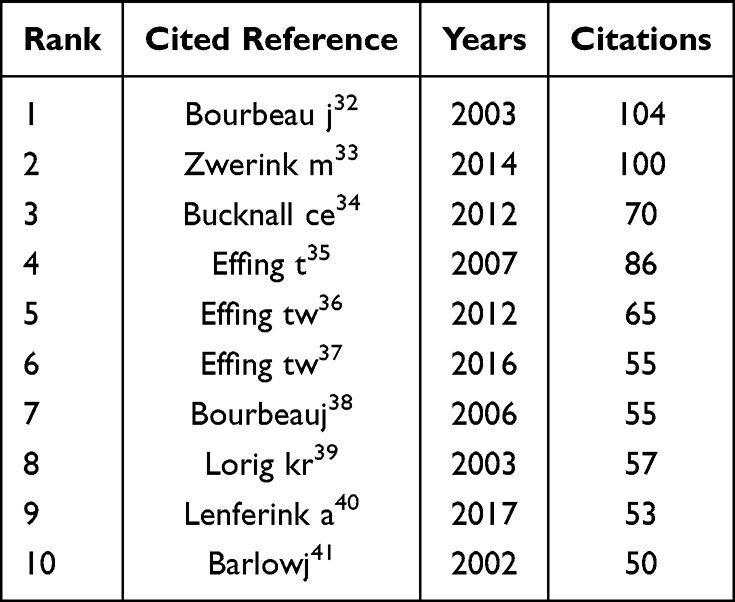 |
Table 9 Ranking of Highly Cited References in the COPD Self-Management Field (Sorted by Citation Count) |
If two academic papers are frequently cited together in subsequent research, this generally suggests that there is a substantial conceptual relationship within the academic discussion. This is the core logic of co-citation analysis. The core of this commonly used bibliometric method lies in tracking the co-citation frequency of published pairs of publications to discover the hidden intellectual connections in academic literature and provide a quantitative basis for organizing the ideological context of the relevant field. The co-cited reference knowledge graph Figure 16 includes 764 nodes and 2624 connections, with a network density of 0.0099 and distinct clustering patterns (modularity Q=0.58, well above the 0.3 threshold for significant community structure). Among the top 10 most-cited works, key studies such as Bourbeau (2003) and Zwerink (2014) provided critical evidence for the self-management component of the GOLD guidelines, and their findings continue to shape clinical practice and academic research to date. We found three main document clusters by analyzing key nodes. Bourbeau (2003) and Effing (2007)’s studies set up the central theoretical framework for self-management. Zwerink (2014), Trappenburg (2011) and others’ research developed clinical behavioral intervention plans. Russell (2018) and McCarthy (2018) first built a digital management model.
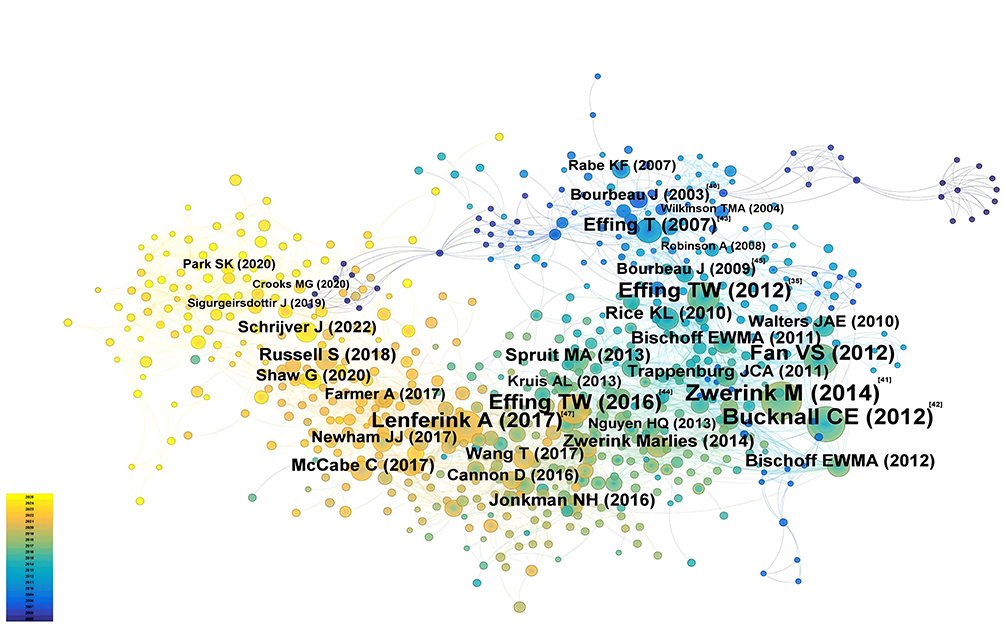 |
Figure 16 The co-citation literature analysis map in the field of COPD self-management drawn based on CiteSpace can clearly show the co-citation relationships among core literatures represented by studies related to Bourbeau J and Effing T, as well as the knowledge inheritance context of this field. |
Discussion
Combining CiteSpace and VOSviewer for the analysis, we moved beyond simple numerical summaries to clarify the overall landscape of COPD self-management research. This work traces the evolution of research hot topics and clarifies the knowledge structures and collaboration networks that have emerged over the past two decades. Below is a detailed discussion of key findings.
Research Growth Patterns: What Drives Peaks, and Why Do Disparities Linger?
Scientific articles published between 2020 and 2021 peaked at 41 per year. This matches two major changes. The 2020 GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines included self-management as key intervention. The pandemic promoted telemedicine spread and reduced hospitalization rate.42 Growth has inequalities, resource-poor regions like South Asia and sub-Saharan Africa have few related scientific publications but make up 30% of global COPD-related deaths.43 Research now focuses on high-income countries. The regions most affected by the disease and most needing self-management strategies get little researchers’ attention. This clear difference is the heart of the problem.
Research results show research focuses on digital healthcare tools and customized treatment plans. It overlooks areas with little resources and high biomass exposure. It does not meet the real management needs of clinical settings.
Collaboration Networks: Structural Gaps and Quality-Volume Trade-Offs
In international research on chronic obstructive pulmonary disease, differences between the West and East Asia are very clear. For cooperation, European and North American countries (like the Netherlands, the UK, the US) have built close cooperation networks. Relevant papers have 27.33 to 48.48 citations, which is quite high. East Asian countries such as China and South Korea are relatively isolated in international cooperation. These regional differences also show in research focuses. Western scholars prefer to explore digital health tools. East Asian research teams mainly study chronic obstructive pulmonary disease related to biomass smoke.
Developed countries focus on digital intervention technologies. The reason is the practical problem of poor patient compliance. In East Asia, biomass smoke exposure is a big problem that needs attention. Local researchers pay more attention to making personalized management plans through their studies.
North America and Europe show a striking gap in citation performance in COPD self-management research: North American papers have an average of 27.33 citations per article, 43% lower than the 48.48 from the Netherlands in Europe. This disparity points to a core issue in international collaboration— “networking without effective integration”—rooted in the mismatch between research output and quality. The key driver behind the citation gap is North America’s research focus: most studies are small-scale empirical investigations, with far fewer large-scale trials that carry wide influence. This unbalanced research orientation not only fails to fully leverage the strengths of each region but also prevents effective integration of East Asian teams’ insights from biomass research and Europe’s strict clinical trial methodologies.
Strategic Implications and Evidence-Based Actions
Global research on COPD self-management is very fragmented. This key finding of the study gives clear guidance for future work. When we compare regions, we see different patterns: Europe has built a strong core of high-impact research, North America leads in the number of published papers, and East Asia is relatively isolated with little international collaboration. To fix this fragmentation, we have made specific plans for key stakeholders. The goal is to help build more global cooperation in this field:
For International Research Funders
We will advance the Trans-Pacific Research Alliance through multi-party collaboration. The European Union’s “Horizon Europe” program, US National Institutes of Health (NIH), and National Natural Science Foundation of China (NSFC) are working together to set up a special fund. This fund will be essential support for building the alliance.
We have set three key research areas based on the basic principle of utilizing the region’s strengths:
- “Digital health adaptation” is about combining Western digital health tools with East Asia’s social service models. This helps make technology rollout more effective;
- In the “Biomass energy” field, we can learn from East Asia’s experiences. We also use the rigor of Western experimental protocols. This makes intervention projects more scientifically effective;
- Localized solutions for low- and middle-income countries: Based on basic data from Africa and South Asia, we will integrate global resources and develop solutions tailored to local needs.
Governance Mechanism
We may consider setting up a special steering committee. It will make sure Europe, North America, East Asia, and low- and middle-income countries have fair representation. The committee will meet every year. It will check how the research is going, reevaluate priorities if needed, and help the collaboration go well.
For Research Institutions and Universities
There’s a problem in the academic community: people “emphasize quantity more than quality”. Reforming the academic reward system may help solve this problem. When checking for promotion or regular jobs, do not just use traditional bibliometric indicators. You should also consider important research achievements. For example, research that helps create international clinical guidelines, research that develops evaluation scales used around the world, and influential papers published in practice-related journals.
Each region has its own unique traits and strengths, and they fit well together. Make a knowledge exchange platform. Partners from different groups of organizations — like the East Asian cluster — can work together here. Focus on active participation, helping each other, making research plans, and using everyone’s strengths well. This way, we can solve global problems.
For National Health Systems and Policymakers
European research’s influence stems from the strong coordination across its entire healthcare system. This example offers a clear takeaway: policymakers might encourage “field-based research”, urging researchers to address healthcare needs while keeping patients’ true priorities in mind.
Some parts of East Asia have their own separate research groups. Local health offices focus on two key jobs. Turn international evidence-based materials into practice guides that work locally. Check if these guides fit the local culture. Back special studies on regional public health problems — like air pollution and specific ways of eating. Add real data to the world’s public health knowledge bank.
Key Insights from Bibliometric Data: A Policy Relevance Perspective
From the perspective of policy relevance, the bibliometric data of this study also identifies three key issues that are of great significance for promoting policy improvement in this field. Research on COPD self-management in the Netherlands is characterized by “high influence but low publication volume”36: although the number of published papers is less than that in the United States, the citation performance of its research outcomes is significantly better. This advantage stems from the rigorous research methodology adopted in Dutch academia, the close collaboration between clinical and academic teams, and the “quality-over-quantity” funding policy of the Netherlands Organization for Health Research and Development (ZonMw).44 This development model provides practical ideas to better link academic research with its specific impacts.
Patients with COPD can engage in real-time health management using personalized digital tools, which deliver practical support.45,46 Beyond simple technological advancement, these tools pave the way for novel treatment paradigms. Yet digital divide, data protection concerns and related challenges may compromise long-term effectiveness. Proactive policies are therefore needed to facilitate integration of such tools into routine clinical practice and ensure their appropriate governance.47
Research Limitations
This research carries certain limitations that warrant acknowledgment:
- Web of Science database often includes English academic journals and well-known Western journals. Its high-quality metadata is useful for literature analysis. But relying only on this database may miss important research results in non-English journals, Scopus, PubMed, and region-specific databases. So be aware of this bias — most importantly when looking at geographical distribution in Asia, Africa, South America and research institution participation. Future studies work better with multiple databases together.
- We tried to be as objective as possible, but personal judgments may have affected the manual selection. But do not worry—we followed strict steps to reduce this. For this survey, we did independent double-checks to make sure evaluators agreed.
- Two related studies from 2003 had clear differences. Bourbeau’s study focused on cutting readmission rates, got 104 total citations and became noticed in the scientific community. Lorig’s study put forward a self-management education framework, focusing more on patients’ problem-solving skills than disease-related knowledge. This study only got 57 citations but has more practical value in low- and middle-income countries. This difference shows the limits of bibliometric analysis — citation numbers, a key evaluation rule, cannot accurately judge research impact in clinical work.
Conclusion
This study conducted a bibliometric analysis on the self-management field of COPD. As a result of analyzing 426 innovative research achievements, three important findings were summarized.: Research on this theme has progressed steadily across different phases. Early efforts centered on building theoretical foundations, with subsequent work involving clinical validation and recent strides in technological use. Current focus should move toward larger and more practical randomized studies, rather than confining work to small feasibility trials. This approach will produce reliable evidence for digital health tools tailored to boost health literacy. A robust knowledge inheritance framework emerges from co-citation network analysis. Future research should actively link basic knowledge with emerging disciplines. Integrating behavioral science theories into intervention design, for instance, can improve research efficiency and reproducibility. In this study, we conducted a systematic investigation into COPD self-management, aiming to clarify the epistemological shifts, knowledge frameworks, and global research trends within the field. This work provides a foundation for developing tailored research agendas and refining clinical practice strategies. Turning to global research dynamics, international collaboration exhibits distinct regional specialization. In response to this, funding bodies and research institutions may launch targeted collaborative initiatives.
Acknowledgment
This project has made significant progress thanks to the sincere investment of each team member. It is their enthusiastic work and valuable contributions that have made everything possible.
Author Contributions
Xingyu Huang and Jiacai Feng led PRISMA-compliant literature retrieval, screening, and dual-independent review (Cohen’s Kappa=0.85), identifying 426 valid articles. Rongqing Wu and Luxiong Zheng performed data cleaning/standardization and assisted in CiteSpace/VOSviewer-based visualizations. Xiaoting Gan and Cui Su focused on result interpretation, including keyword clustering and research hotspots, providing key evidence for discussions. Renli Deng proposed the research topic and overall design, led study implementation, oversaw academic quality, and coordinated paper drafting/revision. All authors made substantial contributions to the design and conception of the study, and acquisition, analysis and interpretation of data, and took part in either drafting or revising the manuscript. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–29. doi:10.1016/s2214-109x(23)00217-6
2. Kong CW, Wilkinson TMA. Predicting and preventing hospital readmission for exacerbations of COPD. Erj Open Research. 2020;6(2):325. doi:10.1183/23120541.00325-2019
3. WHO Guidelines Approved by the Guidelines Review Committee. WHO Guideline on Self-Care Interventions for Health and Well-Being, 2022 Revision. World Health Organization © World Health Organization 2022; 2022.
4. Duckworth C, Cliffe B, Pickering B, et al. Characterising user engagement with mHealth for chronic disease self-management and impact on machine learning performance. NPJ Digit Med. 2024;7(1):66. doi:10.1038/s41746-024-01063-2
5. Newham JJ, Presseau J, Heslop-Marshall K, et al. Features of self-management interventions for people with COPD associated with improved health-related quality of life and reduced emergency department visits: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:1705–1720. doi:10.2147/copd.S133317
6. Galev G, Nagoti S, Sansano I, Armstrong SM, Herman M, Mukhopadhyay S. Smoking and the lung: landmark papers (1929–2023). J Diagn Acad Patholo. 2024;1(1):3–12. doi:10.4103/jdap.jdap_9_24
7. Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
8. Kainu A, Timonen K, Lindqvist A, Piirilä P. GOLD criteria overestimate airflow limitation in one-third of cases in the general Finnish population. ERJ Open Res. 2016;2(4):00084–2015. doi:10.1183/23120541.00084-2015
9. Martinez-Pozas O, Melendez-Oliva E, Rolando LM, Rico JAQ, Corbellini C, Sanchez Romero EA. The pulmonary rehabilitation effect on long covid-19 syndrome: a systematic review and meta-analysis. Physiother Res Int. 2024;29(2):e2077. doi:10.1002/pri.2077
10. Stephan P, Veugelers R, Wang J. Reviewers are blinkered by bibliometrics. Nature. 2017;544(7651):411–412. doi:10.1038/544411a
11. Liu Y, Huang J, Li E, et al. Analysis of research trends and hot spots on COPD biomarkers from the perspective of bibliometrics. Respir Med. 2025;240:108030. doi:10.1016/j.rmed.2025.108030
12. Rousseau R. Library science: forgotten founder of bibliometrics. Nature. 2014;510(7504):218. doi:10.1038/510218e
13. Durieux V, Gevenois PA. Bibliometric indicators: quality measurements of scientific publication. Radiology. 2010;255(2):342–351. doi:10.1148/radiol.09090626
14. Lv H, Hua Q, Wang Y, et al. Mapping the knowledge structure and emerging trends of efferocytosis research: a bibliometric analysis. Am J Transl Res. 2023;15(2):1386–1402.
15. Chen C, Hu Z, Milbank J, Schultz T. A visual analytic study of retracted articles in scientific literature. J Am Soc Inf Sci Technol. 2012;64(2):234–253. doi:10.1002/asi.22755
16. Chen C, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: a scientometric update (2000 - 2014). Expert Opin Biol Ther. 2014;14(9):1295–1317. doi:10.1517/14712598.2014.920813
17. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. 2005;57(3):359–377. doi:10.1002/asi.20317
18. Chen C, Ibekwe‐SanJuan F, Hou J. The structure and dynamics of cocitation clusters: a multiple‐perspective cocitation analysis. J Am Soc Inf Sci Technol. 2010;61(7):1386–1409. doi:10.1002/asi.21309
19. Chen C. A glimpse of the first eight months of the COVID-19 literature on microsoft academic graph: themes, citation contexts, and uncertainties. Front Res Metr Anal. 2020;5:607286. doi:10.3389/frma.2020.607286
20. Sabe M, Pillinger T, Kaiser S, et al. Half a century of research on antipsychotics and schizophrenia: a scientometric study of hotspots, nodes, bursts, and trends. Neurosci Biobehav Rev. 2022;136:104608. doi:10.1016/j.neubiorev.2022.104608
21. Chen CM, Leydesdorff L. Patterns of connections and movements in dual-map overlays: a new method of publication portfolio analysis. J Assoc Inf Sci Technol. 2014;65(2):334–351. doi:10.1002/asi.22968
22. Mittermeir R, Knorr KD. Scientific productivity and accumulative advantage: a thesis reassessed in the light of international data. R&D Management. 2007;9(s1):235–239. doi:10.1111/j.1467-9310.1979.tb01302.x
23. Coile RC. Lotka’s frequency distribution of scientific productivity. J Am Soc Inf Sci. 2007;28(6):366–370. doi:10.1002/asi.4630280610
24. Bornmann L, Mutz R. Growth rates of modern science: a bibliometric analysis based on the number of publications and cited references. J Assoc Inf Sci Technol. 2015;66(11):2215–2222. doi:10.1002/asi.23329
25. Vogelmeier CF, Criner GJ, Martínez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Arch Bronconeumol. 2017;53(3):128–149. doi:10.1016/j.arbres.2017.02.001
26. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
27. Bourbeau J, Saad N, Joubert A, et al. Making collaborative self-management successful in COPD patients with high disease burden. Respir Med. 2013;107(7):1061–1065. doi:10.1016/j.rmed.2013.03.003
28. Waltman L, Calero‐Medina C, Kosten J, et al. The Leiden ranking 2011/2012: data collection, indicators, and interpretation. J Am Soc Inf Sci Technol. 2012;63(12):2419–2432. doi:10.1002/asi.22708
29. Leydesdorff L, de Moya-Anegón F, de Nooy W. Aggregated journal-journal citation relations in scopus and web of science matched and compared in terms of networks, maps, and interactive overlays. J Assoc Inf Sci Technol. 2016;67(9):2194–2211. doi:10.1002/asi.23372
30. Leydesdorfl L, Wagner CS, Porto-Gomez I, Comins JA, Phillips F. Synergy in the knowledge base of US innovation systems at national, state, and regional levels: the contributions of high-tech manufacturing and knowledge-intensive services. J Assoc Inf Sci Technol. 2019;70(10):1108–1123. doi:10.1002/asi.24182
31. Ballreich JM, Gross CP, Powe NR, Anderson GF. Allocation of national institutes of health funding by disease category in 2008 and 2019. JAMA Network Open. 2021;4(1):e2034890. doi:10.1001/jamanetworkopen.2020.34890
32. Bourbeau J, Julien M, Maltais F, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management intervention. Arch Intern Med. 2003;163(5):585–591. doi:10.1001/archinte.163.5.585
33. Zwerink M, Brusse-Keizer M, van der Valk P, et al. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;2014(3):Cd002990. doi:10.1002/14651858.CD002990.pub3
34. Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060. doi:10.1136/bmj.e1060
35. Effing T, Monninkhof EM, van der Valk PD, et al. Self-management education for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2007;(4):CD002990. doi:10.1002/14651858.CD002990.pub2
36. Effing TW, Bourbeau J, Vercoulen J, et al. Self-management programmes for COPD: moving forward. Chron Respir Dis. 2012;9(1):27–35. doi:10.1177/1479972311433574
37. Effing TW, Vercoulen JH, Bourbeau J, et al. Definition of a COPD self-management intervention: international Expert Group consensus. Eur Respir J. 2016;48(1):46–54. doi:10.1183/13993003.00025-2016
38. Bourbeau J, Nault D, Dang-Tan T. Self-management and behaviour modification in COPD. Patient Educ Couns. 2004;52(3):271–277. doi:10.1016/s0738-3991(03)00102-2
39. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
40. Lenferink A, Brusse-Keizer M, van der Valk PD, et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8(8):Cd011682. doi:10.1002/14651858.CD011682.pub2
41. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns Oct–Nov. 2002;48(2):177–187. doi:10.1016/s0738-3991(02)00032-0
42. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
43. de Oca MM, Perez-Padilla R, Celli B, et al. The global burden of COPD: epidemiology and effect of prevention strategies. Lancet Respir Med. 2025;13(8):709–724. doi:10.1016/S2213-2600(24)00339-4
44. Duenk RG, Verhagen C, Bronkhorst EM, et al. Development of the ProPal-COPD tool to identify patients with COPD for proactive palliative care. Int J Chron Obstruct Pulmon Dis. 2017;12:2121–2128. doi:10.2147/COPD.S140037
45. Pozza M, Navarin N, Sakkalis V, Gabrielli S. Artificial intelligence methods and digital intervention strategies for predicting and managing chronic obstructive pulmonary disease exacerbations: an umbrella review. Healthcare. 2025;13(23):3037. doi:10.3390/healthcare13233037
46. Sanchez-Romero EA, Garcia-Barredo-Restegui T, Martinez-Rolando L, et al. Addressing post-COVID-19 musculoskeletal symptoms through pulmonary rehabilitation with an evidence-based eHealth education tool: preliminary results from a pilot randomized controlled clinical trial. Medicine. 2025;104(10):e41583. doi:10.1097/MD.0000000000041583
47. Adler-Milstein J, Holmgren AJ, Kralovec P, Worzala C, Searcy T, Patel V. Electronic health record adoption in US hospitals: the emergence of a digital “advanced use” divide. J Am Med Inform Assoc. 2017;24(6):1142–1148. doi:10.1093/jamia/ocx080
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Exercise Adherence Prediction Model for Patients with COPD: A Prospective Cohort Study

Ricke E, Bakker EW
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:385-398
Published Date: 22 March 2023
Factors Associated with Non-Adherence to Self-Management Among Patients with Chronic Obstructive Pulmonary Disease: A Survey Using the Delphi Technique and Analytic Hierarchy Process
Choi JY, Ryu EJ
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1247-1259
Published Date: 4 June 2024
A Bibliometric and Visual Analysis of Oliceridine Research (2013–2024)
Song C, Huang X, Chen N, Song Q, Qiu Y
Drug Design, Development and Therapy 2025, 19:1305-1321
Published Date: 24 February 2025
The Cost-Effectiveness of a Personalised Early Warning Decision Support System (The COPDPredict™ System) to Predict and Prevent Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Hall JA, Turner AM, Gkini E, Mehta R, Spiteri M, Patel N, Jowett S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1693-1710
Published Date: 25 May 2025
From Weight Loss to Standardized Sarcopenia Assessment: A Multi-Database Bibliometric Study of COPD with Sarcopenia (2005–2025)
Fang H, Zhao Y, Wang J, Wu H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:605351
Published Date: 14 May 2026