")
Back to Journals » Journal of Pain Research » Volume 16
Global Status and Future Trends of Fascia and Pain Research in 2013–2022: Bibliometric Analysis Based on CiteSpace and VOSviewer
Authors Du Y , Cai X , Xu B , Wu Y , Chen M , Wang J , Yuan B , Zhang W, Zhu J, Yang C
Received 12 March 2023
Accepted for publication 19 July 2023
Published 28 July 2023 Volume 2023:16 Pages 2633—2653
DOI https://doi.org/10.2147/JPR.S412161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Natalie Strand
Yikuan Du,1,* Xiaolin Cai,2,3,* Bijun Xu,2,3 Yuqing Wu,2,3 Mianhai Chen,2,3 Jinjin Wang,2,3 Bing Yuan,2,3 Weichui Zhang,2,3 Jinfeng Zhu,2,3 Chun Yang2,3
1Central Laboratory, The Tenth Affiliated Hospital of Southern Medical University, Dongguan, 523059, People’s Republic of China; 2Dongguan Key Laboratory of Chronic Inflammatory Diseases, The First Dongguan Affiliated Hospital, Guangdong Medical University, Dongguan, 523808, People’s Republic of China; 3Dongguan Key Laboratory of Stem Cell and Regenerative Tissue Engineering, Guangdong Medical University, Dongguan, 523808, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chun Yang, Dongguan Key Laboratory of Chronic Inflammatory Diseases, The First Dongguan Affiliated Hospital, Guangdong Medical University, Dongguan, People’s Republic of China, Tel +86 150 1915 9295, Email [email protected]
Background: Fascial pathological pain is the main type of chronic pain in older adults today, and studying the relationship between fascia and pain can help in the clinical search for effective treatments. However, in the face of the vast amount of research findings, there is no systematic assessment of the relationship between fascia and pain in a bibliometric analysis. Therefore, the purpose of this study is to analyze studies on fascia and pain using CiteSpace and VOSviewer to identify research hotspots and future directions.
Materials and Methods: A total of 744 papers related to fascia and pain from 2013 to 2022 were collected from the core collection database of Web of Science, and the authors, countries, institutions, keyword co-occurrence, keyword clustering, and keyword emergence were analyzed by CiteSpace and VOSviewer to construct a knowledge map.
Results: Literature publication has shown an overall upward trend over the past decade, but there have been some fluctuations. Carmelo Pirri, Caterina Fede, and Raffaele De Caro are the top three authors with the most articles. The United States, China, and Spain are major contributors to fascial and pain research. The University of Padua, Universidad Complutense and Harvard Medical School are leading institutions in this field. However, it is noteworthy that the collaboration between authors, countries and institutions is not active. Keyword analysis showed that hot spots and trends in research on fascia and pain focused on hot diseases, major interventions, and mechanism exploration.
Conclusion: This analysis identifies the most influential authors, institutions, and countries in the field of fascial and pain research and provides a reference for assessing their academic impact. The analysis of keywords and co-cited literature is useful for analyzing research hotspots and their evolution, as well as for predicting future trends.
Keywords: fascia, pain, bibliometrics analysis, knowledge graph, research progress
Introduction
Fascia has traditionally been thought of as a simple structure that encircles muscles and organs.1 However, as research continues, it has been discovered that fascia is found throughout the body and has the potential to influence the whole body. This is reflected in the fascia’s ability to support and shape,2 coordinate body movements and maintain biomechanical balance,3 maintain internal environmental homeostasis,4 receive and transmit signals and respond to stimulation accordingly,5 promote wound repair and regeneration,6 and regulate the aging process7 and so on. In addition, studies have shown that fascia is also closely associated with lymphoedema, gastrointestinal symptoms, and cancer processes.8,9 With the development of traditional Chinese medicine culture, the theory of traditional Chinese medicine is gradually understood by modern medicine and plays an important role. The two-system theory (Fasciology) proposed by Professor Yuan et al10 explains the biological basis and treatment mechanism of traditional Chinese medicine therapy and provides a medical-biological basis for the realization of modern Chinese medicine meridian research. At the same time, it also provides a new way for the mechanism research of clinically difficult diseases such as tumors. It is evident that the in-depth study of fascia is of great significance.
Recent studies have shown that there is a close relationship between fascia and pain. According to epidemiological surveys, fascial pathological pain accounts for 85% of pain in outpatient visits, and 95% of chronic pain patients in the elderly and sports population are related to this.11 Fascial aging is an important cause of chronic pain. The patient’s pain site has also been found clinically to have thickened fascial thickness, increased density, altered fibrous composition, and reduced gliding ability at the site of pain and other phenomena.12,13 These changes may be associated with stress changes in fibroblasts14 and a decrease in hyaluronic acid secretion by fascial cells,15 and the presence of injury receptors in the fascia may be a source of local pain and referred pain.16 These findings suggest that the role of fascia in pain cannot be underestimated. However, the exact relationship between fascia and pain and how it intervenes is not clear and further research is needed.
In the current era of information explosion, it has become a challenge for researchers to obtain valid information from the vast amount of research findings. Bibliometrics is a quantitative method that helps researchers quickly grasp the dynamics and progress of a discipline or research area by visually analyzing relevant literature using correlation analysis software.17 CiteSpace and VOSviewer are currently recognized as professional software for mapping knowledge domains. To our knowledge, no researcher has yet conducted a bibliometric analysis of the field of fascia and pain. To fill this gap, this study uses CiteSpace 6.1.R6 software and VOSviewer 1.6.18 to analyze the English literature related to fascia and pain research in the past ten years, and draw a network map of authors, countries, institutions, and keywords to interpret the hotspots of pain and fascia related research and speculate the frontier direction to provide a reference for future scholars in this field to carry out relevant research.
Data and Methods
Data Source
The Web of Science Core Collection (WoSCC), the world’s leading database of scholarly information, has been following strict selection criteria for many years to select the world’s most influential and high-quality journals, and is the most commonly used database for bibliometric analysis. Similar studies in the past have also demonstrated the scientific validity of bibliometric analyses based solely on the WoSCC database.18,19 Therefore, we selected the WoSCC database and used an advanced search strategy for the literature collection. After several pre-searches, we identified the search formula as ((TS= (fascia)) OR TS= (connective tissue)) AND TS= (pain). The search time period was from 1 January 2013 to 31 December 2022 and the literature types were Article and Review.
Inclusion Criteria
All studies with titles, abstracts and keywords related to the search subject terms were included, WoSCC language was limited to English, and the type of study was not restricted.
Exclusion Criteria
(1) The subject of the article is “fascia” and the type of disease is not related to “pain”. (2) Only “pain” is covered, not “fascia” related content. (3) The types of literature are news stories, contracted information and newspaper articles, dissertations and conference papers. (4) The literature is duplicated.
Data Analysis
In this study, VOSviewer (https://www.vosviewer.com/, version 1.6.18), CiteSpace (http://cluster.cis.drexel.edu/~cchen/citespace/, version 6.1.R6) and Excel Office 2019 were used for bibliometric analysis and data visualization. First of all, we will export the documents retrieved from WoSCC as a complete record in plain text and name it download_.txt. Then import the data into NoteExpress (version 3.5.0) for data cleaning and screening. Two researchers independently screened the search results to exclude irrelevant, repetitive and inconsistent articles, and the documents with differences were resolved by consultation with the third researcher, resulting in 744 documents being included. Then these data are imported into VOSviewer and CiteSpace for bibliometric and visual analysis. VOSviewer is used to analyze and draw the co-occurrence map of keywords. CiteSpace is used to analyze the temporal distribution and spatial distribution of documents, analyze the keyword clusters that appear at the same time, capture the keywords with strong citation bursts over time, and determine the research frontiers and emerging trends. Excel is used to analyze the time distribution of documents, and the growth of publications in the following year is estimated by a polynomial model:  .
.
Results
Posting Trend
The search yielded 1841 papers, excluding 1031 not related to the research topic, 17 duplicates, 26 conferences, 12 editorial materials and 11 replies to letters, resulting in 744 papers, including 124 Reviews and 620 Articles (Figure 1). The number of papers published by a discipline in a certain period can not only explain the development speed of this discipline, but also reflect the attention of researchers to this discipline to a certain extent. A statistical analysis of the annual publication volume and publication trends of these 744 articles (Figure 2) shows an overall fluctuating upward trend in the number of articles published from 2013 to 2022. It can be roughly divided into three phases: the first phase, from 2013–2016, shows a slow growth in the number of publications, indicating that at this stage, the relevant theories in the field have not yet been fully validated and the pain field is gradually focusing on the role played by fascia in this. The second phase is from 2017–2019, during which the number of publications decreases, indicating that the field may have hit a bottleneck during this period and new insights are needed to seek new breakthroughs. The third phase, from 2020 to the present, shows a rapid increase in the number of articles published in this phase, which indicates that more and more scholars are focusing on this area and conducting research, resulting in more research findings. The above results suggest that research on the relationship between fascia and pain has become a hot topic and is entering a phase of rapid development.
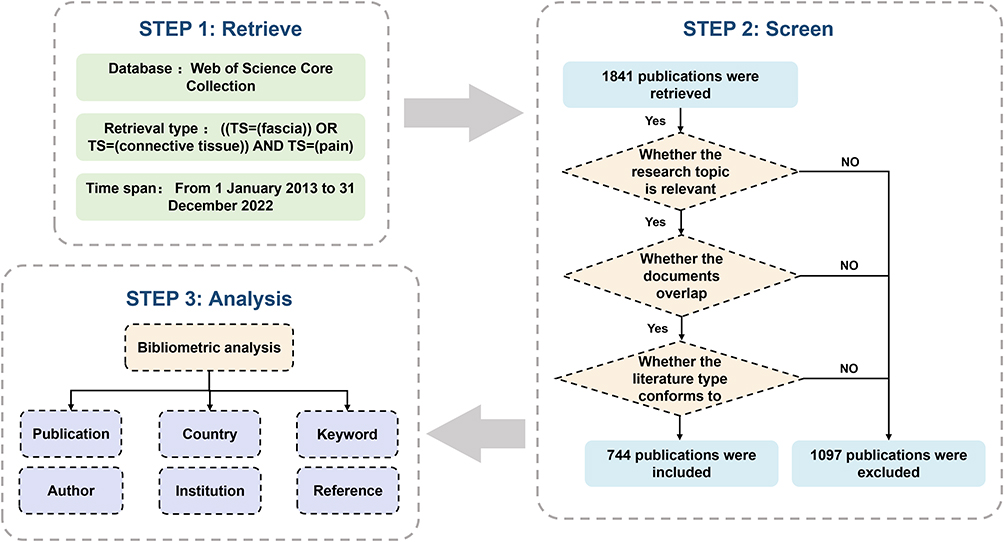 |
Figure 1 Literature screening process. |
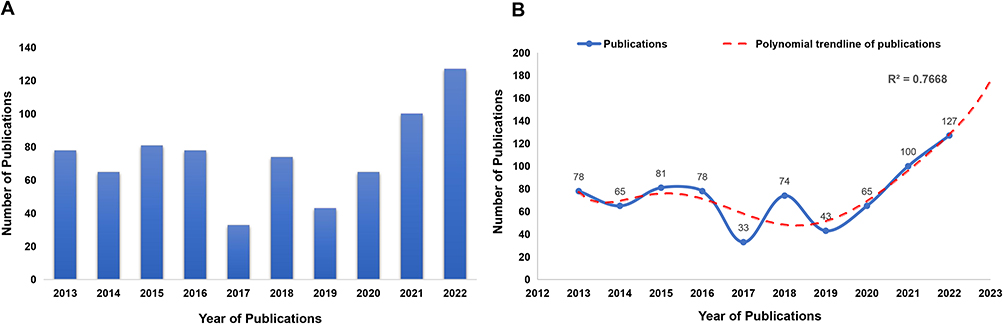 |
Figure 2 (A) Annual number of publications from 2013 to 2022. (B) Polynomial curve fitting for publication growth. |

Distribution of Authors
A total of 3386 authors participated in the research on fascia and pain. Carla Stecco (16 articles, H-index 35), followed by Carmelo Pirri (10 articles, H-index 12), Caterina Fede (9 articles, H-index 17), Raffaele De Caro (8 articles, H-index 40), Wolnei Caumo (8 articles, H-index 35) and Felipe Fregni (8 articles, H-index 94) published the most articles as shown in Table 1. CiteSpace 6.1.R6 software is used to visually analyze the Author collaboration network (Figure 3). The node is “author” and the size of the node is directly proportional to the number of articles published by the author. The collaboration and closeness between different authors are represented by the connecting line and the thickness between the nodes. The graph shows the number of author nodes is 335, the line of communication between authors is 339 and the density is 0.0061. Several author sub-network structures have been formed in the atlas, with three groups working more closely together: first, the network structure formed by Carla Stecco, Caterina Fede, Carmelo Pirri, Raffaele De Caro and others; second, the network structure formed by Wolnel Laumo, Fellpe Fregni, Iraci L S Torres, Allcia Deltos and others form the network structure; third, Daniel Lopez-lopez, Cesar Calvo-lobo, Ricardo Becerro-de-bengoa-vallejo and others form the network structure. These three network structures are densely connected in the visual knowledge map, reflecting the close collaboration of the groups they form, but the groups are not yet collaborating to form a more stable network system. Secondly, there are many individual researchers, such as Mark Driscoll, who has a high volume of dispersed publications. The above results show that there is still a lot of room for research in the field of fascia and pain, and that the awareness of communication and cooperation between researchers and academic exchange needs to be strengthened.
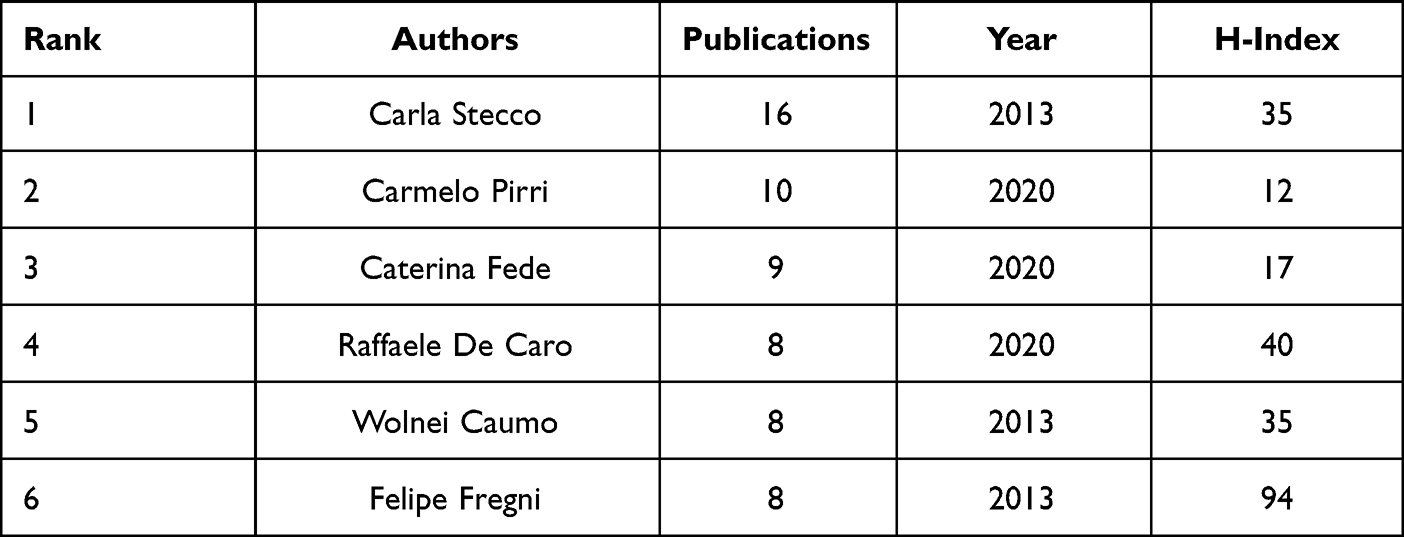 |
Table 1 Top 6 Authors from 2013 to 2022 According to the Publications Related to Fascia and Pain |
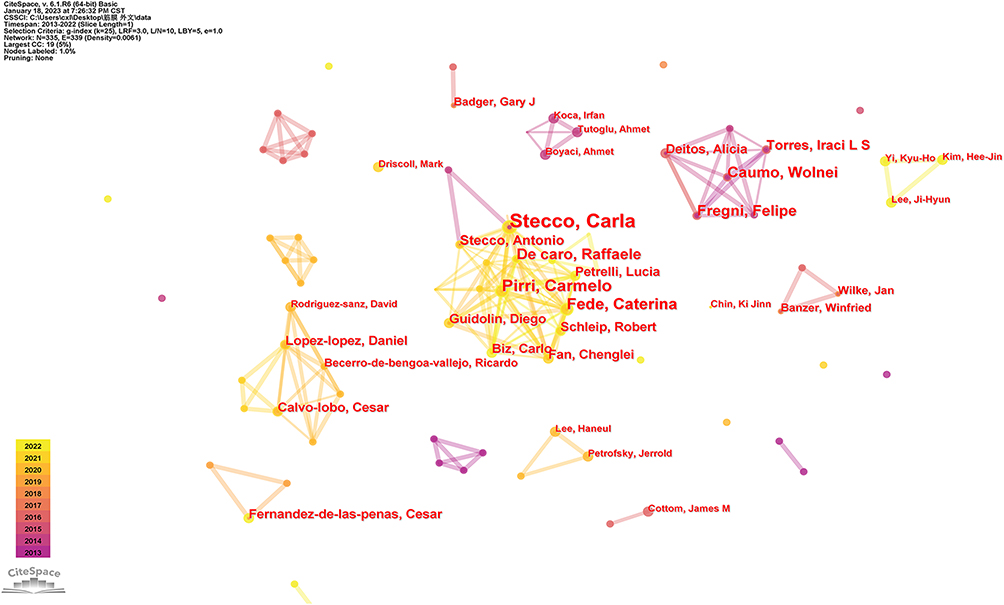 |
Figure 3 Co-occurrence network of authors in the field of fascia and pain. Notes: The size of nodes represents the number of papers published by authors, and the connection between nodes reflects the strength of cooperative relationship. |
Distribution of Countries and Institutions
From 2013 to 2022, 2259 institutions in 240 countries or regions published articles in the field of fascia and pain (Figure 4). As shown in Table 2, the top three countries with the most articles are the United States (186 articles, 25%, Citations 3743), China (91 articles, 12.23%, Citations 489) and Spain (68 articles, 9.14%, Citations 695). Among these, the centrality of the United States is the highest at 0.53, indicating that the United States also maintains its core position in the field of fascia and pain. In addition, the centrality of Germany (0.16), the UK (0.15) and Canada (0.13) are all greater than 0.1, suggesting that these four countries have close collaborations with other countries and regions. Although China has the second largest number of published documents, its collaborations with other countries are not close. The above results show that the international collaborative environment of fascia in pain research has begun to form, but more forces are still needed to participate in it.
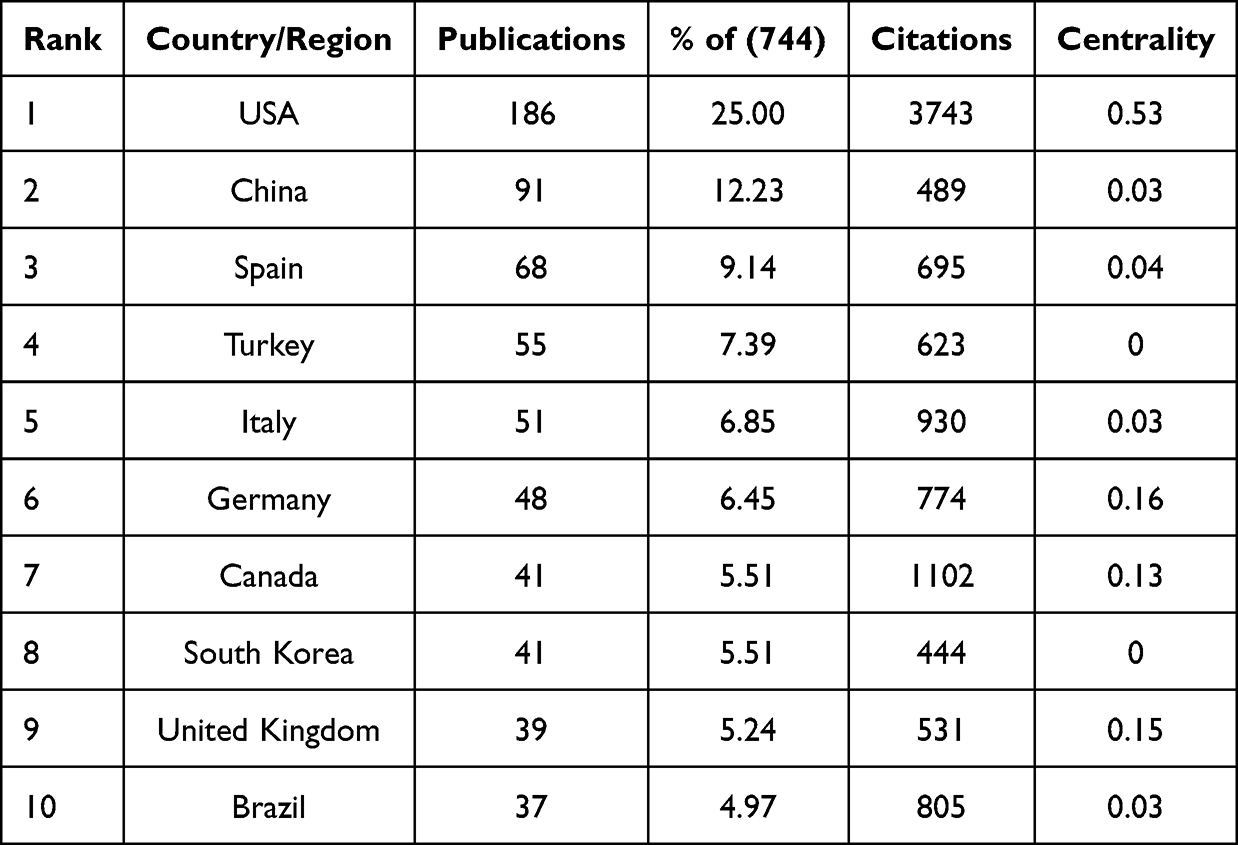 |
Table 2 Top 10 Countries/Regions with the Most Publications from 2013 to 2022 |
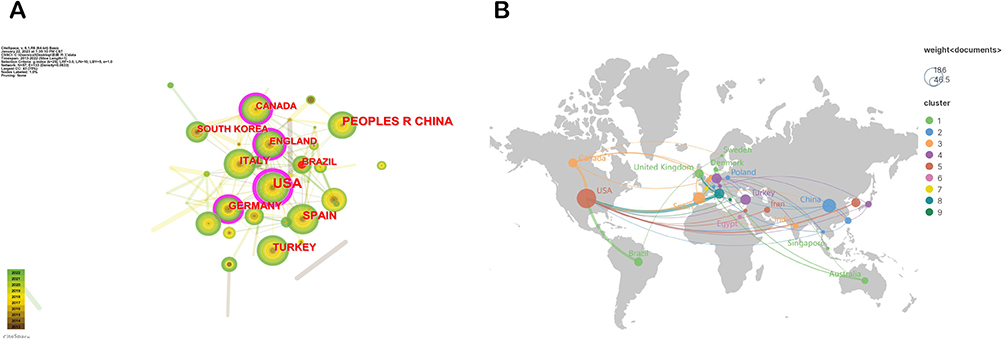 |
Figure 4 (A) Distribution of publications by country/region. (B) A national/regional collaboration map for fascia and pain. Notes: (A) The size of the nodes represents the number of papers published in that region, and the connection between nodes reflects the strength of the collaboration. The region with the purple outer ring represents the high centrality (> 0.1). (B) The closer the connection between countries, the thicker the connection. |
Figure 5 shows the symbiotic network between the 307 institutions with the highest number of papers, with 209 lines of connection and a density of 0.0044. Table 3 lists the top five institutions with the highest number of papers, among which the University of Padua is the first among the core publishing institutions (25 papers, 3.36%), followed by Complutense University of Madrid (14 papers, 1.88%), Harvard Medical School (13 papers, 1.75%), Universidad Rey Juan Carlos (12 papers, 1.61%) and Harvard University (11 papers, 11.61%). The top five institutions are mainly from Italy (n=1), the United States (n=2) and Spain (n=2), which shows that Italy, the United States and Spain have great influence in the field of fascia and pain. However, the centrality of these institutions is low, suggesting that the communication between them is not close.
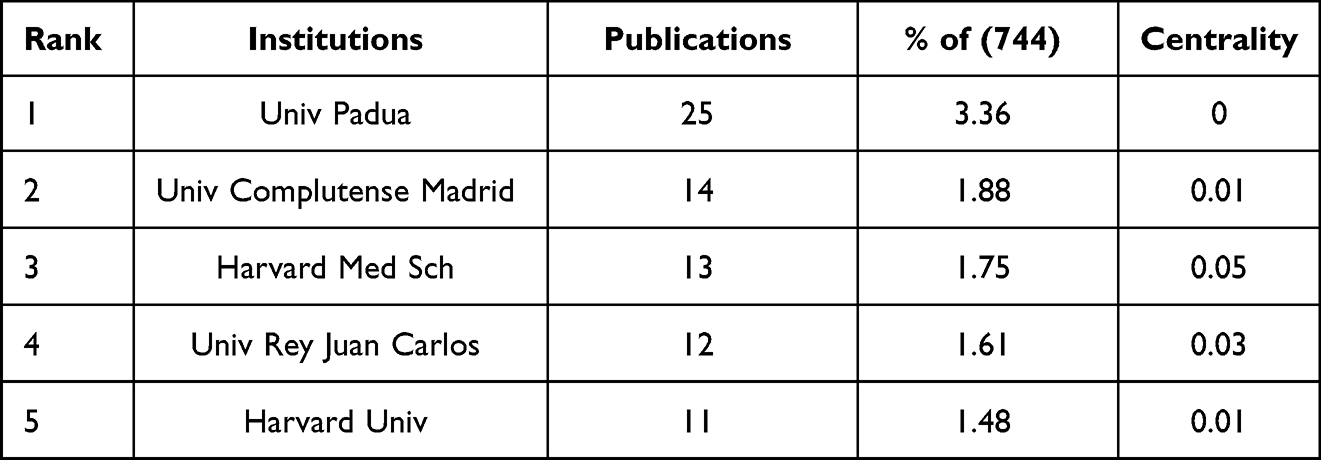 |
Table 3 Top 5 Institutions with the Most Publications from 2013 to 2022 |
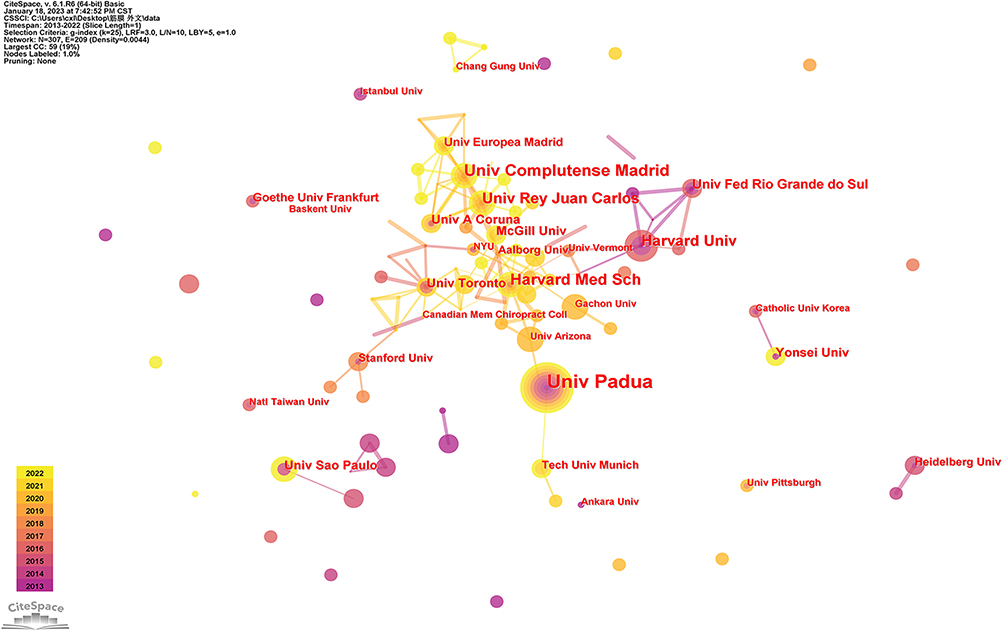 |
Figure 5 Institutional co-occurrence network of documents in the field of fascia and pain. Notes: The size of nodes represents the number of papers published by institutions, and the connection between nodes reflects the strength of cooperative relationship. |
Distribution of Journals
The articles were published in 323 journals. Figure 6 shows 11 journals with 10 articles or more. Impact factor is a common index for periodical evaluation among nations. It is not only an index to measure the usefulness and display of periodicals, but also an important index to measure the academic level of periodicals and even the quality of papers. The Journal Citation Indicator (JCI) is a measure of the average Category Normalized Citation Impact (CNCI) of citable items (articles and reviews) published by a journal over a recent three years, and it is another important index for evaluating periodicals besides Journal Impact Factor (JIF). According to the data, JOURNAL OF FOOT and ANKLE SURGERY (18 articles) published the most articles, followed by MEDICINE (16 articles), Regional Anesthesia and Pain Medicine (13 articles) and Current Pain and Headache Reports (13 articles). Among the top 11 journals, the influence factors and citation index of Regional Anesthesia and Pain Medicine (IF 5.564, JCI 1.91) are the highest, followed by Journal of Clinical Medicine (IF 4.964, JCI 1.02), PAIN MEDICINE (IF 3.637, JCI 1.12), Foot and Ankle International (IF 3.569, JCI 1.1) and American Journal of Physical Medicine and Rehabilitation (IF 3.412, JCI 1.01). The JCI of these journals is greater than 1.0, which shows that these journals are above the average citation level, which suggests that they play an active role in the field of fascia and pain.
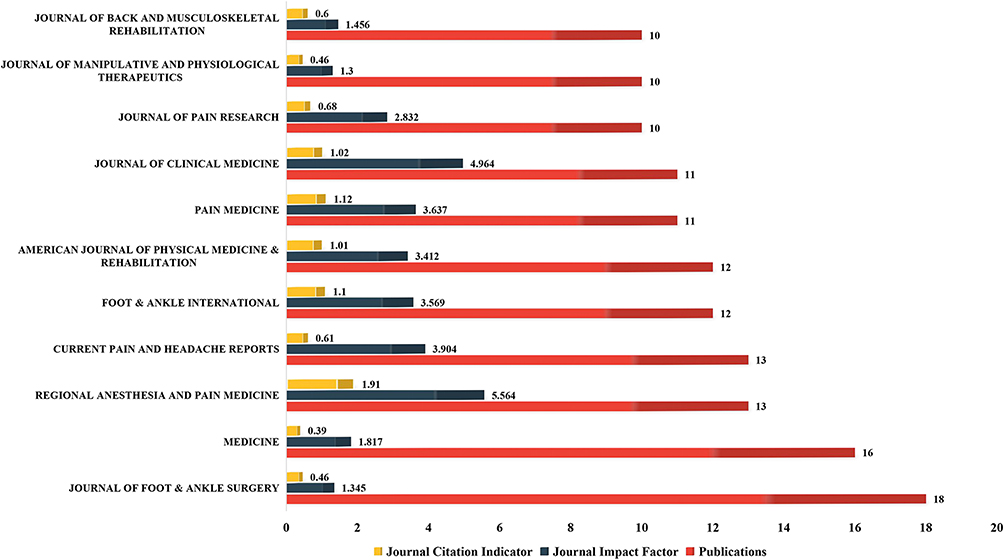 |
Figure 6 Distribution of productive journal publications. |
Keywords
Atlas Co-Occurrence Analysis
Keywords are a highly condensed version of the core content of an article. VOSviewer’s keyword co-occurrence function is based on the literature, from which keywords are extracted and analyzed to find research hotspots in the field. A total of 2920 keywords were extracted by VOSviewer, and keywords with more than 3 occurrences were displayed through the mapping. Based on the average time of occurrence of the keywords, the keywords are presented in a labelled view, as shown in Figure 7. The keywords in blue appear earlier and those in red have appeared in recent years and are recent research hotspots. The keywords are presented in a density view based on the amount of literature in which the keyword appears, as shown in Figure 8. The closer the color is to red, the greater the volume of literature. Table 4 lists the top 10 keywords in terms of centrality, with pain (0.16), low back pain (0.11) and acupuncture (0.10) all having good centrality (> 0.1).
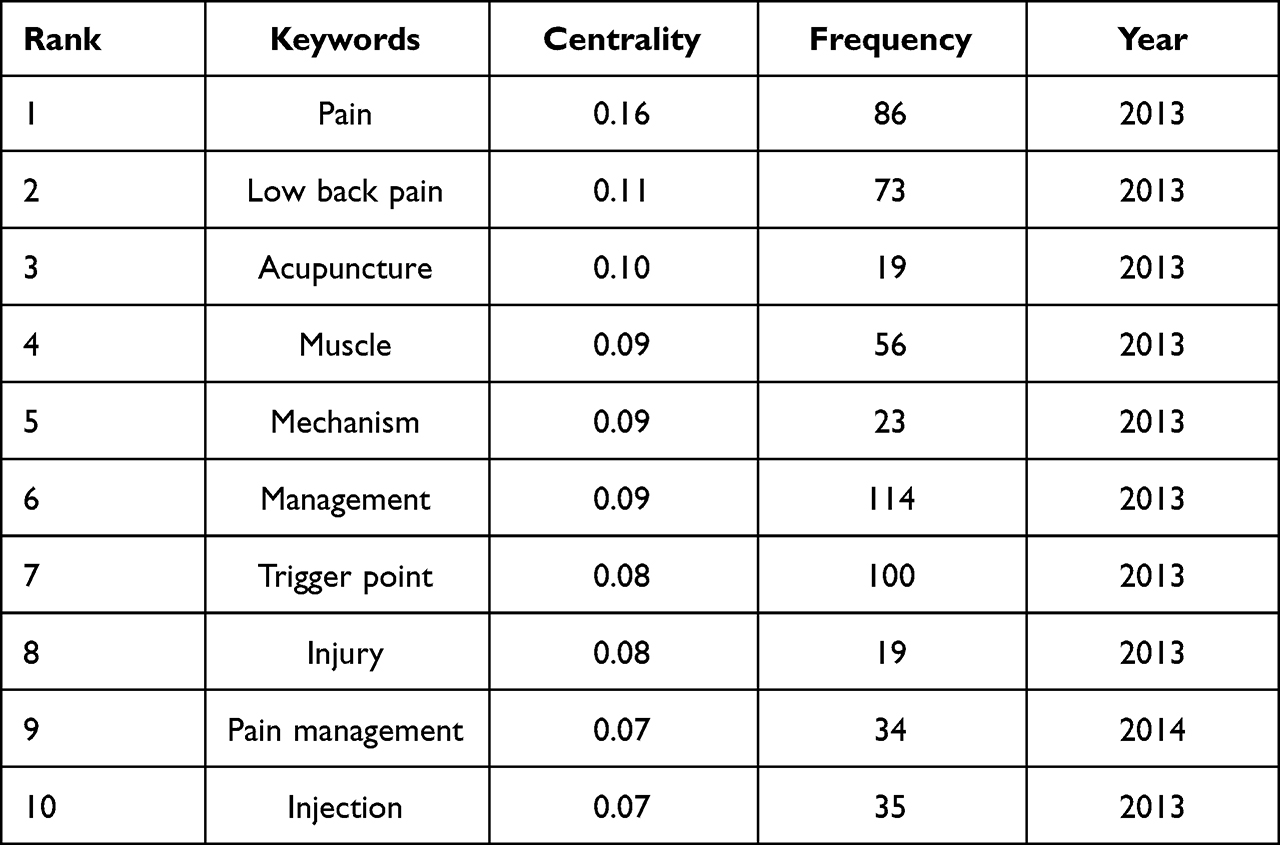 |
Table 4 Top 10 Keywords with High Centrality |
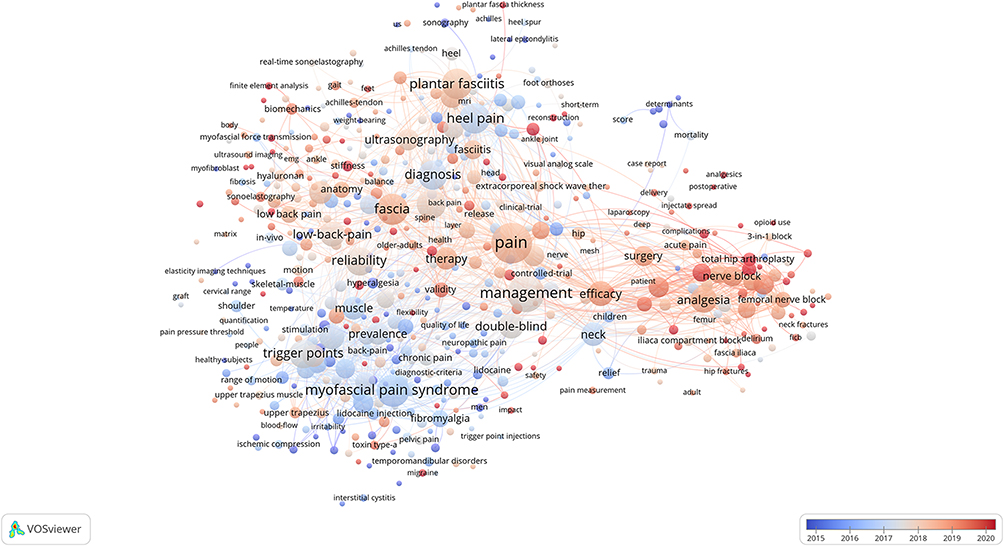 |
Figure 7 Keyword label view. Notes: The color bars represent time, with blue appearing after and red appearing before. |
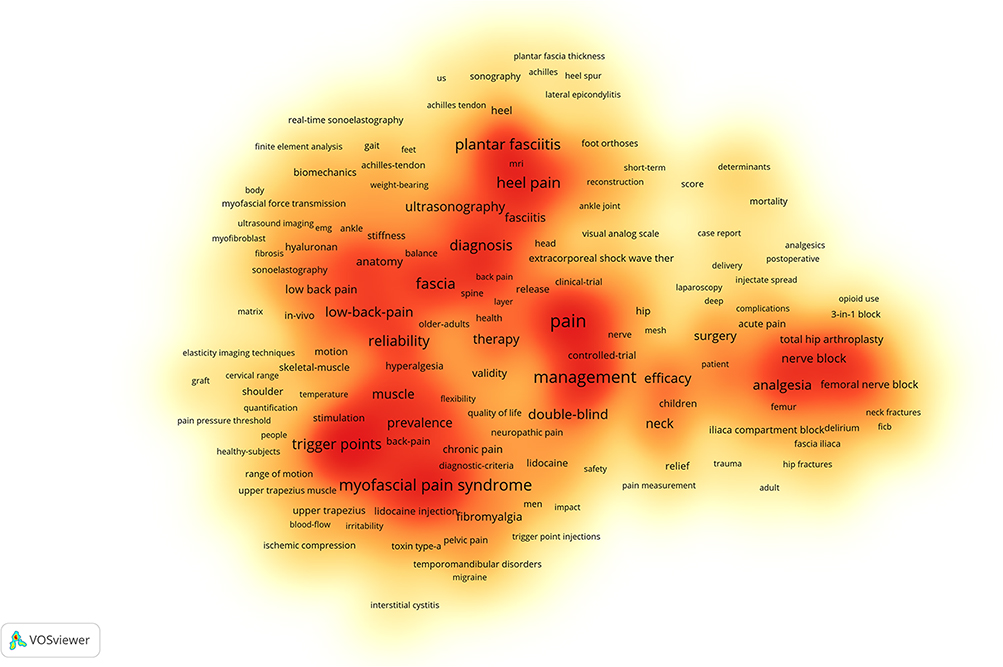 |
Figure 8 Density view of keywords. Notes: The greater the number of items in the neighborhood of a point, the higher the weight of the items in the neighborhood, and the closer the point is to red. |
Keyword Clustering Analysis
We also used CiteSpace to cluster the keywords and obtained 8 clusters. CiteSpace provides two metrics, Modularity (Q value) and Silhouette (S value), based on the clarity of network structure and clustering, which can be used as the basis for us to judge the effectiveness of mapping. In general, the Q value is generally within [0.1), and Q > 0.3 means that the delineated clustering structure is significant. When S > 0.5, the clustering is considered reasonable, while when S > 0.7, it means that the clustering is convincing. As show in Figure 9, the Q value of the keyword map module is 0.4631 and the S value is 0.7805. Among the 8 clusters we obtained, 7 clusters have S > 0.7 and 1 cluster has S > 0.5, which shows that our results are convincing enough. The eight clusters were then grouped into three categories (Table 5), namely research topics, diseases and treatments. In terms of research objects, #3 suggests that thoracolumbar fascia and connective tissue are the main research objects. In terms of diseases, #0, #2, #4, #5 and #6 suggest that plantar fasciitis, myofascial pain syndrome, chronic pain, fibromyalgia and prostatitis are the main research contents. In terms of treatment, the main keywords contained in #1 suggest that the use of fascia iliaca compartment block in analgesia has been widely addressed. The keywords in #7 suggest that surgery is the main treatment for fasciitis necrosis and diabetic foot.
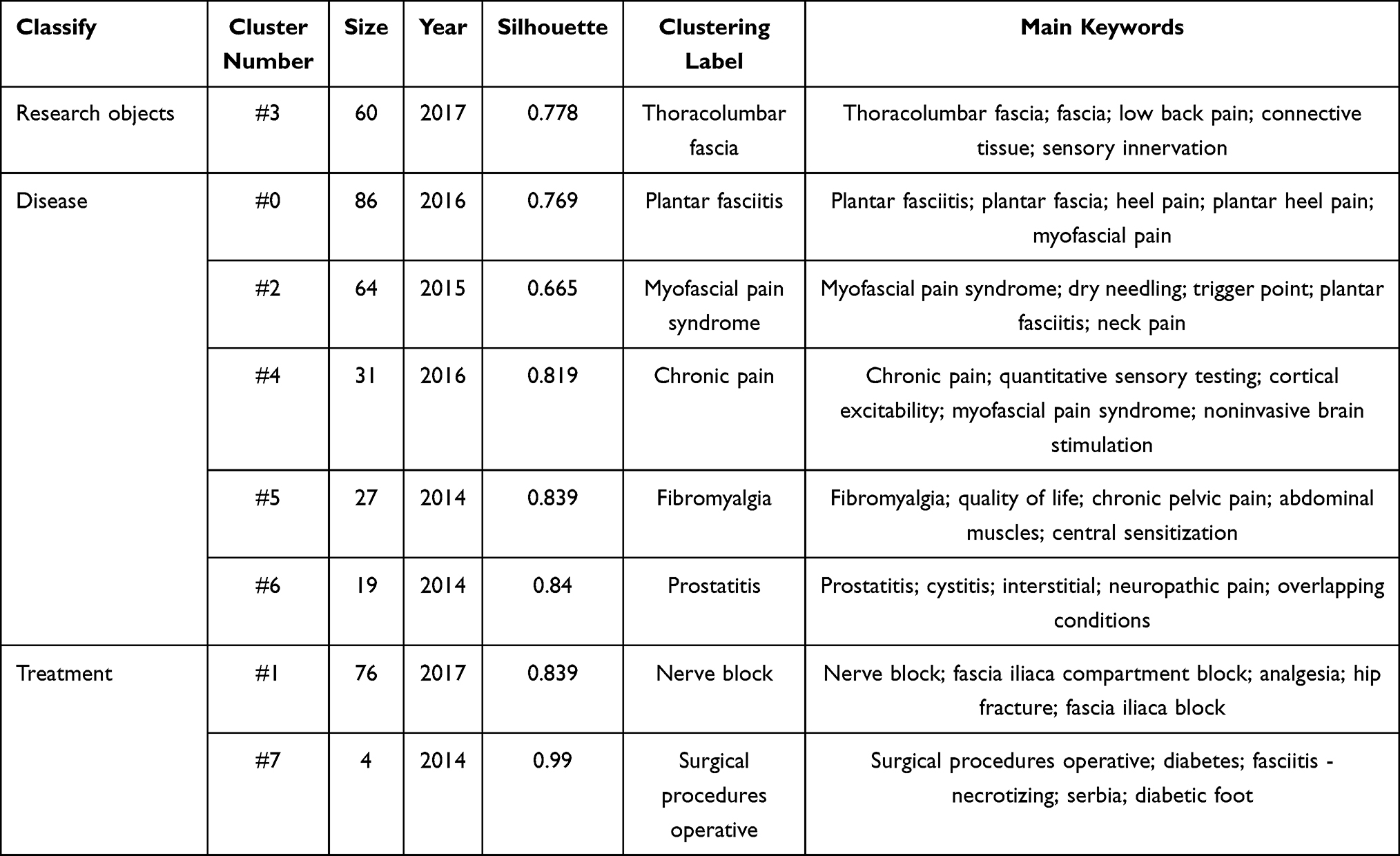 |
Table 5 Keyword Clustering for Fascia and Pain |
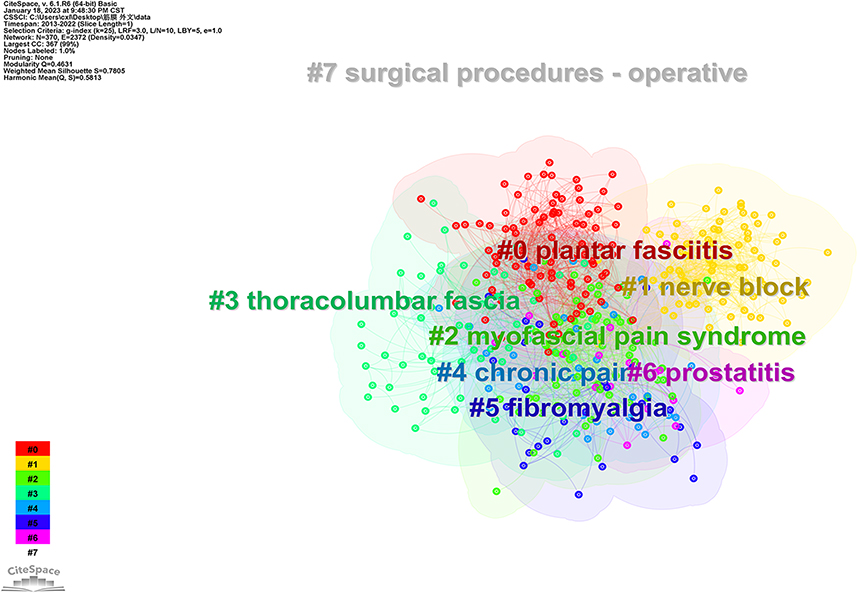 |
Figure 9 Visualization of the keyword clustering analysis. Note: The same color represents a category. |
Keyword Emergence
Burst detection is used to detect the rise or fall of a subject term or keyword and can reveal the most active areas and emerging trends on the web. To further explore the research hotspots and frontiers of fascia and pain, we use the burst detection algorithm to analyze the keywords (Figure 10). It can be broadly divided into two phases. The first phase, from 2013 to 2016, focused on clinically relevant fascia-related pain conditions, including myofascial pain syndrome, back pain, musculoskeletal pain, myo-abdominal pain syndrome and referred pain. The research methodology consists mainly of randomized controlled trials. Mechanistic studies include sensory innervation and nociceptive hyperalgesia. The second phase is from 2017 to the present, where the use of fascial tissues in analgesia has been identified, including femoral nerve blocks, regional anesthesia, postoperative analgesia and pain management, and the methods of study are mainly Meta-analysis.
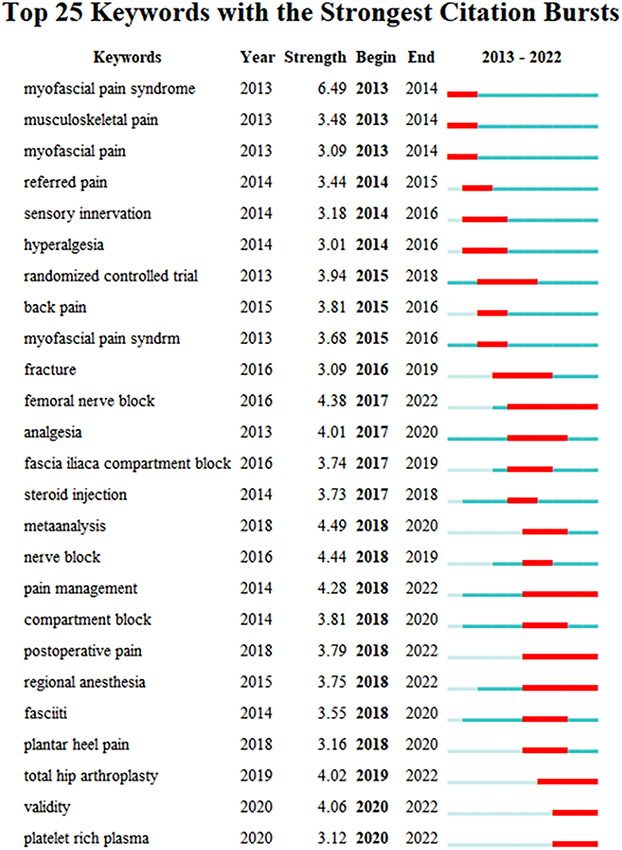 |
Figure 10 Quote the top 25 keywords with the strongest outbreak. Notes: The year indicates the time when the keyword first appeared. Intensity describes the degree of the cited variation. The start and end indicate the start and end times of each burst. The red bar indicates the time when keywords frequently appear, and the blue bar indicates the time when keywords rarely appear. |
Related Areas of Analysis
The results of the double map overlay of journals (Figure 11) show the location of research on fascia and pain in relation to the main research disciplines. The map is divided into two sections, on the left are the downloaded references, and on the right are the quoted references. The curves between them indicate their connections, and these connected trajectories provide an understanding of the interdisciplinary relationships in the field. The Z-Sores function highlights the stronger, smoother trajectories, with higher scores indicated by thicker connecting lines. The results show that publications in medicine, medical, clinical are significantly influenced by health, nursing, medicine (z=3.18, f=2324) and sports, rehabilitation, sport (z=2.48, f=1868). Publications in neurology, sports, ophthalmology were significantly influenced by sports, rehabilitation, sport (z=5.53, f=3854), health, nursing, medicine (z=2.96, f=2176) and psychology, education, social work (z=1.99, f=1548). In addition, there are curves between other disciplines which, despite their lower scores, undeniably have many different cited references underlying all downloadable references.
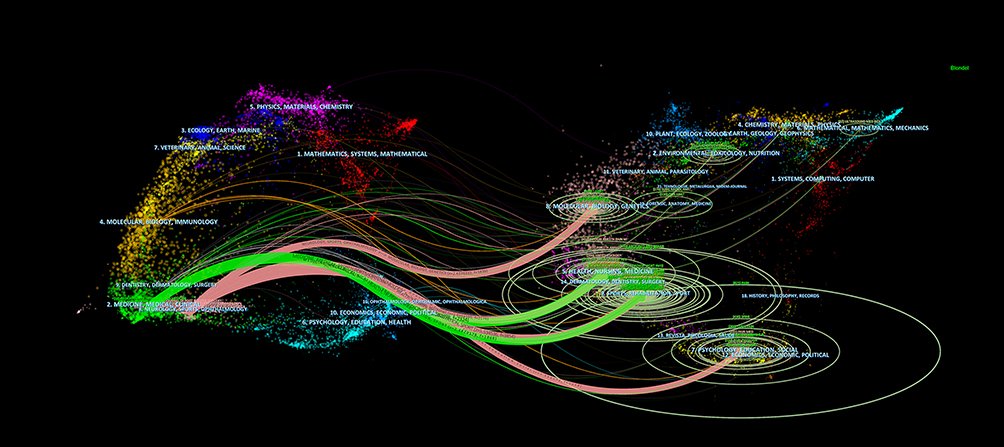 |
Figure 11 Biplot overlay of journals. Notes: The length of the horizontal axis of the ellipse represents the number of authors, the length of the vertical axis of the ellipse indicates the number of published literatures, and the curves are citation curves; the higher the z-Scores function score, the thicker the curve. |
Analysis of Co-Cited Literature
The co-citation analysis provides insight into past fascial and pain research hotspots and predicts future research directions. The top 15 most cited publications are listed in Table 6. The most cited of these is by Desmet,20 published in Reg Anesth Pain Meds in 2017, with 22 citations in this dataset and a total of 82 citations in Web of Science. The next most cited article is by Tesarz,21 published in Neuroscience in 2011, with 19 citations in this dataset and a total of 146 citations in Web of Science. The third highest ranked article was published by Mense in Eur J Transl Myol in 2019,22 with 17 citations in this dataset and 43 total citations in Web of Science. In addition, we paid particular attention to literature with citation bursts; finding the references with the strongest citation bursts may help researchers identify popular topics that are suddenly becoming increasingly popular in a particular field and changes in research direction. The results show (Figure 12) that the early outbreaks were stronger in Sikdar in Arch Phys Med Rehabil 200923 and Tesarz in Neuroscience 2011,21 with outbreak intensities of 6 and 5.31 respectively. Mense in Eur J Transl Myol in 201922 with an outbreak intensity of 6.85 and an outbreak that started in 2021 and continues today.
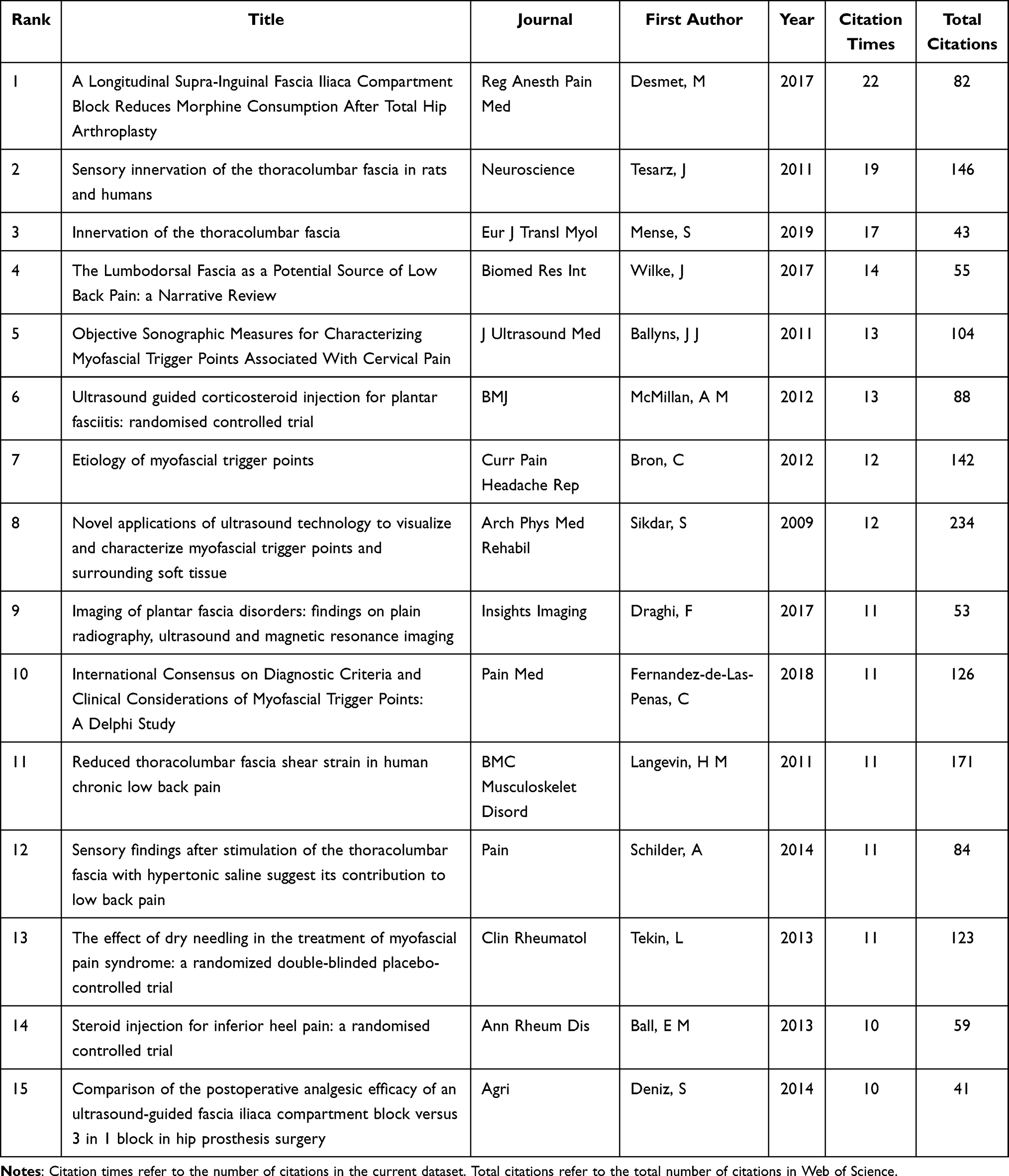 |
Table 6 The Top 15 Most Cited Publications |
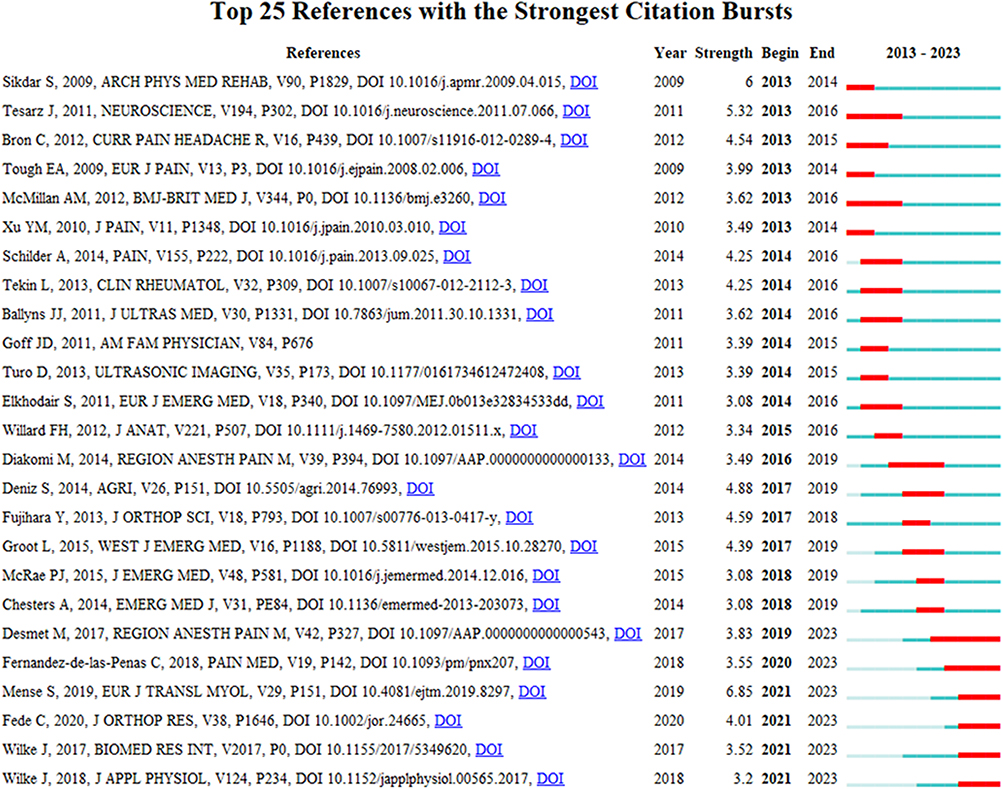 |
Figure 12 The top 25 references with the strongest citation bursts. Notes: The year indicates when the citation first appeared. Intensity describes the degree of variation in citations made. Start and end indicate when each burst began and ended. |
Discussion
Basic Information
This study used CiteSpace and VOSviewer to analyze the literature on fascia and pain in the WOS database core collection from January 1, 2013, to December 31, 2022. The visualization of the knowledge map intuitively reflects the publication trend of literature in the field of fascia and pain, the cooperation network of main research countries/regions and institutions, the main research content, and the research frontier hotspots to provide a reference for the further research of fascia in the field of pain.
The trend of literature published over the last decade shows a general increase in the amount of literature on fascia in pain, particularly in the last three years, indicating that this area is being actively researched. The United States, China, and Spain contributed the most. Half of the top ten countries with the most published articles are from Europe, which means that European countries have a positive academic influence on fascial and pain research. Among the national cooperation networks, the United States, Germany, the United Kingdom, Canada, and other countries have extensive national cooperation networks, among which the United States has the highest centrality and plays a bridge role in the cooperation between various countries. The above results indicate that the international cooperation environment of fascia in pain research has initially formed, but more forces are still needed to participate in it. The analysis of institutions showed that the top 10 institutions by volume of publications were from many countries, but the collaboration between institutions was not close. This phenomenon is also reflected in the co-occurrence map of author cooperation. Three main network structures have been formed, represented by Carla Stecco, Wolnel Laumo, and Daniel Lopez-lopez, but there is no cooperation among these groups. Establishing high-quality academic exchange relations between institutions of different countries and promoting the friendly collaboration of researchers from other countries are conducive to the emergence of high-quality research results. Therefore, encouraging national researchers to establish collaborative partnerships with global institutions to enhance their literary influence further is a crucial move to expand research outcomes.
Research Frontiers and Hotspots
Global research trends in fascia and pain can be explored by analyzing keyword bursts, reference bursts, and timelines. We found that myofascial pain syndrome, nerve blocks, ultrasound, and treatment in keyword bursts appeared late and continued to increase attention, which was at the forefront of current research.
Fascia has the continuity of non-adjacent areas that envelop the human body’s viscera, muscles, etc., forming a three-dimensional system.24 Nowadays, the medical community is looking at fascia with a new perspective. The functional characteristics of the fascia are mainly reflected in the following aspects. (1) Support and shaping: the capsule, ligament, septum, and intermembrane formed by fascia play a mechanical role, such as fixing the position of organs and maintaining their morphology,25 and it can limit the spread of diseases on different fascial planes.26 (2) The generation and conduction of force: the fascial structure essentially gives its ability to transmit the produced power. The latter is a transporter of the created tension and stores mechanical energy in order to save myoelectric energy.27 This function is determined to a large extent by fibroblasts.4,28 (3) Maintenance of internal environmental homeostasis: the rich capillaries in the fascia provide the necessary nutrients for the metabolism of various organ cells.27 The fibroblasts contained in it can maintain the homeostasis of the internal environment by regulating the pressure and flow of fluid penetrating the fascia and releasing growth factors.6 (4) Information communication: sensory neurons, special receptors, and microparticle receptors contained in the fascia can play an essential role in the reception and transmission of information.5,12 In addition, studies have found that it regulates emotions29 and forms memory.30 (5) Repair and regeneration: the collective migration of the fascial fibroblasts and the mobilization of the fascial matrix play a crucial role in wound repair and resurrection.6 (6) Life span: the aging process of the human body is a process of gradual depletion of stem cell reserve in the fascia.10 Therefore, maintaining the fascia’s normal state and differentiation of stem cells is critical to prolonging life. It can be seen that the balance of the fascial system plays an essential role in all aspects of the body.
Recent studies have found a close relationship between fascia and pain. Clinical data show that the pain nerve content of lumbar fascia in patients with low back pain is several times higher than that of ordinary people,31 and ultrasound shows that pain is related to increased fascia thickness and decreased shear force.32 This may be related to fascial aging caused by reduced secretion of fascial cells, such as fibroblasts, fibroblasts and telangiectasia, leading to fascial adhesions.33 In addition, fascia contains many hormone receptors and nociceptors, which also play an essential role in the reception and transmission of pain signals and the corresponding response to stimuli.34 Myofascial pain syndrome (MPS) is a chronic pain syndrome with complex etiology and mechanism accompanied by neurological dysfunction. It is often believed that MPS pain occurs in any part between muscle and motor endplate.35 People overuse these areas in their lives, causing them to be in a state of stress, and pain ensues.36 The fascia is the material basis for MPS to produce pain, and the commonly used treatment methods are mostly acting on the fascia.37 Therefore, MPS may define the relationship between fascia and pain, and to explore the more scientific definition of MPS is closely related to the relationship between fascia and pain. The prevalence of MPS in clinic due to pain can reach 30% to 93%,38 and patients and doctors often overlook the importance of MPS as a disease.39 It often leads to poor prognosis, increased treatment costs, ineffective drug treatment, and the risk of addiction when treated with analgesics. Among various treatment methods, ultrasound and traditional Chinese medicine therapy have become an international trend.40 A randomized trial found that ultrasound improved fatigue, anxiety, and enhanced pain in MPS patients compared with usual care.41 Acupuncture is an effective and safe method for treating MPS, and its combination with drug therapy is more effective than single-drug therapy.42 Baduanjin can relieve pain by stretching the fascia and relaxing muscles.43 Pain is the leading cause of life expectancy and quality of life. As promising non-drug treatments, ultrasound, and traditional Chinese medicine therapy can relieve chronic pain caused by MPS. However, more evidence is needed to verify the potential mechanisms and clinical efficacy of its intervention for pain relief in MPS.
Nerve block plays an essential role in the management of surgical analgesia. Imaging studies have shown that the fascial system is involved in pain management through nerve block techniques.44 A prospective, double-blind, randomized, controlled clinical trial has shown that hyaluronic acid is better for nerve blocking than traditional drugs.45 Besides, receptors in the fascia can also change the thickness of the fascia in real time in addition to affecting the analgesic effect of a nerve block,46 and the thickness of the fascia can affect the diffusion of blocking drugs,47 which may be used as a reliable evaluation index of analgesic effect. Clinically, nerve blocks for neuropathic pain,48 surgical pain,49 primary dysmenorrhea,50 and fibromyalgia51 involve the central nervous system. Studies have shown that mechanical force applied to the fascia can affect changes in brain activity, which affects the dissociation or interaction between the anterior cingulate cortex and the S1 brain area.52 Or the activated orbitofrontal cortex, superior temporal sulcus, and somatosensory cortex to achieve the effect of pain relief.53 Therefore, in using nerve block analgesia, we should consider the collocation of drugs and be supplemented by fascial intervention.
In summary, the research hotspots and trends of fascia and pain mainly focus on hot diseases, primary interventions, and mechanism exploration. This study summarizes current research hotspots, trends, and ways to improve the quality of research to provide valuable insights for researchers interested in investigating fascial effects on pain.
Knowledge Base
Highly co-cited references can be considered domain-specific knowledge bases; references with intense citation bursts can also characterize the research foundation of a field.54 Through co-citation analysis of references, this study found some influential fascial and pain studies with high co-citation counts and intense citation bursts published between 2013 and 2022. We found that the top 15 commonly cited reference studies can be grouped into three periods: (1) Early (2009–2013) studies focused on the pathophysiology of fascial pain such as myofascitis, quantifying painful fascia, and effective ways of analgesia. (2) The mid-term (2014–2018) improved the fascia theory and further broadened the diagnosis of fascial pain-related diseases. (3) In the later period (2019-present), with the increasing rise of traditional Chinese medicine therapy, the related research in the past three years mainly focused on the clinical and mechanism research of traditional Chinese medicine therapy such as meridian sinew, moxibustion and plantar pressure. These studies have well explained how the fascia, as the material basis of pain, interacts with pain and what kind of external intervention can reverse pain. These results provide a research reference for the readers and help locate the development status and hotspots in fascial pain research.
Previous studies have revealed that the fascia can adapt to various states by reversibly changing biomechanical and physical properties.55 When the tendon mold is excessively tightened or in a stress state, pain will follow. The mechanism of fascial pain is closely related to the characteristics of the fascia itself, including the innervation of the fascia, the density of the fascia itself, and the sliding between the fascia and the muscle, which all affect the occurrence and development of pain. In a high-cited review, the new direction of fascia biology and its various hypotheses in myofascial pain syndrome were summarized. For the first time, the important position of fascia in myofascial syndrome was systematically demonstrated.56 Another highly cited review details the multiple possible causes of myofascial trigger points, which play an important role in myofascial syndrome. It suggests that this research stage supports the development of myofascial pain trigger points after muscle overuse. However, whether the overuse of mechanical devices is a key trigger or a persistent noxious input remains controversial and requires further study.57 In a clinical observational study, intensive sensory innervation in the thoracolumbar fascia, including nociceptive fibers, was described, indicating that it may play an important role in low back pain. Two other highly cited literature studies have also increased the reliability of the thoracolumbar fascia as a source of low back pain.58,59 Its most sensitive properties to chemical stimuli make it a major candidate for non-specific low back pain rather than local pressure hyperalgesia.58 The comparison between the inflamed and intact fascia showed that the calcitonin gene-related peptide and substance P-positive fibers in the inflamed thoracolumbar fascia were relatively increased, which caused pain.22 With the in-depth study of fascia and pain, it has been found that some common pain-related diseases such as low back pain, postpartum pain, and plantar fascia pain are closely related to fascia. Therefore, it is particularly important to accurately identify and diagnose the fascia under pathological conditions. Imaging examination is mainly used to evaluate the morphology of the fascia. Ultrasound technique was used to quantify the myofascial trigger point and measure the shear strain of the fascia. When the ultrasound showed that the fascia became fibrosis, densification, thickness thickening, stiffness increased, shear strain decreased, and focal nodules and abnormal blood flow in the fascia, it was suggested that the fascia was in a pathological state.12,23,60,61 In the diagnosis of fascial pain, Fernández-de-Las-Peñas et al improved the basic diagnostic criteria of trigger point (TrP) and provided two directions for future research.62 One is to investigate the magnitude and duration of pressure during TrP examination. Second, it should be investigated whether the presence of referred pain is a basic diagnostic criterion for TrP, whether it is active or latent, to determine whether there are potential neurophysiological and electromyography differences. In order to dig out the gold standard for the diagnosis of myofascial syndrome from TrP as a starting point. At the same time, Draghi F et a. used imaging techniques to explore the plantar fascia in depth, and described the specific lesion signs more accurately.63 Ultrasound and MRI should be used as the first-line and second-line examination methods to evaluate the plantar fascia pain disease, respectively. The important conclusion that X-ray plain film examination can exclude the indirect discovery of plantar fascia pain disease. In the treatment of fascial pain, it involves fascial block, steroid injection, dry needle therapy, ultrasound-guided drug injection, etc. In western medicine, Ball et al proposed a new method of steroid injection for the treatment of fascial pain.64 The effect of dry acupuncture on myofascial syndrome in traditional Chinese medicine is significant. The needle produces mechanical stimulation on myofascial trigger point (MTrP) in order to provide the maximum analgesic effect by piercing the most painful point,65 indicating that acupuncture MTrP is effective in reducing pain. It is worth noting that according to the meridian theory, traditional Chinese medicine has great potential in the treatment of fascial pain. Among them, many highly co-cited literatures have explained the important role of acupuncture myofascial trigger points, involving gate control theory and specificity theory, quality evaluation of randomized controlled trial reports, etc.66,67 In addition, related studies have shown that moxibustion can significantly improve the injury of medial vastus muscle tissue in rats with myofascial pain syndrome and increase the thermal pain threshold. Some of its central mechanisms may be related to the inhibition of microglia activation in the spinal dorsal horn and the reduction of BDNF protein expression.68 At this stage, the research on the sensory function of fascial nerve is more detailed, which provides a neuroanatomical basis for the selectivity and specificity of acupoints in driving specific autonomic nerve pathways.69 It helps clinicians to study further and improve the performance of erector spinae plane block to optimize the analgesic effect and improve the prognosis of postoperative patients.70
In the analysis of the literature on fascia and pain in the past decade, we have discussed that the techniques for quantifying fascia pain are mainly focused on ultrasound or MRI to evaluate fascia thickness and abnormal signals of fascia tissue. Strain elastic ultrasound to evaluate fascia elasticity; Doppler signal to assess whether local fascia congestion.13,71 There are a large number of clinical efficacy observation studies. Still, there are problems, such as a large number of clinical data that cannot be converted into scientific reference data, which limits the development of research on the mechanism of fascia pain to a certain extent. Here we summarize three main reasons for the failure of clinical transformation. (1) The sample size is small, and there is heterogeneity, which may be related to age and weight. (2) The existing research tends to evaluate the difference in the fascia between the control and treatment groups before and after the treatment and lacks systematic review and collection of specific data. (3) Various new technologies have emerged to evaluate the morphological changes of fascia, but the research is still immature and innovative. For example, MRE has been used to examine the mechanical properties of stiffness increase, viscosity change, and strain reduction, as well as the structural characteristics of scar formation, fibrosis, and structural disorder. It can also quantify the degree of adhesion at the functional myofascial interface. New research using T1ρ MR imaging shows that high levels of unbound water, indicating hyaluronan aggregation, may also lead to increased stiffness and reduced fascia mobility.12
In summary, future research should be based on reliable preclinical data to find ways of quantifying pain and establishing uniform standards. This will help ensure that more clinical data can be used for experimental analysis and research and thus help to improve the clinical management of fascial pain.
Advantage and Limitation
This study has the following advantages. The study is the first bibliometric analysis article on the research in the field of fascia and pain. Through the statistics and analysis of relevant literature, it sorts out the current global status and future trends in the field of fascia and pain. The authors, countries and institutions that play a central role in the articles have guiding significance for scholars who want to deepen the exchange and research in this field. The analysis of keywords and co-citation literature summarizes the current research hotspots and frontiers. And the analysis of keyword bursts will provide feasible scientific research ideas or clinical directions for clinical and scientific doctors. Among them, myofascial pain syndrome and nerve block are the representatives of clinical fascia to produce pain and apply fascia to affect body pain. Ultrasound or other methods such as nuclear magnetic resonance can be used to identify and diagnose the pathological state of fascia in anterior myofascial pain syndrome and nerve block, as well as the mechanism between fascia and pain. Whether it is medicine, yoga or acupuncture and moxibustion of traditional Chinese medicine, tai chi, etc. are excellent means of clinical intervention of fascia and are also hot spots in scientific research. Through big data analysis, we integrate time, space and region. Through the analysis and discussion of keywords and frontier hotspots, we explain our understanding of fascia and pain to readers, hoping to give some help to clinical and scientific research.
At the same time, there inevitably existed some limitations in this study. (1) All the articles in this study were obtained from the WoSCC database. Although previous studies have proved that the bibliometric analysis based on the WoSCC database was scientific and practical, it might still be missing. (2) The types of articles included are limited to original articles and reviews published in English, making the analysis somewhat incomplete. (3) Although VOSviewer and CiteSpace were able to provide objective research, there may be some subjective judgment as the previous literature screening was manual.
Conclusion
Fascia is closely associated with the onset and development of pain, as confirmed by imaging techniques such as ultrasound, magnetic resonance imaging, and infrared thermal imaging. Studying the relationship between fascia and pain will provide new insights into the clinical management of pain. This study used bibliometric analysis to provide researchers with a panoramic and holistic view of research in the field of fascia and pain over the last decade. Based on the 744 articles retrieved from WoSCC, the literature volume in this area shows an overall upward trend, but there are some fluctuations. The significant increase in research output over the last three years suggests that the field has opened up new opportunities. At the same time, we identify the authors, countries, and institutions that play a central role and further analyze the research network. The keywords and co-cited articles analysis revealed that researchers have been discussing fascia from different angles. The current research foci in the fascia and pain are the relationship between fascia and hot spots, critical interventions, mechanism research, and quantification of fascial pain.
Abbreviations
WoSCC, Web of Science Core Collection; MPS, Myofascial pain syndrome; MTrP, myofascial trigger point; TrP, trigger point.
Acknowledgments
We are indebted to all the individuals who participated in, or helped with, our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Natural Science Foundation of Guangdong Province (No. 2021A1515011580; 2021B1515140012; 2023A1515010083); Dongguan Science and Technology of Social Development Program (No. 20211800905342); the Administration of Traditional Chinese Medicine of Guangdong Province (No. 20211216); the Medical Scientific Research Foundation of Guangdong Province (No. A2020096; B2021330); the Research and Development Fund of Dongguan People’s Hospital (No. k202005); Guangdong Medical University Students’ Innovation Experiment Project (No. 2021ZZDS006; 2021ZCDS003; 2022ZYDS003; 2022FYDB009; 2022FCDS003); the Guangdong Medical University students’ innovation and entrepreneurship training program (No. GDMU2021003; GDMU2021049; GDMU2022031; GDMU2022047; GDMU2022063; GDMU2022077; GDMU2022078); the Provincial and national college students’ innovation and entrepreneurship training program (No.202110571010; No.S202110571078; No.202210571008; No.S202210571075); Guangdong Medical University-Southern Medical University twinning research team project (No.4SG23033G); the Scientific Research Fund of Guangdong Medical University (No. GDMUZ2020009); and the Cai Limin National Traditional Chinese Medicine Inheritance Studio.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. van der Wal J. The architecture of the connective tissue in the musculoskeletal system-an often overlooked functional parameter as to proprioception in the locomotor apparatus. Int J Ther Massage Bodywork. 2009;2(4):9–23. doi:10.3822/ijtmb.v2i4.62
2. Wilke J, Behringer M. Is “delayed onset muscle soreness” a false friend? The potential implication of the fascial connective tissue in post-exercise discomfort. Int J Mol Sci. 2021;22(17):9482. doi:10.3390/ijms22179482
3. Wilke J, Schleip R, Yucesoy CA, Banzer W. Not merely a protective packing organ? A review of fascia and its force transmission capacity. J Appl Physiol. 2018;124(1):234–244. doi:10.1152/japplphysiol.00565.2017
4. Fede C, Pirri C, Fan C, et al. A closer look at the cellular and molecular components of the deep/muscular fasciae. Int J Mol Sci. 2021;22(3):1411. doi:10.3390/ijms22031411
5. Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. J Anat. 2012;221(6):507–536. doi:10.1111/j.1469-7580.2012.01511.x
6. Jiang D, Rinkevich Y. Furnishing wound repair by the subcutaneous fascia. Int J Mol Sci. 2021;22(16):9006. doi:10.3390/ijms22169006
7. Wilke J, Macchi V, De Caro R, Stecco C. Fascia thickness, aging and flexibility: is there an association? J Anat. 2019;234(1):43–49. doi:10.1111/joa.12902
8. Stecco A, Stern R, Fantoni I, De Caro R, Stecco C. Fascial disorders: implications for treatment. PM R. 2016;8(2):161–168. doi:10.1016/j.pmrj.2015.06.006
9. Mike M, Kano N. Laparoscopic surgery for colon cancer: a review of the fascial composition of the abdominal cavity. Surg Today. 2015;45(2):129–139. doi:10.1007/s00595-014-0857-9
10. Yuan L, Wang J, Wang CL, Shen BL, Dai JX, Huang Y. Fasciology: a new theory on the human self- supervision and control system. Sci Technol Rev. 2006;06:85–89.
11. Yang ZM, Ma LJ, Xu JF, Lin RZ. Clinical application of TCM therapy for pain based on fascia theory. Chin Manipul Rehabil Med. 2022;13(10):61–63. doi:10.19787/j.issn.1008-1879.2022.10.018
12. Langevin HM. Fascia mobility, proprioception, and myofascial pain. Life. 2021;11(7):668. doi:10.3390/life11070668
13. Drake C, Whittaker GA, Kaminski MR, et al. Medical imaging for plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res. 2022;15(1):4. doi:10.1186/s13047-021-00507-2
14. Hendy BA, Fertala J, Nicholson T, et al. Profibrotic behavior of fibroblasts derived from patients that develop posttraumatic shoulder stiffness. Health Sci Rep. 2023;6(2):e1100. doi:10.1002/hsr2.1100
15. Fantoni I, Biz C, Fan C, et al. Fascia lata alterations in hip osteoarthritis: an observational cross-sectional study. Life. 2021;11(11):1136. doi:10.3390/life11111136
16. Cheng LL, Li DJ, Yu YY, Chen ZH. Manipulation treatment of knee osteoarthritis based on the theory of myofascial chain. J Anhui Univ Chin Med. 2022;41(05):8–11.
17. Bai M, Zhang J, Chen D, et al. Insights into research on myocardial ischemia/reperfusion injury from 2012 to 2021: a bibliometric analysis. Eur J Med Res. 2023;28(1):17. doi:10.1186/s40001-022-00967-7
18. Zhang J, Liu H, Che T, Zheng Y, Nan X, Wu Z. Nanomaterials for diabetic wound healing: visualization and bibliometric analysis from 2011 to 2021. Front Endocrinol. 2023;14:1124027. doi:10.3389/fendo.2023.1124027
19. Pan D, Xu L, Shi D, Guo M. Knowledge mapping of mitochondrial calcium uniporter from 2011 to 2022: a bibliometric analysis. Front Physiol. 2023;14:1107328. doi:10.3389/fphys.2023.1107328
20. Desmet M, Vermeylen K, Van Herreweghe I, et al. A longitudinal supra-inguinal fascia iliaca compartment block reduces morphine consumption after total hip arthroplasty. Reg Anesth Pain Med. 2017;42(3):327–333. doi:10.1097/AAP.0000000000000543
21. Tesarz J, Hoheisel U, Wiedenhofer B, Mense S. Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience. 2011;194:302–308. doi:10.1016/j.neuroscience.2011.07.066
22. Mense S. Innervation of the thoracolumbar fascia. Eur J Transl Myol. 2019;29(3):8297. doi:10.4081/ejtm.2019.8297
23. Sikdar S, Shah JP, Gebreab T, et al. Novel applications of ultrasound technology to visualize and characterize myofascial trigger points and surrounding soft tissue. Arch Phys Med Rehabil. 2009;90(11):1829–1838. doi:10.1016/j.apmr.2009.04.015
24. Yang C, Du YK, Wu JB, et al. Fascia and primo vascular system. Evid Based Complement Alternat Med. 2015;2015:303769. doi:10.1155/2015/303769
25. Yuan L, Zhong SZ. Human auto-testing and modulating system——anatomic basis involved in meridianal system. Tianjin J Tradit Chin Med. 2004;05:356–359.
26. Phan T, Lay J, Scali F. The alar fascia and danger space: a modern review. Cureus. 2022;14(12):e32871. doi:10.7759/cureus.32871
27. Bordoni B, Mahabadi N, Varacallo M. Anatomy, Fascia. Treasure Island (FL): StatPearls Publishing; 2022.
28. Bordoni B, Zanier E. Understanding fibroblasts in order to comprehend the osteopathic treatment of the fascia. Evid Based Complement Alternat Med. 2015;2015:860934. doi:10.1155/2015/860934
29. Bordoni B, Marelli F. Emotions in motion: myofascial interoception. Complement Med Res. 2017;24(2):110–113. doi:10.1159/000464149
30. Bordoni B, Simonelli M. The awareness of the fascial system. Cureus. 2018;10(10):e3397. doi:10.7759/cureus.3397
31. Cozacov R, Minerbi A, Haddad M, Vulfsons S. Differential sensitization of muscle versus fascia in individuals with low back pain. Bioengineering. 2022;9(9). doi:10.3390/bioengineering9090440
32. Tamartash H, Bahrpeyma F, Mokhtari DM. Ultrasound evidence of altered lumbar fascia in patients with low back pain. Clin Anat. 2023;36(1):36–41. doi:10.1002/ca.23964
33. Stecco C, Fede C, Macchi V, et al. The fasciacytes: a new cell devoted to fascial gliding regulation. Clin Anat. 2018;31(5):667–676. doi:10.1002/ca.23072
34. Fede C, Albertin G, Petrelli L, et al. Hormone receptor expression in human fascial tissue. Eur J Histochem. 2016;60(4):2710. doi:10.4081/ejh.2016.2710
35. Weller JL, Comeau D, Otis J. Myofascial pain. Semin Neurol. 2018;38(6):640–643. doi:10.1055/s-0038-1673674
36. Annaswamy TM, De Luigi AJ, O’Neill BJ, Keole N, Berbrayer D. Emerging concepts in the treatment of myofascial pain: a review of medications, modalities, and needle-based interventions. PM R. 2011;3(10):940–961. doi:10.1016/j.pmrj.2011.06.013
37. Paoletta M, Moretti A, Liguori S, Toro G, Gimigliano F, Iolascon G. Efficacy and effectiveness of extracorporeal shockwave therapy in patients with myofascial pain or fibromyalgia: a scoping review. Medicina. 2022;58(8):1014. doi:10.3390/medicina58081014
38. Urits I, Charipova K, Gress K, et al. Treatment and management of myofascial pain syndrome. Best Pract Res Clin Anaesthesiol. 2020;34(3):427–448. doi:10.1016/j.bpa.2020.08.003
39. Lu W, Li J, Tian Y, Lu X. Effect of ischemic compression on myofascial pain syndrome: a systematic review and meta-analysis. Chiropr Man Therap. 2022;30(1):34. doi:10.1186/s12998-022-00441-5
40. Fredy DM, Harpin D, Mihardja H. The role of acupuncture for myofascial pain syndrome (MPS) in interventional pain management. J Complement Integr Med. 2022;19(2):213–217. doi:10.1515/jcim-2021-0525
41. Baltazar M, Russo J, De Lucca V, et al. Therapeutic ultrasound versus injection of local anesthetic in the treatment of women with chronic pelvic pain secondary to abdominal myofascial syndrome: a randomized clinical trial. BMC Womens Health. 2022;22(1):325. doi:10.1186/s12905-022-01910-y
42. Handa T, Ichinohe T. Acupuncture combined with trigger point injection in patient with chronic myofascial and referred pain. Bull Tokyo Dent Coll. 2020;61(2):121–126. doi:10.2209/tdcpublication.2019-0017
43. Yang Q, Yu S, Wang J, et al. Effects of Baduanjin on patients with chronic nonspecific low back pain: a randomized controlled trial. Medicine. 2021;100(4):e24448. doi:10.1097/MD.0000000000024448
44. Karmakar MK, Reina MA, Sivakumar RK, Areeruk P, Pakpirom J, Sala-Blanch X. Ultrasound-guided subparaneural popliteal sciatic nerve block: there is more to it than meets the eyes. Reg Anesth Pain Med. 2021;46(3):268–275. doi:10.1136/rapm-2020-101709
45. Ko S, Jun C, Lee JJ, Nam J. Comparison of the effects of corticosteroid and hyaluronic acid-carboxymethylcellulose solution on selective nerve root block for lumbar radiculopathy: a prospective, double-blind, randomized controlled clinical trial. Pain Pract. 2021;21(7):785–793. doi:10.1111/papr.13018
46. Jiang ZZ, Shen HL, Zhang Q, Ye G, Li XC, Liu XT. Elasticity evaluation of the plantar fascia: a shear wave elastography study involving 33 early-stage plantar fasciopathy subjects. Front Physiol. 2022;13:1060728. doi:10.3389/fphys.2022.1060728
47. Chin KJ, Lirk P, Hollmann MW, Schwarz S. Mechanisms of action of fascial plane blocks: a narrative review. Reg Anesth Pain Med. 2021;46(7):618–628. doi:10.1136/rapm-2020-102305
48. Murphy D, Lester D, Clay SF, Balakhanlou E, Zasler N. Peripheral neuropathic pain. NeuroRehabilitation. 2020;47(3):265–283. doi:10.3233/NRE-208002
49. Criss CR, Melton MS, Ulloa SA, et al. Rupture, reconstruction, and rehabilitation: a multi-disciplinary review of mechanisms for central nervous system adaptations following anterior cruciate ligament injury. Knee. 2021;30:78–89. doi:10.1016/j.knee.2021.03.009
50. Zhou Y, Jiang P, Wu J. Anterior quadratus lumborum block in the management of severe drug-resistant pain due to primary dysmenorrhoea. Eur J Pain. 2022;26(8):1821–1822. doi:10.1002/ejp.2001
51. Perez-Neri I, Sandoval H, Estevao MD, et al. Central and peripheral mechanisms of pain in fibromyalgia: scoping review protocol. Rheumatol Int. 2023;43(4):757–762. doi:10.1007/s00296-023-05275-9
52. Shi Y, Yao S, Shen Z, et al. Effect of electroacupuncture on pain perception and pain-related affection: dissociation or interaction based on the anterior cingulate cortex and S1. Neural Plast. 2020;2020:8865096. doi:10.1155/2020/8865096
53. Li Q, Becker B, Wernicke J, et al. Foot massage evokes oxytocin release and activation of orbitofrontal cortex and superior temporal sulcus. Psychoneuroendocrinology. 2019;101:193–203. doi:10.1016/j.psyneuen.2018.11.016
54. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285–296. doi:10.1016/j.jbusres.2021.04.070
55. Plaut S. Scoping review and interpretation of myofascial pain/fibromyalgia syndrome: an attempt to assemble a medical puzzle. PLoS One. 2022;17(2):e0263087. doi:10.1371/journal.pone.0263087
56. Stecco A, Gesi M, Stecco C, Stern R. Fascial components of the myofascial pain syndrome. Curr Pain Headache Rep. 2013;17(8):352. doi:10.1007/s11916-013-0352-9
57. Bron C, Dommerholt JD. Etiology of myofascial trigger points. Curr Pain Headache Rep. 2012;16(5):439–444. doi:10.1007/s11916-012-0289-4
58. Schilder A, Hoheisel U, Magerl W, Benrath J, Klein T, Treede RD. Sensory findings after stimulation of the thoracolumbar fascia with hypertonic saline suggest its contribution to low back pain. Pain. 2014;155(2):222–231. doi:10.1016/j.pain.2013.09.025
59. Wilke J, Schleip R, Klingler W, Stecco C. The lumbodorsal fascia as a potential source of low back pain: a narrative review. Biomed Res Int. 2017;2017:5349620. doi:10.1155/2017/5349620
60. Ballyns JJ, Shah JP, Hammond J, Gebreab T, Gerber LH, Sikdar S. Objective sonographic measures for characterizing myofascial trigger points associated with cervical pain. J Ultrasound Med. 2011;30(10):1331–1340. doi:10.7863/jum.2011.30.10.1331
61. De Coninck K, Hambly K, Dickinson JW, Passfield L. Measuring the morphological characteristics of thoracolumbar fascia in ultrasound images: an inter-rater reliability study. BMC Musculoskelet Disord. 2018;19(1):180. doi:10.1186/s12891-018-2088-5
62. Fernandez-de-Las-Penas C, Dommerholt J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: a delphi study. Pain Med. 2018;19(1):142–150. doi:10.1093/pm/pnx207
63. Draghi F, Gitto S, Bortolotto C, Draghi AG, Ori BG. Imaging of plantar fascia disorders: findings on plain radiography, ultrasound and magnetic resonance imaging. Insights Imaging. 2017;8(1):69–78. doi:10.1007/s13244-016-0533-2
64. Ball EM, McKeeman HM, Patterson C, et al. Steroid injection for inferior heel pain: a randomised controlled trial. Ann Rheum Dis. 2013;72(6):996–1002. doi:10.1136/annrheumdis-2012-201508
65. Tekin L, Akarsu S, Durmus O, Cakar E, Dincer U, Kiralp MZ. The effect of dry needling in the treatment of myofascial pain syndrome: a randomized double-blinded placebo-controlled trial. Clin Rheumatol. 2013;32(3):309–315. doi:10.1007/s10067-012-2112-3
66. Zheng B, Zhu J, Wu XL, Huang QM, Wu ZH. Research progress of acupuncture myofascial trigger point in pain treatment. Chin J Rehabil Med. 2022;37(01):117–120.
67. Chen XH, Liu BP, Xiao W, et al. Quality evaluation of randomized controlled trial report of acupuncture stimulating pain points for myofascial pain syndrome based on CONSORT and STRICTA. Chin J Rehabil Med. 2020;35(11):1372–1376.
68. Ma JJ, Ma TM, Wang L, Hu Z. Effect of moxibustion on the expression of microglia and brain-derived neurotrophic factor protein in the spinal cord of rats with myofascial pain syndrome. AcupunctRes. 2021;46(09):769–774. doi:10.13702/j.1000-0607.20210222
69. Liu S, Wang Z, Su Y, et al. A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature. 2021;598(7882):641–645. doi:10.1038/s41586-021-04001-4
70. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/s12630-020-01875-2
71. Zhou J, Lin Y, Zhang J, et al. Reliability of shear wave elastography for the assessment of gastrocnemius fascia elasticity in healthy individual. Sci Rep. 2022;12(1):8698. doi:10.1038/s41598-022-12786-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.