Back to Journals » Journal of Inflammation Research » Volume 16
Gastrointestinal Fistulas in Necrotizing Pancreatitis Receiving a Step-Up Approach Incidence, Risk Factors, Outcomes and Treatment
Authors Liu Z, Ke H, Xiong Y, Liu H, Yue M, Liu P ![]()
Received 3 August 2023
Accepted for publication 10 November 2023
Published 22 November 2023 Volume 2023:16 Pages 5531—5543
DOI https://doi.org/10.2147/JIR.S433682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Zheyu Liu,1 Huajing Ke,1 Yuwen Xiong,1 Hui Liu,1 Mengli Yue,2 Pi Liu3
1Department of Gastroenterology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Affiliated Longhua People’s Hospital, The Third School of Clinical Medicine, Southern Medical University, Shenzhen, People’s Republic of China; 3Department of Gastroenterology, Affiliated Longhua People’s Hospital, Southern Medical University, Shenzhen, People’s Republic of China
Correspondence: Pi Liu, Department of Gastroenterology, Affiliated Longhua People’s Hospital, Southern Medical University, Shenzhen, People’s Republic of China, Tel +86- 13507913736, Email [email protected]
Purpose: Necrotizing pancreatitis (NP) complicated by gastrointestinal fistula is challenging and understudied. As the treatment of necrotizing pancreatitis changed to a step-up strategy, we attempted to evaluate the incidence, risk factors, clinical outcomes and treatment of gastrointestinal fistulas in patients receiving a step-up approach.
Methods: Clinical data from 1274 patients with NP from 2014– 2022 were retrospectively analyzed. Multivariable logistic regression analysis was conducted to identify risk factors and propensity score matching (PSM) to explore clinical outcomes in patients with gastrointestinal fistulas.
Results: Gastrointestinal fistulas occurred in 8.01% (102/1274) of patients. Of these, 10 were gastric fistulas, 52 were duodenal fistulas, 14 were jejunal or ileal fistulas and 41 were colonic fistulas. Low albumin on admission (OR, 0.936), higher CTSI (OR, 1.143) and invasive intervention prior to diagnosis of gastrointestinal fistula (OR, 5.84) were independent risk factors for the occurrence of gastrointestinal fistula, and early enteral nutrition (OR, 0.191) was a protective factor. Patients who developed a gastrointestinal fistula were in a worse condition on admission and had a poorer clinical outcome (p< 0.05). After PSM, both groups of patients had similar baseline information and clinical characteristics at admission. The development of gastrointestinal fistulas resulted in new-onset persistent organ failure, increased open surgery, prolonged parenteral nutrition and hospitalization, but not increased mortality. The majority of patients received only conservative treatment and minimally invasive interventions, with 7 patients (11.3%) receiving surgery for upper gastrointestinal fistulas and 11 patients (26.9%) for colonic fistulas.
Conclusion: Gastrointestinal fistulas occurred in 8.01% of NP patients. Independent risk factors were low albumin, high CTSI and early intervention, while early enteral nutrition was a protective factor. After PSM, gastrointestinal fistulas resulted in an increased proportion of NP patients receiving open surgery and prolonged hospitalization. The majority of patients with gastrointestinal fistulas treated with step-up therapy could avoid surgery.
Keywords: necrotizing pancreatitis, a step-up approach, gastrointestinal fistula, minimally invasive step-up intervention
Introduction
Acute pancreatitis (AP) is a common disease of the gastrointestinal (GI) tract.1 Approximately 10–30% of patients progress to necrotizing pancreatitis(NP), which results in varying degrees of necrosis of the pancreatic parenchyma and/or peripancreatic tissue and severe local or systemic complications.2,3 Gastrointestinal fistula is one of the delayed complications secondary to necrotizing pancreatitis.4 The location of the fistula may involve the stomach, duodenum, jejunum, ileum and colon simultaneously or separately.5
The development of gastrointestinal fistulas is associated with direct erosion of adjacent gastrointestinal tissue by pancreatic enzymes released from pancreatic necrosis.6 Severe pancreatic inflammatory response also results in affecting the blood supply to the gastrointestinal tract thereby leading to gastrointestinal necrosis.7 In addition, as the treatment of necrotizing pancreatitis moves into the era of minimally invasive step-up strategy, the previous increase in catheter drainage interventions may also raise the risk of gastrointestinal fistula.8,9 Previously upper gastrointestinal fistulas (gastric and duodenal) were usually treated conservatively, whereas colonic fistulas usually required surgical treatment.7,10–13 With current changes in treatment strategies, recent studies have shown that minimally invasive percutaneous and endoscopic transcatheter treatment modalities can reduce the proportion of patients with gastrointestinal fistulas undergoing surgery.14,15
There are relatively few studies of necrotizing pancreatitis complicated by gastrointestinal fistulas receiving step-up therapy,12,15,16 which consist mainly of small sample studies or case reports; Therefore, we attempted to determine the incidence, specific risk factors, clinical outcomes, and effectiveness of minimally invasive interventions for gastrointestinal fistulas with this large retrospective sample of necrotizing pancreatitis.
Method
Study Design and Population
This retrospective study reviewed patients with necrotizing pancreatitis treated between January 1, 2014 and July 31, 2022 at the First Affiliated Hospital of Nanchang University. Patient hospitalization information was collected from the electronic medical record database of the First Affiliated Hospital of Nanchang University. The study was reviewed and approved by the institutional ethical review board (NO: 2023–201). This study was designed in accordance with the principles of the Declaration of Helsinki. All patient data were anonymously analyzed using an electronic data acquisition system without informed consent. The patient screening flowchart for this study is shown in Figure 1.
 |
Figure 1 Flow chart of patient enrolment. |
Definitions
Necrotizing pancreatitis was defined as a lack of pancreatic parenchymal enhancement and/or peripancreatic necrosis detected on imaging (contrast-enhanced computed tomography). Specialist radiologists reviewed all radiological images to diagnose necrotizing pancreatitis. Gastrointestinal fistula was defined as a pathological connection of any part of the gastrointestinal tract (stomach, duodenum, jejunum, ileum and colon) to the pancreas and/or peripancreatic necrotic cavity.17 However, gastrointestinal fistulas due to medical intervention were excluded (ie medical fistulas formed after the necrotic fluid collection of the pancreas has been drained via the stomach or duodenum). Organ failure was defined based on the modified Marshall Organ Dysfunction Scoring System. Patients with chronic pancreatitis, pancreatic cancer, gastrointestinal fistulas due to medically induced interventions and under-aged patients were excluded. The full definitions of this study are given in Table S1.
Diagnosis of Gastrointestinal Fistula
1) presence of gastrointestinal contents (faecal or nutritional fluid) in the drainage tube, 2) discharge of methylene blue from the drainage tube (after oral administration of methylene blue by the patient), 3) gastroenteroscopy, 4) imaging findings, 5) finding during minimally invasive necrosectomy, 6) finding during open surgery, 7) contrast fistula angiography.
Observation Outcome
Demographic variables including age, sex, etiology of pancreatitis, comorbidities, laboratory tests including white blood cells, procalcitonin, blood urea nitrogen and albumin within 48 hours of admission, computed tomography severity index(CTSI), clinical course variables including single organ failure, multi-organ failure and persistent multi-organ failure during hospitalization, duration of parenteral and enteral nutrition, the total length of stay in hospital, length of stay in intensive care unit, readmission, infected necrosis and associated complications (gastrointestinal hemorrhage, intra-abdominal hemorrhage, abdominal compartment syndrome, pancreatic fistula and symptomatic vein thrombosis), treatment included percutaneous catheter drainage or endoscopic transluminal drainage, the total number of catheter drains, the total number of minimally invasive necrosectomy, and whether open surgery was performed. Organ failure and ICU admissions were classified as either “early” or “delayed” periods. Early and delayed were defined by one week of admission, and this cut-off value is chosen based on the duration of necrotizing pancreatitis.
Patient Management
According to current evidence-based guidelines,2,18 patients were given supportive treatment on admission, including fluid resuscitation, suppression of pancreatic exocrine function and nutritional support. For patients without nausea and vomiting and without signs of severe gastrointestinal obstruction, a nasoduodenal nutrition tube was placed as soon as possible for enteral nutrition. Antibiotic therapy was used for patients with confirmed or strongly suspected infected pancreatic necrosis or other infections (eg blood, biliary, urinary, respiratory, etc.). Patients with NP were treated with a step-up approach, including percutaneous catheter drainage or endoscopic transluminal drainage as the first step in necrotic intervention and subsequent minimally invasive necrosectomy (videoscopically assisted retroperitoneal resection or endoscopic transluminal necrosectomy).
A similar step-up treatment strategy was used for patients with a confirmed diagnosis of gastrointestinal fistula. If symptoms did not improve with conservative treatment, including medication and keeping previously placed drains open, minimally invasive interventions including catheter drainage and endoscopic treatment (endoscopic clip closure) strategies were used. If the patient’s symptoms continued to worsen or did not improve significantly, a surgical enterostomy was performed if necessary.
Statistical Analysis
Data for categorical variables were shown as frequencies and percentages. Continuous variables were described as means and standard deviations (SD) when normally distributed and as medians and interquartile distances when non-normally distributed. Differences between groups were assessed using chi-square or Fisher’s exact test for categorical variables and Student’s t-test or Mann–Whitney U-test for continuous variables. Logistic regression analysis was performed to assess risk factors for GI fistula in NP. Variables found to be significant for GI fistula in the one-way logistic regression analysis (p < 0.1) were selected for inclusion in the multifactorial analysis to identify them as independent risk factors. Variables were selected in a stepwise forward manner for the multi-factor analysis and the ratio (OR) with a 95% confidence interval (CI) was calculated. Subgroup analyses were performed to explore risk factors for the occurrence of upper gastrointestinal fistula, lower gastrointestinal fistula, and patients admitted to the hospital within 72 h of onset. To assess and validate the clinical outcome of GI fistulas in NP, a 1:1 propensity score-matched analysis was performed to balance the confounding bias of each group between groups, with a caliper value of 0.02. Propensity score-matching incorporated age, serum albumin, CTSI, early persistent organ failure, early ICU admission, early enteral nutrition, early intervention, and infected necrosis (where early intervention and infected necrosis occurred before the diagnosis of gastrointestinal perforation or fistula). Variables were selected based on differences in demographic variables and clinical characteristics of all NP patients at admission. P values < 0.05 were regarded as statistically significant differences. In this study, we used SPSS 26.0 (IBM Corp., Armonk, NY, USA) for statistical analysis.
Results
Incidence and Clinical Characteristics at Admission
A total of 1274 patients treated for necrotizing pancreatitis were enrolled in the study between 2014 and 2022 (Table 1), of which 102 patients (8.01%) developed a gastrointestinal fistula. The most common etiology in all patients with necrotizing pancreatitis was biliary pancreatitis (n = 561, 44.0%). 816 patients (64.0%) had pancreatic parenchymal necrosis with or without peripancreatic necrosis, and 458 patients (36.0%) had peripancreatic necrosis only. According to demographic and clinical characteristics at admission (Table 1), patients with GI fistulas had lower albumin (p<0.001) and higher CTSI (p<0.001) compared to those without GI fistulas. Patients with GI fistulas were more likely to have early persistent organ failure (p = 0.004), a higher proportion of early ICU admissions (p = 0.011) and a lower proportion receiving early enteral nutrition (p<0.001). Patients with combined GI fistula (before GI fistula was diagnosed) were more likely to have infected necrosis (p<0.001) and invasive interventions (p<0.001) compared to those without GI fistula. Baseline and clinical characteristics of patients with necrotizing pancreatitis on admission after propensity score matching are shown in Table S2.
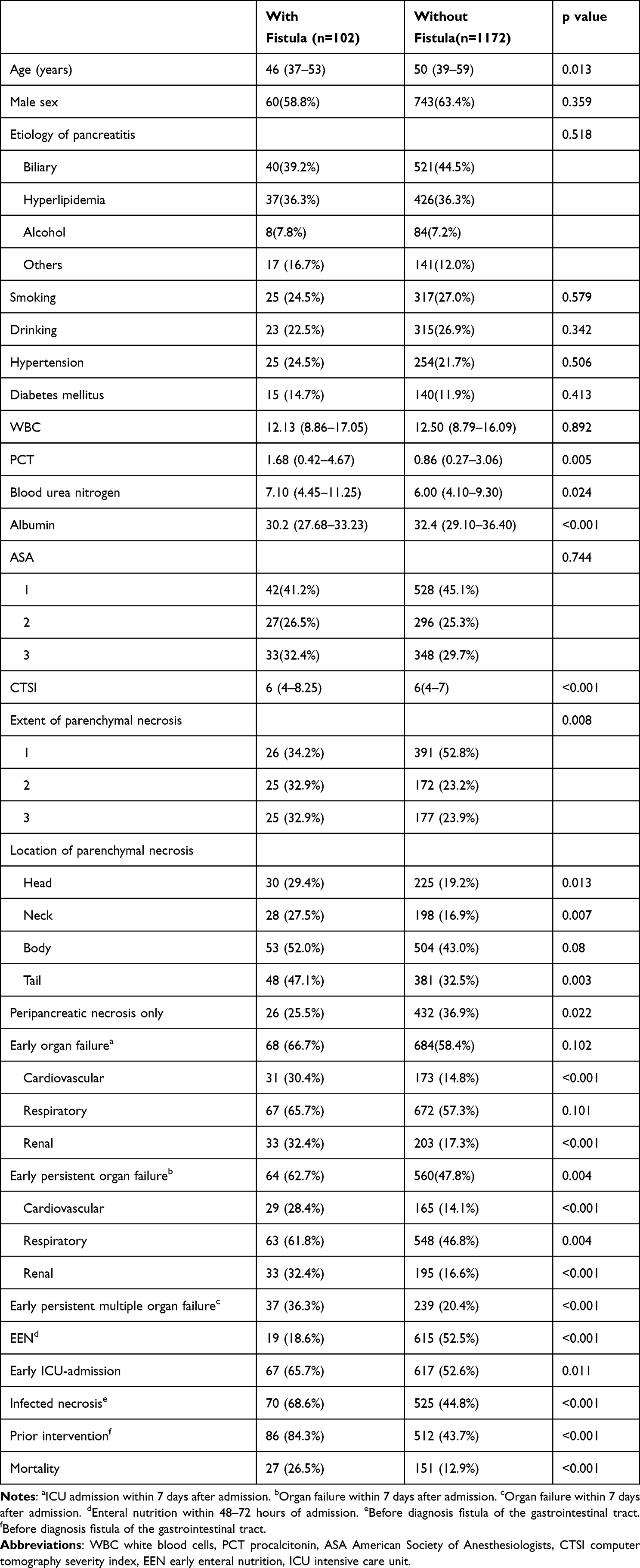 |
Table 1 Baseline Characteristics and Clinical Characteristics of Patients with Necrotizing Pancreatitis at Admission to the Hospital |
Risk Factors
The results of multifactorial analyses are reported in Table 2. In multivariate logistic regression models, low albumin within 48 hours of admission (OR, 0.936; 95% CI, 0.898–0.976; p=0.002), higher CTSI (OR, 1.143; 95% CI, 1.041–1.255; p= 0.005) and invasive intervention prior to diagnosis of gastrointestinal fistula (OR, 5.84; 95% CI, 3.364–103,644; p<0.001) were independently associated with the development of gastrointestinal fistula. In addition, early enteral nutrition (OR, 0.194; 95% CI, 0.112–0.327; p<0.001) was identified as a protective factor for the development of gastrointestinal fistula. In subgroup analyses, pancreatic head and neck necrosis (OR, 2.319; 95% CI, 1.367–3.934; P= 0.002) was likewise an independent risk factor for upper gastrointestinal fistula, as were pancreatic body and tail necrosis (OR, 2.366; 95% CI, 1.221–4.584; P= 0.011) and early persistent respiratory failure (OR, 2.065; 95% CI, 1.062–4.014; P= 0.033) were also independent risk factors for lower gastrointestinal fistula. Early persistent respiratory failure (OR, 2.866; 95% CI, 1.051–7.818; P= 0.04) was an independent risk factor for gastrointestinal fistula in patients admitted within 72 h after onset of the disease. Univariate logistic regression analyses of the risk factors associated with the total number of patients and subgroups who developed GI fistulas are shown in Table S3.
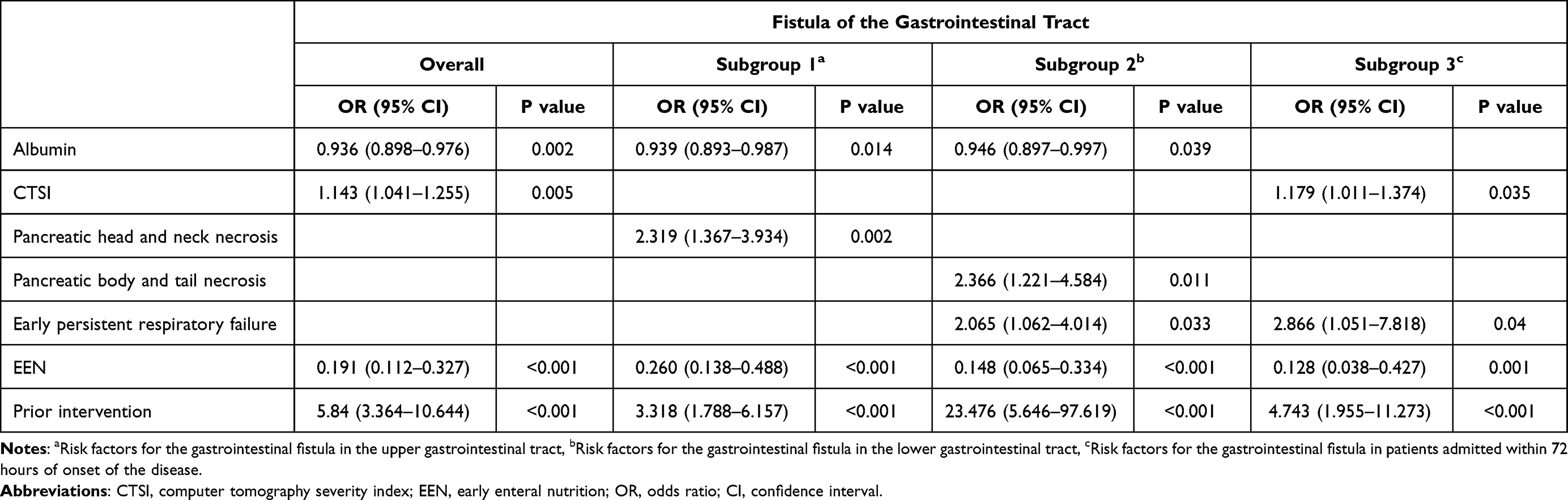 |
Table 2 Multifactorial Logistic Regression Analysis of the Occurrence of a Gastrointestinal Fistula in Patients with Necrotizing Pancreatitis |
Location and Diagnosis of Gastrointestinal Fistula
A total of 117 gastrointestinal fistulas were involved in 102 patients (Table 3). The stomach was involved in 10 (8.5%) patients and the duodenum in 52 (44.4%). The jejunum or ileum was involved in 14 (12.0%) patients, and 41 patients (35.1%) had colonic involvement. Thirteen of these patients had simultaneous or sequential involvement of multiple sites of the gastrointestinal tract. The median (interquartile) interval between the onset of necrotizing pancreatitis and the diagnosis of gastrointestinal fistula was 57 (34.5–93.5) days. The median number of days between the first invasive intervention and the diagnosis of a gastrointestinal fistula was 28 (11.5–52) days. Upper gastrointestinal fistulas (gastric and duodenal) were primarily detected by gastroscopy (36/62) and, to a lesser extent during minimally invasive necrosectomy (6/62). Lower gastrointestinal fistulas (jejunum, ileum and colon) were diagnosed mainly by finding faeces in the external drainage fluid (19/55), followed by open necrosectomy (8/55).
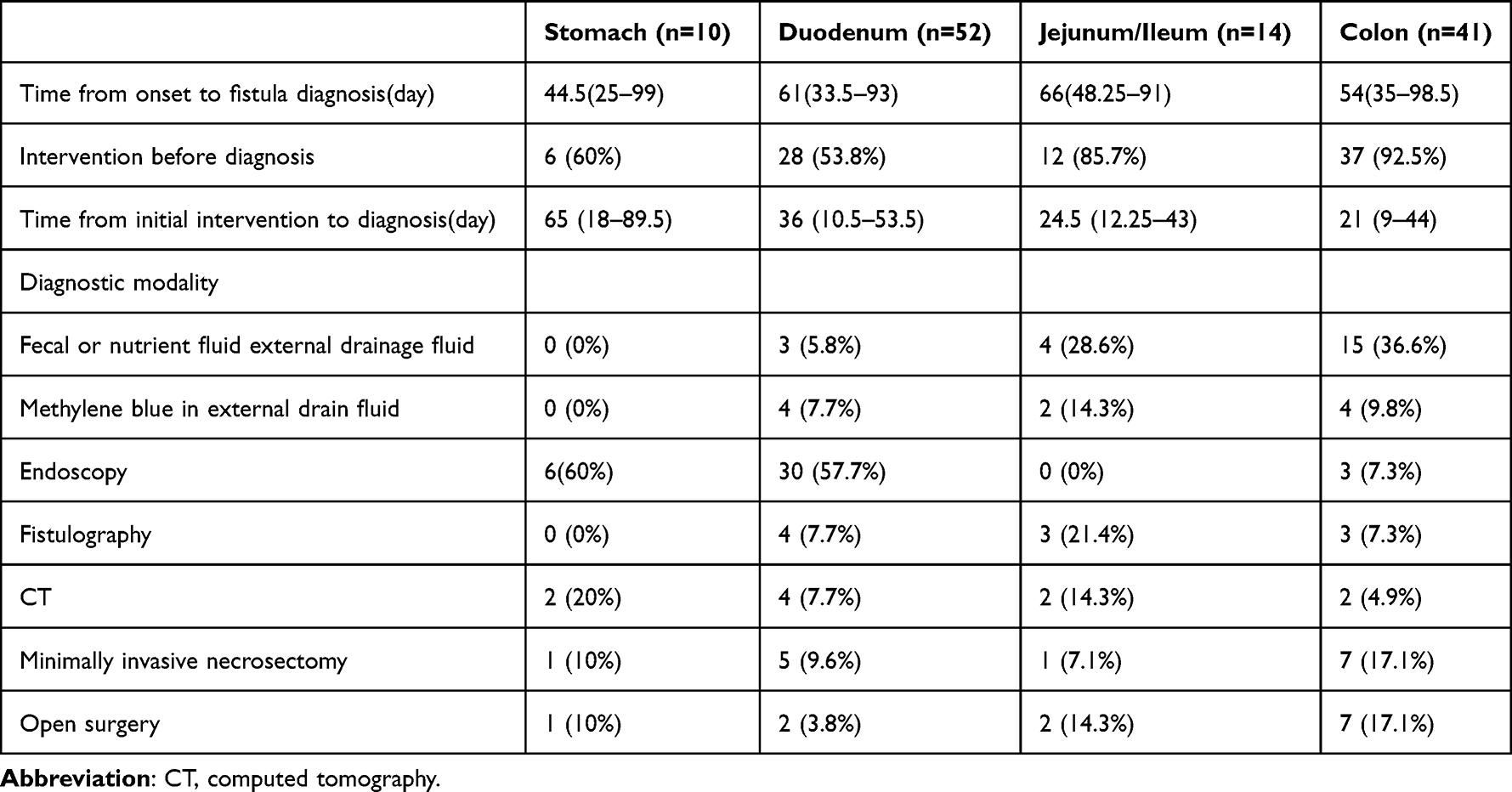 |
Table 3 Diagnostic Modalities of Gastrointestinal Fistulas |
Clinical Outcomes
Compared to NP patients without GI fistula, those with GI fistula were more likely to have persistent organ failure (single and multiple organs, p<0.05), required longer-term nutritional support (parenteral and enteral nutrition, p<0.05), received more invasive interventions (minimally invasive interventions and open surgery, p<0.05) and were more prone to pancreatic-related complications (hemorrhage, abdominal compartment syndrome and symptomatic vein thrombosis). Patients with GI fistulas had a significantly longer duration of illness (length of hospital stay, length of ICU stay and readmission, p<0.05) and a significantly higher mortality rate (Table 4).
 |
Table 4 Clinical Outcome of Patients with Necrotizing Pancreatitis |
Patients admitted with the presence of GI fistulas were clearly in serious condition by comparing baseline data and clinical characteristics at admission. We performed propensity score matching analyses to control for and reduce confounding bias in each group, and we compared clinical outcomes between the two groups with similar backgrounds. After propensity score matching analysis, the clinical characteristics of the two groups on admission were generally balanced. The proportion of new-onset persistent renal failure, the proportion receiving minimally invasive interventions, the occurrence of pancreas-related complications, and mortality were similar in the two groups. However, the proportion of new-onset persistent cardiovascular and respiratory failure, duration of parenteral nutritional support, receipt of open surgical interventions, and length of hospital stay were significantly higher in patients with gastrointestinal fistula than in those without gastrointestinal fistula (P<0.05).
Therapy
The treatment of the GI fistula is shown in Table 5.
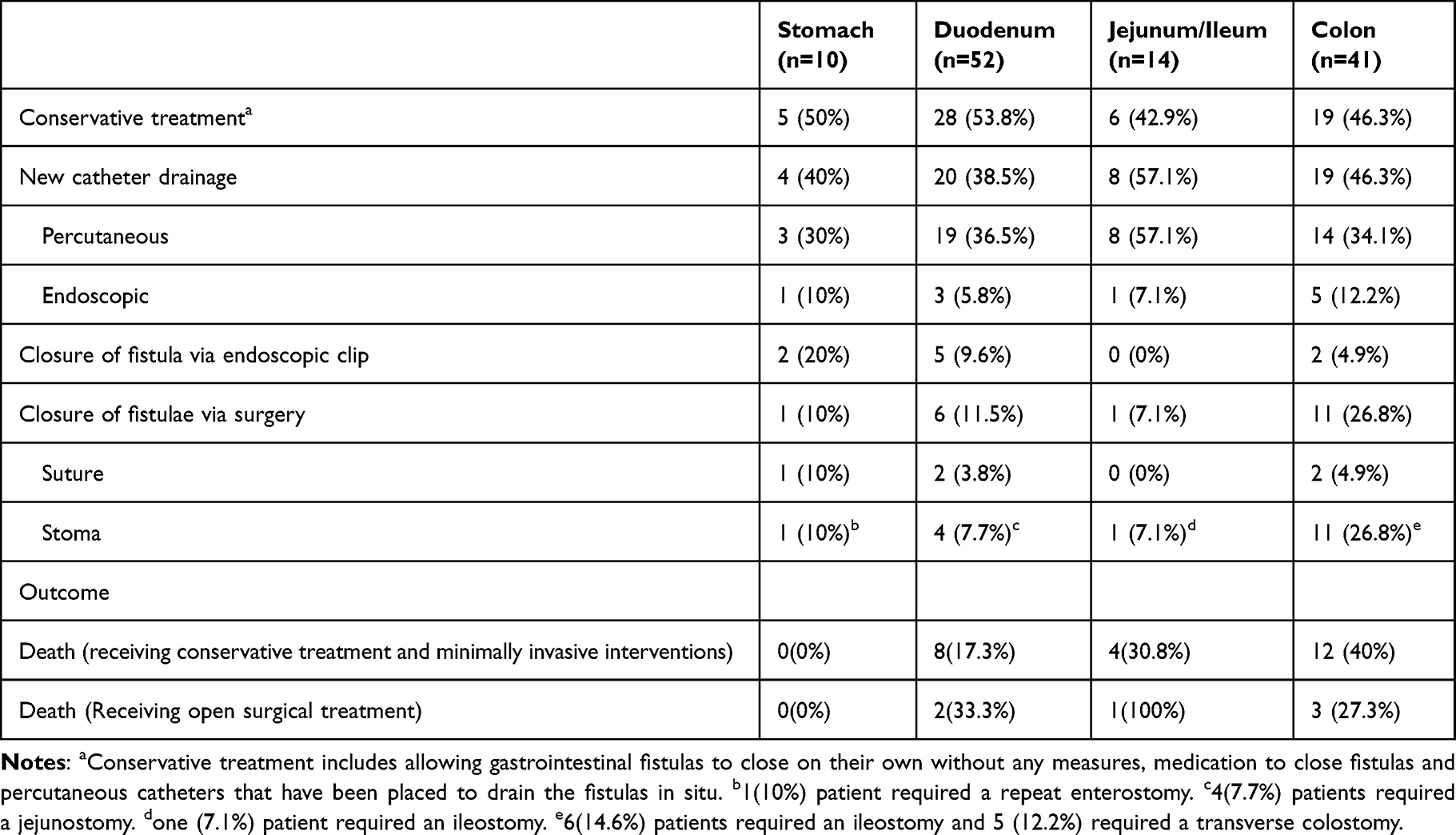 |
Table 5 Treatment Strategies for Gastrointestinal Fistulas |
Five (50%) patients with gastric fistulas were treated conservatively and the fistula was closed, four (40%) patients had drainage of the fistula, two (20%) patients had endoscopic closure of the fistula, and one (10%) patient required a repeat enterostomy. No mortality was observed in patients with gastric fistulas.
Twenty-eight (53.8%) patients with duodenal fistulas received only conservative treatment (including catheter drainage prior to diagnosis of fistula), 20 (38.5%) had catheter drainage of the fistula, 5 (9.6%) had endoscopic closure of the duodenal fistula, 2 (3.8%) had intraoperative closure of the fistula and 4 (7.7%) had a jejunostomy. The mortality rate for patients with duodenal fistula without surgical intervention was 17.3% (8 out of 46) compared to 33.3% (2 out of 6) for patients with duodenal fistula with surgical intervention.
Six (42.9%) patients with jejunal or ileal fistulas were treated conservatively only, eight (57.1%) had catheter drainage of the fistula and one (7.1%) had an ileostomy. The mortality rate of patients with jejunal or ileal fistulas who did not receive surgical intervention was 30.8% (4 of 13), and the only patient who did receive surgical intervention died after an ileostomy.
Nineteen (46.3%) patients with colonic fistulas were treated conservatively without further invasive intervention, 19 (46.3%) patients had drainage of colonic fistulas, 2 (5.0%) patients had endoscopic closure of colonic fistulas, 2 (5.0%) patients had intraoperative closure of fistulas, 6 (14.6%) patients had an ileostomy, and 5 (12.2%) had a transverse colostomy. The mortality rate for patients with colonic fistulas who did not receive surgical intervention was 40% (12 out of 30), slightly higher (3 out of 11) than patients who received surgical intervention for colonic fistulas.
Discussion
Since the management of necrotizing pancreatitis shifted to an approach of minimally invasive step-up based on first-step catheter drainage, there has been a lack of large series evaluating the incidence, specific risk factors, clinical outcomes and treatment of gastrointestinal fistulas in patients with necrotizing pancreatitis receiving step-up therapy. The incidence of gastrointestinal fistula in necrotizing pancreatitis in this large retrospective study was 8.01%. This large series found a relatively low incidence of gastrointestinal fistulas compared to previous studies, where the incidence of GI fistulas ranged from 4–41%.6,9,12,13,16,21 This could be explained by the fact that the previous studies mainly originated from patients with necrotizing pancreatitis in the open surgery era or a different study population (eg including only patients with infected necrotizing pancreatitis). Gastrointestinal fistulas, as a delayed complication of necrotizing pancreatitis, usually occurred after the first month. The time to diagnosis of gastrointestinal fistula in this study was 57 (34.5–93.5) days, which is similar to previous studies.9
Current research identified several important risk factors for the development of gastrointestinal fistula in NP. Low albumin within 48 hours of admission was an independent risk factor for fistula development, and early enteral nutrition was a protective factor. Previous studies have shown that when pancreatic necrosis occurs, the gastrointestinal tract is directly exposed to necrotic material and pancreatic enzymes, leading to a deterioration in the condition of the gastrointestinal tract and failure of the intestinal barrier.22 In addition, a severe local inflammatory response promotes thrombosis and reduces the blood supply to the relevant gastrointestinal segments.23 This eventually leads to focal necrosis of the gastrointestinal tract and the formation of a fistula that connects the pancreatic and/or peripancreatic necrotic cavity or peritoneum. A decrease in albumin represents deterioration in the nutritional status of the patient. When patients with pancreatitis lack essential nutrition, this disrupts the integrity of the intestinal tract leading to increased gastrointestinal dysfunction.24 Early enteral nutrition helps to maintain intestinal barrier function, reduce the inflammatory response, treat malnutrition and reduce the risk of infected necrosis.25 Moreover, in subgroup analyses, early enteral nutrition was also a protective factor against the development of gastrointestinal fistula in patients admitted to the hospital within 72 h of onset.
A high CTSI after admission was also an independent risk factor for the development of a fistula. High CTSI is manifested by more extensive pancreatic necrosis and more peripancreatic necrotic fluid collections.26 The direct compressive effect of large amounts of necrotic pancreatic tissue affects the blood supply to the gastrointestinal tract. This may lead to the formation of gastrointestinal fistulas. Subgroup analyses showed that the site of pancreatic necrosis had an effect on the location of gastrointestinal fistula involvement. Pancreatic head and neck necrosis was an independent risk factor for upper gastrointestinal fistula, and pancreatic body and tail necrosis was an independent risk factor for lower gastrointestinal fistula. This appears to correlate with the anatomical location of the pancreas in relation to neighboring organs. The duodenum is anatomically connected to the head of the pancreas, while the body and tail of the pancreas are anatomically closely related to the transverse colon and the splenic flexure of the colon.19,27 A previous study by Timmerhuis et al reported early intervention as being an important risk factor for the development of lower gastrointestinal fistulas, which is similar to our findings.9 This may be related to the prolonged contact of the drainage tube with the gastrointestinal tract and its invasive and compressive effect on the gastrointestinal tract. There is a lack of standardized diagnostic tests for the identification of gastrointestinal fistulas. Patients with NP who have a gastrointestinal fistula do not always have clear clinical signs and bubbles detected on CECT imaging in the retroperitoneum outside the lumen or within the necrotic zone are often confused with infected necrosis of the pancreas.28 Gastrointestinal fistulas are suspected in more than half of patients because of the presence of nutrient fluid or faeces in the drainage tube, which in turn leads to further diagnosis by other invasive procedures. This also seems to explain early invasive interventions as a risk factor for the development of gastrointestinal fistula. It is therefore of interest to clinicians to clarify the risk factors for gastrointestinal fistulas and the timing of their occurrence for definitive diagnosis and treatment.
In the present study, the occurrence of gastrointestinal fistulas was associated with poor clinical outcomes. A previous study by Timmerhuis et al reported that patients with NP who developed a gastrointestinal fistula had a higher rate of organ failure and longer lengths of hospital and ICU stay.9 Furthermore, in all patients with necrotizing pancreatitis, the occurrence of a gastrointestinal fistula increased the risk of death, which is also consistent with the previous study by Jiang et al.12 After balancing the baseline and clinical characteristics of the two groups of patients on admission by propensity score matching, we found that the occurrence of gastrointestinal fistulas significantly increased the rate of persistent respiratory organ failure. As the development of a gastrointestinal fistula required patients to receive longer nutritional support and more invasive interventions to facilitate its closure, this resulted in a prolonged clinical course for patients who developed a gastrointestinal fistula.
Previously, for most upper gastrointestinal fistulas (gastric and duodenal), jejunal and ileal fistulas could be self-closing with conservative treatment.13 However, most colonic fistulas were persistent and required surgical treatment.7,20 Previous studies have shown that frequent open surgery disrupts the pancreatic ducts to release pancreatic enzymes, which in turn leads to an increased risk of gastrointestinal fistulas.29 A study of gastrointestinal fistulas in patients undergoing surgical treatment for necrotizing pancreatitis by Tsiotos et al showed that only close to a quarter of patients had a gastrointestinal fistula identified during the initial surgical intervention, with the majority having a combined gastrointestinal fistula after surgery occurred.6 In recent years, the standard approach to necrotizing pancreatitis has shifted from open surgery to a step-up strategy based on minimally invasive interventions.30 In this study, all patients with NP were treated with a step-up strategy based on minimally invasive interventions. Despite the relatively low incidence of gastrointestinal fistulas in our patients, our study cohort lacked patients who underwent only open surgery for a controlled study. Previous studies have observed no significant difference in the occurrence of gastrointestinal fistulas requiring intervention between patients who underwent the step-up strategy and those who underwent surgery (14% vs 22%).31 It is therefore not possible to confirm the superiority of minimally invasive intervention strategies over surgical strategies in preventing the occurrence of gastrointestinal fistulas.
A significant proportion of patients in our cohort (73.7%) with upper gastrointestinal (gastric and duodenal), jejunal and ileal fistulas could be successfully treated with conservative treatment or minimally invasive interventions (catheter drainage or endoscopic clips). The mortality rate for patients with upper gastrointestinal fistulas (gastric and duodenal), jejunum and ileocecal fistulas was 19.7%. Unlike previous studies of colonic fistulas, a total of 43.9% of patients with colonic fistulas in this study were treated conservatively or with minimally invasive interventions (catheter drainage or endoscopic clips) resulting in self-closing fistulas. The mortality rate for patients with colonic fistulas was 36.6%, with a slightly higher mortality rate for those who did not receive surgical treatment (40%) than for those who did (27%). This is related to the deterioration of the clinical status of some patients (eg persistent multi-organ failure or combined infectious shock), which does not allow for surgical intervention. A previous study of colonic fistulas in patients with infected pancreatic necrosis treated with a step-up treatment strategy showed that close to half of the patients did not undergo open surgical treatment, which is similar to the results of our study.14 In addition to catheter drainage, one patient with a gastric fistula, five with a duodenal fistula and two with a colonic fistula attempted to close the fistula by endoscopic clamping in this study. For small fistulas with uninflamed margins, the fistula could be closed with a clip. Some case reports similarly described the closure of gastrointestinal perforations or fistulas by the endoscopic clamp system (OTSC).32–34 This suggests the potential benefit of endoscopy for the treatment of gastrointestinal fistulas. For the treatment of gastrointestinal fistulas, our current experience is that patients whose fistulas do not close spontaneously after conservative treatment should be treated first with catheter drainage and endoscopic treatment. For gastrointestinal fistulas that cannot be closed by minimally invasive intervention, the optimal timing of surgery should be assessed based on the patient’s clinical status, including nutritional status and local and systemic complications. More prospective studies are needed in the future to determine specific treatment strategies.
There are certain limitations to this study. Firstly there may be undiagnosed gastrointestinal fistulas in patients who have not undergone invasive interventions and have no significant clinical symptoms, which distort the true potential incidence. In addition, this was a single-centre retrospective study, and some patients had received long-term treatment at other institutions. As opposed to defined clinical outcomes and treatments, the clinical indicators involved were influenced by the detail of the clinical information available at the time the patients were referred, leading to the possibility of some statistical bias regarding the factors that contribute to the occurrence of gastrointestinal fistulas.
Conclusion
The incidence of gastrointestinal fistulas in patients with NP was 8.01%. Low albumin, high CTSI and early invasive interventions were identified as independent risk factors, and early enteral nutrition was shown to be a significant protective factor. Gastrointestinal fistulas were associated with poorer clinical outcomes, and after PSM the occurrence of gastrointestinal fistulas did not increase mortality, but only led to an increased rate of new-onset persistent organ failure, an increase in the proportion of patients receiving open surgery, and a prolongation of the duration of parenteral nutritional support and the clinical course of the disease. Gastrointestinal fistulas could be effectively managed in most patients with a step-up strategy while avoiding open surgical treatment.
Ethical Approval and Consent to Participate
The clinical data of the patients in this study were obtained from the electronic medical record system of the First Affiliated Hospital of Nanchang University and reviewed and approved by the Review Committee of the First Affiliated Hospital of Nanchang University (No. 2023-201). As this was a retrospective study analyzing only available clinical data, informed consent from patients was not required.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interest.
References
1. Mederos MA, Reber HA, Girgis MD. Acute pancreatitis: a review. JAMA. 2021;325(4):382–390. doi:10.1001/jama.2020.20317
2. Trikudanathan G, Wolbrink DRJ, van Santvoort HC, Mallery S, Freeman M, Besselink MG. Current concepts in severe acute and necrotizing pancreatitis: an evidence-based approach. Gastroenterol. 2019;156(7):1994–2007.e3. doi:10.1053/j.gastro.2019.01.269
3. Maatman TK, Mahajan S, Roch AM, et al. High rates of readmission in necrotizing pancreatitis: natural history or opportunity for improvement? J Gastrointest Surg. 2019;23(9):1834–1839. doi:10.1007/s11605-018-04097-6
4. Maatman TK, Roch AM, Ceppa EP, et al. The continuum of complications in survivors of necrotizing pancreatitis. Surg. 2020;168(6):1032–1040. doi:10.1016/j.surg.2020.07.004
5. Danilov MV, Vishnevskii VA, Kaltaev KK. External gastric and intestinal fistulas as a complication of acute pancreatitis. Vestn Khir Im I I Grek. 1972;107(3):122–123.
6. Tsiotos GG, Smith CD, Sarr MG. Incidence and management of pancreatic and enteric fistulas after surgical management of severe necrotizing pancreatitis. Arch Surg. 1995;130(1):48–52. doi:10.1001/archsurg.1995.01430010050010
7. Van Minnen LP, Besselink MG, Bosscha K, Van Leeuwen MS, Schipper ME, Gooszen HG. Colonic involvement in acute pancreatitis. A retrospective study of 16 patients. Dig Surg. 2004;21(1):33–38. doi:10.1159/000075824
8. Arvanitakis M, Dumonceau JM, Albert J, et al. Endoscopic management of acute necrotizing pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) evidence-based multidisciplinary guidelines. Endoscopy. 2018;50(5):524–546. doi:10.1055/a-0588-5365
9. Timmerhuis HC, van Dijk SM, Hollemans RA, et al. Perforation and fistula of the gastrointestinal tract in patients with necrotizing pancreatitis: a nationwide prospective cohort. Ann Surg. 2022;278(2):e284–e292. doi:10.1097/sla.0000000000005624
10. Bouillot JL, Alexandre JH, Vuong NP. Colonic involvement in acute necrotizing pancreatitis: results of surgical treatment. World J Surg. 1989;13(1):84–87. doi:10.1007/bf01671159
11. Gumaste VV, Gupta R, Wasserman D, Dave PB, Vieux U. Colonic involvement in acute pancreatitis. Am J Gastroenterol. 1995;90(4):640–641.
12. Jiang W, Tong Z, Yang D, et al. Gastrointestinal fistulas in acute pancreatitis with infected pancreatic or peripancreatic necrosis: a 4-year single-center experience. Medicine. 2016;95(14):e3318. doi:10.1097/md.0000000000003318
13. Kochhar R, Jain K, Gupta V, et al. Fistulization in the GI tract in acute pancreatitis. Gastrointest Endosc. 2012;75(2):436–440. doi:10.1016/j.gie.2011.09.032
14. Gao L, Zhang JZ, Gao K, et al. Management of colonic fistulas in patients with infected pancreatic necrosis being treated with a step-up approach. HPB. 2020;22(12):1738–1744. doi:10.1016/j.hpb.2020.03.021
15. Rana SS, Sharma R, Dhalaria L, Kang M, Gupta R. A case series of late gastrointestinal fistulization in 16 Patients with walled-off necrosis. Dig Dis Sci. 2022;67(2):661–666. doi:10.1007/s10620-021-06900-y
16. Hua Z, Su Y, Huang X, et al. Analysis of risk factors related to gastrointestinal fistula in patients with severe acute pancreatitis: a retrospective study of 344 cases in a single Chinese center. BMC Gastroenterol. 2017;17(1):29. doi:10.1186/s12876-017-0587-8
17. Falconi M, Pederzoli P. The relevance of gastrointestinal fistulae in clinical practice: a review. Gut. 2001;49 (Suppl 4):iv2–10. doi:10.1136/gut.49.suppl_4.iv2
18. Baron TH, DiMaio CJ, Wang AY, Morgan KA. American Gastroenterological Association clinical practice update: management of pancreatic necrosis. Gastroenterology. 2020;158(1):67–75.e1. doi:10.1053/j.gastro.2019.07.064
19. Banter LR, Maatman TK, McGuire SP, et al. Duodenal complications in necrotizing pancreatitis: challenges of an overlooked complication. Am J Surg. 2021;221(3):589–593. doi:10.1016/j.amjsurg.2020.11.022
20. Mohamed SR, Siriwardena AK. Understanding the colonic complications of pancreatitis. Pancreatology. 2008;8(2):153–158. doi:10.1159/000123607
21. Ho HS, Frey CF. Gastrointestinal and pancreatic complications associated with severe pancreatitis. Arch Surg. 1995;130(8):817–822. doi:10.1001/archsurg.1995.01430080019002
22. Doberneck RC. Intestinal fistula complicating necrotizing pancreatitis. Am J Surg. 1989;158(6):581–583. doi:10.1016/0002-9610(89)90198-0
23. Russell JC, Welch JP, Clark DG. Colonic complications of acute pancreatitis and pancreatic abscess. Am J Surg. 1983;146(5):558–564. doi:10.1016/0002-9610(83)90288-x
24. Ramanathan M, Aadam AA. Nutrition management in acute pancreatitis. Nutr Clin Pract. 2019;34(Suppl 1):S7–S12. doi:10.1002/ncp.10386
25. Jabłońska B, Mrowiec S. Nutritional support in patients with severe acute pancreatitis-current standards. Nutrients. 2021;13(5):1498. doi:10.3390/nu13051498
26. Vriens PW, Van de linde P, Slotema ET, Warmerdam PE, Breslau PJ. Computed tomography severity index is an early prognostic tool for acute pancreatitis. J Am Coll Surg. 2005;201(4):497–502. doi:10.1016/j.jamcollsurg.2005.06.269
27. Sunkara T, Etienne D, Caughey ME, Gaduputi V. Small bowel obstruction secondary to acute pancreatitis. Gastroenterol Res. 2017;10(1):42–44. doi:10.14740/gr758w
28. Balthazar EJ. Complications of acute pancreatitis: clinical and CT evaluation. Radiol Clin North Am. 2002;40(6):1211–1227. doi:10.1016/s0033-8389(02)00043-x
29. Pemberton JH, Nagorney DM, Becker JM, Ilstrup D, Dozois RR, Remine WH. Controlled open lesser sac drainage for pancreatic abscess. Ann Surg. 1986;203(6):600–604. doi:10.1097/00000658-198606000-00003
30. van Brunschot S, van Grinsven J, van Santvoort HC, et al. Endoscopic or surgical step-up approach for infected necrotising pancreatitis: a multicentre randomised trial. Lancet. 2018;391(10115):51–58. doi:10.1016/s0140-6736(17)32404-2
31. van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010;362(16):1491–1502. doi:10.1056/NEJMoa0908821
32. Gray DM, Mullady DK. Attempted endoscopic closure of a pancreaticocolonic fistula with an over-the-scope clip. J Pancr. 2012;13(6):712–714. doi:10.6092/1590-8577/1220
33. Choi JH, Kim SW. Endoscopic management of a colonic fistula communicating with a walled-off pancreatic necrosis. Digest Liver Dis. 2018;50(9):971. doi:10.1016/j.dld.2018.04.017
34. Ito K, Igarashi Y, Mimura T, et al. Severe acute pancreatitis with complicating colonic fistula successfully closed using the over-the-scope clip system. Case Rep Gastroenterol. 2013;7(2):314–321. doi:10.1159/000354276
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.