Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Gamification and Virtual Reality for Enhancing Disaster Preparedness Among University Students and Health Workers: A Scoping Review
Authors Emaliyawati E ![]() , Sugiharto F
, Sugiharto F ![]() , Ibrahim K
, Ibrahim K ![]() , Trisyani Y
, Trisyani Y ![]() , Songwathana P
, Songwathana P ![]()
Received 28 January 2026
Accepted for publication 7 May 2026
Published 20 May 2026 Volume 2026:19 599619
DOI https://doi.org/10.2147/JMDH.S599619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Etika Emaliyawati,1 Firman Sugiharto,2 Kusman Ibrahim,3 Yanny Trisyani,1 Praneed Songwathana4
1Department of Emergency and Critical Care Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Doctoral Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Medical-Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Adult and Elderly Nursing, Faculty of Nursing, Prince of Songkla University, Songkhla, 90110, Thailand
Correspondence: Etika Emaliyawati, Department of Emergency and Critical Care Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Fax +622287793411, Email [email protected]
Background: Effective disaster training is essential for developing competencies in rapid decision-making, teamwork, and protocol-based actions. However, conventional approaches, such as lectures and limited simulations, often face challenges, including low engagement and difficulty replicating complex disaster scenarios. These limitations have driven the adoption of innovative strategies, such as gamification and virtual reality (VR), to enhance disaster education.
Purpose: This scoping review aimed to synthesise and critically evaluate evidence on the effectiveness of gamification and VR-based interventions in improving disaster preparedness learning outcomes among university students and health workers.
Methods: This scoping review followed the Arksey and O’Malley framework. Studies were searched in EBSCOhost, PubMed, Scopus, SAGE Journal, and Taylor & Francis using relevant keywords. Included studies were original research in English that evaluated gamification or VR in disaster training contexts. The data were analysed using descriptive, qualitative, and narrative synthesis.
Results: A total of 24 studies were included, with diverse designs. Across the included studies, interventions were divided into two categories: gamification and virtual reality-based interventions. In addition, learning outcomes were consistently reported across three domains: cognitive outcomes (e.g. disaster preparedness knowledge, triage knowledge, crisis management competence), psychomotor outcomes (e.g. triage skills, triage accuracy, intervention correctness, decision speed), and affective outcomes (e.g. self-efficacy, satisfaction, motivation, preparedness attitudes).
Conclusion: Gamification and VR interventions improve disaster preparedness learning outcomes among students and health workers across cognitive, psychomotor, and affective domains. These approaches offer flexible and engaging alternatives to conventional training and may support scalable disaster education programs. Future studies should use more rigorous comparative designs, standardized outcome measures, and long-term follow-up to assess skill retention and transfer to real-world settings.
Keywords: disaster preparedness, gamification, good health and well-being, health workers, university students, virtual reality
Introduction
Natural disasters and emergencies can occur anytime, anywhere, requiring high levels of preparedness from all levels of society, especially students and health workers, who are often at the forefront of disaster response.1 Effective disaster training is essential to ensure that individuals involved in disaster management possess the skills for rapid decision-making, team coordination, and the implementation of safety protocols.2 Good training also helps improve response efficiency and minimise the risks and impacts posed by disasters.
Disaster preparedness is a crucial element in reducing the impact of disasters on communities. With the increasing frequency of disasters due to climate change, disaster education is becoming increasingly important to improve public awareness and response to emergency situations.3,4 However, traditional training methods such as field simulations and evacuation drills are often expensive, difficult to replicate, and lack flexibility.5 A previous study reported that obstacles to conventional learning include low participant involvement, limitations in replicating realistic disaster scenarios, and high operational costs.6,7 Therefore, innovative approaches such as gamification and virtual reality (VR) technology have emerged as potential solutions to improve the effectiveness of disaster preparedness training.
Literature Review
Gamification and VR are complementary innovative approaches in education with distinct focuses. Gamification refers to the use of game design elements such as points, levels, and feedback in non-game contexts to enhance learner motivation, supported by Self-Determination Theory.8 In contrast, VR provides immersive, computer-generated environments that enable interaction with realistic scenarios without real-world risk, making it particularly effective for developing practical skills and decision-making.9 Thus, while gamification focuses on enhancing how learning is experienced, VR emphasises where learning takes place, and their integration offers strong potential to improve overall learning effectiveness.
Gamification and VR have been increasingly used in professional education and training and have been shown to improve learning outcomes, including in emergency and disaster contexts.2,10–12 Various forms of gamification, such as board games, scenario-based simulations, and VR-based games, have been applied to train students, health workers, and disaster response personnel.10,13 Learning outcomes in disaster education include improvements in theoretical knowledge, practical skills, and psychological preparedness, which are essential components of disaster readiness.14 Gamification, defined as the application of game elements in non-game contexts, has been shown to enhance participant engagement, comprehension and retention of learning materials.15 Meanwhile, VR enables participants to experience immersive and realistic simulation environments.16
Empirical evidence supporting the use of gamification and VR in emergency and disaster contexts has grown rapidly over the past decade.10,17–19 Cavalcanti et al20 demonstrated that gamified VR environments can increase user engagement, support experiential learning, and allow participants to explore the consequences of their actions in a safe yet immersive setting, thereby improving understanding and decision-making in high-risk situations.20 Similarly, other studies have shown that gamification elements, such as challenges, rewards, and interactive scenarios, can enhance motivation and knowledge retention, while VR-based simulations provide realistic environments that strengthen practical skills and behavioural responses.21,22 A study among nursing students showed that participants who used VR had better knowledge retention than those who only took web-based modules.17 Furthermore, immersive and simulation-based learning approaches have been found to improve not only cognitive outcomes but also users’ confidence and preparedness in handling emergencies.
Despite this expanding evidence base, several important gaps remain. Previous studies have largely examined gamification and VR separately, with limited comparative analysis across cognitive, psychomotor, and affective domains.10 In addition, previous reviews focus on describing intervention features and outcomes without adequately addressing the underlying theoretical mechanisms, such as immersion, presence, and motivation.23 There is no existing review that systematically integrates and compares gamification and VR within a unified framework across cognitive, psychomotor, and affective learning domains, particularly in disaster preparedness training for both students and health workers. Therefore, this scoping review aims to systematically map and synthesise the available evidence on gamification and VR-based interventions in enhancing disaster preparedness training among university students and health workers, while providing a more integrated understanding of their roles in improving learning outcomes.
Materials and Methods
Study Design
This study uses a scoping review design, guided by the Arksey and O’Malley framework,24 to map the scientific evidence broadly related to a particular topic and to identify research characteristics, intervention types, and remaining gaps in the evidence. The scoping review was chosen because the topic of using gamification and VR in disaster preparedness has a variety of interventions, simulation contexts, and diverse learning outcomes.
Eligibility Criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension (PRISMA) framework was used in this literature review to assess the efficacy of gamification and virtual reality in disaster training (see Figure 1).25 Research questions and eligibility criteria for research articles using the PICO approach (Population, Intervention, Comparison, Outcome).
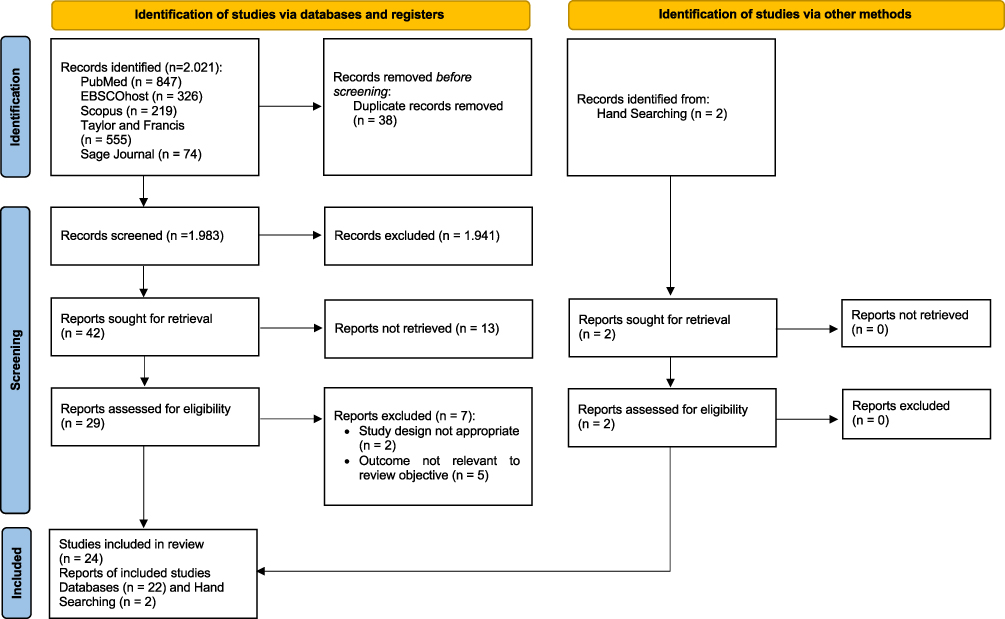 |
Figure 1 PRISMA Flow Diagram adapted from Page MJ, McKenzie JE, Bossuyt PMet al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.25 |
P (Population): University students and Health workers
I (Intervention): Gamification and Virtual Reality
C (Comparison): Usual methods or traditional methods
O (Outcome): Learning outcome (cognitive, psychomotor, and affective aspects).
In this review, articles not published in English and classified as secondary research were excluded. Only original research articles were included. Full-text availability was required for data extraction and analysis. To minimise potential bias related to access limitations, multiple retrieval strategies were undertaken, including searching across different databases, screening reference lists of relevant studies, and accessing institutional resources. Despite these efforts, some articles could not be retrieved and were therefore excluded. This limitation is acknowledged and may have affected the completeness of the evidence synthesis. Additionally, no restriction was placed on the year of publication to ensure comprehensive coverage of the development of gamification and virtual reality in disaster training, allowing identification of trends and comparison of interventions over time.
Search Strategy
Systematically, literature searches are conducted across five main databases: EBSCOhost, PubMed, Scopus, SAGE Journal, and Taylor & Francis. The keywords used were “(University students OR Student OR Health workers OR Healthcare professionals) AND (Gamification OR Serious games OR Game-based learning AND Virtual reality OR VR simulation OR Immersive learning OR Augmented reality) AND. (Disaster Preparedness OR Disaster Training OR Emergency preparedness OR Learning outcome)”. Each keyword is verified using MeSH (Medical Subject Headings). Synonyms are applied to ensure all relevant articles are captured. In addition, the author uses Boolean operators such as “AND” and “OR” to filter or expand search results based on various word variations.
In addition to database searching, hand searching was also performed to identify potentially eligible studies that may not have been captured through the electronic search strategy. This process included screening the reference lists of included articles and relevant review papers to locate additional studies that matched the eligibility criteria.
Study Selection
The study selection process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines. All identified records were exported and managed using Mendeley Reference Manager, and duplicate records were removed prior to screening. Title and abstract screening were conducted independently by two reviewers (F.S. and EE) based on predefined inclusion and exclusion criteria to identify potentially relevant studies. Articles that met the initial screening criteria were subsequently retrieved for full-text assessment. Full-text screening was also performed independently by the same reviewers to confirm final eligibility. To ensure consistency and minimize selection bias, any discrepancies between reviewers at each stage of the selection process were discussed and resolved through consensus, including consultation with the third and fourth authors via online meetings when necessary. The overall study selection process is presented in the PRISMA flow diagram (Figure 1).
Data Extraction and Analysis
Data were extracted independently by two authors (E.E and F.S) using a standardized extraction table In this review, the extraction table was designed to systematically capture key information from each included study and ensure consistency across the dataset. Extracted variables included study characteristics such as author(s) and year of publication, study design, country, participant characteristics, intervention type, and key findings.
Following extraction, the results were organized and summarized descriptively in tabular form to provide an overview of the evidence base. The analytical process began by identifying patterns across the included studies and comparing findings by intervention category and reported learning outcomes. Subsequently, all authors collaboratively interpreted the extracted evidence and conducted a narrative analysis to synthesize key themes related to intervention characteristics and outcome domains. Finally, the included studies and extracted entries were rechecked to minimise extraction errors and to ensure the accuracy and completeness of the review findings.
Results
Study Selection
The literature search identified a total of 2,021 records across databases, including PubMed (n = 847), EBSCOhost (n = 326), Scopus (n = 219), Taylor & Francis (n = 555), and SAGE Journals (n = 74) (see Figure 1). After removing 38 duplicate records, 1,983 records remained and were screened based on titles and abstracts. During the screening stage, 1,941 records were excluded for failing to meet eligibility criteria, leaving 42 reports for full-text retrieval.
Of the 42 reports sought, 13 full-text articles could not be retrieved, leaving 29 reports to be assessed for eligibility. Following full-text assessment, 7 reports were excluded, including 2 studies with an inappropriate study design and 5 studies with outcomes not relevant to the review objective. As a result, 22 studies were included from the database search. In addition, 2 records were identified through hand searching. Both reports were successfully retrieved and assessed for eligibility, and no studies were excluded at this stage. Therefore, a total of 24 studies were included in the final review, comprising 22 identified through database searches and 2 through hand searching.
Characteristics of Studies
A total of 24 studies were identified in this review with diverse research designs (see Tables 1 and 2). The majority of studies used a quasi-experimental design (n = 10),26–35 followed by a pre-experimental one-group pre–post design (n = 5) and randomised controlled trials (RCTs) (n = 5). Other designs included comparative, crossover, and prospective observational studies (n = 4). The dominance of quasi-experimental designs indicates that research in disaster education and triage still largely focuses on evaluating the effectiveness of interventions in the context of education and training, rather than on rigorous causal tests such as RCTs.36–40
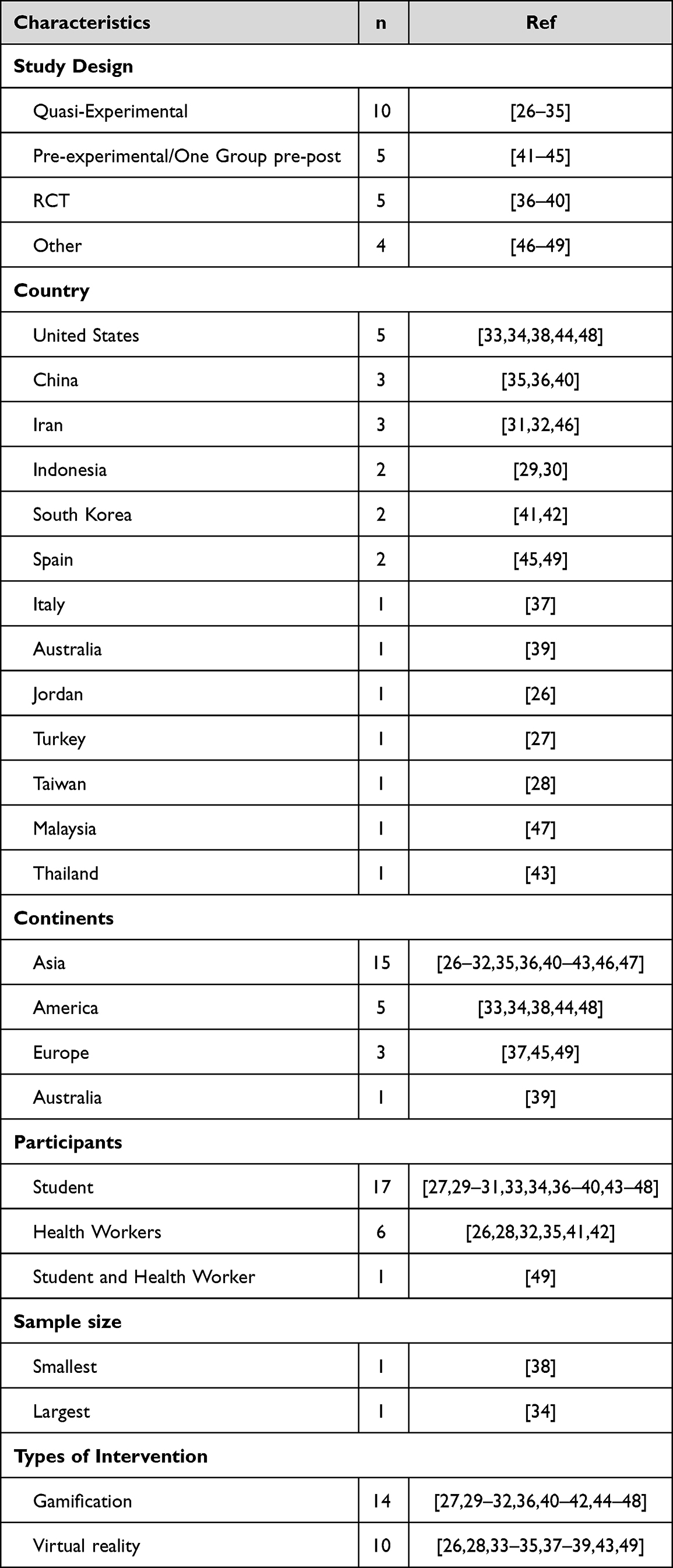 |
Table 1 Summary of Studies |
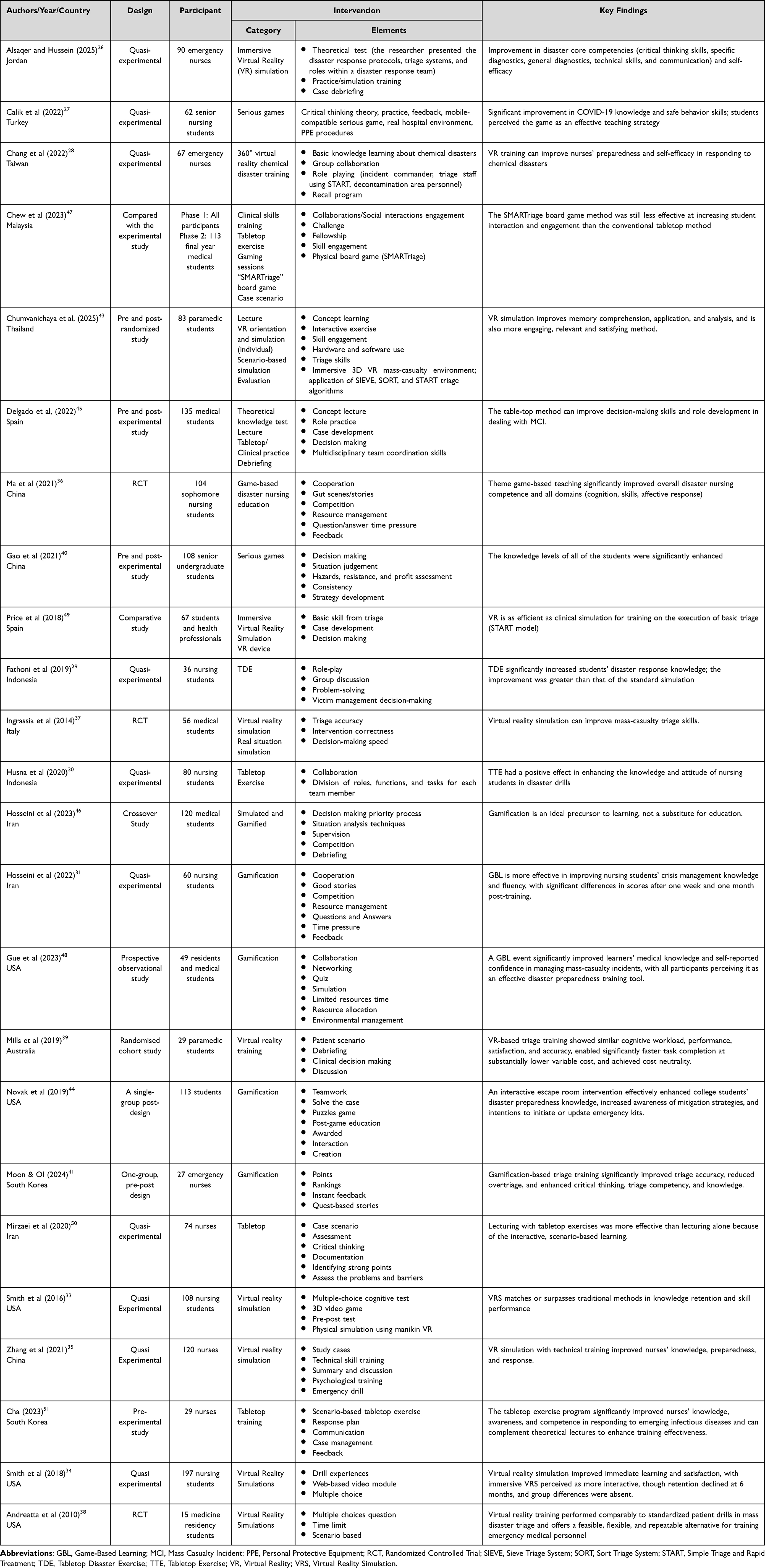 |
Table 2 Characteristics of the Study |
In terms of geographical distribution, most studies (n = 15) originated in Asia, particularly China, Iran, Indonesia, and South Korea.26–32,35,36,40–43,46,47 The Americas region contributed five studies, all from the United States.33,34,38,44,48 This pattern shows that gamification and virtual reality (VR)-based learning innovations in disaster preparedness are being explored more in Asian countries (see Table 1).
Characteristics of Participants
The majority of study participants were students (n = 17), primarily nursing and medical students.27,29–31,33,34,36–40,43–48 Healthcare professionals, primarily nurses and emergency nurses, were involved in six studies,26,28,32,35,41,42 while one study involved a combination of students and healthcare workers.49 Sample sizes range widely, from small-scale studies with fewer than 30 participants to studies with nearly 197 respondents.34 This variability reflects differences in educational context, technology availability, and the goals of intervention evaluation in each study (see Table 2).
Characteristics of Intervention
In this review, interventions are divided into two categories, namely gamification and virtual reality-based interventions (see Figure 2 and Table 3).
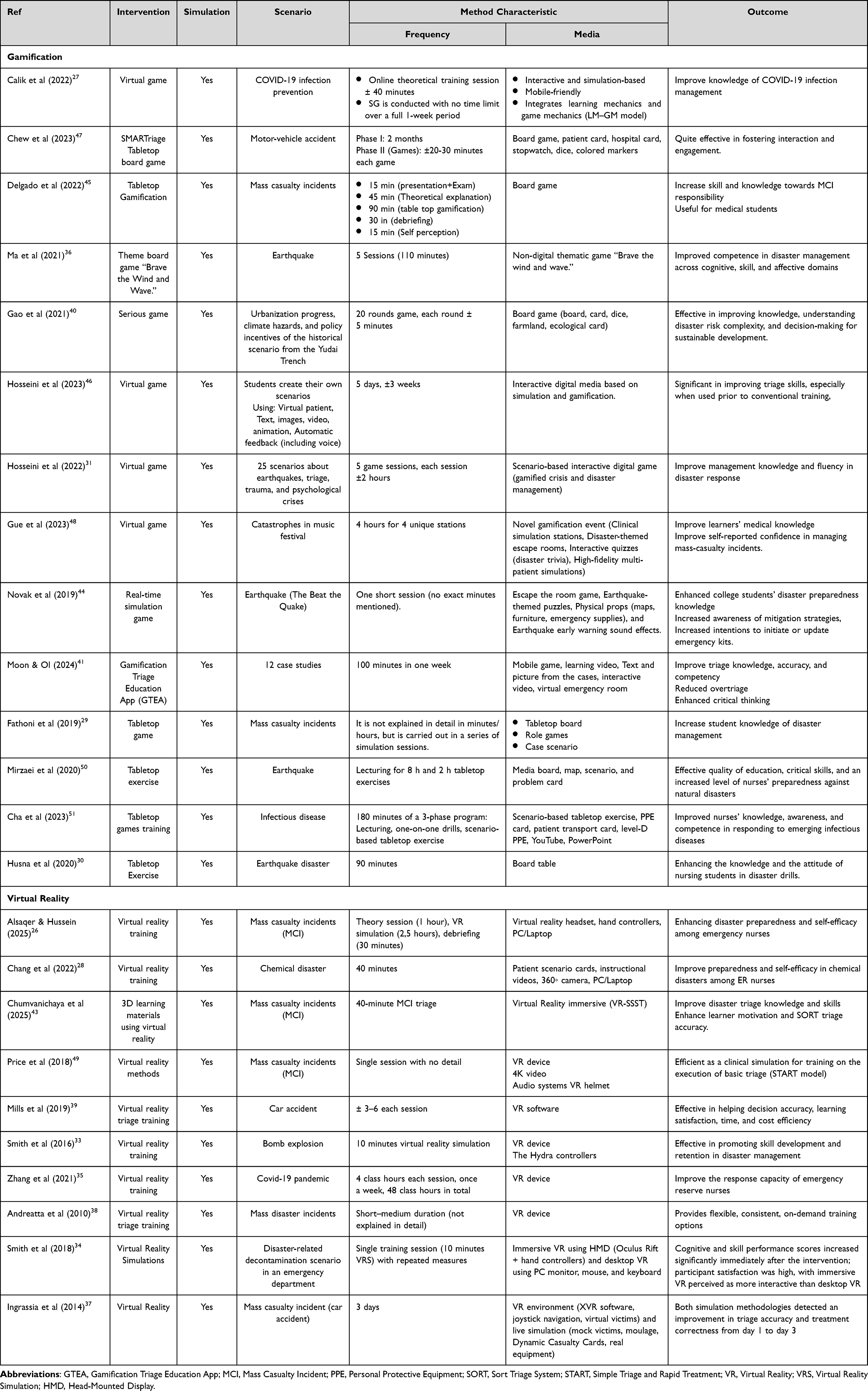 |
Table 3 Characteristics of Gamification and Virtual Reality |
 |
Figure 2 Categorization of Intervention. |
Category I: Gamification-Based Intervention
Gamification-based interventions are implemented through a variety of educational formats, including serious digital simulation games, mobile apps, board and tabletop games, and escape room-based activities.27,36,44,45,47 This intervention is consistently designed with a scenario-based learning approach, where participants are involved in structured disaster cases such as mass casualty incidents, earthquakes, infectious disease outbreaks, including COVID-19, traffic accidents, and disasters at large-scale public events.26,41,43,45,48 In some studies, scenarios are structured into multiple rounds, levels, or stations to allow for repeated practice of decision-making in a variety of contexts.31,36,46
Instructional design in gamification interventions emphasizes game mechanics as a core component, such as points, scoring systems, rankings or leaderboards, rewards, competition, and time pressure.27,36,41 These mechanisms are often combined with resource constraints, requiring participants to prioritize patients, allocate limited resources, and manage competing demands in a simulated emergency. Furthermore, many studies also integrate team-based games that involve collaboration, role-playing, participant discussion, and both cooperative and competitive social interaction.44,47,48
Learning activities in gamification interventions typically require participants to perform decision-making and problem-solving tasks, such as triage prioritization, situational assessment, and strategic planning.40,41,45 Feedback mechanisms are an integral part of most interventions and are provided through direct in-game feedback, quizzes, post-game summaries, and structured debriefing sessions.31,36,46 Several studies also emphasized the repeatability and flexibility of interventions through the use of multiple scenarios, repeated sessions, or participant-designed scenarios, allowing for reinforcement of learning and adaptation to different educational goals.
Category II: Virtual Reality
VR are generally implemented as immersive simulation-based training using head-mounted displays, 360-degree videos, or fully interactive three-dimensional virtual environments.26,33,34,38 This intervention reconstructs realistic disaster and emergency environments, including mass casualty incidents, chemical disasters, trauma events such as motor vehicle accidents and bomb explosions, infectious disease scenarios including COVID-19, and decontamination processes in emergency departments.28,33–35,37
Most VR interventions follow a structured training sequence, starting with an orientation or case debriefing, followed by a discussion and a recall program, to familiarize participants with the VR hardware and software interface and the learning objectives.26,28,33,39,43 This stage is followed by an immersive simulation or role-play simulation phase, where participants actively interact with the virtual environment.26,28,33,37,43,49 In this phase, participants perform a variety of clinical and disaster response tasks, including victim assessment, triage using standard algorithms such as START, SORT, and SIEVE, navigation at the disaster site, and assuming specific roles as part of the response team.
VR interventions also often integrate objective performance measurements, with systems that track indicators such as triage accuracy, decision-making accuracy, intervention accuracy, decision-making speed, and task completion time.35,37,39,43,49 This data was used to support individual and group feedback. Nearly all studies included a post-simulation debriefing component, either through an automated system or an instructor-led discussion, allowing participants to reflect on their actions, decision-making processes, and overall performance. VR is a flexible, repeatable, and appropriate training modality for customized use in disaster education.
Characteristics of Outcomes
Across the included studies, outcomes of disaster education interventions were consistently reported in three main domains: cognitive, psychomotor, and affective. These domains were observed in both gamification-based interventions and virtual reality (VR)-based interventions, although the specific outcome indicators varied according to the instructional approach used.
Category I: Cognitive Outcomes
Cognitive outcomes primarily reflected improvements in knowledge acquisition and higher-order cognitive processes. In gamification-based interventions, cognitive outcomes encompassed COVID-19 knowledge,27 disaster preparedness knowledge,44 disaster response knowledge,29,45 knowledge of disaster management,30,31 crisis management knowledge and fluency,31 triage knowledge and accuracy,41 and understanding of disaster risk complexity.40 In addition, in VR-based interventions, cognitive outcomes included theoretical test performance, disaster core competencies,26 capability in memory comprehension,43 basic knowledge acquisition related to chemical disasters, application, and analysis abilities, knowledge retention, cognitive performance scores, and response capacity in disaster situations.26,28,33–35,43
Category II: Psychomotor Outcomes
Psychomotor outcomes focused on the development of practical skills and performance in disaster response and triage. Gamification interventions reported psychomotor outcomes, including skills for MCI response, triage skills, triage accuracy, triage competency, reduced overtriage, and critical thinking as a performance-related competency in triage decision-making.36,41,45,46 In VR-based interventions, reported psychomotor outcomes included triage skills, SORT and START triage accuracy, execution of basic triage procedures, decision accuracy, intervention correctness, decision-making speed, technical skill training, skill performance scores, and improvements in triage accuracy and treatment correctness.33–35,37,39,43,49 These outcomes were commonly embedded within scenario-based gameplay requiring active task execution.
Category III: Affective Outcomes
Affective outcomes captured learners’ attitudes, motivation, confidence, and perceived readiness to respond to disasters. In gamification-based interventions, reported affective outcomes include self-reported confidence, interaction engagement, enjoyment or fun activity, perceived effectiveness of the teaching strategy, disaster preparedness as an attitude, awareness of mitigation strategies, intention to initiate or update emergency kits, learner motivation, satisfaction, and perceived interactivity.27,36,44,47,48 Similarly, in VR-based interventions, affective outcomes included disaster preparedness, self-efficacy, self-preparedness, learner motivation, satisfaction, perceived interactivity, and perceived feasibility or flexibility of VR as an on-demand training modality.26,28,34,38,39,43
Discussion
This scoping review identified and synthesized the evidence on the effectiveness of gamification and virtual reality (VR) in improving learning outcomes in disaster training among university students and health workers. The included interventions were grouped into two categories, namely gamification-based interventions (n = 14) and VR-based interventions (n = 10), and the learning outcomes were consistently reported across three domains: cognitive, psychomotor, and affective. This pattern demonstrates that the effectiveness of these approaches extends beyond knowledge acquisition to include practical skills and attitudinal readiness, and the pattern is consistent in both students and health workers.
Compared to previous reviews, this review is novel in integrating two strategic approaches (gamification and VR) into a single evidence map, thereby providing a more complete picture of disaster preparedness education strategies. Bai et al’s (2024) review examined gamification in disaster education. It confirmed its benefits on engagement and learning, but did not position VR as a primary intervention category for parallel analysis, and the number of studies was limited.10 In addition, previous reviews of the studies analyzed were quite limited, and almost all of them were conducted in Asian countries.52,53 Magi et al (2023), in contrast, focused on VR and augmented reality in disaster medicine but did not address non-VR innovations such as tabletop exercises or escape rooms.23 By including 24 studies across four continents and extending beyond earlier reviews that contained 16 or fewer studies,10,52 this review broadens the geographic and populational coverage, with participants ranging from undergraduate students to emergency nurses working in clinical settings.26,28,32,35 The contribution of this review therefore lies less in the number of studies added than in providing a more operational interpretive framework for designing disaster education and training across the cognitive, psychomotor, and affective domains.
Disaster preparedness is an important competency for health students and health workers because both play a role as candidates or implementers of initial responses in crisis conditions.53,54 Low preparedness can lead to triage delays, prioritization errors, and decreased action accuracy, especially in MCI situations that require rapid decisions and team coordination.55 The findings of this review suggest that preparedness training can be strengthened through strategies that keep participants actively thinking and acting within realistic scenarios rather than passively receiving material. In the context of services, increasing competence and self-efficacy is also relevant because it influences health workers’ readiness to act during disaster events.26,28 Both gamification and VR operationalize this cycle: learners engage with structured scenarios, receive feedback, conceptualize rules of action, and re-apply them in subsequent rounds or cases, which plausibly explains the consistent improvements observed across cognitive, psychomotor, and affective outcomes.56,57
Within the gamification category, improvements were most visible in the cognitive and affective domains across digital games, serious games, tabletop exercises, and escape rooms.27,31,40,46 A plausible mechanism for these effects is provided by Self-Determination Theory (SDT), which argues that intrinsic motivation is strengthened when learning environments satisfy learners’ needs for competence, autonomy, and relatedness.10,58 Game mechanics such as points, leaderboards, immediate feedback, and progressive challenges support perceived competence; choice of strategy and path within scenarios supports autonomy; and cooperative or competitive team play supports relatedness.58,59 This motivational base helps explain why gamification consistently improved engagement, self-reported confidence, triage competency, and knowledge retention in the included studies,41,45,48 even though several approaches used low-cost, non-digital formats. Gamification is also attractive operationally because it is relatively flexible and scalable, adapting to institutions with limited simulation infrastructure.10,52 Nevertheless, when gamified designs over-emphasize play without structured reflection and debriefing, transfer to real-world decision-making can remain superficial, highlighting the importance of skilled facilitation and explicit alignment between game elements and learning objectives.53
Within the VR category, the most consistent gains were observed in the combined cognitive and psychomotor domains, particularly where training required high realism, role performance, and measurable action accuracy37,39,49 Immersive environments are well-suited to psychomotor learning because they afford repeated rehearsal of procedures under realistic sensory conditions, without the physical or clinical risks associated with real MCI, chemical exposure, or decontamination settings.28,34 From an experiential-learning perspective, VR provides a concrete experience that is sufficiently close to the real clinical environment to support transfer, while also allowing structured debriefing for reflection.57 Cognitive Load Theory provides a complementary mechanism: by integrating visual, auditory, and procedural information within the simulated task, VR can either distribute cognitive load effectively or, if poorly designed, exceed working-memory capacity and impede retention.60,61 This may explain why some VR studies in this review showed strong immediate effects on triage accuracy and decision speed but attenuated retention at six months,34 and why structured pre-briefings and instructor-led debriefings appear to be important design features in the included studies. In practical terms, VR also allows objective performance tracking of triage accuracy, intervention correctness, and task completion time that is difficult to replicate with conventional simulation.35,39
Taken together, the three outcome domains correspond to the pedagogical goals of ensuring that learners “know” (cognitive), “can do” (psychomotor), and “feel ready and confident” (affective) in disaster response.26,36 Cognitive outcomes were prominent across studies that addressed disaster management knowledge, triage knowledge, and understanding of disaster risk complexity.27,31,40,41 Psychomotor outcomes were most visible in MCI and trauma-oriented studies that demanded precision in action, such as triage accuracy, intervention correctness, and decision-making speed.37,39,45,49 Affective outcomes including self-efficacy, preparedness attitudes, motivation, and perceived interactivity were reported across both gamification and VR studies.26,28,47,48 This tri-domain pattern strengthens the argument that effective disaster education cannot rely on knowledge transmission alone but must deliberately target all three domains simultaneously.
Several considerations influence how these findings should be interpreted. The evidence base is dominated by quasi-experimental designs, with relatively few randomized controlled trials, which limits causal inference about the comparative superiority of gamification or VR over conventional training.26–28 Outcome measures varied considerably across studies, with most relying on short-term knowledge quizzes, locally developed checklists, or self-reported confidence rather than validated, disaster-specific instruments; this variability limits cross-study comparison and is consistent with a broader pattern in disaster-medicine education research.62 Differences in intervention duration, training intensity, and scenario complexity likely contributed to the heterogeneity of effect sizes, particularly for performance-based outcomes such as triage accuracy and decision speed.
Geographically, most included studies were conducted in Asia and the United States, which may restrict generalizability to settings with different educational systems, technological infrastructure, or disaster profiles. In addition, several studies suggested that learning gains may attenuate over time, underscoring the need for longer follow-up to judge retention and real-world transfer. Finally, some disaster types in particular chemical, biological, radiological, and nuclear events, as well as conflict-related and displacement scenarios remain underrepresented in this literature despite documented deficits in health workers’ preparedness for such events.63,64 These observations should be read as boundary conditions on the evidence rather than as reasons to discount the consistent positive effects observed.
Implication for Practice
Practically, these findings offer several concrete recommendations for educators and healthcare institutions. First, the choice between gamification and VR should be guided by learning goals and available resources rather than technological novelty alone. Institutions with limited infrastructure or a strong need for scalable, low-cost training, for example, undergraduate nursing programs or hospitals in low-resource settings, can prioritise gamification approaches such as tabletop exercises, board games, and mobile serious games, which have demonstrated meaningful gains in cognitive and affective outcomes. Second, institutions targeting psychomotor precision in high-risk tasks, such as MCI triage, chemical decontamination, or trauma management, should consider VR-based simulation when feasible, as immersive environments enable safe, repeatable practice of clinically relevant actions. Third, a blended design that uses gamification as a motivational entry point and VR as a rehearsal platform, bridged by structured debriefing, is consistent with the evidence from experiential learning and may maximise outcomes across all three domains. Finally, curriculum planners should pair any such technology with explicit competency frameworks and validated assessment tools to ensure that learning gains translate to clinical practice rather than remaining at the level of self-reported confidence.
Conclusions
The findings in this scoping review indicate that VR and gamification have different but complementary roles in improving learning outcomes. VR tends to be more effective in improving psychomotor skills and practical experience due to its ability to simulate real situations in an immersive manner. Meanwhile, gamification plays a greater role in increasing motivation, engagement, and cognitive aspects through game elements such as rewards, challenges, and feedback. This difference indicates that the effectiveness of the intervention is highly dependent on the learning objectives to be achieved. However, the variety of study designs, intervention methods, and measurement tools used indicates significant heterogeneity, limiting the generalizability of the findings. In addition, most studies still focus on short-term results and have not explored long-term impacts much. Therefore, further research with more robust designs and more consistent outcome standards is needed. Overall, the combination of VR and gamification has the potential to be a more optimal, innovative approach in supporting the learning process, especially in the context of simulation-based training and skills development.
Abbreviations
GBL, Game-Based Learning; MCI Mass Casualty Incident; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses PRISMA-ScR; RCT– Randomized Controlled Trial; SDT-Self-Determination Theory; SORT, Simple Triage and Rapid Treatment; START, Simple Triage and Rapid Treatment; TDE, Tabletop Disaster Exercise; VR, Virtual Reality.
Acknowledgments
All authors thank Universitas Padjadjaran, Bandung, West Java, Indonesia, for facilitating the database for us in this study. This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this research.
References
1. World Health Organization. Strengthening health emergency preparedness for disasters resulting from natural hazards. In: Seventy-Seventh World Health Assembly. 2024:1–19.
2. Lin CH, Tzeng WC, Chiang LC, Lu MC, Lee MS, Chiang SL. Effectiveness of a structured disaster management training program on nurses’ disaster readiness for response to emergencies and disasters: a randomized controlled trial. J Nurs Manag. 2024;2024. doi:10.1155/2024/5551894
3. Bai S, Zeng H, Zhong Q, Shen Y, Cao L, He M. Application of gamification teaching in disaster education: scoping review. JMIR Serious Games. 2024;12:e64939–e64939.
4. Sermet Y, Demir I. Flood action VR: a virtual reality framework for disaster awareness and emergency response training. In: ACM SIGGRAPH 2019 Posters, SIGGRAPH 2019. 2019.
5. Molka-Danielsen J, Prasolova-Forland E, Fominykh M, Lamb K. Use of a collaborative virtual reality simulation for multi-professional training in emergency management communications. In:
6. Shirani Bidabadi N, Nasr Isfahani A, Rouhollahi A, Khalili R. Effective teaching methods in higher education: requirements and barriers. J Adv Med Educ Prof. 2016;4(4):170–178.
7. Thelma CC, Sain ZH, Banda E, Phiri EV. International Journal of Research (IJR) barriers to effective research methodology training for undergraduate and postgraduate students: a case of selected higher learning institutions in Lusaka District, Zambia. Int J Res. 2025;12(02).
8. Deterding S, Dixon D, Khaled R, Nacke L. From game design elements to gamefulness: defining “gamification”. In:
9. Makransky G, Petersen GB. The cognitive affective model of immersive learning (CAMIL): a theoretical research-based model of learning in immersive virtual reality. Educ Psychol Rev. 2021;33(3):937–958. doi:10.1007/s10648-020-09586-2
10. Bai S, Zeng H, Zhong Q, Shen Y, Cao L, He M. Application of gamification teaching in disaster education: scoping review. JMIR Serious Games. 2024;12(e64939):1–11.
11. Mansoory MS, Khazaei MR, Azizi SM, Niromand E. Comparison of the effectiveness of lecture instruction and virtual reality-based serious gaming instruction on the medical students’ learning outcome about approach to coma. BMC Med Educ. 2021;21(1):1–8. doi:10.1186/s12909-021-02771-z
12. Ulmer J, Braun S, Cheng CT, Dowey S, Wollert J. Gamification of virtual reality assembly training: effects of a combined point and level system on motivation and training results. Int J Hum Comput Stud. 2022;165(May):102854. doi:10.1016/j.ijhcs.2022.102854
13. Arinta RR, Emanuel AWR, Suyoto S. Effectiveness of gamification for flood emergency planning in the disaster risk reduction area. Int J Eng Pedagog. 2020;10(4):108–124. doi:10.3991/ijep.v10i4.13145
14. Wilson LO. Blooms taxonomy revised - understanding the new version of bloom’s taxonomy. a taxon learn teaching, assess a revis bloom taxon educ object. Second Principle. 2016;1(1):1–8.
15. Hew KF, Huang B, Chu KWS, Chiu DKW. Engaging Asian students through game mechanics: findings from two experiment studies. Comput Educ. 2016;92–93:221–236. doi:10.1016/j.compedu.2015.10.010
16. Makransky G, Lilleholt L. A structural equation modeling investigation of the emotional value of immersive virtual reality in education. Educ Technol Res Dev. 2018;66(5):1141–1164. doi:10.1007/s11423-018-9581-2
17. Farra S, Miller E, Timm N, Schafer J. Improved training for disasters using 3-D virtual reality simulation. West J Nurs Res. 2013;35:655–671. doi:10.1177/0193945912471735
18. Farra S, Hodgson E, Miller E, et al. Effects of virtual reality simulation on worker emergency evacuation of neonates. Disaster Med Public Health Prep. 2018;13:301–308. doi:10.1017/dmp.2018.58
19. Farra S, Miller E, Hodgson E. Virtual reality disaster training: translation to practice. Nurse Educ Pract. 2015;15(1):53–57. doi:10.1016/j.nepr.2013.08.017
20. Cavalcanti J, Valls V, Contero M, Fonseca D. Gamification and hazard communication in virtual reality: a qualitative study. Sensors. 2021;21(14):4663. doi:10.3390/s21144663
21. Dincelli E. Presence by design: a multi-method examination of design considerations for immersive virtual reality in corporate training. Int J Inf Manage. 2026;87:102999. doi:10.1016/j.ijinfomgt.2025.102999
22. Lampropoulos G, Kinshuk. Virtual Reality and Gamification in Education: A Systematic Review. Vol. 72. Educational Technology Research and Development. Springer US; 2024:1691–1785.
23. Magi CE, Bambi S, Iovino P, et al. Virtual reality and augmented reality training in disaster medicine courses for students in nursing: a scoping review of adoptable tools. Behav Sci. 2023;13(616):1–13. doi:10.3390/bs13070616
24. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8(1):19–32. doi:10.1080/1364557032000119616
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
26. Alsaqer K, Hussein S. Impact of virtual reality training on nurses ‘preparedness and self-efficacy in emergencies and disasters: a quasi-experimental study. Int Emerg Nurs. 2025;82(June):101662. doi:10.1016/j.ienj.2025.101662
27. Calik A, Cakmak B, Kapucu S, Inkaya B. The effectiveness of serious games designed for infection prevention and promotion of safe behaviors of senior nursing students during the COVID- 19 pandemic. Am J Infect Control. 2022; 50:1360–1367.
28. Chang CW, Lin CW, Huang CY, Hsu CW, Sung HY, Cheng S-F. Effectiveness of the virtual reality chemical disaster training program in emergency nurses: a quasi experimental study. Nurse Educ Today. 2022;119(October):105613. doi:10.1016/j.nedt.2022.105613
29. Fathoni M, Yueniwati Prabowowati Wadjib Y, Addiarto W. The effect of learning Tabletop Disaster Exercise (TDE) to improve knowledge among nursing students for disaster emergency response. Res J Life Sci. 2019;6(1):29–35. doi:10.21776/ub.rjls.2019.006.01.4
30. Husna C, Kamil H, Yahya M, Tahlil T, Darmawati D. Does tabletop exercise enhance knowledge and attitude in preparing disaster drills? Nurse Media J Nurs. 2020;10(2):182–190. doi:10.14710/nmjn.v10i2.29117
31. Hosseini MM, Hosseini TM, Qayumi K, Baeradeh N. Game-based vs. case-based training for increasing knowledge and behavioral fluency of nurse students regarding crisis and disaster management; a quasi- experimental study. Arch Academic Emerg Med. 2022;10(1):1–10.
32. Mirzaei S, Eftekhari A, Mohammadinia L, Dehghani Tafti AA, Norouzinia R, Nasiriani K. Comparison of the effect of lecturing and tabletop exercise methods on level of preparedness of nurses against natural disasters. J Holist Nurs Midwifery. 2020;30(1):17–26. doi:10.32598/JHNM.30.1.3
33. Smith SJ, Farra S, Ulrich DL, Hodgson E, Nicely S, Matcham W. Learning and retention using virtual reality in a decontamination simulation. Nurs Educ Perspect. 2016;37(4):210–214. doi:10.1097/01.NEP.0000000000000035
34. Smith SJ, Farra SL, Ulrich DL, Hodgson E, Nicely S, Mickle A. Effectiveness of two varying levels of virtual reality simulation. Nurs Educ Perspect. 2018;39:10–15. doi:10.1097/01.NEP.0000000000000369
35. Zhang D, Liao H, Jia Y, et al. Effect of virtual reality simulation training on the response capability of public health emergency reserve nurses in China: a quasiexperimental study. BMJ Open. 2021;11:1–9.
36. Ma D, Shi Y, Zhang G, Zhang J. Does theme game-based teaching promote better learning about disaster nursing than scenario simulation: a randomized controlled trial. Nurse Educ Today. 2021;103(April):104923. doi:10.1016/j.nedt.2021.104923
37. Ingrassia PL, Ragazzoni L, Carenzo L, Colombo D, Gallardo AR, Della CF. Virtual reality and live simulation : a comparison between two simulation tools for assessing mass casualty triage skills. Eur J Emerg Med. 2014;29–31.
38. Andreatta PB, Maslowski E, Petty S, et al. Virtual reality triage training provides a. Sci Simul Emerg Med. 2010;17(8):870–876.
39. Mills B, Dykstra P, Hansen S, et al. Virtual reality triage training can provide comparable simulation efficacy for paramedicine students compared to live simulation-based scenarios. Prehospital Emerg Care. 2019;1545–1566.
40. Gao W, Guo Y, Jiang F. Playing for a resilient future: a serious game designed to explore and understand the complexity of the interaction among climate change, disaster risk, and urban development. Int J Environ Res Public Heal. 2021;18:8949. doi:10.3390/ijerph18178949
41. Moon S-H, Kim SO. Enhancing triage accuracy in emergency nurses: the impact of a game-based triage educational app. Int Emerg Nurs. 2024;72:101398. doi:10.1016/j.ienj.2023.101398
42. Cha KS, Lee K. Effect of a tabletop program for training emerging infectious disease responses in nurses at small- to medium-sized hospitals in areas with poor healthcare access. Healthc. 2023;11(17):2370. doi:10.3390/healthcare11172370
43. Chumvanichaya K, Yuksen C, Nuanprom P, Aramvanitch K. A comparison of SIEVE, SORT, and START triage training effectiveness between immersive interactive 3D learning materials using virtual reality (VR-SSST) and traditional methods in mass casualty incidents. Int J Emerg Med. 2025;18(55):1–12. doi:10.1186/s12245-025-00850-2
44. Novak J, Lozos JC, Spear SE. Development of an interactive escape room intervention to educate college students about earthquake preparedness. Nat Hazards Rev. 2019;20(1):1–5. doi:10.1061/(ASCE)NH.1527-6996.0000322
45. Delgado RC, García LF, Cernuda JA, Álvarez TC, González PA. Training of medical students for mass casualty incidents using table-top gamification. Disaster Med Public Health Prep. 2022;21(17):e255.
46. Hosseini MM, Toktam S, Hosseini M, Qayumi K. Crossover design in triage education: the effectiveness of simulated interactive vs. routine training on student nurses ‘performance in a disaster situation. BMC Res Notes. 2023;16(313):1–13. doi:10.1186/s13104-023-06596-5
47. Chew KS, Siew S, Wong L, Safiah I, Koh JW, Wan Allam SASB. Tutorless board game as an alternative to tabletop exercise for disaster response training: perception of interaction engagement and behavioral intention. BMC Med Educ. 2023;23(432):1–8. doi:10.1186/s12909-023-04356-4
48. Gue S, Cohen S, Tassone M, et al. Disaster day: a simulation ‑ based competition for educating emergency medicine residents and medical students on disaster medicine. Int J Emerg Med. 2023;1:1–7. doi:10.1186/s12245-023-00520-1
49. Price F, Tortosa E, Antonio NFP, et al. Comparative study of a simulated incident with multiple victims and immersive virtual reality. Nurse Educ Today. 2018;71(April):48–53. doi:10.1016/j.nedt.2018.09.006
50. Mirzaei S, Eftekhari A, Mohammadinia L, Tafti AAD, Norouzinia R, Nasiriani K. Comparison of the effect of lecturing and tabletop exercise methods on level of preparedness of nurses against natural disasters. J Holist Nurs Midwifery. 2020;30(1):17–26.
51. Sook CK. Effect of a tabletop program for training emerging infectious disease responses in nurses at small- to medium-sized hospitals in areas with poor healthcare access. Healthcare. 2023;11(2370).
52. Bai S, Zeng H, Zhong Q, Cao L, He M, He M. Effectiveness of gamified teaching in disaster nursing education for health care workers: systematic review. J Med Internet Res Rev. 2025;27(e74955):1–14. doi:10.2196/74955
53. Emaliyawati E, Ibrahim K, Trisyani Y, et al. Tabletop disaster exercises: a scoping review of benefits for health workers and students enhancing disaster preparedness through tabletop disaster exercises: a scoping review of benefits for health workers and students. Adv Med Educ Pract ISSN. 2025;(16):1–11.
54. AlOtaibi SS, Almutairi HA, Alotaibi MK, Alharbi K, Bahari G. Enhancing nurses’ disaster management and preparedness: evaluating the effectiveness of an online educational program through a quasi-experimental study. Risk Manag Healthc Policy. 2024;17:101–111. doi:10.2147/RMHP.S446704
55. Tankel J, Einav S. Preparing for mass casualty events despite COVID-19. British J Anaesthesia Eng. 2022;128:e104–8. doi:10.1016/j.bja.2021.11.012
56. Hur HK, Kim J, Jung JS. Enhancing nursing team communication and collaboration: impact of immersive virtual reality simulation on nursing students. Clin Simul Nurs. 2025;102:101685. doi:10.1016/j.ecns.2025.101685
57. Chan AWK, Chair SY, Sit JWH, Wong EML, Lee DTF, Fung OWM. Case-Based web learning versus face-to-face learning: a mixed-method study on university nursing students. J Nurs Res. 2016;24(1):31–40. doi:10.1097/jnr.0000000000000104
58. Oliveira W, Hamari J, Shi L, et al. Tailored Gamification in Education: A Literature Review and Future Agenda [Internet]. Vol. 28. Education and Information Technologies. Springer US; 2023:373–406. doi: 10.1007/s10639-022-11122-4
59. Min S, Atan NA, Habibi A. Gamification with self-determination theory to foster intercultural communicative competence and intrinsic motivation. Int J Eval Res Educ. 2025;14(3):1985–1994. doi:10.11591/ijere.v14i3.29858
60. Andersen SAW, Mikkelsen PT, Konge L, Cayé-Thomasen P, Sørensen MS. The effect of implementing cognitive load theory-based design principles in virtual reality simulation training of surgical skills: a randomized controlled trial. In: Adv Simul. 1. (London, England); 2016:20.
61. Juliano JM, Schweighofer N, Liew SL. Increased cognitive load in immersive virtual reality during visuomotor adaptation is associated with decreased long-term retention and context transfer. J Neuroeng Rehabil. 2022;19(1):106. doi:10.1186/s12984-022-01084-6
62. García Ulerio J, Al Khatib M, Aammar B, Ragazzoni L, Barone-Adesi F, Caviglia M. Simulation technology use in disaster medicine education and training: a scoping review. Front Disaster Emerg Med. 2025;2025.
63. Qzih ES, Ahmad MM. Hospital-Based preparedness measures for CBRNE disasters: a systematic review. Environ Health Insights. 2024;18:11786302241288860. doi:10.1177/11786302241288859
64. Kako M, Hammad K, Mitani S, Arbon P. Existing Approaches to Chemical, Biological, Radiological, and Nuclear (CBRN) education and training for health professionals: findings from an integrative literature review. Prehosp Disaster Med. 2018;33(2):182–190. doi:10.1017/S1049023X18000043
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Enhancing Disaster Preparedness Through Tabletop Disaster Exercises: A Scoping Review of Benefits for Health Workers and Students
Emaliyawati E, Ibrahim K, Trisyani Y, Nuraeni A, Sugiharto F, Miladi QN, Abdillah H, Christina M, Setiawan DR, Sutini T
Advances in Medical Education and Practice 2025, 16:1-11
Published Date: 8 January 2025
Gamification-Based Interventions in Chronic Disease Care: A Systematic Review of Randomised Controlled Trials
Emaliyawati E, Ibrahim K, Kurniawan T, Fitria N, Songwathana P
Risk Management and Healthcare Policy 2025, 18:3921-3936
Published Date: 18 December 2025