Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Functional Predictors Discriminating Asthma–COPD Overlap (ACO) from Chronic Obstructive Pulmonary Disease (COPD)
Authors Kraemer R ![]() , Gardin F, Smith HJ, Baty F
, Gardin F, Smith HJ, Baty F ![]() , Barandun J, Piecyk A, Minder S, Salomon J, Frey M
, Barandun J, Piecyk A, Minder S, Salomon J, Frey M ![]() , Brutsche MH
, Brutsche MH ![]() , Matthys H
, Matthys H
Received 19 July 2022
Accepted for publication 11 October 2022
Published 21 October 2022 Volume 2022:17 Pages 2723—2743
DOI https://doi.org/10.2147/COPD.S382761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Richard Kraemer,1,2,* Fabian Gardin,3,* Hans-Jürgen Smith,4 Florent Baty,5 Jürg Barandun,3 Andreas Piecyk,3 Stefan Minder,1 Jörg Salomon,1 Martin Frey,6 Martin H Brutsche,5 Heinrich Matthys7
1Centre of Pulmonary Medicine, Hirslanden Private Hospital Group, Salem-Hospital, Bern, Switzerland; 2Center for Translational Medicine and Biomedical Entrepreneurship, University of Bern, Bern, Switzerland; 3Centre of Pulmonary Medicine, Hirslanden Private Hospital Group, Clinic Hirslanden, Zürich, Switzerland; 4Medical Development, Research in Respiratory Diagnostics, Berlin, Germany; 5Department of Pneumology, Cantonal Hospital St, Gallen, Switzerland; 6Department of Pneumology, Barmelweid Hospital, Barmelweid, Switzerland; 7Department of Pneumology, University Hospital of Freiburg, Freiburg, Germany
*These authors contributed equally to this work
Correspondence: Richard Kraemer, Center of Pulmonary Medicine, Hirslanden Private Hospital Group, Schänzlistrasse 39, Berne, CH-3013, Switzerland, Tel +41 79 300 26 53, Email [email protected]
Background: A significant proportion of patients with obstructive lung disease have clinical and functional features of both asthma and chronic obstructive pulmonary disease (COPD), referred to as the asthma–COPD overlap (ACO). The distinction of these phenotypes, however, is not yet well-established due to the lack of defining clinical and/or functional criteria. The aim of our investigations was to assess the discriminating power of various lung function parameters on the assessment of ACO.
Methods: From databases of 4 pulmonary centers, a total of 540 patients (231 males, 309 females), including 372 patients with asthma, 77 patients with ACO and 91 patients with COPD, were retrospectively collected, and gradients among combinations of explanatory variables of spirometric (FEV1, FEV1/FVC, FEF25-75), plethysmographic (sReff, sGeff, the aerodynamic work of breathing at rest; sWOB), static lung volumes, including trapped gases and measurements of the carbon monoxide transfer (DLCO, KCO) were explored using multiple factor analysis (MFA). The discriminating power of lung function parameters with respect to ACO was assessed using linear discriminant analysis (LDA).
Results: LDA revealed that parameters of airway dynamics (sWOB, sReff, sGeff) combined with parameters of static lung volumes such as functional residual capacity (FRCpleth) and trapped gas at FRC (VTGFRC) are valuable and potentially important tools discriminating between asthma, ACO and COPD. Moreover, sWOB significantly contributes to the diagnosis of obstructive airway diseases, independent from the state of pulmonary hyperinflation, whilst the diffusion capacity for carbon monoxide (DLCO) significantly differentiates between the 3 diagnostic classes.
Conclusion: The complexity of COPD with its components of interaction and their heterogeneity, especially in discrimination from ACO, may well be differentiated if patients are explored by a whole set of target parameters evaluating, interactionally, flow limitation, airway dynamics, pulmonary hyperinflation, small airways dysfunction and gas exchange disturbances assessing specific functional deficits.
Keywords: COPD, COPD and coexisting asthma, ACO, aerodynamic work of breathing, airway dynamics, pulmonary hyperinflation, small airways dysfunction, precision medicine, multiple factor analysis, MFA, linear discriminant analysis, LDA
Plan Language Summary
COPD is a complex and heterogeneous disease, making it difficult to understand disease etiology, detect early onset and define robust therapeutic strategies to reduce disease progression. Therefore, there is a dearth of information on understanding lung physiology of this disease because most functional assessment is only based on spirometric parameters, and the lack of reliable biomarkers for COPD emphasizes the inherent need for larger data evaluation and integration of multiple implicated pathophysiological processes differentiating the various subtypes of COPD. Lung function trajectories in COPD differ significantly between patients, and currently cannot reverse lung damage. Moreover, the assessment of early onset COPD is critical in mitigating disease progression. Given the complexity of this disease, it has been anticipated to address innovative analytical methods in terms of an approach towards precision medicine in COPD, especially also between COPD and the asthma overlap in COPD. Therefore, we developed a concept to define discriminating functional markers, focusing on a whole set of spirometric, plethysmographic and gas-exchange parameters, featuring traits within a conditional inference tree to help in decision making.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, complex and heterogeneous disease, characterized by an assortment of different functional disorders due to an increased inflammatory response of the lungs.1,2 It is supposed that the complexity refers to components and their interactions, while heterogeneity occurs because not all especially functional components are present in all patients concurrently3,4 throughout the whole lifetime.5 In our understanding, therefore, physiologic management can hardly only be assessed by one or two spirometric parameters. Physiologically, COPD is a disease characterized by a combination of either pulmonary hyperinflation, small airways dysfunction, airway dysfunction, air trapping, and gas-exchange disturbances and, therefore, an attempt to objectify such interactive functional deficits implicates the assessment of a whole set of discriminating target parameters. Moreover, a substantial proportion of patients show characteristics of both asthma and COPD, referred to as the asthma–COPD overlap (ACO),6–12 although the nosology of this overlap remains controversial.13–15 ACO combines clinical and functional features of both diseases, asthma and COPD. Whereas COPD, depending on which lung function parameter is used,16 is characterized by poorly reversible airflow limitation and airway obstruction, patients with ACO are thought to present a bronchodilator response (BDR) that serves as a major criterion for the diagnosis of ACO.11,13,17–20 Although some consensus documents contain precise classification criteria for ACO,21,22 there is still a lack of an internationally accepted definition of ACO and, in consequence, research into ACO has been.23 Some physicians and researchers still consider ACO to be a specific syndrome,24 whereas other physicians and researchers see ACO as a theoretical construct with no clear biological grounds.25 However, in no longer referring to the term ACO but, instead, increasing emphasis on individual treatment approaches tailored to COPD and/or asthma, a focus on precision medicine in these patients should be adopted. It is important to recognize that there are differentiating features in asthma and AOC: from etiology, symptoms, type of airway inflammation, inflammatory cells and mediators, consequences of inflammation, response to therapy, and disease course.26 For a patient with COPD, a diagnosis of concomitant asthma must be considered, based on an individualized assessment to assure adequate treatment.27,28
Until recently, the plethysmographic parameters, such as effective specific airway resistance (sReff), its reciprocal parameter, the effective specific airway conductance (sGeff) and notably the plethysmographic parameter expressing the specific aerodynamic work of breathing at rest (sWOB), have not yet gained enough attention concerning their potential to differentiate COPD from ACO. This may be due to the fact that the relationship between parameters of airway dynamics and anthropometric measurements is rather complex, and hence only a few reference values are available.29–31 There is, however, up-coming work indicating that the major mathematical component of airway dynamics (sReff and sGeff) is sWOB,32,33 from which normalized reference equations have recently been defined.34
Therefore, the purpose of the present study was to address the complexity of chronic obstructive airway diseases physiologically, selecting specific target parameter values expressed in z-scores,35–38 with proven discriminatory statistical power, and hence to present a multidimensional perception of a treatable trait strategy39 within a new concept of precision.39,40
Patients and Methods
Study Design and Ethics
In the present study we refer to retrospectively evaluated data obtained from 4 Swiss centers (Center of Pulmonary Diseases, Hirslanden Private Hospital Group, Salem-Hospital, Bern, Switzerland; Clinic of Pneumology, Cantonal Hospital St. Gallen, Switzerland; Center of Pulmonology, Clinic Hirslanden, Zürich, Switzerland; Clinic of Pneumology, Barmelweid Hospital, Switzerland). Patients’ records were anonymized before analysis to maintain their confidentiality. The patients had been referred to the centers for extended pulmonary function testing and optimizing therapy. Data were collected from patients with a clinical diagnosis of chronic obstructive pulmonary diseases: (i) COPD, (ii) COPD with coexisting asthma (ACO), or (iii) bronchial asthma, according to international standards.1 The anamnestic and clinical features were assessed by experienced pulmonary physicians based on history-taking, chest radiographs, high-resolution CT-scans, and functional investigations such as spirometry, whole-body plethysmography, measurements of carbon monoxide diffusion capacity (DLCO) and measurement of the fraction of exhaled nitric oxide (FeNO).
The study was planned according to the Federal Law of Human Research, conceptualized according to the Swiss Ethics Committees on research involving humans, and was conducted in accordance with the tenets of the Declaration of Helsinki. The study is a part of the framework of the project entitled “Functional Diversification of the Asthma-ACO-COPD Multi-center Study” (ID 2017–00259), approved by the Governmental Ethics Committees of the State of Bern, St. Gallen, Solothurn, and Zürich (Project KEK-BE PB_2017-00104). Written informed consent was waived because of the retrospective study design, which followed the institutional and national policies concerning research approvals.
Differential Diagnosis and Patient Cohort
COPD was defined by a history of smoking (current or ex-tobacco smokers) or equivalent indoor/outdoor air pollution, with chronic cough, sputum and dyspnea, previously documented persistent airflow limitation with post-bronchodilator values of FEV1/FVC <70% and FEV1 <80%, not fully reversible with a bronchodilator.6,14 Asthma was diagnosed based on a past history of atopy and/or allergies with symptoms such as wheezing, shortness of breath, chest tightness and cough that vary over time in their occurrence, frequency and intensity, and proven bronchial hyperreactivity (BHR),6 or a positive bronchodilation test.41 ACO was diagnosed when the subject had features of COPD and asthma, with documented bronchodilator response in a FEV1 >12% and 200 mL.6 Patients previously diagnosed with cystic fibrosis, interstitial lung disease, pulmonary thromboembolic disease, active tuberculosis, chest wall disease, neuromuscular disorder, malignant tumor, or a history of thoracotomy with pulmonary resection were excluded.
From the database of the 4 centers, 540 measurement-sets fulfilled the inclusion criteria of a correctly conducted post-bronchodilator response-test to 200 µg Salbutamol, defined as positive if the conditions ∆FEV1 and/or ∆FVC ≥12%, and ≥200 mL are fulfilled.42–44 These data sets were obtained from a total of 540 patients, 231 males (42.8%) and 309 females (57.2%), containing 372 patients with asthma (68.9%), 77 patients with ACO (14.3%) and 91 patients with COPD (16.9%), with a mean age of 51.4 years (18.0–92.2 years). Patients with asthma were significantly younger than patients with ACO (mean difference 4.5±2.3 years) and COPD (mean difference 21.5±2.2 years).
Pulmonary Function Procedures
In all 4 centers, plethysmography including spirometry and diffusing capacity for carbon monoxide (DLCO), corrected for alveolar volume (KCO) by single breath analysis, was performed using a constant-volume body plethysmograph (Master Screen Body, Erich Jaeger GmbH, Würzburg, Germany) by standard techniques according to ATS-ERS criteria30,43,45,46 and revised Swiss guidelines.28 Apart from a daily calibration procedure given by the software of the Master Screen Body, monthly so-called “biological controls” were performed, measuring lung function in a healthy, non-smoking technician. The sequence of measurements was as follows. In the first step, measurements of airway dynamics giving the effective, specific airway resistance (sReff), the reciprocal value of the specific airway conductance (sGeff), and the specific aerodynamic airway conductance (sWOB), as well as the determination of the specific total resistance (sRtot) were conducted. Since the integral method evaluates changes of airway dynamics concomitantly with changes in the end-expiratory lung volume (EELV) at FRC,16,30,32,41,47,48 it was important that parameters of airway dynamics were assessed in this first phase of plethysmographic assessment, and hence not influenced by deep inspiration or forced breathing maneuvers or other efforts.49–52 In the second step, measurements of static lung volume such as functional residual capacity (FRCpleth) obtained by 3 shutter-closure maneuvers were applied, closely linked with the third step of slow maximal expiratory and inspiratory maneuver, giving the measures of residual lung volume (RVpleth), inspiratory capacity (IC), vital capacity (VC) and total lung capacity (TLCpleth). Only in the fourth and final step was forced spirometry recorded and presented as flow-volume-loop and volume-time-trend, deriving the forced expiratory volume in one second (FEV1), the forced vital capacity (FVC) and its ratio to FEV1 (FEV1/FVC) and the forced expiratory flows between 25% and 75% of exhaled FVC (FEF25-75). More detailed information regarding computation of the parameters of airway dynamics are given in the Supplemental Material (Section 1).32,33,53–63 The plethysmographic and spirometric measurements were then followed by measurements of the diffusing capacity for carbon monoxide (DLCO) corrected for alveolar volume (KCO). The DLCO measurements were obtained by standard procedures,64 as single breath-hold maneuver, calculated from the alveolar volume (VA) of the lung, breath-hold time, and the initial and final alveolar concentrations of carbon monoxide. The inhaled and exhaled helium concentrations are used to calculate a single breath estimate of the VA. Applying VA, the initial alveolar concentration of carbon monoxide can be calculated and TLCHe is derived by adding the anatomic dead space to it. The parameter TLCHe finally allows determination of FRCHe and RVHe by subtraction of IC, VC respectively. Inspiratory capacity (IC) was calculated indirectly by measuring the expiratory reserve volume (ERV) and vital capacity (VC) as the difference in predicted z-scores of TLCpleth and FRCpleth, respectively. Values were expressed as z-scores based on reference equations from Cotes et al.45 Theoretically, the volumes of trapped gases (VTG) can be calculated on three levels of static lung volume. Combining the 3 static volume levels express as z-scores of TLCpleth, FRCpleth and RVpleth with the corresponding gas-dilution volume levels TLCHe, FRCHe and RVHe enables the calculation of trapped gases defined as VTGTLC = TLCpleth-TLCHe, VTGFRC=FRCpleth-FRCHe and VTGRV= RVpleth-RVHe.65 Since there is not yet a clear appreciation of how trapped gases should be defined, we tested the discriminative power of 3 VTG-ratios (VTGTLC, VTGFRC, VTGRV) and perceived that the highest discriminative power was given by VTGFRC (AUC 0.802±0.038; p <0.0001). A special export software was developed by PanGas Ltd, Dagmersellen, Switzerland, enabling access to all routinely stored parameters in every JLab- and Sentry-Suite databases.
Z-score transformation. All data were transformed to z-scores as a standardized measure of the positioning of an observed measurement in the distribution of the reference population, taking both between-subject and age- and growth-related variability into account.34–38,43,66–69 To allow clinical interpretation of test results numerically independent from sex, age and ethnicity, measurement results were transferred into z-scores, as a standardized measure of the positioning of an observed measurement in the distribution of the reference population taking both between-subject as well as age- and growth-related variability into account.34–38,43,66–69 Using this procedure, the lower limit of normal (LLN), identical with z = −1.645, or the 5th percentile in the distribution of FEV1, FEV1/FVC ratio, FEF25-75, as well as the upper limit of normal (ULN), identical with +1.645 z-scores or the 95th percentile for sReff, sRtot, sWOB, TLCpleth, FRCpleth, RV/TLC and DLCO, KCO were obtained, respectively, and transformed into z-scores according to standard prediction equations45,70,71 (Figure 1).
 |
Figure 1 Comparison of z-score distribution of initial values of all lung function parameters within the 3 diagnostic groups. |
Functional severity. In order to upgrade the former issue of GOLD regarding functional severity, we replaced the fixed ratio of FEV1/FVC < 0.70 as criterium of functional severity by z-scores over the whole range of baseline z-scores for each lung function parameter, as previously presented in this journal.16 By that the degree of functional severity of airflow limitation (FEV1, FEV1/FVC), small airways dysfunction (FEF25-75), dynamic airway dysfunction (sReff, sRtot, sWOB), pulmonary hyperinflation (FRCpleth), trapped gases (VTGFRC) and gas diffusion disturbance (DLCO, KCO) could be assessed within the 3 diagnostic classes, with the advantage that all parameters could functionally be comparable since they have been expressed as z-scores and, hence, gender-, age-, height- and ethnicity-corrected, as previously recommended.16,35–38
Assessment of airway dynamics. Although numerous parameters of airway dynamics can be calculated from the plethysmographic sRaw-loop,56 we used the approach proposed by Matthys and Orth57 defining the so-called “effective specific resistance” (sReff) as the ratio of the area of the shift-volume versus tidal volume ( ), to the area of the tidal flow/volume loop (
), to the area of the tidal flow/volume loop ( ) (see Figure S1). The mathematical background of the integral technique to obtain parameters of airway dynamics (sReff, sGeff, sWOB) has been previously established.33,41,57,65 Details of the methodological and mathematical approach of the so-called “integral method” are given in the Supplemental Material (Section 1).32,33,53–63 The advantage of this integral method compared with parameters of the two-point analysis defining sRaw, sGaw, respectively, is that data points throughout the entire respiratory cycle are evaluated. Moreover, the integral
) (see Figure S1). The mathematical background of the integral technique to obtain parameters of airway dynamics (sReff, sGeff, sWOB) has been previously established.33,41,57,65 Details of the methodological and mathematical approach of the so-called “integral method” are given in the Supplemental Material (Section 1).32,33,53–63 The advantage of this integral method compared with parameters of the two-point analysis defining sRaw, sGaw, respectively, is that data points throughout the entire respiratory cycle are evaluated. Moreover, the integral  embodies the specific, aerodynamic work of breathing (sWOB) at rest.57 For the parameters of airway dynamics (sWOB, sGeff, and sReff), normative reference equations were used, recently worked out,34 and provided in the Supplemental Material (Section 2).29,34,47,70–81
embodies the specific, aerodynamic work of breathing (sWOB) at rest.57 For the parameters of airway dynamics (sWOB, sGeff, and sReff), normative reference equations were used, recently worked out,34 and provided in the Supplemental Material (Section 2).29,34,47,70–81
Statistical Approach, Data Analysis and Statistical Methods
The distribution of all parameters presented as age- and gender-corrected z-scores is reported. Two-sided tests with a type-I error α=5% were used. P-values under 0.05 were considered statistically significant. There were 3 diagnostic classes (asthma, ACO, COPD) to be discriminated, and discrimination was based on 17 lung function parameters as potential predictors, separately evaluated within 5 lung function categories (flow limitation, airway dynamics, static lung volumes, trapped gases, CO-diffusion). Linear discriminant analysis was performed, and discriminate functions were identified. A confusion matrix summarizing the leave-one-out cross-validation classification accuracy of lung functions was created. Wilks’s lambda (Λ) test statistics was used for refined variable selection. The stepwise assessment of the R-statistics is given in the Supplemental Material (Section 3).
All analyses were done using the IBM SPSS software (version 28.0 (SPSS Inc., Chicago, IL), and R statistical software, version 4.1.2 (R Statistics, Vienna, Austria), together with the extension packages MASS, FactoMineR, caret and ade4.
Results
Assessment of Functional Deficits
The distribution of the lung function parameters expressed as z-scores within the 3 diagnostic classes, asthma, ACO and COPD, for spirometric flow limitation (FEV1, FEV1/FVC, FEF25-75), plethysmographic airway dynamics (sReff, sRtot, sWOB) static lung volumes (TLC, FRCpleth, RV, IC/TLC, FRC/TLC, RV/TLC), trapped gases obtained on 3 lung volume levels (VTGTLC, VTGFRC, VTGRV) and the CO-diffusion (DLCO, KCO) are given in Figure 1. Highest range of z-score distribution was found within the diagnosis class “COPD”, especially for sWOB (asthma: 18.8; ACO: 13.5; COPD 15.9).
In Table 1 the prevalence of each parameter in this study is given, showing some unexpected new findings. In row a, the number (in %) of measurements of each parameter within its normal range is given. The prevalence of spirometric parameters (row b, all: FEV1: 25.4%; FEV1/FVC: 20.9%; FEF25-75: 15.9%) was significantly lower than those of plethysmographic parameters (row b, all: sReff: 31.7%; sRtot: 64.1%; sWOB: 75.2%; FRCpleth: 35.9%; VTGFRC: 36.9%). Moreover, z-scores of spirometric parameters (row c, all: FEV1: −2.78±0.88; FEV1/FVC: −3.79±1.62; FEF25-75: −2.24±0.46) were significantly lower and less widespread than those of plethysmographic parameters (row c, all: sReff: −2.52±0.79; sRtot: 3.38±1.31; sWOB: 3.05±2.85; FRCpleth: 2.75±0.83). Accordingly, the F-statistic of ANOVA differentiating between the 3 diagnostic classes was highest for sWOB, followed by sRtot and sReff. Noteworthy is that a high prevalence was found for sWOB (asthma: 67.2%; ACO: 85.7%; COPD: 98.9%), with highest z-scores in patients with COPD (asthma: 1.98±1.79; ACO: 1.89±1.94; COPD: 6.89±2.49), significantly different between the 3 diagnostic classes (F=214.1, p <0.001). Remarkably, the prevalence of pulmonary hyperinflation in COPD patients was high and severe (76.9%; z = 3.31±0.92) and also in combination with trapped gases (VTGFRC: 82.4% z = 3.13±1.01). Expectedly, prevalence and severity of CO-transfer disturbances were considerably pronounced in patients with COPD (DLCO: 82.4%; z = −2.94±0.90, KCO: 75.8%; z = −2.90±0.85, respectively).
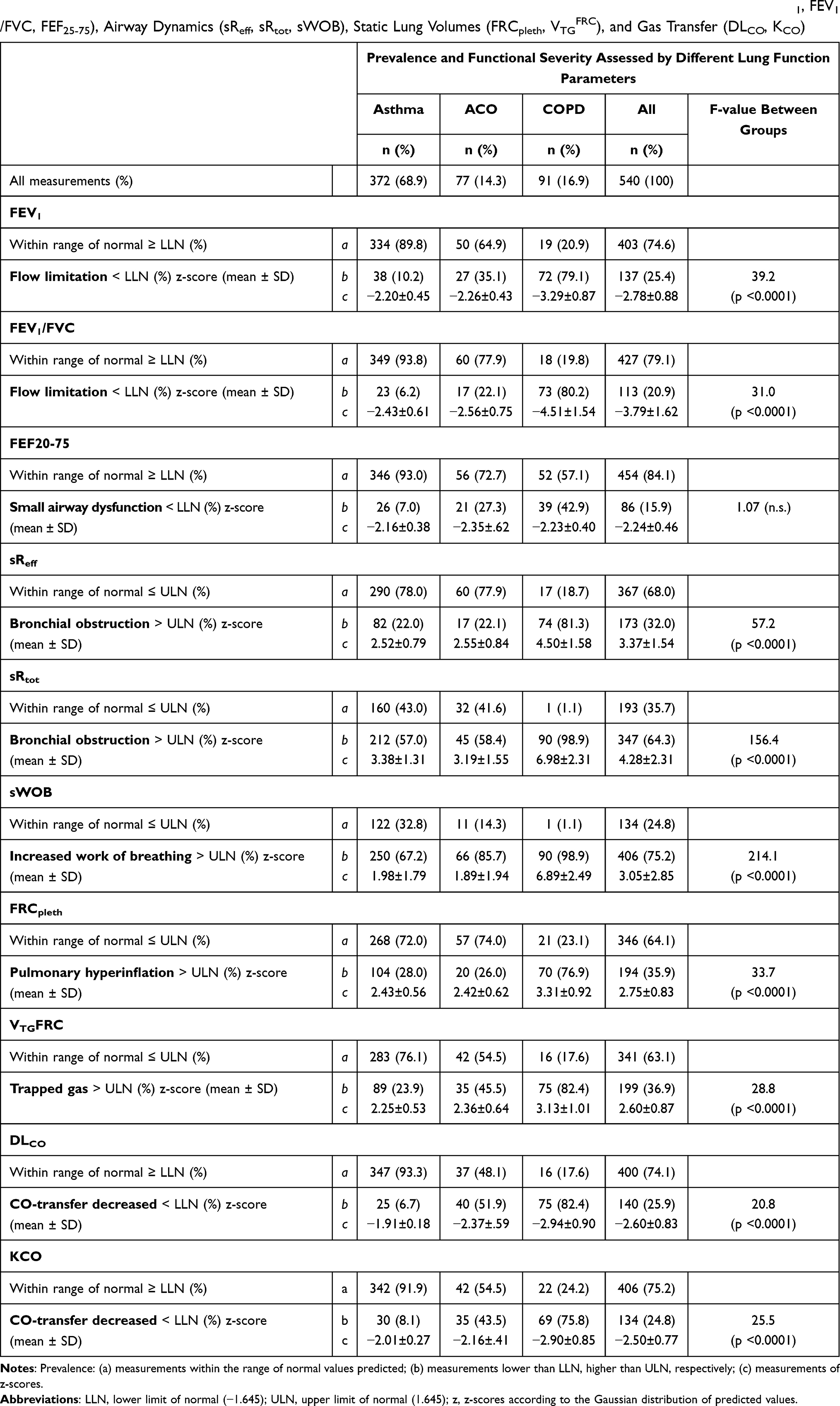 |
Table 1 Prevalence and Functional Severity of All Lung Function Parameters Within 4 Indicator Sets for Flow Limitation (FEV1, FEV1/FVC, FEF25-75), Airway Dynamics (sReff, sRtot, sWOB), Static Lung Volumes (FRCpleth, VTGFRC), and Gas Transfer (DLCO, KCO) |
MANOVA followed by a stepwise forward variable selection was applied to the original 17-variable dataset. The 17 original variables (predictors) were grouped within 5 categories (spirometry: FEV1, FEV1/FVC, FEF25-75; airway dynamics: sReff, sRtot, sWOB; static lung volumes: TLC, FRCpleth, RV, IC/TLC, FRC/TLC, RV/TLC; trapped gases: VTGTLC, VTGFRC, VTGRV; and CO-diffusion: DLCO, KCO) (Figure S2). Following the variable selection based on Wilks’s lambda statistics (Λ), FEV1, FRCpleth, RV/TLC, VTGTLC and KCO were excluded from the model. Details are given in the Supplemental Material (Section 3). A linear discriminant analysis based on the remaining 12 variables is given in Figure 2, demonstrating that the first function discriminated COPD from asthma, and the second function differentiated asthma from ACO, with a classification accuracy of 90% (asthma: 87%; ACO: 75%; COPD: 94%).
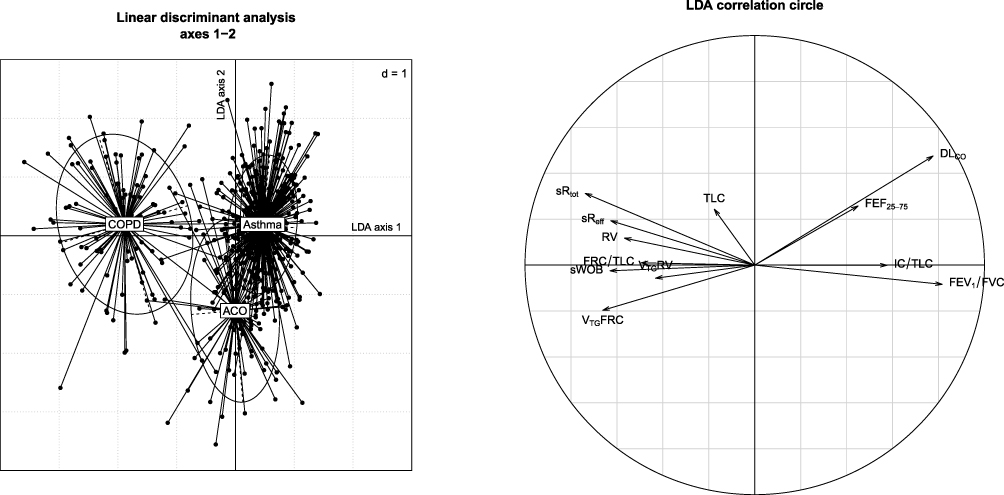 |
Figure 2 Linear discriminant analysis (LDA) discriminating COPD from asthma (first function, x-axis) and asthma from ACO (second function, y-axis), based on 12 lung function parameters selected from the 17 original variables by MANOVA. |
This evaluation of the probability of the group membership between the 3 diagnostic classes (asthma, ACO, COPD) revealed that 12 parameters, DLCO (Λ: 0.489), FEV1/FVC (Λ: 0.328), sRtot (Λ: 0.267), sWOB (Λ: 0.244), FEF25-75 (Λ: 0.227), VTGFRC (Λ: 0.214), sReff (Λ: 0.204), RV (Λ: 0.215197), TLC (Λ: 0.190), IC/TLC (Λ: 0.187), VTGRV (Λ: 0.186) and FRC/TLC (Λ: 0.185), significantly entered the model (p <0.001).
Onset of Lung Function Deterioration in ACO and COPD
Recent evidence shows that failure to attain peak lung function is a risk factor for early onset of COPD.82,83 However, it is well known that, even with normal attainment of lung function, the risk of COPD is significantly increased among patients with accelerated lung function decline.84 Although we do not dispose over repeated measurements over the life course, we have been interested to evaluate comparatively our parameters as potential predictors that influence underlying disease onset. In Figure 3, the most significant parameter onsets within the data set of ACO compared to COPD are shown. Whereas in ACO a substantial splitting of parameter onsets can be observed, such a separation (apart from FEF25-75) cannot be found in COPD. A comparison of ACO versus COPD within parameter-specific cumulative percentage onset of abnormal lung function is shown in Figure 4. As most sensible trajectory parameters classify sWOB with cumulative percentage onsets of 5–10%, respectively, in ACO at age 27.8–33.0 years and COPD at 50.2–56.4 years (χ2=23.6, p <0.0001), followed by VTGFRC at 35.3–38.1 years for ACO and 54.0–58.0 years for COPD, respectively (χ2=6.2, p <0.02), and DLCO at 31.6–39.3 years for ACO and 54.0–58.0 years for COPD, respectively (χ2=5.6, p <0.02). Whereas in patients with ACO a certain diversity of parameter onsets could be observed, such distinction could not be found in patients with COPD. FEV1 and FEV1/FVC are presented as late onset parameters (FEV1: 38.4–52.9 years in ACO and 54.0–58.0 years in COPD; FEV1/FVC: 39.3–58.6 in ACO and 54.0–58.0 years in COPD). Noteworthy is that abnormal lung function started much earlier in patients with ACO (age 20–30 years) than in COPD (age 45–55 years).
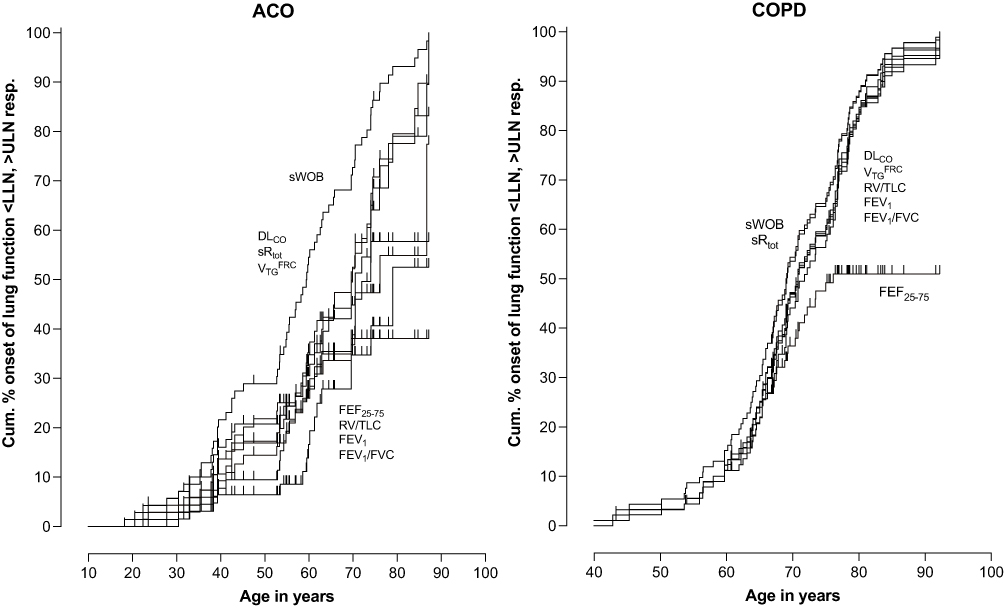 |
Figure 3 Cumulative present onset of the most significant lung function parameters within COPD compared to ACO exceeding the lower limit of normal (LLN) for DLCO, FEV1, FEV1/FVC, FEF25-75, or exceeding the upper level of normal (ULN) for sWOB, sRtot VTGFRC and RV/TLC. |
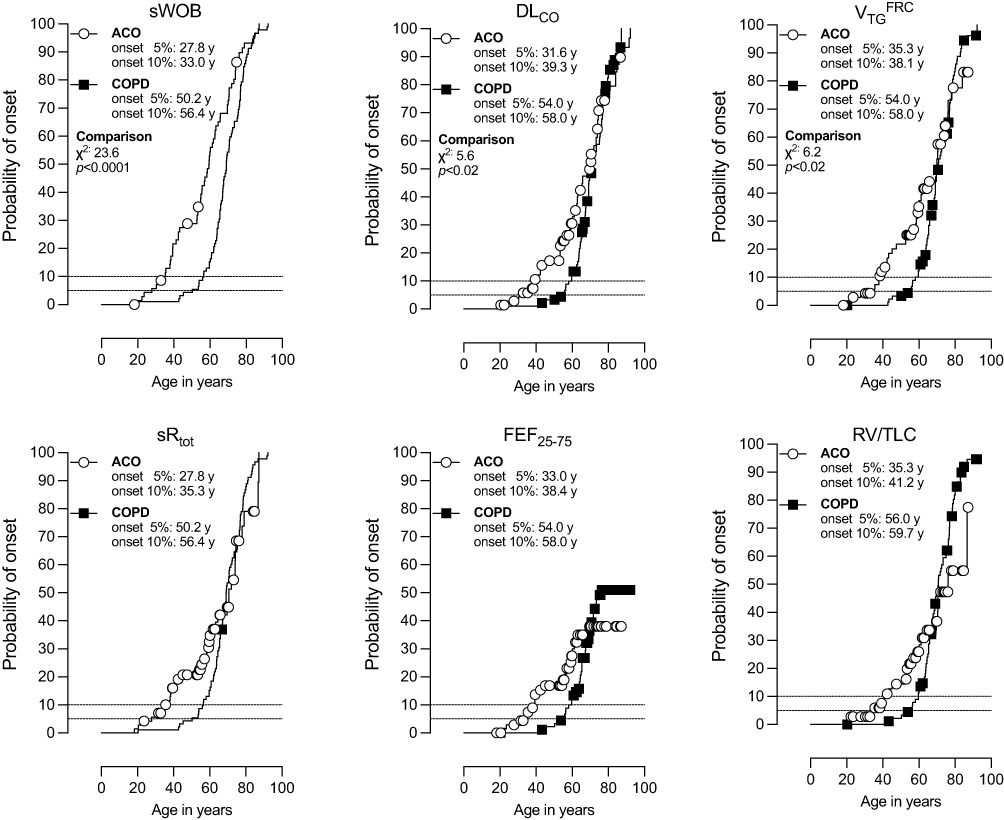 |
Figure 4 Probability of onset of disease at ages in years calculated at 5%- and 10%-levels of 6 lung function parameters (sWOB, DLCO, VTGFRC, sRtot, FEF25-75, an RV/TLC comparing ACO with COPD. |
Discussion
For years there has been ongoing and growing interest in characterizing functional diversities between asthma, ACO and COPD by lung function assessment. Specific efforts were to define discriminating factors for demarcation of ACO from COPD.11,13,17–20 A further task should be to identify within these diseases the onset of abnormal lung function and to assess its progression in functional severity85–89 for appropriate scheduling of treatment.28,90 In most studies, however, exclusively spirometric parameters are used. In contrast, the present study focuses on a multivariate approach of a whole set of parameters, looking at the various functional facets of the physiological complexity within and between the 3 diagnostic classes of asthma, ACO and COPD.
Findings of the Present Study
The main findings of the present study are that, in addition to spirometric parameters (FEV1, FEV1/FVC, FEF25-75), plethysmographic parameters, especially parameters of airway dynamics (sReff, sRtot, sWOB), and parameters of monoxide gas exchange are important trajectories for differentiating the different subtypes of COPD. In addition to diffusion capacity for carbon monoxide, the aerodynamic work of breathing at rest (sWOB) substantially contribute to differentiating the different types of obstructive airway diseases.
There are two components to the gas-dynamic work of breathing during respiration in patients with severe obstructive ventilatory defects and a closing volume above FRC level, which can be assessed with the plethysmograph: the aerodynamic work of breathing and the gas-dynamic work of breathing, performed on a trapped air volume which exceeds the ERV during spontaneous breathing at FRC level. The former refers to the work to overcome the frictional (aerodynamic) resistance of gas flow within the ventilated airways, whereas the latter is a waste of muscle force to compress non-ventilated lung volumes, so called trapped air. This can be recognized by a shift-volume difference between the end-inspiratory and end-expiratory zero-flow points. The new finding is that sWOB increases significantly in parallel with the deterioration of all parameters (Figure 3) but much earlier in ACO (Figure 4). Significant earlier percentage onset in ACO compared to COPD was also found for DLCO and VTGFRC (Figure 4). Interestingly, if sWOB is taken as primary parameter expressing functional severity, it could be shown that, in patients with COPD, sWOB increased in parallel with the significant deterioration of 3 other parameters (Figure 5: DLCO, RV/TLC, VTGFRC; p <0.0001). Such an association, however, was not found in patients with ACO. Moreover, our study also shows, that the deployment of trapped gas territories calculated as difference between the z-scores of plethysmographic FRCpleth and the FRCHe obtained by gas dilution in the lung may be a surrogate of what is already known through histologic studies.89,91–93 Briefly, these main findings clearly feature arguments that a discrimination between ACO and COPD can be achieved if a modelling profile of multidimensional acting outcome parameters is applied.
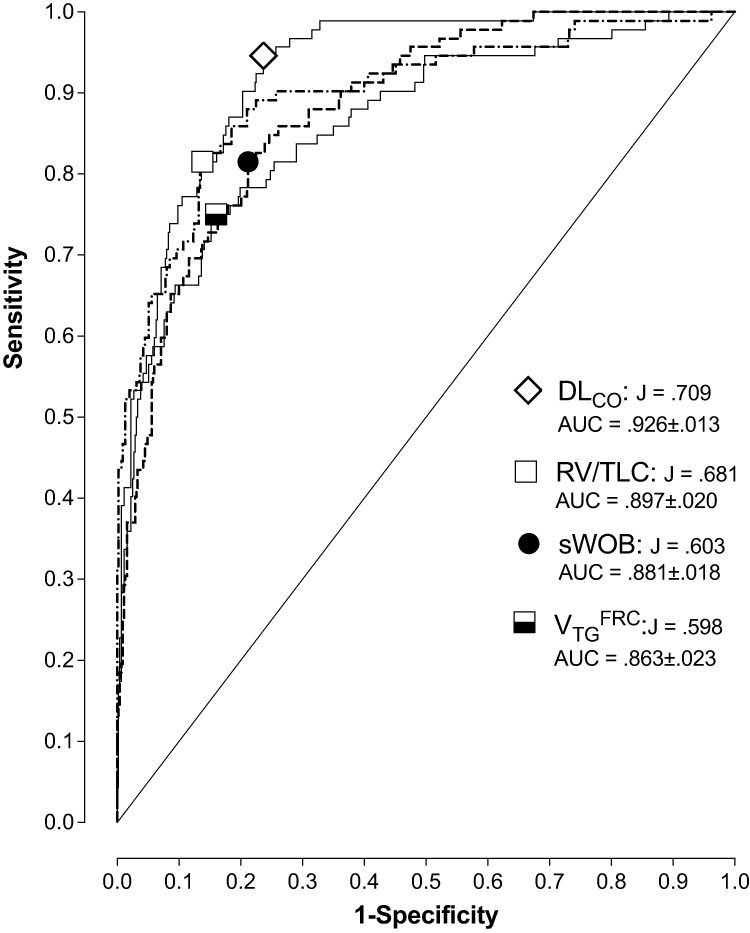 |
Figure 5 Sensitivity and specificity of the two gas-dynamic components of the work of breathing: (i) the specific aerodynamic work of breathing (sWOB) to overcome the frictional (aerodynamic) resistance of gas flow within the ventilated airways, on the one hand, and (ii) the trapped air at FRC (VTGFRC) indicating the waste of muscle forces to compress non-ventilated airways, on the other hand. |
In the following, we discuss some important features which discriminate ACO from COPD. Numerous comprehensive reviews of the natural history of COPD have been published.83,87,88,93 Early COPD diagnosis has remained challenging due to the small impact of early lung function loss within spirometric target parameters.94 Some studies reported relatively few cases diagnosed before the age of 50 years,85 and that patients started inhaled medication for COPD only at an average of 67.8 years.86 Therefore, several population-based studies have shown that underdiagnosis of COPD is substantial,95 and many experts consider the late diagnosis of COPD as the most important factor responsible for the poor outcome in a substantial proportion of patients. Both cross-sectional and longitudinal studies have identified numerous factors associated with the risk of being diagnosed with COPD, mainly in association with active smoking.89 In none of these studies, however, was lung function assessed by lung function parameters other than FEV1, and in none of these studies was a distinction between ACO and COPD identified.
The Copenhagen City Heart Study followed up lung function trajectories, exacerbations and survival in individuals with ACO with early-onset asthma (<40 years of age), and ACO with late-onset asthma (>40 years of age).96 Patients with late-onset asthma experienced a FEV1 decline at a faster rate than those with early-onset asthma, and an increased risk of hospital admissions and reduced life expectancy, which was even more pronounced than in those with COPD and, hence, without asthma. We cannot comment on that phenomenon because we have no information regarding the onset of asthma in COPD patients. However, the observation that in our data sWOB presented a 5% cumulative percentage onset in asthmatics 30 years earlier than in those with COPD (53.6 minus 23.4 years), and a notation of the cumulative decrease in DLCO in ACO patients 23.4 years earlier than in COPD patients (55.0 minus 31.6) confirms previous findings, that COPD evolving from early-onset asthma is in a more benign condition than COPD that is complicated by the development of late-onset asthmatic features.96
It is estimated that patients with ACO are prone to experiencing more frequent and more severe exacerbations, and evidence-based effective treatments for ACO have yet to be defined. One problem with ACO is still that there have been many clinical trials performed in patients with chronic obstructive lung diseases, excluding patients with ACO, mainly because no definitive inclusion criteria have been developed for this subtype of disease. Therefore, ACO refers to a group of poorly studied and characterized patients making both diagnosis and treatment challenging for the clinicians. It is our understanding and belief that this uncertainty regarding the diagnosis of ACO could be resolved and the elaboration of an adequate study-based treatment of patients with ACO could be found if a discrimination between ACO and COPD is achieved by a modelling profile of multidimensional acting outcome parameters, including those separate from spirometric parameters and the addition of parameters of the airway dynamics.
Only a limited number of studies evaluate functional severity by combining spirometric and plethysmographic assessment in COPD patients.16,97–100 To our knowledge, only our previous study evaluated airway dynamics (sReff, sRtot, and especially sWOB) by the plethysmographic integral method.16 By using such an approach, a much more profound insight into lung physiology is provided, insofar as not only the degree of flow limitation (FEV1, FEV1/FVC) but also the degree of bronchial obstruction (sReff, sRtot) and the costs of breathing at rest (sWOB) are specified. In addition, the magnitude of pulmonary hyperinflation (FRCpleth), the occurrence of gas trapping (VTGFRC) due to bronchial collapse inclination, and the degree of small airways dysfunction (FEF25-75, sGeff) may lead to intrabronchial gas distribution dysfunction, which can be estimated by DLCO and KCO, respectively. Although parameters of airway dynamics and parameters of CO-diffusion capacity may overlap with the disturbed pattern of a respiratory disorder, they may reveal unique components in the differentiation of diagnosis, if it is assumed that a distinction can be made between ACO and COPD, on the one hand, and ACO and asthma on the other. Our multifunctional assessment demonstrates that certain combinations of target parameters significantly contribute to the discrimination of these respiratory diseases.
Small Airways Dysfunction (SAD)
There is considerable evidence that, pathologically, both small airways disease and emphysema are related to airflow limitation in COPD,101 suggesting that SAD is present at all stages of COPD. Therefore, the detection of SAD in early stages of COPD should be an important target. SAD appears to be a precursor to the development of emphysema,91,101–103 and pharmacological targeting should be focused earlier rather than later in the natural history of COPD. Most of the available information derives from either pathological studies or review articles, and there is little data on the natural history of small airways dysfunction in the onset or progression of asthma and COPD. Labaki et al104 showed that regions with SAD on CT-scans are subsequently converted into emphysema after 5 years, supporting the concept that small airways are a primary pathological site for all COPD phenotypes. Several lung function indices have been proposed and evaluated as markers of small airways function. Among these, the FEF25-75 is the most cited indicator of small airways dysfunction, although the literature on its reliability is not conclusive. One problem with FEF25–75 is related to alteration of the so-called “volume history” that occurs with air trapping and bronchodilation by shifting the lung volume range at which the FEF25–75 is computed. According to Sorkness et al,105 the characteristics of small airways dysfunction include premature airway closure, dynamic airway compression and air trapping, leading to regional heterogeneity and exaggerated volume dependence of airway dynamics. The question, however, is how progression of such combined structural alterations can be assessed physiologically. RV/TLC has been proposed as a potential marker for small airways function.106–109 However, RV/TLC varies with age and sex, implicating that the RV/TLC must be evaluated as z-scores from reference equations. If we select patients with presumed SAD according to the criteria proposed by Sorkness et al,105 combining abnormal z-scores of RV/TLC, VTGFRC and DLCO in our data collective, SAD could be attributed to 63.0% of patients with COPD (11.3% in ACO, 0.8% in asthmatics), highly correlated with all spirometric parameters and with sGeff, and, interestingly, with highest z-score mean difference between SAD and non-SAD of 2.9.
Pulmonary hyperinflation (PHI)
Pulmonary hyperinflation, defined as an increased volume of air remaining in the lungs at end-expiration, is present when resting end-expiratory lung volume (EELV) is increased above normal.110–112 PHI is a key feature in the disease course of COPD, and clinically important, because it contributes to dyspnea and reduced physical activity.106,111–113 In healthy individuals, the level of EELV remains positioned on the steep portion of the respiratory PV-compliance curve, and hence the static recoil-tidal volume relationship is favorable. In patients with obstructive pulmonary diseases, however, the tidal breathing may be shifted upwards to TLC, especially during an exacerbation or when exercising. Although by increasing distending forces on the bronchial tree expiratory flows may be optimized, it has the detrimental effect of forcing the respiratory system to operate on the flatter part of the compliance-PV curve, where the progressive pressure increases but generates smaller incremental volume changes. It follows that pulmonary hyperinflation imposes a restraining mechanical constraint on the respiratory system, where tidal volume expansion is limited in relation to increasing inspiratory effort, and hence the resistive work of sWOB.
Changes in static lung volume, especially trapped gases, may well disclose unrecognizable underlying disease processes, with functional consequences. An increase of FRCpleth above the upper limit of natural variability detects pulmonary hyperinflation, suggestive of the presence of emphysema and may hence be present as an early sign already in ACO. Defining patients with presumed PHI according to criteria proposed by different authors,114–118 we combined abnormal z-scores of FRCpleth with RV/TLC, and VTGFRC.. PHI including trapped gas could be attributed in 70.1% of patients with COPD (8.0% in ACO, 21.8% in asthmatics). Moreover, sWOB demostrated highest z-score mean difference between PHI and non-PHI of 5.4.
Airway Dynamics
A decrease in airway radius may be the result of increased amount of mucus and inflammatory cells obstructing the airway lumen, increased thickness of the submucosa related to inflammation, fibrosis or increase in smooth muscle mass, and distortion and narrowing of the lumen by the loss of alveolar attachments. Therefore, it is important to assess parameters reflecting these progressive processes, such as parameters of airway dynamics (sWOB, sGeff and sReff), measurements obtained by the integral method and hence independent of the value of FRCpleth. What was previously anticipated for the measurement of specific airway resistance (sRaw) regarding strength, repeatability and inter-dependence from the breathing pattern119–121 was no longer valuable, and has been resolved by the introduction of the integral method featuring airway dynamics such as sWOB, sReff and sGeff.32,34,57,122 It follows that, due to the proven clinical usefulness of airway resistance measurement in COPD patients, airway dynamic measurements deserve to be investigated.106 Moreover, since bronchodilator response (BDR) is considered an important potential phenotypic marker for several subtypes of COPD, dynamic tests (post-bronchodilation and/or provocations tests) could well serve as candidates for COPD subtyping. We have recently demonstrated that the discriminating power of BDR distinguishing asthma from ACO and COPD is significantly better achieved by sGeff than FEV1.16 Moreover, sWOB also improved in asthma by 76.2%, in ACO by 47.8%, and in COPD by 46.9%, compared to FEV1 (asthma: 21.8%; ACO: 18.6%; COPD: 4.2%).16 BDR assessed by several advanced lung function parameters was recently also studied by Jarenbäck et al,99 suggesting that in addition to flow-response, volume-response should also be evaluated. The overall clinical aim in COPD is to improve function in the small peripheral airways by improving flow (flow responders), as well as decreasing air trapping and pulmonary hyperinflation (volume responders). The evaluation of BDR is thus important and goes beyond the information provided by FEV1, which mainly reflects flow limitation in the central airways.123 The conclusion of Jarenbäck et al was that volume- and resistance-responses do not follow the flow response measured with FEV1.99
The content of the sRaw-loop consisting of the shift volume (Vpleth) and the tidal flow (V’) plot seems to be rather complex, especially in COPD patients when the sRaw-loop becomes the shape of a golf club within the expiratory limb, and a disease of the peripheral airways must be assumed. Consequently, different investigators have utilized different portions of the loop to approximate a representative value for the entire cycle. The sReff and sRtot have been well established as functional characteristics approximating the shape of such sRaw-loops.16,32,33,41,106,124 Noteworthy, is that, in contrast to the previously used sRaw reflecting proximal airway abnormalities, sReff and the reciprocal value sGeff were proven to be a target parameter reflecting small airways function.16,97,98,125 Moreover, Mahut et al suggested that sRtot and sReff can be considered equivalent and correlated with indices that explore peripheral airways (RV/TLC), and that these two parameters are statistically linked to activity-related dyspnea in COPD patients.106 The open shape of the sRaw-loop is associated with changes in the elastic recoil pressure and collapse during quiet tidal breathing due to the changes in airway resistance exhibited between inspiratory and expiratory flow. The shape also indicates unequal ventilation of the lung areas, which is a typical early sign of a pulmonary disease. Moreover, we have shown previously that the area of the sRaw-loop is related to the flow-resistive work of breathing sWOB,16 which may explain its correlation with activity-related dyspnea; as demonstrated by Mahut et al,106 sReff is a better descriptor of lung function due to its dual nature, eg, including resistance and volume components that may be related to the viscoelastic behavior of the lung. In COPD patients with nonhomogeneous small airway partial obstruction, the sRaw-loop area increases during expiratory flow, representing expiratory flow limitation and/or dynamic airway compression, the former being clearly linked to activity-related dyspnea in COPD patients.126 sReff and sRtot, therefore, represent surrogates of activity-related dyspnea in moderate to severe COPD patients.106
Regarding results of airway dynamics obtained in the present study, an important new finding can be presented insofar as sWOB was detected as the most sensible trajectory parameter, demonstrating much earlier onset of abnormal z-scores with cumulative percentage onsets of 5–10% in ACO at age 27.8–33.0 years and COPD at 50.2–56.4 years (p <0.0001), followed by DLCO at 31.6–39.3 years for ACO and 54.0–58.0 years for COPD (p <0.02), and VTGFRC at 35.3–38.1 years for ACO and 54.0–58.0 years for COPD (p <0.02).
Gas Exchange Disturbance
Diffusing capacity of the lung for carbon monoxide is a measure of gas exchange reflecting the complex interactions occurring at the alveolar–capillary interface. The analyses of Ni et al127 showed that diffusion capacity may be a useful objective assessment criterion for COPD. As diffusion capacity incorporates pulmonary ventilation and perfusion at the same time, it may be able to explain why some patients have more symptoms while their FEV1 is not very low. In their meta-analysis, DLCO was an important measurement for COPD patients in terms of severity, exacerbation risk, mortality, emphysema domination, and presence of pulmonary hypertension.127 In a similar context, Yanagisawa et al128 plead that COPD should be assessed by using DLCO and CT, because this variable in combination with this imaging method are strongly associated with the destruction of the alveolar wall.
The cascade of physiological events and their influence on expiratory flow limitation leading to pulmonary hyperinflation appears to be the pivotal abnormality and this has disastrous implications with respect to the mechanical and gas exchange functions of the respiratory system. While there are some studies evaluating DLCO as a predictor in COPD, especially to assess the integrity of the alveolar–capillary interface,129,130 only the study of Perez de Llano et al refers to the accuracy of algorithms to identify it in ACO.129 However, in that study, neither by a single variable nor by any combination of clinical, functional or inflammatory variables could the authors distinguish ACO patients from those in other categories of chronic obstructive airway disease.129 In contrast, however, applying the same technique using ROC data analyses we could define quite interesting target parameters discriminating between asthma, ACO and COPD. Figure 6 shows an ROC analysis of 4 prioritized lung function parameters presenting an area under the curve (AUC) of >0.80, dissociating the 3 diagnostic classes. The most pronounced dissociation was found for DLCO (AUC = 0.926±.013), followed by RV/TLC (AUC = 0.897±.020), sWOB (AUC = 0.881±.018) and VTGFRC (AUC = 0.863±.023). In contrast to previous studies, these ROC curves are computed based on z-scores and using the LLN of −1.645 SDS of precited normal as the cut-off.
 |
Figure 6 “Conditional Inference Tree” as a trait for decision making in the pathways of “precision medicine” distinguishing asthma and ACO from COPD, represented by the 4 most discriminating lung function parameters (DLCO, FEV1/FVC sRtot, VTGFRC). |
Conditional Inference Tree
To define and select the most discriminating lung function parameters within their functional severity (z-scores) to differentiate between asthma, ACO and COPD, a decision tree using the 4 highest discriminating parameters (DLCO, FEV1/FVC sRtot, VTGFRC) obtained by the MANOVA was constructed. The recursive partitioning by conditional inference (implemented in the R package party) of dependent variables based on the value of correlations is provided in Figure 6. The first split is given by the z-score of DLCO ≤ or >1.586, separating DLCO from asthma and ACO. In a second split (FEV1/FVC ≤−2.414 SDS) and in a third split COPD can be significantly distinguished from ACO if sRtot >3.669 SDS (60/91) and if sRtot >5.294 SDS (15/91) and hence in the total of 82.4%. If DLCO >−1.586 SDS VTGFRC > or ≤3.141, SDS primarily differentiates between asthma and ACO, especially if, in addition, FEV1/FVC >-2.964 SDS (369/372) in 99.2% of cases.
Limitations and Strengths of the Study
Several limitations need to be mentioned: The present study is a retrospective evaluation of lung function data obtained using various parameters and there are no longitudinal observations, a feature that can only be achieved by a prospectively designed study. Our actual challenge was to find surrogate markers superior to FEV1 and/or FEV1/FVC, to establish functional parameters significantly helping differentiation between COPD and ACO. As it turned out, such an evaluation based on various functional parameters of airway dynamics, static lung volume and gas transfer disclosed a variety of fundamentally different archetypes, which thus requires new definitions of functional assessment in COPD.
The main limitation of our study is that it addresses functional trajectories representing the complex lung physiology in COPD, not directly linked to clinical settings. However, the aerodynamic specific work of breathing at rest (sWOB) features presumably the closest parameter associated with clinical signs such as wheezing, shortness of breath, chest tightness and cough, and could well be taken as a marker for longitudinal follow-up and treatment efficacy. Other limitations are the relatively small number of subjects per center and within the subgroups of COPD. However, there were no differences if the centers were compared to one another (data not shown). Therefore, the population-based retrospective nature of our study and its highly standardized multicenter framework has a reliable force of expression.
The strengths of the present study are that we used pulmonary function data from well-characterized spirometric and plethysmographic target parameters, which allowed us to examine the interrelationships between several facets of lung function trajectory through early adulthood. We used an unsupervised modeling strategy that did not require arbitrary cut-offs to define “abnormal” lung function. In addition, our model was flexible in that it allowed the changes in lung function over time to vary between the different lung function trajectory classes.
Conclusion
Being aware of the enormous functional, structural, and biological heterogeneities occurring in patients with COPD, we like to anticipate considerable interest in evaluating the discrimination between COPD and ACO by a whole set of target parameters evaluating, interactionally, flow limitation, airway dynamics, small airways dysfunction, pulmonary hyperinflation, airway gas trapping, and gas-exchange characteristics, and hence assessing specifically the complex diagnostic class-specific functional deficits. The summary of these various ventilatory defects in COPD and their combination and interactions underscores the heterogeneous physiological mechanisms of this complex disease.131 Extended lung function testing could presumably be helpful in the tracking of dynamics and changes over time in patients with COPD. In view of the serious disease burden in COPD, a more sophisticated assessment of functional deficits and their reversibility would be justified, and not only because treatment could be adequately adjusted. Moreover, a further step in diagnosing the different phenotypes and corresponding treatment strategies could be provided.3,28 Noteworthy is that, despite the disagreement on the definition and recognition of ACO as a distinct pathophysiological entity,132,133 it seems important to us to identify ACO patients by highly discriminating factors of lung physiology, in order to allow better-targeted therapy,and, hopefully, improved clinical course. Moreover, this subgroup of ACO patients deserves to be included in therapeutic trials, to enable individualized management.
Abbreviations
ACO, asthma–COPD overlap; ATS, American Thoracic Society; AUC, area under the curve (ROC analysis); BDR, bronchodilator response; COPD, chronic obstructive pulmonary disease; DLCO, carbon monoxide diffusion capacity; ∆Vpleth, plethysmographic shift volume: EELV, end-expiratory lung volume; ERS, European Respiratory Society; FEF25-75, forced expiratory flow between 25 and 75% vital capacity; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; FRCpleth, plethysmographic functional residual capacity; FRCHe, functional residual capacity obtained by helium dilution technique; FVC, forced vital capacity; IC, inspiratory capacity; KCO, carbon monoxide transfer factor; LDA, linear discriminant analysis; LLN, loser limit of normal; Ln, natural logarithm; MFA, multiple factor analysis; MMEF, maximal mid-expiratory flow; Pamb, ambient pressure; PH2O, water pressure; PHI, pulmonary hyperinflation; ROC, receiver operating characteristics; RVHe, total lung capacity obtained by helium dilution technique; RVpleth, plethysmographic residual volume; SAD, small airways dysfunction; SD, standard deviation; sGaw, specific airway conductance (angle method); sGeff, effective specific airway conductance (integral method); sReff, effective specific airway resistance (integral method); sWOB, effective resistive work of breathing (integral method); TLCHe, total lung capacity obtained by helium dilution technique; TLCpleth, plethysmographic total lung capacity; ULN, upper limit of normal; VC, vital capacity; VIF, variance inflation factor; V’, flow; VT, tidal volume; VTGTLC, trapped gas on the level TLC, defined as TLCpleth – TLCHE; VTGFRC, trapped gas on the level FRC, defined as FRCpleth – FRCHE; VTGRV, trapped gas on the level RV, defined as RVpleth – RVHE.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was planned according to the Federal Law of Human Research, conceptualized by the Swiss Ethics Committee on Research involving humans, and approved by the Governmental Ethics Committees of the State of Berne, Zürich, and St. Gallen. Master-files have been stored and secured in the REDCap-system of the Clinical Trial Unit, Medical Faculty, University of Berne, Switzerland. Written informed consent was waived because of the retrospective study design, which is following the institutional and national policies concerning research approvals.
Acknowledgment
We are grateful to the staff of all study centers, especially to the study nurses for their excellent and enduring work in data collection, and we would like to thank Prof. Sabina Gallati from Human Genetics of Hirslanden Precise, Zürich, for the critical reviews of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors have no conflicts of interests to declare in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. 2020 Global strategy for prevention, diagnosis and management of COPD; 2020. Available from: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf).
2. Agusti A, Vestbo J. Current controversies and future perspectives in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;184(5):507–513. doi:10.1164/rccm.201103-0405PP
3. Faner R, Agusti A. Multilevel, dynamic chronic obstructive pulmonary disease heterogeneity. A challenge for personalized medicine. Ann Am Thorac Soc. 2016;13(Suppl 2):S466–S470. doi:10.1513/AnnalsATS.201605-372AW
4. Han MK, Quibrera PM, Carretta EE, et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(8):619–626. doi:10.1016/S2213-2600(17)30207-2
5. Agusti A, MacNee W. The COPD control panel: towards personalised medicine in COPD. Thorax. 2013;68(7):687–690. doi:10.1136/thoraxjnl-2012-202772
6. Gibson PG, Simpson JL. The overlap syndrome of asthma and COPD: what are its features and how important is it? Thorax. 2009;64(8):728–735. doi:10.1136/thx.2008.108027
7. Zeki AA, Schivo M, Chan A, Albertson TE, Louie S. The asthma-COPD overlap syndrome: a common clinical problem in the elderly. J Allergy. 2011;2011:861926. doi:10.1155/2011/861926
8. Kauppi P, Kupiainen H, Lindqvist A, et al. Overlap syndrome of asthma and COPD predicts low quality of life. J Asthma. 2011;48(3):279–285. doi:10.3109/02770903.2011.555576
9. Diaz-Guzman E, Khosravi M, Mannino DM. Asthma, chronic obstructive pulmonary disease, and mortality in the U.S. population. Copd. 2011;8(6):400–407. doi:10.3109/15412555.2011.611200
10. Louie S, Zeki AA, Schivo M, et al. The asthma-chronic obstructive pulmonary disease overlap syndrome: pharmacotherapeutic considerations. Expert Rev Clin Pharmacol. 2013;6(2):197–219. doi:10.1586/ecp.13.2
11. de Marco R, Pesce G, Marcon A, et al. The coexistence of asthma and chronic obstructive pulmonary disease (COPD): prevalence and risk factors in young, middle-aged and elderly people from the general population. PLoS One. 2013;8(5):e62985. doi:10.1371/journal.pone.0062985
12. Milanese M, Di Marco F, Corsico AG, et al. Asthma control in elderly asthmatics. An Italian observational study. Respir Med. 2014;108(8):1091–1099. doi:10.1016/j.rmed.2014.05.016
13. Postma DS, Rabe KF. The asthma-COPD overlap syndrome. N Engl J Med. 2015;373(13):1241–1249. doi:10.1056/NEJMra1411863
14. Woodruff PG, van den Berge M, Boucher RC, et al. American thoracic society/national heart, lung, and blood institute asthma-chronic obstructive pulmonary disease overlap workshop report. Am J Respir Crit Care Med. 2017;196(3):375–381. doi:10.1164/rccm.201705-0973WS
15. Mekov E, Nunez A, Sin DD, et al. Update on asthma-COPD overlap (ACO): a narrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1783–1799. doi:10.2147/COPD.S312560
16. Kraemer R, Smith HJ, Gardin F, et al. Bronchodilator response in patients with COPD, asthma-COPD-overlap (ACO) and asthma, evaluated by plethysmographic and spirometric z-score target parameters. Int J Chron Obstruct Pulmon Dis. 2021;16:2487–2500. doi:10.2147/COPD.S319220
17. Sin DD, Miravitlles M, Mannino DM, et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur Respir J. 2016;48(3):664–673. doi:10.1183/13993003.00436-2016
18. Cosio BG, Soriano JB, Lopez-Campos JL, et al. Defining the asthma-COPD overlap syndrome in a COPD cohort. Chest. 2016;149(1):45–52. doi:10.1378/chest.15-1055
19. Suzuki M, Makita H, Konno S, et al. Asthma-like features and clinical course of chronic obstructive pulmonary disease. an analysis from the Hokkaido COPD cohort study. Am J Respir Crit Care Med. 2016;194(11):1358–1365. doi:10.1164/rccm.201602-0353OC
20. de Marco R, Marcon A, Rossi A, et al. Asthma, COPD and overlap syndrome: a longitudinal study in young European adults. Eur Respir J. 2015;46(3):671–679. doi:10.1183/09031936.00008615
21. Soler-Cataluna JJ, Cosio B, Izquierdo JL, et al. Consensus document on the overlap phenotype COPD-asthma in COPD. Arch Bronconeumol. 2012;48(9):331–337. doi:10.1016/j.arbres.2011.12.009
22. Koblizek V, Chlumsky J, Zindr V, et al. Chronic Obstructive Pulmonary Disease: official diagnosis and treatment guidelines of the Czech Pneumological and Phthisiological Society; a novel phenotypic approach to COPD with patient-oriented care. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2013;157(2):189–201. doi:10.5507/bp.2013.039
23. Roman-Rodriguez M, Kaplan A. GOLD 2021 strategy report: implications for asthma-COPD overlap. Int J Chron Obstruct Pulmon Dis. 2021;16:1709–1715. doi:10.2147/COPD.S300902
24. Rogliani P, Ora J, Puxeddu E, Cazzola M. Airflow obstruction: is it asthma or is it COPD? Int J Chron Obstruct Pulmon Dis. 2016;11:3007–3013. doi:10.2147/COPD.S54927
25. Miravitlles M, Alvarez-Gutierrez FJ, Calle M, et al. Algorithm for identification of asthma-COPD overlap: consensus between the Spanish COPD and asthma guidelines. Eur Respir J. 2017;49(5):1700068. doi:10.1183/13993003.00068-2017
26. Cukic V, Lovre V, Dragisic D, Ustamujic A. Asthma and chronic obstructive pulmonary disease (COPD) - differences and similarities. Mater Sociomed. 2012;24(2):100–105. doi:10.5455/msm.2012.24.100-105
27. Miravitlles M, Andreu I, Romero Y, Sitjar S, Altes A, Anton E. Difficulties in differential diagnosis of COPD and asthma in primary care. Br J Gen Pract. 2012;62(595):e68–e75. doi:10.3399/bjgp12X625111
28. Stolz D, Barandun J, Borer H, et al. Diagnosis, prevention and treatment of stable COPD and acute exacerbations of COPD: the Swiss recommendations 2018. Respiration. 2018;96(4):382–398. doi:10.1159/000490551
29. Stocks J, Godfrey S, Beardsmore C, Bar-Yishay E, Castile R. Plethysmographic measurements of lung volume and airway resistance. ERS/ATS task force on standards for infant respiratory function testing. European Respiratory Society/ American Thoracic Society. Eur Respir J. 2001;17(2):302–312. doi:10.1183/09031936.01.17203020
30. Goldman M, Smith HJ, Ulmer WT. Lung function testing: whole-body plethysmography. Eur Respir Mon. 2005;31:15–43.
31. Crieé CP, Sorichter S, Smith HJ, et al. Body plethysmography–its principles and clinical use. Respir Med. 2011;105(7):959–971. doi:10.1016/j.rmed.2011.02.006
32. Kraemer R, Blum A, Schibler A, Ammann RA, Gallati S. Ventilation inhomogeneities in relation to standard lung function in patients with cystic fibrosis. Am J Respir Crit Care Med. 2005;171(4):371–378. doi:10.1164/rccm.200407-948OC
33. Kraemer R, Delosea N, Ballinari P, Gallati S, Crameri R. Effect of allergic bronchopulmonary aspergillosis on lung function in children with cystic fibrosis. Am J Respir Crit Care Med. 2006;174(11):1211–1220. doi:10.1164/rccm.200603-423OC
34. Kraemer R, Smith HJ, Matthys H. Normative reference equations of airway dynamics assessed by whole-body plethysmography during spontaneous breathing evaluated in infants, children, and adults. Physiol Rep. 2021;9(17):e15027. doi:10.14814/phy2.15027
35. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Consensus Development Conference. Am J Respir Crit Care Med. 2001;163(5):1256–1276. doi:10.1164/ajrccm.163.5.2101039
36. Swanney MP, Ruppel G, Enright PL, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Multicenter Study. Thorax. 2008;63(12):1046–1051. doi:10.1136/thx.2008.098483
37. Quanjer PH, Enright PL, Miller MR, et al. The need to change the method for defining mild airway obstruction. Eur Respir J. 2011;37(3):720–722. doi:10.1183/09031936.00135110
38. Scholes S, Moody A, Mindell JS. Estimating population prevalence of potential airflow obstruction using different spirometric criteria: a pooled cross-sectional analysis of persons aged 40–95 years in England and Wales. BMJ Open. 2014;4(7):e005685. doi:10.1136/bmjopen-2014-005685
39. McDonald VM, Fingleton J, Agusti A, et al. Treatable traits: a new paradigm for 21st century management of chronic airway diseases: treatable Traits Down Under International Workshop report. Eur Respir J. 2019;53(5):1802058. doi:10.1183/13993003.02058-2018
40. Cardoso J, Ferreira AJ, Guimaraes M, Oliveira AS, Simao P, Sucena M. Treatable traits in COPD - A proposed approach. Int J Chron Obstruct Pulmon Dis. 2021;16:3167–3182. doi:10.2147/COPD.S330817
41. Kraemer R, Smith HJ, Sigrist T, Giger G, Keller R, Frey M. Diagnostic accuracy of methacholine challenge tests assessing airway hyperreactivity in asthmatic patients - a multifunctional approach. Respir Res. 2016;17(1):154. doi:10.1186/s12931-016-0470-0
42. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Officiaö statement of the European Respiratory Society. Eur Respir J. 1993;16:5–40. doi:10.1183/09041950.005s1693
43. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Practice Guideline. Eur Respir J. 2005;26(5):948–968. doi:10.1183/09031936.05.00035205
44. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49(3):1700214. doi:10.1183/13993003.00214-2017
45. Cotes JE, Chinn DJ, Quanjer PH, Roca J, Yernault JC. Standardization of the measurement of transfer factor (diffusing capacity). Eur Respir J. 1993;6(Suppl 16):41–52. doi:10.1183/09041950.041s1693
46. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
47. Matthys H. The assessment of airways obstruction. Bull Physiopathol Respir. 1973;9(4):961–978.
48. Kirkby J, Stanojevic S, Welsh L, et al. Reference equations for specific airway resistance in children: the Asthma UK initiative. Eur Respir J. 2010;36(3):622–629. doi:10.1183/09031936.00135909
49. Kapsali T, Permutt S, Laube B, Scichilone N, Togias A. Potent bronchoprotective effect of deep inspiration and its absence in asthma. J Appl Physiol. 2000;89(2):711–720. doi:10.1152/jappl.2000.89.2.711
50. Salome CM, Thorpe CW, Diba C, Brown NJ, Berend N, King GG. Airway re-narrowing following deep inspiration in asthmatic and nonasthmatic subjects. Eur Respir J. 2003;22(1):62–68. doi:10.1183/09031936.03.00117502
51. Slats AM, Janssen K, van Schadewijk A, et al. Bronchial inflammation and airway responses to deep inspiration in asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;176(2):121–128. doi:10.1164/rccm.200612-1814OC
52. Nensa F, Kotschy-Lang N, Smith HJ, Marek W, Merget R. Assessment of airway hyperresponsiveness: comparison of spirometry and body plethysmography. Comparative Study. Adv Exp Med Biol. 2013;755:1–9. doi:10.1007/978-94-007-4546-9_1
53. Dubois AB, Botelho SY, Bedell GN, Marshall R, Comroe JH. A rapid plethysmographic method for measuring thoracic gas volume: a comparison with a nitrogen washout method for measuring functional residual capacity in normal subjects. J Clin Invest. 1956;35(3):322–326. doi:10.1172/JCI103281
54. Dubois AB, Botelho SY, Comroe JH. A new method for measuring airway resistance in man using a body plethysmograph: values in normal subjects and in patients with respiratory disease. J Clin Invest. 1956;35(3):327–335. doi:10.1172/JCI103282
55. Jaeger MJ, Otis AB. Measurement of airway resistance with a volume displacement body plethysmograph. J Appl Physiol. 1964;19:813–820. doi:10.1152/jappl.1964.19.4.813
56. Ulmer WT, Marek W, Rasche K. Strömungswiderstandskurven bei obstruktiven Atemwegserkrankungen. Acht Typen der Strömungswiderstandskurven unter Spontanatmung [Airway resistance curves in obstructive respiratory tract diseases. 8 types of airway resistance curves in spontaneous respiration]. Fortschr Med. 1988;106(33):663–664. German
57. Matthys H, Orth U. Comparative measurements of airway resistance. Respiration. 1975;32(2):121–134. doi:10.1159/000193642
58. Kraemer R. Whole-body plethysmography in the clinical assessment of infants with bronchopulmonary diseases. Respiration. 1993;60(1):1–8. doi:10.1159/000196165
59. Kusenbach G, Pott H, Breuer A, et al. Evaluation of a commercial infant body plethysmography. Eur Respir J. 1998;11(5):1211–1213. doi:10.1183/09031936.98.11051211
60. Zaiss AW, Matthys H. A multiuser system for whole body plethysmographic measurements and interpretation. Lung. 1990;168:Suppl:1185–92. doi:10.1007/BF02718260
61. Agostoni E, Mead J. Statics of the respiratory system. In: Fenn WO, Rahn H, editors. Handbook of Physiology. Washington D.C: American Physiological Society; 1964:411–427.
62. Mead J, Turner JM, Macklem PT, Little JB. Significance of the relationship between lung recoil and maximum expiratory flow. J Appl Physiol. 1967;22(1):95–108. doi:10.1152/jappl.1967.22.1.95
63. Duggan CJ, Castle WD, Berend N. Effects of continuous positive airway pressure breathing on lung volume and distensibility. J Appl Physiol. 1990;68(3):1121–1126. doi:10.1152/jappl.1990.68.3.1121
64. Cerfolio RJ, Bryant AS. Different diffusing capacity of the lung for carbon monoxide as predictors of respiratory morbidity. Ann Thorac Surg. 2009;88(2):405–410. doi:10.1016/j.athoracsur.2009.04.015
65. Kraemer R, Baldwin DN, Ammann RA, Frey U, Gallati S. Progression of pulmonary hyperinflation and trapped gas associated with genetic and environmental factors in children with cystic fibrosis. Respir Res. 2006;7:138. doi:10.1186/1465-9921-7-138
66. Hardie JA, Buist AS, Vollmer WM, Ellingsen I, Bakke PS, Morkve O. Risk of over-diagnosis of COPD in asymptomatic elderly never-smokers. Eur Respir J. 2002;20(5):1117–1122. doi:10.1183/09031936.02.00023202
67. Celli BR, Halbert RJ, Isonaka S, Schau B. Population impact of different definitions of airway obstruction. Eur Respir J. 2003;22(2):268–273. doi:10.1183/09031936.03.00075102
68. Hansen JE, Sun XG, Wasserman K. Spirometric criteria for airway obstruction: use percentage of FEV1/FVC ratio below the fifth percentile, not < 70%. Chest. 2007;131(2):349–355. doi:10.1378/chest.06-1349
69. Miller MR, Quanjer PH, Swanney MP, Ruppel G, Enright PL. Interpreting lung function data using 80% predicted and fixed thresholds misclassifies more than 20% of patients. Chest. 2011;139(1):52–59. doi:10.1378/chest.10-0189
70. Stocks J, Quanjer PH. Reference values for residual volume, functional residual capacity and total lung capacity. ATS workshop on lung volume measurements. official statement of the European respiratory society. Eur Respir J. 1995;8(3):492–506. doi:10.1183/09031936.95.08030492
71. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159(1):179–187. doi:10.1164/ajrccm.159.1.9712108
72. Zapletal A, Samanek M, Paul T. Lung Function in Children and Adolescents. Karger; 1987.
73. Quanjer PH, Stocks J, Polgar G, Wise M, Karlberg J, Borsboom G. Compilation of reference values for lung function measurements in children. Eur Respir J Suppl. 1989;4:184S–261S.
74. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
75. Kraemer R, Meister B. Fast real-time moment-ratio analysis of multibreath nitrogen washout in children. J Appl Physiol. 1985;59(4):1137–1144. doi:10.1152/jappl.1985.59.4.1137
76. Lum S, Stocks J, Stanojevic S, et al. Age and height dependence of lung clearance index and functional residual capacity. Eur Respir J. 2013;41(6):1371–1377. doi:10.1183/09031936.00005512
77. Stanojevic S, Wade A, Stocks J, et al. Reference ranges for spirometry across all ages: a new approach. Am J Respir Crit Care Med. 2008;177(3):253–260. doi:10.1164/rccm.200708-1248OC
78. Cole TJ, Stanojevic S, Stocks J, Coates AL, Hankinson JL, Wade AM. Age- and size-related reference ranges: a case study of spirometry through childhood and adulthood. Stat Med. 2009;28(5):880–898. doi:10.1002/sim.3504
79. Doershuk CF, Fisher BJ, Matthews LW. Specific airway resistance from the perinatal period into adulthood. Alterations in childhood pulmonary disease. Am Rev Respir Dis. 1974;109(4):452–457. doi:10.1164/arrd.1974.109.4.452
80. Beardsmore CS, Godfrey S, Shani N, Maayan C, Bar-Yishay E. Airway resistance measurements throughout the respiratory cycle in infants. Respiration. 1986;49(2):81–93. doi:10.1159/000194864
81. Yammine S, Singer F, Gustafsson P, Latzin P. Impact of different breathing protocols on multiple-breath washout outcomes in children. J Cyst Fibrosis. 2014;13(2):190–197. doi:10.1016/j.jcf.2013.08.010
82. Lange P, Celli B, Agusti A. Lung-function trajectories and chronic obstructive pulmonary disease. N Engl J Med. 2015;373(16):1575. doi:10.1056/NEJMc1510089
83. Agusti A, Faner R. Lung function trajectories in health and disease. Lancet Respir Med. 2019;7(4):358–364. doi:10.1016/S2213-2600(18)30529-0
84. Marott JL, Ingebrigtsen TS, Colak Y, Vestbo J, Lange P. Lung function trajectories leading to chronic obstructive pulmonary disease as predictors of exacerbations and mortality. Am J Respir Crit Care Med. 2020;202(2):210–218. doi:10.1164/rccm.201911-2115OC
85. Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991–996. doi:10.1016/S0140-6736(11)60990-2
86. Jakobsen M, Anker N, Dollerup J, Poulsen PB, Lange P. Study on drug costs associated with COPD prescription medicine in Denmark. Clin Respir J. 2013;7(4):328–337. doi:10.1111/crj.12010
87. Postma DS, Bush A. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909. doi:10.1016/S0140-6736(14)60446-3
88. Vestbo J, Lange P. Natural history of COPD: focusing on change in FEV1. Respirology. 2016;21(1):34–43. doi:10.1111/resp.12589
89. Lange P, Ahmed E, Lahmar ZM, Martinez FJ, Bourdin A. Natural history and mechanisms of COPD. Respirology. 2021;26(4):298–321. doi:10.1111/resp.14007
90. Diab N, Gershon AS, Sin DD, et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1130–1139. doi:10.1164/rccm.201804-0621CI
91. Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway obstruction in chronic obstructive lung disease. N Engl J Med. 1968;278(25):1355–1360. doi:10.1056/NEJM196806202782501
92. Bignon J, Khoury F, Even P, Andre J, Brouet G. Morphometric study in chronic obstructive bronchopulmonary disease. Pathologic, clinical, and physiologic correlations. Am Rev Respir Dis. 1969;99(5):669–695. doi:10.1164/arrd.1969.99.5.669
93. Higham A, Quinn AM, Cancado JED, Singh D. The pathology of small airways disease in COPD: historical aspects and future directions. Respir Res. 2019;20(1):49. doi:10.1186/s12931-019-1017-y
94. Martinez FJ, Han MK, Allinson JP, et al. At the root: defining and halting progression of early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(12):1540–1551. doi:10.1152/jappl.1967.22.1.95
95. Han MK, Steenrod AW, Bacci ED, et al. Identifying patients with undiagnosed COPD in primary care settings: insight from screening tools and epidemiologic studies. Chronic Obstr Pulm Dis. 2015;2(2):103–121. doi:10.15326/jcopdf.2.2.2014.0152
96. Lange P, Colak Y, Ingebrigtsen TS, Vestbo J, Marott JL. Long-term prognosis of asthma, chronic obstructive pulmonary disease, and asthma-chronic obstructive pulmonary disease overlap in the Copenhagen City Heart study: a prospective population-based analysis. Lancet Respir Med. 2016;4(6):454–462. doi:10.1016/S2213-2600(16)00098-9
97. Santus P, Radovanovic D, Henchi S, et al. Assessment of acute bronchodilator effects from specific airway resistance changes in stable COPD patients. Respir Physiol Neurobiol. 2014;197:36–45. doi:10.1016/j.resp.2014.03.012
98. Topalovic M, Derom E, Osadnik CR, et al. Airways resistance and specific conductance for the diagnosis of obstructive airways diseases. Respir Res. 2015;16:88. doi:10.1186/s12931-015-0252-0
99. Jarenback L, Eriksson G, Peterson S, Ankerst J, Bjermer L, Tufvesson E. Bronchodilator response of advanced lung function parameters depending on COPD severity. Int J Chron Obstruct Pulmon Dis. 2016;11:2939–2950. doi:10.2147/COPD.S111573
100. Topalovic M, Exadaktylos V, Troosters T, Celis G, Aerts JM, Janssens W. Non-linear parameters of specific resistance loops to characterise obstructive airways diseases. Respir Res. 2017;18(1):9. doi:10.1186/s12931-016-0484-7
101. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
102. McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease. N Engl J Med. 2011;365(17):1567–1575. doi:10.1056/NEJMoa1106955
103. Koo HK, Vasilescu DM, Booth S, et al. Small airways disease in mild and moderate chronic obstructive pulmonary disease: a cross-sectional study. Lancet Respir Med. 2018;6(8):591–602. doi:10.1016/S2213-2600(18)30196-6
104. Labaki WW, Gu T, Murray S, et al. Voxel-wise longitudinal parametric response mapping analysis of chest computed tomography in smokers. Acad Radiol. 2019;26(2):217–223. doi:10.1016/j.acra.2018.05.024
105. Sorkness RL, Bleecker ER, Busse WW, et al. Lung function in adults with stable but severe asthma: air trapping and incomplete reversal of obstruction with bronchodilation. J Appl Physiol. 2008;104(2):394–403. doi:10.1152/japplphysiol.00329.2007
106. Mahut B, Caumont-Prim A, Plantier L, et al. Relationships between respiratory and airway resistances and activity-related dyspnea in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2012;7:165–171. doi:10.2147/COPD.S29745
107. Crisafulli E, Pisi R, Aiello M, et al. Prevalence of small-airway dysfunction among COPD patients with different GOLD stages and its role in the impact of disease. Respiration. 2017;93(1):32–41. doi:10.1159/000452479
108. Li K, Gao Y, Pan Z, et al. Influence of emphysema and air trapping heterogeneity on pulmonary function in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:2863–2872. doi:10.2147/COPD.S221684
109. Li Y, Li XY, Yuan LR, Wang HL, Pang M. Evaluation of small airway function and its application in patients with chronic obstructive pulmonary disease (Review). Exp Ther Med. 2021;22(6):1386. doi:10.3892/etm.2021.10822
110. Gibson GJ. Pulmonary hyperinflation a clinical overview. Eur Respir J. 1996;9(12):2640–2649. doi:10.1183/09031936.96.09122640
111. Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:187–201. doi:10.2147/COPD.S38934
112. Rossi A, Aisanov Z, Avdeev S, et al. Mechanisms, assessment and therapeutic implications of lung hyperinflation in COPD. Respir Med. 2015;109(7):785–802. doi:10.1016/j.rmed.2015.03.010
113. O’Donnell DE, Bertley JC, Chau LK, Webb KA. Qualitative aspects of exertional breathlessness in chronic airflow limitation: pathophysiologic mechanisms. Am J Respir Crit Care Med. 1997;155(1):109–115. doi:10.1164/ajrccm.155.1.9001298
114. Calverley PM, Koulouris NG. Flow limitation and dynamic hyperinflation: key concepts in modern respiratory physiology. Eur Respir J. 2005;25(1):186–199. doi:10.1183/09031936.04.00113204
115. Puente-Maestu L, Stringer WW. Hyperinflation and its management in COPD. Int J Chron Obstruct Pulmon Dis. 2006;1(4):381–400. doi:10.2147/copd.2006.1.4.381
116. Santus P, Radovanovic D, Di Marco F, Raccanelli R, Valenti V, Centanni S. Faster reduction in hyperinflation and improvement in lung ventilation inhomogeneity promoted by Aclidinium compared to glycopyrronium in severe stable COPD patients. A randomized crossover study. Pulm Pharmacol Ther. 2015;35:42–49. doi:10.1016/j.pupt.2015.11.001
117. Park J, Lee CH, Lee YJ, et al. Longitudinal changes in lung hyperinflation in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:501–508. doi:10.2147/COPD.S122909
118. Poor HD, Kawut SM, Liu CY, et al. Pulmonary hyperinflation due to gas trapping and pulmonary artery size: the Mesa COPD Study. PLoS One. 2017;12(5):e0176812. doi:10.1371/journal.pone.0176812
119. Aurora P, Bush A, Gustafsson P, et al. Multiple-breath washout as a marker of lung disease in preschool children with cystic fibrosis. Am J Respir Crit Care Med. 2005;171(3):249–256. doi:10.1164/rccm.200407-895OC
120. Lowe L, Murray CS, Custovic A, Simpson BM, Kissen PM, Woodcock A. Specific airway resistance in 3-year-old children: a prospective cohort study. Lancet. 2002;359(9321):1904–1908. doi:10.1016/S0140-6736(02)08781-0
121. Subbarao P, Hulskamp G, Stocks J. Limitations of electronic compensation for measuring plethysmographic airway resistance in infants. Pediatr Pulmonol. 2005;40(1):45–52. doi:10.1002/ppul.20217
122. Matthys H, Keller R, Herzog H. Plethysmographic assessment of trapped air in man. Respiration. 1970;27(5):447–461. doi:10.1159/000192700
123. Calverley PM, Burge PS, Spencer S, Anderson JA, Jones PW. Bronchodilator reversibility testing in chronic obstructive pulmonary disease. Thorax. 2003;58(8):659–664. doi:10.1136/thorax.58.8.659
124. Bisgaard H, Nielsen KG. Plethysmographic measurements of specific airway resistance in young children. Chest. 2005;128(1):355–362. doi:10.1378/chest.128.1.355
125. Kaminsky DA. What does airway resistance tell us about lung function? Respir Care. 2012;57(1):85–96;discussion 96–9. doi:10.4187/respcare.01411
126. Eltayara L, Becklake MR, Volta CA, Milic-Emili J. Relationship between chronic dyspnea and expiratory flow limitation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;154(6 Pt 1):1726–1734. doi:10.1164/ajrccm.154.6.8970362
127. Ni Y, Yu Y, Dai R, Shi G. Diffusing capacity in chronic obstructive pulmonary disease assessment: a meta-analysis. Chron Respir Dis. 2021;18:14799731211056340. doi:10.1177/14799731211056340
128. Yanagisawa S, Ichinose M. Definition and diagnosis of asthma-COPD overlap (ACO). Allergol Int. 2018;67(2):172–178. doi:10.1016/j.alit.2018.01.002
129. Perez de Llano L, BG Cosio, Miravitlles M, Plaza V; group Cs. Accuracy of a new algorithm to identify asthma-COPD overlap (ACO) patients in a cohort of patients with chronic obstructive airway disease. Arch Bronconeumol. 2018;54(4):198–204. doi:10.1016/j.arbres.2017.10.007
130. Balasubramanian A, Kolb TM, Damico RL, Hassoun PM, McCormack MC, Mathai SC. Diffusing capacity is an independent predictor of outcomes in pulmonary hypertension associated with COPD. Chest. 2020;158(2):722–734. doi:10.1016/j.chest.2020.02.047
131. O’Donnell DE, Parker CM. COPD exacerbations. 3: pathophysiology. Review. Thorax. 2006;61(4):354–361. doi:10.1136/thx.2005.041830
132. Miravitlles M. Asthma-COPD Overlap (ACO) PRO-CON Debate. ACO: call Me by My Name. Copd. 2020;17(5):471–473. doi:10.1080/15412555.2020.1817883
133. Papi A. Asthma COPD overlap PRO-CON debate. ACO: the mistaken term. Copd. 2020;17(5):474–476. doi:10.1080/15412555.2020.1817882
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023