Back to Journals » Patient Related Outcome Measures » Volume 12
Functional Disability in Patients with Mood Disorders at St Paul’s Hospital Psychiatry Clinic, Addis Ababa, Ethiopia, 2019
Authors Tesfaye E ![]() , Kassaw C
, Kassaw C ![]() , Agenagnew L
, Agenagnew L ![]()
Received 4 December 2020
Accepted for publication 10 May 2021
Published 14 June 2021 Volume 2021:12 Pages 181—189
DOI https://doi.org/10.2147/PROM.S295680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Elias Tesfaye,1 Chalachew Kassaw,2 Liyew Agenagnew1
1Department of Psychiatry, Faculty of Medical Sciences, Institute of Health, Jimma University, Jimma, Ethiopia; 2Department of Psychiatry, College of Health Science, Dilla University, Dilla, Ethiopia
Correspondence: Chalachew Kassaw Post Box 419, Dilla, Ethiopia
Tel +251-93-709-6759
Email [email protected]
Background: Functional disability is defined as limitations in performing socially defined roles and tasks expected within a sociocultural and physical environment. Functionality is a result of good mental health care. This study aimed to assess the magnitude and determinants of functional disability among patients with a mood disorders treated at St Paul’s Hospital outpatient psychiatry clinic, Addis Ababa, Ethiopia in 2019.
Methods: This was a cross-sectional study. We used consecutive sampling to select respondents. Data were collected through face-to-face interviews using the 12-item World Health Organization Disability Assessment Schedule version 2.0. Data were entered into EpiData 3.1 and exported to SPSS 22.0 for analysis. Linear regression analysis was used to identify significant variables associated with outcomes.
Results: This study enrolled 235 respondents with a 100% nonresponse rate, and 62.5% were diagnosed with major depressive disorder. Mean disability score was 30.2%± 32.4%. Nearly a quarter of respondents had had difficulties every day with day-to-day activity for the past 30 days. Current level of improvement (no change, β=10.5, 95% CI 3.85– 17.2), relapse (β=6.15, 95% CI 1.34– 10.9) and self-stigma (β=4.36, 95% CI 1.39– 7.33) were strong predictors of disability score (P< 0.05).
Conclusion: This study found a mean disability score of 30.2%. Current level of improvement and self-stigma were variables associated with disability, so working with stakeholders to focus on patients’ clinical improvement from their illness and self-stigma will be vital to enhance their functionality.
Keywords: functional disability, mood disorder, St Paul’s hospital, Addis Ababa, Ethiopia
Introduction
Functional impairment in mental illness is a common challenge in which normal bodily functions are at less than full capacity. It ranges from a mild situation involving only a slight loss of function to total impairment.1 According to the World Health Organization (WHO) disease-burden calculation, mental disorders account for 25.3%–33.5% of all years lived with a disability in low- and middle-income countries. The most common mental disorders worldwide that cause disability are unipolar depressive disorders, schizophrenia, bipolar disorder, and alcohol-use disorders, with 19.1% being mood disorders.2
Mood disorders have a significant negative impact on daily quality of life and psychosocial functioning among patients, parents, and relatives. In a study conducted in six European countries, mood disorders were ranked second among disabling mental illnesses.3,4
Bipolar disorder has higher disability-adjusted life-years than cancer, ischemic heart disease, and neurological conditions, due to its early onset and chronicity across the life span.5
According to a WHO report, by 2030 major depressive disorder will be the leading cause of years of disability.6 Major depressive disorder is more common than chronic medical conditions, such as cardiovascular disorders. Moreover, the impairment continues even during remission from clinical symptoms.7,8
Patients with a mood disorders syndromic recovery (no longer fulfilling the formal criteria of a mood episode) do not necessarily move to a level of functioning comparable to healthy persons, which may in part be due to persistent subsyndromic symptoms.9
Among all bipolar disorder patients, only a third achieve full social and occupational recovery with interpersonal and cognitive–behavioral therapies.10,11
Mood disorders affects patient functionality by reducing their ability to perform day-to-day activities, which results in devastating losses of their contribution to family, community, and the country at large. They also cause stigma, poverty, and family burden.12–14
Factors contributing to disability in mood-disorder patients are age atonset, duration of treatment, delays in treatment, type of mood disorder, current symptom severity, self-esteem, nonadherence, stigma resistance, and internalized stigma.15–22
Despite these facts, there are few data available on functional disability in patients with mood disorders in Ethiopia. Therefore, this study aimed to examine functional disability and determinant factors among patients with mood disorders. The results might be vital for mental health professionals, policymakers, and organizations working in mental health to work on factors contributing to disability and enhance the functionality of patients with mood disorders.
Methods
Study Area, Period, and Design
This institutional-based cross-sectional study design, conducted from February 2 to March 10, 2019 at St Paul’s Hospital, Addis Ababa, capital of Ethiopia, on outpatients attending monthly psychiatry sessions. A total of 3,500 patients with mood disorders were receiving follow-up treatment.
Eligibility Criteria
Respondents with a current diagnosis of bipolar or major depressive disorder and aged ≥18 years were eligible to participate.
Respondents were diagnosed using DSM-5 criteria by a licensed psychiatrist. Exclusion criteria were were acute symptoms needing emergency treatment, comorbid physical illness (from medical records), or other mental disorders (using DSM-5 criteria).
Sample-Size Calculation and Sampling Technique
Calculation of magnitude of the outcome variable (functional disability), a continuous variable and scored out of 100, used SD (variance) from a similar previous study. To calculate sample size, a single population–proportion formula of a continuous variable (n = Z [α/2)2 σ2/d2]), and the SD from the previous study (σ2=0.18) was used,23 where n =is the required sample size — n = Z (α/2)2 σ2/d2, σ2 = 0.18:
(1.96) (1.96) (0.18) (0.82)/(0.05) (0.05) = 226
and Z the reliability coefficient at 95% confidence (1.96)
W (margin of error) = 0.05
N (nonresponse rate 10%) = 26
As such the sample size was 226+26 =252
Since the population was <10,000, a correction formula was used: nf = n/1 + n/N = 252/1+252/3,500=235
We used consecutive sampling. All respondents who came for psychiatry-outpatient visits during the data-collection period and fulfilled the inclusion criteria were selected sequentially, based on their order of arrival at the hospital.
Data-Collection Instruments
The WHO Disability Assessment Schedule (WHODAS) version 2.0 was used to assess the functional disability of patients with mental illness. This has 12 items and is scored using percentages.24
To assess internalized stigma, we used theInternalized Stigma of Mental Illness (ISMI) scale. This has a total of 24 items using a four-point Likert scale (1 = strongly agree to 4 = strongly disagree) on five subscales: alienation (six items), stereotype endorsement (seven items), discrimination experience (five items), and social withdrawal (six items).25
To assess stigma resistance, we used a subcomponent of Internalized Self-Stigma scale, which is scored on a four-point Likert scale: 1 = strongly disagree, 2 = disagree, 3 = agree, and 4= strongly agree. Scores are then summed (20 points maximum), with higher scores indicating higher resistance.26
The Rosenberg Self-Esteem Scale was used to measure self-esteem among respondents. We used ten items. Each item is scored on a four-point Likert scale: 1 = strongly disagree, 2 = disagree, 3 = agree, and 4= strongly agree. Higher scores indicate higher self-esteem.27
To measure the current clinical improvement, we used the Clinical Global Impression scale, which is scored from very much improved (1) to very much worse (7). For this study, we adapted as to fully improved (1), partially improved (2), no change (3), and relapse (4), as assessed by the clinician.26
Dependent Variable
This was functional disability.
Independent Variables
These were age, sex, educational status, occupational status, marital status, and monthly income.
These were duration of mental illness, suicide attempt(s), current clinical improvement, latency and length of treatment, age at mental illness onset, history of stopping medication, and type of diagnosis.
This study hypothesized that internalized stigma, stigma resistance, and self-esteem have a negative relationship with the functionality disability of patients with a mood disorder.
Data-Collection Procedures and Quality Control
All questionnaires were translated into the local Amharic language before data collection and back-translated to English. Finally, we used the Amharic questionnaire for data collection. Data were collected through face-to-face interviews using the WHODAS 2.0. Data collectors and supervisors were trained for 2 days on the purpose of the study, details of the questionnaire, interviewing techniques, the importance of privacy, and ensuring the confidentiality of respondents. Supervisors and investigators corrected all before data entry.
Data Processing and Analysis
Data entered into EpiData software package. After double data-entry verification, data were exported to and analyzed using the SPSS22.
Descriptive statistics such as, frequencies, percentages and cross-tabulation were calculated to see the distribution of study variables among study participants. Results are summarized using tables, graphs, and narrative descriptions.
We used bivariate logistic regression analysis at 95% confidence(P<0.25) to identifycandidate variables for multivariate linear regression analysis, which also used95% confidence(P<0.05) to determine independent predictors of the outcome variable. Logistic regression assumptionsof normality, linearity, and homogeneity of variance were checked and met. To avoid highly correlated variables, We used exploratory correlation analysis.
Results
A majority of participants were female 142 (60.4%), with mean age37.94±13.2 years, and 104 (44.3%) were single. In sum 218 (92.8%), had had some education and 93 (39.6%) were in either college or university. Around a quarter (65, 27.7%) were unemployed, and nearly half were either government or private employees (109, 46.4%). Around half (100, 42.6%) had no income, and mean monthly income was US$59.65±$85.7 (Table 1).
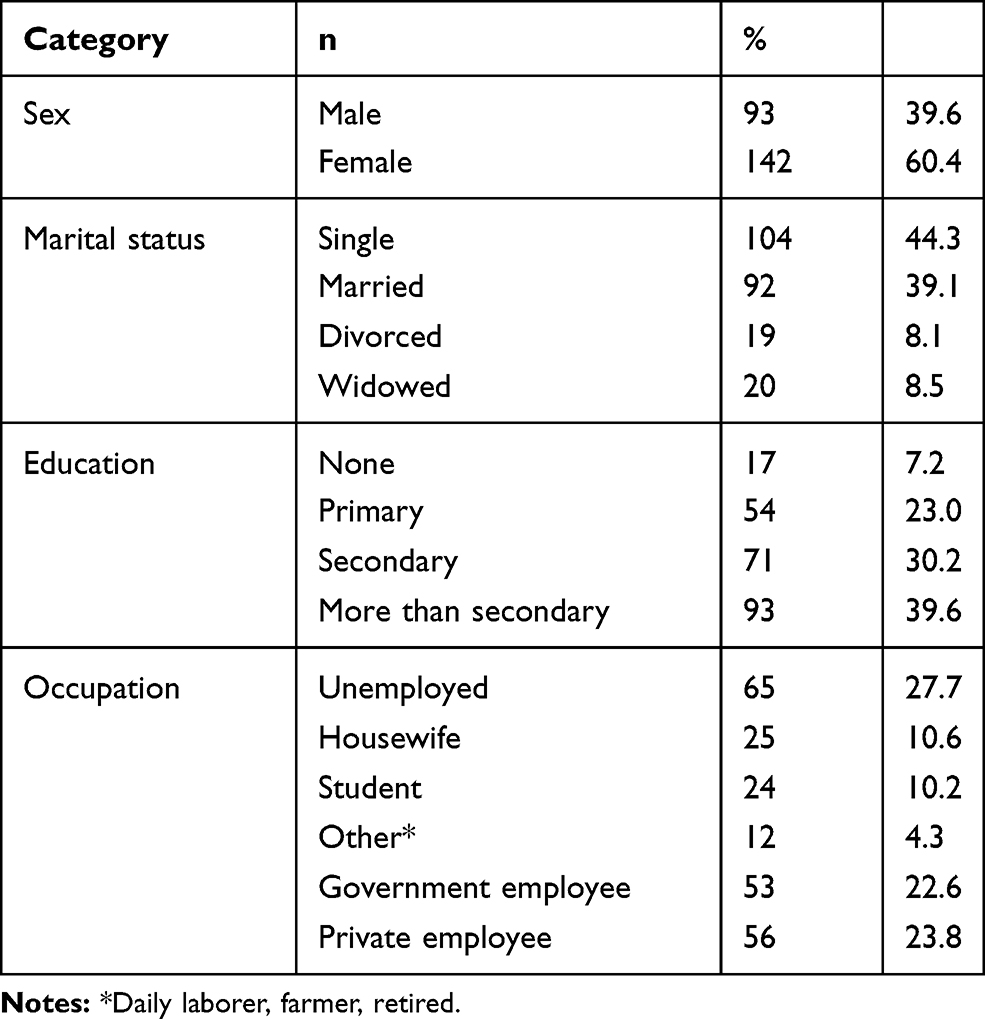 |
Table 1 Sociodemographic Characteristics of the Patients (n =235) |
Clinically Related Factors
All respondents had been diagnosed using DSM-5 criteria by a licensed psychiatrist. In total, 88 (37.4%) had bipolar disorder and nearly two-thirds (147, 62.6%) major depression disorder. Among those with bipolar disorder 88 (37.4%), 56 (63.6%) were taking carbamazepine 600–1,000 mg and the remainder (32, 36.4%) sodium valproate 800–1500 mg.
Among those with major depressive disorder (147), 95 (64.6%) were taking 75 mg amitriptyline, 30 (20.4%) fluoxetine 20 mg, and 20 (13.6%) sertraline.
Mean age of onset of illness, duration of illness, duration of treatment delay, and duration of treatment was 27.89±1.2, 10±9.4, 2.6±1.8, and 7.45±6.1 years, respectively.
A total of 203 (86.4%) respondents had current partial or ful clinical improvement. Mean of self-esteem score was 26±4 (13–37). More than a third (35.7%) had a history of suicide attempts. Half(48.5%) had a history of treatment non,adherence, and of these, almost a third (29.8%) claimed stigma play a role in their nonadherence (Table 2).
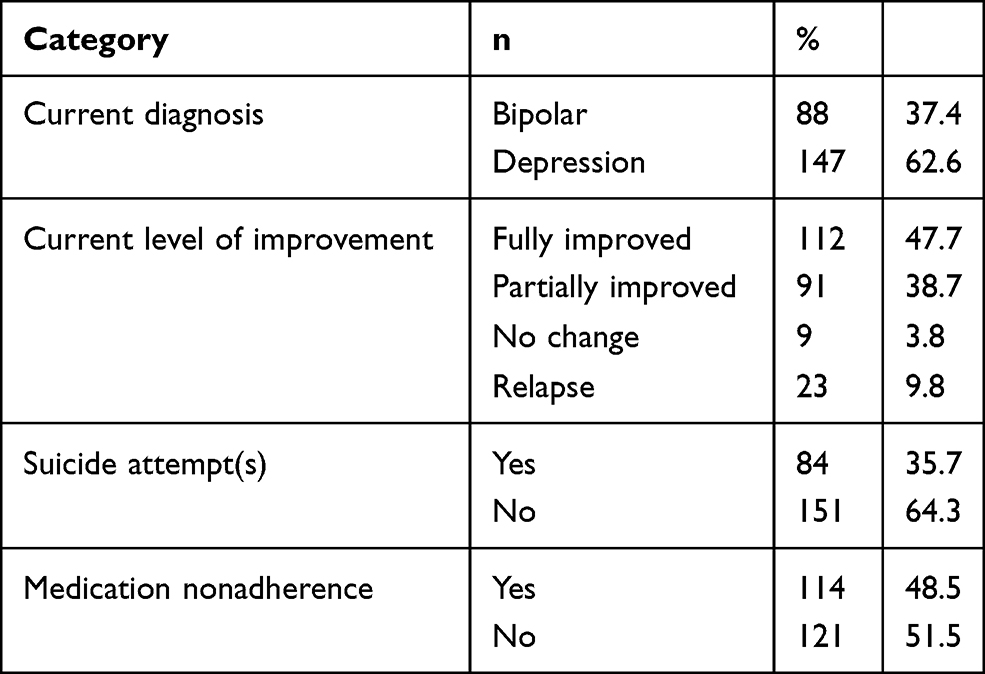 |
Table 2 Clinically Related Characteristics of Patients (n =235) |
Functionality Status (Last 30 Days)
In total, 135 (57.4%) respondents reported having had difficulties (needing to cut back) in performing their activities compared to before the illness, 71 (30.2%) were totally unable to perform their activities, and 149 (63.4%) had had difficulties present for 1–30 days.
WHODAS Scores
Mean disability score was 30.2%±32.4%, and from all the items used to measure disability, nearly half the respondents reported being extremely emotionally affected by their illness. Of these, 76% had been diagnosed with major depressive disorder (Table 3).
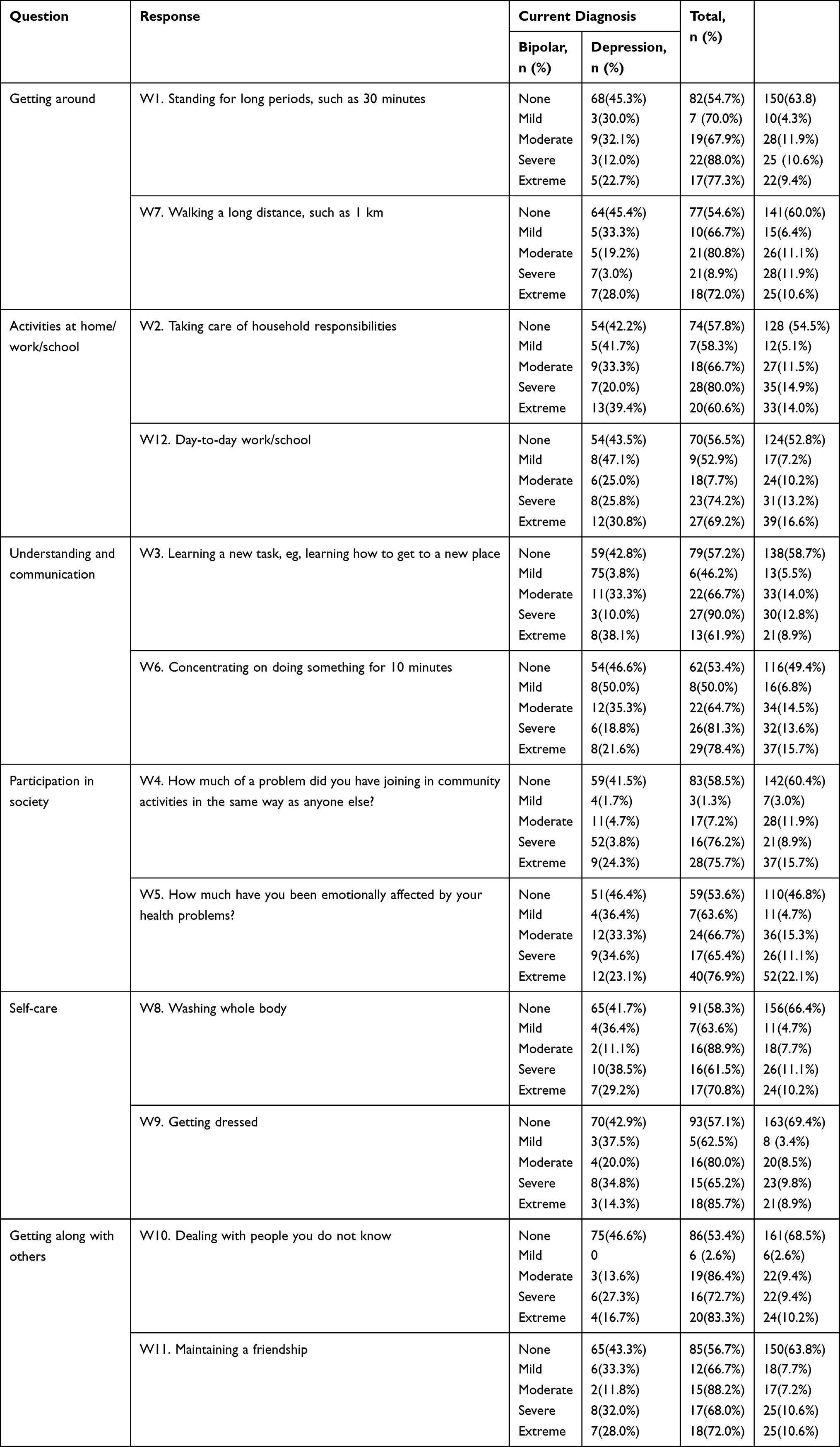 |
Table 3 WHODAS 2.0 Responses by Current Diagnosis (n=235) |
Internalized Self-Stigma Components
Thhe overall mean score on the 24-item ISMI scale was 2.2±0.63, and 80.4% of participant had responded with “agree” or “strongly agree” on at least one item Table 4).
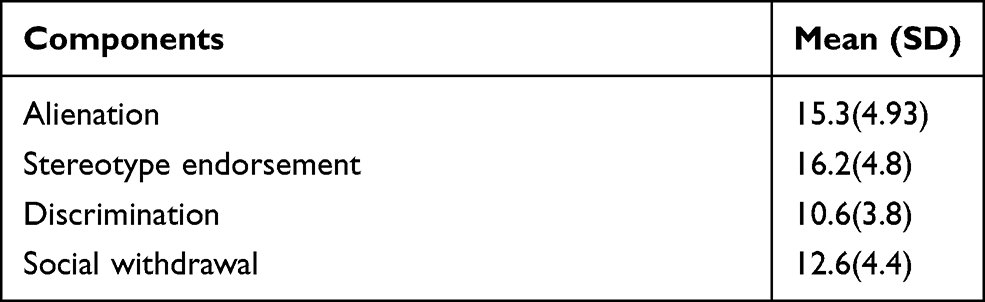 |
Table 4 Internalized Stigma Results of Respondents (n=235) |
Correlation Analysis
Respondents who reported suicide attempt(s) had high disability scores (r=1.74, P=0.007) and high self-stigma scores (r=0.463, P=0). Men had lower disability scores (r=−0.151, P=0.02; Table 5).
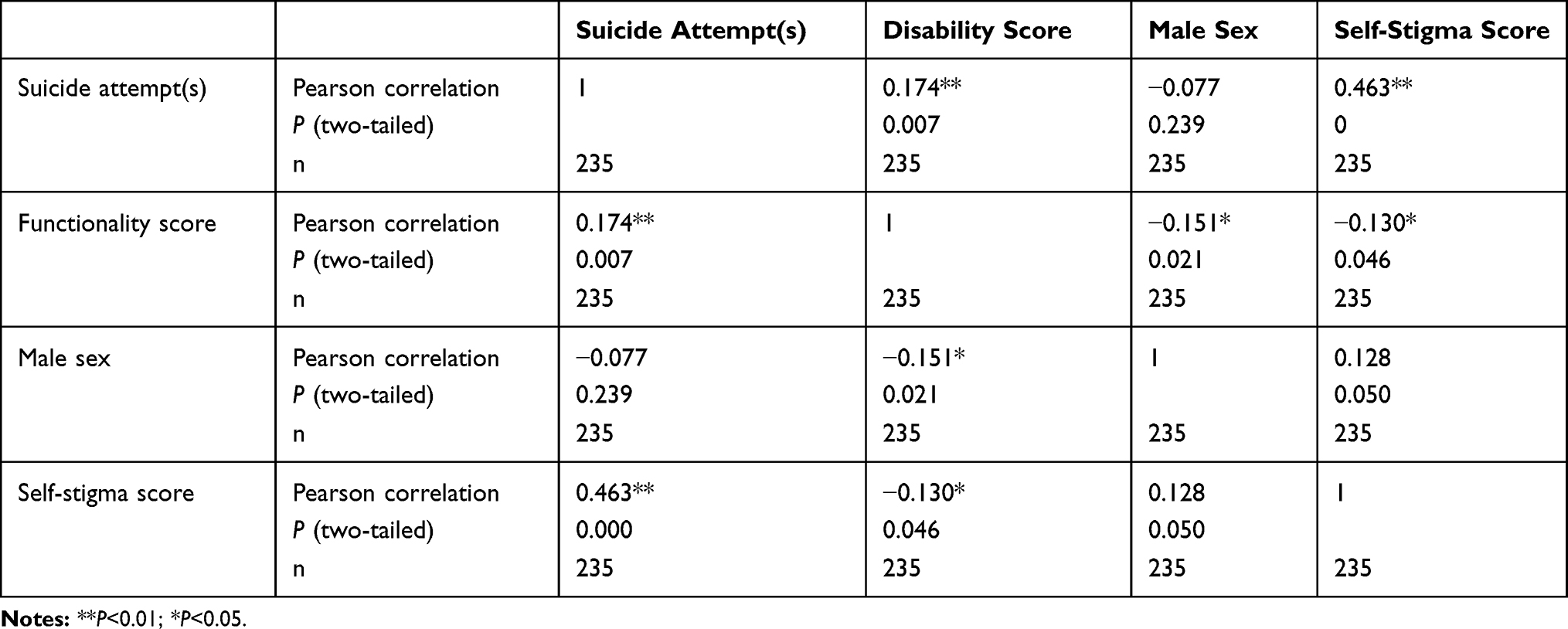 |
Table 5 Correlations among Functionality Score, Previous Suicide Attempt(s), Self-Stigma, and Sex of Respondents (n=235) |
Bivariate Linear Regression Analysis
Factors Associated with Functional Disability
Variables associated with disability on bivariate logistic regression analysis at 95% CI and P<0.25 were duration of treatment, level of improvement, suicide attempt(s), stigma resistance, self-esteem, and self-stigma and proceeded to multivariate linear regression.
Multivariate Linear Regression Analysis
On multivariate linear regression analysis (95% CI, P<0.05), variables associated with the outcome variable (functional disability) were current level of improvement (no change, β=10.5, 95% CI 3.85–17.2), relapse, (β=6.15, 95% CI 1.34–10.9), and self-stigma (β=4.36, 95% CI 1.39–7.33; Table 6).
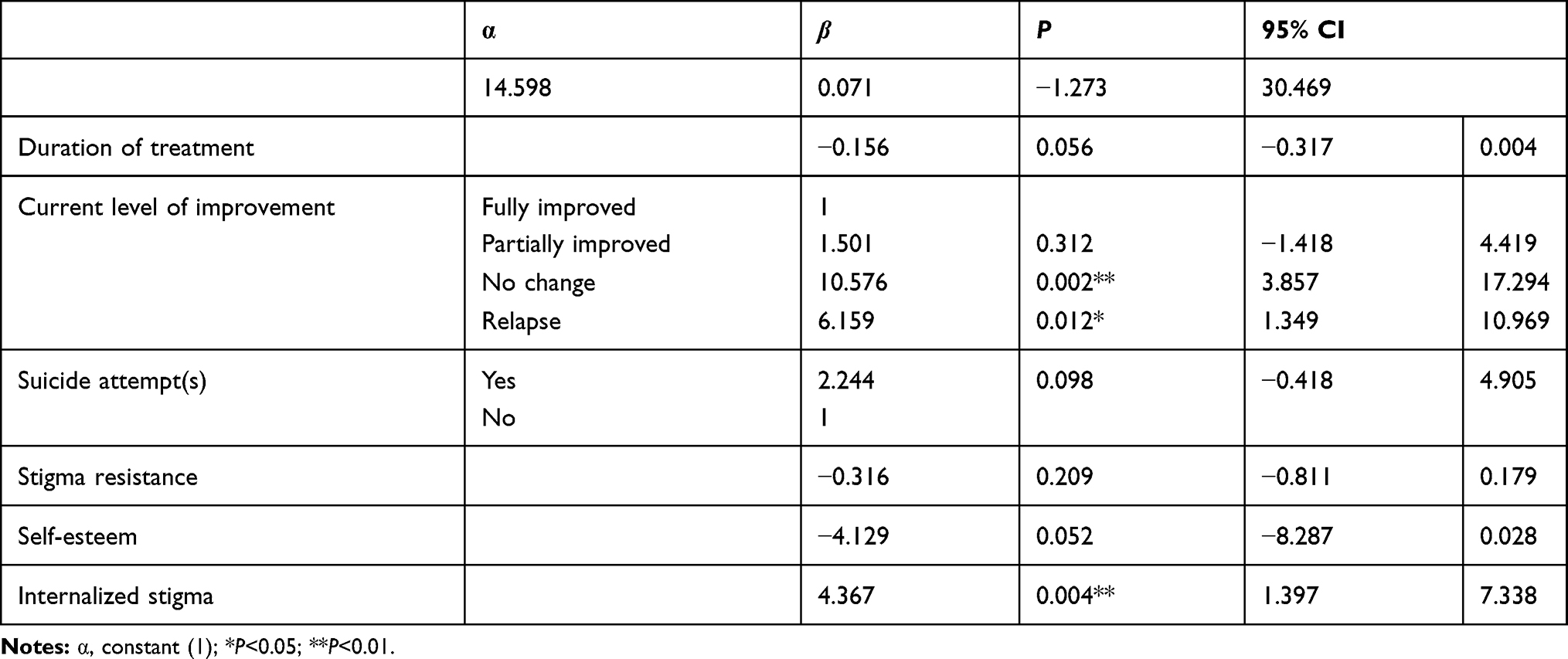 |
Table 6 Multiple Linear Regression Analysis of Respondents Attending Treatment (n=235) |
Discussion
Functional disability is a common negative consequence of mental illness that affects the cognition, interpersonal communication, self-care, and motor function of patients. The degree of impairment among mentally ill patients living in low- and middle-countries is considerable, due to various psychosocial stressors within families and communities. This study recruited patients diagnosed with a mood disorder and aimed to assess functional impairment as a result of their illness.
We found that 90% of respondents with a diagnosis of depression were severely affected in terms of learning new tasks. However, only 10% of respondents with bipolar disorder reported being were severely affected due to their illness, supported by studies conducted in the US,28 UK,29 and Canada.30 This might be explained by the nature of depression, which predominantly affects attention, concentration, memory, decision-making, motivation, and reasoning, which are vital for performing a new task.
The mean disability score in this study was 30.2%, higher than studies from Sudan (24.4%)23 and Nigeria (24.93%).23 This might be due to differences in frequency of current psychiatric diagnosis. A majority of respondents in this study were diagnosed with major depressive disorder, which is associated with high disability score.
Respondents with a history of suicidal attempts showed a 1.74-unit increase (P=0.007) in disability scores, similar to studies conducted in the US,31 sub-Saharan Africa,32 and north Africa.33 Suicidal ideation has negative consequences for self-esteem, social relationships, stigma resistance, and day-to-day activities, which are directly related to poor adherence, treatment outcomes, and functionality.
Male sex decreased disability scores 0.15 unitscompared to female sex, supported by studies conducted in Switzerland,34 London,35 and China.36 Women, have low levels of the hormone kynurenine, a metabolite of tryptophan that is responsible for speedy processing, cognition, learning, and normal psychosocial functioning.
Respondents with no change in clinical improvement showed a 10.5-unit increase in disability scores compared to those who had full improvement, in line with a community-based study conducted in Ethiopia.24
Respondents’ current clinical improvement had an impact on their self-care, social activity, emotions, work performance, and other domains of functional disability.
A one-unit increase in self-stigma scores resulted in an increasein disability scores of 4.36 units (β=4.36, 95% CI 1.39–7.33), similar to studies done in Asia37 and India.38 Self-stigma causes low self-esteem that directly affects the patient’s day-to-day activity, social interaction, community participation, and other major domains of psychosocial functioning.
Limitations
Despite this study having much strength, it has also limitations, such as recall bias for memory of age at onset and relapses, clinician bias for interpretation ofclinical improvement based on clinical experience, and social desirability bias for disclosing self-harm (suicide attempts). Inadequate data on the same population (mood disorders) hinder comparable discussion of the results. Also, the cross-sectional study nature of the study was not able to reflect the exact cause–effect relationship of the outcome variable.
Conclusion
The mean disability score in this study was 30.2%±32.4%. Relapse, internalized stigma, and patients with no change in clinical response were variables associated with disability, pointing to a need to work needed to enhance patients’ clinical improvement through integrating the biopsychosocial model treatment approach. For tackling self-stigma, giving psychoeducation, teaching coping mechanisms, which help in reducing self-criticism, and providing quality care through integrating community mental-health services will be a solution to increase the functionality of patients. There should be collaboration among patients, families, clinicians, health organizations, and the Ministry of Health addressing medication adherence and self-stigma, fundamental to clinical improvement and functionality.
Abbreviations
iISMI, Internalized Stigma of Mental Illness; WHODAS, World Health Organization Disability Assessment Schedule.
Data Sharing Statement
The data sets used/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We obtained clearance to proceed from the ethics review board of Addis Ababa University. Written informed consent was obtained from each respondent after the objectives and aims of the research had been discussed.
Acknowledgments
We would like to thank the clients who participated in the study.
Funding
This study was funded by Addis Ababa University.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Üstün B, Kennedy C. What is “functional impairment”? Disentangling disability from clinical significance. World Psychiatry. 2009;8(2):82–85. doi:10.1002/j.2051-5545.2009.tb00219.x
2. Subedi S, Shyangwa PM. Disability in mental illness: a neglected issue. J Psychiatr Assoc Nepal. 2018;7(1):1–4. doi:10.3126/jpan.v7i1.22931
3. Ma B, Wam V, Alonso J, Alonso J, Bruffaerts R, Ormel J. Functional disability of mental disorders and comparison with physical disorders: a study among the general population of six European countries. ACTA Psychiatr Scand Funct. 2006;113(6):492–500. doi:10.1111/j.1600-0447.2005.00684.x
4. Edlund MJ, Wang J, Gulledge K, et al. Which mental disorders are associated with the greatest impairment in functioning? Soc Psychiatry Psychiatr Epidemiol. 2018;53:1265–1276. doi:10.1007/s00127-018-1554-6
5. Azzam P, Obeid S, Haddad C, et al. Relationship between impulsivity and clinical and sociodemographic variables among Lebanese patients with bipolar disorder: results of a cross-sectional study. J Nerv Ment Dis. 2019;207(7):596–603. doi:10.1097/NMD.0000000000001012
6. Bonadiman CS, Passos VM, Mooney M, Naghavi M, Melo AP. The Burden of disease attributable to mental and substance use disorders in Brazil: Global Burden of Disease Study, 1990 and 2015. Rev Bras De Epidemiol. 2017;20:191–204. doi:10.1590/1980-5497201700050016
7. Chala MB, Mekonnen S, Andargie G, et al. Prevalence of disability and associated factors in Dabat Health and Demographic Surveillance System site, northwest Ethiopia. BMC Public Health. 2017;17(1):1–8. doi:10.1186/s12889-017-4763-0
8. Verduijn J, Verhoeven JE, Milaneschi Y, et al. Reconsidering the prognosis of major depressive disorder across diagnostic boundaries: full recovery is the exception rather than the rule. BMC Med. 2017;15(1):1–9. doi:10.1186/s12916-017-0972-8
9. Sanchez-Moreno J, Martinez-Aran A, Vieta E. Treatment of functional impairment in patients with bipolar disorder. Curr Psychiatry Rep. 2017;19(1):3. doi:10.1007/s11920-017-0752-3
10. Agenagnew L, Mamaru A, Hailesilassie H, et al. Disability among patients with mental illness in Jimma Town, Southwest Ethiopia, 2017, communitybased crosssectional studyquestionnaire. J Ment Health Hum Behav. 2019;24(1):27. doi:10.4103/jmhhb.jmhhb_42_19
11. Huxley N, Baldessarini RJ. Disability and its treatment in bipolar disorder patients. J Schizophernia Bipolar Disord. 2007;9(5):183–196. doi:10.1111/j.1399-5618.2007.00430.x
12. Tesfaye E, Worku B, Girma E, Agenagnew L. Internalized stigma among patients with mood disorders in Ethiopia: a cross-sectional facility-based study. Int J Ment Health Syst. 2020;14(1):1–10. doi:10.1186/s13033-020-00365-8
13. Esan O, Medubi A. The self-perceived health-care needs of patients with bipolar disorder in Nigeria. J Psycho Rehabil Ment Health. 2018;5(2):159–168. doi:10.1007/s40737-018-0120-6
14. Kebede D, Fekadu A, Teshome K, et al. Neurology, psychiatry and brain research, the 11-year functional outcome of bipolar and major depressive disorders in. Neurol Psychiatry Brain Res. 2019;32(April):68–76. doi:10.1016/j.npbr.2019.04.003
15. Brummel NE, Bell SP, Girard TD, et al. Frailty and subsequent disability and mortality among patients with critical illness. Am J Respir Crit Care Med. 2017;196(1):64–72. doi:10.1164/rccm.201605-0939OC
16. Shah A, Wheeler L, Sessions K, Kuule Y, Agaba E, Merry SP. Community perceptions of mental illness in rural Uganda: an analysis of existing challenges facing the Bwindi Mental Health Programme. African J Prim Health Care Fam Med. 2017;9(1):1–9. doi:10.4102/phcfm.v9i1.1404
17. Yoshimura Y, Bakolis I, Henderson C. Psychiatric diagnosis and other predictors of experienced and anticipated workplace discrimination and concealment of mental illness among mental health service users in England. Soc Psychiatry Psychiatr Epidemiol. 2018;53(10):1099–1109. doi:10.1007/s00127-018-1561-7
18. Bo Q, Tian L, Li F, et al. Quality of life in euthymic patients with unipolar major depressive disorder and bipolar disorder. Neuropsychiatr Dis Treat. 2019;15:1649. doi:10.2147/NDT.S201567
19. Fleury MJ, Grenier G, Bamvita JM. Associated and mediating variables related to quality of life among service users with mental disorders. Qual Life Res. 2018;27(2):491–502. doi:10.1007/s11136-017-1717-z
20. López-Villarreal A, Sánchez-Morla EM, Jiménez-López E, et al. Predictive factors of functional outcome in patients with bipolar I disorder: a five-year follow-up. J Affect Disord. 2020;272:249–258. doi:10.1016/j.jad.2020.03.140
21. Davis L, Brekke J. Social support and functional outcome in severe mental illness: the mediating role of proactive coping. Psychiatry Res. 2014;215(1):39–45. doi:10.1016/j.psychres.2013.09.010
22. Grover S, Sahoo S, Chakrabarti S, Avasthi A. Association of internalized stigma and insight in patients with schizophrenia. Int J Cult Ment Health. 2018;11(3):338–350. doi:10.1080/17542863.2017.1381750
23. Adegbaju DA, Olagunju AT, Uwakwe R. A comparative analysis of disability in individuals with bipolar affective disorder and schizophrenia in a sub-Saharan African mental health hospital: towards evidence-guided rehabilitation intervention. Soc Psychiatry Psychiatr Epidemiol. 2013;48(9):1405–1415. doi:10.1007/s00127-013-0654-6
24. Habtamu K, Medhin G, Selamu M, Tirfessa K, Hanlon C. Functional impairment among people diagnosed with depression in primary healthcare in rural Ethiopia: a comparative cross ‑ sectional study. Int J Ment Health Syst. 2019;13:1–12. doi:10.1186/s13033-019-0305-8
25. Tanabe Y, Hayashi K, Ideno Y, Birner UW, Nowak D, Sabariego C. The Internalized Stigma of Mental Illness (ISMI) scale: validation of the Japanese version. BMC Psychiatry. 2016;16:1–8. doi:10.1186/s12888-016-0825-6
26. Lau YW, Picco L, Pang S, et al. Stigma resistance and its association with internalised stigma and psychosocial outcomes among psychiatric outpatients. Psychiatry Res. 2017;257(November 2016):72–78. doi:10.1016/j.psychres.2017.07.027
27. Makhubela M, Mashegoane S. Psychological validation of the rosenberg self-esteem scale (Rses) in south africa: method effects and dimensionality in black african and white university students. J Psychol Africa. 2017;27(3):277–281. doi:10.1080/14330237.2017.1294303
28. Keller AS, Leikauf JE, Holt-Gosselin B, Staveland BR, Williams LM. Paying attention to attention in depression. Transl Psychiatry. 2019;9(1):1–12. doi:10.1038/s41398-019-0616-1
29. Rupprechter S, Stankevicius A, Huys QJM, Steele JD, Seriès P. Major depression impairs the use of reward values for decision-making. Sci Rep. 2018;8(1):1–8. doi:10.1038/s41598-018-31730-w
30. Zuckerman H, Pan Z, Park C, et al. Recognition and treatment of cognitive dysfunction in major depressive disorder. Front Psychiatry. 2018;9(December):1–11. doi:10.3389/fpsyt.2018.00655
31. Lutz J, Fiske A. Functional disability and suicidal behavior in middle-aged and older adults: a systematic critical review. J Affect Disord. 2018;227:260–271. doi:10.1016/j.jad.2017.10.043
32. Quarshie ENB, Waterman MG, House AO. Self-harm with suicidal and non-suicidal intent in young people in sub-Saharan Africa: a systematic review. BMC Psychiatry. 2020;20(1):1–26. doi:10.1186/s12888-020-02587-z
33. El Halabi S, El Hayek R, Kahil K, Nofal M, El Hayek S. Characteristics of attempted suicide in the Middle East and North Africa Region: the mediating role of arab culture and religion. Mediterr J Emerg Med Acute Care. 2020;1(3).
34. Riecher-Rössler A. Sex and gender differences in mental disorders. Lancet Psychiatry. 2017;4(1):8–9. doi:10.1016/S2215-0366(16)30348-0
35. Howard LM, Ehrlich AM, Gamlen F, Oram S. Gender-neutral mental health research is sex and gender biased. Lancet Psychiatry. 2017;4(1):9–11. doi:10.1016/S2215-0366(16)30209-7
36. Zhou Y, Zheng W, Liu W, et al. Cross-sectional relationship between kynurenine pathway metabolites and cognitive function in major depressive disorder. Psychoneuroendocrinology. 2019;101:72–79. doi:10.1016/j.psyneuen.2018.11.001
37. Sun Y, Chen G, Wang L, et al. Perception of stigma and its associated factors among patients with major depressive disorder: a multicenter survey from an Asian population. Front Psychiatry. 2019;10(MAY):1–8. doi:10.3389/fpsyt.2019.00321
38. Grover S, Hazari N, Aneja J, Chakrabarti S, Avasthi A. Stigma and its correlates among patients with bipolar disorder: a study from a tertiary care hospital of North India. Psychiatry Res. 2016;244:109–116. doi:10.1016/j.psychres.2016.07.012
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.