Back to Journals » Advances in Medical Education and Practice » Volume 16
From Theory to Clinic: Exploring Dental Student Perspectives on Preventive Dentistry in Baghdad – a Qualitative Study
Authors Alhuwaizi HR ![]() , Alzubidi MI, Alhamdani FY
, Alzubidi MI, Alhamdani FY ![]()
Received 28 August 2025
Accepted for publication 29 October 2025
Published 11 November 2025 Volume 2025:16 Pages 2063—2073
DOI https://doi.org/10.2147/AMEP.S559876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Huda Raed Alhuwaizi,1 Mohammed Ibrahim Alzubidi,1 Faaiz Yaqoub Alhamdani2
1Department of Pedodontics, Orthodontic and Preventive, Mustansiriyah University, College of Dentistry, Baghdad, Iraq; 2Department of Oral and Maxillofacial Surgery and Oral Diagnosis, Ibn Sina University of Medical and Pharmaceutical Sciences, Baghdad, Iraq
Correspondence: Huda Raed Alhuwaizi, Department of Pedodontics, Orthodontic and Preventive, Mustansiriyah University, College of Dentistry, Baghdad, Iraq, Email [email protected]
Background: Although preventive dentistry is generally acknowledged as the foundation of oral health, its actual use in clinical settings frequently takes a backseat to curative care. The viewpoints of dental students are essential for comprehending the systemic and educational elements influencing the direction of preventive care in the future.
Aim: To explore students’ opinions on preventive dentistry, related challenges, and dental students’ aspirations toward preventive dental practice.
Methods: Twenty participants were purposively sampled between 13 semi-structured interviews and one focus group discussion (seven participants), from two of the largest universities in Baghdad, both Mustansiriyah university and Baghdad University. Discussions were based on a well framed topic – guide questions that included open-ended questions. All interviews and focus group discussion were audio-recorded and transcribed verbatim. Inductive thematic analysis was used for data analysis.
Results: Findings revealed mainly negative views and experiences represented as structural barriers and cultural obstacles that students have encountered. Highlighting the significance of mentorship, communication skills, the aspirational vision students hold and the integration of theory and practice. They were grouped into four major themes: sociocultural influences on education and oral health, school curriculum issues, students’ appeal for preventive dentistry as future specialty, and challenges students encounter with preventive dentistry inside clinics. Fifteen different codes categorized these themes.
Conclusion: Dental students view the importance of prevention as a concept rather than as a clinical specialty. Although students appreciate and acknowledge the value of preventive dentistry, some systemic, educational and sociocultural barriers hamper its effective implementation. This mainly highlights the educational foundation for the subject of preventive dentistry, which does not have the required attention in dental schools. This problem is beyond mentors, curricula, and the educational establishment. It might be deeply rooted within the cultural and environmental influences. There is a need for improvement in the curricula and policies to incorporate preventive approaches more thoroughly, and empower students in a more preventive-oriented direction, which may significantly alter the way oral health care being provided.
Keywords: preventive dentistry, dental students, dental education, qualitative research
Introduction
A major public health concern is the burden of oral health worldwide.1 The great majority of oral diseases, which affect billions of people globally, can be avoided with early interventions, behavior change, and patient education.2 Many people face challenges getting dental treatment, to detect diseases and receive preventive information on how to avoid them. Infrequent dental visits decease the chances for early oral disease detection, which frequently necessitates more expensive and complex procedures.1
According to a recent report published by the World Health Organization (WHO), oral health conditions affect nearly 3.5 billion individuals worldwide, encompassing approximately two billion individuals suffering from dental caries in their permanent dentition and over half a billion children experiencing caries in their primary dentition, predominantly from middle-income countries. This highlight the urgent necessity to redirect the emphasis of dental services toward preventive measures, in accordance with WHO recommendations.3 In Iraq, the high risk of dental caries among adults and school-aged children might be associated with a lack of information about preventive measures, limited access to oral health services, high sugar intake, and inadequate fluoride exposure.4
In the past, dentistry field was thought of as a medical specialty that solely treated conditions affecting the jaws, gums, or other oral cavity conditions. Patients only sought dental care when there was an obvious need, and they did so exclusively for traditional treatments.4 Dental practitioners are anticipated to fulfill their responsibilities in the prevention of oral diseases, not only for their individual patients, but also as proponents of health promotion within the broader community.3
The principal strategy for the primary prevention of dental caries involves the dissemination of health education among the populace.5 For students to be adequately prepared for their future careers, undergraduate dental education must be effective. Educators need to come up with many ways to improve the educational experience in order to increase student learning, engagement, and motivation.6 Research indicates diverse levels of awareness and perspectives concerning preventive dental care among dental students and practicing dentists.3 Recent investigations revealed that a significant proportion of Iraqi dentists adhere to conventional invasive, non-conservative methodologies during their clinical practices, a phenomenon attributed to the nature of their undergraduate training.3
Despite being in a time where prevention is said to be better than a cure, technical and restorative skills are still given priority in dental curricula, often at the expense of preventive care. This disparity calls into question whether aspiring dentists will be prepared to provide comprehensive, preventative care.5
As there is a raising concern that dental curricula do not efficiently prepare dental students to value preventive measures in practice, this study offers important insights into how dental education and clinical practice can change for better and support a preventive approach by giving voice to students’ experiences.
Even though numerous quantitative studies have evaluated students’ understanding and knowledge of preventive measures, there is a relative lack of qualitative studies in the Middle East within this context. This study examines the subjective experiences, challenges and viewpoints that influence students’ attitudes and motivations, through their engagement with preventive dentistry while also highlighting all the gapes in the educational foundation through student perspectives.
Methodology
Study Design
A qualitative study was conducted to investigate dental student experiences and interest in preventive dentistry. A combination of two of the most widely used methods for data collection in qualitative research were used, focus group and semi-structured interviews. Discussion was moderated by the first researcher and, observed by the third researcher. The discussion reliability and flexibility were ensured, as the third researcher is a qualitative research expert and is not part of the academic staff of the universities included in the study or a preventive specialist. A set of open-ended questions was adapted based on similar literature3,7,8 and then was updated and supported by the second and the third authors based on their 30-year educational experience in this field (see supplementary file 1:Topic guide questions). The topic guide questions used first in the focus group and yielded many divers and interesting views more than was expected by the authors, and after viewing the satisfactory results, it was also used in the next 13 interviews.
Participants’ Recruitment
Data collection was carried out over a period from December 11, 2024 to February 14, 2025. This duration involved the time required for participants’ recruitment and for conducting a focus group discussion and interviews. Online class platforms were used to announce this study, to ensure diversity and accessibility. This announcement included study purpose, type of participation and participants criteria. Interested participants were given additional details and information through a social media group. Participants were chosen purposively based on their marks (including levels fair, good, and very good), background (including low and high socially and economically) and gender (including females and males), selected from two universities to ensure more diverse and high quality information. Data collection and analysis were conducted concurrently, which permitted assessment after each interview, saturation was considered reached with 20 participants, as subsequent interviews yielded no new concepts or codes. All participants were chosen from Dental School of Al- Mustansiriyah University and Dental School of Baghdad University, from both 5 year and 4 year dental students.
This inclusion aimed for information-rich participants, who had preventive dentistry course (5 year) and community dentistry courses (4 year).
The majority were of participants were female (13 females and 7 males). Females showed more interest and enthusiasm to participate in the study and share their experiences. Age ranged from 22 to 26 years for all participants. Participants’ demographic information is listed in Table 1.
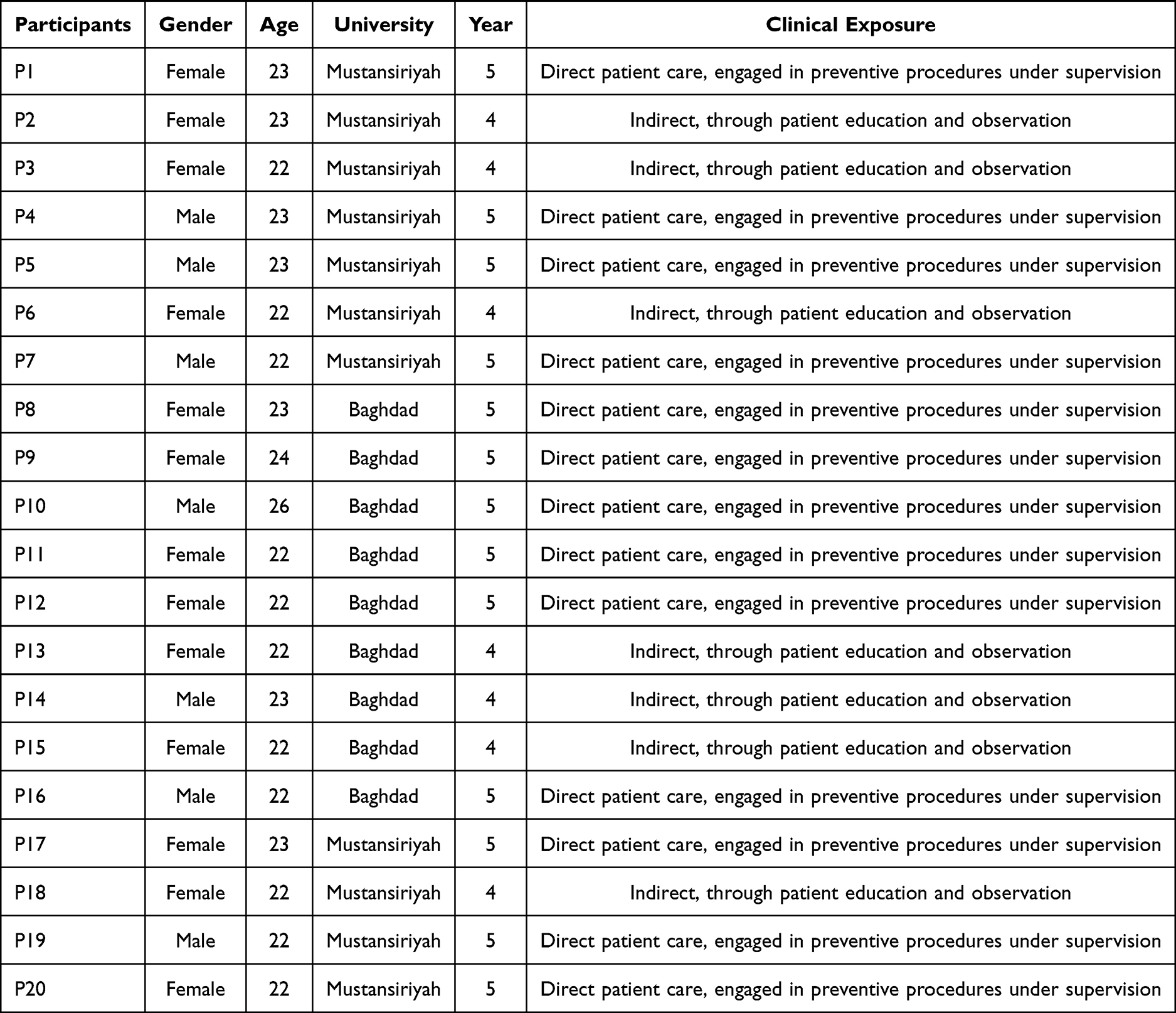 |
Table 1 Demographic Profile of the Study Participants |
Data Collection
According to9 examination process of 170 articles which revealed that focus group discussion is seldom used as the only methodology technique, therefore in this study, both focus group and interviews were utilized for data collection.
In this study one focus group (7 participants) was conducted in Al- Mustansiriyah University library discussion hall. An additional 13 semi-structured interviews were conducted, nine in Baghdad University at the prevention department discussion hall and four were held in Al- Mustansiriyah University at the library discussion hall. Discussions were based on well-framed topic-guide questions. The topic-guide questions included open-ended to allow the participants to express and share their beliefs and perspectives freely. The dialogue intended to elucidate the significance of their experiences and to reveal their lived realities.10
The focus group discussion took about 50 min, whereas each interview lasted 30–35 min. A welcoming, friendly environment was prepared with snacks and coffee to ensure the comfort of participants. The moderator (the first researcher) held the discussion with the presence of the observer (the third researcher) to monitor and supervise the efficiency and flexibility of the discussion.
Analysis
The interviews and discussion were audio recorded and transcribed verbatim. Participants’ quotes were translated to English by the first and third researchers (participants spoke in mixed Arabic and scientific-English phrases). The translation process was then checked by the third researcher and double -by the second researcher as both authors are fluent in both languages. The first researcher read the transcriptions independently multiple times to become familiar with the data.
Then codification was performed, multiple coding was implemented whereby codes serve as instrumental tools for recognizing and categorizing the concepts and topics present in the data. All the codes were initially discussed and compared by the first and the third researchers. Reflexive document, including personal thoughts and assumptions was maintained throughout the study, to reduce the influence of prior academic knowledge. Afterward, codes were arranged in tables using Microsoft Excel by the first researcher, several sheets and copies were organized to establish the Initial codes. Systematic documentation and recording of the decisions, analytical memos and the coding process was also ensured, which were revised and discussed several times by the first and third researchers. Codes were then categorized into potential themes. Next, all three researchers discussed and agreed on the final coding consensually. Codes were grouped based on relevance and similarity into themes, which captured the core patterns of participants’ narratives. Therefore, the key themes were identified, which represent the overarching concepts and subject areas prevalent within the corpus of research data.11
Analysis was done following the six-phase approach thematic analysis.12 Data analysis adapted an inductive approach in which concepts and patterns were derived from the data inductively to emerge the themes.13
Ethical Approval
Ethical approval for this study was obtained from the research ethics Scientific Committee, Al- Mustansiriyah University, College of Dentistry (no. REC193). All participants provided informed consent; they were fully informed about the purpose of the study, and their roles. Participants were informed that anonymized data and selected direct quotations might be used in a publication to illustrate study findings; however no personal identifiers would be revealed. They were given the total freedom to withdraw from the study at any time. Confidentiality was ensured by replacing participants’ names by code numbers (see Supplementary files 2 & 3: Participant information sheet and consent form).
Results
Study analysis revealed the following recurring four themes which, described dental students' experiences and interests toward preventive dentistry: sociocultural influences on education and oral health, school curriculum issues, students' appeal for preventive dentistry as future specialty, and challenges students encounter with preventive dentistry inside clinics. Each theme has its own related codes, which represent the key ideas and views discussed. In this study, each theme grouped 3–4 codes. The themes and their codes are showed in Table 2.
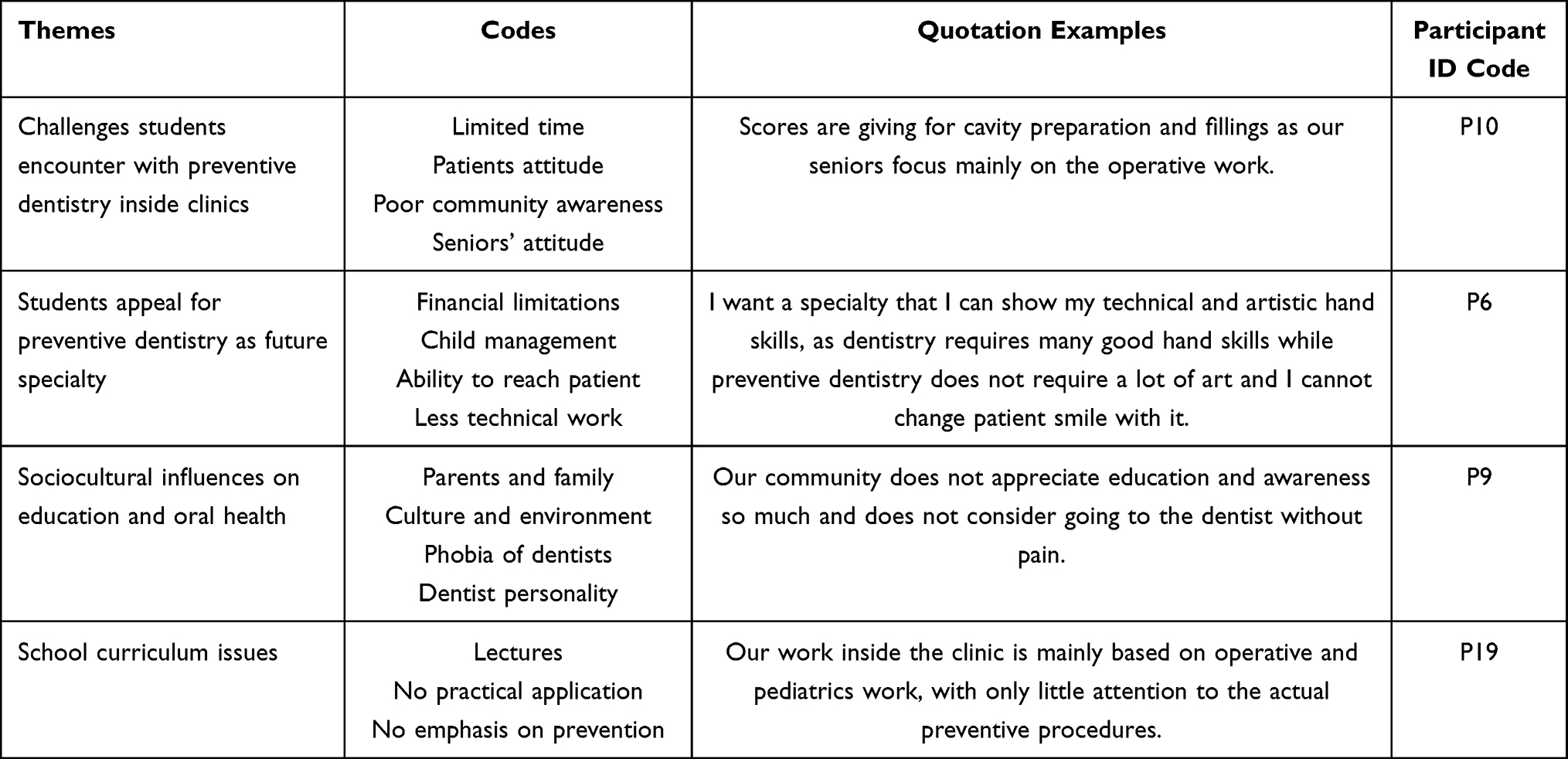 |
Table 2 Study Themes and Codes |
These findings highlighted the complexity of students’ views on preventive dentistry; however, the majority of the themes and codes were negative feedback with only a few positive in addition to some remarks suggested by the participants, which represent areas needed to improve preventive dentistry that need to be considered. Themes were analyzed and revised by the three researchers.
Challenges Students Encounter with Preventive Dentistry Inside Clinics
This theme represents all the difficulties and obstacles that dental students had experienced in their practical stage in dental prevention clinic.
Most of the participants (n =14) agreed that community awareness is very poor. Patients themselves do not seem to show any interest or attention to dental education or to learning the correct hygienic techniques and checking their teeth more often. The low educational background of patients, adds many barriers for delivering preventive messages. Students also mentioned that they do not have enough experience to create strong impact in patients with low and sometimes even no educational background. As some patients are hard to deal with, this makes it even more challenging to change their habits and beliefs.
I think that patient background and family especially for kids have the strongest influence on their habits. P15, F
Some parents are hard to talk to and leave negative impact on children. P18, F
Students also mentioned that seniors in dental prevention clinic seemed to care about the operative work much more than the preventive and educational procedures, which in turn forced students to neglect preventive care and awareness and in some cases even not consider it at all. This attitude gave students the impression that preventive dentistry is far less important and is not needed.
We are not assessed for the type of education we tell patients about in our case sheets, and only get scores for our clinical work. P16, M
This also leads us to another related challenge, as some students (n =6) talked about the setting and environment of the clinic being very stressful and uncomfortable for them. In addition, to the limited time available in clinics, which was merely enough to complete their cases, and in turn barred them from delivering a quality work and preventive consultation while concentrating on finishing the requirements instead.
It is hard to give patients a lot of time and attention because of the limited time we have at the clinic and the continuous pressure and stressful environment that forces us to finish each case at a specific time. P12, F
For me the main obstacle was the huge score requirement we are obligated to finish in the clinic despite the limited time we have making it hard to care about the educational part. P10, M
Students Appeal for Preventive Dentistry as Future Specialty
This theme was generated by student interests in preventive dentistry as a future specialty. Most of the participants (n =16) said that they would not choose prevention as a specialty, Students showed some hesitation and others even rejection for preventive dentistry as their future specialty, a variety of views were shared and discussed to explain their position. In this theme, we are discussing students’ reasons and explanations for their refusal for preventive dentistry as their future specialty.
The most agreed view was that child management is both energy- and time-consuming. On top of that, students also said that child management techniques are being delivered to them theoretically without being trained and practiced inside the clinic. Dentists need to expend a lot of effort before even starting the actual treatment, and in some cases, might even require behavior management on multiple visits to build the desired habits.
I don’t think I will choose preventive dentistry because most of the work is directed for children, and they require behavior management before starting the treatment which is very tiring and needs a lot of energy. P12, F
Despite that, some said that the lower cost of preventive procedures compared to the other treatment options is the main issue, as preventive procedures do not meet their financial expectations after graduation.
Furthermore, the ability to reach and target patients also mentioned as an important reason for not preferring preventive dentistry. Other participants (n =3) saw that sharing cases of their preventive work would not leave a strong impact in patients comparing to other specialties. Considering the power of social media nowadays and its importance to demonstrate the skills and work of dentists with their good results, students thought that preventive dentistry will decrease their chances to standout, mainly because community seems to be attracted more by aesthetic and major changes.
I don’t think that prevention as a specialty is useful for my work in clinic in the future, because I will not be able to share before and after photos for my cases, so I will not to be able to reach patients easily, and at the same time preventive procedures has the least income. P5, M
Other dental students (n =2) preferred a specialty that include some artistic and hand skills like aesthetic fillings, orthodontic and implantology.
I want a specialty that I can show my artistic hand skills as dentistry requires good hand skills and with preventive dentistry, I can’t change people smiles. P6, F
Sociocultural Influences on Education and Oral Health
This theme reflected a broader issue within dental education, students talked about all the obstacles that limit or affect the process of education from many different aspects.
The majority of participants (n = 17) noted that preventive procedures are not familiar for most of patients. A lack of education and misinformation might be the main reason for it, and that this negligent behavior is deeply rooted and tends to run in families across generations. Uncooperative parents and family tend to be a major problem because children would listen to what they are being taught by their parents. Thus, building a consistent habit is required, otherwise all the effort taken by the dentists at the clinic would be meaningless.
One visit is not enough for an educational process to change or even create some influence I will need multiple visits which is something I cannot provide as a student. P13, F
Sometimes phobia of dentists can also lead to negative responses from patients especially if fear is being transmitted to the child from mothers or even friends. However, he personality and ability of the dentist to deliver good educational knowledge with great responsibility was also mentioned as an important factor. Some students (n =5) said that some dentists are not taking the process of educating their patients seriously and that their attention is being directed only to place a treatment plan. Students believe that preventive measures are not being valued as they should be, and their significance and importance are being overlooked.
Prevention is simply based on operative and pediatric work with only few attention to the actual preventive procedures as our community does not appreciate education and awareness so much and does not consider going to the dentist without having pain. P19, M
Many patients avoid going to the dentist until having unbearable pain, because they fear injections and clinic environment. P8, F
School Curriculum Issues
This theme demonstrated students’ views toward the concept of prevention in the curriculum and at dental school with special highlight to the main issues experienced with it.
Many participants (n =14) pointed that before dental school, they had limited knowledge about the concept of prevention and oral hygiene routine or even check-up appointments referring to the limited engagement of the general population to the basic preventive measures and the great need for more educational programs and spreading more awareness.
We need more school programs because it is so important to educate people in our community since childhood. P8, F
Students also talked about the theoretical part and the lectures being given to them as not so useful; because it does not have a strong connection to the practical part and that, it has a lot of unnecessary information without emphasizing the preventive procedures and techniques. This in turn created a huge gap and confusion in students to understand the true meaning of preventive dentistry. Nevertheless, another issue raised by students was the similarity between preventive and pediatrics dentistry, which created some misunderstanding and blurred vision to the approaches, and scope each one of them addresses.
Lectures contain general information and is not so related to the practical part and there is a discrepancy between them. P1, F
There is constant repetition in lectures, and many information are repeated in different forms, which makes it harder for me to understand each meaning. P10, M
For me, preventive dentistry is not interesting like other specialties, because it does not contain many techniques and hand work to learn. P14, M
Discussion
Dental students face many difficulties as they become engaged with the dental profession.14 According to our findings, the range of challenges dental students’ face that tend to discourage their engagement with preventive dentistry include several interrelated barriers. These barriers are consistent with various literature.15,16 One major issue was the limited time inside clinics,17 which led students to emphasize on finishing the operative procedures and neglecting patient education and preventive instructions.
In addition, the influence of the clinical instructors, caring less about the preventive measures, which led to students’ discouragement from preventive dentistry. This aligns with18 findings on the challenges found to estimate students’ performance by their mentors. Dental students are influenced by their mentors not only in practice, but also in their attitudes and behaviors seeing what they prioritize as most important and what being neglected as not necessary, therefore, changing this mindset should begin with the senior staff and spread to include dental students.19
Community poor awareness and education, places another huge pressure on dental students to promote and spread preventive knowledge.20 Curative procedures are still more prevalent and valued in Iraq much more than the preventive measures.3
These findings align with prior research on the current challenges in dental education, which has also stated that any challenges during the student training process may affect their confidence and qualification during practice.18
According to our findings, preventive dentistry was not greatly wanted as a specialty mainly because preventive care is overlooked when compared to other more procedure-based specialties.21 Participants frequently expressed their concern about child management as being the major reason for not preferring prevention. As child management is not only time consuming, but also it requires a lot of energy and effort before even starting the treatment.22 Management techniques are an important means to decrease fear and stress in children during dental procedures.23 Whether it is tell-show-do technique or voice control, modeling, positive reinforcement or distraction, dental students need to become more familiar and get the necessary training to become more qualified and know the right way to manage children wisely and professionally inside the clinic.
Furthermore, the less income of all the preventive procedures comparing to other treatment options and other specialties greatly decrease students’ motivation and desire toward preventive dentistry.24 Opposed to treating more serious oral health issues, routine dental check-ups, preventive procedures, and cleaning are comparatively less expensive.25
Through acknowledging and encouraging dental students more into the concept of prevention, academic institutions should place more effort to reshape students minds into a more prevention-oriented paradigm for their professional future. In addition, enhancing the assessment system by adjusting and reshaping seniors’ behavior are needed and providing more time inside the clinics to decrease the pressure and tension students encounter as well as giving them enough time for properly educating their patients, to redirect students interest and views toward dental prevention.
Another notable aspect is the effect of cultural norms and family beliefs on oral health behavior.26 Environment and heredity have many effects on a person’s life, from the intrauterine period to the multifaceted and holistic development.23
Dental caries is quite common among Iraqi children, with rates for primary and permanent dentitions of 61% and 84%, respectively.27
The clinically documented high incidence rate of dental caries in all age categories among Iraqi populations is mostly due to the low economic status of a substantial number of households, the attitudes of the general public, sociodemographic and the low level of education.20
A recent systematic analysis discovered that school-based programs to promote dental health often had a desirable influence on adolescents and children.28 However, Information about the impact of school oral health programs on dental caries in Iraq is still missing.27
Dental students need to be trained more about preventive dentistry at a community level, so that they become able to distinguish and understand all the cultural barriers they may encounter. As an earlier study29 also emphasized on providing preventive awareness to the lower socioeconomic communities. Therefore, many educational strategies need to be considered that go beyond the clinic. Numerous activities, such as fluoride application, fissure sealant, supervised tooth brushing, and oral health education, can be incorporated into school programs.27 Furthermore, dentist personality and the communication skills, sufficient knowledge and empathy are so important in the delivery of preventive care.30
It is important that a psychological manner is applied between dentist and patient to help build trust and confidence and lessen stress and anxiety.23 Students expressed that some dentists lack the patience and empathy required, as some dentists do not see the value of prevention and education and consider dentistry only within the clinical therapeutic care,31 and this careless behavior severely affects patient compliance and response.
Communicational skills and behavioral change techniques as well as patient motivation should be emphasized in the school curriculum with an effective practical implementation inside the clinic. Dentists need to be proficient in social and interpersonal communication, use technology effectively, act professionally while adhering to ethical standards, and possess problem-solving abilities.6
However, in some cases phobia of dentists is the main barrier,32 especially when patients attend with negative expectations due to a previous unpleasant experience. Students need to educate patients more on the consequences of postponing dental visits, which might make a simple oral issue worse, necessitating more invasive procedures and specialized care over time (and thus a higher chance of experiencing physical discomfort), as well as higher treatment costs.23 Students should be aware of dental competences, which are the skills necessary for dental education. Understanding situations, demonstrating critical-thinking skills, competency, self-directed learning proficiency, problem-solving abilities, moral principles, and practical and mechanical capabilities.6 Dentists should be more educated and have the emotional intelligence to recognize patient fears, prospect, cultural diversity, and their attitude toward oral hygiene.18
Researchers argued that present curriculum and classrooms cannot give students the real practical experience they need to succeed in the profession.33 Participants reported that despite all the preventive content in lectures, students could not see the whole picture yet, because none of it is being practiced and emphasized in the clinics. This not only affect students understanding to the preventive techniques, but also gives them the wrong impression that preventive dentistry is not necessary and not needed at the clinic. It has been reported18 that the dental curriculum does not meet the population and community requirements. This might suggest changes should be implemented to connect the theoretical knowledge with the clinical practice in a more integrated curriculum that incorporate community expectations and needs.
Integrating theoretical course material, community service, and active student reflection to enable students to critically analyze the significant relationship between the community and a future health care provider.33
Numerous dental schools all over the world provide community-based training programs. This community education has many definitions in different countries and papers, however despite their variety, the conception of the importance of community education to accomplish educational goals outside the environment of dental school is the same.34
Moreover, even when it comes to lectures prevention is not being incorporated in a clear and efficient way according to some students, whether in its lectures or interventions, the attention and education is always directed to the restorative part. Academic medical curriculum lacks creative teaching methodologies, which limit future improvements.6
The dynamic process of education necessitates constant improvement. Curriculums need to embrace more technological and digital advancements to improve the teaching process. For instance, the implementation of teledentistry, particularly mobile health (m Health) applications, as clinical instruments for fostering oral health and managing oral health conditions for patients unable to access dental facilities.35 This would enhance students’ familiarization with the modern tools and techniques not only in technical skills, but also in patient communication, improving accuracy and compliance, and stimulating student critical thinking, alongside the integration of cloud-based artificial intelligence for delivering more individualized oral health management.35
Improving the curriculum with technological advancements and providing more training and requirements while also giving students sufficient clinic time are becoming necessary to overcome this gap and improve the learning process, as this may raise dentists who view preventive dentistry as an important, evolving and dynamic specialty.
Strengths and Limitations
One strength of this work is in using of two different methodologies for collecting the data: individual interviews and focus group discussions. Each one offers a different environment that we believe might have helped in this study because some participants refused to be part of a focus group discussion and felt more comfortable to share their visions in an individual interview, while other participants in contrast the dynamic and fun environment of the focus group was more encouraging to them. Within a focus group discussion, the researcher enables or oversees a collective dialogue among participants rather than engaging in direct conversation with each participant.9
One of the limitations of this study might be the timing of data collection, which happened at the end of the first course hence, students might have different opinions after the second course, as they might become more familiar and more knowledgeable about prevention. In addition, there might be a possibility for selection-bias, as the participation nature was voluntary, which may have led to only more enthused and motivated dental students participating. In addition, gender imbalance was reported, which might have limited the generalizability of the results.
Last, although inter-rater reliability was maintained through collaborative approaches and researchers discussion throughout the transcription and analytic processes to improve the credibility and consistency of the findings, a potential limitation may result inadvertently. Due to reviewers’ prior assumptions about dental education and prevention, which might have influenced the neutrality in interpreting participant perspectives; however, efforts were maintained to ensure reflexivity and trustworthiness of the analysis. Reflexive discussions, analytic memos and transparency in documenting was ensured to minimize this limitation.
In addition, special attention was given to the dynamics of the group and all participants were actively encouraged to contribute in the discussion. Moreover, quieter participants were constantly invited to share their views whenever needed in a supportive manner, while participants who tended to dominate were gently redirected by summarizing their views. This approach helped in minimizing potential bias while also collecting a wide range of views.
Conclusion
Although students appreciate and acknowledge the value of preventive dentistry, some systemic, educational and sociocultural barriers hamper its effective implementation. It seems that the educational foundation for preventive dentistry subject does not have the required attention in dental schools. This problem is beyond mentors, curricula, and the educational establishment. It might be deeply rooted within cultural and environmental influences.
School curricula should be realigned with preventive principles with strong reinforcement through clinical practice. Addressing all the barriers is necessary to develop dental professionals with prevention orientation. This study highlights student experiences and voices behind preventive dentistry in dental education.
This study offers possible opportunities to improve dental education and preventive dentistry in practice and prioritizes curriculum enhancement with special focus on providing more practical engagement for dental students inside clinic and into community programs, Future qualitative studies could build on these findings comparing and assessing the influence of prolonged preventive focused curricula.
Acknowledgments
We should like to thank and express our appreciation to every dental student who participated in this study and shared their invaluable experiences and perspectives. We also thank all the faculty members for encouraging academic growth and providing a suitable environment throughout our study.
Funding
This study is self-funded.
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Chau RC-W, Thu KM, Hsung RT-C, McGrath C, Lam WY-HJ, Dentistry P. Self-monitoring of oral health using smartphone selfie powered by artificial intelligence: implications for preventive dentistry. Oral Health Preventive Dentistry. 2024;22:5758200. doi:10.3290/j.ohpd.b5758200
2. O’Brien KJ, Forde VM, Mulrooney MA, Purcell EC, Flaherty GT. Global status of oral health provision: identifying the root of the problem. Public Health Challenges. 2022;1(1):e6. doi:10.1002/puh2.6
3. Alsheekhly B, Namdari M, Abbas MJ, Ghasemi HJC. Knowledge of and attitude toward preventive care among Iraqi dentists and senior dental students: a cross-sectional study. Cureus. 2024;16(7):e65120. doi:10.7759/cureus.65120
4. Abbasi MS, Lal A, Das G, et al. Impact of social media on aesthetic dentistry: general practitioners’ perspectives. Paper presented at: healthcare. 2022.
5. Zarnigor J, Studies M. Main role of hygienic education in the system primary prevention of dental diseases of patient. European Int J Multidisciplinary Res Manag Stud. 2023;3(11):157–163.
6. Rubaia’an MA. Dental education: a guide for novice tutors. Cureus. 2023;15(8).
7. Al-Wesabi MA. Knowledge, attitude and practice on preventive dentistry among senior dental students in Yemen. Int J Public Health Res. 2015;5(1):560–568.
8. Inci MA, Ağmaz O, Özer HJ. Evaluation of dental students’ awareness and attitude about preventive dental treatments: survey research. European Ann Dental Sci. 2021;48(Suppl 1):11–13.
9. Nyumba TO, Wilson K, Derrick CJ, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Methods Ecol Evol. 2018;9(1):20–32.
10. Ruslin R, Mashuri S, Rasak MSA, Alhabsyi F, Syam HJ. Semi-structured Interview: a methodological reflection on the development of a qualitative research instrument in educational studies. IOSR J Res Method Educ. 2022;12(1):22–29.
11. Rosairo HJ. Thematic analysis in qualitative research. J Agricultural Sci. 2023;18(3).
12. Braun V, Clarke VJ. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3(2):77–101.
13. Vears DF, Gillam L. Inductive content analysis: a guide for beginning qualitative researchers. Focus Health Prof Educ. 2022;23(1):111–127.
14. Fita S, Alshuraim F, Almulhim A, AlHumaid J, Alhareky M, Nazir MJ. Possible future career challenges and associated factors among dental students and interns. Int J Dentistry. 2020;2020(1):9730125. doi:10.1155/2020/9730125
15. Harnagea H, Couturier Y, Shrivastava R, et al. Barriers and facilitators in the integration of oral health into primary care: a scoping review. BMJ Open. 2017;7(9):e016078. doi:10.1136/bmjopen-2017-016078
16. Bracksley-O’Grady S, Anderson K, Masood MJ. Oral health academics’ conceptualisation of health promotion and perceived barriers and opportunities in dental practice: a qualitative study. BMC Oral Health. 2021;21(1):165. doi:10.1186/s12903-021-01508-0
17. Al-Omari WM. Perceived sources of stress within a dental educational environment. J Contemporary Dental Pract. 2007;6(4):64–74.
18. Annamma LM, Varma SR, Abuttayem H, et al. Current challenges in dental education-a scoping review. BMC Med Educ. 2024;24(1):1523.
19. Pizanis VG, Pizanis C. Effective and ineffective clinical teaching in dental hygiene education: a qualitative study. J Dental Educ. 2019;83(8):904–913. doi:10.21815/JDE.019.087
20. Kumail IA, Alasady MS. The impact of socioeconomic status on oral health of southern population in Iraq. Trop Med Public Heal. 2021;24.
21. Sezer B, Kolay D, Şen Yavuz B, Güneyligil Kazaz T, Kargül BJ. Motivations, attitudes for choosing dental profession and preferred dental specialties amongst Turkish dental students. European J Dental Educ. 2022;26(2):422–433. doi:10.1111/eje.12749
22. Han S-Y, Chang C-L, Wang Y-L, et al. A narrative review on advancing pediatric oral health: comprehensive strategies for the prevention and management of dental challenges in children. Children. 2025;12(3):286. doi:10.3390/children12030286
23. Silva MV, Bussadori SK, Santos EM, Rezende KM. Behaviour management of the contemporary child in paediatric dentistry: an overview of the research. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2021;21:e0209.
24. Wei L, Griffin SO, Robison VA. Disparities in receipt of preventive dental services in children from low-income families. Am J Preventive Med. 2018;55(3):e53–e60. doi:10.1016/j.amepre.2018.04.039
25. Aftab SM, Khalid I, Shabir M, et al. Explore the importance of preventive dental care in maintaining a healthy and radiant smile throughout lifetime. 2023.
26. Gomes AC, Rebelo MAB, de Queiroz AC, et al. Socioeconomic status, social support, oral health beliefs, psychosocial factors, health behaviours and health-related quality of life in adolescents. Quality Life Res. 2020;29(1):141–151. doi:10.1007/s11136-019-02279-6
27. Ghasemi H, Alautry HF, Khoshnevisan MH, Namdari MJ. Effectiveness of a school-based oral health promotion program on dental caries among Iraqi school children: a cluster randomised controlled trial. Int Dental J. 2025;75(2):744–751. doi:10.1016/j.identj.2024.07.1214
28. Minervini G, Franco R, Marrapodi MM, Di Blasio M, Ronsivalle V, Cicciù MJ. Children oral health and parents education status: a cross sectional study. BMC Oral Health. 2023;23(1):787. doi:10.1186/s12903-023-03424-x
29. Leggett H, Vinall-Collier K, Csikar J, Veronica Ann Douglas GJ. Barriers to prevention in oral health care for English NHS dental patients: a qualitative study of views from key stakeholders. BMC Oral Health. 2023;23(1):332. doi:10.1186/s12903-023-03030-x
30. Sarhan MM, Aljohani LN, Alsaleh RI, Mubaraki RA, Almozaen MA, Alharbi RS. Barriers faced by undergraduate dental students when conducting research: a qualitative study. BMC Med Educ. 2025;25(1):191. doi:10.1186/s12909-025-06790-y
31. Wagle M, Acharya G, Basnet P, Trovik TA. Knowledge about preventive dentistry versus self-reported competence in providing preventive oral healthcare–a study among Nepalese dentists. BMC Oral Health. 2017;17(1):76. doi:10.1186/s12903-017-0366-5
32. Ochshorn J, Daly KA, Zaninovic V, Heyman RE, Smith Slep AM, Wolff MS. Examining barriers and facilitators of dental fear treatment adoption: a qualitative study of practicing dentists. PLoS One. 2025;20(5):e0322884. doi:10.1371/journal.pone.0322884
33. Khabra K, Compton SM. Integrating community service-learning into a dental hygiene curriculum: a document analysis. Canadian J Dental Hygiene. 2024;58(1):26.
34. Elsheli J, Patrick A, Stokes CJ. Community‐based education programmes in the context of dental education: a scoping review. European J Dental Educ. 2024;28(2):576–590. doi:10.1111/eje.12986
35. Chau RCW, Thu KM, Chaurasia A, Hsung RTC, Lam WY. A systematic review of the use of mHealth in oral health education among older adults. Dentistry J. 2023;11(8):189. doi:10.3390/dj11080189
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Skill Retention of Light-Curing Technique Using Only Verbal Instructions versus Using an Instructional Video: A 2-Year Follow-Up Study of Dental Students
Al-Zain AO, Alsolami AH, Jamalellail HM, Price RB
Advances in Medical Education and Practice 2023, 14:391-405
Published Date: 21 April 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Evaluation of Preclinical Class II Composite Restoration Performed by Dental Students Using Analytic Rubric Parameters
Daghrery A, Pereira GKR, Bin Hassan SA, Abogazalah NN, Alamoudi NA, Alqahtani SA, Alamri MA, Algarni SA, Al Moaleem MM
Advances in Medical Education and Practice 2026, 17:594133
Published Date: 18 April 2026