Back to Journals » Journal of Pain Research » Volume 16
Fremanezumab for Episodic Migraine Prevention in Japanese Patients: Subgroup Analysis from Two International Trials
Authors Saigoh K, Takeshima T, Nakai M ![]() , Shibasaki Y, Ishida M, Ning X, Barash S, Isogai Y, Koga N
, Shibasaki Y, Ishida M, Ning X, Barash S, Isogai Y, Koga N ![]()
Received 21 October 2022
Accepted for publication 8 May 2023
Published 18 May 2023 Volume 2023:16 Pages 1673—1682
DOI https://doi.org/10.2147/JPR.S393896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Kazumasa Saigoh,1 Takao Takeshima,2 Masami Nakai,3 Yoshiyuki Shibasaki,4 Miki Ishida,5 Xiaoping Ning,6 Steve Barash,6 Yuki Isogai,4 Nobuyuki Koga7
1Department of Neurology, Kindai University School of Medicine, Osaka, Japan; 2Headache Center, Department of Neurology, Tominaga Hospital, Osaka, Japan; 3Medical Affairs, Otsuka Pharmaceutical Co, Ltd, Osaka, Japan; 4Medical Affairs, Otsuka Pharmaceutical Co, Ltd, Tokyo, Japan; 5Headquarters of Clinical Development, Otsuka Pharmaceutical Co, Ltd, Osaka, Japan; 6Teva Branded Pharmaceutical Products R&D, Inc, West Chester, PA, USA; 7Medical Affairs, Otsuka Pharmaceutical Co, Ltd, Tokushima, Japan
Correspondence: Masami Nakai, Medical Affairs, Otsuka Pharmaceutical Co., Ltd, 3-2-27 Otedori, Chuo-ku, Osaka, 540-0021, Japan, Tel +81-80-9026-3806, Email [email protected]
Purpose: The monoclonal antibody fremanezumab has been shown effective and well tolerated in numerous Phase 2 and Phase 3 trials. This subgroup analysis of the international HALO episodic migraine (EM; [NCT02629861]) trial and a similarly designed phase 2b/3 trial in Japanese and Korean patients (NCT03303092) sought to evaluate the efficacy and safety of fremanezumab in Japanese patients with EM.
Patients and Methods: In both trials, eligible patients were randomly assigned at baseline to receive subcutaneous monthly fremanezumab, quarterly fremanezumab, or placebo in a 1:1:1 ratio. The primary endpoint was the mean change from baseline in the monthly (28-day) average number of migraine days during the 12-week period after the first dose of fremanezumab or placebo. Secondary endpoints assessed other aspects of efficacy, including disability and medication use.
Results: A total of 301 patients in the Japanese and Korean phase 2b/3 trial and 75 patients in the HALO EM trial were Japanese with baseline and treatment characteristics similar between treatment groups. According to ANCOVA analysis of the primary endpoint, both fremanezumab quarterly and monthly led to greater reductions in the monthly (28-day) average number of migraine days than placebo. This was supported by MMRM analysis of the primary endpoint over the initial 4 weeks, highlighting the rapid onset of action of fremanezumab. Results of secondary endpoint analysis supported the primary endpoint analyses. Fremanezumab was well tolerated with no new safety signals seen in this population of Japanese patients.
Conclusion: Fremanezumab appears to be an effective and well-tolerated preventive medication for Japanese patients with EM.
Keywords: calcitonin gene-related peptide, episodic migraine, fremanezumab, Japanese
Introduction
Episodic migraine (EM), defined as “<15 migraine or headache days per month with or without aura”, causes less headache-related disability, impairment in quality of life, and comorbidity than chronic migraine (CM).1–3 However, EM is responsible for >90% of the migraine cases,3 and progresses to CM in a small proportion of patients annually and, conversely, CM may switch back to EM.1
Monoclonal antibodies that act on the calcitonin gene-related peptide (CGRP), a trigeminal sensory neuropeptide, or the CGRP receptor have demonstrated efficacy for migraine with good tolerability.4 On this basis, the European Headache Federation guidelines have made evidence-based recommendations regarding use of monoclonal CGRP or CGRP receptor antibodies for EM and CM prevention.5
Fremanezumab, a fully humanized monoclonal antibody, potently and selectively binds to both CGRP isoforms. The efficacy and safety of fremanezumab have been shown in phase 3 trials of EM patients,6–10 and numerous related subgroup analysis studies.11–16 The pivotal multinational phase 3 trial (HALO)6 found that, over a 12-week period, subcutaneous fremanezumab significantly reduced the mean number of monthly migraine days compared with placebo in patients with EM. Similarly, subcutaneous monthly or quarterly administration of fremanezumab has been shown to be effective and well tolerated compared with placebo for EM prevention in Japanese and Korean patients.9 In addition, the safety and tolerability of fremanezumab have been verified over a period of 52 weeks in Japanese patients with CM or EM.10
This subgroup analysis of the international HALO EM (NCT02629861) trial and a similarly designed phase 2b/3 trial in Japanese and Korean patients (NCT03303092) sought to evaluate the efficacy and safety of fremanezumab in Japanese patients with EM.
Materials and Methods
Study Design
This study is a subgroup analysis of Japanese EM patients from two multicenter, randomized, double-blind, placebo-controlled, parallel-group trials: the HALO EM (NCT02629861) trial6 and the phase 2b/3 trial in Japanese and Korean patients (NCT03303092).9 For both trials, details including study design, populations, and criteria for inclusion and exclusion have been published previously.6,9
A written informed consent form documented patient consent. The form was approved by the institutional review board or independent ethics committee/ethics committee that approved the trial protocol as outlined in the original trials (see Supplementary Table 1 and Supplementary Table 2 for list of independent ethics committees for each trial). Both trials complied with the principles of the Declaration of Helsinki and complied with the International Conference on Harmonisation Good Clinical Practice Guideline and local regulatory requirements.
Treatment
Following initial screening (Visit 1), randomization was performed in a 1:1:1 ratio at baseline (Visit 2) with eligible patients receiving monthly fremanezumab, quarterly fremanezumab, or placebo via subcutaneous injection (Supplementary Figure 1). Fremanezumab monthly group patients received fremanezumab 225 mg via single active subcutaneous injection (225 mg/1.5 mL) and placebo as two 1.5 mL injections at baseline (Visit 2) and then fremanezumab 225 mg as a single active injection (225 mg/1.5 mL) at month 1 (Visit 3) and month 2 (Visit 4). Fremanezumab quarterly group patients received fremanezumab 675 mg (3 active injections of 225 mg/1.5 mL each) at baseline (Visit 2) and placebo as a single 1.5 mL injection at month 1 (Visit 3) and month 2 (Visit 4). Placebo group patients received three 1.5 mL placebo injections at baseline (Visit 2) and a single 1.5 mL placebo injection at month 1 (Visit 3) and month 2 (Visit 4).
Outcomes
Post hoc analyses of primary and secondary outcome data collected in both clinical trials were conducted in Japanese patients only.
As noted previously in both source trials, the primary endpoint was the least square mean (LSM) change from baseline in the monthly (28-day) average number of migraine days during the 12-week period after the first dose of fremanezumab or placebo.
Secondary efficacy endpoints also related to the 12-week period after the first dose of fremanezumab or placebo as follows: (i) proportion of patients who obtained a ≥50% reduction in the monthly average number of migraine days, (ii) mean change from baseline in the monthly average number of days with use of any acute headache medications, (iii) mean change from baseline in the monthly average number of migraine days in patients not receiving concomitant preventive migraine medications. A final secondary endpoint was the mean change from baseline in disability score (based on the Migraine Disability Assessment [MIDAS] questionnaire) 4 weeks after the final (third) fremanezumab dose.17 Overall safety was also assessed in Japanese patients only from each trial.
Statistics
All randomly assigned patients who received ≥1 dose of a trial regimen in Cohort 2 comprised the safety set. The full analysis set (FAS) was equivalent to patients from the safety set with ≥10 days of baseline and post-baseline assessment data related to monthly average number of migraine days.
An analysis of covariance (ANCOVA) model was used to analyze the primary endpoint with fixed effects of treatment, sex, country, and baseline preventive medication use and covariates of baseline number of migraine days and years since migraine onset. A mixed-effects model for repeated measures (MMRM) analysis was also applied to the weekly change in average number of migraine days over the first 4 weeks after initial administration to assess the rapidity of effect in this subgroup analysis.
Secondary endpoints, also analyzed using the ANCOVA model, were the mean change from baseline in the monthly average number of days with use of any acute headache medications and the monthly average number of migraine days in patients not receiving concomitant preventive migraine medications. Differences were computed between each fremanezumab group and the placebo group, which included the two-sided 95% confidence interval (a Mantel–Haenszel estimator of the difference and its two-sided 95% confidence interval). Data from patients who had monthly variables with <10 days of data and weekly variables with <3 days of data were considered missing. A migraine day was normalized to 28 days for the monthly analysis and 7 days for the weekly analysis.
All statistical calculations used SAS version 9.4 (SAS Institute, Cary, NC).
Results
Patient Disposition and Baseline Characteristics
In the Japanese and Korean phase 2b/3 trial, a total of 301 patients were Japanese (fremanezumab monthly group, n=102; fremanezumab quarterly group, n=101; placebo group, n=98). In the HALO EM trial, a total of 75 patients were Japanese (fremanezumab monthly group, n=25; fremanezumab quarterly group, n=26; placebo group, n=24). Baseline characteristics of Japanese patients enrolled in both trials are summarized in Table 1.
 |
Table 1 Demographic and Baseline Clinical Characteristics of Japanese Patients Enrolled in the Japanese and Korean Phase 2b/3 Trial and International HALO trial6,9 |
Efficacy
The mean change from baseline in the monthly (28-day) average number of migraine days during the 12-week period (primary endpoint) by ANCOVA for both the Japanese and Korean phase 2b/3 trial and HALO trial is shown in Figure 1. Significant differences between each treatment group and placebo were observed. In the Japanese and Korean phase 2b/3 trial, the LSM (SE, 95% CI) difference in the primary endpoint compared with placebo was –3.04 (0.43, 95% CI –3.88, –2.20, p<0.0001) for the fremanezumab quarterly group and –2.90 (0.43, 95% CI −3.74, –2.06, p<0.0001) for the fremanezumab monthly group. In the HALO trial, corresponding differences in the primary endpoint compared with placebo were –2.4 (0.96, 95% CI –4.30, –0.46, p=0.0157) in the fremanezumab quarterly group and –2.9 (0.96, 95% CI –4.82, –0.97, p=0.0037) in the fremanezumab monthly group. According to the MMRM analysis of the primary endpoint, the LSM ± SE change from baseline in the average number of migraine days was significantly greater in the fremanezumab quarterly and monthly groups compared with placebo (Figure 2).
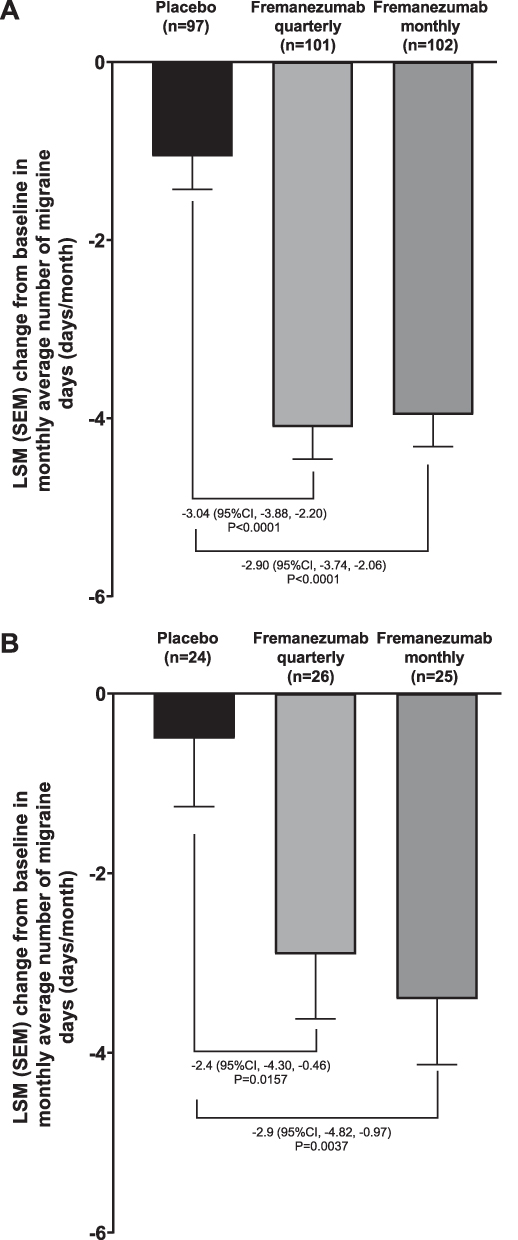 |
Figure 1 Primary endpoint according to ANCOVA analysis for Japanese patients enrolled in the (A) Japanese and Korean phase 2b/3 trial, (B) HALO trial. Abbreviations: LSM, least square mean; SEM, standard error of the mean. |
 |
Figure 2 Changes from baseline in the average number of weekly migraine days (MMRM analysis) over (A) 3 months (B) 4 weeks for Japanese patients enrolled in the Japanese and Korean phase 2b/3 trial. An asterisk (*) denotes p<0.05 and a dagger (†) denotes p<0.0001 for the comparison of fremanezumab monthly or quarterly with placebo; mixed-effects model for repeated measures (MMRM) analysis. |
Table 2 and Supplementary Table 3 summarize the results of the secondary efficacy endpoints in Japanese patients enrolled in the Japanese and Korean phase 2b/3 trial and HALO trial, respectively. In the subgroup analysis of the Japanese and Korean phase 2b/3 trial, changes in all secondary endpoints were significantly greater in both fremanezumab groups compared with placebo. Analyses of the HALO trial Japanese population were mixed with statistically significant differences between both fremanezumab groups and the placebo group noted for the monthly average number of acute medication use days during the 12-week treatment period and responder rates for the ≥50% reduction in the average number of migraine days per month.
 |
Table 2 Summary of Primary and Secondary Endpoints of Japanese Patients Enrolled in the Japanese and Korean Phase 2b/3 trial9 |
Safety
Table 3 and Supplementary Table 4 summarize the AEs that occurred in Japanese patients from the Japanese and Korean phase 2b/3 trial and HALO trial, respectively. In the analysis of Japanese patients from the Japanese and Korean phase 2b/3 trial, the incidence of AEs, including those potentially related to study medication, was similar in the placebo group to both fremanezumab groups. However, the subgroup analysis of the HALO trial showed a lower incidence of AEs in the placebo group compared with the fremanezumab groups. In both trials, the most common treatment-emergent AEs were nasopharyngitis and injection-site reactions. These tended to occur at a similar rate in placebo and fremanezumab groups in the Japanese and Korean phase 2b/3 trial analysis and a lower rate in placebo-treated patients in the HALO trial analysis.
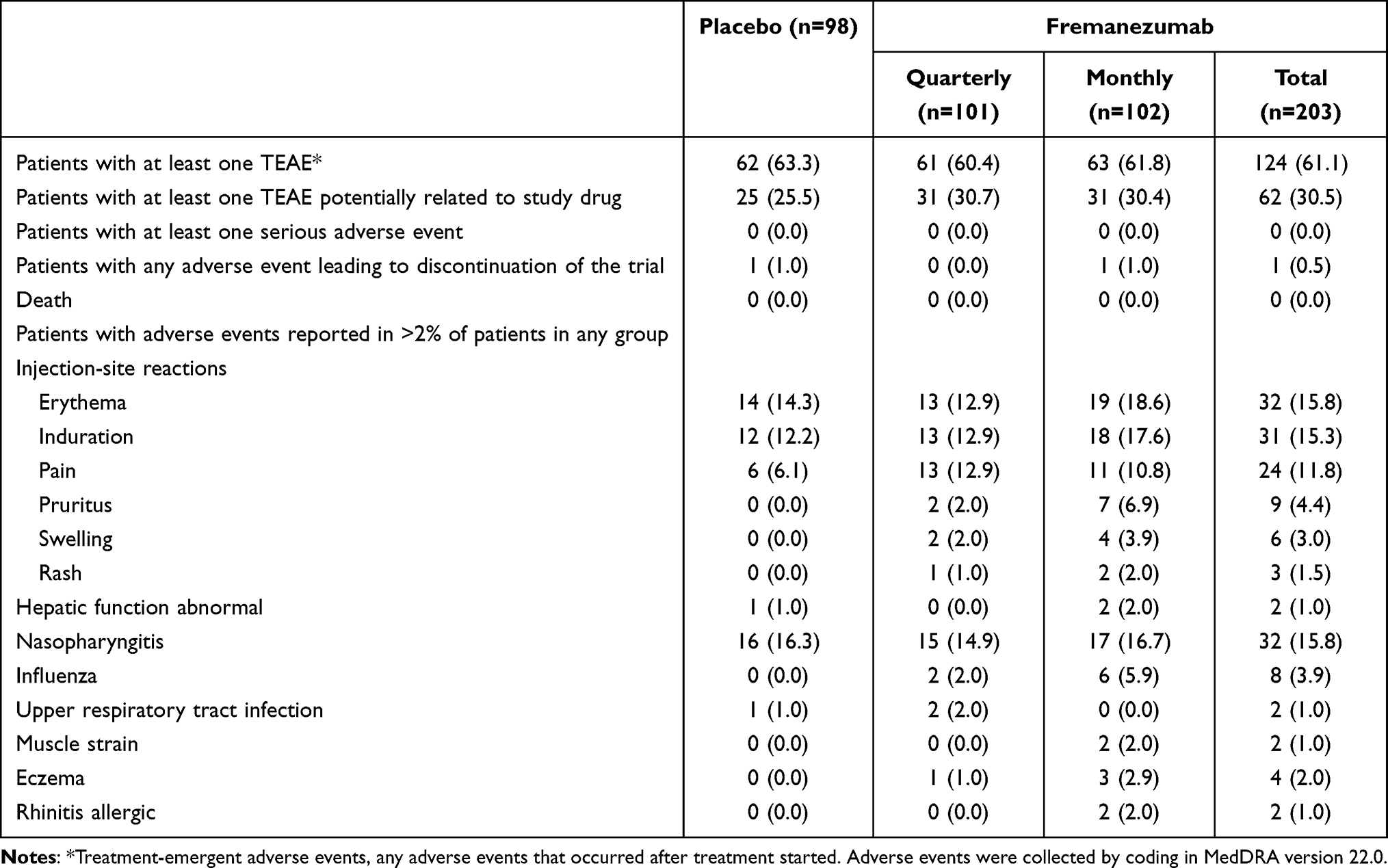 |
Table 3 Adverse Events Overall and in Patients with Incidence of Adverse Events >2% Reported in Any Treatment Group for Japanese Patients Enrolled in the Japanese and Korean Phase 2b/3 trial9 |
Discussion
The epidemiology and burden of migraine have been reported to vary among countries,18 and the efficacy of migraine prophylactic drugs in Japan may be different from that in the other countries. Thus, a subgroup analysis was performed in Japanese EM patients who live in Japan and were enrolled in two global clinical trials. This subgroup analysis of Japanese patients with EM enrolled in two trials found significant differences in the primary endpoint between fremanezumab and placebo. Results for each subgroup were very similar with those of the main trial population, thus confirming the efficacy of fremanezumab in Japanese patients. In addition, MMRM analysis of the primary endpoint over the first 4 weeks confirmed the rapid onset of action of fremanezumab as reported elsewhere in subgroup analyses of international and Japanese populations.
For secondary endpoints, the Japanese population in the HALO trial was small and the number of Japanese patients from Japanese and Korean phase 2b/3 trial alone was considered adequate enough to discuss, we mainly evaluated the result from Japanese and Korean phase 2b/3 trial. Results for all secondary efficacy endpoints in both subgroups were very similar to those from the respective main trials, thus confirming the efficacy of fremanezumab in Japanese patients with EM. Secondary efficacy endpoint results demonstrated the benefits of fremanezumab in relation to the proportion of patients with ≥50% reduction in the monthly average number of migraine days, the mean change from baseline in the monthly average number of days with use of any acute headache medication, and the MIDAS score.
The potential mechanisms involved in the association between migraine frequency and obesity are not fully understood; however, it has been suggested that obesity is a risk factor for CM.19 Previous studies have also reported that obese patients have elevated plasma CGRP levels.20 Clinically, a subgroup analysis of the PROMISE-1 and PROMISE-2 trials of the anti-CGRP antibody drug epitinezumab showed that the ≥50% migraine responder rates of both 100 mg and 300 mg doses of epitinezumab versus placebo were adversely affected in a subpopulation of EM and CM patients with obesity class II (BMI >35 kg/m2).21 Further, in patients with frequently recurrent EM and CM from the GARLIT study,22 analysis of the mean change in monthly migraine days with the anti-CGRP antibody drug galcanezumab suggested a weaker effect, as evidenced by a lower rate of persistent responders, in overweight patients than in normal weight patients.23 These results suggest that obese migraine patients may require more aggressive inhibition of the CGRP pathway to achieve similar effects to those needed in non-obese patients. In EM patients with a mean BMI range of 26.2–27.2 kg/m2 for treatment groups in the HALO trial of fremanezumab,6 the primary endpoint of mean change in monthly migraine day and the secondary endpoint of ≥50% migraine responder rate were –1.3 days and 16.5% for the quarterly group, and –1.5 days and 19.8% for the monthly group (difference vs placebo). In the Japanese subgroup of the HALO study, the mean BMI range across treatment groups was 22.9–23.3 kg/m2, and the corresponding results for the primary and secondary endpoints were –2.4 days and 26.4% for quarterly group, and –2.9 days and 26.8% for monthly group (difference vs placebo). In the Japanese subgroup of the Japanese and Korean Phase 2b/3 study, the mean BMI range was 22.5–22.8 kg/m2, and the corresponding primary and secondary endpoints were –3.04 days and 37.3% for the quarterly group, and –2.90 days and 41.2% for the monthly group (difference vs placebo). Compared with obesity class II (BMI >35 kg/m2), which affected the efficacy of epitinezumab as suggested by results of the PROMISE-1 and PROMISE-2 studies,21 the mean BMI ranges of treatment groups in the fremanezumab HALO study (26.2–27.2 kg/m2), the Japanese subgroup BMI of the HALO study (22.9–23.3 kg/m2), and the Japanese subgroup of the Japanese and Korean Phase 2b/3 study (22.5–22.8 kg/m2), were relatively low. This suggests that the marginal numerically greater effect of fremanezumab noted in the Japanese subpopulations from the two trials, compared with the overall population of the HALO trial, is unlikely to be associated with differences in BMI. In general, the Japanese population is characterized by a low prevalence of obesity. Indeed, World Health Organization data (2016) show that the prevalence of obesity (BMI ≥30 kg/m2) in Japan (male, 4.8%; female, 3.7%) is substantially lower than, for example, that of the USA (male, 35.5%; female, 37.0%).24 However, despite the fact that Japanese are characterized by a lower prevalence of obesity than Westerners, fremanezumab exposure in Japanese compared to Westerners has been shown to be approximately equivalent in an analysis of data including Phase 2b and HALO trials, and the Japanese and Korean Phase 2b/3 study (unpublished data).
In terms of safety, the most common adverse events were nasopharyngitis and injection-site reactions. The safety profiles noted in these subgroup analyses are consistent with those previously noted in several trials, including a long-term trial of Japanese EM patients.6,9,10
Limitations of this study primarily relate to those of the main trials, including difficulties in assessing the efficacy or safety of fremanezumab over evaluation periods greater than 12 weeks. Further, the trials treatment-refractory patients with three or more failed preventive drug clusters or with continuous headache were not included. However, inclusion criteria in both trials were less strict than in other trials and at least partially allowed patients who were receiving concomitant preventive medication. Finally, limitations inherent in non-prespecified post hoc analyses also apply to this subgroup analysis.
Conclusion
These results confirm the potential of fremanezumab as a preventive medication with good efficacy and tolerability profiles for Japanese patients with EM. Results of both the primary and secondary endpoint analyses were similar in Japanese patients to those of the respective main trials.
Data Sharing Statement
De-identified individual participant data underlying the results of this analysis as well as relevant study protocols may be shared with researchers to achieve aims prespecified in a methodologically sound research proposal upon request to the corresponding author (Masami Nakai).
Acknowledgments
We would like to thank all patients for their participation in the trials, and all trial sites, investigators, and all clinical research staff for their contributions. We also thank Yoshiko Okamoto, PhD, and Mark Snape, MBBS, of inScience Communications, Springer Healthcare, for helping write the outline and first draft of the manuscript. This medical writing assistance was funded by Otsuka Pharmaceutical Co., Ltd.
Disclosure
KS has received grants from Sumitomo Pharma Co., Ltd.; consulting fees from Takeda Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd.; payment for lectures from AMGEN Inc., Daiichi Sankyo Company, Eisai Co., Ltd., Eli Lilly Japan, Otsuka Pharmaceutical Co., Ltd., Sanofi Japan, Sumitomo Pharma Co., Ltd., Takeda Pharmaceutical Co., Ltd.; committee member for Japanese Society of Headache, Japanese Society of Human Genetics. TT has received honoraria for lectures from Eisai Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Amgen K.K., Eli Lilly and Company, Daiichi Sankyo; research funds under contract from Eisai Co., Ltd., Eli Lilly and Company, Amgen K.K., Allergan Japan K.K., Shionogi & Co., Ltd., Lundbeck Japan K.K. MN, YS, MI, YI, and NK are full-time employees of Otsuka Pharmaceutical Co., Ltd. XN and SB are full-time employees of Teva Branded Pharmaceutical Products. The authors report no other conflicts of interest in this work.
References
1. Katsarava Z, Buse DC, Manack AN, Lipton RB. Defining the differences between episodic migraine and chronic migraine. Curr Pain Headache Rep. 2012;16(1):86–92. doi:10.1007/s11916-011-0233-z
2. Kim SY, Park SP. The role of headache chronicity among predictors contributing to quality of life in patients with migraine: a hospital-based study. J Headache Pain. 2014;15:68. doi:10.1186/1129-2377-15-68
3. Lipton RB, Manack Adams A, Buse DC, Fanning KM, Reed ML. A comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: demographics and headache-related disability. Headache. 2016;56(8):1280–1289. doi:10.1111/head.12878
4. Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies - successful translation from bench to clinic. Nat Rev Neurol. 2018;14(6):338–350. doi:10.1038/s41582-018-0003-1
5. Sacco S, Bendtsen L, Ashina M, et al. European headache federation guideline on the use of monoclonal antibodies acting on the calcitonin gene related peptide or its receptor for migraine prevention. J Headache Pain. 2019;20(1):6. doi:10.1186/s10194-018-0955-y
6. Dodick DW, Silberstein SD, Bigal ME, et al. Effect of fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. 2018;319(19):1999–2008. doi:10.1001/jama.2018.4853
7. Ferrari MD, Diener HC, Ning X, et al. Fremanezumab versus placebo for migraine prevention in patients with documented failure to up to four migraine preventive medication classes (FOCUS): a randomised, double-blind, placebo-controlled, phase 3b trial. Lancet. 2019;394(10203):1030–1040. doi:10.1016/S0140-6736(19)31946-4
8. Goadsby PJ, Silberstein SD, Yeung PP, et al. Long-term safety, tolerability, and efficacy of fremanezumab in migraine: a randomized study. Neurology. 2020;95:e2487–2499. doi:10.1212/WNL.0000000000010600
9. Sakai F, Suzuki N, Kim BK, et al. Efficacy and safety of fremanezumab for episodic migraine prevention: multicenter, randomized, double-blind, placebo-controlled, parallel-group trial in Japanese and Korean patients. Headache. 2021;61(7):1102–1111. doi:10.1111/head.14178
10. Sakai F, Suzuki N, Ning X, et al. Long-term safety and tolerability of fremanezumab for migraine preventive treatment in Japanese outpatients: a multicenter, randomized, open-label study. Drug Saf. 2021;44(12):1355–1364. doi:10.1007/s40264-021-01119-2
11. Blumenfeld AM, Stevanovic DM, Ortega M, et al. No “wearing-off effect” seen in quarterly or monthly dosing of fremanezumab: subanalysis of a randomized long-term study. Headache. 2020;60(10):2431–2443. doi:10.1111/head.13994
12. Brandes JL, Kudrow D, Yeung PP, et al. Effects of fremanezumab on the use of acute headache medication and associated symptoms of migraine in patients with episodic migraine. Cephalalgia. 2020;40(5):470–477. doi:10.1177/0333102419885905
13. Fiedler-Kelly J, Passarell J, Ludwig E, Levi M, Cohen-Barak O. Effect of fremanezumab monthly and quarterly doses on efficacy responses. Headache. 2020;60(7):1376–1391. doi:10.1111/head.13845
14. Nahas SJ, Naegel S, Cohen JM, et al. Efficacy and safety of fremanezumab in clinical trial participants aged ≥60 years with episodic or chronic migraine: pooled results from 3 randomized, double-blind, placebo-controlled phase 3 studies. J Headache Pain. 2021;22(1):141. doi:10.1186/s10194-021-01351-2
15. Silberstein SD, Rapoport AM, Loupe PS, et al. The Effect of Beginning Treatment With Fremanezumab on Headache and Associated Symptoms in the Randomized Phase 2 Study of High Frequency Episodic Migraine: post-Hoc Analyses on the First 3 Weeks of Treatment. Headache. 2019;59(3):383–393. doi:10.1111/head.13446
16. Takeshima T, Nakai M, Shibasaki Y, et al. Early onset of efficacy with fremanezumab in patients with episodic and chronic migraine: subanalysis of two phase 2b/3 trials in Japanese and Korean patients. J Headache Pain. 2022;23(1):24. doi:10.1186/s10194-022-01393-0
17. Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001;56(6 Suppl 1):S20–8. doi:10.1212/wnl.56.suppl_1.s20
18. Stovner LJ, Nichols E, Steiner TJ. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/s1474-4422(18)30322-3
19. Ornello R, Ripa P, Pistoia F, et al. Migraine and body mass index categories: a systematic review and meta-analysis of observational studies. J Headache Pain. 2015;16:27. doi:10.1186/s10194-015-0510-z
20. Recober A, Goadsby PJ. Calcitonin gene-related peptide: a molecular link between obesity and migraine? Drug News Perspect. 2010;23(2):112–117. doi:10.1358/dnp.2010.23.2.1475909
21. Martin V, Nagy AJ, Janelidze M, et al. Impact of baseline characteristics on the efficacy and safety of eptinezumab in patients with migraine: subgroup analyses of PROMISE-1 and PROMISE-2. Clin Ther. 2022;44(3):389–402. doi:10.1016/j.clinthera.2022.01.006
22. Vernieri F, Altamura C, Brunelli N, et al. Galcanezumab for the prevention of high frequency episodic and chronic migraine in real life in Italy: a multicenter prospective cohort study (the GARLIT study). J Headache Pain. 2021;22(1):35. doi:10.1186/s10194-021-01247-1
23. Vernieri F, Brunelli N, Marcosano M, et al. Maintenance of response and predictive factors of 1-year GalcanezumAb treatment in real-life migraine patients in Italy: the multicenter prospective cohort GARLIT study. Eur J Neurol. 2023;30(1):224–234. doi:10.1111/ene.15563
24. World Health Organization. Prevalence of obesity among adults, BMI ≥ 30 (age-standardized estimate) (%); 2023. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-obesity-among-adults-bmi-=-30-(age-standardized-estimate)-(-).
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fremanezumab for Chronic Migraine Prevention in Japanese Patients: Subgroup Analysis from Two International Trials
Saigoh K, Takeshima T, Nakai M, Shibasaki Y, Ishida M, Ning X, Barash S, Isogai Y, Koga N
Journal of Pain Research 2023, 16:1311-1319
Published Date: 20 April 2023
Real-World Clinical Effectiveness and Migraine-Related Healthcare Resource Utilization in Patients Initiating Fremanezumab in Germany and the United Kingdom
Heinze A, Afridi SK, Totev TI, Krasenbaum LJ, Terasawa E, Akcicek H, Hipp J, Dhiraj D, Sun R, Yim E, Yilma B, Driessen MT
Therapeutics and Clinical Risk Management 2026, 22:529550
Published Date: 14 January 2026