Back to Journals » Clinical Interventions in Aging » Volume 21
Frailty-Informed Deprescribing of Glucose-Lowering Therapy in Older Adults with Type 2 Diabetes: A Pragmatic Clinical Framework
Authors Rangraze IR, Wali AF ![]() , Khan S, El-Tanani M
, Khan S, El-Tanani M ![]() , Matalka II, Rizzo M
, Matalka II, Rizzo M ![]() , Oo M
, Oo M
Received 6 May 2026
Accepted for publication 16 June 2026
Published 7 July 2026 Volume 2026:21 622440
DOI https://doi.org/10.2147/CIA.S622440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Imran Rashid Rangraze1, Adil Farooq Wali2, Shehla Khan1, Mohamed El-Tanani2, Ismail I Matalka1, Manfredi Rizzo1,3, Moe Oo4
1RAK College of Medical Sciences, RAK Medical and Health Sciences University, Ras Al Khaimah, United Arab Emirates; 2RAK College of Pharmacy, RAK Medical and Health Sciences University, Ras Al Khaimah, United Arab Emirates; 3School of Medicine, PROMISE Department of Health Promotion Sciences Maternal and Infantile Care, University of Palermo, Palermo, Italy; 4School of Medicine, University of Leeds, Leeds, UK
Correspondence: Imran Rashid Rangraze, Email [email protected]
Background: Older adults with type 2 diabetes are often subjected to intensive glucose-lowering therapies with a high likelihood of hypoglycaemia, falls, functional decline, and treatment burden. While international recommendations advocate for individualised glycaemic targets, they provide little clarification on when, or how, to de-intensify therapies as health status changes.
Methods: We undertook a targeted evidence synthesis of randomised controlled trials, observational cohort studies, target trial emulation studies, and international clinical guidelines focusing on glucose-lowering agents for the treatment of diabetes mellitus in patients aged 65 years and older. Evidence was synthesised and prioritised based on relevance for the important outcomes in later life, including hypoglycaemia, hospitalisation, functional decline, quality of life, and mortality. From this evidence and the principles of geriatric medicine, we constructed a pragmatic, frailty-informed clinical decision framework for the purposes of guiding deprescribing and the de-intensification of glucose-lowering therapy.
Results: Older adults in a variety of care continuum settings, particularly with frailty, multimorbidity, cognitive impairment, or a limited life expectancy, tend to stay on intensive glucose-lowering therapies for very little, if any, benefit. Target trial emulation studies and observational studies most often show that hypoglycaemia and treatment burden are lowered by de-intensifying high-risk medications, particularly insulin and sulfonylureas, without any clinically important deterioration in glycaemic control. Even with the evidence, existing guidance lacks a practical operational framework to implement such evidence in everyday clinical practice.
Conclusion: We suggest a frailty-informed clinical decision framework that integrates functional status, physiologic vulnerability, treatment-related risks, and patient preferences in making glucose-lowering treatment decisions in older adults with type 2 diabetes. This framework shifts the focus to patient safety and functional outcomes, instead of HbA1c targets, to provide a practical approach to deprescribing and de-intensifying treatment to minimise iatrogenic harm and, most importantly, to align care with the preferences of older adults.
Keywords: frailty, deprescribing, glucose-lowering therapy, older adults, type 2 diabetes
Introduction
The number of older adults living with type 2 diabetes continues to rise, reflecting population ageing and improved survival. While glucose-lowering therapy reduces microvascular complications in younger populations, the balance between benefit and harm changes substantially in later life, particularly in the presence of frailty, multimorbidity, and functional decline.1,2
Despite this shift in risk benefit profile, intensive glucose-lowering regimens remain common in routine practice.3 Many older adults continue to receive insulin or sulfonylureas even when glycaemic control is tight and expected long-term benefit is limited. This pattern reflects a persistent reliance on HbA1c-centred targets, performance metrics that prioritise biochemical outcomes over safety, and uncertainty about how and when to safely reduce treatment intensity as health status evolves.3,4
Although international guidelines increasingly advocate individualised glycaemic targets in older adults, they provide limited practical guidance on implementing de-intensification in day-to-day care.5 Consequently, treatment reduction is often delayed until after adverse events have occurred. There remains a need for a clinically usable approach that integrates frailty, functional status, treatment-related risk, and patient priorities to support proactive and safe deprescribing.6,7
This article synthesises current evidence and proposes a frailty-informed clinical decision framework to guide deprescribing and de-intensification of glucose-lowering therapy in older adults with type 2 diabetes.
To our knowledge, no existing framework integrates frailty stratification, medication risk hierarchy, and structured monitoring into a single operational deprescribing algorithm for older adults with type 2 diabetes.
Methods: Evidence Synthesis and Framework Development
This review was conducted as a targeted evidence synthesis aimed at informing development of a clinically applicable deprescribing framework. MEDLINE, Embase and the Cochrane Library were searched from inception to January 2025 using combinations of the terms: “type 2 diabetes”, “older adults”, “frailty”, “deprescribing”, “de-intensification”, “glycaemic targets”, “hypoglycaemia”, and “polypharmacy”.
We included randomised trials, observational studies, target-trial emulations, implementation studies, and major guideline statements involving adults aged ≥65 years or populations enriched for frailty. Studies focused exclusively on type 1 diabetes, gestational diabetes, perioperative glycaemic control, or intensive care settings were excluded.
Titles and abstracts were screened for relevance to deprescribing or glycaemic de-intensification in later life. Evidence was prioritised based on clinical applicability, methodological robustness, and relevance to frailty-informed decision-making. Given the heterogeneity of study designs and outcomes, formal quantitative synthesis and structured risk-of-bias scoring were not undertaken; instead, emphasis was placed on triangulation across study types and consistency of directionality of findings.
The final framework was developed iteratively through integration of published evidence, guideline recommendations, and geriatric clinical reasoning principles. Summary of Key Evidence Informing Deprescribing in Older Adults with Type 2 Diabetes are shown in Table 1.
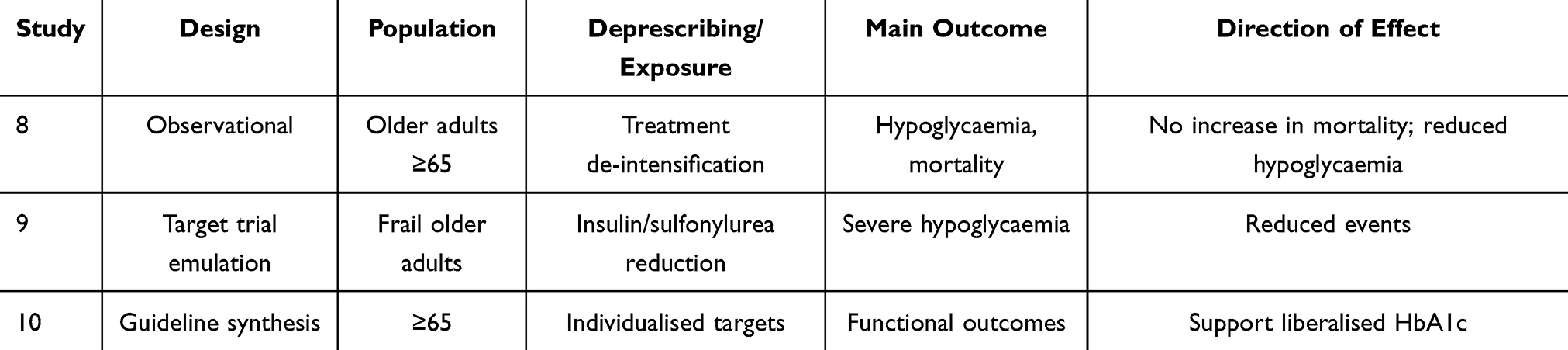 |
Table 1 Summarises Representative High-Quality Studies That Inform the Proposed Framework |
Evidence was synthesised thematically and organised into clinically relevant domains, including overtreatment, hypoglycaemia risk, frailty, functional outcomes, and implementation challenges. These themes informed development of the proposed clinical framework. To illustrate practical application of the framework, representative clinical vignettes based on common geriatric diabetes scenarios were included for educational purposes.
Why Overtreatment Persists in Older Adults with Diabetes
Overtreatment in older adults with diabetes reflects a combination of systemic, cultural, and cognitive factors. HbA1c remains the dominant marker guiding treatment intensity, despite well-recognised limitations in older populations, including altered red blood cell turnover, chronic kidney disease, anaemia, and acute illness.8–10 HbA1c also fails to capture glycaemic variability and hypoglycaemia, which are more strongly associated with adverse outcomes in later life.11,12
Clinical inertia contributes in both directions: while failure to intensify treatment is recognised in younger populations, failure to de-intensify treatment as health status changes is equally prevalent in older adults. Once initiated, glucose-lowering therapies often continue indefinitely, even as frailty, comorbidity, and life expectancy evolve.13,14
System-level incentives reinforce this pattern. Performance metrics frequently reward biochemical targets rather than safety or functional outcomes, and fragmented care can obscure responsibility for reassessing treatment intensity.15 Patients and caregivers are rarely engaged in explicit discussions about treatment trade-offs, leading to regimens that may no longer align with individual priorities.16
Frailty as the Central Determinant of Treatment Intensity
Chronological age alone provides limited guidance for diabetes management. Frailty is a multidimensional state of reduced physiological reserve and increased vulnerability to stressors and offers a more clinically meaningful basis for individualising care.17
Frailty is strongly associated with adverse outcomes related to glucose-lowering therapy, including hypoglycaemia, falls, hospitalisation, and mortality.18 It also alters the balance between short-term harm and long-term benefit. In robust older adults, moderate glycaemic control may still confer benefit, whereas in those with moderate or severe frailty, intensive control is unlikely to improve long-term outcomes and may increase immediate risk.19
Frailty further influences pharmacokinetics and pharmacodynamics through changes in renal function, body composition, sarcopenia, and cognitive capacity. These factors are poorly captured by conventional treatment algorithms but are central to safe prescribing in later life.20
Evidence Supporting De-Intensification and Deprescribing
Across observational cohorts and target trial emulation studies, de-intensification of glucose-lowering therapy in older adults has not been associated with clinically meaningful deterioration in glycaemic control. In contrast, reductions in hypoglycaemia, emergency admissions, and treatment burden are consistently observed, particularly when high-risk agents such as insulin and sulfonylureas are reduced or withdrawn.21–23 Importantly, across these studies, de-intensification was not associated with excess short-term mortality, addressing a common clinician concern.
The evidence base remains limited by a scarcity of randomised trials and heterogeneity in study populations and outcome reporting. Notably, few studies stratify outcomes by frailty status or functional impairment, limiting the applicability of trial findings to routine geriatric practice. Nonetheless, the consistency of safety-related findings across diverse settings supports a shift toward risk-based, rather than target-based, treatment decisions in older adults.24,25
Rationale for a Frailty-Informed Clinical Decision Framework
Although individualised glycaemic targets are increasingly recognised, their consistent translation into routine clinical decision-making remains limited, particularly in the context of evolving frailty and competing care priorities.
A frailty-informed framework addresses this gap by integrating four interdependent domains: physiological vulnerability, treatment-related risk, patient priorities, and anticipated clinical benefit By explicitly aligning treatment intensity with functional reserve and life expectancy, such an approach supports safer, more consistent deprescribing decisions.26
The following section presents a pragmatic stepwise framework to identify candidates for de-intensification, prioritise medication withdrawal, and monitor outcomes after treatment modification.
The Frailty-Informed Clinical Decision Framework
The proposed framework provides a structured approach to identifying overtreatment, aligning treatment goals, prioritising deprescribing actions, and monitoring outcomes. It is designed to be applied across care settings and revisited as health status evolves.
Step 1: Identify Candidates for Review
Consider deprescribing in patients with:
- HbA1c persistently <7.0% (53 mmol/mol) while on insulin or sulfonylureas
- Clinical Frailty Scale (CFS) ≥5
- Recurrent hypoglycaemia or falls
- Cognitive impairment
- Chronic kidney disease (eGFR <45 mL/min/1.73m2)
- Significant weight loss or sarcopenia
- Treatment burden or injection complexity
Frailty Assessment in Practice
The Clinical Frailty Scale (CFS) can be administered in less than two minutes during routine clinical encounters. A score ≥5 (mild frailty) should prompt reconsideration of intensive glycaemic targets and potential treatment de-intensification. Where formal frailty assessment tools are unavailable, pragmatic markers such as gait speed <0.8 m/s, unintentional weight loss, or dependence in one or more activities of daily living may serve as practical alternatives.
Step 2: Stratify Frailty and Functional Vulnerability
Frailty assessment forms the foundation of decision-making. Pragmatic measures, such as the Clinical Frailty Scale, dependence in activities of daily living, unintentional weight loss, reduced mobility, or cognitive impairment, may be used. Patients can be broadly categorised as robust, moderately frail, or severely frail.
Step 3: Evaluate Treatment-Related Risk
Treatment risk should be considered independently of frailty. High-risk features include complex insulin regimens, sulfonylurea use, renal impairment, fluctuating nutritional intake, and difficulty managing treatment complexity.
Baseline biochemical assessment should accompany evaluation of treatment-related risk. Relevant investigations include HbA1c and, where available, capillary blood glucose measurements to identify unrecognised hypoglycaemia or glycaemic variability. Renal function (eGFR and serum creatinine), urinary albumin-to-creatinine ratio, serum electrolytes, and liver function tests should also be reviewed, as organ dysfunction may alter drug handling and increase vulnerability to adverse events. The purpose of these assessments is not to support tighter glycaemic control, but rather to facilitate safe and individualised deprescribing decisions.
Step 4: Prioritise Deprescribing Actions
Deprescribing should focus first on agents most likely to cause harm or treatment burden in the context of frailty. In most cases, prioritisation follows a risk hierarchy:
- Insulin (particularly complex basal–bolus regimens)
- Sulfonylureas
- Other agents contributing to polypharmacy or treatment complexity
Insulin remains a leading contributor to hypoglycaemia and regimen burden in older adults, particularly in the presence of cognitive impairment, renal dysfunction, or variable nutritional intake. Sulfonylureas similarly carry substantial hypoglycaemia risk and are often appropriate early targets for dose reduction or discontinuation.
Dose reductions should generally proceed gradually (for example, 10–20% insulin reduction every 1–2 weeks), with closer monitoring in those with preserved endogenous insulin secretion. Regimen simplification is often preferable to abrupt discontinuation, allowing incremental assessment of clinical response and minimising anxiety related to treatment change.
Deprescribing should typically proceed one medication at a time to facilitate attribution of effects and reduce clinical uncertainty.
Step 5: Monitor and Reassess
Reassess within 2–4 weeks after dose adjustment in frail patients and within 4–8 weeks in robust older adults. Monitoring should prioritise symptomatic hyperglycaemia, hypoglycaemia episodes, falls, functional decline, and weight change rather than HbA1c alone.
Figure 1 summarises the frailty-informed clinical decision framework, outlining a stepwise approach to identifying overtreatment, stratifying risk, aligning treatment goals, and implementing safe deprescribing and monitoring strategies.
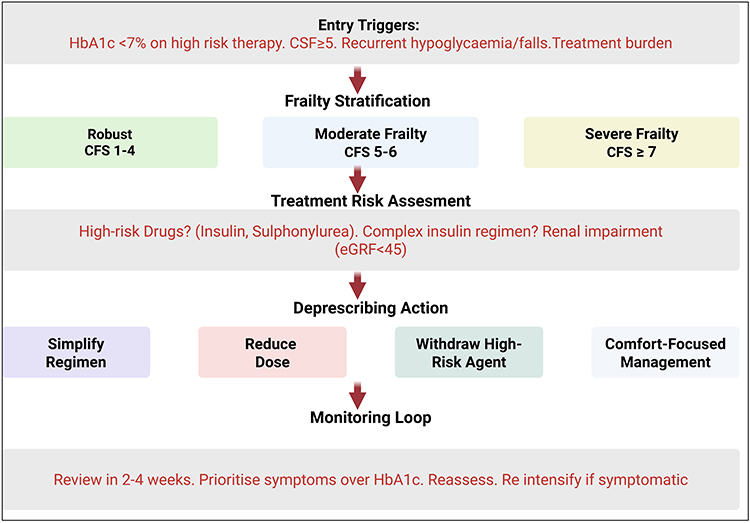 |
Figure 1 Frailty-Informed Deprescribing Algorithm for Older Adults with Type 2 Diabetes. Proposed stepwise clinical framework to guide de-intensification of glucose-lowering therapy in older adults. The algorithm begins with identification of patients at risk of overtreatment (eg, HbA1c <7% on high-risk therapy, recurrent hypoglycaemia, Clinical Frailty Scale ≥5, or high treatment burden), followed by frailty stratification, treatment risk assessment, prioritisation of deprescribing actions, and structured monitoring. Emphasis is placed on simplifying regimens, reducing hypoglycaemia risk, and aligning glycaemic targets with functional status and patient goals. Regular reassessment ensures that treatment remains aligned with evolving health status and care goals. Importantly, re-intensification should be considered only when clinically indicated and consistent with patient priorities. Abbreviation: CFS, Clinical Frailty Scale. |
Implementing Deprescribing in Clinical Practice
Deprescribing and de-intensification of glucose-lowering therapy should be undertaken as a deliberate, supervised clinical process rather than as an ad hoc response to adverse events. When approached systematically, treatment reduction can improve safety and reduce treatment burden while maintaining symptom control and patient confidence. This section outlines practical considerations for implementing the frailty-informed framework in routine care.6
Clinical Readiness and Documentation
Before de-intensifying therapy, clinicians should confirm that treatment reduction is clinically appropriate and aligned with the patient’s priorities. This requires review of recent hypoglycaemic events, functional status, comorbid conditions, and overall goals of care. Clear documentation of the rationale for deprescribing—particularly when driven by frailty, functional decline, or hypoglycaemia risk is essential to ensure continuity across care settings and to reduce the likelihood of inappropriate re-intensification by other clinicians.27
Communication with patients and caregivers should emphasise that deprescribing represents an active safety-focused intervention rather than withdrawal of care.
Tapering versus Discontinuation
The choice between dose reduction and discontinuation depends on the medication involved, duration of therapy, and patient vulnerability. Gradual dose reduction is often preferable for agents such as insulin, allowing monitoring for symptomatic hyperglycaemia and minimising anxiety related to abrupt change. Abrupt discontinuation may be appropriate for low-dose agents or medications posing immediate risk, provided appropriate follow-up is in place. In general, deprescribing should proceed one medication at a time to facilitate attribution of effects and reduce clinical uncertainty.28
Monitoring and Reassessment
Following de-intensification, monitoring should prioritise clinical outcomes over isolated biochemical changes. In frail older adults, symptoms of hyperglycaemia, functional change, falls, or treatment-related distress are more informative than modest increases in HbA1c. Follow-up intervals should be individualised, with closer monitoring during the weeks immediately after treatment changes. Deprescribing should be viewed as a dynamic process, with reassessment as health status or goals of care evolve.29
Recognising When to Pause or Reverse Deprescribing
Deprescribing is reversible. Re-intensification may be appropriate in the presence of symptomatic hyperglycaemia, acute intercurrent illness, or a change in care priorities. Decisions to re-escalate therapy should be guided by clinical status rather than biochemical thresholds alone, particularly in the absence of symptoms or functional deterioration.30
Drug-Specific Considerations in Older Adults
Different classes of glucose-lowering therapies pose distinct risks and benefits in later life.
Understanding these differences is essential for prioritising deprescribing decisions within a frailty-informed approach.24,31 Figure 2 presents a drug-specific deprescribing priority matrix stratified by patient vulnerability and treatment-related risk.
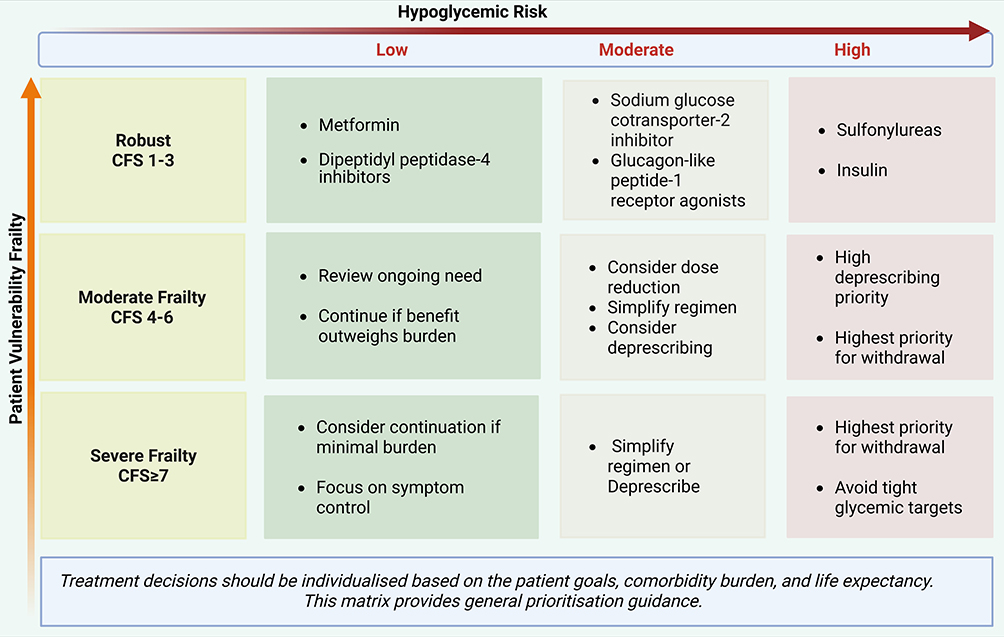 |
Figure 2 Drug Class Prioritisation for Deprescribing Based on Frailty and Hypoglycaemia Risk. Matrix illustrating relative deprescribing priority of glucose-lowering drug classes according to patient vulnerability (frailty severity) and hypoglycaemia risk. In robust individuals, continuation of low-risk agents may be appropriate, whereas in moderate to severe frailty, high-risk therapies such as insulin and sulfonylureas warrant early review and potential withdrawal. The matrix supports individualised decision-making that balances safety, treatment burden, and patient-centred outcomes. |
Insulin
Insulin remains a leading cause of iatrogenic harm in older adults, particularly when delivered using complex basal–bolus regimens. Frailty, cognitive impairment, renal dysfunction, and variable nutritional intake increase susceptibility to hypoglycaemia and dosing errors. In many cases, simplification to a lower-dose basal regimen can substantially reduce risk while maintaining symptom control. Complete withdrawal may be appropriate when insulin was initiated for transient indications or when goals of care have shifted toward comfort-focused management.
Sulfonylureas
Sulfonylureas are consistently associated with hypoglycaemia in older adults, especially in the presence of renal impairment or irregular eating patterns. These agents should be among the first considered for dose reduction or discontinuation, particularly when glycaemic control is tight or hypoglycaemic events have occurred.32
SGLT2 Inhibitors
Sodium–glucose cotransporter 2 (SGLT2) inhibitors are associated with a low intrinsic risk of hypoglycaemia and may confer cardiovascular and renal benefits in selected populations. However, in older adults—particularly those with frailty—their use warrants careful reassessment. Risks related to volume depletion, dehydration, postural hypotension, genitourinary infections, and unintentional weight loss may outweigh potential long-term benefits, especially in individuals with limited physiological reserve or reduced life expectancy. In such contexts, continuation should be guided by tolerability, functional status, and patient priorities rather than disease-specific indications alone.33
GLP-1 Receptor Agonists
Glucagon-like peptide-1 receptor agonists have minimal hypoglycaemia risk when used without insulin or sulfonylureas, but their role in frail older adults is complex. Gastrointestinal adverse effects, appetite suppression, and weight loss may contribute to sarcopenia and functional decline in vulnerable individuals. While these agents may be appropriate in robust older adults, ongoing reassessment is required as frailty progresses. Discontinuation should be considered when treatment burden increases or when goals of care shift away from long-term cardiometabolic risk reduction.34
DPP-4 Inhibitors
Dipeptidyl peptidase-4 inhibitors are generally well tolerated, carry a low risk of hypoglycaemia, and impose minimal treatment burden. Although their glycaemic efficacy is modest, they may be reasonable to continue in older adults when symptom control is required and other agents have been withdrawn. Nonetheless, in advanced frailty or limited life expectancy, even low-risk therapies should be reviewed to ensure ongoing alignment with patient priorities.35
Case Vignettes: Applying the Frailty-Informed Framework in Practice
Case 1: Overtreatment in a Robust Older Adult
A 68-year-old man with a 12-year history of type 2 diabetes is reviewed in primary care. He is independent in all activities of daily living, physically active, and cognitively intact. His HbA1c is 6.3% (45 mmol/mol). Current treatment includes metformin, a sulfonylurea, and basal insulin. He reports intermittent dizziness but no documented severe hypoglycaemia.
Application of the framework identifies a mismatch between treatment intensity and physiological vulnerability. Although robust, the patient is exposed to unnecessary hypoglycaemia risk. Following shared decision-making, the sulfonylurea is discontinued and the insulin dose reduced. At follow-up, HbA1c rises modestly to 7.1% (54 mmol/mol), with resolution of dizziness and no hypoglycaemic episodes.
This case illustrates that even in robust older adults, de-intensification may be appropriate when treatment-related risk outweighs anticipated benefit.
Case 2: Moderate Frailty and Recurrent Hypoglycaemia
An 82-year-old woman with long-standing type 2 diabetes lives independently but requires assistance with medication management and shopping. She has stage 3 chronic kidney disease and has experienced two falls in the past year. Her HbA1c is 6.7% (50 mmol/mol). She is treated with a basal–bolus insulin regimen.
Frailty assessment indicates moderate frailty with high vulnerability to treatment-related harm. Care priorities focus on safety and maintenance of independence. Mealtime insulin is discontinued and the regimen simplified to low-dose basal insulin, with monitoring directed toward symptoms rather than tight biochemical targets.
Over three months of follow-up, no further hypoglycaemic episodes or falls occur, and the patient reports reduced treatment burden and improved confidence.
Case 3: Advanced Frailty and Limited Life Expectancy
A 90-year-old man with advanced dementia, severe frailty, and multiple comorbidities is admitted with pneumonia. He is dependent for all activities of daily living and receives insulin and oral glucose-lowering agents. HbA1c is 6.9% (52 mmol/mol).
Within the framework, diabetes management is aligned with comfort-focused care. Non-essential glucose-lowering agents are discontinued, and insulin is reduced to conservative doses used only if symptomatic hyperglycaemia develops. During admission and subsequent care, no symptomatic hyperglycaemia is observed.
This case highlights the shift from long-term metabolic targets to symptom control and harm avoidance in advanced frailty.
Summary of Clinical Application
Across these scenarios, the frailty-informed framework supports proactive treatment simplification, prioritisation of safety, and alignment of care with patient priorities. The cases illustrate that de-intensification is not synonymous with undertreatment, but rather reflects recalibration of therapy in response to changing vulnerability and goals of care.
Implementation Challenges
Despite growing recognition of the risks associated with overtreatment in later life, translating deprescribing principles into routine diabetes care remains challenging. Barriers arise at the clinician, system, and patient levels, and must be addressed for a frailty-informed approach to be implemented consistently and safely.36
Clinician-Level Barriers
Clinicians may hesitate to de-intensify glucose-lowering therapy due to concerns about loss of glycaemic control, deviation from disease-focused guidelines, or medico-legal consequences. These concerns are compounded by limited formal training in deprescribing and uncertainty about balancing short-term safety against long-term metabolic outcomes.37
Clear documentation of the clinical rationale for treatment reduction—particularly when guided by frailty, functional decline, or hypoglycaemia risk—can mitigate these concerns. Framing deprescribing as an evidence-informed safety intervention, rather than therapeutic withdrawal, is essential to support clinician confidence.38
System-Level and Organisational Barriers
Healthcare systems often reinforce HbA1c-centred management through performance metrics that prioritise biochemical thresholds over safety or functional outcomes. Such incentives may inadvertently discourage appropriate treatment de-intensification. Fragmented care across settings further complicates responsibility for reassessing treatment intensity.39
Embedding frailty assessment and structured medication review within routine diabetes care pathways, supported by shared records and decision support tools, may facilitate more consistent implementation.40
Patient and Caregiver Perspectives
Patients and caregivers may interpret treatment reduction as a sign of therapeutic neglect or loss of disease control. This perception can be particularly strong in individuals who have been taught to view strict glycaemic control as essential to preventing complications. Without clear communication, deprescribing may generate anxiety or undermine trust.41
Engaging patients and caregivers in shared decision-making, with explicit discussion of treatment trade-offs and evolving goals of care, is therefore critical. Emphasising that deprescribing aims to reduce harm and maintain quality of life can help align expectations and support adherence to revised treatment plans.1,38
Implications for Practice and Policy
Adopting a frailty-informed approach to glucose-lowering therapy requires a shift from fixed biochemical targets toward ongoing assessment of patient vulnerability, functional status, and treatment burden. From an ethical perspective, deprescribing aligns with principles of non-maleficence and proportionality, particularly when treatment-related harm outweighs the likelihood of long-term benefit in frail older adults.42
In routine practice, this implies that frailty and functional capacity should be evaluated alongside glycaemic measures when setting or revising treatment goals in older adults with type 2 diabetes. Regular medication review, explicitly incorporating deprescribing as a proactive option, should become a standard component of diabetes care in later life.43
While newer glucose-lowering agents with low hypoglycaemia risk may be appropriate in selected, robust older adults, this framework deliberately avoids promoting any specific drug class and instead emphasises ongoing reassessment of benefit, tolerability, and treatment burden as frailty and care priorities evolve. Such an approach supports individualised care without privileging disease-specific targets over patient-centred outcomes.44
From a policy perspective, aligning quality indicators with outcomes that matter in later life—such as avoidance of hypoglycaemia, preservation of functional independence, and reduction of treatment burden—may better support appropriate deprescribing. Integrating frailty assessment and proactive medication review into standard diabetes management pathways could promote safer prescribing across care settings.45–47
Educational initiatives targeting clinicians, patients, and caregivers are also essential. Training programmes that incorporate principles of geriatric pharmacology and deprescribing may enhance clinician confidence, while patient-facing education can help reframe treatment reduction as an active, evidence-informed strategy aimed at maintaining quality of life.
Limitations
This review is not a formal systematic review and did not include structured risk-of-bias assessment. Selection of evidence may therefore reflect emphasis on clinically applicable studies. However, findings were triangulated across randomised trials, observational analyses, and guideline consensus statements. In addition, the framework has not yet been prospectively validated in interventional trials. Prospective validation of this framework in pragmatic interventional trials will be necessary to determine its impact on safety, hospitalisation rates, and patient-centred outcomes.
Conclusions
Deprescribing and de-intensification of glucose-lowering therapy are essential components of high-quality diabetes care in older adults. As frailty, multimorbidity, and functional vulnerability increase, the balance between benefit and harm associated with intensive glycaemic control shifts toward greater risk of hypoglycaemia, treatment burden, and functional decline.
This review proposes a frailty-informed clinical decision framework that places physiological vulnerability, treatment-related risk, and patient priorities at the centre of therapeutic decision-making. By moving beyond HbA1c-centred targets and adopting a dynamic, risk-based approach, clinicians can more safely recalibrate treatment intensity as health status and goals of care evolve.
Normalising deprescribing as a proactive and iterative process rather than a reactive response to adverse events has the potential to reduce iatrogenic harm, improve quality of life, and align diabetes management with what matters most to older people. Wider adoption of frailty-informed deprescribing frameworks may support safer, more person-centred diabetes care across diverse clinical settings. Importantly, de-intensification should remain dynamic, with re-escalation considered where symptomatic hyperglycaemia or changing clinical priorities warrant reassessment.
Data Sharing Statement
No new data were generated or analysed in this mini review. Data supporting the findings discussed are available within the cited literature.
Acknowledgments
The authors thank their affiliated institutions for academic support. No third party assistance was used in writing or preparing this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was received for the preparation of this mini review. Any resources used were part of the authors’ routine academic and institutional support.
Disclosure
The authors declare that they have no known financial or personal relationships that could inappropriately influence or bias the content of this mini review.
References
1. Doucet J, Gourdy P, Meyer L, et al. Management of glucose-lowering therapy in older adults with type 2 diabetes: challenges and opportunities. Clin Interventions Aging. 2023;18:1687–12. doi:10.2147/CIA.S423122
2. Bradley D, Hsueh W. Type 2 diabetes in the elderly: challenges in a unique patient population. J Geriatr Med Gerontol. 2016;2(2):14. doi:10.23937/2469-5858/1510014
3. Perry T. Minimizing harms of tight glycemic control in older people with type 2 diabetes. In: Therapeutics Letter. Therapeutics Initiative; 2024.
4. Munshi M, Kahkoska AR, Neumiller JJ, et al. Realigning diabetes regimens in older adults: a 4S Pathway to guide simplification and deprescribing strategies. Lancet Diabetes Endocrinol. 2025;13(5):427–437. doi:10.1016/S2213-8587(24)00372-3
5. Bolt J, Carvalho V, Lin K, et al. Systematic review of guideline recommendations for older and frail adults with type 2 diabetes mellitus. Age Ageing. 2024;53(11):fae259. doi:10.1093/ageing/afae259
6. Samajdar SS, Joshi SR. The A–G mnemonic: a practical framework for deprescribing in older adults with type 2 diabetes. Diabetes Care. 2025;48(10):e119–e121. doi:10.2337/dc25-1348
7. Lega IC, Thompson W, McCarthy LM. Deprescribing diabetes medications for older adults living with frailty. CMAJ. 2024;196(16):E562–E562. doi:10.1503/cmaj.231411
8. Lipska KJ, Ross JS, Miao Y, Shah ND, Lee SJ, Steinman MA. Potential overtreatment of diabetes mellitus in older adults with tight glycemic control. JAMA Intern Med. 2015;175(3):356–362. doi:10.1001/jamainternmed.2014.7345
9. McAlister F, van Walraven C. External validation of the hospital frailty risk score and comparison with the hospital-patient one-year mortality risk score to predict outcomes in elderly hospitalised patients: a retrospective cohort study. BMJ Qual Saf. 2019;28(4):284–288. doi:10.1136/bmjqs-2018-008661
10. American Diabetes Association. Standards of Care in Diabetes-2026. Available from: http://professional, diabetes.org/standards of care.
11. Diggle J. HbA 1c: practicalities and pitfalls. Diabetes & Prim Care. 2025;27(3).
12. Christiaens A, Baretella O, Del Giovane C, et al. Association between diabetes overtreatment in older multimorbid patients and clinical outcomes: an ancillary European multicentre study. Age Ageing. 2023;52(1):fac320. doi:10.1093/ageing/afac320
13. Byambasukh O, Nordog M, Suya B, et al. Age and HbA1c in diabetes: a negative association modified by red cell characteristics. J Clin Med. 2024;13(23):7487. doi:10.3390/jcm13237487
14. Correa MF, Li Y, Kum H-C, Lawley MA. Assessing the effect of clinical inertia on diabetes outcomes: a modeling approach. J Gen Intern Med. 2019;34(3):372–378. doi:10.1007/s11606-018-4773-3
15. Andreozzi F, Candido R, Corrao S, et al. Clinical inertia is the enemy of therapeutic success in the management of diabetes and its complications: a narrative literature review. Diabetol Metab Syndr. 2020;12(1):52. doi:10.1186/s13098-020-00559-7
16. Meier R, Chmiel C, Valeri F, et al. The effect of financial incentives on quality measures in the treatment of diabetes mellitus: a randomized controlled trial. J Gen Intern Med. 2022;37(3):556–564. doi:10.1007/s11606-021-06714-8
17. Kondo KK, Damberg CL, Mendelson A, et al. Implementation processes and pay for performance in healthcare: a systematic review. J Gen Intern Med. 2016;31(Suppl 1):61–69. doi:10.1007/s11606-015-3567-0
18. Strain WD, Down S, Brown P, et al. Diabetes and frailty: an expert consensus statement on the management of older adults with type 2 diabetes. Diabetes Therapy. 2021;12(5):1227–1247. doi:10.1007/s13300-021-01035-9
19. Abd. Ghafar MZA, O’Donovan M, Sezgin D, et al. Frailty and diabetes in older adults: overview of current controversies and challenges in clinical practice. Front Clin Diabetes Healthc. 2022;3:895313. doi:10.3389/fcdhc.2022.895313
20. Wightman H, Butterly E, Wei L, et al. Frailty in randomized controlled trials of glucose-lowering therapies for type 2 diabetes: an individual participant data meta-analysis of frailty prevalence, treatment efficacy, and adverse events. PLoS Med. 2025;22(4):e1004553. doi:10.1371/journal.pmed.1004553
21. Álvarez-Bustos A, Andres-Lacueva C, Ara I, et al. Consensus document on frailty: conceptualization, detection, multidisciplinary management and future roadmap. J Nutr Health Aging. 2026;30(3):100793. doi:10.1016/j.jnha.2026.100793
22. Christiaens A, Cochard A, Tubach F, et al. Association between hypoglycaemic drug de-intensification, mortality and hospital admission in older adults with type 2 diabetes: a cohort study emulating a target trial. Age Ageing. 2025;54(6):faf160. doi:10.1093/ageing/afaf160
23. Kosjerina V, Parsa M, Scheuer SH, et al. Comparative cardiovascular effectiveness of newer glucose-lowering drugs in elderly with type 2 diabetes: a target trial emulation cohort study. EClinicalMedicine. 2025;82.
24. Seidu S, Seewoodharry M, Khunti K. De-intensification in older people with type 2 diabetes: why, when and for whom? Lancet Healthy Longev. 2021;2(9):e531–e532. doi:10.1016/S2666-7568(21)00204-X
25. O’Mahoney L, Highton P, Abdala R, et al. Deintensification of potentially inappropriate medications amongst older frail people with type 2 diabetes: protocol for a cluster randomised controlled trial (D-MED study). Primary Care Diabetes. 2024;18(2):132–137. doi:10.1016/j.pcd.2023.12.001
26. Oktora M, Kerr K, Hak E, Denig P. Rates, determinants and success of implementing deprescribing in people with type 2 diabetes: a scoping review. Diabetic Med. 2021;38(2):e14408. doi:10.1111/dme.14408
27. Lindner N, Hoffmann M-C, Haasenritter J, et al. Assessing physicians’ agreement and the completeness of the decision aid ‘arriba Diabetes’: a cross-sectional study. BMC Primary Care. 2025;26(1):218. doi:10.1186/s12875-025-02887-x
28. Koons M, Hughes MD, Choe MD, et al. Deprescribing type 2 diabetes mellitus medications in older adults in an urban primary care setting. 2025.
29. Bradley MD, Arnold ME, Biskup BG, et al. Medication deprescribing among patients with type 2 diabetes: a qualitative case series of lifestyle medicine practitioner protocols. Clin Diabetes. 2023;41(2):163–176. doi:10.2337/cd22-0009
30. Denig P, Stuijt PJ. Perspectives on deprescribing in older people with type 2 diabetes and/or cardiovascular conditions: challenges from healthcare provider, patient and caregiver perspective, and interventions to support a proactive approach. Expert Rev Clin Pharmacol. 2024;17(8):637–654. doi:10.1080/17512433.2024.2378765
31. Parker MM, Lipska KJ, Gilliam LK, et al. Deprescribing in older adults with type 2 diabetes: associations with patients’ perspectives: the diabetes and aging study. J Am Geriatr Soc. 2025;73(4):1155–1167. doi:10.1111/jgs.19352
32. Hamada S, Gulliford MC. Antidiabetic and cardiovascular drug utilisation in patients diagnosed with type 2 diabetes mellitus over the age of 80 years: a population-based cohort study. Age Ageing. 2015;44(4):566–573. doi:10.1093/ageing/afv065
33. Dias DL, Gomes EJ. Insulin prescribing pattern in geriatric type 2 diabetic mellitus patients of different nutritional status at a tertiary level of health care: a retrospective study. Int J Basic Clin Pharmacol. 2019;8(3):584. doi:10.18203/2319-2003.ijbcp20190669
34. Simes BC, MacGregor GG. Sodium-glucose cotransporter-2 (SGLT2) inhibitors: a clinician’s guide. Diabetes Metab Syndr Obes. 2019;Volume 12:2125–2136. doi:10.2147/DMSO.S212003
35. Kutz A, Kim DH, Wexler DJ, et al. Comparative cardiovascular effectiveness and safety of SGLT-2 inhibitors, GLP-1 receptor agonists, and DPP-4 inhibitors according to frailty in type 2 diabetes. Diabetes Care. 2023;46(11):2004–2014. doi:10.2337/dc23-0671
36. Qaseem A, Obley AJ, Shamliyan T, et al. Newer pharmacologic treatments in adults with type 2 diabetes: a clinical guideline from the American College of Physicians. Ann Internal Med. 2024;177(5):658–666. doi:10.7326/M23-2788
37. Sinclair A, Dunning T, Rodriguez-Mañas L. Diabetes in older people: new insights and remaining challenges. Lancet Diabetes Endocrinol. 2015;3(4):275–285. doi:10.1016/S2213-8587(14)70176-7
38. Mogale NM, Ntuli TS, Chelule PK. Barriers to effective management of type 2 diabetes mellitus in primary healthcare facilities. J Public Health Afr. 2025;16(1):1420. doi:10.4102/JPHIA.v16i1.1420
39. Sinclair AJ, Abdelhafiz AH. Challenges and strategies for diabetes management in community-living older adults. Diabetes Spectr. 2020;33(3):217–227. doi:10.2337/ds20-0013
40. Messina R, et al. Patient-Reported Outcome Measures in Adults with Type 2 DiabetesWith a Focus on Older Populations: an AI-Assisted Rapid Review of Use and Implementation in Clinical and Organizational Practice. In: Healthcare. MDPI; 2025.
41. Boccardi V, Bahat G, Balci C, et al. Challenges, current innovations, and opportunities for managing type 2 diabetes in frail older adults: a position paper of the European Geriatric Medicine Society (EuGMS)—special interest group in diabetes. Eur Geriatric Med. 2025;16(4):1231–1247. doi:10.1007/s41999-025-01168-1
42. Wu C, Xu R, Cao J, et al. Barriers and facilitators of self-management for older adults living with type 2 diabetes mellitus: a qualitative study in China. Sci Diabetes Self Manag Care. 2024;50(1):44–55. doi:10.1177/26350106231221454
43. Pandya N, Hames E, Sandhu S. Challenges and strategies for managing diabetes in the elderly in long-term care settings. Diabetes Spectr. 2020;33(3):236–245. doi:10.2337/ds20-0018
44. Li J, Me RC, Fakhruddin NNINM, et al. Investigating the needs of older adults with type 2 diabetes and conceptualizing a healthy diet management application: a conceptual design. BMC Geriatr. 2025;25(1):697. doi:10.1186/s12877-025-06265-1
45. Yous M-L, Ganann R, Ploeg J, et al. Older adults’ experiences and perceived impacts of the Aging, Community and Health Research Unit-Community Partnership Program (ACHRU-CPP) for diabetes self-management in Canada: a qualitative descriptive study. BMJ open. 2023;13(4):e068694. doi:10.1136/bmjopen-2022-068694
46. Committee, A.D.A.P.P. 13. older adults: standards of care in diabetes—2026. Diabetes Care. 2025;49(Suppl 1):S277.
47. Hamasaki H. Patient experience in older adults with diabetes: a narrative review on interventions to improve patient experience and research gaps. In: Healthcare. MDPI; 2024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combined Vision and Hearing Impairment is Associated with Frailty in Older Adults: Results from the West China Health and Aging Trend Study
Zhao Y, Ding Q, Lin T, Shu X, Xie D, Gao L, Yue J
Clinical Interventions in Aging 2022, 17:675-683
Published Date: 2 May 2022
Intrinsic Capacity Declines with Elevated Homocysteine in Community-Dwelling Chinese Older Adults
Lin S, Wang F, Zheng J, Yuan Y, Huang F, Zhu P
Clinical Interventions in Aging 2022, 17:1057-1068
Published Date: 7 July 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Recognition and Management of Hospital-Acquired Sepsis Among Older General Medical Inpatients: A Multi-Site Retrospective Study
Barker N, Scott IA, Seaton R, Mehta N, Kalke VR, Redpath L
International Journal of General Medicine 2023, 16:1039-1046
Published Date: 21 March 2023
Management of Glucose-Lowering Therapy in Older Adults with Type 2 Diabetes: Challenges and Opportunities
Doucet J, Gourdy P, Meyer L, Benabdelmoumene N, Bourdel-Marchasson I
Clinical Interventions in Aging 2023, 18:1687-1703
Published Date: 9 October 2023