Back to Journals » Drug Design, Development and Therapy » Volume 20
Fosaprepitant versus Ondansetron for Preventing Postoperative Nausea and Vomiting After Video-Assisted Thoracoscopic Lung Resection: A Randomized Controlled Clinical Trial
Authors Qi X ![]() , Zhang J
, Zhang J ![]() , Sun J
, Sun J ![]() , Wang X, Chang T
, Wang X, Chang T ![]() , Yi W
, Yi W ![]() , Zhang Y
, Zhang Y ![]() , Zhang P
, Zhang P ![]()
Received 16 December 2025
Accepted for publication 2 March 2026
Published 10 March 2026 Volume 2026:20 584402
DOI https://doi.org/10.2147/DDDT.S584402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Xiuqing Qi,1,* Jinying Zhang,1,* Jiaojiao Sun,1 Xuyang Wang,2– 4 Tongmin Chang,5 Wenbo Yi,1 Yan Zhang,1 Peng Zhang1
1Department of Anesthesiology, Qilu Hospital of Shandong University, Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of Anesthesiology, The First Affiliated Hospital of Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 3Shandong Institute of Anesthesia and Respiratory Critical Care Medicine, The First Affiliated Hospital of Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 4Shandong Provincial Clinical Research Center for Anesthesiology, the First Affiliated Hospital of Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 5Department of Clinical Epidemiology, Qilu Hospital of Shandong University, Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peng Zhang, Department of Anesthesiology, Qilu Hospital of Shandong University, Shandong University, Jinan, Shandong, People’s Republic of China, Tel +86-18560083816, Email [email protected]
Purpose: Postoperative nausea and vomiting (PONV) is a frequent complication after video-assisted thoracoscopic lung resection, particularly in patients at moderate to high risk, and substantially hinders recovery. Fosaprepitant, a neurokinin-1 (NK-1) receptor antagonist, is approved for PONV prevention; however, its efficacy in video-assisted thoracoscopic lung resection remains uncertain. This randomized trial evaluated the efficacy of fosaprepitant versus ondansetron in preventing PONV in high-risk patients undergoing video-assisted thoracoscopic lung resection.
Patients and Methods: In this prospective, double-blind, randomized controlled clinical trial, 233 adults aged 18– 70 years undergoing elective video-assisted thoracoscopic lung resection with an Apfel score ≥ 2 were randomized 1:1 to receive intravenous fosaprepitant 150 mg or ondansetron 8 mg, each combined with dexamethasone 5 mg. The primary outcome was the incidence of PONV at 24 hours postoperatively. Secondary outcomes included the incidence and severity of PONV at 6, 12, and 48 hours postoperatively, the use of rescue antiemetics, adverse events, and recovery outcomes.
Results: The 24-hour incidence of PONV was 31.0% [36] in the fosaprepitant group and 41.0% [48] in the ondansetron group (OR, 0.76; 95% CI, 0.53 to 1.07; P= 0.112). Fosaprepitant significantly reduced PONV at 48 hours (10.3% [12] vs 20.5% [24]; OR, 0.51; 95% CI, 0.27 to 0.96; P= 0.032), as well as vomiting at 24 hours (8.6% [10] vs 21.4% [25]; OR, 0.40; 95% CI, 0.20 to 0.80; P= 0.006) and 48 hours (0% [0] vs 5.1% [6]; OR, 0.07; 95% CI, 0.00 to 1.32; P= 0.040).
Conclusion: Fosaprepitant was superior to ondansetron in preventing early postoperative vomiting and delayed-phase PONV, and it represents an effective antiemetic strategy for high-risk thoracic surgical patients.
Trial Number and Registry Url: Registration number, NCT05881486; https://clinicaltrials.gov.
Keywords: neurokinin-1 receptor antagonist, 5-HT3 receptor antagonist, antiemetic prophylaxis, dexamethasone, video-assisted thoracoscopic surgery
Introduction
Postoperative nausea and vomiting (PONV) is among the most frequent and distressing complications following general anesthesia, affecting approximately 30% of surgical patients and up to 80% of those at high risk.1,2 The incidence of PONV after video-assisted thoracoscopic lung resection is high and may reach 68.4%–73.7%.3 A high incidence of PONV delays oral intake and mobilisation, increases the risk of regurgitation and aspiration.2,4,5 Regurgitation and aspiration caused by PONV aggravate patient discomfort may also lead to aspiration pneumonitis, increasing the risk of postoperative pulmonary complications (PPCs).6,7
Numerous strategies have been explored to prevent and treat PONV after thoracic procedures, particularly in moderate and high risk patients.8 Currently, a combination of a 5-hydroxytryptamine type 3 (5-HT3) receptor antagonist, such as ondansetron, combined with dexamethasone for PONV prophylaxis, is recommended by clinical guidelines.4,9 However, this regimen remains suboptimal in patients at moderate to high risk, largely due to the short elimination half-life of ondansetron (3–5 h), which limits its coverage during the prolonged postoperative risk period.1,10–12 Consequently, long-acting antiemetics targeting alternative mechanisms are of growing clinical interest.
Fosaprepitant, a long-acting neurokinin-1 (NK-1) receptor antagonist and prodrug of aprepitant, has shown efficacy in preventing chemotherapy-induced nausea and vomiting and PONV.9,13–16 A retrospective analysis reported that fosaprepitant significantly reduced vomiting compared with ondansetron at 0–48 hours after surgery in patients at moderate to high risk of PONV.17 Notably, no significant differences were observed in nausea scores, rescue antiemetic use, or complete response rates between the fosaprepitant and ondansetron groups within 48 hours after surgery.17 Similar results were reported among patients undergoing lower-limb surgery.18 Interestingly, different results have been reported in neurosurgery patients; fosaprepitant reduced the incidence of vomiting, and also increased the complete response rate during the 24 and 48 hours after craniotomy.19 These findings confirm the antiemetic efficacy of fosaprepitant, highlighting the heterogeneity of surgical populations studied.
To our knowledge, the antiemetic effect of fosaprepitant in video-assisted thoracoscopic lung resection has not been explored previously. Thoracic procedures are characterized by one-lung ventilation, high opioid consumption, and dynamic intrathoracic pressure changes, which may modify both the incidence and mechanisms of PONV and its association with PPCs.20 Based on the above considerations, we conducted a randomized, double-blind clinical trial to evaluate the efficacy of fosaprepitant versus ondansetron, each combined with dexamethasone, for preventing PONV in patients undergoing elective video-assisted thoracoscopic lung resection who were identified as being at moderate to high risk according to the Apfel score. Secondary outcomes included PPCs, postoperative quality of life, and drug-related adverse events.
Materials and Methods
Study Design
This study is a prospective, single-center, randomized, double-blind, controlled clinical trial conducted at Qilu Hospital of Shandong University from October 2023 to March 2025 (See Supplementary Material 1, which provides the full study protocol). The study protocol was approved by the Institutional Review Board of Qilu Hospital, Shandong University, Jinan, Shandong, China, on November 28, 2022 (the Chairperson: Xiaoyang Chen, approval number: KYLL-202210-072-1). The trial was prospectively registered at clinicaltrials.gov (registration number: NCT05881486). The trial adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.21
Ethics
All participants provided written informed consent. This study was conducted in accordance with the latest clinical trial guidelines. The first patient was registered on October 7, 2023, and the last was followed up on December 9, 2024.
Participants
Patients scheduled for elective video-assisted thoracoscopic lung resection were eligible for inclusion. Inclusion criteria included: age 18–70 years, ASA physical status I–III, expected postoperative hospital stay≥24 hours, and moderate to high risk of PONV. The risk of PONV was assessed using a simplified Apfel score. Patients with an Apfel score of 2 or higher were classified as moderate to high risk and were eligible for inclusion. Exclusion criteria included: nausea or vomiting within 24 hours prior to surgery; use of antiemetic medications, steroids, or psychotropic drugs within 24 hours prior to surgery; cognitive impairment; severe hepatic or renal dysfunction; morbid obesity (BMI>35 kg m−2); known allergy to fosaprepitant, ondansetron, or dexamethasone; pregnancy or breastfeeding. All participants were recruited by trained research personnel from the thoracic surgery ward. Participants could withdraw at any time. Smoking status was collected from patient medical records and self-reports. “History of smoking” was defined as current or former regular cigarette use, and the cumulative smoking amount (pack-years) was not considered.
Randomization and Blinding
Eligible patients who signed informed consent were randomized in a 1:1 ratio. Randomization was performed using a computer-generated simple block randomization sequence with block sizes of 2 or 4. The randomization process was conducted by an independent researcher, without the use of stratification factors. To maintain blinding, all study medications (fosaprepitant 150 mg, ondansetron 8 mg, or 0.9% saline) were prepared by anesthesia assistants who were not involved in the study or patient care. The drugs were placed in identical 100 mL 0.9% saline infusion bags. The prepared drug bags were placed in opaque, sequentially numbered envelopes labeled “antiemetic medication” and handed to the anesthesiologists by the anesthesia assistants. All study personnel, including anesthesiologists, outcome assessors, clinical staff administering rescue antiemetics, statisticians, and participants, were blinded to treatment allocation.
Anesthesia and Interventions
All patients received general anesthesia with thoracic paravertebral nerve block. No thoracic epidural anesthesia was used. Each patient was administered 5 mg of dexamethasone (Qilu Pharmaceutical Co., Ltd., China) intravenously at the time of anesthesia induction. Patients in the fosaprepitant group received 150 mg of fosaprepitant (Qilu Pharmaceutical Co., Ltd., China) intravenously 30 minutes prior to surgery, while patients in the ondansetron group received 8 mg of ondansetron (Qilu Pharmaceutical Co., Ltd., China) intravenously 30 minutes prior to the end of surgery. The timing of administration was determined based on pharmacokinetic profiles and previous clinical evidence in PONV research.9,22 To maintain blinding, patients in the fosaprepitant group received 100 mL of 0.9% saline 30 minutes before the end of surgery, and patients in the ondansetron group received 100 mL of 0.9% saline 30 minutes before surgery (See Supplementary Material 2 for further details regarding interventions).
Surgical Procedures
All participants underwent elective video-assisted thoracoscopic surgery (VATS) for lung resection. Procedures included lobectomy, segmentectomy, or wedge resection. No pneumonectomies were performed. Surgical technique and perioperative management were standardized across patients to minimize variability in PONV risk.
Postoperative Analgesia
Postoperative analgesia was standardized for all patients. Intravenous patient-controlled analgesia (PCA) with sufentanil (2 ug kg−1) was used, consisting of a loading dose of 0.1 μg kg−1 at the end of surgery, a background infusion of 2 mL h−1, and patient-controlled bolus doses of 0.5 mL with a lockout interval of 15 minutes. In addition, flurbiprofen axetil 50 mg was administered intravenously every 12 hours. Additional analgesics were provided as needed upon patient request, except in cases of contraindications. The analgesic regimen was identical across both study groups to minimize confounding effects on PONV.
Study Visits and Assessment Procedures
Baseline demographic and clinical data were collected prior to enrollment. Postoperative assessments were conducted by trained personnel at 6, 12, 24, and 48 hours, including the occurrence of nausea and vomiting, the number of rescue antiemetic doses, and supplementary records from patient diaries. Additionally, drug-related adverse events, hospital stay duration, and other secondary outcomes were recorded. To comprehensively evaluate the severity of PONV, both a Visual Analog Scale (VAS) and the Rhodes Index of Nausea, Vomiting, and Retching (INVR) were employed.23–25 Rescue antiemetics were administered according to predefined criteria, including patient request or the occurrence of moderate-to-severe nausea or vomiting, and were applied uniformly across both groups, independent of treatment allocation.
Primary and Secondary Outcomes
The primary endpoint of this study was the incidence of PONV at 24 hours after surgery, defined as the occurrence of nausea, vomiting, or the use of rescue antiemetic medication during the 12–24-hour postoperative period.
While secondary endpoints encompassed several outcomes, including: the incidence of PONV at 6, 12, and 48 hours postoperatively (defined as nausea, vomiting, or rescue antiemetic use during the 0–6-hour, 6–12-hour, and 24–48-hour intervals, respectively); the severity of PONV at 6, 12, 24, and 48 hours after surgery; the individual incidence rates and severity scores for both nausea and vomiting at each timepoint;26 the maximum VAS score for PONV within 48 hours postoperatively; the proportion of patients requiring rescue antiemetic medication at each timepoint and cumulatively within 48 hours; the incidence of postoperative adverse events, including headache, dizziness, constipation, pulmonary complications, and surgical complications;27,28 fasting blood glucose level measured on postoperative day 2; postoperative sleep quality assessed via the Richards-Campbell Sleep Questionnaire (RCSQ);29 quality of recovery at 24 hours postoperatively evaluated using the Quality of Recovery-15 (QoR-15) questionnaire;30 and postoperative ambulation distance, duration of hospital stay, and time to chest drain removal as recorded by investigators.
Sample Size
Sample size calculation was based on the anticipated incidence of postoperative vomiting (POV) within 24 hours. Previous trials in adult surgical patients receiving ondansetron prophylaxis reported 24-hour POV incidences of approximately 15–27%.31–33 Given that our study population comprised patients at moderate-to-high risk of PONV, for whom the incidence of POV is expected to be higher,34,35 we selected an intermediate value within this range and assumed a 22% 24-hour POV incidence in the ondansetron group. This assumption is consistent with a trial involving patients undergoing thoracoscopic lung resection, in which the incidence of postoperative vomiting in the ondansetron-based prophylaxis group was 23.3%.36 Fosaprepitant has demonstrated high antiemetic efficacy in chemotherapy-induced nausea and vomiting, with complete response rates up to 93%.37,38 Furthermore, in moderate-to-high PONV-risk surgical patients, it significantly reduced POV compared with ondansetron (2% vs 17–28%).17 Based on these data, we assumed a 7% 24-hour POV incidence in the fosaprepitant group. Using PASS software (version 15.0; NCSS, Kaysville, UT, USA), with a two-sided α of 0.05 and 90% power, we calculated that 111 patients per group were required. Accounting for a potential 5% dropout, 117 patients were planned per group.
Statistical Analysis
Continuous variables were reported as mean±SD or median [IQR], as appropriate; categorical variables were reported as counts and percentages. Normality of continuous variables was assessed using the Shapiro–Wilk test, and homogeneity of variance was assessed using Levene’s test. Variables were considered normally distributed if the Shapiro–Wilk test yielded P>0.05, and variances were considered equal if Levene’s test yielded P>0.05. Between-group differences were assessed using independent-samples t-tests for normally distributed variables with equal variances (reported as mean difference with 95% CI) and Mann–Whitney U-tests for non-normally distributed variables or variables that violated variance homogeneity (reported as median difference with 95% CI using the Hodges–Lehmann estimator). Categorical variables were compared using the χ2-test or Fisher’s exact test, with effect sizes reported as odds ratios (OR) and 95% CI. For outcomes with zero events in one group, the Haldane–Anscombe continuity correction was applied for OR estimation. Binary logistic regression was used to evaluate predictors of PONV. Univariate analysis was performed for outcomes at 24 and 48 hours. Due to sparse data, sex, smoking, and alcohol use were excluded from regression models. Variables with P<0.20 in univariate analysis and key baseline covariates (age, BMI, hypertension) were included in multivariable models.39 All analysis were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA), and a two-sided P-value<0.05 was considered statistically significant. Adjusted OR and 95% CI were reported.
Results
Baseline Characteristics
From October 7, 2023, to March 9, 2025, a total of 428 patients scheduled for video-assisted thoracoscopic lung resection were screened. Among them, 195 patients were excluded: 167 did not meet the inclusion criteria, and 28 declined to participate. One patient initially eligible withdrew consent prior to randomization. Ultimately, 233 patients provided written informed consent and were randomly assigned in a 1:1 ratio to receive either fosaprepitant (n=116) or ondansetron (n=117) (Figure 1). Baseline characteristics were comparable between the two groups (Table 1), and the achieved sample size retained sufficient statistical power for the primary outcome. In our cohort, most patients had no history of smoking. The high proportion of non-smokers resulted from the Apfel risk score≥2 inclusion criterion. Female non-smokers were enrolled, while many male smokers did not meet the score threshold.
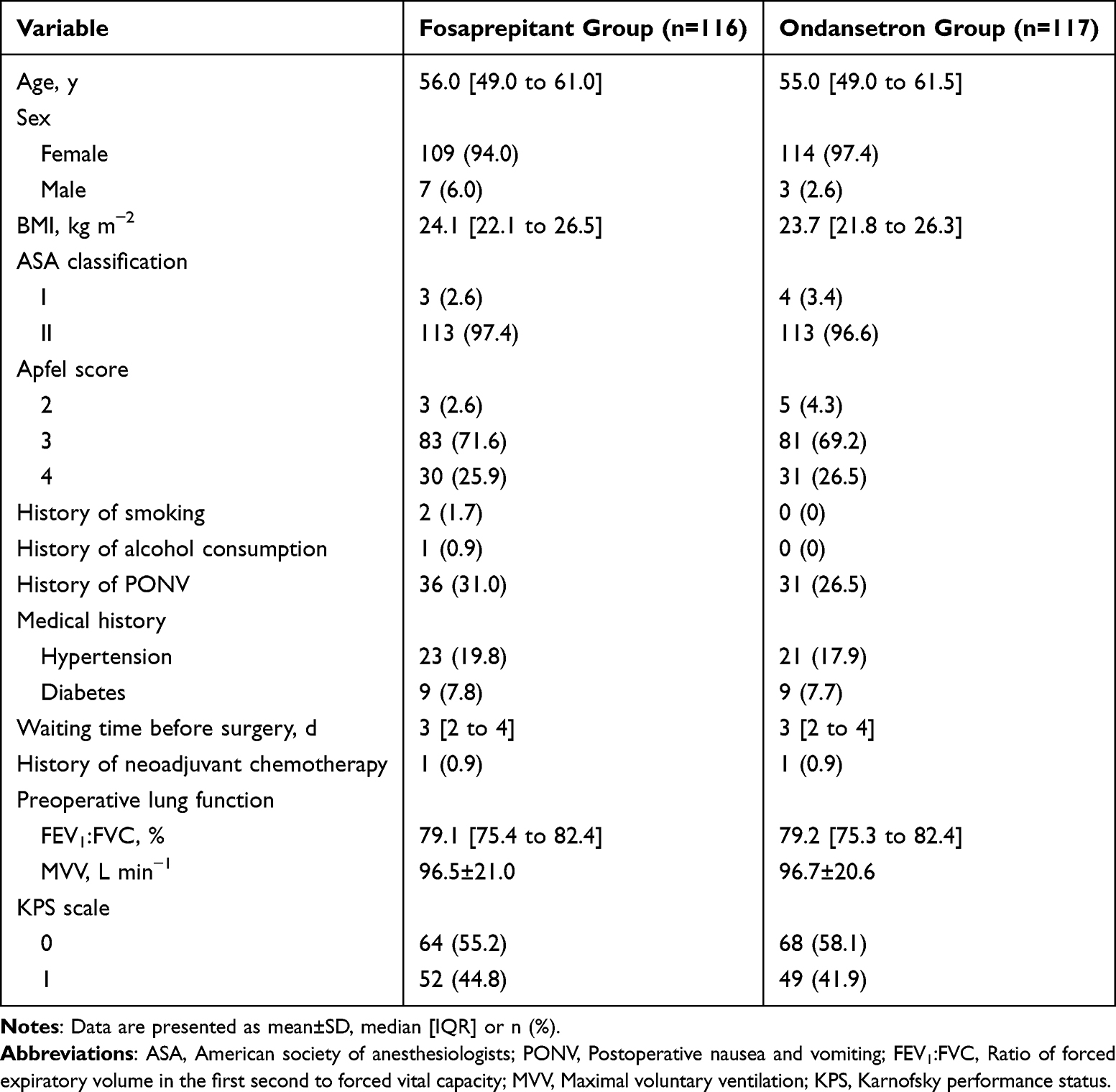 |
Table 1 Baseline Characteristics of Patients in the Fosaprepitant and Ondansetron Groups |
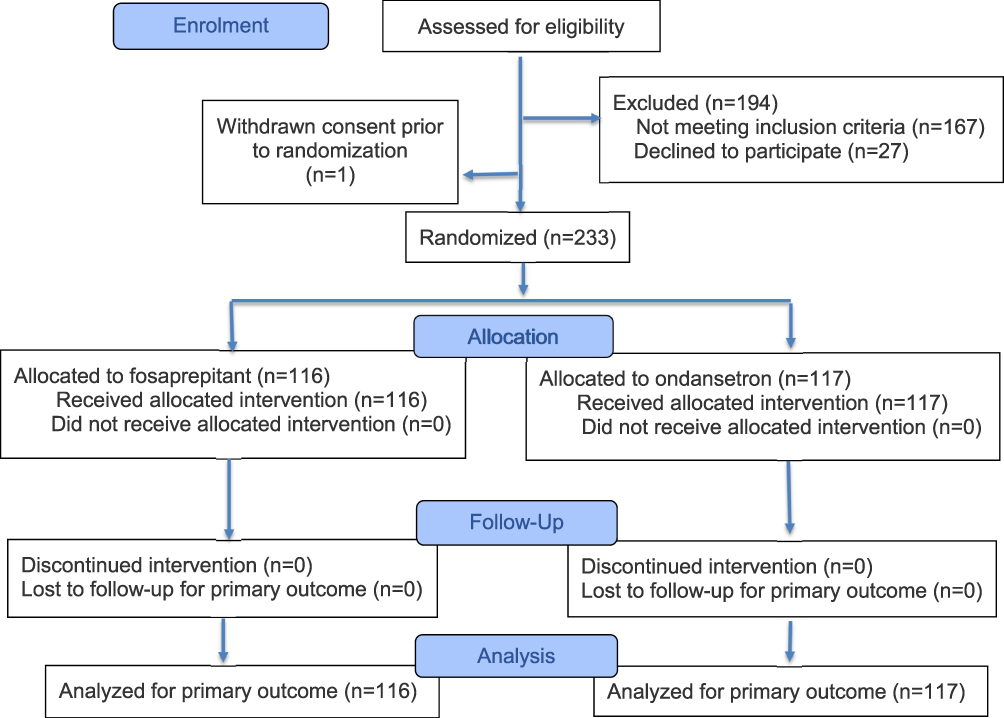 |
Figure 1 Flow chart of study design. |
Primary Outcome
The incidence of PONV at 24 hours postoperatively did not differ significantly between the fosaprepitant and ondansetron groups. Specifically, 36 patients (31.0%) in the fosaprepitant group experienced PONV compared to 48 patients (41.0%) in the ondansetron group, yielding an OR of 0.76 (95% CI, 0.53 to 1.07; P=0.112) (Figure 2A).
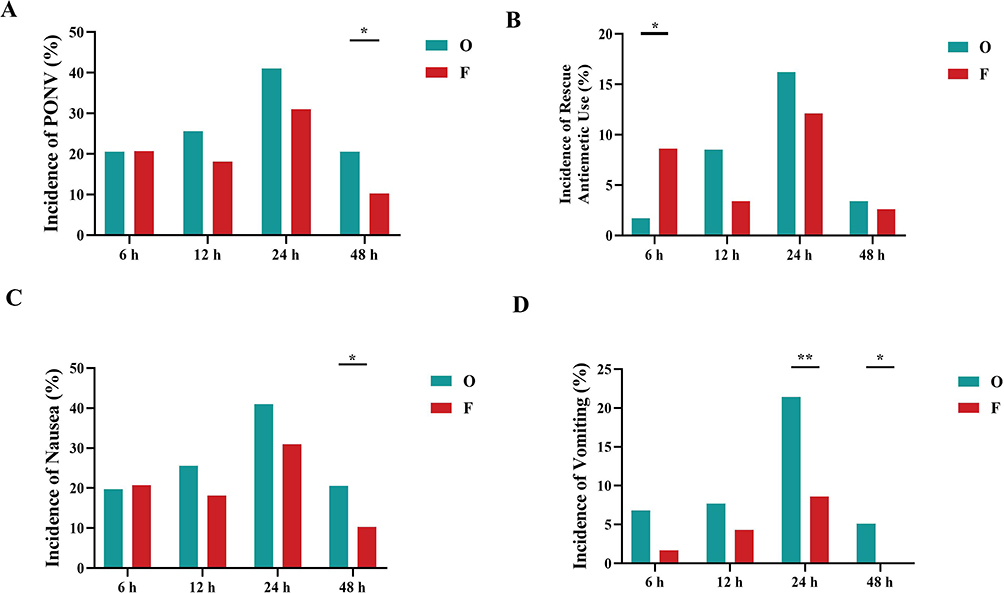 |
Figure 2 Effects of Fosaprepitant and Ondansetron on Postoperative Nausea, Vomiting, and Rescue Medication Use. (A) Incidence of postoperative nausea and vomiting (PONV) at 6, 12, 24, and 48 hours postoperatively. (B) Incidence of rescue antiemetic use at corresponding time points. (C) Incidence of nausea alone. (D) Incidence of vomiting alone. Data are presented as percentages. Patients in the fosaprepitant group (F) exhibited significantly lower rates of vomiting and overall PONV at 24 and 48 hours compared with the ondansetron group (O). Notably, rescue antiemetic use was higher in the fosaprepitant group at 6 hours, but cumulative differences were not significant. *P<0.05, **P<0.01 for between-group comparisons using χ2-test or Fisher exact test where appropriate. F indicates fosaprepitant; O, ondansetron. |
Secondary Outcomes
Time Course of PONV
PONV incidence was comparable between groups at 6 and 12 hours postoperatively. At 48 hours, the fosaprepitant group exhibited a significantly lower PONV incidence compared with the ondansetron group (10.3% [12] vs 20.5% [24]; OR, 0.51; 95% CI, 0.27 to 0.96; P=0.032) (Figure 2A).
Rescue Antiemetic Use
During the first 6 hours postoperatively, the rescue antiemetics were required more frequently in the fosaprepitant group than in the ondansetron group (8.6% [10] vs 1.7% [2]; OR, 5.04; 95% CI, 1.13 to 22.52; P=0.017). Over the entire 48-hour postoperative period, the cumulative incidence of rescue antiemetic use was comparable between the groups (23.3% [27] vs 23.9% [28]; OR, 0.97; 95% CI, 0.61 to 1.54; P=0.906) (Figure 2B).
Nausea and Vomiting Separately
To comprehensively evaluate the character of PONV, nausea and vomiting were recorded separately. At 24 hours, nausea incidence did not differ significantly between groups (31.0% [36] vs 41.0% [48]; OR, 0.76; 95% CI, 0.53 to 1.07; P=0.112) (Figure 2C), whereas vomiting was less frequent in the fosaprepitant group (8.6% [10] vs 21.4% [25]; OR, 0.40; 95% CI, 0.20 to 0.80; P=0.006) (Figure 2D). At 48 hours, both nausea (10.3% [12] vs 20.5% [24]; OR, 0.50; 95% CI, 0.27 to 0.96; P=0.032) and vomiting (0.0% [0] vs 5.1% [6]; OR, 0.07; 95% CI, 0.00 to 1.32; P=0.040) were lower in the fosaprepitant group, contributes to the overall reduction in PONV incidence.
PONV Severity
VAS scores revealed the proportion of patients experiencing moderate-to-severe PONV (VAS≥5) was significantly lower in the fosaprepitant group than in the ondansetron group at both 24 hours (7.8% [9] vs 22.2% [26]; P=0.013) and 48 hours (0.0% [0] vs 5.2% [6]; P=0.029) (Figure 3A). Similarly, stratified analysis of the Rhodes INVR scores demonstrated a lower proportion of moderate-to-severe PONV in the fosaprepitant group at 24 hours (13.8% [16] vs 24.8% [29]; P=0.075) and 48 hours (2.6% [3] vs 6.0% [7]; P=0.278) (Figure 3B). The Rhodes INVR score–based analysis did not reach statistical significance, the observed trend consistently favored fosaprepitant.
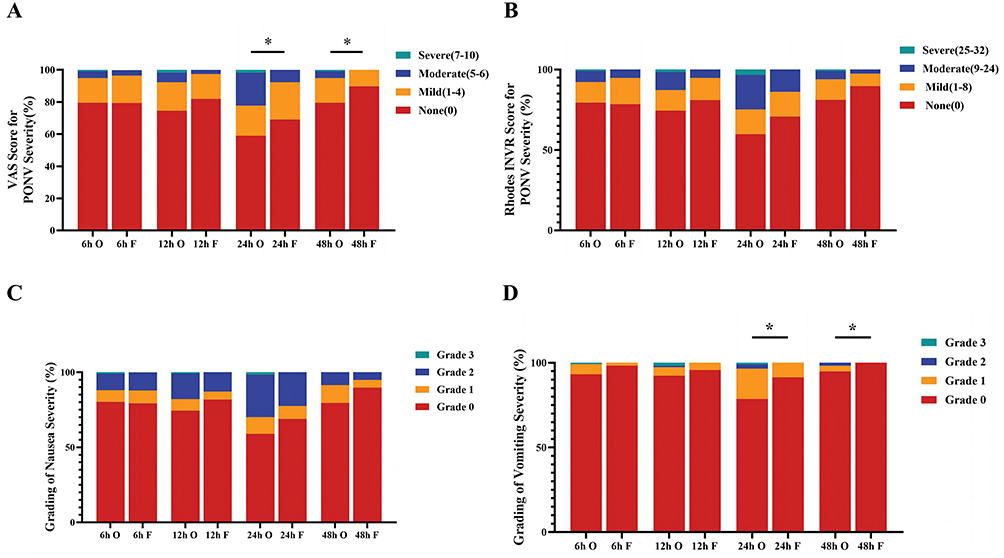 |
Figure 3 Multidimensional Assessment of Postoperative Nausea and Vomiting Severity. (A) Distribution of the most severe PONV scores assessed using the Visual Analog Scale (VAS). Patients in the fosaprepitant (F) group showed significantly lower proportions of moderate-to-severe PONV (VAS≥5) compared with the ondansetron (O) group at 24 and 48 hours. (B) Distribution of PONV severity assessed by the Rhodes Index of Nausea, Vomiting, and Retching (INVR). Although a trend favoring fosaprepitant was observed in the delayed phase, differences between groups were not statistically significant. (C) Grading of nausea severity from 0 to 48 hours postoperatively. No significant differences were observed between groups across time points. (D) Grading of vomiting severity, indicating significantly lower rates of vomiting in the fosaprepitant group at 24 and 48 hours postoperatively. Grading was based on the institutional classification system (Grade 0–3), with higher grades indicating greater severity of the condition. *P<0.05. F indicates fosaprepitant; O, ondansetron. |
At all postoperative time points (6, 12, 24, and 48 hours), the distribution of nausea severity grades was comparable between the fosaprepitant and ondansetron groups, with no statistically significant differences observed (Figure 3C). This trial demonstrated a significant difference in the severity of vomiting grading observed at both 24 hours (P=0.012) and 48 hours (P=0.029) postoperatively between the two groups (Figure 3D). No vomiting events occurred in the fosaprepitant group at 48 hours postoperatively; the Haldane-Anscombe continuity correction was applied to ensure the stability of the OR estimate.
Finally, the maximum 48-hour PONV scores (VAS) were higher in the ondansetron group, with moderate and severe PONV occurring in 26.5% [31] and 2.6% [3] of patients, compared with 12.9% [15] and 0% [0] in the fosaprepitant group (P=0.011) (Figure 4).
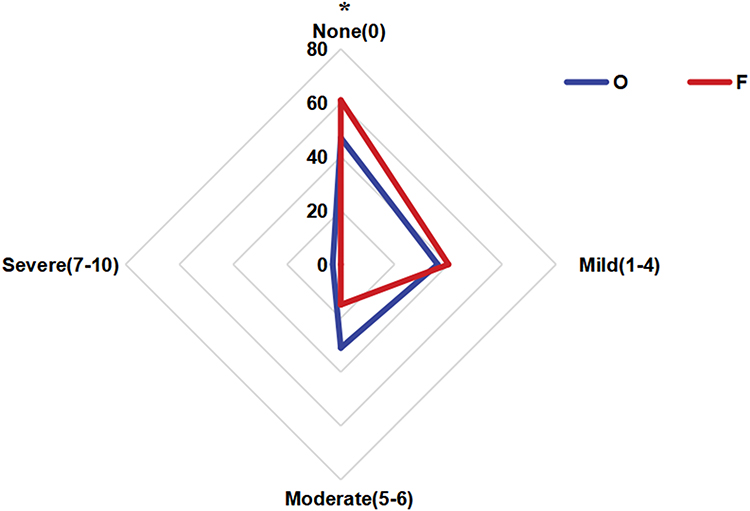 |
Figure 4 Distribution of worst PONV severity within 48 hours based on VAS score. Radar chart depicting the distribution of the most severe postoperative nausea and vomiting (PONV) scores within 48 hours after surgery, assessed using a visual analog scale (VAS). Severity was categorized as None (0), Mild (1–4), Moderate (5–6), and Severe (7–10). The chart compares the proportion of patients in each category between the fosaprepitant group (n=116) and the ondansetron group (n=117). A greater proportion of patients in the fosaprepitant group reported no PONV, while fewer experienced moderate to severe symptoms. *P<0.05 for the overall between-group comparison of PONV severity distribution (P=0.011). |
Logistic Regression Analysis of Risk Factors for PONV
To identify predictors of PONV, binary logistic regression was performed. For 24-hour PONV, univariate analysis revealed no significant risk factors (all P>0.10). The multivariable model, which included variables with P<0.20 from univariate analysis and key covariates (age, BMI, hypertension), also identified no significant predictors. Although the fosaprepitant group had a lower risk of 24-hour PONV, this was not statistically significant (adjusted OR, 0.66; 95% CI, 0.39 to 1.14; P=0.139) (Table 2).
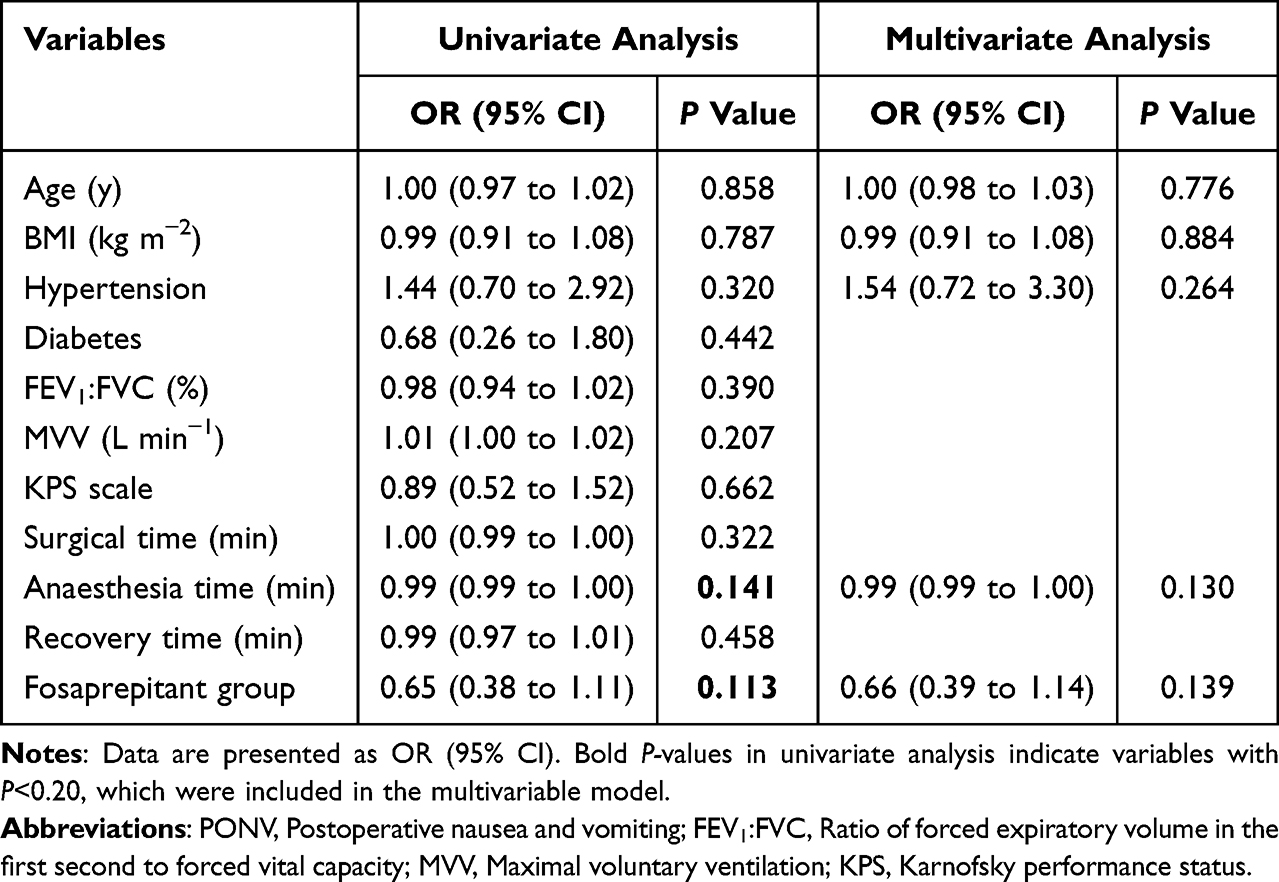 |
Table 2 Logistic Regression Analysis of Risk Factors for PONV Within 24 hours |
For 48-hour PONV, univariate logistic regression identified antiemetic regimen (OR, 0.45; 95% CI, 0.21 to 0.94; P=0.035), FEV1:FVC ratio (OR, 0.95; 95% CI, 0.90 to 1.00; P=0.055) and MVV (OR, 0.99; 95% CI, 0.97 to 1.01; P=0.155) as potential predictors. Multivariable logistic regression confirmed that antiemetic regimen was an independent predictor, with the fosaprepitant group showing a significantly lower risk of PONV compared with the ondansetron group (adjusted OR, 0.44; 95% CI, 0.20 to 0.93; P=0.033) (Table 3).
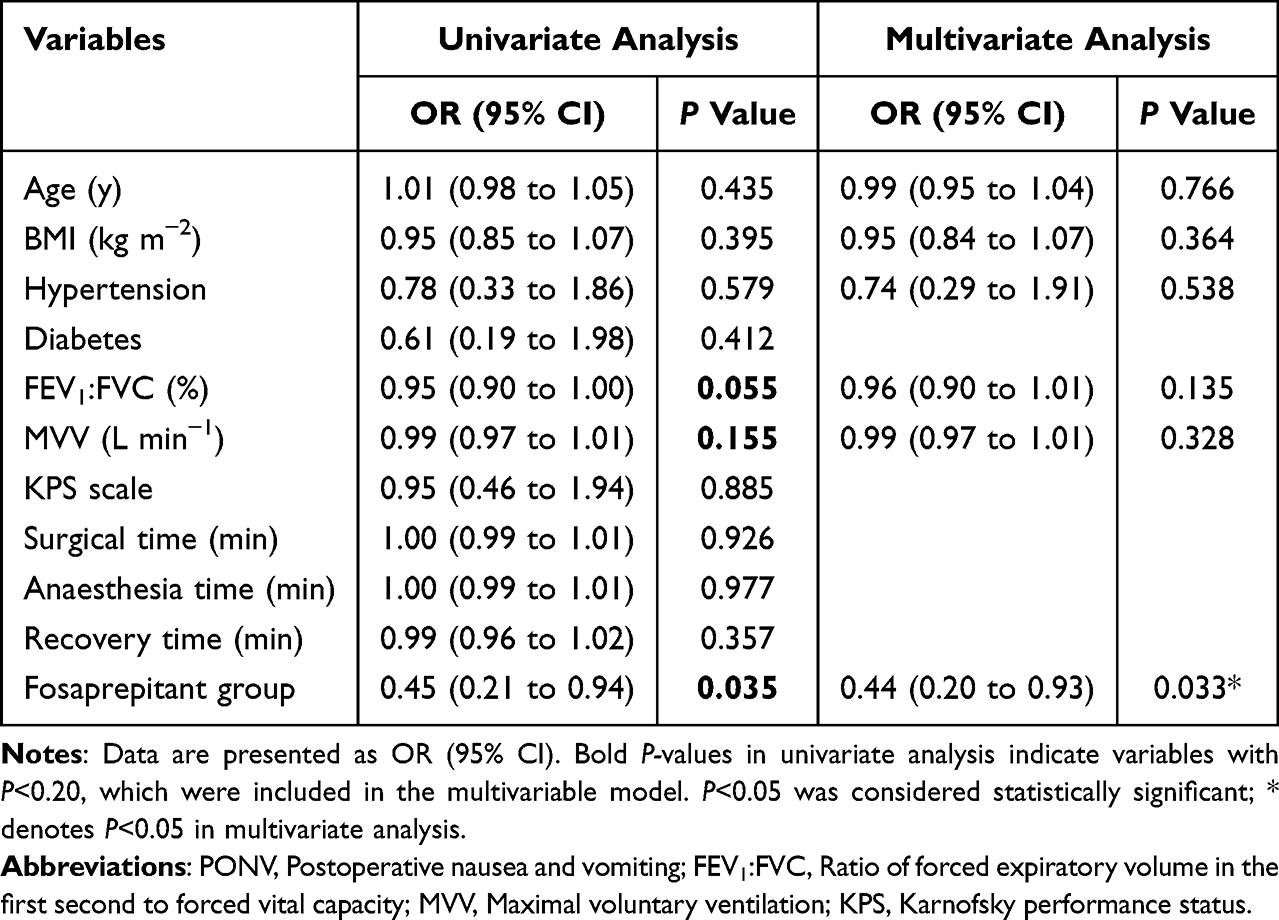 |
Table 3 Logistic Regression Analysis of Risk Factors for PONV Within 48 hours |
Postoperative Complications, Adverse Events, and Recovery Outcomes
In this study, there was no significant difference in the overall incidence of PPCs between the fosaprepitant and ondansetron groups (50.9% [59] vs 53.8% [63]; OR, 0.95; 95% CI, 0.74 to 1.21; P=0.648). The incidence of common adverse events such as headache, dizziness, and constipation, as well as other postoperative complications, was comparable between the two groups. No additional adverse reactions were attributed to fosaprepitant, supporting its favorable safety profile. Furthermore, no significant differences were observed between the two groups in terms of postoperative length of hospital stay or time to chest tube removal. Regarding other postoperative indicators, fasting blood glucose levels on the morning of postoperative day 1 were significantly higher in the fosaprepitant group compared to the ondansetron group (median [IQR], 7.0 [6.2 to 8.0] vs 6.3 [5.7 to 7.7]; MD, 0.50; 95% CI, 0.10 to 0.80; P=0.011), though the clinical significance of this finding remains to be elucidated. At 48 hours postoperatively, sleep quality was significantly better in the fosaprepitant group (median [IQR], 156.5 [142.8 to 173.8] vs 150.0 [130.0 to 165.0]; MD, 10.0; 95% CI, 0.00 to 15.00; P=0.017), while no significant difference was observed at 24 hours (Table 4).
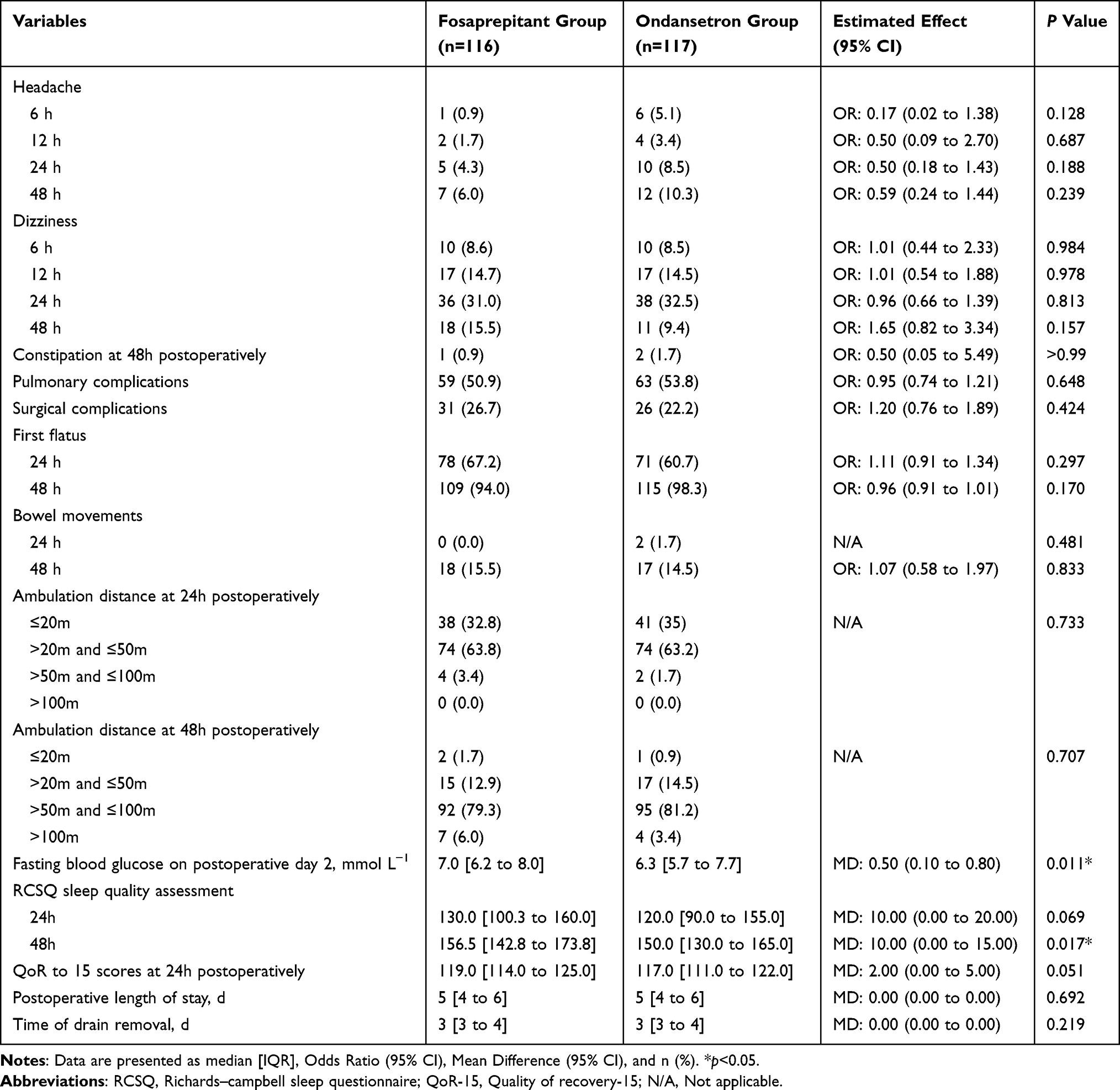 |
Table 4 Comparison of Postoperative Adverse Effects and Recovery Outcomes Between Fosaprepitant and Ondansetron Groups |
Discussion
This study compared the efficacy of fosaprepitant plus dexamethasone versus ondansetron plus dexamethasone in preventing PONV among patients at moderate-to-high risk undergoing video-assisted thoracoscopic lung resection. Our study did not find a statistically significant reduction in the incidence of PONV at 24 hours postoperatively in the fosaprepitant group compared to the ondansetron group; however, findings from secondary outcomes offer valuable insights into the potential benefits of fosaprepitant.
Currently, studies directly comparing the efficacy of fosaprepitant and ondansetron for PONV prevention remain limited. A retrospective study in moderate-to-high-risk patients reported no significant difference in PONV incidence between the two agents.17 Similar findings were observed in neurosurgical,19 gynecologic,40 and orthopedic18 populations. In contrast, our study demonstrated that fosaprepitant significantly reduced the incidence of vomiting at both 24 and 48 hours postoperatively, with a notable reduction in overall PONV incidence at 48 hours—an outcome not previously reported. Discrepancies across studies may be attributed to differences in patient populations, surgical types, and sample sizes. In the present study, all patients underwent video-assisted thoracoscopic procedures and received identical postoperative analgesia regimens to minimize the confounding effects on PONV. These inconsistencies underscore the importance of large, adequately powered randomized trials in specific surgical settings. Our findings address the evidence gap in video-assisted thoracoscopic lung resection and provide strong support for the use of fosaprepitant as a prophylactic antiemetic in this population.
We conducted an exploratory multivariable logistic regression analysis to evaluate potential factors associated with PONV. For the primary outcome (24-hour PONV incidence), no significant predictors were identified, and the incidence was comparable between the fosaprepitant and ondansetron groups. For the secondary outcome (48-hour PONV incidence), fosaprepitant remained an independent protective factor after adjusting for potential confounders, including age, BMI, hypertension, and baseline pulmonary function. None of the baseline variables were significantly associated with 48-hour PONV. However, since the secondary outcome (48-hour PONV incidence) was analyzed in a post hoc exploratory manner, the results should be interpreted with caution and require confirmation in future prospective studies.
This study independently analyzed nausea and vomiting to more accurately assess the pharmacological effects of the interventions. The results showed that fosaprepitant provided significantly better control of nausea at 48 hours postoperatively, with a lower incidence also observed at 12 and 24 hours. In the fosaprepitant group, the incidence, frequency, and severity of vomiting were consistently reduced at 24 and 48 hours postoperatively. The sustained antiemetic effect, consistent with its conversion to aprepitant and prolonged action (up to 72 hours), aligns with its pharmacologic mechanism.9,41–47 In contrast, ondansetron’s short half-life limits its efficacy in preventing delayed-phase PONV.10,48 Effective control of vomiting significantly reduces serious complications such as aspiration, electrolyte imbalance, wound dehiscence, and delayed recovery, thereby preventing prolonged hospitalization and increased healthcare costs.9 Effective management of vomiting, especially in moderate-to-high-risk patients undergoing video-assisted thoracoscopic lung resection, is crucial for promoting enhanced recovery after surgery.49
Patients receiving fosaprepitant showed improved postoperative recovery, with significantly better sleep quality at 48 hours and a trend toward higher QoR-15 scores at 24 hours. These improvements may be attributed to more effective control of delayed-phase PONV, highlighting the potential clinical value of fosaprepitant in optimizing postoperative recovery.
The incidence of rescue antiemetic use within 6 hours postoperatively was significantly higher in the fosaprepitant group than in the ondansetron group, highlighting the importance of considering the temporal dynamics of PONV management. This finding suggests that long-acting NK-1 receptor antagonists provide sustained protection against delayed PONV, additional early-phase coverage may be required to optimize immediate postoperative symptom control. Multimodal antiemetic strategies, particularly the combination of long-acting NK-1 receptor antagonists with short-acting 5-HT3 receptor antagonists, can provide more comprehensive protection during both early and delayed phases while reducing the risk of adverse effects associated with high-dose monotherapy.1,50
Adverse events associated with NK-1 receptor antagonists are generally uncommon, with occasional reports indicating a slightly increased incidence of dizziness and headache.14,51,52 In this study, the safety profiles of fosaprepitant and ondansetron were comparable, with no significant differences observed in the incidence of common adverse events. Additionally, there were no significant differences between the two groups in terms of chest drain duration or length of hospital stay. The incidence of PPCs did not differ significantly between groups. Although fosaprepitant significantly reduced delayed-phase vomiting, this advantage did not translate into a reduction in PPCs. Further large-scale studies are warranted to determine whether improved PONV control can effectively reduce the risk of pulmonary complications.
This study has several limitations. First, it was conducted at a single center, which may limit the external generalizability of the findings. Second, patient recruitment based on the Apfel score resulted in a predominantly female population, introducing potential selection bias. Third, the study focused exclusively on patients undergoing video-assisted thoracoscopic lung resection, and the results may not be generalizable to other surgical populations. In addition, postoperative follow-up was limited to 48 hours and did not capture long-term outcomes, such as readmissions. The observed between-group difference in the primary endpoint was smaller than assumed in the a priori sample size calculation. Consequently, this study may have been underpowered to detect a modest but clinically relevant difference in 24-hour PONV. Future larger-scale, multicenter trials are warranted to confirm these findings.
Notably, fosaprepitant demonstrated superior control of delayed-phase PONV, patients in the fosaprepitant group required rescue antiemetic medication more frequently during the early postoperative period (within 6 hours). This finding highlights a potential limitation of relying on one long-acting antiemetic to provide sufficient coverage during the immediate postoperative phase. It underscores the importance of the temporal dynamics of PONV and suggests that optimal prophylaxis may require tailored multimodal regimens. The combination of long-acting NK-1 antagonists and short-acting drugs may be a promising antiemetic strategy to achieve balanced protection against PONV covering both the early and delayed postoperative periods in thoracoscopic lung resection patients.
Conclusion
Both regimens effectively prevented PONV, with no significant difference in the incidence of PONV at 24 hours postoperatively. Fosaprepitant demonstrated superior control of early postoperative vomiting, delayed-phase nausea and vomiting, and several secondary endpoints, although the observed differences were smaller than anticipated. These findings support the potential role of fosaprepitant in controlling PONV after video-assisted thoracoscopic lung resection. Future multicenter trials are warranted to validate these findings and to refine multimodal prophylactic regimens.
Abbreviations
PONV, Postoperative Nausea and Vomiting; PPCs, Postoperative Pulmonary Complications; 5-HT3, 5-Hydroxytryptamine Type 3; NK-1, Neurokinin-1; CONSORT, Consolidated Standards of Reporting Trials; VATS, Video-Assisted Thoracoscopic Surgery; PCA, Patient-Controlled Analgesia; VAS, Visual Analog Scale; INVR, Index of Nausea, Vomiting, and Retching; RCSQ, Richards-Campbell Sleep Questionnaire; QoR-15, Quality of Recovery-15; POV, Postoperative Vomiting.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding author if reasonable.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board (Ethics Committee) of Qilu Hospital of Shandong University, Jinan, Shandong, China (Approval No. KYLL-202210-072-1). Written informed consent was obtained from all participants prior to enrollment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Shandong Medical Association (grant number YXH2022ZX02086).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2014;118(1):85–14. doi:10.1213/ANE.0000000000000002
2. Goldson KV, Brennan E, Burton BN, et al. Does Management of Postoperative Nausea and Vomiting Differ by Patient Demographics? An Evaluation of Perioperative Anesthetic Management-An Observational Study. Anesthesiology. 2025;142(4):704–715. doi:10.1097/ALN.0000000000005367
3. Vijitpavan A, Kittikunakorn N, Komonhirun R. Comparison between intrathecal morphine and intravenous patient control analgesia for pain control after video-assisted thoracoscopic surgery: a pilot randomized controlled study. PLoS One. 2022;17(4):e0266324. doi:10.1371/journal.pone.0266324
4. Gan TJ, Belani KG, Bergese S, et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
5. Griffiths JD, Gyte GML, Popham PA, et al. Interventions for preventing nausea and vomiting in women undergoing regional anaesthesia for caesarean section. Cochrane Database Syst Rev. 2021;2021(5):CD007579. doi:10.1002/14651858.CD007579.pub3
6. Kuratomi H, Idei M, Takaki S, Yokoyama N, Yokose M. Life-Threatening Aspiration Pneumonia as a Rare Complication of Postoperative Nausea and Vomiting (PONV) in a Young Patient Following Cardiac Surgery: a Case Report. Cureus. 2025;17(4):e83254. doi:10.7759/cureus.83254
7. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
8. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS(R)) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
9. Huang Q, Wang F, Liang C, et al. Fosaprepitant for postoperative nausea and vomiting in patients undergoing laparoscopic gastrointestinal surgery: a randomised trial. Br J Anaesth. 2023;131(4):673–681. doi:10.1016/j.bja.2023.06.029
10. Swaika S, Pal A, Chatterjee S, Saha D, Dawar N. Ondansetron, ramosetron, or palonosetron: which is a better choice of antiemetic to prevent postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy? Anesth Essays Res. 2011;5(2):182–186. doi:10.4103/0259-1162.94761
11. Carlisle JB, Stevenson CA. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2006;2006(3):CD004125. doi:10.1002/14651858.CD004125.pub2
12. Kovac AL. Comparative Pharmacology and Guide to the Use of the Serotonin 5-HT(3) Receptor Antagonists for Postoperative Nausea and Vomiting. Drugs. 2016;76(18):1719–1735. doi:10.1007/s40265-016-0663-3
13. Yang Q, Zou X, Xie YL, et al. Fosaprepitant Weekly vs Every 3 Weeks for the Prevention of Concurrent Chemoradiotherapy-Induced Nausea and Vomiting: a Pilot Randomized Clinical Trial. JAMA Network Open. 2023;6(7):e2326127. doi:10.1001/jamanetworkopen.2023.26127
14. Becherini C, Salvestrini V, Desideri I, et al. Impact of fosaprepitant in the prevention of nausea and emesis in head and neck cancer patients undergoing cisplatin-based chemoradiation: a pilot prospective study and a review of literature. Radiol Med. 2024;129(3):457–466. doi:10.1007/s11547-024-01757-3
15. Zhao Y, Zhao B, Chen G, et al. Validation of different personalized risk models of chemotherapy-induced nausea and vomiting: results of a randomized, double-blind, Phase III trial of fosaprepitant for cancer patients treated with high-dose cisplatin. Cancer Commun. 2023;43(2):246–256. doi:10.1002/cac2.12397
16. Weibel S, Rucker G, Eberhart LH, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev. 2020;10(10):CD012859. doi:10.1002/14651858.CD012859.pub2
17. Murakami C, Kakuta N, Kume K, et al. A Comparison of Fosaprepitant and Ondansetron for Preventing Postoperative Nausea and Vomiting in Moderate to High Risk Patients: a Retrospective Database Analysis. Biomed Res Int. 2017;2017:5703528. doi:10.1155/2017/5703528
18. Kakuta N, Kume K, Hamaguchi E, et al. The effects of intravenous fosaprepitant and ondansetron in the prevention of postoperative nausea and vomiting in patients who underwent lower limb surgery: a prospective, randomized, double-blind study. J Anesth. 2015;29(6):836–841. doi:10.1007/s00540-015-2054-4
19. Tsutsumi YM, Kakuta N, Soga T, et al. The effects of intravenous fosaprepitant and ondansetron for the prevention of postoperative nausea and vomiting in neurosurgery patients: a prospective, randomized, double-blinded study. Biomed Res Int. 2014;2014:307025. doi:10.1155/2014/307025
20. Zhu H, Wang S, Wang R, Li B, Zhang J, Zhang W. Effect of dexmedetomidine on postoperative nausea and vomiting in female patients undergoing radical thoracoscopic lung cancer resection. Front Pharmacol. 2024;15:1353620. doi:10.3389/fphar.2024.1353620
21. Hopewell SCA, Collins GS, Hróbjartsson A, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. JAMA. 2025;405(10489):1633–1634. doi:10.1001/jama.2025.4347
22. Cruz NI, Portilla P, Vela RE. Timing of ondansetron administration to prevent postoperative nausea and vomiting. P R Health Sci J. 2008;27(1):43–47.
23. Kushner BS, Freeman D, Sparkman J, Salles A, Eagon JC, Eckhouse SR. Assessment of postoperative nausea and vomiting after bariatric surgery using a validated questionnaire. Surg Obes Relat Dis. 2020;16(10):1505–1513. doi:10.1016/j.soard.2020.05.017
24. Brearley SG, Clements CV, Molassiotis A. A review of patient self-report tools for chemotherapy-induced nausea and vomiting. Support Care Cancer. 2008;16(11):1213–1229. doi:10.1007/s00520-008-0428-y
25. Moradian S, Shahidsales S, Ghavam Nasiri MR, Pilling M, Molassiotis A, Walshe C. Translation and psychometric assessment of the Persian version of the Rhodes Index of Nausea, Vomiting and Retching (INVR) scale for the assessment of chemotherapy-induced nausea and vomiting. Eur J Cancer Care (Engl). 2014;23(6):811–818. doi:10.1111/ecc.12147
26. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the Common Terminology Criteria for Adverse Events (CTCAE - Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies [CTCAE versión 5.0. Evaluación de la gravedad de los eventos adversos dermatológicos de las terapias antineoplásicas]. Actas Dermosifiliogr. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
27. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: european Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
28. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
29. Zhang Y, Yang Y, Cheng C, Hou G, Ding X, Ma J. Based -evidence, an intervention study to improve sleep quality in awake adult ICU patients: a prospective, single-blind, clustered controlled trial. Crit Care. 2024;28(1):365. doi:10.1186/s13054-024-05161-1
30. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
31. Kienbaum P, Schaefer MS, Weibel S, et al. Update on PONV-What is new in prophylaxis and treatment of postoperative nausea and vomiting?: summary of recent consensus recommendations and Cochrane reviews on prophylaxis and treatment of postoperative nausea and vomiting. Anaesthesist. 2022;71(2):123–128. Update PONV - Was gibt es Neues bei der Prophylaxe und Therapie von postoperativer Ubelkeit und postoperativem Erbrechen?: Zusammenfassung rezenter Konsensusempfehlungen sowie Cochrane-Reviews zu Prophylaxe und Therapie postoperativer Ubelkeit und postoperativen Erbrechens. doi:10.1007/s00101-021-01045-z
32. Yokoi A, Mihara T, Ka K, Goto T. Comparative efficacy of ramosetron and ondansetron in preventing postoperative nausea and vomiting: an updated systematic review and meta-analysis with trial sequential analysis. PLoS One. 2017;12(10):e0186006. doi:10.1371/journal.pone.0186006
33. Wu S, Gan C, Huang X, et al. Incidence and risk factors of postoperative nausea and vomiting in lung cancer patients following lobectomy and application of analgesic pumps. The Journal of International Medical Research. 2022;50:03000605221105343. doi:10.1177/03000605221105343
34. Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
35. Apfel CC, Korttila K, Abdalla M, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350(24):2441–2451. doi:10.1056/NEJMoa032196
36. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
37. Weinstein C, Jordan K, Green SA, et al. Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with moderately emetogenic chemotherapy: results of a randomized, double-blind phase III trial. Ann Oncol. 2016;27(1):172–178. doi:10.1093/annonc/mdv482
38. Hata A, Okamoto I, Inui N, et al. Randomized, Double-Blind, Phase III Study of Fosnetupitant Versus Fosaprepitant for Prevention of Highly Emetogenic Chemotherapy-Induced Nausea and Vomiting: CONSOLE. J Clin Oncol. 2022;40(2):180–188. doi:10.1200/jco.21.01315
39. Frank E, Harrell J. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis. 2015.
40. Soga T, Kume K, Kakuta N, et al. Fosaprepitant versus ondansetron for the prevention of postoperative nausea and vomiting in patients who undergo gynecologic abdominal surgery with patient-controlled epidural analgesia: a prospective, randomized, double-blind study. J Anesth. 2015;29(5):696–701. doi:10.1007/s00540-015-2006-z
41. Yang C, Xu P, Wu T, et al. Safety assessment of neurokinin-1 receptor antagonist: real-world adverse event analysis from the FAERS database. Front Pharmacol. 2024;15:1413709. doi:10.3389/fphar.2024.1413709
42. Lee DJ, Douglas JE, Chang J, et al. The use of aprepitant for the prevention of postoperative nausea and vomiting in endoscopic transsphenoidal pituitary surgery. Int Forum Allergy Rhinol. 2023;13(12):2180–2186. doi:10.1002/alr.23208
43. Milnes V, Gonzalez A, Amos V. Aprepitant: a New Modality for the Prevention of Postoperative Nausea and Vomiting: an Evidence-Based Review. J Perianesth Nurs. 2015;30(5):406–417. doi:10.1016/j.jopan.2014.11.013
44. Liu M, Zhang H, Du BX, et al. Neurokinin-1 receptor antagonists in preventing postoperative nausea and vomiting: a systematic review and meta-analysis. Medicine (Baltimore). 2015;94(19):e762. doi:10.1097/MD.0000000000000762
45. Sharun K, Jambagi K, Arya M, et al. Clinical Applications of Substance P (Neurokinin-1 Receptor) Antagonist in Canine Medicine. Arch Razi Inst. 2021;76(5):1175–1182. doi:10.22092/ari.2021.356171.1797
46. Horn CC, Wallisch WJ, Homanics GE, Williams JP. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi:10.1016/j.ejphar.2013.10.037
47. Karthaus M, Schiel X, Ruhlmann CH, Celio L. Neurokinin-1 receptor antagonists: review of their role for the prevention of chemotherapy-induced nausea and vomiting in adults. Expert Rev Clin Pharmacol. 2019;12(7):661–680. doi:10.1080/17512433.2019.1621162
48. Ganguly S, Sasi A, Nagaraju SKK, Bakhshi S. Anti-Emetics in Children Receiving Chemotherapy for Solid Tumors and Leukemia: pharmacology and Optimization of Therapy for Nausea and Vomiting. Pharmaceuticals. 2024;17(5):616. doi:10.3390/ph17050616
49. Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery A Review. Review. JAMA Surgery. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
50. Kovac AL. Update on the management of postoperative nausea and vomiting. Drugs. 2013;73(14):1525–1547. doi:10.1007/s40265-013-0110-7
51. Diemunsch P, Joshi GP, Brichant JF. Neurokinin-1 receptor antagonists in the prevention of postoperative nausea and vomiting. Br J Anaesth. 2009;103(1):7–13. doi:10.1093/bja/aep125
52. Weibel S, Schaefer MS, Raj D, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: an abridged Cochrane network meta-analysis. Anaesthesia. 2021;76(7):962–973. doi:10.1111/anae.15295
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Perineural Dexamethasone with Ropivacaine in Continuous Serratus Anterior Plane Block for Postoperative Analgesia in Patients Undergoing Video-Assisted Thoracoscopic Surgery
Chen JQ, Chen JR, Wang S, Gao W, Gu H, Yang XL, Hu JC, Chai XQ, Wang D
Journal of Pain Research 2022, 15:2315-2325
Published Date: 13 August 2022