Back to Journals » Advances in Medical Education and Practice » Volume 10
Five decades of research and theorization on clinical reasoning: a critical review
Authors Yazdani S ![]() , Hoseini Abardeh M
, Hoseini Abardeh M
Received 26 April 2019
Accepted for publication 22 July 2019
Published 27 August 2019 Volume 2019:10 Pages 703—716
DOI https://doi.org/10.2147/AMEP.S213492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Video abstract presented by Maryam Hoseini Abardeh.
Views: 1346
Shahram Yazdani, Maryam Hoseini Abardeh
Department of Medical Education, School of Medical Education, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence: Maryam Hoseini Abardeh
School of Medical Education, Shahid Beheshti University of Medical Sciences, Shahid Chamran Highway, Tehran Velenjak Street, Tehran, Iran
Tel +98 212 243 9982
Fax +98 212 243 9784
Email [email protected]
Abstract: Clinical reasoning is a complex cognitive process that is essential to evaluate and manage a patient’s medical problem. The aim of this paper was to provide a critical review of the research literature on clinical reasoning theories and models. To conduct our study, we applied the process of conducting a literature review in four stages in accordance with the approach of Carnwell and Daly. First, we defined the scope of the review as being limited to clinical reasoning theories and models in medical education. In the second stage, we conducted a search based on related words in PubMed, Google Scholar, PsycINFO, ERIC, ScienceDirect and Web of Science databases. In the third stage, we classified the results of the review into three categories, and in the fourth stage, we concluded and informed further studies. Based on the inclusion and exclusion criteria, 31 articles were eligible to be reviewed. Three theories and two models were recognized and classified into three categories. Several theories and models have been proposed in relation to clinical reasoning, but it seems that these theories and models could only explain part of this complex process and not the whole process. Therefore, to fulfill this gap, it may be helpful to build a Meta-model or Meta-theory, which unified all the models, and theories of clinical reasoning.
Keywords: clinical reasoning, medical education, review
Introduction
Clinical reasoning is a complex cognitive process that is essential to evaluate and manage a patient’s medical problem.1 It includes the diagnosis of the patient problem, making a therapeutic decision and estimating the prognosis for the patient.2 In describing the importance of clinical reasoning, it has been acknowledged that clinical reasoning is the central part of physician competence,3 and stands at the heart of the clinical practice,4 it has an important role in physicians’ abilities to make diagnoses and decisions.1 Clinical reasoning has been the subject of academic and scientific research for decades;5 and its theoretical underpinning has been studied from different perspectives.6 Clinical reasoning is a challenging, promising, complex, multidimensional, mostly invisible,7 and poorly understood process.8 Researchers have explored its nature since 1980,9 but due to the lack of theoretical models, it remains vague. Most used theoretical models have limited explanatory power, and are based on certain assumptions about what constitutes clinical reasoning.10 In the literature of clinical reasoning, several competing theories and models have been raised.1,11–13 Although most of the theoretical contributions on clinical reasoning belong to the 20th century, proposing new models are well continued into the 21st century, for example, Haring and her colleagues proposed a conceptual model for expert judgment of clinical reasoning of medical students.14 However, there is no general agreement as to which of these is the best.15 The purpose of this paper is to provide a critical review of the research literature on clinical reasoning theories and models and present a comprehensive view of main models and theories of clinical reasoning in medical education. A clearer understanding of clinical reasoning models and theories help medical teachers for teaching, planning, and assessment of clinical reasoning. This paper tries to clarify the current knowledge regarding the clinical reasoning models and theories and present a classification of the main theories and models.
Materials and methods
Grant noted, “A critical review aims to demonstrate that the writer has extensively researched the literature and critically evaluated its quality.”16 It included a degree of analysis and conceptual innovation.16 In this study, we applied the process of conducting a literature review according to Carnwell and Daly.17 They proposed a “four-stage” method that included: 1) “Defining the scope of the review,” 2) “Identifying and selecting the sources of relevant information,” 3) “Organizing the results of the review into categories,” and 4) “Concluding and informing further studies.”17
Step 1: defining the scope of the review
The scope of this review was limited to the main clinical reasoning theories and models proposed in medical education literature. We concentrated our review on published works in scholarly journals between the years 1970 and 2018.
Step 2: identifying and selecting the sources of relevant information
At this stage, each of the two reviewers conducted a separate search based on keywords – “clinical reasoning,” “diagnostic reasoning,” “clinical reasoning theory,” “clinical reasoning model,” “script theory,” “hypothetico–deductive model,” “cognitive continuum theory,” and “dual processing theory” – in PubMed, Google Scholar, PsycINFO, ERIC, ScienceDirect and Web of Science databases. The results were pooled and extensive literature were found (n=305) which was from 1970 to 2018, but due to lack of access to the full text of some articles, and after removing duplicated studies, the title and abstract of articles from 1974 up to 2018 have been reviewed by researchers (n=170) (Table 1).
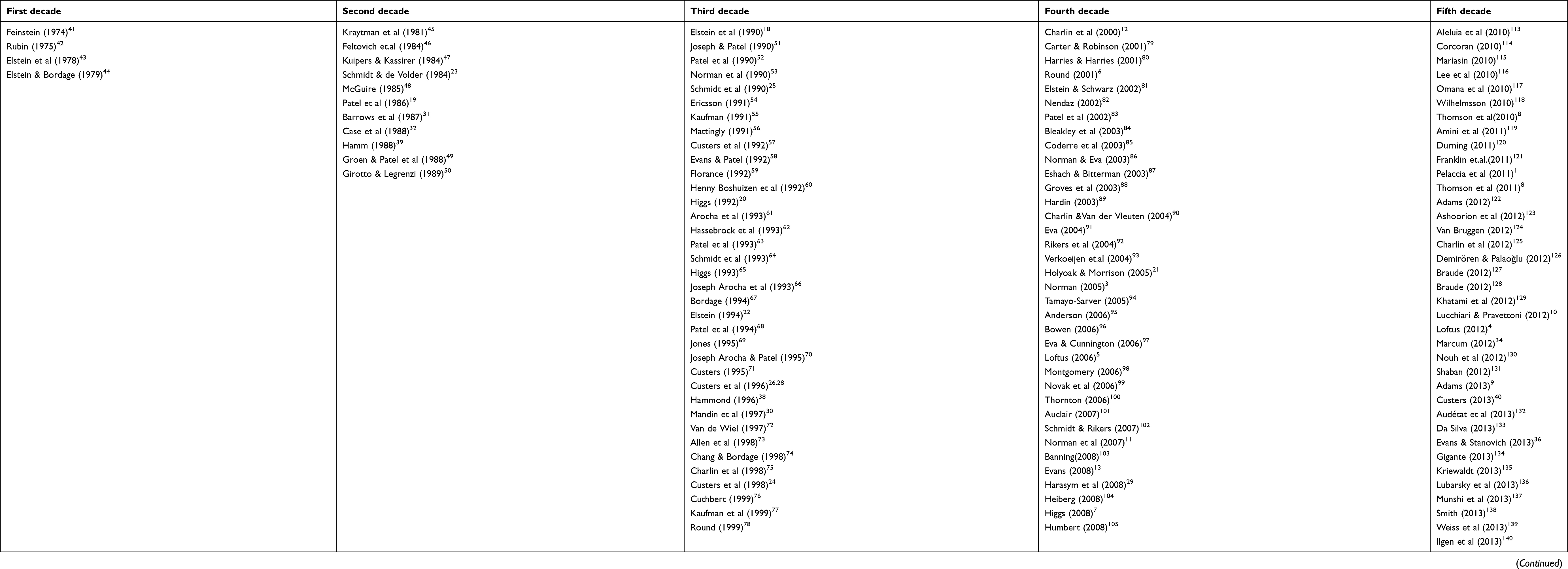 |
Table 1 Scientific studies about clinical reasoning that has been title and abstract reviewed |
Then, the articles that presented theories or models of clinical reasoning in medicine or provided evidence in relation to them were selected to full-text study. Studies were eligible for this critical review if they presented a model or a theory of clinical reasoning, or related critiqued models and theories or the studies that add some features to the theories and models of clinical reasoning (n=47). The inclusion criteria of selecting studies were: 1) published articles in English and Persian and 2) published articles in the field of medicine. Studies were excluded if they provided clinical reasoning models or theories in other fields (like nursing and optometry), examined the clinical reasoning in the field of artificial intelligence (like clinical decision support systems), and/or examined brain biology and brain functions (like fMRI studies).
Step 3: organizing the results of the review into categories
After excluding irrelevant studies, a total of 31 documents were initially selected for review which is shown in PRISMA flowchart below (Figure 1).
 |
Figure 1 PRISMA flowchart. |
Models and theories which were extracted from studies, classified to three categories and each category, based on Carnwel and Daly approach, reviewed in three steps: first, we present a summary of the models and theories, and then reflect other author’s views and finally, we present our view (Table 2).17 If a model or theory explains about the process of clinical reasoning our first category owns it while models and theories which clarified the formation of knowledge structures and their application during the clinical reasoning process belongs to the second category, and our third category consisted models and theories which consider more than one processing modes of clinical reasoning.
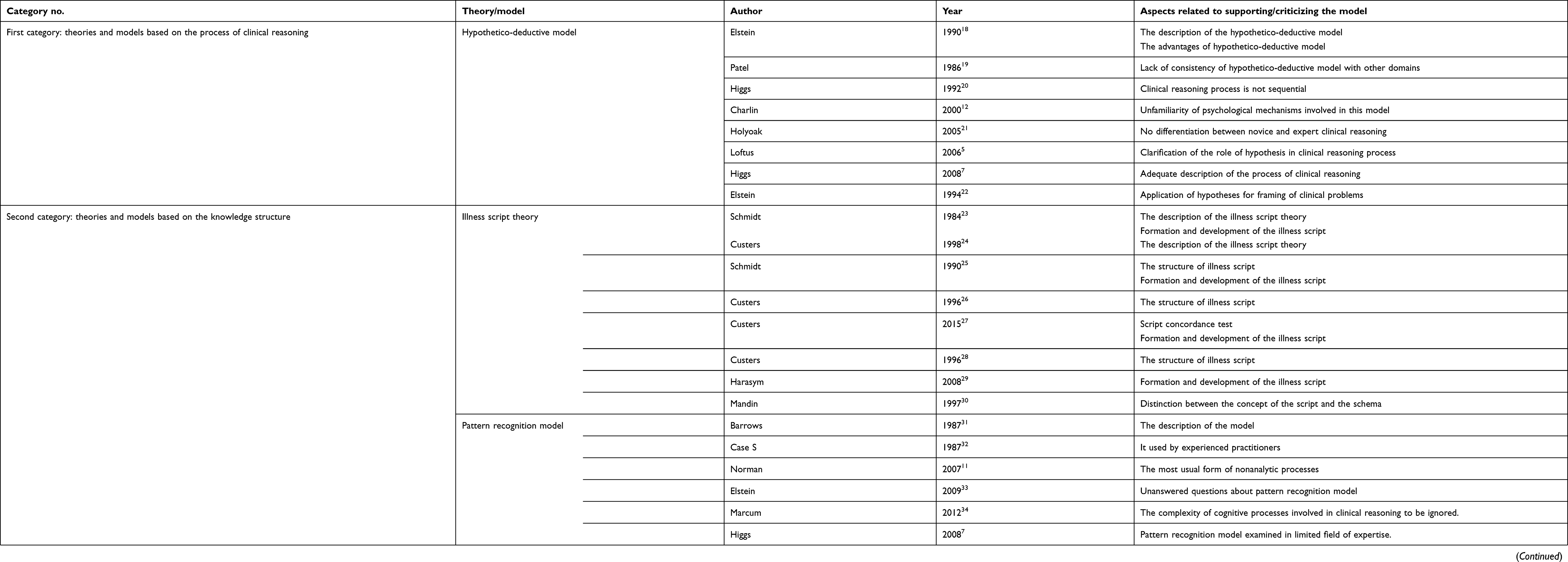 |
Table 2 The list of 31 related literatures that included in the review |
Results
First category: theories and models based on the process of clinical reasoning
This category includes the models and theories that explain the clinical reasoning process, between models and theories that we reviewed, only hypothetico-deductive model was eligible to get placed in the first category as the most reputed model that explains the clinical reasoning process. This model was proposed by Elstein (1978), and, according to this model, the physicians primarily generate a limited number of diagnostic hypotheses or problem formulations in the process of solving a diagnostic problem and then testing them. These hypotheses guide further patient information.18,19 Unlike the findings of hypothetico-deductive model that claim: “primarily generated and tested hypotheses by expert and novice are the same,” Patel believed that it is not consistent in other domains, like physics.19
Higgs argued that this model posits the idea that the process of clinical reasoning is largely a sequential process.20 Charlin pointed out that the psychological mechanisms involved in the generation and testing of relevant hypotheses are unfamiliar,12 and Holyoak argued that this model does not distinguish between novice and expert clinical reasoning strategies.21 Loftus believed that the collected information and the way they interpreted, distorted by the used hypothesis.5 This model as an adequate description of the process of clinical reasoning has challenged by the case specificity findings.7
Nevertheless, some researchers defend hypothetico-deductive model, Elstein argued that the small set of solutions that generated in this model transformed an unstructured problem to structured one and it is an effective way to solve diagnostic problems.18 This model is recommended by medical experts as a useful reasoning strategy for medical students.22 Hypothetico-deductive model is applicable when data are vague or reveal over time,22 and is a representation of clinical reasoning.20 This model represents a description of the mental processes used by physicians and has repeatedly been validated by empirical studies and is the basis for modern clinical education.12
Hypothetico-deductive model assumes the physician starts hypothesizing after collecting patient information and then tests hypotheses, while we believe the physician starts hypothesizing initially from his/her clinical encounter. The initial hypotheses can be strong or weak, depending on whether the physician is an expert or novice, the difference between the novice and the expert lies in the quality of the hypotheses they made. Therefore, since the initial hypothesis of an expert has good quality, hypothesis testing will be fast and efficient. The simplicity of this model in describing the process of clinical reasoning is both strength and the weakness of it, as a strength, because it simply portrays the start point of the process of clinical reasoning so it can be used to design the teaching plan and evaluate clinical reasoning. As a weakness, because it considers the process of diagnostic reasoning very simple, while even for a novice, this process does not occur so easily, and other factors (such as the individual’s knowledge structure, the context, the health system, etc.) affect the process of clinical reasoning, but this model does not consider these factors.
Second category: theories and models based on the knowledge structure
For this category, we considered theories and models that explain the formation of knowledge structures in the clinical reasoning process, by this description and the inclusion criteria just one theory and one model of clinical reasoning gain eligibility to include, the “illness script theory” and the “pattern recognition model.”
The illness script theory proposed by Barrows and Feltovich consists of three components: 1) enabling conditions, 2) fault, and 3) consequences.23 The first component is the factors such as age, sex, current medication, previous medical history, occupation, risk behavior, hereditary, and environment affect the probability of someone gets a disease, are the patient’s contextual and background factors that refer to “Enabling conditions.” These “Enabling conditions” can cause the latter pathophysiological malfunctioning that called “fault” which is the second component of illness script. Consequences of this fault are complaints, signs, and symptoms that consist of the third component.24 Illness scripts are the list-like structures,25 which conceptualized as a specific representation of clinical knowledge.26 Script concordance test designed according to this theory.27
While we were studying about Illness script theory, we realized that we could categorize studies into two broad groups. The first group is the studies that deal with the concept of the script, the schema, and the illness script, and their features, distinctions, and components (Table 3).24,26–28
 |
Table 3 The studies that deal with the concept of “script,” “schema,” and “illness script,” and their features, distinctions, and components |
The second group deals with the formation and development of the illness script during the acquisition of expertise and changes in the physician’s knowledge structure (Table 4).23,25,26,29
 |
Table 4 The studies that deal with the formation and development of “illness script” during the acquisition of expertise and changes in the physician’s knowledge structure |
The first group of studies also looked at the distinction between the concept of the script and the schema, but this distinction was not clear in the literature. The schemas and scripts are stored in long-term memory.30
Schema as a knowledge structure has an “if/then” formatting and occurs sequentially, in the sense that this sequence divided into two branches: “if” and “then,” so we can claim out that its format is algorithmic. This algorithm starts with a hypothesis in a person’s mind or something that a person thinks about and then continues with inquiries and searches that a physician has performed and then with the findings that a physician has reached, and finish with the decisions that he/she has finally taken (Figure 2).
 |
Figure 2 Generic flow of events in a typical schema. D1: Decision No 1; D5: Decision No 6; F1: Finding No 1; F5: Finding No 5; H1: Hypothesis No 1; H2: Hypothesis No 2; I1: Inquiry No 1; I3: Inquiry No 3. |
In terms of the structure of the script, we also agree with Schmidt’s view that the scripts are list-like structures, but unlike Charlin, who believed that “the script describes the structure of clinical knowledge,” we believe that the script is not necessarily the structure of clinical knowledge, but a knowledge structure that has clinical applications. The script is schemas for common situations, which include a packet or a list of expectations of what people see or do at a given location. The schemas and scripts are stored in long-term memory, and if physicians encounter a clinical case that matches with them, they will retrieve it from long-term memory and move it to short-term memory (Figure 3).
 |
Figure 3 Script as a routinized pathway of previously used schema. D1: Decision No 1; D5: Decision No 6; F1: Finding No 1; F5: Finding No 5; H1: Hypothesis No 1; H2: Hypothesis No 2; I1: Inquiry No 1; I3: Inquiry No 3. |
Pattern recognition model
In the pattern recognition model, a physician directly compares the pattern of the patient’s problem with disease patterns and if found them similar to each other, then select the pattern that matches it.31 Experienced practitioners often use pattern recognition to achieve a medical diagnosis.32 Norman and his colleagues argue that pattern recognition is the most usual form of nonanalytic processes.11 However, Elstein proposed some questions about this model, as followed:
- When dose a person use a pattern recognition model?
- When is this method preferable to the hypothetico-deductive method?
- What guarantees that the choice of a pattern or an illness script is correct?
- What happens if the pattern or script stored in the knowledge base is wrong?33
This model considers the complexity of cognitive processes involved in clinical reasoning to be insignificant.34
Based on the definition of the pattern recognition model, it only mentions the existence of patterns in mind, but does not explain how the construction of these patterns occurred. The studies which designed to prove that the pattern recognition model happens in reality are in a limited field of expertise, like radiology, dermatology, and pathology. 7 So the pattern recognition model is not extendable to all medical specialties.
Third category: compilation theories and model
Some of the included documents were about “dual processing” and “cognitive continuum” theories that explain two modes of reasoning – “analytical” and “non-analytical,” these modes are the characteristics of both first and second category, so we cannot involve them in one of them, therefore they form our third category.
The dual-processing theories commonly have two different processing modes in which they refer to: System 1 and System 2.13 System 1 described as a fast, automatic and intuitive mode, which shares similarities through perception, while System 2 is slow and analytic mode that applies rules without inferring emotions.7
Croskerry believed that dual-processing theory is an applicable model in multiple domains of health care like decision-making and it can be useful in teaching decision theory or in making a platform to future research.35 Pelaccia et al noted that in the framework of this theory, the pattern recognition and hypothetico-deductive models are the basis of the intuitive system and the analytic system, respectively.1
Evans and Stanovich criticized this theory in five major themes: 1) various theorists have proposed multiple and vague definitions for this theory, 2) there is no consistency in associated attribute clusters with dual systems, 3) distinctions are referred to the continuum of processing and not to discrete processing; 4) the apparent dual-process phenomenon can present by single-process accounts; and 5) the evidence base for the dual-processing theory is ambiguous or unconvincing.36
In the reviewing of the literature, we found out that some of the researchers established their models based on dual-processing theory like Marcum,34 Croskerry,35,37 and Lucchiari and Pravettoni.10
Dual-processing theory employs many of the seemingly contradictory features that have been proposed for clinical reasoning in the literature (such as fast, slow, reflective, etc.). It seems that, in reality, a physician does not use just intuitive or analytic systems and the mind of physician operates in the space between them, while the dual-processing theory ignores this.
The theories and models that have been proposed following this theory have led to the introduction of cognitive concepts such as metacognition and perception and their role in the process of clinical reasoning. This theory has relatively clarified the role of emotions and their place of influence in the process of clinical reasoning, and has also contributed to clarifying the concept of intuition in clinical reasoning.
The second theory that has placed in third categories is cognitive continuum, as Hammond claimed, this theory considered two poles, an intuitive cognition and an analytical cognition, in which various modes or forms of cognition have relational order on a continuum, and this assumption rejected the dual-processing approach.38 Hamm believed, this theory does not explain the information processing that is the basis of analysis and intuition, but based on analytical and intuitive cognitive attributes it gives us various techniques in describing cognitive modes. Also, he believed that this theory did not offer an instruction about thinking analytically or intuitively, and it just presented a general framework. Cognitive continuum theory described the features of cognition and their correlation with the characteristics of the task.39 Custers noted that this theory illustrates the cognitive processes and the cognitive tasks on a continuum, and this theory can be used to provide advice on how to structure clinical tasks in an educational setting.40 In criticizing cognitive continuum theory, we did totally agree with Hamm and Custers.
Conclusion
The present study was conducted to critically review theories and models of clinical reasoning that have often been raised in the medical education literature within five decades (1970–2018). Several theories and models presented in relation to clinical reasoning and it seems that they can explain only part of the complex process, but not the whole process. For example, the models and theories of the first category in our study just address the process of clinical reasoning and do not pay attention to knowledge structures and cognition; in the second category, they just focused on knowledge structures and their formations during clinical reasoning process and do not clarify the process of clinical reasoning. In addition, the dual processing and cognitive continuum theories that form the third category just covered the cognition part of the clinical reasoning. Therefore, to fulfill this gap, it may be helpful to build a Meta-model or Meta-theory, which unified all the models, and theories of clinical reasoning. Although our focus was on the main models and theories of clinical reasoning in the field of medical education, but we acknowledge that there are other models and theories of clinical reasoning in the literature and their absence can be the bias of this study.
Acknowledgment
This work was part of a PhD dissertation, funded and financially supported by the Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pelaccia T, Tardif J, Triby E, Charlin B. An analysis of clinical reasoning through a recent and comprehensive approach: the dual-process theory. Med educ online. 2011;16.
2. Daly P. A concise guide to clinical reasoning. J Eval Clin Pract. 2018;24(5):966–972.
3. Norman G. Research in clinical reasoning: past history and current trends. Med educ. 2005;39(4):418–427.
4. Loftus S. Rethinking clinical reasoning: time for a dialogical turn. Med educ. 2012;46(12):1174–1178.
5. Loftus SF. Language in Clinical Reasoning: Learning and Using the Language of Collective Clinical Decision Making.Sydney, Australia: University of Sydney. 2006
6. Round A. Introduction to clinical reasoning. J Eval Clin Pract. 2001.
7. Higgs J, Jones M, Loftus S, Christensen N. Clinical Reasoning in the Health Professions.
8. Thomson O, Petty N, J, Moore A. Clinical reasoning in osteopathy e More than just principles? Int J Osteopath Med. 2011;14: 71–76.
9. Adams L. Clinical Reasoning and Causal Attribution in Medical Diagnosis.Thesis. University of Plymouth. 2013.
10. Lucchiari C, Pravettoni G. Cognitive balanced model: a conceptual scheme of diagnostic decision making. J Eval Clin Pract. 2012;18(1):82–88.
11. Norman G, Young M, Brooks L. Non‐analytical models of clinical reasoning: the role of experience. Med educ. 2007;41(12):1140–1145.
12. Charlin B, Tardif J, Boshuizen H. Scripts and medical diagnostic knowledge: theory and applications for clinical reasoning instruction and research. Acad Med. 2000;75(2):182–190.
13. Evans JSB. Dual-processing accounts of reasoning, judgment, and social cognition. Annu. Rev. Psychol. 2008;59:255–278.
14. Haring CM, et al. Observable phenomena that reveal medical students' clinical reasoning ability during expert assessment of their history taking: a qualitative study. . BMC med educ. 2017;17(1):147.
15. Stempsey WE. Clinical reasoning: new challenges. Theor Med Bioeth. 2009;30(3):173–179.
16. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009;26(2):91–108.
17. Carnwell R, Daly W. Strategies for the construction of a critical review of the literature. Nurse Educ Pract. 2001;1(2):57–63.
18. Elstein AS, Shulman LS, Sprafka SA. Medical problem solving a ten-year retrospective. Eval Health Prof. 1990;13(1):5–36.
19. Patel VL, Groen GJ. Knowledge based solution strategies in medical reasoning. Cogn Sci. 1986;10(1):91–116.
20. Higgs J. Developing clinical reasoning competencies. Physiotherapy. 1992;78(8):575–581.
21. Holyoak KJ, Morrison R. The Cambridge Handbook of Thinking and Reasoning. Cambridge, UK: Cambridge University Press; 2005.
22. Elstein AS. What goes around comes around: return of the hypothetico‐deductive strategy. TEACH LEARN MED: An International Journal. 1994;6(2):121–123.
23. Schmidt HG, de Volder ML. Tutorials in Problem-based Learning: New Directions in Training for the Health Professions. 1st International Symposium. Van Gorcum; 1984.
24. Custers EJ, Boshuizen HP, Schmidt HG. The role of illness scripts in the development of medical diagnostic expertise: Results from an interview study. Cogn Instr. 1998;16(4):367–398.
25. Schmidt H, Norman G, Boshuizen H. A cognitive perspective on medical expertise: theory and implication [published erratum appears in Acad Med 1992 Apr; 67 (4): 287]. Acad med. 1990;65(10):611–621.
26. Custers EJ, Boshuizen HP, Schmidt HG. The influence of medical expertise, case typicality, and illness script component on case processing and disease probability estimates. Mem Cognit. 1996;24(3):384–399.
27. Custers EJ. Thirty years of illness scripts: Theoretical origins and practical applications. Med teach. 2015;37(5):457–462.
28. Custers E, Regehr G, Norman GR. Mental representations of medical diagnostic knowledge: a review. Acad Med. 1996;71(10):S55–61.
29. Harasym PH, Tsai T-C, Hemmati P. Current trends in developing medical students' critical thinking abilities. Kaohsiung J Med Sci. 2008;24(7):341–355.
30. Mandin H, Jones A, Woloschuk W, Harasym P. Helping students learn to think like experts when solving clinical problems. Acad med: journal of the Association of American Medical Colleges. 1997;72(3):173–179.
31. Barrows HS, Feltovich PJ. The clinical reasoning process. Med Educ. 1987;21(2):86–91.
32. Case S, Swanson D, Stillman P Evaluating diagnostic pattern recognition: the psychometric characteristics of a new item format. Paper presented at: Research in medical education: proceedings of the … annual Conference. Conference on Research in Medical Education; United States: Whashington, DC; 1987.
33. Elstein AS. Thinking about diagnostic thinking: a 30-year perspective. Adv Health Sci Educ Theory Pract. 2009;14(1):7–18.
34. Marcum JA. An integrated model of clinical reasoning: dual‐process theory of cognition and metacognition. J Eval Clin Pract. 2012;18(5):954–961.
35. Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv Health Sci Educ. 2009;14(1):27–35.
36. Evans JSB, Stanovich KE. Dual-process theories of higher cognition advancing the debate. Perspect Psychol Sci. 2013;8(3):223–241.
37. Croskerry P. A universal model of diagnostic reasoning. Acad med. 2009;84(8):1022–1028.
38. Hammond KR. Human Judgment and Social Policy: Irreducible Uncertainty, Inevitable Error, Unavoidable Injustice. New York: Oxford University Press; 1996.
39. Hamm RM. Clinical intuition and clinical analysis: expertise and the cognitive continuum. In: Professional Judgment: A Reader in Clinical Decision Making. Cambridge, UK: Cambridge University Press; 1988:78–105.
40. Custers EJ. Medical education and cognitive continuum theory: an alternative perspective on medical problem solving and clinical reasoning. Acad Med. 2013;88(8):1074–1080.
41. Feinstein AR. An analysis of diagnostic reasoning. 3. The construction of clinical algorithms. Yale J Biol Med. 1974;47(1):5.
42. Rubin AD. Hypothesis formation and evaluation in medical diagnosis. 1975. Available from: https://dspace.mit.edu/handle/1721.1/6919.
43. Elstein AS, Shulman LS, Sprafka SA. Medical problem solving an analysis of clinical reasoning. Cambridge,US: Harvard University Press 1978.
44. Elstein A, Bordage G. Psychology or clinical reasoning. Stone G, Cohen F, Adler N, editors. Health psychology: a handbook. San Francisco: Jossey-Bass. 1979:335-367.
45. Kraytman M. The preparation of medical students in our country: some clinical observations. Acta clinica Belgica. 1981;36(5):223–226.
46. Feltovich PJ, Patel VL. The Pursuit of Understanding in Clinical Reasoning. 1984.
47. Kuipers B, Kassirer JP. Causal reasoning in medicine: analysis of a protocol. Cogn Sci. 1984;8(4):363–385.
48. McGuire CH. Medical problem-solving: a critique of the literature. J Med Educ.1985: 60(8):587–95
49. Groen GJ, Patel VL. The relationship between comprehension and reasoning in medical expertise. In: In M. T. H. Chi, R. Glaser, & M. J. Farr (Eds.), The nature of expertise . Hillsdale, NJ, US: Lawrence Erlbaum Associates, Inc1988: 287–310
50. Girotto V, Legrenzi P. Mental representation and hypothetico-deductive reasoning: The case of the THOG problem. Psychol Res. 1989;51(3):129–135.
51. Joseph G-M, Patel VL. Domain knowledge and hypothesis genenation in diagnostic reasoning. Med Decis Making. 1990;10(1):31–44.
52. Patel VL, Groen GJ, Arocha JF. Medical expertise as a function of task difficulty. Mem Cognit. 1990;18(4):394–406.
53. Norman GG, Patel V, Schmidt HH. Clinical inquiry and scientific inquiry. Med educ. 1990;24(4):396–399.
54. Ericsson KA, Smith J. Toward a general theory of expertise: Prospects and limits. New York, US: Cambridge University Press; 1991.
55. Kaufman SG. A Formal Theory of Spatial Reasoning. In Allen J, Fikes RE, Sandewall E..Principles of Knowledge Representation and Reasoning: Proceedings of the Second International Conference. Morgan Kaufmann Publishers.1991.
56. Mattingly C. The narrative nature of clinical reasoning. Am J Occup Ther. 1991;45(11):998–1005.
57. Custers EJ. The Relationship between Medical Expertise and the Development of Illness-Scripts. 1992-Apr. Belgium; Netherlands
58. Evans C, Kakas AC. Hypothetico-deductive Reasoning. Paper presented at: Fifth Generation Computer Systems. 1992. Tokyo, Japan
59. Florance V. Medical knowledge for clinical problem solving: a structural analysis of clinical questions. Bull Med Libr Assoc. 1992;80(2):140.
60. Boshuizen HP, Schmidt HG. On the role of biomedical knowledge in clinical reasoning by experts, intermediates and novices. Cogn Sci. 1992;16(2):153–184.
61. Arocha JF, Patel VL, Patel YC. Hypothesis generation and the coordination of theory and evidence in novice diagnostic reasoning. Med Decis Making. 1993;13(3):198–211.
62. Hassebrock F, Johnson PE, Bullemer P, Fox PW, Moller JH. When less is more: Representation and selective memory in expert problem solving. Am J Psychol. 1993:155–189.
63. Patel VL, Groen GJ, Norman GR. Reasoning and instruction in medical curricula. Cogn Instr. 1993;10(4):335–378.
64. Schmidt HG, Boshuizen HP. On acquiring expertise in medicine. Educ Psychol Rev. 1993;5(3):205–221.
65. Higgs J. A programme for developing clinical reasoning skills in graduate physiotherapists. Med teach. 1993;15(2–3):195–205.
66. Arocha JF, Patel VL, Patel YC. Hypothesis generation and the coordination of theory and evidence in novice diagnostic reasoning. Med Decis Making: an international journal of the Society for Medical Decision Making. Jul-Sep 1993;13(3):198–211.
67. Bordage G. Elaborated knowledge: a key to successful diagnostic thinking. Acad Med. 1994.
68. Patel V, Arocha JF, Kaufman D. Diagnostic reasoning and medical expertise.In. Medin, DL Advances in Research and Theory . 1994;31(C):187–252.
69. Jones M. Clinical reasoning and pain. Man Ther. 1995;1(1):17–24.
70. Arocha JF, Patel VL. Novice diagnostic reasoning in medicine: accounting for evidence. J Learn Sci. 1995;4(4):355–384.
71. Custers EJFM. The development and function of illness scripts: studies on the structure of medical diagnostic knowledge. Thesis. Maastricht University; 1995.
72. Van de Wiel M. Knowledge encapsulation:Studies on the deve;opment of medical expertise. thesis.Maastricht university, 1997.
73. Allen VG, Arocha JF, Patel VL. Evaluating evidence against diagnostic hypotheses in clinical decision making by students, residents and physicians. Int J Med Inform. Aug-Sep 1998;51(2–3):91–105.
74. Chang RW, Bordage G, Connell KJ. COGNITION, CONFIDENCE, AND CLINICAL SKILLS: the importance of early problem representation during case presentations. Acad Med. 1998;73(10):S109–111.
75. Charlin B. Script questionnaires: their use for assessment of diagnostic knowledge in radiology. Med Teach. 1998;20(6):567–571.
76. Cuthbert L, Duboulay, B., Teather, D., Teather, B., Sharples, M., & Duboulay, G. . Expert/novice differences in diagnostic medical cognition-A review of the literature. University of Sussex Cognitive Science Research paper CSRP #508, Feb. 1999, ISSN 1350–3162.
77. Kaufman DR, Kushniruk AW, Yale JF, Patel VL. Conceptual knowledge and decision strategies in relation to hypercholesterolemia and coronary heart disease. Int J Med Inform. Nov 1999;55(3):159–177.
78. Round AP. Teaching clinical reasoning--a preliminary controlled study. Med Educ. Jul 1999;33(7):480–483.
79. Carter MA, & Robinson, S. S. A narrative approach to the clinical reasoning process in pediatric intensive care: The story of Matthew. J Med Humanit. 2001;22(3):173–194.
80. Harries PA, Harries C. Studying clinical reasoning, part 2: Applying social judgement theory. Br J Occup Ther. 2001;64(6):285–292.
81. Elstein AS, Schwartz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ (Clinical research ed.). Mar 23 2002;324(7339):729–732.
82. Nendaz MR, Bordage G. Promoting diagnostic problem representation. Med Educ. Aug 2002;36(8):760–766.
83. Patel VL, Arocha JF, Kushniruk AW. Patients' and physicians' understanding of health and biomedical concepts: relationship to the design of EMR systems. J Biomed Inform. Feb 2002;35(1):8–16.
84. Bleakley A, Farrow R, Gould D, Marshall R. Making sense of clinical reasoning: judgement and the evidence of the senses. Med Educ. Jun 2003;37(6):544–552.
85. Coderre S, Mandin H, Harasym PH, Fick GH. Diagnostic reasoning strategies and diagnostic success. Med Educ. Aug 2003;37(8):695–703.
86. Norman GR, Eva KW. Doggie diagnosis, diagnostic success and diagnostic reasoning strategies: an alternative view. Med Educ. Aug 2003;37(8):676–677.
87. Eshach H, Bitterman H. From case-based reasoning to problem-based learning. Acad Med: journal of the Association of American Medical Colleges. May 2003;78(5):491–496.
88. Groves M, O'Rourke P, Alexander H. Clinical reasoning: the relative contribution of identification, interpretation and hypothesis errors to misdiagnosis. Med Teach. Nov 2003;25(6):621–625.
89. Hardin LE. Research in medical problem solving: a review. J Vet Med Educ. Fall 2003;30(3):230–235.
90. Charlin B, van der Vleuten C. Standardized assessment of reasoning in contexts of uncertainty: the script concordance approach. Eval Health Prof. Sep 2004;27(3):304–319.
91. Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. Jan 2005;39(1):98–106.
92. Rikers RM, Van Gerven PW, Schmidt HG. Cognitive load theory as a tool for expertise development. Instr Sci. 2004;32(1–2):173–182.
93. Verkoeijen PP, Rikers RM, Schmidt HG, van de Wiel MW, Kooman JP. Case representation by medical experts, intermediates and novices for laboratory data presented with or without a clinical context. Med Educ. Jun 2004;38(6):617–627.
94. Tamayo-Sarver JH, Dawson NV, Hinze SW, Cydulka RK, Wigton RS, Baker DW. Rapid clinical decisions in context: a theoretical model to understand physicians’ decision-making with an application to racial/ethnic treatment disparities. Health Care Services, Racial and Ethnic Minorities and Underserved Populations: Patient and Provider Perspectives: Emerald Group Publishing Limited; 2005:183–213.
95. Anderson KJ. Factors affecting the development of undergraduate medical students' clinical reasoning ability. Thesis. The university Adelaide. 2006.
96. Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. Nov 23 2006;355(21):2217–2225.
97. Eva KW, Cunnington JP. The difficulty with experience: does practice increase susceptibility to premature closure? J Contin Educ Health Prof. Summer 2006;26(3):192–198.
98. Mongtomery K. How doctors think: Clinical judgment and the practice of medicine. Oxford, United states: New York: Oxford University Press; 2005.
99. Novak K, Mandin H, Wilcox E, McLaughlin K. Using a conceptual framework during learning attenuates the loss of expert-type knowledge structure. BMC Med Educ. Jul 18 2006;6:37.
100. Thornton T. Tacit knowledge as the unifying factor in evidence based medicine and clinical judgement. PHILOS ETHICS HUM ME. Mar 17 2006;1(1):E2.
101. Auclair F. Problem formulation by medical students: an observation study. BMC med educ. Jun 17 2007;7:16.
102. Schmidt HG, Rikers RM. How expertise develops in medicine: knowledge encapsulation and illness script formation. Med Educ. Dec 2007;41(12):1133–1139.
103. Banning M. A review of clinical decision making: models and current research. J Clin Nurs. Jan 2008;17(2):187–195.
104. Heiberg Engel PJ. Tacit knowledge and visual expertise in medical diagnostic reasoning: implications for medical education. Med Teach. 2008;30(7):e184–188.
105. Humbert A. 15 Assessing the Clinical Reasoning Skills of Emergency Medicine Clerkship Students Using a Script Concordance Test. Acad Emerg Med. 2008;15:S230–S231.
106. Facione NC, Facione PA. Critical thinking and clinical judgment. Critical thinking and clinical reasoning in the health sciences: A teaching anthology. US, Millbrae, California Academic Press, 2008:1–13.
107. Vertue FM, Haig BD. An abductive perspective on clinical reasoning and case formulation. J Clin Psychol. Sep 2008;64(9):1046–1068.
108. Braude HD. Clinical intuition versus statistics: different modes of tacit knowledge in clinical epidemiology and evidence-based medicine. Theor Med Bioeth. 2009;30(3):181–198.
109. Bissessur SW, Geijteman EC, Al-Dulaimy M, et al. Therapeutic reasoning: from hiatus to hypothetical model. J Eval Clin Pract. Dec 2009;15(6):985–989.
110. Carriere B, Gagnon R, Charlin B, Downing S, Bordage G. Assessing clinical reasoning in pediatric emergency medicine: validity evidence for a Script Concordance Test. Annals of emergency medicine. May 2009;53(5):647–652.
111. Rehder B, Kim S. Classification as diagnostic reasoning. Mem Cognit. 2009;37(6):715–729.
112. Vosniadou S. International handbook of research on conceptual change. United states: New York. Routledge; 2009.
113. Aleluia IM, Carvalho PM,
114. Corcoran J, Walsh J. Clinical assessment and diagnosis in social work practice. Oxford, United states: New York: Oxford University; 2010.
115. Mariasin M. Novice, Generalist, and Expert Reasoning During Clinical Case Explanation: A Propositional Assessment of Knowledge Utilization and Application, thesis.University of Waterloo; 2010.
116. Lee A, Joynt GM, Lee AK, et al. Using illness scripts to teach clinical reasoning skills to medical students. Fam Med. 2010;42(4):255–261.
117. Elizondo-Omana RE, Morales-Gomez JA, Morquecho-Espinoza O, et al. Teaching skills to promote clinical reasoning in early basic science courses. Anat Sci Educ. Sep-Oct 2010;3(5):267–271.
118. Wilhelmsson N. From basic science knowledge to clinical understanding. Thesis. Karolinska Institutet,2010.
119. Amini M, Moghadami M, Kojuri J, et al. An innovative method to assess clinical reasoning skills: Clinical reasoning tests in the second national medical science Olympiad in Iran. BMC Res Notes. Oct 17 2011;4:418.
120. Durning S, Artino AR,
121. Franklin A, Liu Y, Li Z, et al. Opportunistic decision making and complexity in emergency care. J Biomed Inform. Jun 2011;44(3):469–476.
122. Adams JR, Elwyn G, Legare F, Frosch DL. Communicating with physicians about medical decisions: a reluctance to disagree. Arch Intern Med. Aug 13 2012;172(15):1184–1186.
123. Ashoorion V, Liaghatdar MJ, Adibi P. What variables can influence clinical reasoning? J Res Med Sci: the official journal of Isfahan University of Medical Sciences. 2012;17(12):1170.
124. van Bruggen L, Manrique-van Woudenbergh M, Spierenburg E, Vos J. Preferred question types for computer-based assessment of clinical reasoning: a literature study. Perspect Med Educ. Nov 2012;1(4):162–171.
125. Charlin B, Lubarsky S, Millette B, et al. Clinical reasoning processes: unravelling complexity through graphical representation. Med Educ. May 2012;46(5):454–463.
126. Demirören M, Palaoğlu Ö. Assessment of Medical Student’s Clinical Reasoning Skills in the Problem Based Learning-Integrated Curriculum. J Ankara Univ Fac Med. 2012, 65 (2)
127. Braude HD. Intuition in medicine: A philosophical defense of clinical reasoning. US: Chicago: University of Chicago Press; 2012.
128. Braude HD. Conciliating cognition and consciousness: the perceptual foundations of clinical reasoning. J Eval Clin Pract. 2012;18(5):945–950.
129. Khatami S, MacEntee MI, Pratt DD, Collins JB. Clinical reasoning in dentistry: a conceptual framework for dental education. J Dent Educ. Sep 2012;76(9):1116–1128.
130. Nouh T, Boutros M, Gagnon R, et al. The script concordance test as a measure of clinical reasoning: a national validation study. Am J Surg. Apr 2012;203(4):530–534.
131. Shaban R. Theories of clinical judgment and decision-making: A review of the theoretical literature. AJP. 2015;3(1).
132. Audetat MC, Laurin S, Sanche G, et al. Clinical reasoning difficulties: a taxonomy for clinical teachers. Med Teach. 2013;35(3):e984–989.
133. Da Silva A. Clinical reasoning development in medical students: An educational and transcultural comparative study, PhD thesis, University of; 2013.
134. Gigante J. Teaching Clinical Reasoning Skills to Help your Learners “Get” the Diagnosis. Pediat Therapeut, 2013;3(4).
135. Kriewaldt J, Turnidge D. Conceptualising an approach to clinical reasoning in the education profession. AJTE. 2013;38(6):7.
136. Lubarsky S, Dory V, Duggan P, Gagnon R, Charlin B. Script concordance testing: from theory to practice: AMEE guide no. 75. Med Teach. 2013;35(3):184–193.
137. Munshi FM, AlJarallah BM, Harasym PH. Problem Solving Strategy and Diagnostic Performance at Three Expertise Levels: Does the Problem Solving Approach Matter? J Health Educ Res Dev. 2013.
138. Smith M, Loftus S, Levett-Jones T. Teaching clinical reasoning.In: Loftus, S., Gerzina, T., Higgs, J., Smith, M., & Duffy, E. Educating Health Professionals: Dordrecht, Netherlands: SensePublishers; 2013:269–276.
139. Weiss MJ, Bhanji F, Fontela PS, Razack SI. A preliminary study of the impact of a handover cognitive aid on clinical reasoning and information transfer. Med Educ. Aug 2013;47(8):832–841.
140. Ilgen JS, Bowen JL, McIntyre LA, et al. Comparing diagnostic performance and the utility of clinical vignette-based assessment under testing conditions designed to encourage either automatic or analytic thought. Acad Med. Oct 2013;88(10):1545–1551.
141. L. Bowen J, S. Ilgen J. Now You See It, Now You Don't: What Thinking Aloud Tells Us About Clinical Reasoning. J Grad Med Educ. 2014;6(4):783–785.
142. Delany C, Golding C. Teaching clinical reasoning by making thinking visible: an action research project with allied health clinical educators. BMC Med Educ. Jan 30 2014;14:20.
143. Freiwald T, Salimi M, Khaljani E, Harendza S. Pattern recognition as a concept for multiple-choice questions in a national licensing exam. BMC Med Educ. 2014;14(1):232.
144. Geisler PR, Hummel C, Piebes S. Evaluating evidence-informed clinical reasoning proficiency in oral practical examinations. Athl Train Educ J. 2014;9(1):43–48.
145. Gordon M. Manual of nursing diagnosis. Jones & Bartlett Publishers; 2014.
146. Holmboe ES, Durning SJ. Assessing clinical reasoning: moving from in vitro to in vivo. Diagnosis (Berlin, Germany). Jan 1 2014;1(1):111–117.
147. Hrynchak P, Takahashi SG, Nayer M. Key-feature questions for assessment of clinical reasoning: a literature review. Med Educ. Sep 2014;48(9):870–883.
148. Hochberg L, Alm CO, Rantanen EM, DeLong CM, Haake A. Decision style in a clinical reasoning corpus. Proceedings of BioNLP 2014. USA. Baltimore, Maryland 2014:83–87.
149. Hochberg L, Alm CO, Rantanen EM, Yu Q, DeLong CM, Haake A. Towards automatic annotation of clinical decision-making style. Paper presented at: Proceedings of LAW VIII-The 8th Linguistic Annotation Workshop. Ireland, Dublin, 2014.
150. Monajemi A. The Role of Biomedical Knowledge in Clinical Reasoning: Bridging the Gap between Two Theories. IJBMC. 2014;1(2):102–106.
151. Roots, S. A. Clinical reasoning in osteopathy: an investigation of diagnostic hypothesis generation for patients with acute low back pain . Thesis. Unitec Institute of Technology. 2014.
152. Salkeld EJ. Framework negotiations: diagnostic insights among alternative medical practitioners participating in integrative medicine case conferences. Med Anthropol Q. Mar 2014;28(1):44–65.
153. Smith CS, Hill W, Francovich C, et al. Diagnostic Reasoning across the Medical Education Continuum. Healthcare (Basel, Switzerland). Jul 15 2014;2(3):253–271.
154. Capaldi VF, Durning SJ, Pangaro LN, Ber R. The clinical integrative puzzle for teaching and assessing clinical reasoning: preliminary feasibility, reliability, and validity evidence. Mil Med. Apr 2015;180(4 Suppl):54–60.
155. Gaba A. Teaching Clinical Judgment: A Review with Consideration of Applications for Health Professions. Open Nutr J. 2015;9(1).
156. Islam R, Weir CR, Jones M, Del Fiol G, Samore MH. Understanding complex clinical reasoning in infectious diseases for improving clinical decision support design. BMC Med Inform Decis Mak. Nov 30 2015;15:101.
157. Lafleur A, Cote L, Leppink J. Influences of OSCE design on students' diagnostic reasoning. Med Educ. Feb 2015;49(2):203–214.
158. Lubarsky S, Dory V, Audetat MC, Custers E, Charlin B. Using script theory to cultivate illness script formation and clinical reasoning in health professions education. Can Med Educ J. 2015;6(2):e61–70.
159. Park WB, Kang SH, Lee YS, Myung SJ. Does Objective Structured Clinical Examinations Score Reflect the Clinical Reasoning Ability of Medical Students? Am J Med Sci. Jul 2015;350(1):64–67.
160. Lisk K, Agur AM, Woods NN. Exploring cognitive integration of basic science and its effect on diagnostic reasoning in novices. Perspect Med Educ. Jun 2016;5(3):147–153.
161. McBee E, Ratcliffe T, Goldszmidt M, et al. Clinical Reasoning Tasks and Resident Physicians: What Do They Reason About? Acad Med : journal of the Association of American Medical Colleges. Jul 2016;91(7):1022–1028.
162. Gruppen LD. Clinical Reasoning: Defining It, Teaching It, Assessing It, Studying It. West J Emerg Med. Jan 2017;18(1):4–7.
163. Jarodzka H, Boshuizen HP. Unboxing the Black Box of Visual Expertise in Medicine. Frontline learn research. 2017;5(3):167–183.
164. Norman GR, Monteiro SD, Sherbino J, Ilgen JS, Schmidt HG, Mamede S. The Causes of Errors in Clinical Reasoning: Cognitive Biases, Knowledge Deficits, and Dual Process Thinking Acad Med: journal of the Association of American Medical Colleges. Jan 2017;92(1):23–30.
165. ten Cate O, Durning SJ. Understanding Clinical Reasoning from Multiple Perspectives: A Conceptual and Theoretical Overview. In: ten Cate O, Custers E, Durning SJ, eds. Principles and Practice of Case-based Clinical Reasoning Education: A Method for Preclinical Students. Switzerlan, Cham, Springer: 2018:35–46.
166. Zamani S, Amini M, Masoumi SZ, Delavari S, Namaki MJ, Kojuri J. The comparison of the key feature of clinical reasoning and multiple choice examinations in clinical decision makings ability. Biomed Re. 2017;28(3):1115–1119.
167. Bowen JL, ten Cate O. Prerequisites for Learning Clinical Reasoning. In: ten Cate O, Custers E, Durning SJ, eds. Principles and Practice of Case-based Clinical Reasoning Education: A Method for Preclinical Students. Switzerlan, Cham, Springer. 2018:47–63.
168. Custers EJ. Training Clinical Reasoning: Historical and Theoretical Background.In: In: ten Cate O, Custers E, Durning SJ, eds. Principles and Practice of Case-based Clinical Reasoning Education: A Method for Preclinical Students. Switzerlan, Cham, Springer; 2018:21–33.
169. King L, Kremser S, Deam P, et al. Clinical reasoning in osteopathy: Experiences of novice and experienced practitioners. INT J OSTEOPATH MED. 2018;28:12–19.
170. Keemink Y, Custers E, van Dijk S, Ten Cate O. Illness script development in pre-clinical education through case-based clinical reasoning training. Int J Med Educ. Feb 9 2018;9:35–41.
171. Lopes HF, Polson NG. Bayesian hypothesis testing: Redux. Cornel university.arXiv preprint arXiv:1808.08491. 2018.
172. Yazdani S, Abardeh MH. Clinical Reasoning in Medicine: A Concept Analysis. JMED. 2017;16(3).
173. Yazdani S, Hosseinzadeh M, Hosseini F. Models of clinical reasoning with a focus on general practice: A critical review. J Adv Med Educ Prof. Oct 2017;5(4):177–184.
174. Higgs J. Judgment and reasoning in professional contexts. In: Lanzer, P. ed., 2018. Textbook of Catheter-Based Cardiovascular Interventions: A Knowledge-Based Approach. Springer. 2018:15–25.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.