Back to Journals » Clinical Ophthalmology » Volume 20
First Clinical Results of a Multicentric Prospective Study on the Visual Performance of Patients Implanted with a New Trifocal Aspheric Hydrophobic Intraocular Lens
Authors Auffarth GU ![]() , Kretz FT, Tañá-Rivero P
, Kretz FT, Tañá-Rivero P
Received 2 July 2025
Accepted for publication 1 December 2025
Published 23 January 2026 Volume 2026:20 550873
DOI https://doi.org/10.2147/OPTH.S550873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gerd U Auffarth,1 Florian TA Kretz,2 Pedro Tañá-Rivero3
1Department of Ophthalmology, International Vision Correction Research Centre (IVCRC), The David J. Apple International Laboratory for Ocular Pathology, Ruprecht-Karls-University of Heidelberg, Heidelberg, Germany; 2Department of Ophthalmology, Precise Vision Augenärzte, Rheine, Germany; 3Department of Ophthalmology, Oftalvist Alicante, Alicante, Spain
Correspondence: Gerd U Auffarth, International Vision Correction Research Centre (IVCRC), The David J. Apple International Laboratory for Ocular Pathology, Department of Ophthalmology, Ruprecht-Karls-University of Heidelberg, Heidelberg, Germany, Email [email protected]
Purpose: To determine the postoperative visual performance of patients after bilateral implantation of a new trifocal aspheric hydrophobic intraocular lens (IOL) following cataract or refractive lens exchange surgery.
Methods: This was a prospective, multicentric, open-label clinical study. Patients were implanted bilaterally with the AT ELANA 841P IOL targeted for emmetropia. One and 3 months postoperatively, subjective refraction, binocular uncorrected and distance-corrected visual acuities for far (UDVA, CDVA), intermediate (UIVA, DCIVA), and near (UNVA, DCNVA) distances, monocular and binocular defocus curves, binocular photopic and mesopic contrast sensitivity, patient satisfaction in terms of visual disturbance, and spectacle independence were recorded.
Results: A total of 58 patients were evaluated. Three months postoperatively, the average postoperative spherical equivalent was 0.20± 0.39D and 83.3% and 95.8% of eyes were within ± 0.50D and ± 1.00D, respectively. 88.5% of eyes showed refractive cylinder values of ≤ 0.50D, and 97.9% had values of ≤ 1.00D. For distance vision, 98% of patients had CDVA of 0 logMAR or better; for intermediate vision, 90% and 92% of patients had DCIVA of 0.10 logMAR or better at 80 and 66 cm, respectively; and for near vision 65% and 77% of patients presented DCNVA of 0.10 logMAR or better at 40 cm and preferred distance, respectively. The depth-of-focus from 0D was about 3.0D. The contrast sensitivity curves showed standard patterns under photopic and mesopic conditions. Questionnaires revealed that 87.2% of patients were either completely, very, or somewhat satisfied with their vision. A high spectacle independence rate of 85.1% was reported, while for visual symptoms, high percentages (59.6% to 100%) reported having them never or sometimes.
Conclusion: The AT ELANA 841P trifocal aspheric hydrophobic IOL provides excellent accurate refractive outcomes with very good visual performance across multiple distances, resulting in high spectacle independence rate and satisfaction levels with minimal visual symptoms.
Keywords: trifocal, intraocular lens, hydrophobic, aspheric, diffractive
Introduction
The use of trifocal intraocular lenses (IOLs) in cataract or refractive lens exchange surgery has proven to be a good solution for providing patients with a full range of distance to near vision. A recent systematic review and meta-analysis assessed the efficacy and safety of various IOLs, including monofocal, bifocal, trifocal, extended depth-of-focus, and enhanced monofocal IOLs in cataract surgery through 28 randomized controlled trials involving 2465 patients. It was concluded that in cataract patients being treated for presbyopia, trifocal IOLs demonstrated better visual acuity and spectacle independence at near distances.1 The authors pointed out the fact that trifocal IOLs ranked highest in terms of spectacle independence at various distances. This is supported by another study based on a Bayesian network meta-analysis comparing various types of multifocal and monofocal IOLs.2 That analysis included 27 studies involving 2,605 patients and concluded that for patients considering a multifocal IOL due to presbyopia, bilateral implantation of a trifocal IOL might be the optimal option without compromising distance visual acuity.
A new trifocal aspheric hydrophobic IOL has recently been developed: the AT ELANA 841P IOL (Carl Zeiss Meditec AG). This lens has a fully diffractive trifocal design with aberration-neutral optics made from a hydrophobic acrylic material, differing in this way from its predecessor, the hydrophilic AT LISA tri 839MP model. The AT ELANA 841P IOL was tested in vitro using an optical bench to analyze its optical quality and it showed good optical performance across distances, regardless of spectral and spherical aberration conditions.3 Recently, both IOL models were examined and shown to have comparable optical quality and low potential for photic phenomena. Findings suggest that the hydrophobic trifocal IOL may offer a visual range comparable to its hydrophilic counterpart.4 Another laboratory study assessed the effects of misaligning trifocal IOLs and concluded that the AT ELANA 841P IOL exhibited good tolerance to IOL decentration, which may stem from its aberration-neutral design.5 These publications indicated that clinical studies are essential to confirm the laboratory studies and fully analyze the visual performance of this lens once implanted. For that reason, this clinical study is aimed at assessing the accuracy, visual performance, and patient reported outcomes 3 months after the bilateral implantation of the AT ELANA 841P IOL following cataract or refractive lens exchange surgery. Patients will be followed up to 1 year after surgery. This report shows first data addressing the main aim of the study obtained 3 months postoperatively.
Methods
Study Design and Patients
Patients scheduled for cataract or refractive lens exchange surgery with bilateral implantation of the AT ELANA 841P IOL participated in the study. Three study sites in Europe took part in this prospective open-label multicenter clinical study: Heidelberg University Hospital (Heidelberg, Germany), Precise Vision Augenärzte (Rheine, Germany), and Oftalvist Alicante (Alicante, Spain). The study was approved by the ethics committees Ethikkommission Heidelberg (S-414/2023), Ethikkommission–Aerztekammer Westfalen-Lippe and Comité Ético de Investgación Clínica Hospital Clínico San Carlos, and carried out in accordance with the tenets of the Declaration of Helsinki. The study was registered at www.clinicaltrials.gov (registration number: NCT06111222). Patients were consecutively enrolled once they had signed the informed consent form, and their eligibility was confirmed based on the inclusion and exclusion criteria. The inclusion criteria were: age ≥18 years; phacoemulsification cataract extraction or Femtosecond-Laser-Assisted-Cataract-Surgery (cataract grades 1, 2, or 3 on the LOCSIII scale); AT ELANA 841P IOL implantation with a maximum of 28 days between the two implantations; calculated IOL power within the IOL diopter (D) range of +15.0D to +27.0D; no visual-acuity-limiting pathologies other than cataract; corneal astigmatism <1.0D; availability; willingness; sufficient cognitive awareness to comply with examination procedures; and written informed consent for participation in the study and data protection. The exclusion criteria were: corneal astigmatism ≥1.0D; difficulties in terms of cooperation (distance from their home, general health conditions); history of acute or chronic disease; pathology, illness, or ocular trauma that would, in the surgeon’s opinion, confound the results (eg, corneal pathology, ocular hypertension, suspicion of glaucoma, glaucoma, macular degeneration, cystoid macular edema, proliferative diabetic retinopathy, or amblyopia); visual field loss affecting visual acuity; use of systemic or ocular medication that might affect vision; patients with amblyopia, strabismus, forme fruste keratoconus or keratoconus; pupil abnormalities (non-reactive, tonic pupils, abnormal myosis or mydriasis, abnormally shaped pupils or pupils that do not dilate under mesopic/scotopic conditions); capsular or zonular abnormalities that may affect the postoperative centration or tilt of the lens (eg, pseudoexfoliation syndrome); cataract grades of 4, 5 or 6 on the LOCSIII scale; surgeries with an incision size of ≥2.75mm; immediate sequential bilateral cataract surgery; concurrent participation in another device investigation; and use of contact lenses during participation.
Intraocular Lens
All patients were implanted with the new trifocal aspheric hydrophobic AT ELANA 841P IOL (Figure 1). This is a fully trifocal (+3.33D near addition and +1.66D intermediate addition at the IOL plane), aspheric (aberration neutral), one-piece IOL made of hydrophobic acrylic material (with a heparin-coated surface). The AT ELANA 841P IOL allocates 47.5% light distribution to far focus, 17.5% to intermediate focus, and the remaining 35% to near focus. It has a 6.0 mm optical diameter and a 13.0 mm total diameter. The lens features a modified C-loop haptic and is implanted using a fully preloaded single-use BLUESERT injector with an incision size of 2.2–2.6 mm. The diopter range varies from 0D to +34.00D in 0.50D increments. The Abbe number is 51 and the refractive index is 1.49.
 |
Figure 1 AT ELANA 841P intraocular lens (courtesy of Carl Zeiss Meditec, Inc). |
Pre- and Postoperative Assessment
Biometric measurements of all patients, including axial length, keratometry, anterior chamber depth, central corneal thickness, white-to-white, and lens thickness, were taken prior to the surgery using the IOLMaster 700 SS-OCT biometer (Carl Zeiss Meditec AG, Jena). The Barret true K-TK formula was used to calculate the IOL power. Postoperative examinations were conducted at 1 and 3 months after implantation.
Monocular and binocular corrected distance visual acuity (CDVA), binocular uncorrected distance visual acuity (UDVA), logMAR binocular uncorrected distance intermediate visual acuity (UIVA) at 66 and 80 cm, logMAR binocular uncorrected distance near visual acuity (UNVA) at 40 cm and preferred distance were measured in logMAR under photopic conditions. The monocular and binocular photopic defocus curves were assessed for each patient using standard charts from +2.00D to −4.50D in 0.50D steps. The FACT chart (Optec 5000) was used to determine the binocular contrast sensitivity, both with and without glare, under photopic conditions (85–100 cd/m2) and under mesopic conditions (2.5–3.2 cd/m2). The patients were asked to complete two questionnaires.6,7 One regarding spectacle use for near, intermediate and distance vision, and another assessed visual symptoms and patient satisfaction both before and after surgery.
Statistical Analysis and Sample Size Calculation
Continuous measurements were summarized using the mean, standard deviation, median, minimum, and maximum values. Categorical and incidence measurements were summarized by both count and percentage. A sample size calculation was performed for the primary endpoint: demonstrating that the mean monocular postoperative CDVA was 0.04 logMAR or better. The calculation used the following parameters: continuous endpoint, one sample test; alpha α: 0.05; power (1-β): 0.90, 2-sided test, expected outcome: 0.0 logMAR, and the outcomes of a previous study8 (32 patients) with monocular CDVA of 0.04±0.06 logMAR. This calculation led to a required sample size of 26 patients to investigate whether the mean monocular CDVA of the study eye was 0.04 logMAR or better post-surgery. To account for a potential dropout rate of up to 10% during the study, at least 29 patients had to be enrolled. Some parameters (eg contrast sensitivity) could not be obtained in all patients. This would not lead to exclusion but only render the available number of eyes or patients for the analysis of respective parameters.
Results
Out of the patients enrolled in the study, 58 consecutive patients who underwent cataract extraction and bilateral implantation with the AT ELANA 841P IOL had sufficient monitored and confirmed postoperative data to be included in the interim analysis. Mean age of these patients was 64.8±8.1 years (ranging from 45 to 88 years); 38 were female (65.5%). The descriptive preoperative demographic characteristics of the sample are displayed in Table 1. Standardized graphs depicting refractive and visual acuity outcomes at the 1- and 3- month follow-ups were constructed in line with established reporting guidelines.9
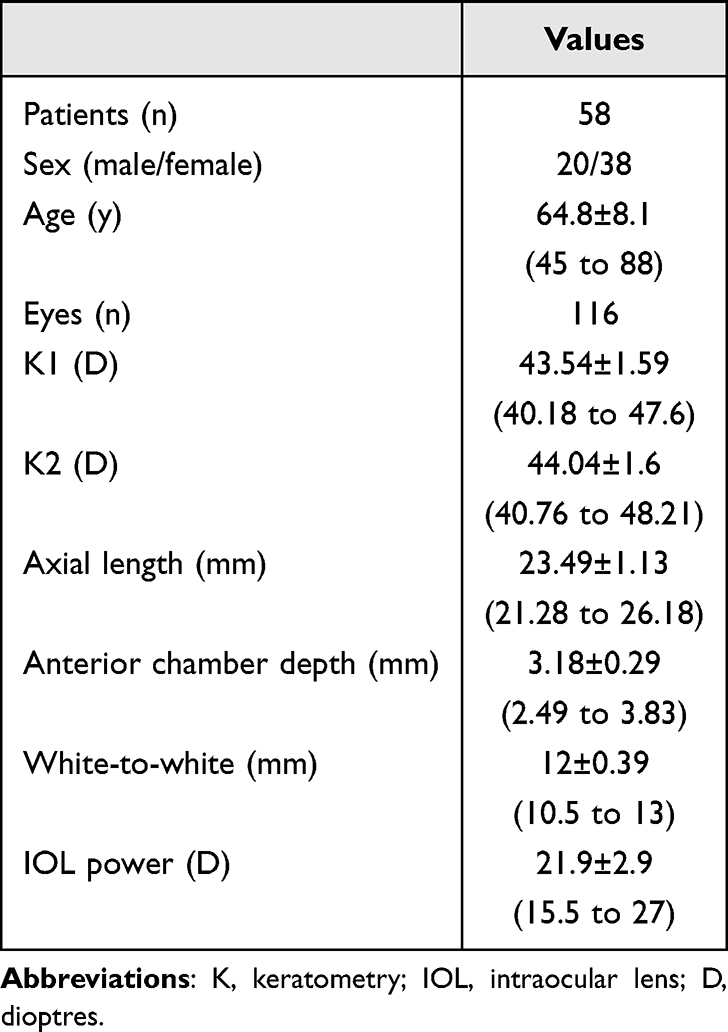 |
Table 1 Demographics and Characteristics of the Eyes Included in This Study, Shown as Means, Standard Deviations (SDs), and Ranges |
To assess the predictability of the procedure, Figure 2A displays a histogram of the postoperative spherical equivalent refraction distribution relative to the intended target, while Figure 2B presents the postoperative refractive cylinder.
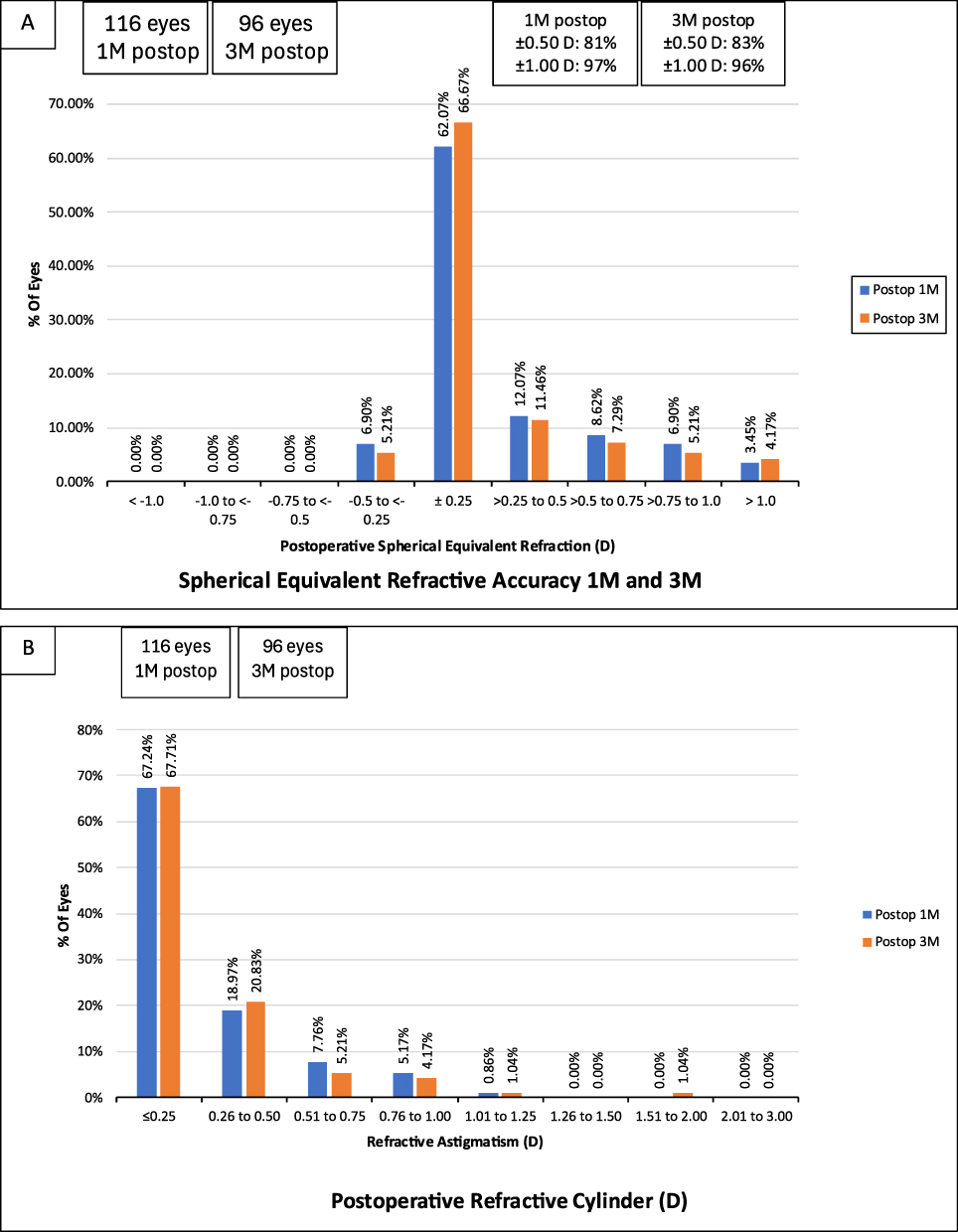 |
Figure 2 Distribution of postoperative spherical equivalent (A) and refractive cylinder (B) at 3 months following AT ELANA 841P IOL implantation. Values indicate the percentage of eyes within each range. Mean and standard deviation are provided for each parameter. |
At the 3-month postoperative visit, the largest proportion of eyes (66.7%) had a spherical equivalent within ±0.25D, followed by 11.46% within the >0.25 to 0.50D range, highlighting the high refractive accuracy. The vast majority of patients achieved results close to the planned refraction, with 95.8% of eyes within ±1.00D and 83.3% within ±0.50D of the target refraction. The mean postoperative spherical equivalent was 0.20 ± 0.39D (range: −0.50D to 1.50D), indicating a high level of refractive accuracy. For astigmatism, 97.9% of eyes had a postoperative refractive cylinder of ≤1.00D, and 88.5% had ≤0.50D. The mean postoperative refractive cylinder was −0.28 ± 0.33D (range: 0 to −1.75D).
With regard to the visual acuity outcomes, Figure 3 shows the cumulative postoperative binocular UDVA and CDVA (A), UIVA and DCIVA at 80 cm (B) and 66 cm (C), UNVA and DCNVA at 40 cm (D), and preferred distance (E), respectively. Specifically, 97.9% of patients presented a UDVA of 0.10 logMAR or better compared to 100.0% for CDVA; at 66 cm, 91.7% of patients had a UIVA and DCVIA of 0.10 logMAR or better (87.5% for UIVA and 89.6% for DCIVA at 80 cm); and 52.1% of patients showed a UNVA at 40 cm of 0.10 logMAR or better compared to 64.6% for DCNVA. For the preferred distance, these values improved to 58.3% for UNVA and 77.1% for DCNVA. Table 2 presents detailed measurements of visual acuity at different distances.
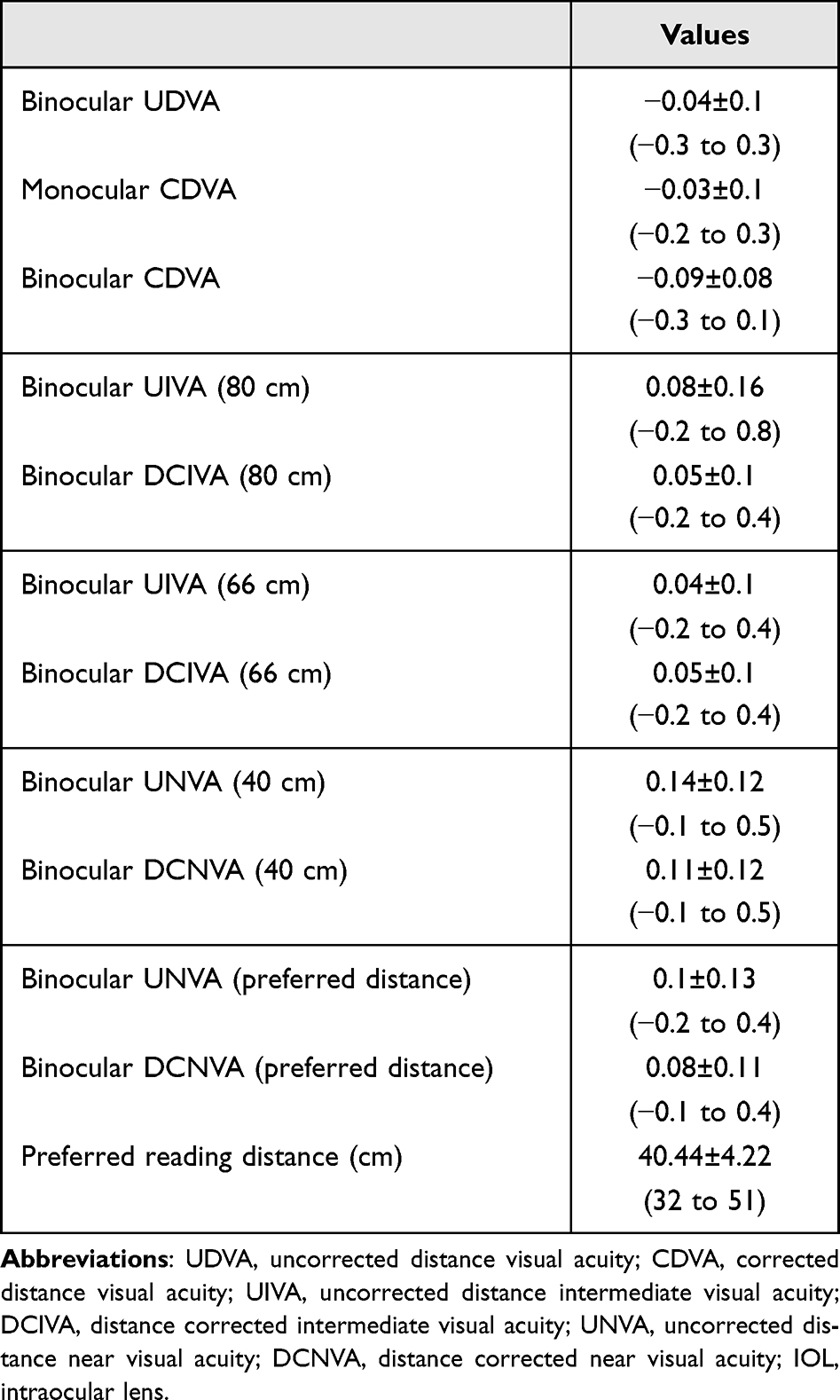 |
Table 2 Logarithmic Visual Acuity Outcomes of the Minimum Angle of Resolution (logMAR) of Eyes Implanted with the AT ELANA 841P Hydrophobic Intraocular Lens Shown as Means, Standard Deviations (SDs), and Ranges at a 3 Month Follow-up Visit |
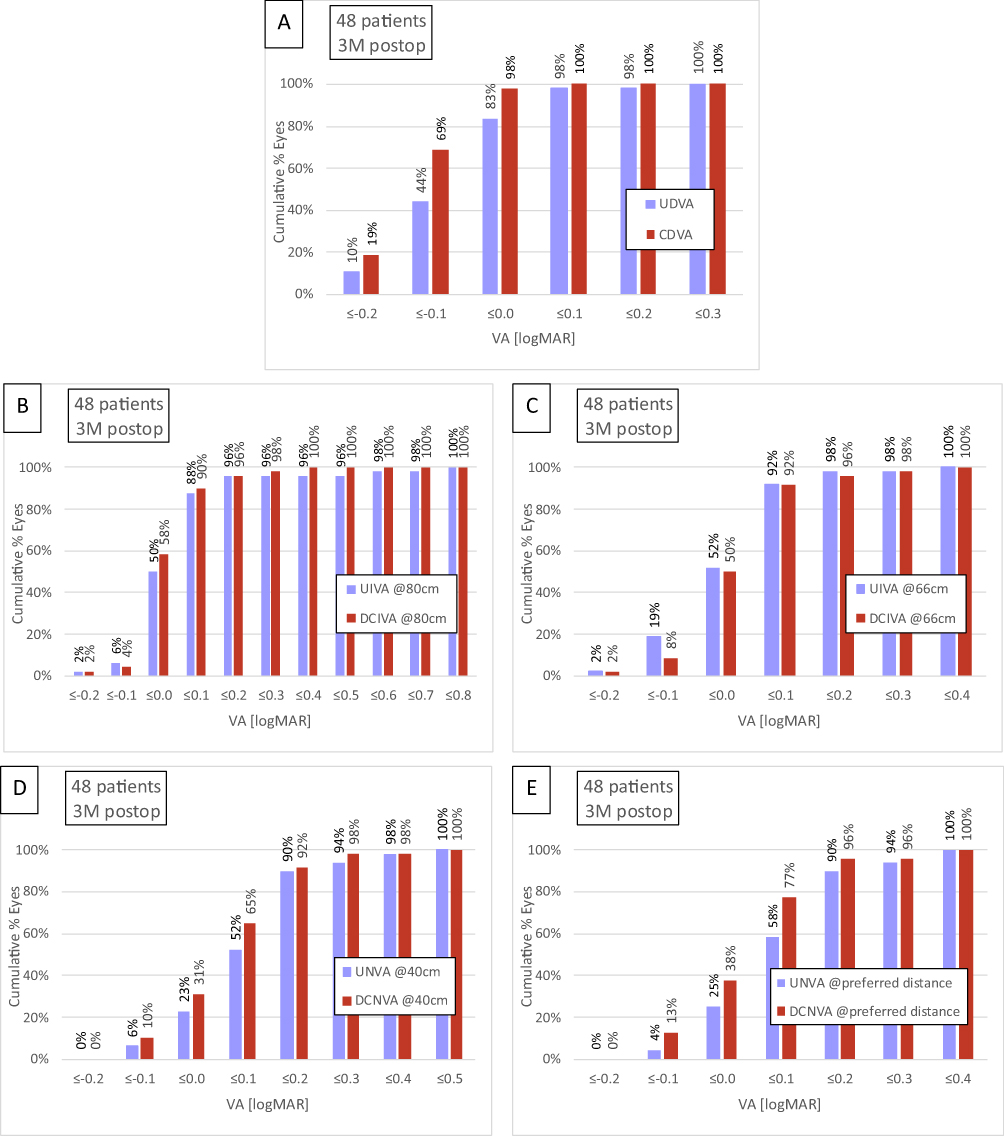 |
Figure 3 Cumulative proportion of patients 3 months after AT ELANA 841P intraocular lens implantation with a given postoperative binocular uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) (A); binocular uncorrected distance intermediate visual acuity (UIVA) and distance corrected intermediate visual acuity (DCIVA) at 80 cm (B) and 66 cm (C); and binocular uncorrected near visual acuity (UNVA) and distance corrected near visual acuity (DCNVA) at 40 cm (D) and preferred distance (E). |
The mean photopic monocular and binocular defocus curves with best correction for distance are detailed in Figure 4. This figure shows that visual acuity remained relatively stable across a wide range of vergences (defocus), with a peak at far distance vision (0D) followed by a smooth and extended depth-of-focus as defocus increased. The results show that binocular vision maintained slightly better performance than monocular vision at all vergences. The depth-of-focus was defined as the lens power range that achieved a mean binocular visual acuity of ≥20/32 (0.2 logMAR) from 0 D. In our study, this depth of focus was approximately 3.0 D indicating that this lens provides functional near and intermediate vision while maintaining excellent distance vision (−0.08±0.08 logMAR at 0D).
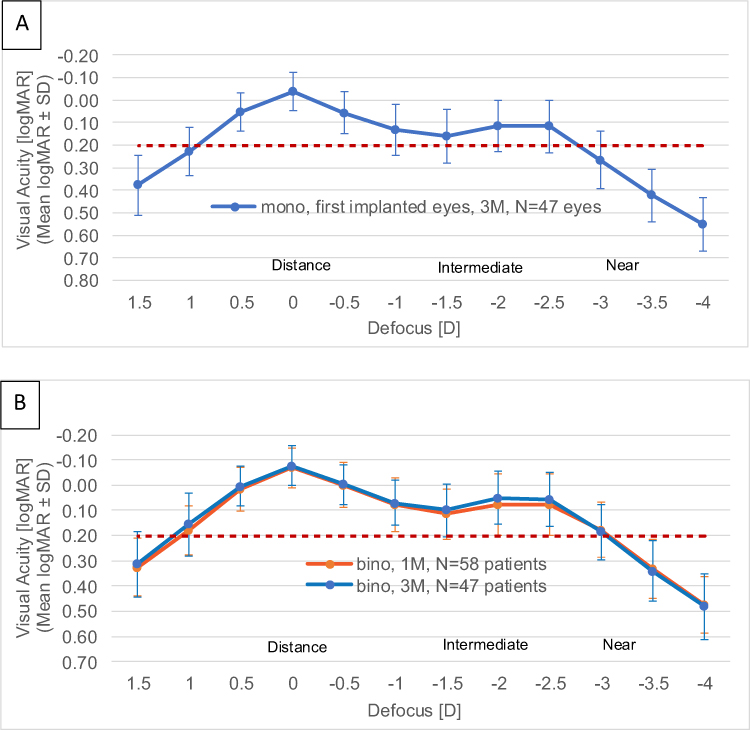 |
Figure 4 Mean photopic monocular (A) and binocular (B) logMAR visual acuity (with best correction for distance) as a function of defocus from +1.50 to −4.50 dioptres (D) at 3 months postoperatively for the AT ELANA 841P IOL. Error bars represent standard deviation. Binocular visual acuity remained superior across all vergences, with a peak at 0D and an extended depth-of-focus reaching approximately 3.0D. |
Figure 5 shows the mean binocular contrast sensitivity for different spatial frequencies measured under photopic and mesopic conditions (both with and without glare). The patients were asked to fill out two questionnaires on their visual symptoms and satisfaction prior to their surgery as well as at 1 and 3 months post-surgery. Figures 6–8 show the distribution of the answers in percentages for the different questions; their satisfaction with their current vision, patient-reported limitations in terms of certain daily activities, and the prevalence of some visual symptoms are summarized.
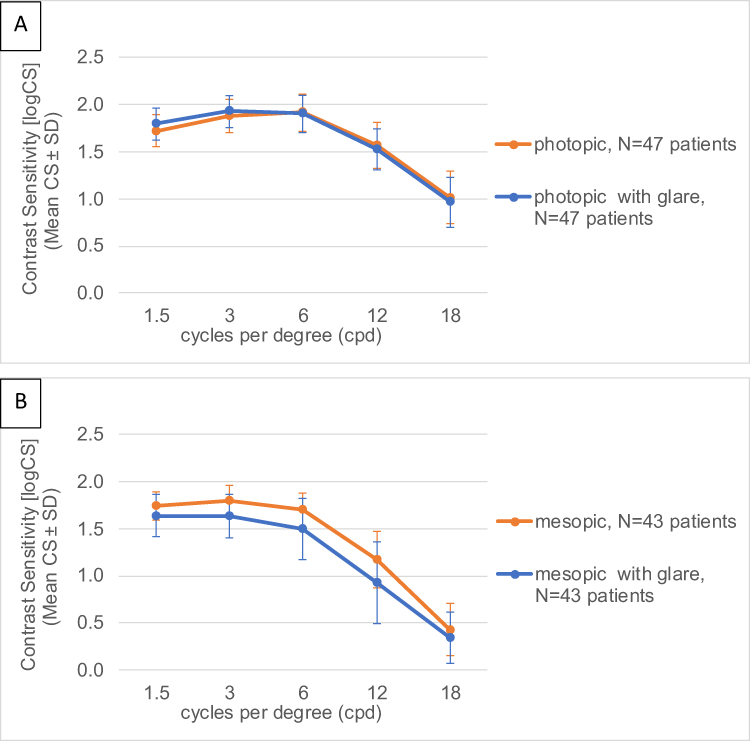 |
Figure 5 Binocular contrast sensitivity measured under photopic (A) and mesopic (B) lighting conditions with and without glare, three months after implantation of the AT ELANA 841P IOL. Measurements were taken across a range of spatial frequencies (cycles per degree) using the FACT chart. Error bars represent standard deviation. |
 |
Figure 6 Patient-reported satisfaction with vision and spectacle Independence before and 1 and 3 months after bilateral implantation of the AT ELANA 841P IOL. Results reflect responses to questions regarding satisfaction and need for spectacle use. Responses are presented as a percentage of total participants. |
 |
Figure 7 Visual symptom questionnaire outcomes before and 1 and 3 months after AT ELANA 841P intraocular lens implantation. |
 |
Figure 8 Patient-reported bothersome of non-photic visual disturbances eg, hazy vision, glare, starburst, floaters at pre op, one month, and three months after bilateral AT ELANA 841P IOL implantation. Responses reflect degree of bother reported. |
Discussion
The main objective of this study was to assess the visual performance of the new AT ELANA 841P IOL following cataract or refractive lens exchange surgery. In addition, postoperative refraction and patient-reported outcome questionnaires were also collated. The findings obtained in our study demonstrate that this IOL provides very good visual performance across multiple distances as well as excellent refractive accuracy. In addition, patient-reported outcomes reveal a high spectacle independence rate and high levels of satisfaction with minimal visual symptoms.
In terms of refraction, the accuracy in our cohort demonstrated excellent outcomes, with a mean spherical equivalent of less than a quarter of a diopter (0.20±0.39 D) and almost all the eyes (95.8%) were within ±1.00 D (Figure 2A). Cylinder values were also well controlled, with 88.5% of eyes ≤0.50 D and 97.9% ≤1.00 D (Figure 2B), and a low mean refractive cylinder of −0.28±0.33 D. Recently, Janeková et al10 has also reported the clinical outcomes of this lens in a sample of 126 patients with 4–6 months of follow-up. They found that most of the eyes (84.9%) were within ±0.50D of spherical equivalent refraction and almost all eyes (98.9%) within ±1.0D, with a mean spherical equivalent value of −0.11±0.37D. These results align with findings from previous clinical trials on other trifocal diffractive hydrophobic IOLs. For example, a recent review of the FineVision HP IOL reported mean postoperative spherical equivalents were close to emmetropia and never greater than a quarter of a diopter, with almost all the eyes from the different studies within 1.00 D of spherical equivalent (note that the studies involved different follow-up periods, from 1 month to 2 years).11 Other IOL models have also been thoroughly analyzed, and a systematic review and meta-analysis reporting data for trifocal and enhanced depth-of-focus IOLs has considered published results on the FineVision, AcrySof IQ PanOptix, and AT LISA tri IOLs. These results show that the mean postoperative spherical equivalent values ranged from −0.39 to 0.25 D.12
In relation to the visual acuity outcomes obtained in our sample, the postoperative far, intermediate, and near vision were very good. Table 2 presents both the binocular uncorrected and corrected mean values (and ranges) for all distances (far, 80 cm, 66 cm, 40 cm, and preferred distance). Note that both binocular UDVA and CDVA were better than 0.0 logMAR (at 3-month binocular mean CDVA and UDVA were −0.09±0.08 and −0.04±0.10 logMAR, respectively). Janeková et al10 found mean monocular CDVA of −0.06±0.08 logMAR and UDVA of −0.01±0.10 logMAR. They also found mean monocular UIVA, UNVA, DCIVA and DCNVA of 0.1 logMAR or better at intermediate (80 cm) and near (40 cm) distances. When compared with published studies, our results broadly align with those found for comparative IOL models. In particular, in the systematic review and meta-analysis,12 several trifocal IOLs showed mean monocular UDVA values ranging from −0.12 to 0.11 logMAR and mean monocular CDVA values ranging from −0.2 to 0.06 logMAR. For the FineVision HP IOL, the monocular UDVA values ranged from 0 to −0.06 logMAR and monocular CDVA values ranged from 0.01 to −0.11 logMAR.11 Our mean monocular CDVA was −0.03 logMAR. The mean outcomes obtained for other distances in our study were also very good, being 0.05 logMAR for binocular DCIVA (80 and 66 cm) and 0.11 logMAR (20/25) for DCNVA (40 cm). Monocular DCIVA values for the FineVision HP IOL ranged from 0.02 to 0.19 logMAR at 80 cm, and from 0.18 to 0.19 logMAR at 66 cm, and DCNVA from 0.02 to 0.20 logMAR at 40 cm.11 The mean values obtained in our cohort are correlated with the cumulative visual acuity depicted in Figure 3 for the different distances. Note, for example, that all patients presented a cumulative CDVA of 0.1 logMAR or better (≥20/25), a DCIVA of 0.4 logMAR or better (≥20/50) both for 80 and 66 cm, and a DCNVA of 0.5 logMAR or better (≥20/63). Specifically, for distance vision, 98% of patients presented a CDVA of 0 logMAR or better (≥20/20); for intermediate vision, 90% and 92% of patients had a DCIVA of 0.1 logMAR or better (≥20/25) at 80 and 66 cm, respectively; and for near vision 65% and 77% of patients presented a DCNVA of 0.1 logMAR or better (≥20/25) at 40 cm and preferred distance, respectively. Janeková et al10 found 97.2%, 59.1% and 59.1% of eyes achieving CDVA, DCIVA, and DCNVA of 0.1 logMAR or better, respectively. UNVA, UIVA and UNVA of 0.1 logMAR or better was achieved in 88.9%, 57.1% and 44.4% of the eyes, respectively. It should be kept in mind that the optical design of the AT ELANA 841P IOL provides focal planes at 80cm and 40 cm, providing patients with a continuous range of vision from far to near distance, thereby reducing spectacle dependence. This is supported by a laboratory study by Łabuz et al,4 which found that the optimal intermediate point for the AT ELANA was at approximately 80 cm and 40 cm for reading. This continuous range of vision is reflected in Figure 5 (defocus curves): from the peak of best vision located at far distance (0D of defocus), there is a smooth transition in vision with increasing vergence (negative X-axis defocus values), reaching another peak at near vision (about −2.5D of defocus, corresponding to 40 cm). Better outcomes are expected under binocular conditions and with a longer follow-up period, as shown in the bottom graph. The depth-of-focus from 0D in our sample under binocular conditions was about 3D, providing our patients with a good continuous range of vision from distance to near. This fully agrees with Janeková et al10 who at 3-months postoperatively reported a continuous range of 0.1 logMAR or better vision from distance to near. They indicated that the depth-of-focus from 0.0D with visual acuity of 0.2 logMAR or better spanned over 3.0 D.
Contrast sensitivity measurements also provide insights into the spatial vision limits across a range of object scales. When measured under different lighting conditions, both with and without glare, these measurements reflect the visual performance of our patients in various circumstances. Due to the multifocal design of the diffractive IOL, both in-focus and out-of-focus images can lead to a reduced-contrast retinal image, resulting in lower contrast sensitivity.13 Our results revealed good contrast sensitivity outcomes across different spatial frequencies (Figure 5). For comparison, binocular photopic contrast sensitivity values reported in patients implanted with monofocal IOLs were 1.55, 1.76 and 1.49 for 3, 6 and 12 cycles/degree, respectively,13 which are similar to those found in our cohort (Figure 5A). This is in line with a meta-analysis of 21 randomized controlled trials involving 2,951 patients,14 which reported lower contrast sensitivity in multifocal IOL patients. However, the difference between these patients and those implanted with monofocal IOLs was only 0.06 units, indicating that the contrast sensitivity disadvantage of multifocal IOLs is minimal. Additionally, it has been shown that the typical neuroadaptation process after multifocal IOL implantation takes at least 3 months to significantly reduce photic phenomena,15 with the greatest improvement likely occurring 1-year later.16 For this reason, we should expect to further improve outcomes with longer follow-up periods than those depicted in Figure 5. In mesopic conditions (Figure 5B), a reduction in contrast sensitivity is observed, particularly at higher spatial frequencies. This finding is consistent with van Ness et al17 study on the effect of luminance level on contrast sensitivity and is also attributed to the splitting of light reaching the retina in multifocal IOLs under low-mesopic environments.15 Janeková et al10 found that contrast sensitivity was in the normal range of a phakic population (40–49 years) at all spatial frequencies in all light conditions they tested (photopic with glare and mesopic with and without glare). They indicated that patients implanted with this IOL model were able to restore contrast sensitivity to the same level as the phakic middle-aged population exposed to daylight conditions.
Patient-reported outcome questionnaires provide valuable data for analyzing the outcomes of patients undergoing any surgical procedure. These questionnaires give surgeons more insight, allowing them to detect patients who may be dissatisfied even when other clinical findings, such as refraction and visual acuity, are satisfactory. The outcomes shown graphically in Figures 6–8 cover several questions related to satisfaction, spectacle or contact use, and potential visual symptoms reported by our patients via the extensive AIOLIS questionnaire. It can be seen that there is a high level of satisfaction and low spectacle dependence (Figure 6). This is supported by 87.2% of patients being either completely, very, or somewhat satisfied with their current vision; and 85.1% spectacle independence rate. Additionally, 19.1% of patients reported needing spectacles a little of the time over the past 7 days, while 66.0% reported not needing them at all. These outcomes are consistent with previous literature on other trifocal IOLs. For example, a comparison of different trifocal IOLs (FineVision HP, AT LISA tri 839MP and AcrySof IQ PanOptix) using the NEI VFQ-25 questionnaire revealed no statistically significant differences between the three lenses. Regardless of the IOL implanted, patient satisfaction was high.18 Similarly, Akahoshi,19 using the Catquest-9SF questionnaire for patients implanted with the FineVision HP IOL, found that 90.57% of patients reported no sight difficulties in their daily lives, and all were “very or quite satisfied” with their vision. Akahoshi also used the PRSIQ questionnaire and found that 98.11 and 98.11% of patients did not need glasses or contacts for far, intermediate and near vision, respectively. Other authors looking at the same IOL model found that between 82.3% to 100% of patients were either very satisfied or satisfied.20–22 Figures 7 and 8 show the frequency distribution of various visual symptoms, such as snowballs, halos, starburst, glare, distortion, hazy vision, and floaters. We found that high percentages of patients reported a frequency of never or sometimes for these symptoms, ranging from 59.6% to 100.0%. From all symptoms, halos had the lowest percentage (59.6%), with 10.6% and 29.8% of patients reporting usually and always, respectively, for this symptom. It has been suggested that trifocal lenses may reduce visual quality due to photic phenomena (ie glare, halo, and starburst), which impact postoperative patient satisfaction.23 The halo effect in trifocal lenses mainly arises from the combined influence of blurred images associated with the intermediate and near addition powers of the lens.24 Our values are reported for a short-term post-IOL implantation period (3 months), and it should be noted that some symptoms may decrease over time due to neuroadaptation. In this sense, a progressive decline in halos has been documented, decreasing from 80% 1 month after implantation with the AT LISA tri IOL to 40% after 6 months.25 This is also expected for our cohort, given the tendency to reduce halo perception from 1 to 3 months post-surgery (from 43.1% to 40.4% combining the answers of usually and always) as shown in Figure 7. We expect an even greater reduction of this symptom with time, and when it does occur, it should not cause significant issues for the patient as demonstrated in our study. After 3 months, only 6.4% reported that halos were quite bothersome, and 4.3% reported them as extremely bothersome. Our results suggest that this IOL model is reliable in terms of visual symptoms, as fewer optical phenomena are reported. The study is still ongoing, and we hope in the near future to show longer follow-ups in order to study possible changes in visual symptoms.
We should consider the following study limitations: first, the follow-up period in our sample was only 3 months; second, we did not include other groups of patients implanted with different trifocal or monofocal IOLs for comparative purposes; and third, we did not assess the decentration and/or tilt of the IOLs and their effect of the outcomes. In this regard, we are currently collecting data for a longer follow-up period, and comparisons have been made with outcomes published by other authors, primarily based on the trifocal IOL models discussed above. Finally, it should be noted that the AT ELANA features an aberration-neutral optic and laboratory studies have shown that this type of design is less sensitive to decentration compared to lenses with high spherical aberration correction.26,27 A laboratory study by Yan et al5 concluded that the aberration-neutral design of the AT ELANA 841P IOL appears more forgiving when optimal centration cannot be guaranteed. Although our study does not assess the impact of decentration on visual outcomes, clinical outcomes observed in our sample correlate well with the in vitro analysis of the misalignment effect, demonstrating the robustness of this IOL when implanted.
Conclusion
In conclusion, patients undergoing phacoemulsification for cataract or refractive lens exchange surgery who are implanted with the AT ELANA 841P IOL demonstrate good visual performance at various distances with accurate refractive outcomes. These patients report minimal visual symptoms and a high level of satisfaction post-surgery, making this lens a valuable option for those seeking spectacle independence with very good visual outcomes. Future studies should consider longer follow-up periods to confirm these outcomes over time, especially in eyes with corneal astigmatism.
Data Sharing Statement
The datasets created and analyzed during the current study available from the corresponding author on reasonable request [G.U.A.].
Disclosure
This study was sponsored and funded by Carl Zeiss Meditec, Inc., USA. Carl Zeiss Meditec, Inc. was involved in the design and conduct of the study. targomed GmbH performed the statistical analyses. FK and GA are consultants for Carl Zeiss Meditec AG. GA reports grants, personal fees from Carl Zeiss Meditec, during the conduct of the study, lecture feesfrom Afidera, Eyebright; grants, personal fees from Alcon, AMO/Johnson&Johnson, Cristalens, Elios, EyeYon, Hanita, Hoya, Kowa, Oculus, Rayner, Teleon; grants from Contamac, Eyedeal, Presbia, 1stQ, EyeD, outside the submitted work. PTR reports grants from AST Products, Alcon Labs, Hoya Surgical, Vialase, Johnson and Johnson, Humanoptics AG, outside the submitted work. The authors report no other conflicts of interest in this work.
Medical writing was provided by targomed GmbH, which was funded by Carl Zeiss Meditec, Inc., in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
References
1. Li J, Sun B, Zhang Y, et al. Comparative efficacy and safety of all kinds of intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2024;24(1):172. doi:10.1186/s12886-024-03446-1
2. Cho JY, Won YK, Park J, et al. Visual outcomes and optical quality of accommodative, multifocal, extended depth-of-focus, and monofocal intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and Bayesian network meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–15. doi:10.1001/jamaophthalmol.2022.3667
3. Łabuz G, Yan W, Khoramnia R, Auffarth GU. Optical-quality analysis and defocus-curve simulations of a novel hydrophobic trifocal intraocular lens. Clin Ophthalmol. 2023;17:3915–3923. doi:10.2147/OPTH.S445461
4. Łabuz G, Yan W, Khoramnia R, Auffarth GU. Comparing optical quality and simulated defocus curves: head-to-head analysis of hydrophilic and hydrophobic trifocal intraocular lenses. J Cataract Refract Surg. 2025;51(2):161–166. doi:10.1097/j.jcrs.0000000000001577
5. Yan W, Auffarth GU, Khoramnia R, Łabuz G. A comparative analysis of the effects of misaligning different trifocal intraocular lenses. J Clin Med. 2024;14(1):187. doi:10.3390/jcm14010187
6. Hays RD, MacRae S, Holladay J, et al. Development of a patient-reported outcome measure to assess symptoms associated with cataract surgery and intraocular lens implants. Ophthalmology. 2023;130(7):715–725. doi:10.1016/j.ophtha.2023.02.026
7. Masket S, Lum F, MacRae S, et al. Symptoms and satisfaction levels associated with intraocular lens implants in the monofocal and premium IOL patient-reported outcome measure study. Ophthalmology. 2023;130(7):726–734. doi:10.1016/j.ophtha.2023.02.027
8. Nováček LV, Němcová M, Tyx K, et al. Comparison of clinical outcomes, visual quality and visual function of two presbyopia-correcting intraocular lenses made from the same material, but with different design and optics. J Clin Med. 2021;10(15):3268. doi:10.3390/jcm10153268
9. Reinstein DZ, Archer TJ, Srinivasan S, et al. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J Refract Surg. 2017;33(4):218–222. doi:10.3928/1081597X-20170302-01
10. Janeková A, Mojžiš P, Němcová I, Kačerík M, Veselý P, Hrčková L. Visual outcomes of a new hydrophobic trifocal intraocular lens in cataract treatment: a prospective clinical study. J Ophthalmol. 2025;2025:2662730. doi:10.1155/joph/2662730
11. Ristvedt D, Bosc C, Thompson V. Clinical outcomes of a hydrophobic trifocal diffractive intraocular lens: a literature review. Front Med. 2025;12:1533161. doi:10.3389/fmed.2025.1533161
12. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
13. Gil MA, Varón C, Cardona G, Vega F, Buil JA. Comparison of far and near contrast sensitivity in patients symmetrically implanted with multifocal and monofocal IOLs. Eur J Ophthalmol. 2014;24:44–52. doi:10.5301/ejo.5000335
14. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and metaanalysis based on randomized controlled trials. Surv Ophthalmol. 2019;64:647–658. doi:10.1016/j.survophthal.2019.02.012
15. Alio JL, Plaza-Puche AB, Férnandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62:611–634. doi:10.1016/j.survophthal.2017.03.005
16. Kaymak H, Fahle M, Ott G, Mester U. Intraindividual comparison of the effect of training on visual performance with ReSTOR and Tecnis diffractive multifocal IOLs. J Refract Surg. 2008;24:287–293. doi:10.3928/1081597X-20080301-11
17. van Nes FL, Koenderink JJ, Nas H, Bouman MA. Spatio temporal modulation transfer in the human eye. J Opt Soc Am. 1967;57:1082–1088. doi:10.1364/JOSA.57.001082
18. Martínez de Carneros-Llorente A, Martínez de Carneros A, Martínez de Carneros-Llorente P, Jiménez-Alfaro I. Comparison of visual quality and subjective outcomes among 3 trifocal intraocular lenses and 1 bifocal intraocular lens. J Cataract Refract Surg. 2019;45:587–594. doi:10.1016/j.jcrs.2018.12.005
19. Akahoshi T. Three patient-reported outcomes questionnaires in Japanese patients undergoing cataract surgery with trifocal IOL implantation. Clin Ophthalmol. 2024;18:2521–2529. doi:10.2147/OPTH.S478292
20. Ang RET. Long term clinical outcomes of hydrophilic and hydrophobic versions of a trifocal IOL with the same optical design. Clin Ophthalmol. 2023;17:623–632. doi:10.2147/OPTH.S403351
21. Khoramnia R, Kretz FTA, Gerl M, Breyer D, Auffarth GU. Long-term clinical outcomes after bilateral implantation of two trifocal diffractive IOLs. J Refract Surg. 2023;39:798–807. doi:10.3928/1081597X-20231006-01
22. Nagy ZZ, Dorman P, Szalczer S, Kiss H. Prospective comparison of clinical outcomes after bilateral implantation of diffractive trifocal extended-depth-of-focus and diffractive trifocal hydrophobic intraocular lenses. J Refract Surg. 2025;41:102–113. doi:10.3928/1081597X-20241113-01
23. Alba-Bueno F, Garzon N, Vega F, Poyales F, Millan MS. Patient-perceived and laboratory-measured halos associated with diffractive bifocal and trifocal intraocular lenses. Curr Eye Res. 2018;43(1):35–42. doi:10.1080/02713683.2017.1379541
24. Łabuz G, van den Berg TJTP, Auffarth GU, Khoramnia R. Light scattering from a diffractive-refractive intraocular lens: a goniometer-based approach for individual zone assessment. Biomed Opt Express. 2022;13(12):6724–6732. doi:10.1364/BOE.474778
25. Law EM, Aggarwal RK, Kasaby H. Clinical outcomes with a new trifocal intraocular lens. Eur J Ophthalmol. 2013;24(4):501–508. doi:10.5301/ejo.5000407
26. Eppig T, Scholz K, Löffler A, Meßner A, Langenbucher A. Effect of decentration and tilt on the image quality of aspheric intraocular lens designs in a model eye. J Cataract Refract Surg. 2009;35(6):1091–1100. doi:10.1016/j.jcrs.2009.01.034
27. Fujikado T, Saika M. Evaluation of actual retinal images produced by misaligned aspheric intraocular lenses in a model eye. Clin Ophthalmol. 2014;8:2415–2423. doi:10.2147/OPTH.S72053
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long Term Clinical Outcomes of Hydrophilic and Hydrophobic Versions of a Trifocal IOL with the Same Optical Design
Ang RET
Clinical Ophthalmology 2023, 17:623-632
Published Date: 21 February 2023
Clinical Performance of a New Trifocal IOL with a 7.0 mm Optical Zone
Pastor-Pascual F, Orts-Vila P, Tañá-Sanz P, Tañá-Sanz S, Tañá-Rivero P
Clinical Ophthalmology 2023, 17:3397-3407
Published Date: 7 November 2023
Clinical Outcomes of a Bi-Aspheric Trifocal Diffractive Intraocular Lens
Tañá-Sanz S, Tañá-Sanz P, Rodríguez-Carrillo MD, Ruiz-Santos M, Álvarez de Toledo C, Tañá-Rivero P
Clinical Ophthalmology 2024, 18:27-40
Published Date: 4 January 2024
Visual Performance Correlation with Corneal Aberrometric Profile and Pupil Size After Implantation of a Trifocal Hydrophobic IOL
Bosc C, Le Maléfan E, Boury P, Bernier M, Barrucand A
Clinical Ophthalmology 2024, 18:4053-4061
Published Date: 31 December 2024
Six-Month Visual and Patient-Reported Outcomes of a Biaspheric Trifocal IOL in Asian and European Cataract Patients: A Comparative Study
Hwang YS, Tañá-Rivero P, Tañá-Sanz S, Lee JS, Tañá-Sanz P, Cerviño A
Clinical Ophthalmology 2025, 19:4481-4491
Published Date: 8 December 2025