")
Back to Journals » Clinical Ophthalmology » Volume 17
Long Term Clinical Outcomes of Hydrophilic and Hydrophobic Versions of a Trifocal IOL with the Same Optical Design
Authors Ang RET
Received 16 January 2023
Accepted for publication 10 February 2023
Published 21 February 2023 Volume 2023:17 Pages 623—632
DOI https://doi.org/10.2147/OPTH.S403351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Robert Edward T Ang
Cataract and Refractive Surgery Department, Asian Eye Institute, Makati City, Philippines
Correspondence: Robert Edward T Ang, Asian Eye Institute, 8th Floor PHINMA Plaza, Rockwell Center, Makati City, Philippines, Email [email protected]
Purpose: To show the visual and refractive outcomes in Asian eyes with cataract when bilaterally implanted with either a hydrophobic FineVision POD F GF or a hydrophilic FineVision POD F intraocular lens (IOL).
Methods: Forty-six patients were randomized to receive POD F GF or POD F IOLs. Visual and refractive outcomes were assessed up to 24 months post-surgery. Measurements included uncorrected-distance visual acuity, corrected-distance visual acuity (CDVA), distance-corrected intermediate visual acuity (DCIVA), distance-corrected near visual acuity (DCNVA), refraction, defocus curve, photopic and mesopic contrast sensitivity, and patient-reported outcomes.
Results: Mean spherical equivalent was close to emmetropia for both groups and stable across postoperative visits. Overall, 97.73% and 100% of eyes in the POD F GF IOL group and 95.65% and 100%, of eyes in the POD F IOL group were within ± 1.00D of the target refraction at 12 and 24 months, respectively. All patients showed a CDVA of ≥ 20/25 at 12- and 24-months post-surgery. In both groups, 24 months post-surgery 91% of patients presented a DCIVA of ≥ 20/25 and 83.3% of patients had a DCNVA of ≥ 20/25. Defocus curve showed continuous visual acuity, being 20/32 or better in both groups over a 4.00D range between 1.00D and − 3.00/-3.50D. Both groups showed good contrast sensitivity values for photopic and mesopic conditions. Overall, 86.4%, 86.4%, and 72.7% of patients implanted with the POD F GF IOL reported not wearing glasses at all for distance, intermediate, and near vision, respectively. These values were 81.8%, 86.4%, and 90.9% for patients implanted with the POD F IOL. Both groups of patients reported similar satisfaction percentages (100% very satisfied/satisfied) and would recommend the procedure (100% definitively yes/probably yes).
Conclusion: This study demonstrates good visual and refractive outcomes for both the FineVision POD F GF and the FineVision POD F IOLs when implanted in Asian eyes.
Keywords: trifocal, Asian, glistening-free, intraocular lens, cataract
Introduction
Developments in intraocular lens technology focusing on both the optical design and the material used to create intraocular lenses (IOLs) have led to excellent refractive and visual outcomes in patients undergoing cataract surgery. For patients considering a multifocal IOL due to presbyopia, bilateral implantation of a trifocal IOL might be an optimal option that does not compromise distant visual acuity.1 A new generation of hydrophobic acrylic materials has been widely used in various commercially available IOLs. It has been reported that the survival rate without the need for capsulotomy is higher in eyes where a hydrophobic IOL is used in contrast to a hydrophilic IOL;2 however, hydrophobic IOLs are particularly affected by the formation of glistening.3
One widely used hydrophobic acrylic material is GF. This has been analyzed to determine its suitability for use in IOLs4 and has been found to be glistening-free with properties that may resist the formation of posterior capsular opacification. This material has been used to create the FineVision POD F GF trifocal IOL (PhysIOL s.a., Liege, Belgium, part of Beaver-Visitec International, Inc. [BVI], Waltham, USA), using the same optical trifocal design as in the hydrophilic FineVision POD F IOL. Previous studies on the POD F GF IOL involving short follow-ups (1 to 6 months)5–11 have demonstrated good clinical performance of the lens and equally good outcomes when compared to its hydrophilic counterpart (POD F).6,7,9 Comparative studies looking at both models have concluded that the good outcomes seen in the two materials give the surgeon the option to choose the preferred IOL for the individual patient based on personal preferences or patient needs.
It has been reported that Asian eyes have different ocular biometric parameters to Caucasian eyes12 (ie, the mean axial length is significantly greater: 23.83 vs 23.48 mm, p<0.001) and that changes in the capsular bag diameter differ in these ethnicities immediately after cataract surgery (about 1 mm larger in Asian eyes).13,14 The different IOL power required for emmetropia and the interaction between the IOL and the capsular bag could affect the stability of the lens once implanted and hence the accuracy of the procedure. However, an analysis of either of these two IOLs in Asian eyes involving a long follow-up period has not been reported to date. Consequently, the main objective of this prospective study was to show the refractive and visual outcomes in Asian patients implanted with the FineVision POD F GF IOL or the FineVision POD F IOL at various times post-cataract surgery.
Methods
Study Design and Patients
This was a single-center prospective comparative study conducted at the Asian Eye Institute, Makati City (Philippines). This study was approved by the SCMC-AEI Ethics Review Committee of the Asian Eye Institute. The study followed the tenets of the Declaration of Helsinki, and after receiving a thorough explanation of the procedure, risks, and possible complications, all the patients provided written informed consent. The study was registered with the National Institutes of Health (clinical trial identifier NCT03306355).
The model implanted was randomized for all patients. The inclusion criteria were cataracts with no comorbidity, spontaneously expressing the desire for spectacle independence after surgery with realistic expectations and availability, willingness, and sufficient cognitive awareness to comply with the examination procedures. The exclusion criteria were unrealistic expectations, age <45 years, irregular astigmatism, regular corneal astigmatism >0.75D measured by an automatic keratometer or biometer or >1.0D if the steep axis of the cylinder was between 90 and 129 degrees, difficulties in cooperation, acute or chronic disease or illness that would increase the risk or confound the study results, any ocular comorbidity, a history of ocular trauma or prior ocular surgery, capsule or zonular abnormalities that could affect postoperative centration or tilt the lens, pupil abnormalities, age macular degeneration and complicated surgery.
Patients were randomly implanted bilaterally with either the trifocal hydrophobic FineVision POD F GF IOL or the trifocal hydrophilic FineVision POD F IOL. Both IOLs have the same haptic (double-C-loop) and optical design (diffractive to create two additions: +3.50D and +1.75D). The POD F IOL model is created with 26% hydrophilic acrylic material and the POD F GF model is created with hydrophobic glistening-free acrylic. The Abbe numbers are 58 and 42 for the POD F and POD F GF models, respectively, and the refractive indexes are 1.46 and 1.52. Both IOL models are available from 0.00 to 35.00D in 0.50D steps.
Cataract surgery was performed using standard phacoemulsification with a 2.75 mm incision, targeting a 5.5 mm diameter capsulorhexis or femtosecond laser-assisted capsulotomy to allow the optic to be fully overlapped by the anterior capsular rim.
Preoperative and Postoperative Assessment
All patients included in this study were comprehensively evaluated prior to the surgery, and the following examinations were carried out: photopic monocular corrected-distance visual acuity (CDVA), refraction, and optical biometry (IOLMaster, Carl Zeiss Meditec AG, Jena, Germany). A constant of 119.0 for the POD F IOL and 119.4 for the POD F GF IOL was used for optical biometry. The IOL power was calculated using the Barrett Universal II formula. The targeted refraction was emmetropia. Postoperatively, the following measurements were performed at 3, 12, and 24 months: binocular uncorrected-distance visual acuity (UDVA), CDVA, distance-corrected intermediate visual acuity (DCIVA) at 70 cm, and distance-corrected near visual acuity (DCNVA) at 35 cm. The binocular photopic defocus curve from +1.50D to −5.00D and binocular photopic and mesopic (3.5 cd/m2) contrast sensitivity were measured at 12 and 24 months. For the refractive error, the sphere, cylinder, and manifest refraction spherical equivalent (MRSE) were also measured at different times post-surgery. Any adverse events or complications were also recorded.
Three months after the operation, patients were asked about their need to wear reading aids for various distances, using the following questions: 1) Do you currently wear glasses for distance vision tasks (eg, reading street signs, going to see movies, sports events, and the theatre)? 2) Do you currently wear glasses for intermediate vision tasks (eg, to see how people react to things you say, to read prices in the supermarket, and to work on a PC)? 3) Do you currently wear glasses for near vision tasks (eg, reading newspapers/magazines/books and sewing)? In addition, they were asked about their general level of satisfaction (How satisfied are you with your overall vision?), whether they would choose the same IOL model again, and if they would recommend this IOL to a friend or family member.
Statistical Analysis and Sample Size
The outcomes were analyzed using Excel (2019, version 16.43, Microsoft Corporation, Redmond, WA, USA). All measurements are given as mean ± standard deviation (SD) and ranges. For the sample size calculation, the following parameters were used: alpha (0.05), power (0.90), two-sided test, expected standard deviation of outcome (0.08 logMAR), and equivalence margin (0.08 logMAR). Using the Sealed Envelope Power calculator and in order to show no difference between the two study cohorts, 22 patients per group were needed.15
Results
In this clinical study, 44 eyes from 22 patients were implanted with POD F GF IOL and 48 eyes from 24 patients were implanted with POD F IOL. Table 1 shows the patient demographics and preoperative characteristics. All patients were available for the follow-up after 1 month, 45 patients (POD F GF: 22 and POD F: 23) after 3 and 12 months, and 24 patients (POD F GF: 12 and POD F: 12) attended the 24-month follow-up.
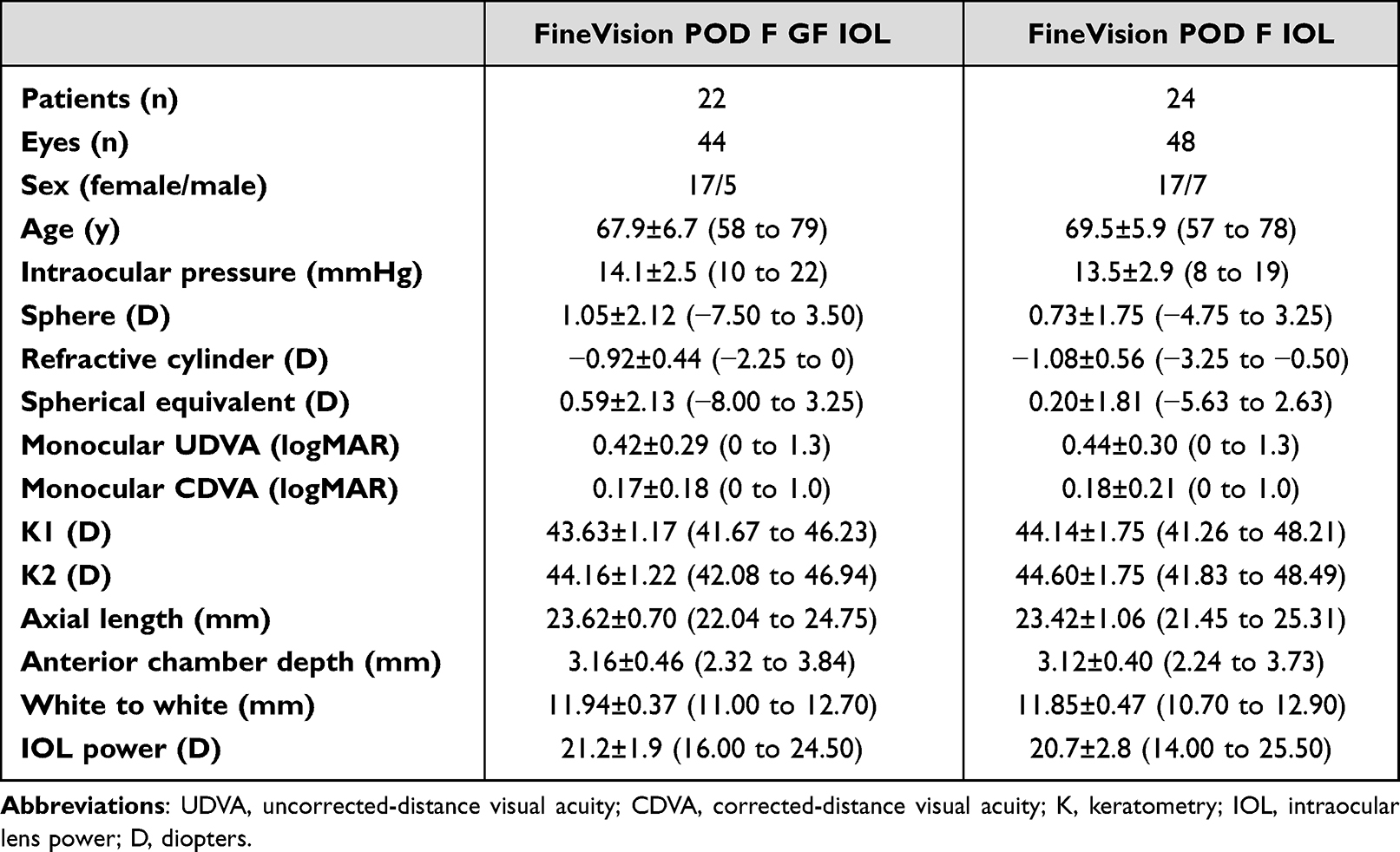 |
Table 1 Demographic Characteristics of Participants Shown as Means, Standard Deviations (SD), and Ranges |
Standard graphs for reporting refractive and visual acuity outcomes were constructed. Figure 1 (refractive accuracy) shows the mean MRSE and cylinder values at different times post-surgery for the POD F GF IOL and POD F IOL groups. All eyes showed a mean MRSE value close to emmetropia (less than 0.25D) at the follow-ups for both groups of IOLs, with similar values for the two (top graph). In relation to the mean refractive cylinder, the outcomes were similar between lenses with values about half a diopter of cylinder across all postoperative visits. Overall, 86.36% and 75% of eyes in the POD F GF IOL group and 80.43% and 75% of eyes in the POD F IOL group, were within ±0.50D of the target refraction at 12 and 24 months, respectively. These percentages changed to 97.73% and 100%, and 95.65% and 100%, respectively, for ±1.00D.
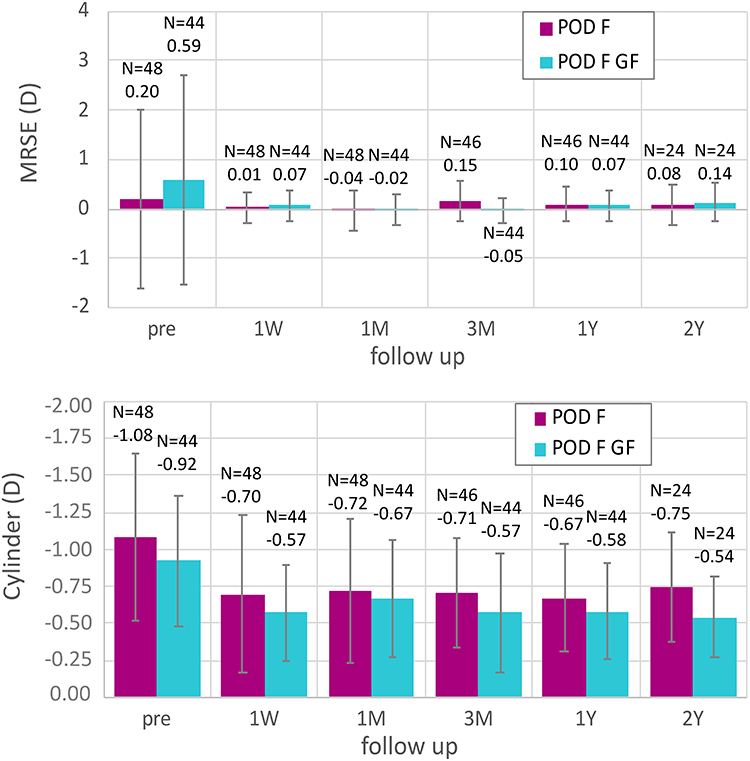 |
Figure 1 Refraction outcomes: manifest refraction spherical equivalent (MRSE) and cylinder values at different times post-surgery for the FineVision POD F GF IOL and FineVision POD F IOL groups. |
Figure 2 shows the cumulative proportion of eyes with a given binocular logMAR UDVA and CDVA values at different times post-surgery for the POD F GF IOL and POD F IOL groups. All the patients presented a CDVA of 20/25 or better (≤0.10 logMAR) at 12- and 24-months post-surgery. The percentages were similar between the two groups and maintained across different post-surgery follow-up times. Specifically, the mean values of binocular CDVA for the POD F GF IOL group were 0.02±0.05, 0.01±0.06, and −0.01±0.05 logMAR at 3, 12, and 24 months, respectively; these values were 0.01±0.05, 0.02±0.05, and 0.03±0.05 logMAR for the POD F IOL group.
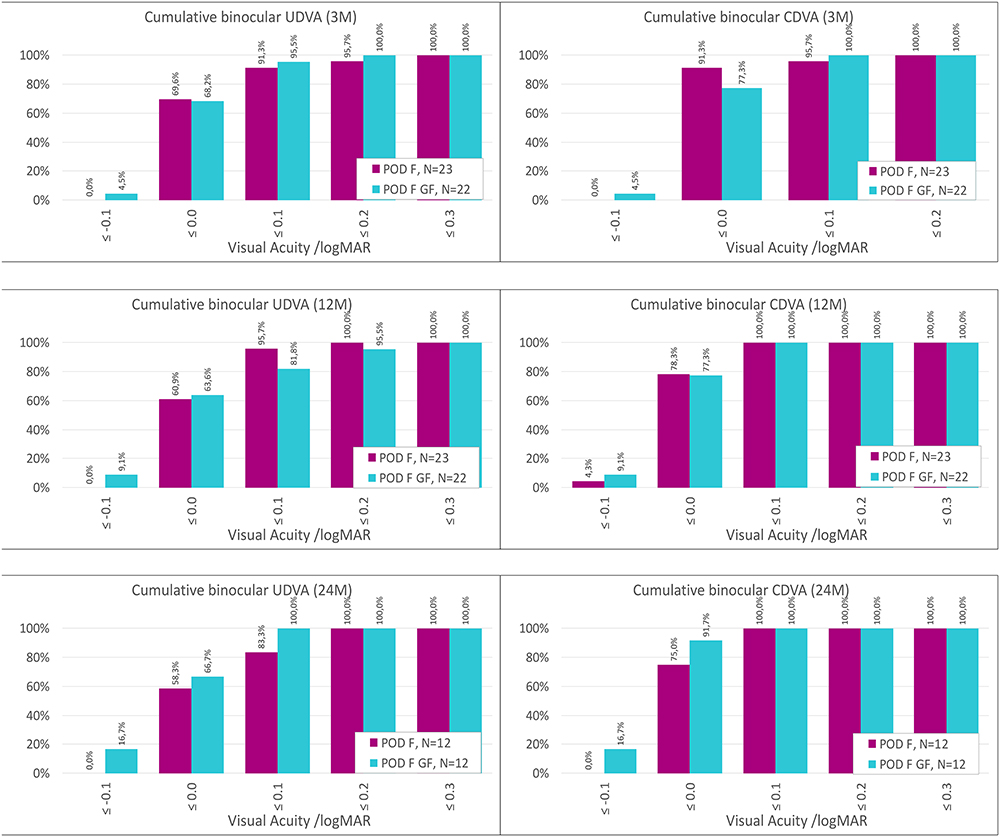 |
Figure 2 Cumulative proportion of eyes having a given binocular logMAR uncorrected-distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) value at different times post-surgery for the FineVision POD F GF IOL and FineVision POD F IOL groups. |
Figure 3 shows the cumulative proportion of eyes with given binocular logMAR DCIVA and DCNVA values at different post-surgery follow-up times for the POD F GF IOL and POD F IOL groups. In both groups, at 24-months post-surgery, 91% of patients presented a DCIVA of 20/25 or better (≤0.10 logMAR) and 83.3% of patients had a DCNVA of 20/25 or better (≤0.10 logMAR). Specifically, the mean values of binocular DCIVA for the POD F GF IOL group were 0.05±0.08, 0.07±0.10, and 0.04±0.08 logMAR at 3, 12, and 24 months, respectively; these values were 0.05±0.08, 0.02±0.07, and 0.04±0.08 logMAR for the POD F IOL group. At near vision, the mean binocular DCNVA values were 0.10±0.12, 0.12±0.13, and 0.06±0.09 logMAR at 3, 12, and 24 months, respectively, for the POD F GF IOL; for the POD F IOL group the values were 0.05±0.07, 0.05±0.07, and 0.08±0.10 logMAR.
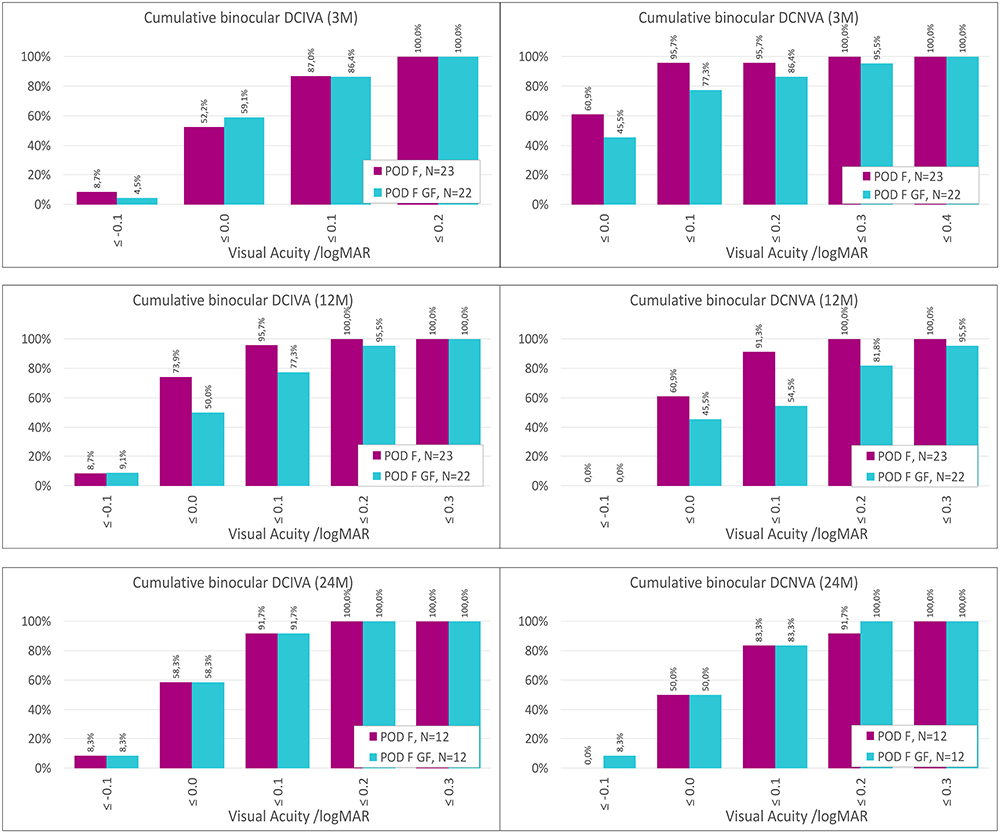 |
Figure 3 Cumulative proportion of eyes having a given binocular logMAR distance-corrected intermediate visual acuity (DCIVA) and distance-corrected near visual acuity (DCNVA) value at different times post-surgery for the FineVision POD F GF IOL and FineVision POD F IOL groups. |
Figure 4 shows the mean photopic binocular defocus curve for the POD F GF IOL and POD F IOL groups at 12- and 24-months post-surgery. The curves for the two groups were similar. The visual acuity was 20/32 or better in both groups over a 4.00D range between 1.00D and −3.00/-3.50D. At 24-months post-surgery it was 20/25 or better in both groups over about a 3.00D range. Figure 5 shows the mean photopic and mesopic binocular contrast sensitivity function for the POD F GF IOL and POD F IOL groups at 12- and 24-months post-surgery. Both groups presented good log contrast sensitivity values at different spatial frequencies analyzed for photopic and mesopic lighting conditions. Note that the photopic values were slightly better than those found under mesopic conditions. Figure 6 shows the patient-reported outcomes at 3 months post-surgery for the POD F GF IOL and POD F IOL groups: spectacle independence for distance, intermediate, and near vision (left column); and patient satisfaction and recommendation (right column). Overall, 86.4%, 86.4%, and 72.7% of patients implanted with the POD F GF IOL reported wearing glasses none of the time for distance, intermediate, and near vision, respectively; these values were 81.8%, 86.4%, and 90.9% in patients implanted with the POD F IOL. The two groups of patients reported similar levels of satisfaction (100% very satisfied or satisfied) and recommendation (100% definitively yes and probably yes).
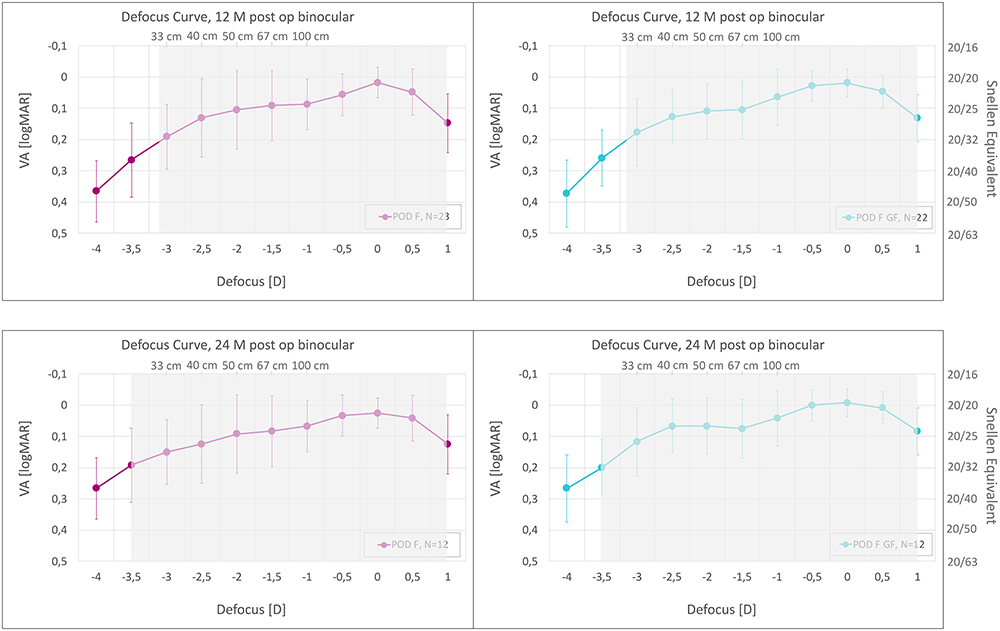 |
Figure 4 Mean photopic binocular logMAR visual acuity with best correction for distance as a function of the chart vergence from 1.5 D to −4.0 D for the FineVision POD F GF IOL and FineVision POD F IOL groups at 12- and 24-months post-surgery. The error bars represent the standard deviation. The right y-axis shows Snellen feet acuity, and the upper x-axis shows distance values (cm). The grey area represents the defocus region where mean visual acuity is above 0.20 logMAR. |
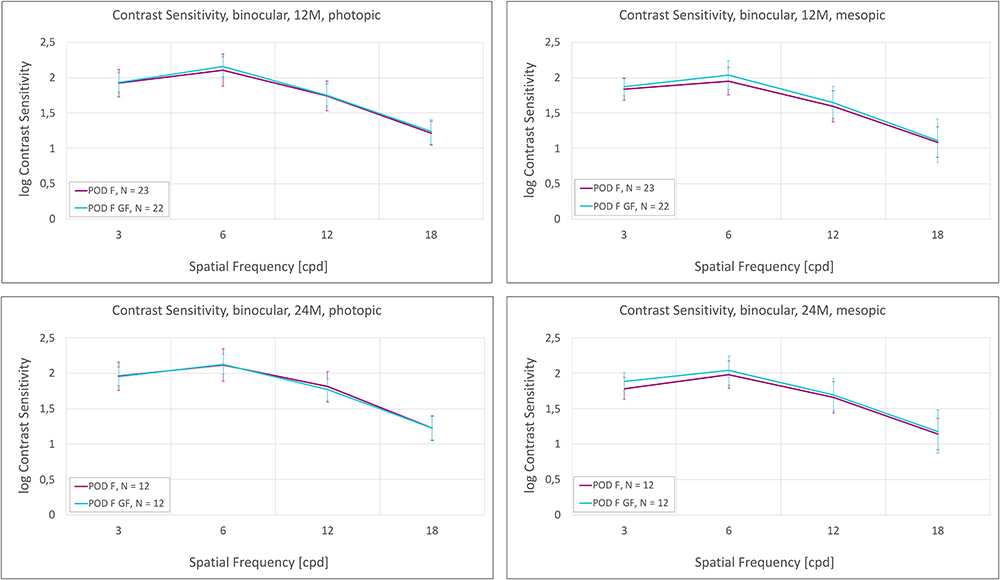 |
Figure 5 Mean photopic and mesopic binocular contrast sensitivity function for the FineVision POD F GF IOL and FineVision POD F IOL groups at 12- and 24-months post-surgery. |
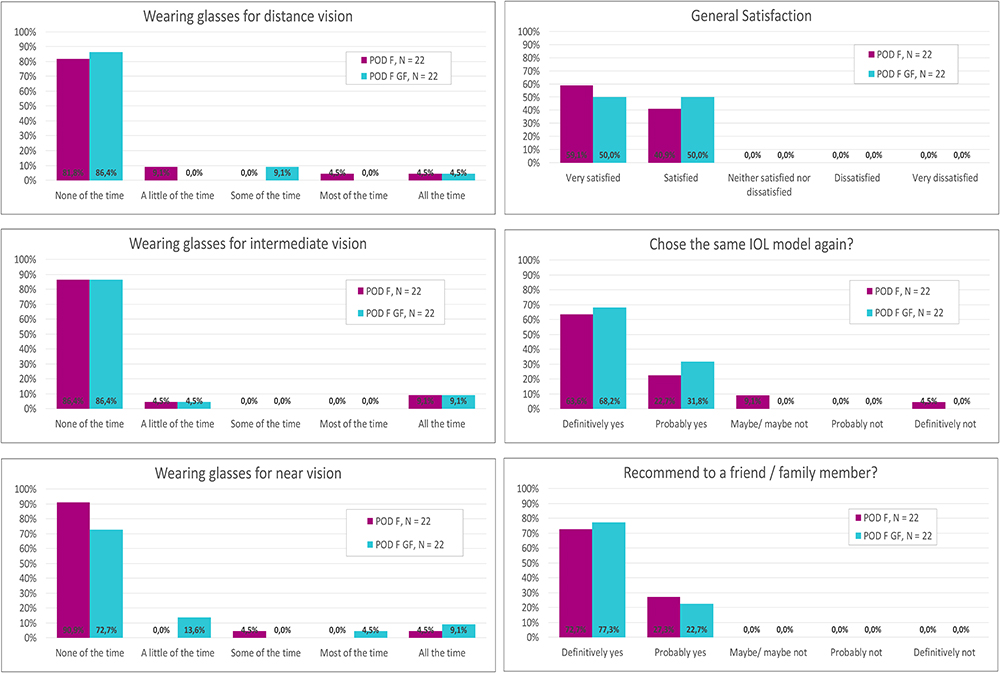 |
Figure 6 Patient-reported outcomes at 3 months post-surgery for the FineVision POD F GF IOL and FineVision POD F IOL groups. Spectacle Independence for distance, intermediate, and near vision (left column); and patient satisfaction and recommendation (right column). |
In the POD F IOL group, one eye required a second operation (lens exchange after loading error and incorrect implantation), and one eye presented a retinal detachment 24-months after the surgery; both were resolved without sequelae.
Discussion
Previous clinical studies on the FineVision POD F GF IOL have reported good refractive outcomes and excellent visual acuities at different distances following cataract surgery.5–11 As mentioned, these studies involved short follow-ups and mainly Caucasian populations. In this study, we have analyzed this lens specifically in Asian eyes and we included a long follow-up in order to provide further evidence for this lens over a longer period in this population.
The refractive accuracy obtained for both groups in this trial was excellent. Figure 1 shows the mean MRSE and cylinder values in the two groups at various times post-surgery. It should be noted that the mean MRSE values were close to emmetropia. Nagy et al6 analyzed both of these IOL models by implanting the POD F GF IOL in one eye and the POD F IOL in the contralateral eye in the same patient, in a group of 25 Hungarian patients, and monitored them for 6 months. Obviously, we cannot compare our study directly with this, but they did report a MRSE value of 0.07±0.19D in the POD F group and 0.05±0.21D in the POD F GF group, with all the eyes being within ±0.50D of the target refraction. In another study, Poyales et al7 analyzed the two models in two groups of Spanish patients, 3 months post-surgery: one group included 25 patients implanted bilaterally with the hydrophilic lens; and in the other group, 26 patients were implanted bilaterally with the hydrophobic lens. The postoperative MRSE was 0.00±0.29 and 0.23D for the POD F and POD F GF IOL groups, respectively. Overall, 83% of eyes with the POD F IOL and 90% of eyes with the POD F GF were within ±0.50D, with 100% and 92% being within ±1.0D of the target refractive spherical equivalent, respectively. Benyoussef et al10 analyzed 21 patients implanted bilaterally with the POD F GF (FineVision HP) IOL at 1-month post-surgery. They found an average MRSE of 0.14±0.64D, with 73% and 92% of eyes being ±0.50D and ±1.0D, respectively. Despite the differences in the population evaluated and the follow-up times in the two studies,6,7,10 the values reported by these authors are similar to those found in our sample, confirming the good refractive accuracy of both IOL models. It should be noted that the two models differ in their curvature and thickness due to the different refractive index and Abbe number of the hydrophobic/hydrophilic material. Theoretically, this could affect the refractive outcomes; however, as shown in Figure 1, there were only small differences between the refractive accuracy for the two groups of IOLs across the visits. It therefore seems that the distinct materials used do not affect the final outcomes. One recent systematic review and meta-analysis of trifocal lenses showed that the mean spherical equivalent of four studies was 0.03D (n=131) and the mean cylinder of six studies was −0.50D (n=191).16 The outcomes from our work were similar to those reported for other trifocal IOLs available on the market, and the different ocular biometric parameters of Asian eyes do not appear to play a significant role in the final refractive outcome.
The DCVA outcomes recorded at the various post-surgery follow-ups were good in terms of both mean values and percentages of cumulative visual acuity (see Figure 2). All the patients presented a CDVA of 20/25 or better (≤0.10 logMAR) at 12- and 24-months post-surgery, and the mean values were approximately 0 logMAR. At intermediate and near vision the outcomes were also good (Figure 3). In both groups, 24 months post-surgery, 91% of the patients presented a DCIVA of 20/25 or better (≤0.10 logMAR) and 83.3% of patients had a DCNVA of 20/25 or better (≤0.10 logMAR). The mean values were similar between the models, being about 0.05 and 0.10 logMAR for DCIVA and DCNVA, respectively. A review of trifocal IOLs showed a mean DCIVA from two published studies (n=59) of 0.24 logMAR and a mean DCNVA from 5 studies (n=149) of 0.11 logMAR.16 Nagy et al6 found no statistically significant differences between the models for visual acuity at any distance (far, 70, and 35 cm). Poyales et al7 found a mean binocular CDVA, DCIVA (80 cm), and DCNVA (40 cm) of −0.04±0.04, 0.09±0.10, and 0.10±0.09 logMAR, respectively, for the POD F IOL, and −0.03±0.03, 0.08±0.10, and 0.13±0.11 logMAR, respectively, for the POD GF IOL. The 100% of patients in each group presented a binocular 0.1 logMAR (20/25) or better CDVA. The 92% and 88% of patients presented a binocular 0.1 logMAR or better DCIVA (70 cm) for the POD F and POD F GF IOL groups, respectively. Additionally, 88% of patients from each group presented a binocular 0.1 logMAR or better DCNVA (35 cm). It should be noted that these measurements were made at the 1-month follow-up visit. In general, there was no statistically significant difference between the two treatment groups at any of the distances assessed (p>0.05). Benyoussef et al10 reported a binocular CDVA, DCIVA (70 cm), and DCNVA (35 cm) of −0.076±0.084, −0.038±0.071, and −0.011±0.092 logMAR, respectively, with 98% of patients having a binocular cumulative decimal of CDVA ≥0.8.
In relation to visual acuity at different vergences, both groups showed good visual acuities across a large range. The grey area in the four graphs of Figure 4 shows the defocus region where the mean visual acuity is above 0.20 logMAR. Similarly, Nagy et al6 found visual acuities of 20/32 or better over a 3.00D range between 0.50D and −3.00D and no differences between IOL models. Additionally, Poyales et al7 found an extended range of clear vision in their defocus curves, with maintained mean visual acuity values of 0.09 logMAR or better in the POD F IOL group and 0.15 logMAR or better in the POD F GF IOL group. Benyoussef et al10 reported a defocus curve with mean values equal to or better than 0.1 logMAR over a range of approximately 4.00D. The good contrast sensitivity outcomes for both IOL models at 12- and 24-months post-surgery are shown in Figure 5. Nagy et al6 found no statistically significant differences between models for photopic and mesopic contrast sensitivity. Poyales et al7 reported that the photopic outcomes were slightly better than the mesopic ones at high and low spatial frequencies. The mesopic values of the POD F IOL group at 3 and 6 cpd were slightly above those found for the POD F GF IOL group; however, the differences were not statistically significant (p>0.05). Benyoussef et al10 reported good outcomes in terms of photopic contrast sensitivity (measured in a subgroup of 15 patients), with similar values to those reported in our study at other times post-surgery. The patient-reported outcomes were good for both IOLs with a high percentage of patients reporting that they had stopped wearing glasses for distance, intermediate, and near vision, as well as 100% satisfaction and recommendation levels (see Figure 6). Benyoussef et al10 used the NEI VFQ-25 questionnaire and found that the satisfaction rate was 85.7%, the proportion of patients who would recommend the procedure was 90.5%, and 95.2% of patients would have the surgery again if they had the choice. As indicated by the authors, the main limitation of the study was the short follow-up.
Other studies have assessed the outcomes of the hydrophobic model in special situations. For example, in a published clinical case, Mayer et al8 showed the use of the POD F GF IOL with the Customflex artificial iris and reported a CDVA, DCNVA (40 cm), and DCIVA (80 cm) of 0.20, 0.20, and 0.22 logMAR, respectively, 3 months after the surgery. Garzón et al9 compared the refractive outcomes in eyes implanted with one of the two IOL models (48 with the POD F GF IOL and 49 with the POD F IOL) at 1-month post-surgery, using subjective and objective methods. Both models have the same optical design but use distinct materials, with different Abbe numbers, which may change the behavior of the chromatic aberration17,18 and therefore the outcomes found using objective methods such as autorefractometers or wavefront aberrometers. They concluded that none of the objective methods were as reliable as subjective refraction, irrespective of the lens material, but the POD F GF objective values seem to differ less with subjective refraction than the POD F objective values. Kim et al11 analyzed 212 eyes (106 patients) with mix-and-match implanted FineVision Triumf and FineVision HP (POD F GF IOL) and 212 eyes (106 subjects) with mix-and-match implanted Zeiss AT LARA and AT LISA IOLs at 6–10 weeks after cataract surgery. They concluded that these lenses provided good visual outcomes at far, intermediate, and near distances, with the FineVision IOLs leading to better visual outcomes in terms of near vision, while the other combination resulted in better visual outcomes for intermediate vision.
Conclusion
The outcomes reported for this cohort of Asian patients bilaterally implanted with the FineVision POD F GF IOL or the FineVision POD F IOL at different times post-cataract surgery show that both models are effective in terms of providing good visual acuity at different distances. For both lenses, patients were very satisfied with the results and would recommend their use.
Data Sharing Statement
Data are not available for sharing.
Funding
This study was funded by PhysIOL s.a., Liege, Belgium, part of Beaver-Visitec International, Inc. [BVI], Waltham, USA.
Disclosure
R. Ang has received research grants from Acevision, Inc., Acufocus, Inc., Bausch&Lomb, Inc.; Beaver-Visitec International, Glaukos Corp., Ivantis, Inc., Hoya, Ivantis, Johnson&Johnson Vision, and STAAR Surgical. The author reports no other conflicts of interest in this work.
References
1. Cho JY, Won YK, Park J, et al. Visual Outcomes and Optical Quality of Accommodative, Multifocal, Extended Depth-of-Focus, and Monofocal Intraocular Lenses in Presbyopia-Correcting Cataract Surgery: a Systematic Review and Bayesian Network Meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–1053. doi:10.1001/jamaophthalmol.2022.3667
2. Chang A, Kugelberg M. Posterior capsule opacification 9 years after phacoemulsification with a hydrophobic and a hydrophilic intraocular lens. Eur J Ophthalmol. 2017;27(2):164–168. doi:10.5301/ejo.5000831
3. Tandogan T, Auffarth GU, Son HS, Merz P, Choi CY, Khoramnia R. In-vitro glistening formation in six different foldable hydrophobic intraocular lenses. BMC Ophthalmol. 2021;21(1):126. doi:10.1186/s12886-021-01879-6
4. Pagnoulle C, Bozukova D, Gobin L, Bertrand V, Gillet-de Pauw MC. Assessment of new-generation glistening-free hydrophobic acrylic intraocular lens material. J Cataract Refract Surg. 2012;38(7):1271–1277. doi:10.1016/j.jcrs.2012.02.041
5. Vinas M, Gonzalez-Ramos A, Dorronsoro C, et al. In vivo measurement of longitudinal chromatic aberration in patients implanted with trifocal diffractive intraocular lenses. J Refract Surg. 2017;33(11):736–742. doi:10.3928/1081597X-20170814-01
6. Nagy ZZ, Popper-Sachetti A, Kiss HJ. Comparison of visual and refractive outcomes between hydrophilic and hydrophobic trifocal intraocular lenses sharing the same optical design. J Cataract Refract Surg. 2019;45(5):553–561. doi:10.1016/j.jcrs.2018.11.034
7. Poyales F, Pérez R, López-Brea I, Zhou Y, Rico L, Garzón N. Comparison of Visual Performance and Patient Satisfaction Outcomes with Two Trifocal IOLs with Similar Optical Design but Different Materials. Clin Ophthalmol. 2020;14:3237–3247. doi:10.2147/OPTH.S273641
8. Mayer CS, Son HS, Łabuz G, et al. Laboratory and Clinical Experience With a Diffractive Trifocal Intraocular Lens Sutured to an Artificial Iris. J Refract Surg. 2022;38(1):61–68. doi:10.3928/1081597X-20211209-02
9. Garzón N, Poyales F, García-Montero M, Vega F, Millán MS, Albarrán-Diego C. Impact of Lens Material on Objective Refraction in Eyes with Trifocal Diffractive Intraocular Lenses. Curr Eye Res. 2022;47(1):51–61. doi:10.1080/02713683.2021.1946563
10. Benyoussef AA, Reboux N, Cochener B. Comparison of Bilateral Reading Performance Among Two Presbyopia-Correcting Intraocular Lenses. J Refract Surg. 2022;38(7):428–434. doi:10.3928/1081597X-20220516-02
11. Kim JW, Eom Y, Park W, et al. Comparison of visual outcomes after two types of mix-and-match implanted trifocal extended-depth-of-focus and trifocal intraocular lenses. Graefes Arch Clin Exp Ophthalmol. 2022;260(10):3275–3283. doi:10.1007/s00417-022-05710-w
12. Yoon JJ, Misra SL, McGhee CN, Patel DV. Demographics and ocular biometric characteristics of patients undergoing cataract surgery in Auckland, New Zealand. Clin Exp Ophthalmol. 2016;44:106–113. doi:10.1111/ceo.12634
13. Tehrani M, Dick HB, Krummenauer F, et al. Capsule measuring ring to predict capsular bag diameter and follow its course after foldable intraocular lens implantation. J Cataract Refract Surg. 2003;29:2127–2134. doi:10.1016/S0886-3350(03)00352-3
14. Kim JH, Lee D, Cha YD, et al. The analysis of predicted capsular bag diameter using modified model of capsule measuring ring in Asians. Clin Exp Ophthalmol. 2008;36:238–244. doi:10.1111/j.1442-9071.2008.01726.x
15. Sealed Envelope Ltd. Power calculator for continuous outcome equivalence trial; 2012. Available from: https://www.sealedenvelop.com/power/continous-equivalence.
16. Shen Z, Lin Y, Zhu Y, Liu X, Yan J, Yao K. Clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2017;7:45337. doi:10.1038/srep45337
17. Vinas M, Gonzalez-Ramos A, Dorronsoro C, et al. In vivo measurement of longitudinal chromatic aberration in patients implanted with trifocal diffractive intraocular lenses. J Refract Surg. 2017;33(11):736–742.
18. Vinas M, Gonzalez-Ramos AM, Aissati S, et al. Longitudinal Chromatic Aberration in Patients Implanted With Trifocal Diffractive Hydrophobic IOLs. J Refract Surg. 2020;36(12):804–810. doi:10.3928/1081597X-20200930-01
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.