Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Factors Influencing Disease Perception Among Elderly Patients with Chronic Obstructive Pulmonary Disease in China: A Cross-Sectional Study
Authors Li H, Liu L, Xu C, Xie J
Received 24 February 2025
Accepted for publication 27 November 2025
Published 30 December 2025 Volume 2025:20 Pages 4191—4204
DOI https://doi.org/10.2147/COPD.S524700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Houmin Li,1 Lijun Liu,1 Chuchu Xu,2 Jun Xie1
1Department of General Medicine, The Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, 230011, People’s Republic of China; 2Department of Respiration and Critical Care Medicine, The Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Hefei, 230011, People’s Republic of China
Correspondence: Jun Xie, Department of General Medicine, The Second People’s Hospital of Hefei, Hefei Hospital Affiliated to Anhui Medical University, Intersection of Guangde Road and Leshui Road, Yaohai District, Hefei, 230011, People’s Republic of China, Tel +86 13731962160, Email [email protected]
Background: Community-based management improve chronic disease outcomes, but their impact on disease perception and frailty in chronic obstructive pulmonary disease (COPD) patients remains underexplored.
Objective: To identify factors influencing disease perception in elderly COPD patients and assess the role of community-based management.
Methods: In this cross-sectional study, 223 COPD patients aged ≥ 60 years (diagnosed per the 2021 Guidelines for Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease) were randomly selected. Dyspnoea severity was graded via the mMRC scale; COPD severity incorporated spirometry (FEV1/FVC) and symptom burden (COPD Assessment Test). Participants completed the Brief Illness Perception Questionnaire (BIPQ), Tilburg Frailty Indicator (TFI), and a general information survey. Differences between community-managed (n=81) and non-community-managed (n=142) groups were compared. Pearson’s correlation and multivariate linear regression analyses identified predictors of disease perception.
Results: Mean BIPQ score was 46.87± 7.47 (moderate threat perception), and frailty score was 8.02± 2.38. Disease perception positively correlated with total frailty and its subdomains (P< 0.05). Community-managed patients had significantly lower BIPQ and TFI scores (P< 0.05). Regression revealed disease duration (β=0.28), dyspnoea severity (β=0.22), and frailty (β=0.19) as positive predictors of disease perception; community management (β=− 0.15) and older age (β=− 0.12) were negative predictors (P< 0.05). The model explained 46.0% of variance (R2=0.46, F=18.03, P< 0.001).
Conclusion: Elderly patients with COPD demonstrated strong links between disease perception and frailty. Community-based management considerably reduced these scores, indicating its potential to improve patient outcomes.
Keywords: chronic obstructive pulmonary disease, the elderly, disease perception, frailty
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of global morbidity and mortality, affecting over 300 million individuals worldwide and contributing to 3.2 million deaths annually, according to the Global Initiative for Chronic Obstructive Lung Disease 2025 report.1 In 2023, COPD accounted for 6% of all deaths worldwide, underscoring its status as a major public health challenge. In China, COPD prevalence among adults aged ≥40 years exceeds 13%, with substantial socioeconomic burdens due to frequent hospitalisations and reduced quality of life.2
Disease perception – patients’ cognitive and emotional interpretation of their illness – profoundly influences self-management behaviours, treatment adherence and clinical outcomes.3 Negative perceptions are associated with heightened anxiety, poor coping strategies and accelerated disease progression. In patients with COPD, a negative disease perception can lead to poor treatment adherence, increased anxiety and a decline in quality of life.4,5 Frailty, a multidimensional syndrome marked by diminished physiological reserves, exacerbates COPD-related disability and mortality.6 In the context of COPD, frailty is a major concern due to its association with adverse outcomes, including increased risk of disability, hospitalisation and mortality.7,8 The GOLD classifies COPD severity into 4 grades (A–D) based on spirometry (FEV1/FVC ratio), symptom burden (assessed via the COPD Assessment Test [CAT]) and exacerbation history.9 Dyspnoea severity is graded using the modified British Medical Research Council (mMRC) scale, whereas the CAT quantifies symptom impact.10 Despite evidence linking disease perception, frailty and clinical severity, the interplay of these factors remains underexplored in community-managed elderly populations. Understanding the relationship between disease perception and frailty is crucial for developing targeted interventions to improve patient outcomes.
Community management refers to the comprehensive chronic disease management provided by community medical institutions, which includes regular follow-ups, health education, psychological support and coordination of medical resources. Patients in the community management group receive long-term structured interventions from community healthcare providers, whereas those in the non-community management group do not. Community-based chronic disease management programmes, which provide comprehensive support for patients with chronic conditions such as COPD, have been shown to improve disease control, reduce hospitalisations and enhance quality of life.11 However, the impact of community management on disease perception and frailty remains underexplored.
This study investigates the predictors of disease perception in elderly patients with COPD, emphasising the roles of frailty, dyspnoea severity and community-based interventions.
Methods
Study Design and Patients
Patients
In this study, a sample of 223 patients with COPD treated at our hospital between January 2023 and September 2024 was selected using the random sampling method. Patients were divided into the community management group and the non-community management group according to whether they had received comprehensive community management for a long period of time.
The inclusion criteria were as follows: (1) participants aged 60 years or older, irrespective of gender; (2) patients diagnosed with COPD according to the GOLD 2023 report.12 The severity of COPD was classified based on the mMRC dyspnoea scale and the CAT scores, which are widely used to assess the impact of COPD on patients’ daily lives.1 Patients with mMRC grades 2 and 3 were considered to have moderate to severe COPD, whereas those with grade 4 were classified as having very severe COPD.9,13
The exclusion criteria were as follows: (1) patients with severe illness or considerable cognitive impairment, defined as a MMSE®-2 (brief version) score of less than 14, who were unable to complete the questionnaire independently;14 (2) patients with malignant tumours, serious cardiovascular and cerebrovascular diseases, severe abnormalities in the liver, kidney or lung function or a recent history of major trauma or surgery.15 This study received approval from the Ethics Committee of The Second People’s Hospital of Hefei. All procedures complied with the Declaration of Helsinki (2013 revision).
Sample Size and Sampling Technique
A priori sample size calculation was performed using G*Power 3.1. Based on a medium effect size (f2 = 0.15), α = 0.05, power = 0.80 and 10 predictors, the required sample size was 200. To account for potential attrition, a total of 235 questionnaires were recruited and distributed. Patients were selected via simple random sampling: a list of eligible patients with COPD was generated from hospital records, and random numbers were assigned using SPSS 23.0. Participants were selected until the target sample size was achieved. For patients who had difficulty reading the questionnaire, researchers provided standardised instructions. It took approximately 15–20 minutes for patients to complete the questionnaire, which was promptly reviewed upon return to minimise potential errors and omissions.
Definition of Community Management
Community management refers to a structured, multidisciplinary approach to chronic disease management provided by community healthcare institutions. This approach aims to improve disease control, enhance patient self-management skills and reduce the burden of chronic conditions through coordinated care. In this study, community management included the following components.
(1) Regular follow-ups: patients received routine medical check-ups and consultations with healthcare providers at community clinics or through home visits, typically scheduled every 1–3 months depending on the patient’s condition.
(2) Health education: community healthcare workers provided education on COPD management, including information on medication adherence, smoking cessation and pulmonary rehabilitation. Educational sessions were conducted either individually or in group settings.
(3) Psychological support: patients had access to psychological counselling to address anxiety, depression and other emotional issues related to chronic illness. This support was provided by trained psychologists or social workers within the community healthcare team.
(4) Coordination of medical resources: community healthcare providers coordinated with specialists (eg pulmonologists, nutritionists) to ensure comprehensive care. They facilitated referrals for specialised treatments, such as pulmonary rehabilitation or home oxygen therapy, as needed.
(5) Self-management programmes: patients were enrolled in self-management programmes that included training on symptom monitoring, inhaler technique and emergency action plans. These programmes aimed to empower patients to take an active role in managing their condition.
(6) Social support: community management also involved assessing and addressing social determinants of health, such as access to healthcare services, social isolation and economic barriers. Support was provided through community resources, including social workers and community health workers.
Patients in the community management group had received these comprehensive interventions for at least 6 months, ensuring a sufficient duration for the impact of the programme to be observed. In contrast, patients in the non-community management group had not received such structured interventions and relied primarily on hospital-based care.
Variable Assignment
The dependent variable was the total disease perception score measured using the Brief Illness Perception Questionnaire (BIPQ). Independent variables included age, gender, disease duration, dyspnoea severity (mMRC) and frailty (TFI) as described in Questionnaire and Scales. Covariates such as educational level, comorbidities and the CAT scores were also included. Table 1 summarises the operational definitions, measurement tools and scoring methods for all variables.
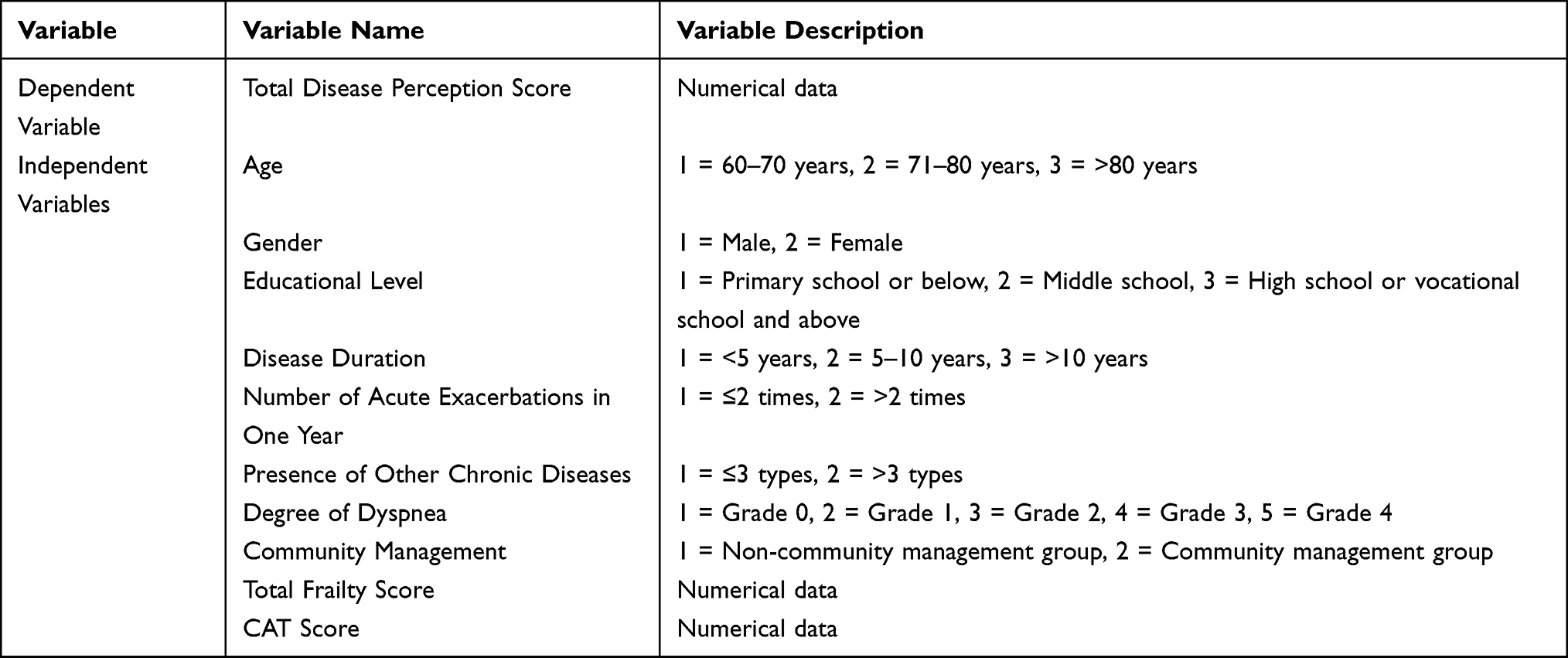 |
Table 1 Variable Assignment |
Questionnaire and Scales
(1) General information questionnaire: information such as the patient’s age, gender, marital status, educational level, economic status, history of smoking and alcohol use, past medical history and community management was collected using a self-designed general information questionnaire.
(2) Disease perception assessment: the BIPQ was used for measurement. The BIPQ was designed to quickly assess the cognitive and emotional manifestations of illness.16 It consists of eight single-item scales and the revised causal scale of the IPQ. Each item is scored on a scale of 0 to 10 and includes 8 aspects: disease impact, disease duration, personal control, treatment control, symptom identification, disease concern, emotion and disease understanding. The causal scale is an open-ended cause evaluation item that requires participants to list the three most important self-perceived causes of their disease. Items 3, 4 and 7 of the BIPQ are reverse-scored. The scores of each item, except for the cause, can be summed. The higher the score, the more severe the perceived disease threat by the patient. The BIPQ has been used in different age groups, disease types and languages, and the scale has good reliability and predictive validity, with a Cronbach’s alpha value of 0.702.8 Currently, the Chinese version of the BIPQ has been confirmed to have good reliability and validity.17
3) Frailty scale assessment: the Tilburg Frailty Indicator (TFI) was used to diagnose frailty in the elderly.18,19 The TFI includes three dimensions – psychological frailty, physical frailty and social frailty – with a total of 15 items. Psychological frailty includes 4 items: coping ability, anxiety, depression and memory. Physical frailty includes 8 items: difficulty walking, physical health, balance, weight loss, grip strength, vision problems, hearing problems and fatigue. Social frailty includes 3 items: social support, social relationships and living alone. The scale uses a binary scoring method, with a total score ranging from 0 to 15. The higher the score, the more severe the degree of frailty. A TFI score of ≥5 is considered indicative of frailty. The Chinese version of the TFI, which was adapted for use in China, was used to assess frailty.20
(4) Comprehensive COPD assessment: the CAT was used as a comprehensive symptom evaluation index.21 This scoring system offers a broader assessment of the impact of disease symptoms. It contains 8 items, each scored from 0 (no symptoms) to 5 (very severe symptoms), with a total score ranging from 0 (healthy) to 40 (extremely severe COPD). The higher the score, the greater the impact of COPD on daily life and the more severe the condition. The mMRC dyspnoea scale was also used. The mMRC scale ranges from grade 0 to grade 4: grade 4 indicates shortness of breath with minimal movement; grade 3 indicates the need to stop and rest after walking a few hundred metres or a few minutes on flat ground; grade 2 indicates walking more slowly than peers or the need to stop due to shortness of breath; grade 1 indicates shortness of breath when walking quickly; and grade 0 indicates no considerable shortness of breath during routine activities.9,22
Data Collection
Data were collected during the patients’ hospital stay, typically within the first 48 hours of admission, to ensure accurate and timely information. All participants were provided with detailed information about the study’s purpose, procedures and potential risks. Written informed consent was obtained from each participant or their legal representative before data collection.
Data Analysis
Data were statistically analysed using SPSS 23.0. Count data were presented as frequency and percentage, whereas measurement data were expressed as X ± S. For data following a normal distribution, independent sample t-tests were used to compare two groups, and one-way analysis of variance was used for comparisons among multiple groups. Normality was tested using the Shapiro–Wilk test. For non-normally distributed data, Generalized Linear Models (GLM) with negative binomial distribution and link functions were employed to assess group differences while controlling for covariates. The normality assumption was evaluated based on residuals. Count data were reported as percentages, and group comparisons were performed using the chi-square (χ2) test. Pearson’s correlation analysis was used to assess relationships between variables, and multiple linear regression was conducted to identify influencing factors. The multiple linear regression model was expressed as Y = β0 + β1X1 + β2X2 +. + βnXn + ε, where Y represented the disease perception score, β0 was the intercept, β1–βn were regression coefficients for predictors (X1–Xn) and ε was the error term.23 A P value of <0.05 was considered statistically significant.
Results
General Situation
A total of 235 questionnaires were distributed, of which 223 were returned (94.9%). The patients’ information was statistically analysed. There were 223 patients with COPD, including 144 men (64.57%) and 79 women (35.43%). The non-community management group comprised 63.68% of the sample, whereas the community management group accounted for 36.32%. On the mMRC scale, the severity of dyspnoea was relatively moderate; most patients scored 2 or 3 (137 cases, 61.4%), whereas severe and extremely severe dyspnoea (score of 4) was reported in only 39 cases (17.5%) (see Table 2).
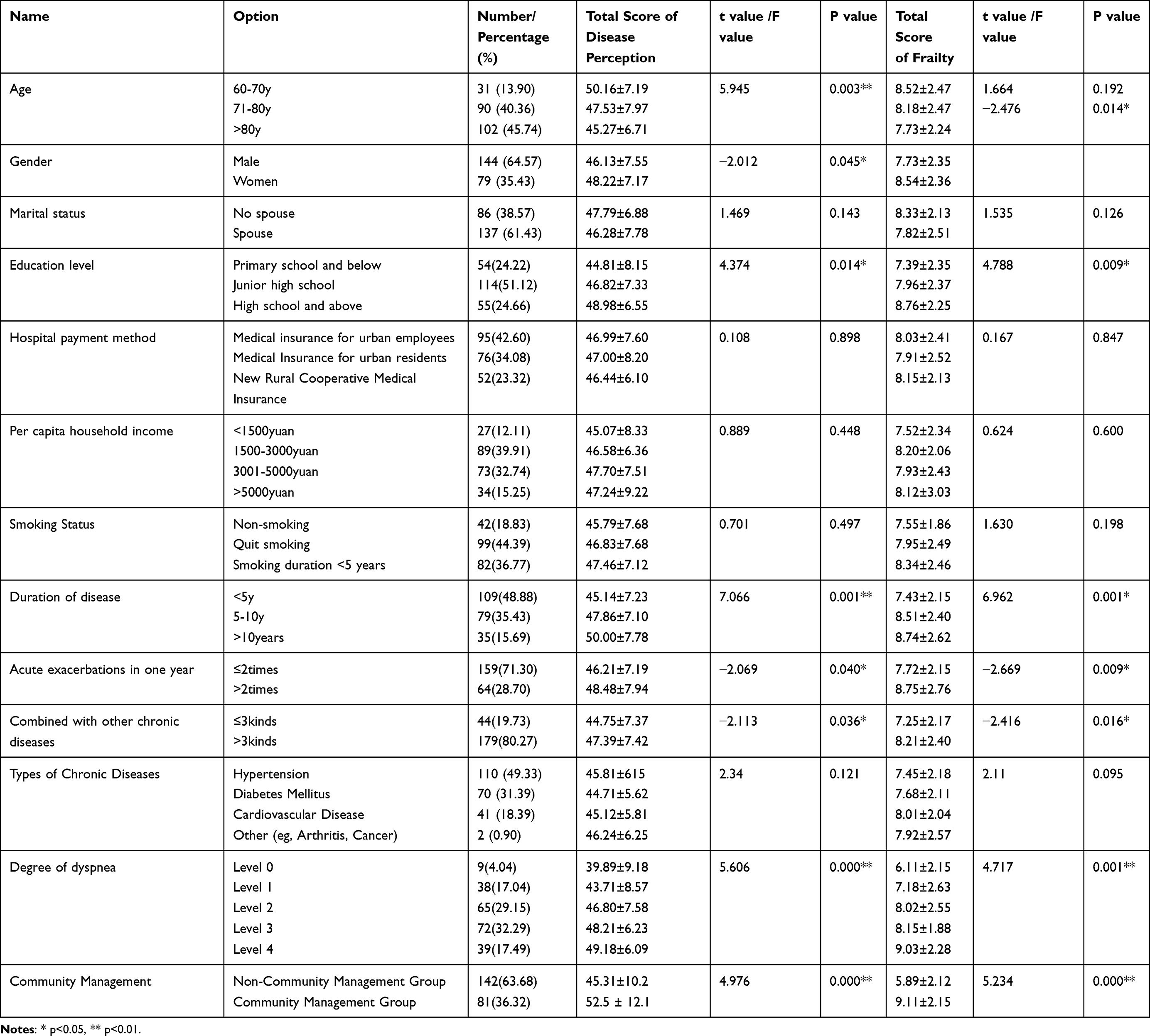 |
Table 2 Comparative Analysis of Demographic and Clinical Data Among Patients |
Scores of BIPQ, Tilburg Frailty Indicator and CAT Scales in Patients with COPD
The mean total BIPQ score was 46.87 ± 7.47. The highest subscale score was observed for the perceived timeline (6.83 ± 1.36), whereas personal control had the lowest score (3.77 ± 1.30). The mean frailty score was 8.02 ± 2.38, with physical frailty contributing most prominently (4.20 ± 1.48) (see Table 3). Additionally, the top three factors that patients with COPD attributed their condition to were smoking, infections and occupational exposures.
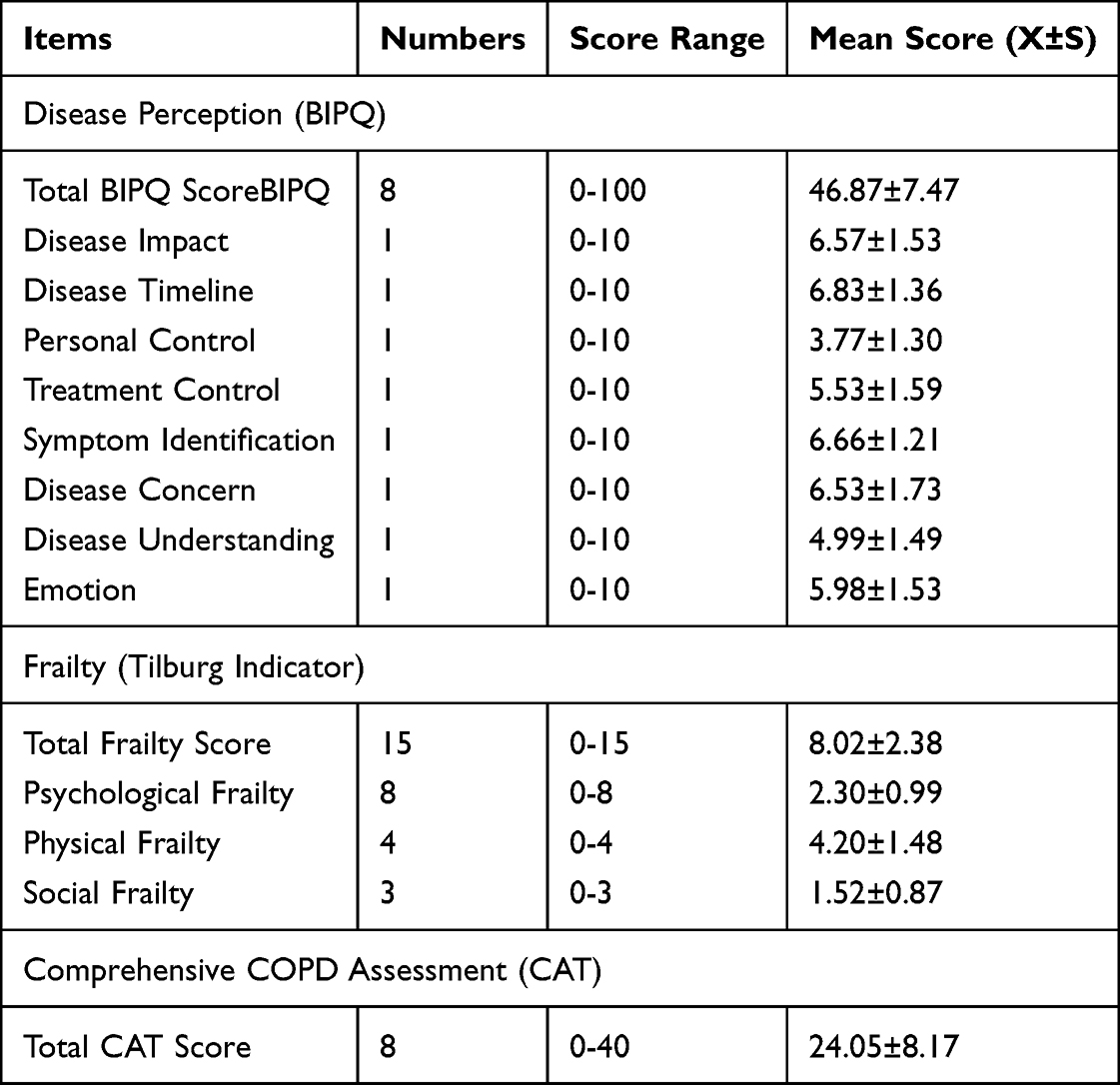 |
Table 3 Scores of BIPQ Scale, Tilburg Scale and CAT Scale in COPD Patients (N=223) |
Analysis of Disease Perception and Frailty Scores Among Patients with COPD with Different Characteristics
The comparative analysis of disease perception and frailty scores among patients with COPD and varying characteristics revealed no statistically significant differences in disease perception scores based on marital status, hospital payment method, family per capita income or smoking status (P > 0.05). However, statistically significant differences were found across different age groups, genders, education levels, disease duration, number of acute exacerbations within 1 year, presence of other chronic diseases, degree of dyspnoea and community management (P < 0.05). Univariate analysis of frailty scores based on general and clinical data showed no significant differences in frailty scores across age, marital status, hospital payment method, family per capita income or smoking status (P > 0.05). Significant differences in frailty scores were observed by gender, education level, disease duration, number of acute exacerbations within 1 year, presence of other chronic diseases, degree of dyspnoea and community management (P < 0.05) (see Table 4).
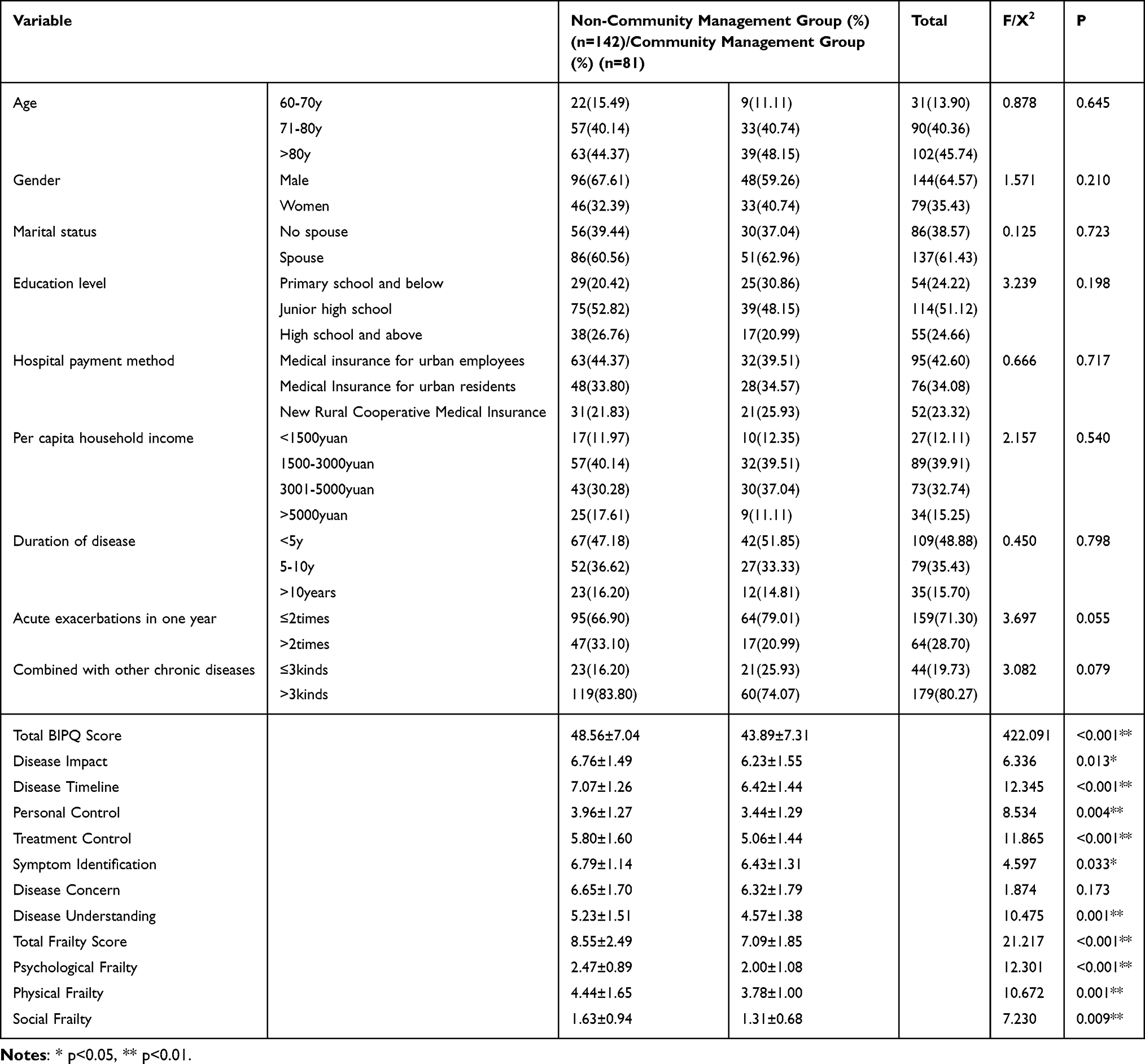 |
Table 4 Comparison of General Information and Scores Between Community Management and Non-Community Management Groups |
Comparisons of General Information and Disease Perception and Frailty Scores Between the Community Management Group and the Non-Community Management Group of Patients with COPD
The results showed no statistically significant differences in age, gender, marital status, education level, hospital payment method, per capita family income, smoking status, disease duration, number of acute exacerbations within 1 year, presence of other chronic diseases or degree of dyspnoea between the community management and non-community management groups (P > 0.05). However, patients in the community management group had significantly lower total disease perception scores (P < 0.01) and frailty scores (P < 0.01) than those in the non-community management group. Subscale analysis indicated greater perceived control, better treatment efficacy and greater emotional stability in the community-managed group (P < 0.05) (see Table 4).
Relationship Analysis Between Disease Perception and Frailty Scores in Elderly Hospitalised Patients with COPD
In this study, correlation analysis was conducted to examine the relationships between the total score of COPD disease perception and its associated factors and the total frailty score and its subdimensions. Pearson’s correlation coefficient was used to indicate the strength of these relationships. A significant positive correlation was observed between the total disease perception score and its components and the total frailty score and its subdimensions, with P < 0.05 (as shown in Table 5).
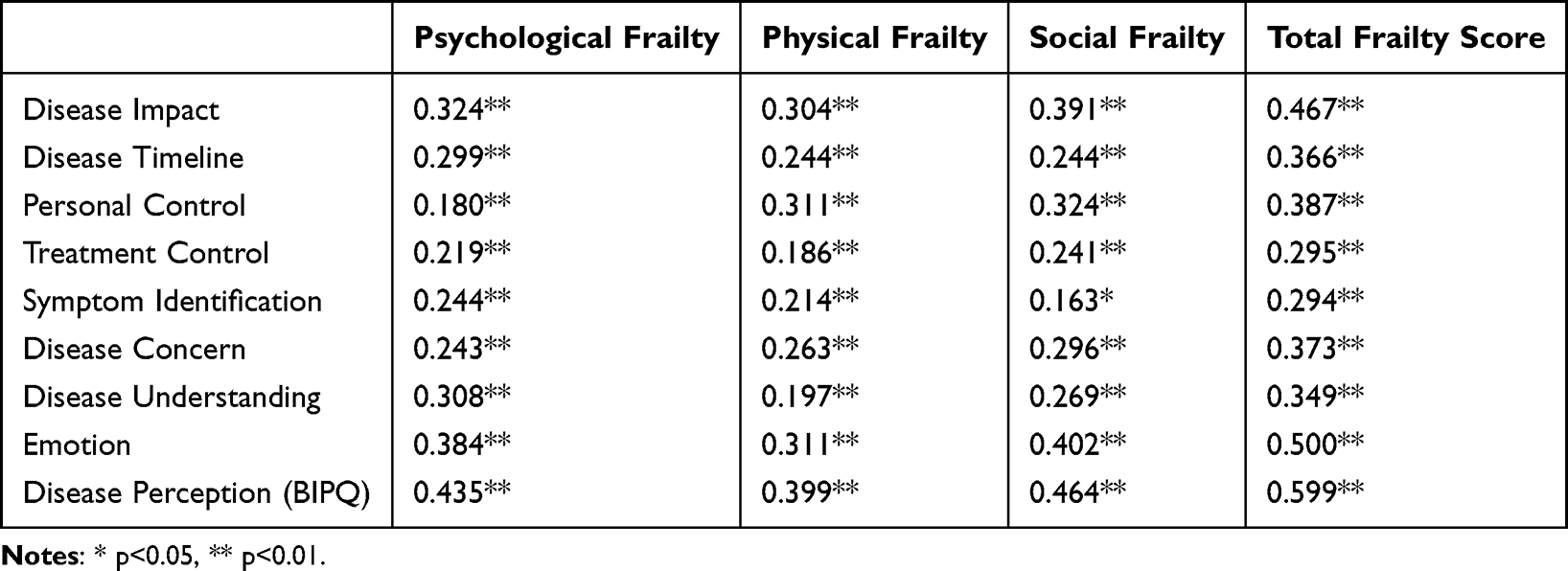 |
Table 5 Comparison of BIPQ Scale Scores Between Groups |
Regression Analysis of the Influencing Factors of Disease Perception in Elderly Hospitalised Patients with COPD
The R-squared value of the model was 0.460, indicating that age, gender, educational attainment, disease duration, the number of acute exacerbations within 1 year, presence of other chronic diseases, degree of dyspnoea, community management, total frailty score and the CAT score explained 46.0% of the variation in the total disease perception score. The model passed the F-test (F = 18.031, P < 0.05), indicating that the results were valid and the model fit well (see Table 6). Multivariate regression identified disease duration (β = 0.28), dyspnoea severity (β = 0.22) and total frailty score (β = 0.19) as significant positive predictors of disease perception (P < 0.05). Community management (β = −0.15) and older age (β = −0.12) were associated with reduced disease perception scores (P < 0.05).
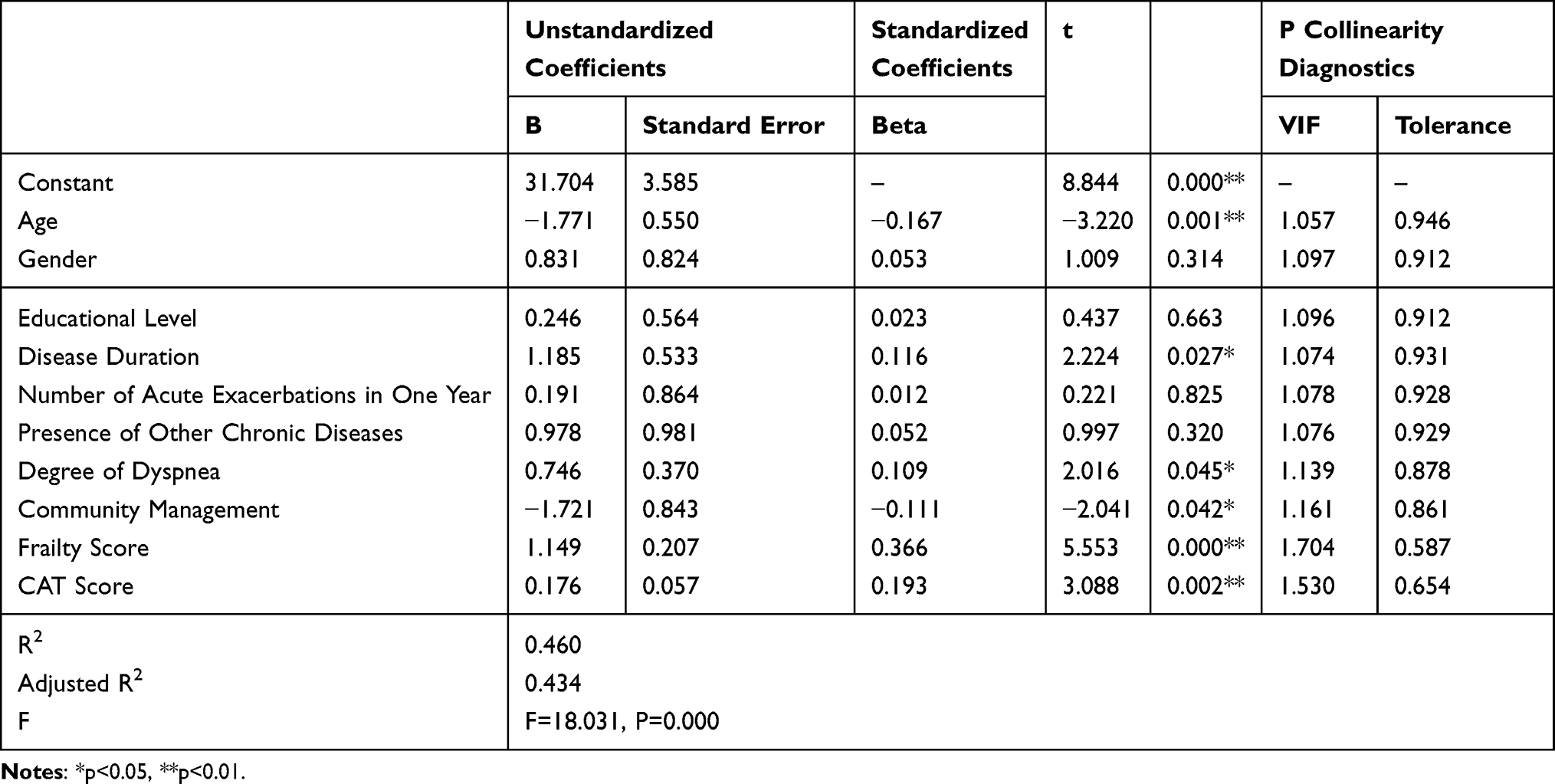 |
Table 6 Linear Regression Analysis Results for COPD Patients (n=223) |
Discussion
Our research contends that COPD is not an isolated respiratory disorder. Factors such as the patient’s age, gender, educational attainment, disease course, frequency of acute exacerbations within a year, number of concurrent chronic diseases, degree of dyspnoea, degree of frailty and whether they have received long-term community chronic disease management all influence disease perception and treatment acceptance.
In this study, patients with COPD demonstrated a moderate perception of disease threat, consistent with findings from similar studies conducted both domestically and internationally.24,25 Among the disease perception factors, items related to disease course, symptom recognition and disease impact were rated highest, whereas understanding and personal control received the lowest scores. A study by Li Sijia et al in Beijing similarly highlighted high scores for concerns about the disease, disease course and symptoms, with relatively low scores for treatment control and emotion.26 Similarly, McInerney’s research on patients with COPD attending community clinics in the United States found that disease course, understanding and treatment control were rated high, whereas emotion and personal control were rated low.5 These findings indicate that the perception of patients with COPD of their condition varies across countries and regions, likely influenced by differences in disease severity and socioeconomic factors such as healthcare access and economic development.
Chronic obstructive pulmonary disease is one of the most debilitating chronic diseases. In this study, frailty was identified as a major factor among patients with COPD, with physical frailty being the most pronounced, followed by psychological frailty.27 These findings align with previous research indicating that frailty negatively impacts biopsychosocial functioning and influences how patients accept and perceive their disease.14 Regarding patients’ views on the causes of COPD, smoking was identified as the most common factor, equally reported by both genders. Other contributing factors included occupational and environmental exposure, stress, genetic susceptibility and infections. This is consistent with findings by Li Sijia et al, who reported smoking, environmental pollution and occupational exposure as the primary causes of COPD. Additionally, they highlighted dyspnoea severity, depressive states and age as key factors influencing disease perception.26 Similarly, Borge et al found that more severe dyspnoea was associated with higher scores in disease outcome, symptom recognition and emotional dimensions, whereas worsening physical and mental health lowered overall quality of life.28
This study also revealed that younger patients exhibited a stronger perception of disease severity. This may be attributed to the multiple pressures faced by younger elderly individuals transitioning into ageing, including role transformations, retirement challenges and diminished social identity. These compounded stressors could amplify their sense of disease threat. Gender differences in disease perception were also observed. Although previous research, such as that by Jankovic et al, noted no substantial difference in total BIPQ scores between male and female patients, women scored higher than men in disease concern and emotional impact, perceiving COPD as a more threatening condition.17 In this study, the higher proportion of male participants may have influenced the observed differences in disease perception, which could be attributed to the convenience sampling method. Finally, disease duration, COPD severity and dyspnoea severity were positively correlated with disease perception, consistent with findings from previous studies.24,25 These results reinforce the critical role of clinical severity and disease progression in shaping patients’ perceptions of COPD.
Some studies have shown that educational level greatly influences self-management behaviours, with lower education associated with poorer disease management. Individuals with limited educational attainment often struggle to acquire and understand health-related information, leading to delays in optimal treatment, recurrent exacerbations and reduced confidence in managing the disease.27 These factors contribute to more negative disease perceptions and hinder effective self-management.
In this study, it was observed that a greater number of chronic comorbidities, longer disease duration and more severe COPD symptoms were associated with higher frailty and disease perception scores. Elderly patients with advanced disease and multiple comorbidities often experience worsening physical health, such as severe dyspnoea, hypoxemia and dependence on long-term oxygen therapy, which negatively impacts mental well-being.26 Studies also highlight that coexisting frailty and COPD are linked to more pronounced respiratory symptoms, increased anxiety and depression, limitations in daily activities and poorer disease-specific quality of life. Frailty is increasingly recognised as a predictor of poor prognosis in patients with COPD.28,29
Psychological frailty, characterised by anxiety and depression, also plays a critical role in shaping disease perceptions. This study found a positive correlation between disease perception and frailty, with patients experiencing greater frailty demonstrating higher disease perception scores.30 In particular, patients in the non-community management group exhibited higher disease perception and frailty scores than those in the community management group, likely due to the lack of regular follow-ups and interventions that community-based programmes provide. Community management may mitigate the psychological and physical burden of COPD by offering consistent support and chronic disease management.
Evidence suggests that psychological factors such as disease perception and emotional responses directly influence daily activities and quality of life. Studies have shown that lower disease perception scores correlate with reduced anxiety and improved quality of life, emphasising the need for psychological interventions in COPD management.15,31 Furthermore, fostering positive disease cognition has been linked to better treatment compliance and satisfaction.17 Therefore, healthcare providers should focus on educating elderly patients about COPD and implement personalised interventions to improve disease understanding, promote self-management behaviours and enhance quality of life.
This study highlights a considerable positive correlation between disease perception and frailty levels in elderly patients with COPD. It also demonstrates that comprehensive community management can greatly reduce disease perception and frailty scores. These findings underscore the critical role of community-based management in improving the overall health of patients with chronic diseases. However, existing literature provides limited insight into the specific mechanisms through which community management influences disease perception and frailty. This study contributes valuable evidence to fill this gap.
Community management offers several advantages in the management of patients with COPD, including regular follow-ups, consistent health education and personalised interventions.32 These interventions ensure better medication adherence, improved symptom management and enhanced patient engagement in self-care. By maintaining close contact with patients, community healthcare teams can promptly identify signs of exacerbation and provide timely intervention, thereby preventing disease progression and reducing hospitalisation rates.33 Moreover, long-term community management programmes foster a supportive environment for patients by involving family members, volunteers and healthcare professionals.34 These findings demonstrate that community-based management programmes, through structured interventions such as regular follow-ups and psychological support, greatly reduce disease perception and frailty scores. This aligns with our regression model, where community management emerged as a negative predictor of heightened disease perception. These results underscore the practical value of integrating community-based care into COPD management protocols. This holistic approach enhances patients’ quality of life and promotes a positive outlook towards disease management.
Clinical Strategies
To further optimise the benefits of community management, the following clinical strategies are proposed.
- Tailored educational programmes: develop customised health education materials targeting different educational levels to improve disease understanding and self-management capabilities.
- Regular psychological support: incorporate routine psychological evaluations and counselling services into community management plans to address mental health issues such as anxiety and depression.
- Technology-driven monitoring: utilise telemedicine platforms and wearable devices for real-time monitoring of symptoms, medication adherence and activity levels, facilitating early intervention for disease exacerbations.
- Multidisciplinary collaboration: strengthen collaboration among pulmonologists, general practitioners and community health workers to deliver comprehensive management plans tailored to individual needs.
- Community engagement: actively involve community volunteers and family members in the management process to provide emotional support and improve patient adherence to management plans.
By implementing these strategies, community management can be further refined to address the unique needs of patients with COPD, ultimately improving clinical outcomes and reducing the burden on healthcare systems. Future research should explore the long-term effects of such interventions to establish evidence-based guidelines for community-based chronic disease management.
Limitations
There are several limitations to our study that warrant consideration. First, although the a priori sample size calculation (n = 200) was met (final n = 223), the study was conducted in a single tertiary hospital in Hefei City, which may limit the generalisability of findings to broader populations, including rural or multicentre cohorts. Future studies should validate these results in diverse settings. Second, this study employed a cross-sectional design, precluding the establishment of causal relationships between variables and preventing the observation of changes over time. Finally, the use of convenience sampling resulted in an overrepresentation of male patients, which may further restrict the generalisability of our results.
Conclusion
This study identifies key predictors of disease perception in elderly patients with COPD and further demonstrates that community-based management greatly reduces disease perception and frailty scores, highlighting its potential to improve disease cognition and mitigate frailty in this population. The results not only provide a new theoretical basis for the community management model of patients with COPD but also offer practical guidance for optimising clinical intervention strategies for patients with chronic disease, which has important innovative and applied value.
Statement
An unauthorized version of the Chinese MMSE®-2 (brief version) was used by the study team without permission, however this has now been rectified with PAR.
The MMSE®-2 (brief version) is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Funding
Hefei Municipal Seventh-Cycle Key Medical Specialty Cultivation Funding Program (Hewei Medical Secretariat [2023] No. 72).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/S2213-2600(24)00413-2
2. Xu J, Ji Z, Zhang P, Chen T, Xie Y, Li J. Disease burden of COPD in the Chinese population: a systematic review. Ther Adv Respir Dis. 2023;17:17534666231218899. doi:10.1177/17534666231218899
3. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
4. Baiardini I, Contoli M, Corsico AG, et al. Exploring the relationship between disease awareness and outcomes in patients with chronic obstructive pulmonary disease. Respiration. 2021;100(4):291–297. doi:10.1159/000513953
5. McInerney GE, Muellers K, O’Conor R, et al. Concordance of patients’ beliefs about chronic obstructive pulmonary disease, their comorbidities, and their medications. Patient Educ Couns. 2020;103(4):677–681. doi:10.1016/j.pec.2019.11.016
6. Marengoni A, Vetrano DL, Manes-Gravina E, et al. The relationship between COPD and frailty: a systematic review and meta-analysis of observational studies. Chest. 2018;154(1):21–40. doi:10.1016/j.chest.2018.02.014
7. Baldi S, Jose PE, Bruschi C, et al. The mediating role of cytokine IL-6 on the relationship of FEV1 upon 6-minute walk distance in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1091–1099. doi:10.2147/COPD.S57845
8. Karpman C, Benzo R. Gait speed as a measure of functional status in COPD patients. Int J Chron Obstruct Pulmon Dis. 2014;9:1315–1320. doi:10.2147/COPD.S54481
9. Backman H, Vanfleteren LEGW, Mannino DM, Ekström M. Severity of airflow obstruction based on FEV1/FVC versus FEV1 percent predicted in the general U.S. population. Am J Respir Crit Care Med. 2024;210(11):1308–1316. doi:10.1164/rccm.202310-1773OC
10. Huang L, Li X, Gu X, et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Lancet Respir Med. 2022;10(9):863–876. doi:10.1016/S2213-2600(22)00126-6
11. An J, Zhou H, Yang T, et al. Relationship of psychological factors with daily activities and quality of life in patients with chronic obstructive pulmonary disease in a Chinese rural population. Ann Palliat Med. 2021;10(2):1675–1684. doi:10.21037/apm-20-1151
12. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
13. Yaqi M, Huiping L, Yajuan Y, et al. Evaluation of the reliability and validity of a simplified Chinese version of the disease perception questionnaire in female patients with breast cancer. J Nursing. 2015;22(24):11–14.
14. Baek MJ, Park YH, Kim S. Comparison between the mini-mental state examination and the mini-mental state examination-2 in patients with mild cognitive impairment and Alzheimer’s disease. J Korean Med Sci. 2025;40(36):e235. doi:10.3346/jkms.2025.40.e235
15. Leitner M, Blum AM, Bals R. Update zu COPD und kardiovaskulären Ereignissen [Update COPD and cardiovascular events]. Dtsch Med Wochenschr. 2025;150(6):298–302. German. doi:10.1055/a-2326-7636
16. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the brief illness perception questionnaire. Psychol Health. 2015;30(11):1361–1385. doi:10.1080/08870446.2015.1070851
17. Jankovic J, Djurdjevic N, Jandric A, et al. The influence of gender differences on the illness perception and women’s point of view on COPD. Bratisl Lek Listy. 2023;124(11):797–801. doi:10.4149/BLL_2023_122
18. Spruit MA, Tan WC. Physical frailty makes matters worse in people with COPD. Chest. 2022;162(1):25–26. doi:10.1016/j.chest.2022.01.049
19. Lee SY, Nyunt MSZ, Gao Q, et al. Co-occurrence of physical frailty and COPD and association with disability and mortality: singapore longitudinal ageing study. Chest. 2022;161(5):1225–1238. doi:10.1016/j.chest.2021.12.633
20. Kennedy CC, Novotny PJ, LeBrasseur NK, Wise RA, Sciurba FC, Benzo RP. Frailty and clinical outcomes in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2019;16(2):217–224. doi:10.1513/AnnalsATS.201803-175OC
21. Uchmanowicz I, Jankowska-Polanska B, Chabowski M, Uchmanowicz B, Fal AM. The influence of frailty syndrome on acceptance of illness in elderly patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2401–2407. doi:10.2147/COPD.S112837
22. Tiemensma J, Gaab E, Voorhaar M, et al. Illness perceptions and coping determine quality oflife in COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:2001–2007. doi:10.2147/COPD.S109227
23. Krzywinski M, Altman N. Multiple linear regression. Nat Methods. 2015;12(12):1103–1104. doi:10.1038/nmeth.3665
24. Santiago LM, Gobbens RJJ, van Assen MALM, Carmo CN, Ferreira DB, Mattos IE. Predictive validity of the Brazilian version of the Tilburg frailty indicator for adverse health outcomes in older adults. Arch Gerontol Geriatr. 2018;76:114–119. doi:10.1016/j.archger.2018.02.013
25. Gobbens RJJ, van der Ploeg T. The prediction of quality of life by frailty and disability among dutch community-dwelling people aged 75 years or older. Healthcare. 2024;12(9):874. doi:10.3390/healthcare12090874
26. Sijia L, Aimin G, Yanwei Z. Analysis of disease perception and its influencing factors among patients with chronic obstructive pulmonary disease. Chinese J Nursing Manag. 2017;17(8):1112–1116.
27. Yijia Z. The correlation between disease perception and quality of life in elderly patients with chronic obstructive pulmonary disease. Henan University, 2021.
28. Borge CR, Moum T, Puline Lein M, et al. Illness perception in people with chronic obstructive pulmonary disease. Scand J Psychol. 2014;55(5):456–463. doi:10.1111/sjop.12150
29. Guo Z, Yang QH, Yang F, et al. Illness perceptions in relation to self-management behaviour among elderly patients with COPD: a cross-sectional study. Int J Nurs Pract. 2024;30(5):e13264. doi:10.1111/ijn.13264
30. Naval E, Gonzalez MC, Giraldos S, et al. Frailty assessment in a stable COPD cohort: is there a COPD-frail phenotype? COPD. 2021;18(5):525–532. doi:10.1080/15412555.2021.1975670
31. Park SK. Frailty in Korean patients with chronic obstructive pulmonary disease, using data from the Korea National Health and Nutrition Examination Survey, 2015 and 2016. Appl Nurs Res. 2021;59:151417. doi:10.1016/j.apnr.2021.151417
32. Jing S, Qian S, Ping Y. Cognitive and psychosocial decline in the elderly. Chinese J Clin Health Care. 2019;25(6):762–766.
33. van der Molen T, van Boven JF, Maguire T, Goyal P, Altman P. Optimizing identification and management of COPD patients - reviewing the role of the community pharmacist. Br J Clin Pharmacol. 2017;83(1):192–201. doi:10.1111/bcp.13087
34. Hu Y, Yao D, Ung COL, Hu H. Promoting community pharmacy practice for chronic obstructive pulmonary disease (COPD) management: a systematic review and logic model. Int J Chron Obstruct Pulmon Dis. 2020;15:1863–1875. doi:10.2147/COPD.S254477
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Frailty and Mortality Risk in COPD: A Cohort Study Comparing the Fried Frailty Phenotype and Short Physical Performance Battery
Brighton LJ, Nolan CM, Barker RE, Patel S, Walsh JA, Polgar O, Kon SSC, Gao W, Evans CJ, Maddocks M, Man WDC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:57-67
Published Date: 20 January 2023
Risk Factors of Readmission Within 90 Days for Chronic Obstructive Pulmonary Disease Patients with Frailty and Construction of an Early Warning Model
Li J, Ma X, Zeng X, Zhou C, Zhu T
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:975-984
Published Date: 23 May 2023
Multidimensional Frailty Instruments Can Predict Acute Exacerbations Within One Year in Patients with Stable Chronic Obstructive Pulmonary Disease: A Retrospective Longitudinal Study
Wei L, Li P, Liu X, Wang Y, Tang Z, Zhao H, Yu L, Li K, Li J, Du M, Chen X, Zheng X, Zheng Y, Luo Y, Chen J, Jiang X, Chen X, Long H
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:859-871
Published Date: 4 April 2024
The Association Between Dietary Magnesium Intake and Frailty in Patients with Chronic Obstructive Pulmonary Disease: National Health and Nutrition Examination Survey
Liang M, Ren X, Zhang Q, Ruan Z, Jin M, Xu Y, Chen X, Qiu Z
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2651-2660
Published Date: 7 December 2024
Impact of Frailty on Major Adverse Cardiovascular Events in Chronic Obstructive Pulmonary Disease
Hamada K, Oishi K, Yamamoto T, Murata Y, Asami-Noyama M, Edakuni N, Hirano T, Abe T, Nakatsui M, Asai Y, Matsunaga K
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3111-3122
Published Date: 4 September 2025