Back to Journals » International Journal of General Medicine » Volume 15
Factors Associated with Unfavorable Functional Outcomes After Intravenous Thrombolysis in Patients with Acute Ischemic Stroke
Authors Satumanatpan N, Tonpho W, Thiraratananukulchai N, Chaichanamongkol P, Lekcharoen P, Thiankhaw K ![]()
Received 15 February 2022
Accepted for publication 17 March 2022
Published 25 March 2022 Volume 2022:15 Pages 3363—3373
DOI https://doi.org/10.2147/IJGM.S362116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Nat Satumanatpan,1,* Warinyupa Tonpho,1,* Nutchanon Thiraratananukulchai,1,* Pheerawat Chaichanamongkol,1,* Pittawat Lekcharoen,1,* Kitti Thiankhaw2,3,*
1Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand; 2Division of Neurology, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand; 3The Northern Neuroscience Center, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand
*These authors contributed equally to this work
Correspondence: Kitti Thiankhaw, Division of Neurology, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, 110 Inthawaroros Road, Sriphum, Chiang Mai, 50200, Thailand, Tel +66 5393 5899, Fax +66 5393 5481, Email [email protected]; [email protected]
Purpose: Intravenous thrombolysis (IVT) has become a standard treatment for eligible ischemic stroke patients. However, functional outcomes after receiving IVT varied widely. Hence the primary goal of this study is to identify characteristics related to poor outcomes.
Patients and Methods: The study enrolled acute ischemic stroke patients aged 18 or older who received IVT within 4.5 hours after onset between January 2018 and December 2020. The data were retrospectively collected from medical records. The patients were classified as having an excellent (0– 2) or poor (3– 6) outcomes based on the 90-day modified Rankin Scale (mRS). Univariable and multivariable logistic regression analyses were used to evaluate the results. The predictive model was determined and developed the score using regression coefficients. The prediction power was validated using the area under the receiver operating characteristic curve analysis.
Results: The study included 138 eligible participants. Forty-eight patients had unfavorable functional outcomes. With multivariable logistic regression analysis, factors significantly associated with poor outcomes were age (adjusted odds ratio (AOR), 1.03; 95% confidence interval (CI), 0.99– 1.07; P = 0.05), diabetes (3.96; 1.61– 9.37; P = 0.003), admission National Institute of Health Stroke Scale (NIHSS) (1.08; 1.01– 1.15; P = 0.02) and initial Alberta Stroke Program Early Computed Tomography Score (ASPECTS) (0.56; 0.37– 0.86; P = 0.009). The predictive model developed from the findings demonstrated good discrimination power (AuROC 0.803, 95% CI 0.728– 0.877).
Conclusion: The current study found that older age, diabetes, atrial fibrillation, higher admission NIHSS, and lower ASPECTS on the initial NCCT brain were related to unfavorable functional outcomes following IVT and served as good predictors of patient functional outcomes.
Keywords: ischemic stroke, intravenous thrombolysis, stroke outcomes
Introduction
Stroke is a prevalent neurological disorder and a significant public health problem globally. There are 80 million stroke cases worldwide, with an annual mortality rate of 5.5 million. The burden of stroke is not only in the high mortality but also in the high morbidity, which results in up to 50% of survivors being permanently impaired.1 Ischemic stroke accounts for the majority of all strokes.1,2 Intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) are two validated reperfusion treatments for acute ischemic stroke (AIS).3 On the other hand, MT is only available in a restricted number of Thai hospitals. As a result, the standard treatment for eligible patients with AIS is IVT with recombinant tissue plasminogen activator (rt-PA). Intravenous rt-PA is generally limited within 4.5 hours of the onset of symptoms, which can enhance the functional outcome of the patients.4–7
However, clinical outcomes differed amongst patients, and a significant number of patients still have poor outcomes despite rt-PA treatment due to individual factors and treatment complications such as IVT-related symptomatic intracerebral hemorrhage (sICH).8 Several factors influencing clinical outcomes are extensively explored, and the findings of the reported studies regarding factors predicting the outcomes for patients receiving rt-PA treatment revealed some inconsistency and a wide range of variability.9–16 Early in the admission process, precise outcome prediction can significantly impact the optimal management approach, and this information is also helpful for informing patients and caregivers about disease progression and prognosis, as this may influence treatment decisions. Therefore, our objective was to identify factors associated with poor outcomes following IVT in patients with acute ischemic stroke and develop a scoring system for predicting functional outcomes based on our findings.
Patients and Methods
Population
The retrospective study was done at Maharaj Nakorn Chiang Mai Hospital, a super tertiary care hospital of the Faculty of Medicine, Chiang Mai University. AIS patients aged 18 years or over who were admitted to the Acute Stroke Unit between January 2018 and December 2020 and received IVT within 4.5 hours after onset were enrolled in the study.
Data Collection and Outcome
The data were collected from the medical records, including demographic characteristics, medical history, laboratory data, TOAST classification, neuroimaging, and clinical outcomes. The clinical outcome was evaluated by the National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), and Barthel Index (BI) at admission, discharge, and 90-day. The complication after treatment as intracranial hemorrhage was recorded, and 90-day mRS presented the functional outcomes. The patients who had mRS scores from 0–2 were classified as having excellent functional outcomes, while an mRS score of more than 2 was an unfavorable functional outcome.
Statistical Analysis
Categorical variables are presented as numbers and proportions, while continuous variables are presented as mean with standard deviation or median with the interquartile range depending on data distribution. Pearson χ2 test, Fischer’s exact 2-sided test, Student’s t-test, or Mann Whitney U (Wilcoxon rank-sum) test were used when appropriate. Univariable and multivariable logistic regression analyses were performed to detect factors associated with unfavorable functional outcomes after IVT.
In the predictive model, the significant predictors were weighted by their coefficient, converted to item score by dividing each variable coefficient with the smallest coefficient number, rounding to the nearest integer, and adding a total predictive score. A receiver operating characteristic (ROC) curve was plotted to evaluate a discriminatory power of predictive score and determine a cut-off value. Hosmer-Lemeshow goodness of fit test was also done to measure the performance of the predictive model. The sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio of this model were performed. The area under the receiver operating characteristic (AuROC) was calculated to evaluate test accuracy. The significant level was defined as a P-value less than 0.05. All analyses were performed by licensed Stata statistical software version 16.1.
Results
Demographics and Neuroimaging Parameters
A total of 138 eligible patients were enrolled in the study (Figure 1). The baseline characteristics of the enrolled patients are shown in Table 1 based on functional outcome classification. Patients with unfavorable functional outcomes had a 12.8 years higher age than those with excellent functional outcomes (74.9 vs 62.1 years, respectively, P < 0.001) and had more prevalent large-artery atherosclerosis (LAA) and cardioembolism (CE) of stroke etiology. Previous medical history, including hypertension, diabetes, dyslipidemia, and atrial fibrillation (AF) was also significantly higher in patients with unfavorable functional outcomes (84.8%, 54.4%, 63.0%, 30.4%, respectively). Patients with initially severe stroke, assessed by NIHSS, mRS, and BI had 90-day unfavorable functional outcomes. Initial and fasting plasma glucose was found to be significantly higher in those with unfavorable functional outcomes.
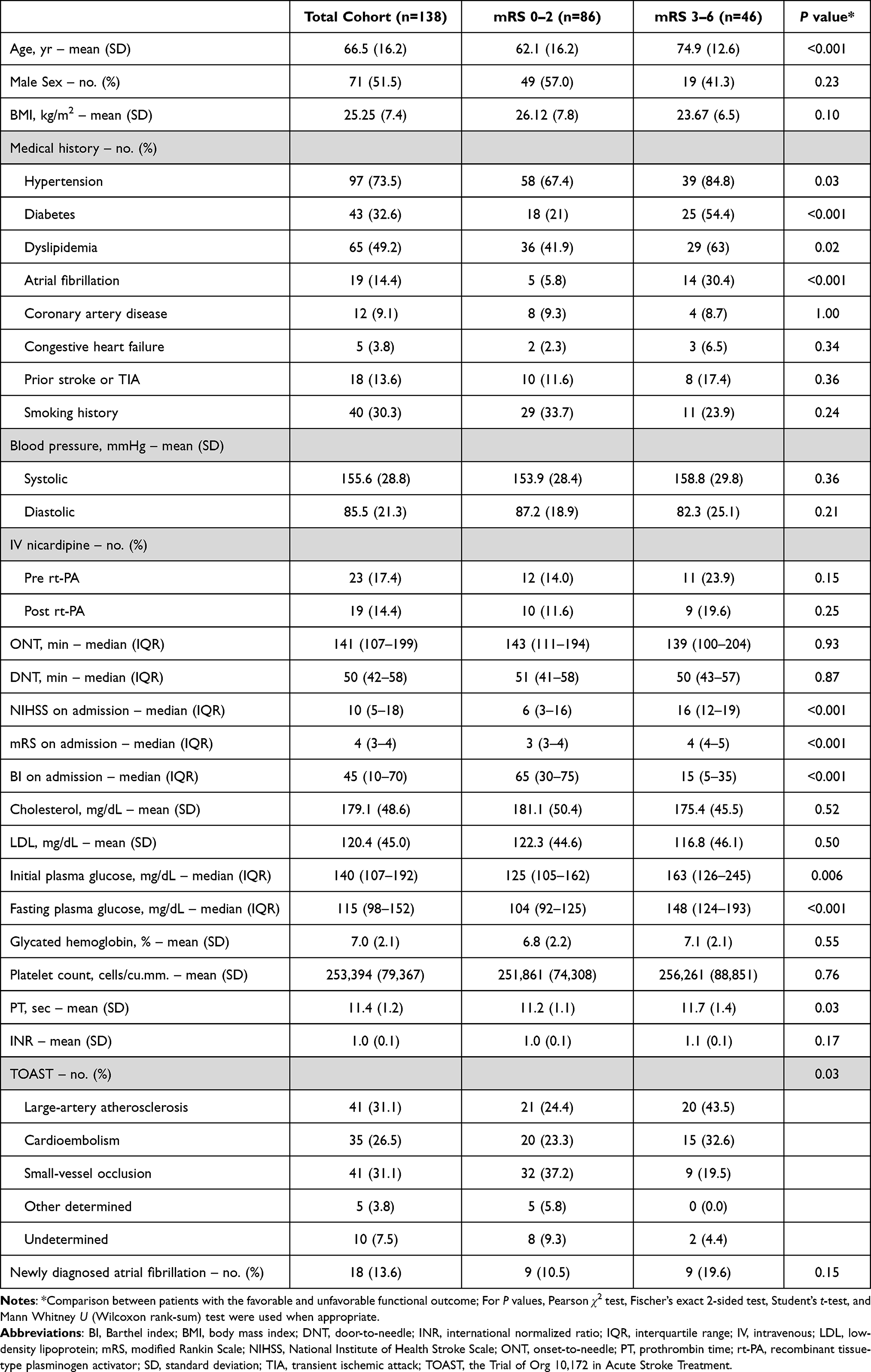 |
Table 1 Baseline Characteristics of Acute Stroke Patients According to Functional Outcomes |
 |
Figure 1 Study flow chart and patient selection procedure. |
Table 2 demonstrated neuroimaging parameters of the enrolled patients according to functional outcomes. Patients with unfavorable functional outcomes had a higher proportion of early infarction signs and hyperdense middle cerebral artery (MCA) sign on initial non-contrast computed tomography (NCCT) brain and significantly lower ASPECTS, the Alberta Stroke Program Early Computed Tomography Score, 10 vs 9, P < 0.001. In addition, there were significant associations with a more length of hyperdense MCA sign and a lower rate of clot disappearance following IVT in those with unfavorable functional outcomes.
 |
Table 2 Neuroimaging Parameters According to Functional Outcomes |
Regression Analysis
Univariable analysis and multivariable logistic regression analysis are shown in Tables 3 and 4. Five independent variables were associated with unfavorable functional outcomes following IVT including, diabetes (adjusted Odds ratio (AOR), 3.96; 95% confident interval (CI), 1.61 to 9.33; P = 0.003), admission NIHSS (1.08; 1.01 to 1.15; P = 0.02), ASPECTS (0.56; 0.37 to 0.86; P = 0.009), age (1.03; 0.99 to 1.07; P = 0.05), and AF (2.94; 0.90 to 9.67; P = 0.07).
 |
Table 3 Univariable Analysis Variables Associated with Unfavorable Functional Outcomes |
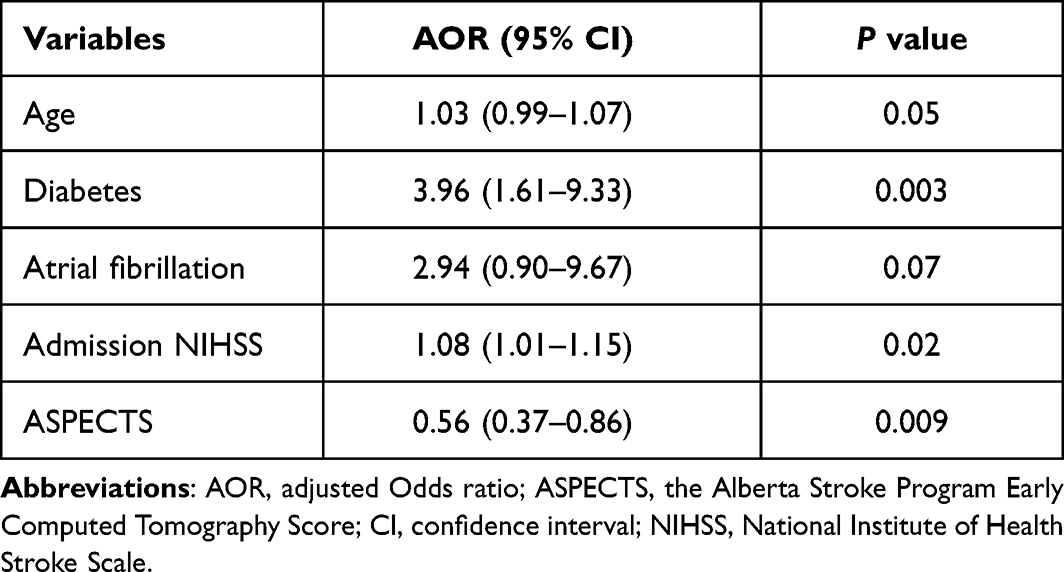 |
Table 4 Multivariable Logistic Regression Analysis Variables Associated with Unfavorable Functional Outcomes |
Model Development
The significant predictors and assigned item scores are performed in Table 5 to show the correlation between variables and a total predictive score of unfavorable outcomes after IVT in AIS patients. As shown, there were five remaining independent variables; age, diabetes, AF, admission NIHSS, and ASPECTS. Age in years was divided into two groups (greater than or equal to 75 = 1, less than 75 = 0). Admission NIHSS was divided into three groups according to the stroke severity (minor (0–5 points) = 0, moderate (6–16 points) = 1, severe (>16 points) = 2). According to early infarction signs on neuroimaging, ASPECTS was divided into two groups (equal to 10 = 1, less than 10 = 0).
 |
Table 5 Significant Predictors and Assigned Item Scores for Unfavorable Functional Outcomes After IVT |
Age, diabetes, AF, and admission NIHSS directly vary to predictive score, whereas ASPECTS has an inverse variation. In the predictive model, an age variable has the smallest coefficient number. The predictive score will increase by 1 point if the patients’ age is greater than or equal to 75. The patient who had diabetes will increase the score by 6 points, while AF will increase by 5 points. The patient whose admission NIHSS is more than 5, will increase the score by 8 points. When ASPECTS equal to 10 will decrease the score by 4 points. The higher the predictive score, the more likelihood of unfavorable outcomes after IVT.
Model Validation
The receiver operating characteristics analysis (ROC) suggests that the total predictive score is accurate (0.69 sensitivity, 0.75 specificity) at the cut-point of 13 (Supplementary Table S1). In other words, patients with unfavorable functional outcomes were correctly predicted at 69%, whereas those with excellent functional outcomes were correctly predicted at 75%. The probability of having a total score greater than or equal to 13 points in the unfavorable functional outcome group is more than another group 2.85 times (LR+ 2.85), whereas the unfavorable functional outcome group has 0.4 times compared to the excellent functional outcome group in the probability of having a total score less than 13 points (LR- 0.403). At the 0.35 prevalence of unfavorable functional outcome following IVT, the patient with poor outcome was correctly predicted with low accuracy (0.60 positive predictive value) when a patient with excellent outcome was excluded with moderate accuracy (0.82 negative predictive value). A total score from the developed scoring system predicts poor outcomes after IVT with good validity, AUC was 0.8026 (95% CI 0.728 to 0.877) (Figure 2) and good calibration (Hosmer-Lemeshow goodness of fit; χ2 = 23.22, P value = 0.0016) (Supplementary Figure S1).
 |
Figure 2 Area under receiver operating characteristics (AuROC) curve of a predictive score for predicting the unfavorable functional outcomes after IVT in acute ischemic stroke. |
Discussion
According to AHA/ASA 2019 guidelines, IVT with alteplase has been first-line reperfusion therapy in acute ischemic stroke.7 In Thailand, after successfully introducing of the first IVT in 1996, the “stroke fast track” system was initiated and developed and a more significant number of acute stroke patients were identified and received IVT within the golden time window of 4.5 hours. The percentage of patients receiving IVT for acute ischemic stroke in Thailand is continuously increasing from 0.38% in 2008 to 4.78% in 2016. This percentage varies between the centers, as high as 15–16% in some tertiary care centers.17 Still, not everyone that receives treatment always has an excellent functional outcome. Hence, our study objective is to find which factor in the patient is associated with unfavorable outcomes after IVT because each person has a different background and characteristics. Our study found that the unfavorable outcome (mRS >2) at discharge was 33.33%, and symptomatic intracranial hemorrhage (sICH) occurred after administration of IV alteplase for treatment of AIS was 4.38%. Complications after treatment as sICH were of concern to physicians because of increased hospital stay and cost, leading to poor recovery after treatment.
Older age, diabetes, AF, high admission NIHSS, and low ASPECTS contributed to be the independent factors associated with unfavorable outcomes after IVT in AIS patients. Diabetes was recognized as one significant risk factor for developing unfavorable outcomes due to impaired blood-brain barrier and microvascular.18 Among 12,686 patients with ischemic stroke from Nikneshan et al’s study found higher death and disability at discharge and long-term mortality in patients with diabetes, but there was no difference in the risk of ICH after IVT.19 The study by Tang et al, which included 419 patients, found that AIS with diabetes had unfavorable neurological outcomes associated with incomplete recanalization after IVT due to hyperglycemia that affects coagulation activation and hyperinsulinemia which increases plasminogen activator inhibitor and leads to hyperfibrinolysis.20,21
AF is another significant risk factor associated with unfavorable outcomes in several studies.22–27 A study by Findler et al with 214 stroke patients found more favorable outcomes in the non-AF than in the AF because thrombus from AF in the atrium was mainly composed of erythrocytes due to slow flow which induced cardioembolic stroke while thrombus in the vessel was composed of fibrin and platelets that correlated to rt-PA mechanisms with less probability to cause rt-PA resistance to compare with cardioembolic stroke.25 Padjen et al, who include 734 AIS patients, found that AF has a worse outcome than those without because of old age and severe stroke at admission.24 Saposnik et al included 12,686 patients found that AF patients had a higher risk of death at 30-day, 1-year, and death or disability at discharge more than non-AF patients.26 A meta-analysis of 8509 patients not only found the same trend as the previous study but also found that AF with stroke increases the risk of ICH due to large infarct size, poor collateral circulation, and large or old thrombi, which lead to IVT resistance, some AF patients may receive the anticoagulant drug before IVT which will increase bleeding risk.23 Cardioembolism due to AF was recognized as one of the predictors for early parenchymal hemorrhagic transformation, related to unfavorable outcomes following IVT.28 In comparison, Frank et al included 77,091 patients, which found that AF is not an independent predictor of unfavorable outcomes.22 In addition, Zhao et al had 267 ischemic stroke patients who found that IVT was beneficial for ischemic stroke with AF. The reason for worse outcomes in stroke patients with AF after rt-PA was that most AF patients were older and had more severe dysfunction at baseline.27
Our study finds that the age of 75 years or older, the more likely poor outcome that assigned score 1. According to previous studies, advanced age is associated with unfavorable outcomes.15,29–31 This is likely to be an effect of comorbidity and greater stroke severity which are found in advancing age. A retrospective study in 88 patients showed that advanced age is related to poor functional outcomes.15 A meta-analysis of nine studies in 3391 patients found no statistical difference of unfavorable outcomes in two age groups, 18–80 years old and more than 80 years old, which receive rt-PA within 0 to 3 hours. The patients whose ages were more than 80 years old seemed to have a higher risk of unfavorable outcomes if they received rt-PA between 3 to 4.5 hours after stroke onset.31 In Thai stroke population, elderly patients over 70 years may carry a higher risk of mortality when treated with IVT.32 In contrast, another prospective study in 121 patients found that age was not statistically associated with unfavorable outcomes following multivariable analysis, but NIHSS at admission and deep MCA infarction are independent factors predicting unfavorable outcomes.30 Our finding was consistent with many studies that advancing age (>80 years old) had an impact on post thrombolytic therapy poor outcomes. However, thrombolysis treatment for patients presenting with AIS should be evaluated on an individual benefit-risk basis. Notably, age alone is no longer a barrier to rt-PA treatment for AIS.29
Admission NIHSS is also a predictive factor in many studies.12,33,34 A Chinese case series study in 101 patients found that patients with lower NIHSS at admission tend to have favorable outcomes following rt-PA.12 A prospective study on 269 Chinese patients found that the higher NIHSS indicated a five times higher risk of unfavorable functional outcomes.34 Our study divided admission NIHSS into three groups, including mild (0–5 points), moderate (6–16 points), severe (>16 points). The finding were consistent with other studies in which admission NIHSS of less than 7 was a predictive factor for an excellent functional outcome [30]. In contrast, NIHSS of greater than 20 to 25 predict a high probability of ICH due to large infarction size.35
ASPECTS is a topographic brain NCCT scan score. Due to the indication for receiving rt-PA, a high proportion of patients in our study have ASPECTS of 8 to 10, resulting in selection bias. Consequently, we categorized the patients’ ASPECTS into two groups: those with a score of 10 and those with less than 10. Our study found that an ASPECTS equal to 10 is a favorable factor which corroborates previous research indicating that patients with an ASPECTS less than 8 after thrombolysis did not have a favorable clinical outcome at three months, defined by mRS of 2 or less.36 A study by Das et al discovered that lower ASPECTS are independently linked with cerebral bleeding following rt-PA.10
Our study found that the total predictive score is accurate (0.69 sensitivity, 0.75 specificity) at the cut-point of 13. This finding was consistent with a previously published scoring system for predicting outcomes post-IVT, however, some predictive score systems have more than five associated factors, and these systems still have some limitations in the aspect of sICH. They do not include other poor outcomes that include morbidity and mortality. As shown in a study conducted in Thailand, the existing sICH risk score was not applicable for the Thai population.37 In addition, our findings provide an accurate predictive model in Thai stroke patients. Apart from onset to treatment time, in-hospital complications, and elderly age, clinical and neuroimaging parameters from our model illustrate important prognostic factors related to functional outcomes after stroke.17,32,38 Besides these predictive models, we should be focused on stroke screening, prevention, and a better control system to improve stroke patients’ outcomes. Recently, fascinating data from China Stroke Prevention Project Committee (CSPPC) provides an unquestionable benefit of three 1-h gold rescue circles (less than 1-h for onset to call time, pre-hospital transfer time, and door-to-needle time) for stroke treatment and should be further promoted worldwide, especially for other developing countries, to improved stroke care.39
Our predictive model demonstrated good discriminatory ability (AuROC 0.803; 95% CI 0.728 to 0.877). Therefore, we expect that the scoring system developed from this model may predict functional outcomes of patients with AIS after IVT has been administered. A better understanding of the factors associated with poor outcomes, along with the use of a predictive tool such as ours in the initial evaluation, may aid in prognosis estimation, clinical decision-making for patients and caregivers regarding the risks and benefits of IVT, and performance improvement of health-care providers by directing monitoring strategies and additional appropriate management interventions. The study has some limitations, including the retrospective collection of data from electronic medical records, which excluded some variables such as 3-month post-stroke outcomes due to missing data and loss to follow-up. Additionally, the sample size was relatively small, as only those who met the criteria of the study were enrolled. This could lead to inadequate statistical power to establish clear associations between certain variables and unfavorable functional outcomes, as well as wide confidence intervals. To validate our findings and increase the precision of the predictive model, we suggest that more prospective studies with a larger sample size be done in the future.
Conclusion
Regarding the findings of the current study, the role of factors including older age, diabetes, AF, a higher admission NIHSS, and a lower ASPECTS on the initial NCCT brain are confirmed to be associated with a greater risk of experiencing unfavorable functional outcomes in the population of Thai acute ischemic stroke patients after treatment with IVT. IVT with alteplase remains the primary approach to stroke reperfusion therapy, while the findings of this study might provide important information regarding the prognostic factors related to functional outcomes after stroke.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary Materials.
Ethical Approval and Informed Consent
The Research Ethics Committees of the Faculty of Medicine, Chiang Mai University, approved this study protocol (Study Code: HOS-2564-07876). The requirement for informed consent was waived because the retrospective and non-interventional study collected data from previous electronic medical record, and did not involve personal privacy and commercial interests. The study involves no more than minimal risk to subjects, and the waiver will not adversely affect the rights and welfare of the subjects. The data were anonymized or maintained with confidentiality. The publication of this study is in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors contributed equally to this manuscript.
Funding
No funding was received for the carrying out of this study and preparing the manuscript.
Disclosure
The authors have no conflicts of interest for this work to declare.
References
1. Donkor ES. Stroke in the 21 (st) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. 2018;2018:3238165. doi:10.1155/2018/3238165
2. Lindsay MP, Norrving B, Sacco RL, et al. World Stroke Organization (WSO): global stroke fact sheet 2019. Int J Stroke. 2019;14(8):806–817. doi:10.1177/1747493019881353
3. Rabinstein AA. Update on treatment of acute ischemic stroke. Continuum. 2020;26(2):268–286. doi:10.1212/CON.0000000000000840
4. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
5. Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N Engl J Med. 2019;380(19):1795–1803. doi:10.1056/NEJMoa1813046
6. Suwanwela NC. Stroke epidemiology in Thailand. J Stroke. 2014;16(1):1–7. doi:10.5853/jos.2014.16.1.1
7. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: a Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
8. Yaghi S, Eisenberger A, Willey JZ. Symptomatic intracerebral hemorrhage in acute ischemic stroke after thrombolysis with intravenous recombinant tissue plasminogen activator: a review of natural history and treatment. JAMA Neurol. 2014;71(9):1181–1185. doi:10.1001/jamaneurol.2014.1210
9. Chen Y-W, Sung S-F, Chen C-H, et al. Intravenous thrombolysis administration 3–4.5 h after acute ischemic stroke: a retrospective, multicenter study. Front Neurol. 2019;10:1038. doi:10.3389/fneur.2019.01038
10. Das S, Mondal GP, Bhattacharya R, et al. Predictors of postthrombolysis outcome and symptomatic postthrombolysis hemorrhage following intravenous thrombolysis with alteplase for acute ischemic stroke. J Neurosci Rural Pract. 2020;11(2):315–324. doi:10.1055/s-0040-1709946
11. Goyal M, Almekhlafi M, Dippel DW, et al. Rapid alteplase administration improves functional outcomes in patients with stroke due to large vessel occlusions. Stroke. 2019;50(3):645–651. doi:10.1161/STROKEAHA.118.021840
12. Huang YH, Zhuo ST, Chen YF, et al. Factors influencing clinical outcomes of acute ischemic stroke treated with intravenous recombinant tissue plasminogen activator. Chin Med J. 2013;126(24):4685–4690.
13. Mehrpour M, Afrakhte M, Shojaei SF, et al. Factors predicting the outcome of intravenous thrombolysis in stroke patients before rt-PA administration. Caspian J Intern Med. 2019;10(4):424–430. doi:10.22088/cjim.10.4.424
14. Tang H, Yan S, Wu C, Zhang Y. Characteristics and outcomes of intravenous thrombolysis in mild ischemic stroke patients. Front Neurol. 2021;12:1915. doi:10.3389/fneur.2021.744909
15. Cetiner M, Aydin HE, Guler M, Canbaz Kabay S, Zorlu Y. Predictive factors for functional outcomes after intravenous thrombolytic therapy in acute ischemic stroke. Clin Appl Thromb Hemost. 2018;24(9_suppl):171S–177S. doi:10.1177/1076029618796317
16. Torres-Aguila NP, Carrera C, Muino E, et al. Clinical variables and genetic risk factors associated with the acute outcome of ischemic stroke: a systematic review. J Stroke. 2019;21(3):276–289. doi:10.5853/jos.2019.01522
17. Suwanwela NC, Chutinet A, Kijpaisalratana N. Thrombolytic treatment in Thailand. J Stroke Med. 2018;1(1):41–44. doi:10.1177/2516608518777934
18. Hawkins BT, Lundeen TF, Norwood KM, Brooks HL, Egleton RD. Increased blood-brain barrier permeability and altered tight junctions in experimental diabetes in the rat: contribution of hyperglycaemia and matrix metalloproteinases. Diabetologia. 2007;50(1):202–211. doi:10.1007/s00125-006-0485-z
19. Nikneshan D, Raptis R, Pongmoragot J, et al. Predicting clinical outcomes and response to thrombolysis in acute stroke patients with diabetes. Diabetes Care. 2013;36(7):2041–2047. doi:10.2337/dc12-2095
20. Tang H, Zhang S, Yan S, et al. Unfavorable neurological outcome in diabetic patients with acute ischemic stroke is associated with incomplete recanalization after intravenous thrombolysis. J Neurointerv Surg. 2016;8(4):342–346. doi:10.1136/neurintsurg-2014-011643
21. Desilles JP, Meseguer E, Labreuche J, et al. Diabetes mellitus, admission glucose, and outcomes after stroke thrombolysis: a registry and systematic review. Stroke. 2013;44(7):1915–1923. doi:10.1161/STROKEAHA.111.000813
22. Frank B, Fulton R, Weimar C, Shuaib A, Lees KR. Impact of atrial fibrillation on outcome in thrombolyzed patients with stroke: evidence from the Virtual International Stroke Trials Archive (VISTA). Stroke. 2012;43(7):1872–1877. doi:10.1161/STROKEAHA.112.650838
23. Hu Y, Ji C. Efficacy and safety of thrombolysis for acute ischemic stroke with atrial fibrillation: a meta-analysis. BMC Neurol. 2021;21(1):66. doi:10.1186/s12883-021-02095-x
24. Padjen V, Bodenant M, Jovanovic DR, et al. Outcome of patients with atrial fibrillation after intravenous thrombolysis for cerebral ischaemia. J Neurol. 2013;260(12):3049–3054. doi:10.1007/s00415-013-7119-4
25. Findler M, Molad J, Bornstein NM, Auriel E. Worse outcome in patients with acute stroke and atrial fibrillation following thrombolysis. Isr Med Assoc J. 2017;19(5):293–295.
26. Saposnik G, Gladstone D, Raptis R, et al. Atrial fibrillation in ischemic stroke: predicting response to thrombolysis and clinical outcomes. Stroke. 2013;44(1):99–104. doi:10.1161/STROKEAHA.112.676551
27. Zhao Q, Li X, Dong W, et al. Factors associated with thrombolysis outcome in ischemic stroke patients with atrial fibrillation. Neurosci Bull. 2016;32(2):145–152. doi:10.1007/s12264-016-0019-8
28. Paciaroni M, Agnelli G, Corea F, et al. Early hemorrhagic transformation of brain infarction: rate, predictive factors, and influence on clinical outcome: results of a prospective multicenter study. Stroke. 2008;39(8):2249–2256. doi:10.1161/STROKEAHA.107.510321
29. Bluhmki E, Danays T, Biegert G, Hacke W, Lees KR. Alteplase for acute ischemic stroke in patients aged >80 years: pooled analyses of individual patient data. Stroke. 2020;51(8):2322–2331. doi:10.1161/STROKEAHA.119.028396
30. Kim DH, Lee DS, Nah HW, Cha JK. Clinical and radiological factors associated with unfavorable outcome after intravenous thrombolysis in patients with mild ischemic stroke. BMC Neurol. 2018;18(1):30. doi:10.1186/s12883-018-1033-4
31. Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929–1935. doi:10.1016/S0140-6736(14)60584-5
32. Dharmasaroja PA, Muengtaweepongsa S, Dharmasaroja P. Intravenous thrombolysis in Thai patients with acute ischemic stroke: role of aging. J Stroke Cerebrovasc Dis. 2013;22(3):227–231. doi:10.1016/j.jstrokecerebrovasdis.2011.08.001
33. Wouters A, Nysten C, Thijs V, Lemmens R. Prediction of outcome in patients with acute ischemic stroke based on initial severity and improvement in the first 24 h. Front Neurol. 2018;9:308. doi:10.3389/fneur.2018.00308
34. Wu Z, Zeng M, Li C, et al. Time-dependence of NIHSS in predicting functional outcome of patients with acute ischemic stroke treated with intravenous thrombolysis. Postgrad Med J. 2019;95(1122):181–186. doi:10.1136/postgradmedj-2019-136398
35. Fugate JE, Rabinstein AA. Absolute and relative contraindications to IV rt-PA for acute ischemic stroke. Neurohospitalist. 2015;5(3):110–121. doi:10.1177/1941874415578532
36. Aviv RI, Mandelcorn J, Chakraborty S, et al. Alberta stroke program early CT scoring of CT perfusion in early stroke visualization and assessment. AJNR Am J Neuroradiol. 2007;28(10):1975–1980. doi:10.3174/ajnr.A0689
37. Kunadison S, Nganwai R. Comparison of accuracy among post-thrombolytic symptomatic intracerebral hemorrhage predictive scores in ischemic stroke patients in Khon Kaen Hospital. J Thai Stroke Soc. 2020;19(3):17.
38. Kongbunkiat K, Kasemsap N, Thepsuthammarat K, Tiamkao S, Sawanyawisuth K. National data on stroke outcomes in Thailand. J Clin Neurosci. 2015;22(3):493–497. doi:10.1016/j.jocn.2014.08.031
39. Chao B-H, Yan F, Hua Y, et al. Stroke prevention and control system in China: CSPPC-Stroke Program. Int J Stroke. 2021;16(3):265–272. doi:10.1177/1747493020913557
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.